")
Back to Journals » Infection and Drug Resistance » Volume 18
18F-FDG PET/CT Imaging of Talaromyces marneffei Infection with Bone Destruction in an HIV-Negative Patient: Case Report and Review
Authors He W, Wang S, Xiong X, Dai W
Received 7 January 2025
Accepted for publication 2 April 2025
Published 8 April 2025 Volume 2025:18 Pages 1745—1752
DOI https://doi.org/10.2147/IDR.S516105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wenting He,1 Senhui Wang,1 Xiaoqi Xiong,2 Wenli Dai1
1Department of Nuclear Medicine, The First College of Clinical Medical Science, China Three Gorges University, Yichang, Hubei, 443003, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, The First College of Clinical Medical Science, China Three Gorges University, Yichang, Hubei, 443003, People’s Republic of China
Correspondence: Wenli Dai, Department of Nuclear Medicine, The First College of Clinical Medical Science, China Three Gorges University, Yichang, Hubei, 443003, People’s Republic of China, Email [email protected]
Background: Talaromycosis is an opportunistic fungal infection caused by Talaromyces marneffei (T. marneffei), commonly occurs in HIV-positive individuals. While less common, it can also affect HIV-negative individuals. We reported a T. marneffei infection in an HIV-negative patient, whose imaging findings and diagnostic process offer valuable clinical insights.
Case Presentation: An HIV-negative male adult patient with an intermittent cough for more than two years and worsened for more than one month. Enhanced CT scan indicated lung cancer with rib and lymph nodes metastasis. The lower respiratory tract and bronchial lavage fluid culture of the patient were negative. He received two bronchoscopies, two biopsies and two metagenomic next-generation sequencing (mNGS) tests, which failed to find the malignant cell but sequentially identified the presence of Pasteurella multocida and the Epstein-Barr virus. His condition did not improve after anti-infective treatment for 2weeks. An 18-fluorodeoxy glucose (18F-FDG) PET/CT scan revealed increased radioactivity in right supraclavicular lymph node, left lung and the right tenth rib. Ultimately, a biopsy at the hypermetabolic lesion of left lung, and a third mNGS test confirmed the presence of Talaromyces marneffei. Subsequently, the patient started antifungal therapy with amphotericin B and itraconazole and showed a favorable response.
Conclusion: We reviewed all reported PET/CT findings of T. marneffei infection patients, suggesting that fungus T. marneffei should be considered in patients identified as infection and exhibited bone destruction and also highlight the role of PET/CT in guiding the biopsy site.
Keywords: Talaromyces marneffei, PET/CT, HIV-negative, bone destruction, metagenomic next-generation sequencing (mNGS)
Introduction
T. Marneffei is a thermally dimorphic fungus that was initially isolated from bamboo rats1 and is generally accepted to infect people by inhaling T. Marneffei conidia. T. Marneffei predominantly affects the monocyte-macrophage system and can easily spread throughout the body due to macrophage paradox effect2 and their capacity to alter macrophage polarisation3 which could evade clearance by the immune system. In addition, insufficient understanding of T. Marneffei infection and lack of specific clinical manifestation and imaging characteristics may result in delayed diagnosis and high death rate. The number of T. Marneffei infections reported worldwide has steadily increased recent years, primarily in southeast Asia, southern China, and northeastern India.4 T. Marneffei infection commonly occurs in patients with human immunodeficiency virus infection (HIV). However, there is a rising incidence of HIV-negative individuals contracting the disease, and even people with healthy immune systems are infected. We present a case of T. Marneffei infection in an HIV-negative patient, the diagnostic process was complicated, and the patient showed a positive response to the treatment.
Case Presentation
A 61-year-old male patient presented with an intermittent cough for more than two years, and it had gotten worse during the last month. One month previously, the patient discovered a Pasteurella pneumotropica infection after a bronchoscopy and an alveolar lavage fluid mNGS analysis in outside facility. No improvement has been observed despite over two weeks of anti-infective treatment. He was revealed having pneumonia caused by Legionella pneumophila, hypertension, severe anemia, and had a history of smoking and alcohol use, alongside blood transfusions. He denied any family history of the condition and occupation history were unremarkable. Physical examination revealed a palpable lump on the right thoracic wall, along with localized pain. Breath sounds in both lungs exhibited coarse qualities, with no dry or wet rales detected.
Laboratory findings reported the following: white blood cell, 10.80×10^9/L (normal range: 3.5–9.5×10^9/L); red blood cell, 3.75×10^12/L (normal range: 4.3–5.8×10^12/L); neutrophil, 8.40×10^9/L (normal range: 1.8–6.3×10^9/L); hemoglobin, 104g/L (normal range: 130–175g/L); total protein, 85.80g/L (normal range: 65–85g/L); albumin, 39.00g/L (normal range: 40–55g/L); globulin, 46.80g/L (normal range: 20–40g/L); glucose, 9.43mmol/L(normal range: 3.9–6.1mmol/L); and C-reactive protein, 119.69mg/L(normal range: 0–6mg/L). The squamous cell carcinoma antigen was measured at 3.7ng/mL (normal range: 0–2.7ng/mL). Antibody tests for HIV, HBV, HCV, EBV and TP were negative, TSPOT, TB-DNA, G test, lower respiratory tract sputum culture and bronchial lavage fluid culture indicated no abnormalities.
An enhanced CT scan showed a new mass in the left lower lung, multiple enlarged lymph nodes and bone destruction in the right tenth rib. Lung cancer with metastasis was suspected. Tumor cells were not found in bronchoscopy. The patient had two percutaneous lung punctures, which revealed inflammatory cell infiltration. A following mNGS tests indicated Epstein-Barr virus. Despite receiving piperacillin-tazobactam and moxifloxacin for 10 days, respectively, the patient’s condition did not improve. A positron emission tomography/computed tomography (PET/CT) scan revealed increased glucose metabolism in right supraclavicular lymph node (the maximum standardized uptake value, SUVmax 5.7), left lung patchy lesions (SUVmax 22.4) and the right tenth rib (SUVmax 6.4) (Figure 1). According to the PET/CT imaging, a third biopsy was performed on the hypermetabolic region of left lung, and a third mNGS confirmed the presence of T. marneffei (specific sequence count 15; specificity 57.69%). The patient promptly began a treatment protocol including an Amphotericin B cholesterol complex (250mg qd) and allergy medications, specifically Dexamethasone and Promethazine. A follow-up chest CT scan taken two weeks later revealed the lung’s extent decreased and the improvement of rib destruction. He continued oral Itraconazole treatment (200mg bid). A subsequent CT scan taken one month later showed a substantial decrease in lung lesion and a sclerotic filling of rib. A CT scan six months later revealed that the bone damage and lung lesions had completely reabsorbed (Figure 2).
 |
Figure 1 A 61-year-old male patient presents with a intermittent cough lasting over two years, which has intensified in the last month. He received an 18F-FDG PET/CT scan. The whole-body maximum intensity projection (MIP) (a) from the 18F-FDG PET/CT showed multiple regions of the body with increased metabolic. The combined PET/CT images (b–d) and the tomographic MIP images (e–g) demonstrate mild increased uptake of glucose in the right supraclavicular lymph nodes (SUVmax 5.7, red arrows), while a significant metabolic abnormality is observed in the left lung (SUVmax 22.4). Furthermore, there is an irregular increase in metabolism in the right 10th rib (SUVmax 6.4, red arrows). |
 |
Figure 2 The chest CT scan of the patient prior to treatment (a and b) showed patches in the left lower lung lobe and partial consolidation. There was obviously bone destruction in the right tenth rib (red arrows). After two weeks of therapy, a follow-up chest CT scan (c and d) demonstrated a decrease in patches and a reduction in the area of consolidation in left lung, and an improvement in bone destruction compared to the initial scan (red arrows). After one month of therapy, a follow-up chest CT scan (e and f) revealed markedly improved infection and a sclerotic filling of rib compared to earlier scans (red arrows). A CT scan (g and h) 6 months later showed complete disappearance of the lung lesions and complete repair of the bone destruction (red arrows). |
Discussion
Talaromycosis is an invasive mycosis endemic in tropical and subtropical Southeast Asia, including Thailand, Vietnam, Cambodia, Laos, Myanmar, as well as southern China, such as Guangxi Province, Guangdong Province and Hong Kong. In addition, it is also found in northeastern India, Japan and other Asian countries.4 T. Marneffei infection may occur through inhaling T. Marneffei conidia. At 37°C, the conidia of T. marneffei change into yeast and enter the lungs, and they mostly multiply in the mononuclear phagocyte system. Macrophages primarily differentiate into two phenotypes: classical M1-like and alternative M2-like. M2-like macrophages cells appear to provide a protective niche for fungal proliferation to evade from myeloperoxidase-dependent neutrophil fungicidal activity during infection establishment in vivo,2 which is known as the macrophage paradox effect. M1-like macrophages inhibiting fungi and M2-like macrophages promoting them. Research has demonstrated that T. marneffei induces tyrosine phosphorylation, leading to the degradation of the SOCS3 protein, thereby diminishing SOCS3’s inhibitory effect on p-STAT6. And p-STAT6 is a key factor in M2-like polarization, T. marneffei can facilitate the transition of macrophages from M1 to M2 polarization, thus evading immune clearance in a certain extent.3 Then the pathogens spread through the bloodstream5 to different parts of the body, including the skin, liver, spleen, lymph nodes, and gastrointestinal tract. Our patient lives in Hubei Province, which is not an endemic area for T. marneffei. However, he had visited Guangxi Province about one and a half months ago, which is one of the regions with a high prevalence of T. marneffei, accounting for 43% of T. Marneffei patients in China, where he was presumed to have contracted the infection.
T. Marneffei infection is a serious opportunistic infection linked to AIDS, with about 89.9% of HIV-positive individuals affected.4 The increasing use of immunosuppressive medications in clinical settings and the ongoing discovery of diseases related to immunodeficiency have changed the epidemiology of T. Marneffei infection, with an increasing number of T. Marneffei infection cases in HIV-negative patients with immunodeficiencies (such as anti-γ-interferon autoantibody-associated immunodeficiency syndrome, systemic lupus erythematosus, solid-organ transplantation, and haematological malignancies) and even in immunocompetent people.6 Talaromycosis is no longer a disease associated solely with AIDS. Studies have shown that most HIV-negative patients with Talaromycosis have comorbidities that affect immune function (such as diabetes, cancer and TB) and chronic lung disorders which compromise the structural integrity of original tissues.7 Our patient had examined the antibody of HIV, HBV, HCV, EBV and TP, TSPOT, TB-DNA, G-tests, bacterial cultures of the lower respiratory tract sputum and bronchial lavage fluid, which were all negative, there was no evidence of immunodeficiency. However, the patient had been hospitalized 17 months earlier for severe pneumonia and severe anemia, and he had been in an elevated blood glucose state, which may have created the conditions for pathogen invasion.
The clinical manifestations of T. Marneffei infection include rash, fever, weight loss, hepatosplenomegaly, lymphadenopathy, and abnormalities in the respiratory and gastrointestinal systems.4 These symptoms are nonspecific and are similar to those of tuberculosis, lung cancer or other common infectious diseases. Moreover, T. Marneffei has harsh culture condition and low positive detection rate. Sometimes multiple tests or more sophisticated genetic testing is required to make a definitive diagnosis. Especially in non-endemic areas, there is a relative lack of physician awareness and vigilance about the disease, the T. Marneffei infection is often underestimated. All of which may lead to a delayed diagnosis of the disorder, with death rates possibly as high as 50.6%.8
The imaging of Talaromycosis shows involvement of multiple systems and lack of specificity. CT scans of Talaromycosis patients have been demonstrated to show pulmonary multiple patches, consolidation, ground-glass shadows, solitary or multiple nodules, masses, cavities, lobular septa and bronchial wall thickening, and fusion of enlarged lymph nodes with necrosis, pleural effusion, pericardial effusion, peritoneal effusion, symmetrical thickening of the small intestinal wall with homogeneous enhancement, and diffuse enlargement of the liver and spleen with homogeneous enhancement.9
To further learn the characteristics of PET/CT images of Talaromycosis, we systematically searched PubMed and Web of Science using the keywords “ marneffei or Talaromycosis” and “PET or FDG or positron emission tomography or 18-fluorodeoxy-glucose”. We finally got 12 articles that included PET/CT characteristics of T. Marneffei infection. One article reported two patients who had received PET/CT and had elevated bone and lymph node metabolism with SUVmax9.6.10 Six individuals in another research had completed PET/CT, showing liver and lung involved with an SUVmax of 19.9.11 The others contains relatively complete patient data, and we present the above results in Table 1. On 18F-FDG PET/CT scans, T. Marneffei infection displays increased metabolic activity, primarily impacting lymph nodes, followed by the lung, bone, intestine, spleen and liver, with SUVmax values ranging from 7.5 to 21.4.12,13 The SUVmax of our patient reached 22.4, surpassing previously documented upper limits. Cheng et al14 reported a 6-year-old child who had a neck mass and had a fever for three months. PET/CT revealed high metabolic active lesions in bilateral cervical, axillary, mediastinal, abdominal, groin lymph nodes, pelvis, the left upper arm, left lateral wall of the nasopharynx, right shoulder joint, spleen and bones of the entire body. The performance was highly similar to lymphoma and PET/CT misdiagnosed it as lymphoma. Likewise, two other cases of T. Marneffei infection presented PET/CT images suggestive of lymphoma.15,16 Another patient’s PET/CT images showed a lobulated and spiculated nodule with rough margins in the right lung apex and increased metabolism in the left hilar lymph node. And this case was misidentified as lung cancer.12 Those all indicated that it is difficult to differentiate T. Marneffei infection from lymphoma, lung cancer, or other malignant tumours with metastases on imaging signs.
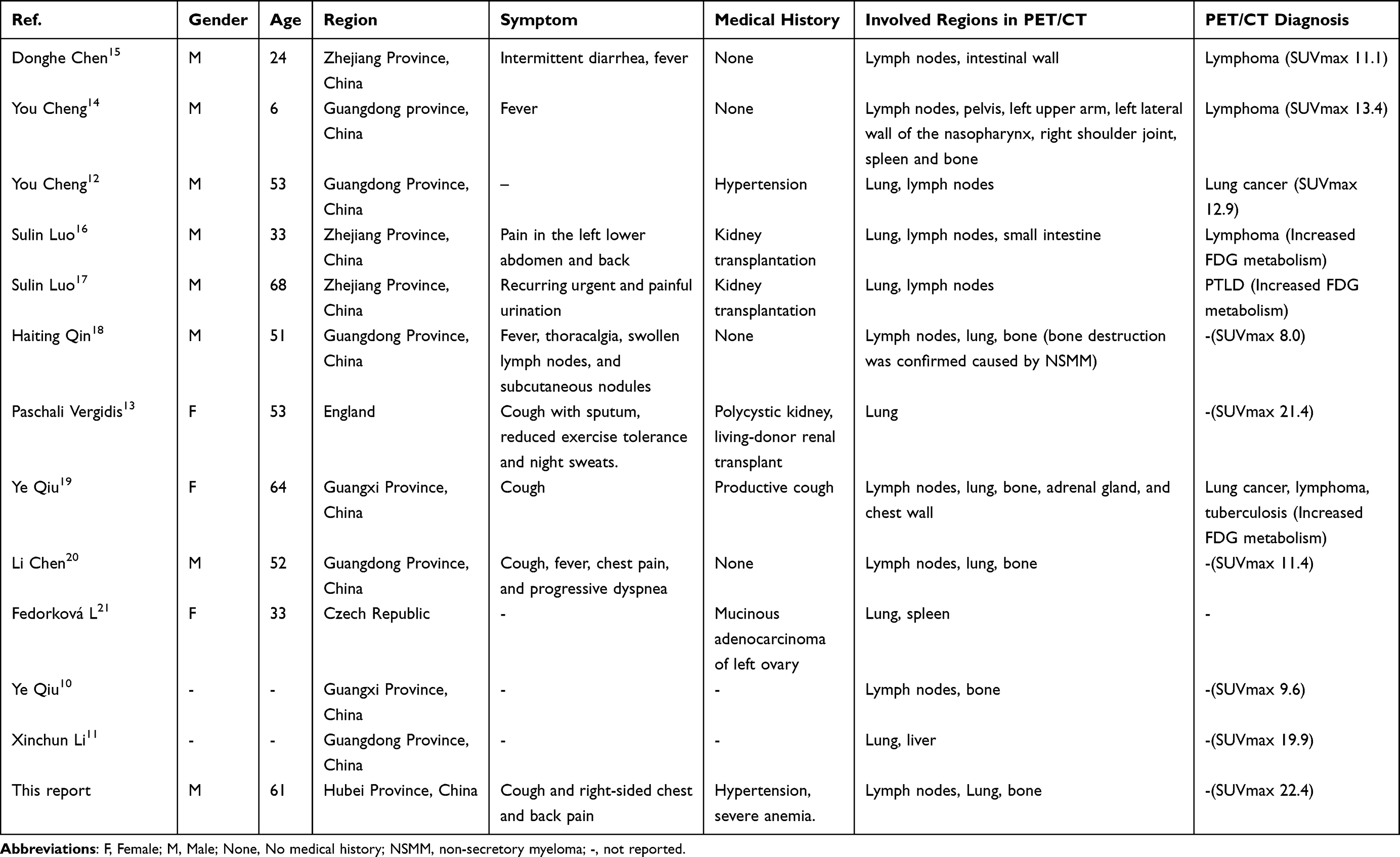 |
Table 1 PET/CT Features of Talaromyces Marneffei Infection Case |
Our patient also exhibited one significant site of bone destruction with increased uptake of glucose. Bone destruction commonly occurs in HIV-negative patients with Talaromycosis, and rare in HIV-positive individuals. In an examination of 165 individuals with T. Marneffei infection, Bai et al22 discovered that 35 developed bone destruction, all of whom were HIV-negative. This result is consistent with Qiu et al10 who examined 100 Talaromycosis patients, among which 14 exhibited osteolytic lesions, all were HIV-negative. According to a study, bone damage occurred in about 20% of the HIV-negative individuals with Talaromycosis.7 When the pathogen spreads throughout the body, the fungal components may trigger host immune cells to release pro-inflammatory factors such as TNF-α and IL-6. These cytokines stimulate osteoclast activation, leading to increased bone destruction. HIV-positive patients have a weaker immune system, and the inflammatory response is not as strong as those of HIV-negative patients, so there is relatively less bone destruction. Meanwhile, HIV-negative patients have certain immune responses, such as neutrophil and macrophage activity, which leads to increased local inflammation and causes bone destruction. The prevailing hypothesis is precisely that the accumulation of neutrophils and the release of proteolytic enzymes lead to osseous tissue lysis, liquefaction, and necrosis.23
PET-CT scan as an imaging method and its main value is to assist diagnosis, assess the degree of infection involvement and for post-treatment assessment. The gold standard for diagnosing Talaromyces marneffei is a positive pathogen culture. Bone marrow and lymph nodes exhibit the highest rates of positive pathogen cultures (100%), followed by skin tissue (90%), blood samples (76%) and sputum (34%).4 Culture methods should be preferred for the identification of pathogens when conditions permit. Recently, advancements in metagenomic next-generation sequencing (mNGS) technology have greatly enhanced the detection of pathogenic microorganisms. A meta-analysis showed that the sensitivity and specificity of mNGS for diagnosing infectious diseases were 75% and 68%, respectively.24 When necessary, such as when systematic testing finds no pathogenetic diagnosis, mNGS can be employed for diagnosis. In this case, We used mNGS test to diagnose. However, a major drawback of this technique is that the microbial nucleic acids from most patient samples are predominantly derived from the human host. Usually, over 99% of the reads originate from the human background. Furthermore, there is a chance for ambient bacteria contaminate the sample, which could lower sensitivity.25 This may help explain why the patient received three times mNGS tests before successfully identifying the T. Marneffei infection. It took about three months from the symptom gotten worse to final diagnosis.
Amphotericin B is the primary pharmacological intervention for treating Talaromyces marneffei. This patient commenced treatment with Amphotericin B cholesterol sulfate complex (250mg qd) for two weeks, and successfully moving to sequential Itraconazole (200mg bid) therapy two weeks later. Fortunately, he responded well to the treatment and did not experience a delayed diagnosis leading to death. A follow-up CT scan conducted after two weeks indicated significant absorption of the lesion, reflecting improvements compared to pre-treatment. And a follow-up CT scan taken one month later showed markedly improved infection. However, Amphotericin B therapy may be accompanied by toxic reactions, including acute infusion-related reactions and dose-related nephrotoxicity.26 His creatinine levels rose to 130 umol/L (57–111 umol/L) during treatment, suggesting that the patient developed acute renal insufficiency. At 6-month follow-up, the patient had not relapsed and CT scan revealed the bone damage and lung lesions had completely reabsorbed, but the patient’s creatinine levels were elevated during all of this time. Although the prognosis for this patient is favorable, additional instances may be required to investigate the diagnostic and treatment approaches for T. marneffei infection.
T. Marneffei infection is likely to be ignored in HIV-negative individuals, especially in those who exhibit bone destruction. The case we report indicates that even in non-endemic areas and in immunocompetent individuals, who identified as infection and exhibited bone destruction should be made aware of the possibility of fungus T. marneffei. Prompt treatment, early application of antifungal drugs to reduce mortality.
Abbreviations
T. marneffei, Talaromyces marneffei; AIDS, Acquired immune deficiency syndrome; mNGS, metagenomic next-generation sequencing; CT, Computed tomography; 18F-FDG, 18-fluorodeoxyglucose; PET/CT, Position emission tomography/computed tomography; SUVmax, The maximum standardized uptake value.
Data Sharing Statement
Data sharing is not applicable to this article as no datasets were generated or analysed.
Ethical Approval
Written informed consent was provided by the patient to allow the case details and any accompanying images to be published, and this report was approved by the Ethics Committees of The first College of Clinical Medical Science, China Three Gorges University, Yichang, Hubei (No. 2024-490-01, date: 2024/11/26). The first College of Clinical Medical Science, China Three Gorges University approved the publication of this report.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Yichang city Science and Technology Bureau project A24-2-019.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Li X, Yang Y, Zhang X, et al. Isolation of Penicillium marneffei from soil and wild rodents in Guangdong, SE China. Mycopathologia. 2011;172(6):447–451. doi:10.1007/s11046-011-9443-5
2. Ellett F, Pazhakh V, Pase L, et al. Macrophages protect Talaromyces marneffei conidia from myeloperoxidase-dependent neutrophil fungicidal activity during infection establishment in vivo. PLoS Pathog. 2018;14(6):e1007063. doi:10.1371/journal.ppat.1007063
3. Wei W, Ning C, Huang J, et al. Talaromyces marneffei promotes M2-like polarization of human macrophages by downregulating SOCS3 expression and activating the TLR9 pathway. Virulence. 2021;12(1):1997–2012. doi:10.1080/21505594.2021.1958470
4. Wang F, Han R, Chen S. An overlooked and underrated endemic mycosis-talaromycosis and the pathogenic fungus talaromyces marneffei. Clin Microbiol Rev. 2023;36(1):e0005122. doi:10.1128/cmr.00051-22
5. Vanittanakom N, Cooper CR, Fisher MC, Sirisanthana T. Penicillium marneffei infection and recent advances in the epidemiology and molecular biology aspects. Clin Microbiol Rev. 2006;19(1):95–110. doi:10.1128/CMR.19.1.95-110.2006
6. Wang P, Chen Y, Xu H, et al. Acute disseminated talaromyces marneffei in an immunocompetent patient. Mycopathologia. 2017;182(7–8):751–754. doi:10.1007/s11046-017-0127-7
7. Wei HY, Liang WJ, Li B, et al. Clinical characteristics and risk factors of Talaromyces marneffei infection in human immunodeficiency virus-negative patients: a retrospective observational study. World J Emerg Med. 2021;12(4):281–286. doi:10.5847/wjem.j.1920-8642.2021.04.005
8. Hu Y, Zhang J, Li X, et al. Penicillium marneffei infection: an emerging disease in mainland China. Mycopathologia. 2013;175(1–2):57–67. doi:10.1007/s11046-012-9577-0
9. Zhu XL, Tang GX, Liu XY, Li R, Lv SX, Wang GX. CT findings of Talaromyces marneffei infection among HIV patients with lymphadenopathy. Front Med Lausanne. 2022;9:930678. doi:10.3389/fmed.2022.930678
10. Qiu Y, Zhang J, Liu G, et al. Retrospective analysis of 14 cases of disseminated Penicillium marneffei infection with osteolytic lesions. BMC Infect Dis. 2015;15(1):47. doi:10.1186/s12879-015-0782-6
11. Li X, Hu W, Wan Q, et al. Non-HIV talaromycosis: radiological and clinical analysis. Medicine. 2020;99(10):e19185. doi:10.1097/MD.0000000000019185
12. Cheng Y, Li WM, Wang SX, Shao D. PET/CT manifestations of a case of penicilliosis marneffei misdiagnosed as lung cancer. Clin Nucl Med. 2023;48(4):e167–e169. doi:10.1097/RLU.0000000000004531
13. Vergidis P, Rao A, Moore CB, et al. Talaromycosis in a renal transplant recipient returning from South China. Transpl Infect Dis. 2021;23(1):e13447. doi:10.1111/tid.13447
14. Cheng Y, Li WM, Huang JJ, Wang SX, Shao D. 18F-FDG PET/CT image analysis of penicilliosis marneffei in an immunocompetent child patient. Clin Nucl Med. 2022;47(4):e358–e359. doi:10.1097/RLU.0000000000004075
15. Chen D, Chang C, Chen M, et al. Unusual disseminated Talaromyces marneffei infection mimicking lymphoma in a non-immunosuppressed patient in East China: a case report and review of the literature. BMC Infect Dis. 2020;20(1):800. doi:10.1186/s12879-020-05526-1
16. Luo S, Wang X, Ren X, et al. A case of TM infection with challenging differential diagnosis from lymphoma post-renal transplant. BMC Infect Dis. 2023;23(1):888. doi:10.1186/s12879-023-08912-7
17. Luo S, Yan P, Wang X, et al. Talaromyces marneffei: a challenging diagnosis in a kidney transplant patient. Clin Case Rep. 2024;12(7):e9028. doi:10.1002/ccr3.9028
18. Qin H, Qiu Y, Huang Y, et al. Rare incidence of non-secretory myeloma with talaromycosis: a case report. BMC Infect Dis. 2021;21(1):964. doi:10.1186/s12879-021-06641-3
19. Qiu Y, Pan M, Zhang J, et al. Two unusual cases of human immunodeficiency virus-negative patients with talaromyces marneffei infection. Am J Trop Med Hyg. 2016;95(2):426–430. doi:10.4269/ajtmh.15-0789
20. Chen L, Yu L, Wu Y, Ming WK, Huang Z, Liu S. A 52-year-old man with an 11-month history of fever, cough, chest pain, pleural effusion, and left lung atelectasis. Chest. 2020;158(4):e153–e157. doi:10.1016/j.chest.2020.05.546
21. Fedorkova L, Vojtech I, He LP, Ondrus D. Multiresistant opportunistic talaromycosis in a patient with ovarian cancer. Klin Onkol. 2020;33(6):464–466. doi:10.48095/ccko2020464
22. Bai Y, Xi D, Chen Q, et al. Characteristics of Talaromyces marneffei with bone destruction in Guangxi Province, China: a retrospective study. Am J Transl Res. 2021;13(10):11491–11500.
23. Liu GN, Huang JS, Zhong XN, et al. Penicillium marneffei infection within an osteolytic lesion in an HIV-negative patient. Int J Infect Dis. 2014;23:1–3. doi:10.1016/j.ijid.2013.12.019
24. Liu J, Zhang Q, Dong YQ, Yin J, Qiu YQ. Diagnostic accuracy of metagenomic next-generation sequencing in diagnosing infectious diseases: a meta-analysis. Sci Rep. 2022;12(1):21032. doi:10.1038/s41598-022-25314-y
25. Gu W, Miller S, Chiu CY. Clinical metagenomic next-generation sequencing for pathogen detection. Annu Rev Pathol. 2019;14:319–338. doi:10.1146/annurev-pathmechdis-012418-012751
26. Hamill RJ. Amphotericin B formulations: a comparative review of efficacy and toxicity. Drugs. 2013;73(9):919–934. doi:10.1007/s40265-013-0069-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Identification of Talaromyces marneffei Infection in an HIV-Negative Patient by ITS Sequencing
Sun A, Gou X, Zhu Y, Lv H, Ge Y
Infection and Drug Resistance 2023, 16:5275-5282
Published Date: 14 August 2023