")
Back to Journals » Vascular Health and Risk Management » Volume 21
A Call to Action for Anticoagulation Stewardship to Address Suboptimal Thromboprophylaxis Practices for at-Risk Non-Orthopedic Surgical Patients in Vietnam: An Explanatory Sequential Mixed-Methods Study
Authors Nguyen TTT , Tong HT, Nguyen HTL , Nguyen TD
Received 18 November 2024
Accepted for publication 12 April 2025
Published 24 April 2025 Volume 2025:21 Pages 305—326
DOI https://doi.org/10.2147/VHRM.S505100
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Harry Struijker-Boudier
Thuy Thi Thu Nguyen,1 Huyen Thanh Tong,2 Huong Thi Lien Nguyen,1 Trung Duc Nguyen2
1Department of Clinical Pharmacy, Faculty of Pharmacology - Clinical Pharmacy, Hanoi University of Pharmacy, Hanoi, Vietnam; 2Department of Pharmacy, 108 Military Central Hospital, Hanoi, Vietnam
Correspondence: Trung Duc Nguyen, Department of Pharmacy, 108 Military Central Hospital, 1 Tran Hung Dao Street, Hai ba Trung District, Hanoi, 10000, Vietnam, Email [email protected]
Purpose: This study aimed to investigate the current practices of VTE prophylaxis in patients undergoing abdominal-pelvic surgery (PAS) and to identify the factors that influence surgeons’ practice of VTE prophylaxis.
Patients and Methods: This two-phase explanatory sequential mixed-method study used chart audits followed by semi-structured interviews based on the theoretical domain framework (TDF). During Phase I, quantitative data from 240 medical records of patients with PAS in April 2023 were audited to measure adherence rates to the standard thromboprophylaxis guidelines. In Phase II, in-depth interviews with 16 surgeons were conducted and analyzed using thematic content analysis based on the TDF framework to understand the determinants of thromboprophylaxis in patients with PAS.
Results: Audits of 240 medical records of patients showed the rate of appropriate prophylactic methods was low (11.7%). For patients on anticoagulant prophylaxis, adherence rates regarding drug selection and dosage were high (100% and 89.3%, respectively), whereas adherence rates regarding time of initiation and length of prophylaxis were low (50% and 28.6%, respectively). A qualitative analysis identified 12 theoretical domains relevant to thromboprophylaxis practices among surgeons. The most encountered barriers included concerns about bleeding risk, resource issues, low beliefs about preventive benefits for certain patients with PAS, inadequate knowledge and training, and a lack of protocol and policy. The most encountered enablers included positive beliefs in prophylaxis benefits, mandatory policy and computerized supportive tools, thromboprophylaxis set as patient safety goals, leadership and multidisciplinary working, and training.
Conclusion: Significant quality gaps were present in VTE prevention practice for abdominal-pelvic surgical patients, and multiple coexisting factors prevented the full adoption of practice standards. The implementation of an anticoagulation stewardship program is essential for addressing practical issues.
Keywords: venous thromboembolism prevention, abdominopelvic surgery, guideline adherence, influencing factors, mixed-methods study, anticoagulant stewardship
Introduction
The frequency of thromboembolic complications in hospitalized patients, along with the adverse consequences of these events and their economic impact strongly justify the prioritization of thromboprophylaxis as a critical patient safety measure for all general hospitals.1–3 Given that venous thromboembolism (VTE) is a prevalent complication in postoperative settings and is associated with substantial short-term and long-term morbidity and mortality, prevention is the key to reducing the burden of this condition.2,4 Extensive evidence from numerous randomized clinical trials conducted over the past 30 years conclusively establishes that the proper implementation of primary thromboprophylaxis in high-risk surgical patients is safe, clinically effective, and cost-effective in mitigating VTE.1 The Agency for Healthcare Research and Quality (AHRQ) conducted a systematic evaluation of 79 safety practices and identified that the appropriate use of thromboprophylaxis was the number one patient safety practice for hospitals.5
Despite the overwhelming evidence supporting thromboprophylaxis for surgical patients, the rates of appropriate prophylaxis remain suboptimal. Reports indicate that a substantial percentage of surgical patients at risk of VTE do not receive recommended prophylactic methods for VTE.6–8 Data from a multinational, cross-sectional survey in the acute hospital care setting show a significant proportion of surgical patients at risk of VTE (64.4%), of whom only 58.5% received recommended prophylaxis. This study also underscores the significant inter-country variation in thromboprophylaxis administration, ranging from as low as 2% in some underdeveloped countries to 84% in Europe.6 Enhanced VTE preventive practices in developed countries can be attributed to several critical factors, including the availability of updated evidence-based guidelines,2,9–11 implementation guidance,5,12 the establishment of anticoagulation stewardship programs,13 and the extensive execution of quality improvement activities in healthcare facilities.5,12 These factors remain limited in developing countries, leading to inadequate adoption of practice guidelines.
There exists considerable difference in the rate of appropriate prophylaxis practice among different types of surgery, with non-orthopedic surgeries generally demonstrating lower compliance with VTE prevention guidelines than orthopedic surgeries.14–17 Real world data indicate that the implementation of VTE preventive measures during hospitalization and post-discharge for major abdominal and pelvic procedures is inadequate, mismatched with the risk profile of this patient population.2,6,18–21 All this evidence highlights the necessity for focused quality improvement initiatives that target on patient population exhibiting substantial gap between VTE risk profile and prophylactic practice, with the objective of significantly diminishing hospital-acquired VTE events.
Vietnam, which is a developing country, currently lacks both a national policy and framework for the implementation of venous thromboembolism practices, as well as regulations on anticoagulant stewardship. Providing quantitative data on current compliance rates in thromboprophylaxis practice is crucial to persuade hospitals and other stakeholders to undertake proactive improvement efforts. Enhancing existing suboptimal practices necessitates a comprehensive understanding of the barriers and facilitators that affect physicians’ adherence to clinical guidelines.5,22–24 Therefore, employing mixed-methods research seems a rational approach to provide quantitative evidence that underscores the need for quality enhancement and to offer an exhaustive perspective on influencing factors, particularly changeable obstacles, to inform intervention design. This is further emphasized when executing quality improvement initiatives in resource-limited settings, where multiple factors may concurrently affect physicians’ prescribing behaviours.22,25,26
To the best of our knowledge, no study has employed such research methods to concurrently investigate the practices and perceptions of surgeons regarding VTE prevention in at-risk surgical patients, particularly those undergoing abdominal and pelvic surgery. In this study, we conducted a sequential, explanatory mixed-methods study to evaluate the current state of VTE prevention practice for patients undergoing abdominal pelvic surgery and to identify barriers and facilitators to the implementation of standard guidelines.
The study was conducted at 108 Military Central Hospitals, one of six special-grade tertiary hospitals recognized for delivering the best quality specialized care in Vietnam. Physicians are also expected to stay up-to-date and constantly follow evidence-based standards. The study results are expected to demonstrate the best level of VTE prevention practice for abdominal pelvic surgical patients in Vietnam, with the objective of convincing Vietnamese healthcare facilities for enhanced venous thromboembolism prevention efforts while concurrently proposing the most appropriate strategies in the context of tertiary care in Vietnam.
Materials and Methods
Study Design
This study adopted an explanatory sequential mixed-methods design. The first quantitative phase was a cross-sectional chart audit to assess the current adherence to thromboprophylaxis guidelines for patients with PAS. This was followed by a qualitative phase of semi-structured interviews with surgeons to understand the factors that influenced their adherence to VTE guidelines when treating PAS patients. The quantitative phase informed the surgeons recruited for the qualitative phase (eg, those with lack of VTE prevention practices) and the development of the interview topic guide. For the qualitative component, the in-depth interview approach was chosen rather than focus group discussion to ensure that participants could express themselves freely without any undue influence from others (eg, senior physicians or department leaders).27
Study Setting
This study was conducted between April and August 2023 at the Institute of Digestive Surgery, 108 Military Central Hospital. The 108 Military Central Hospital, classified as a general hospital, tertiary care provider, and special-grade national facility, delivers specialist care to more than 2000 inpatients each day. The Institute of Digestive Surgery comprises three affiliated departments equipped with the most advanced and synchronized systems in the country, possessing deep professional expertise and the capacity to admit and treat a maximum of 120 patients.
Phase 1: Quantitative Data
Participants
The patient population consisted of adult patients who underwent abdominal or pelvic surgery at the Institute of Digestive Surgery of 108 Military Central Hospital in April 2023. Patients receiving anticoagulant therapeutic purposes (eg, acute coronary syndrome, atrial fibrillation), those transferred to other institutes or hospitals immediately after surgery, pregnant or lactating patients, and dialysis patients were excluded.
A one-month audit was considered sufficient to represent the disease pattern and practice pattern of thromboembolism prevention in the context of a tertiary care hospital with a substantial number of patients hospitalized for abdominopelvic surgical procedures.
Data Collection
Data from the medical charts of eligible patients were retrospectively collected from electronic and paper medical records to a data collection form. After checking for completeness, the data was entered, cleaned, and analyzed using Microsoft Excel 2021. The abstracted data included demographic information, admission and discharge diagnoses, procedural details, risk factors for bleeding and VTE during hospitalization, and characteristics of the administered VTE prophylaxis methods.
VTE risk was evaluated in surgical patients using the Caprini Risk Assessment model, and was then classified into very low, low, moderate, and high risk. Patients were categorized as high-risk or not at risk of major bleeding complications.2 Patients were also determined whether they had absolute contraindications to anticoagulant.28 Taking VTE risk, major bleeding risk and absolute anticoagulant contraindication into account, the proportion of patients receiving recommended prophylaxis was evaluated throughout the duration of the patients’ stay. The criteria for evaluating the appropriateness of prophylaxis, which was based on The VNHA 2022 guideline, are presented in Table 1.28 The VNHA 2022 guideline is almost in agreement with the CHEST guideline 9th and Queensland 2018 guideline.29 Specifically, we evaluated the appropriateness of several aspects of VTE prophylaxis, including the indication and choice of VTE prophylactic method, anticoagulant selection, dosage regimen, initiation time, and length of prevention.
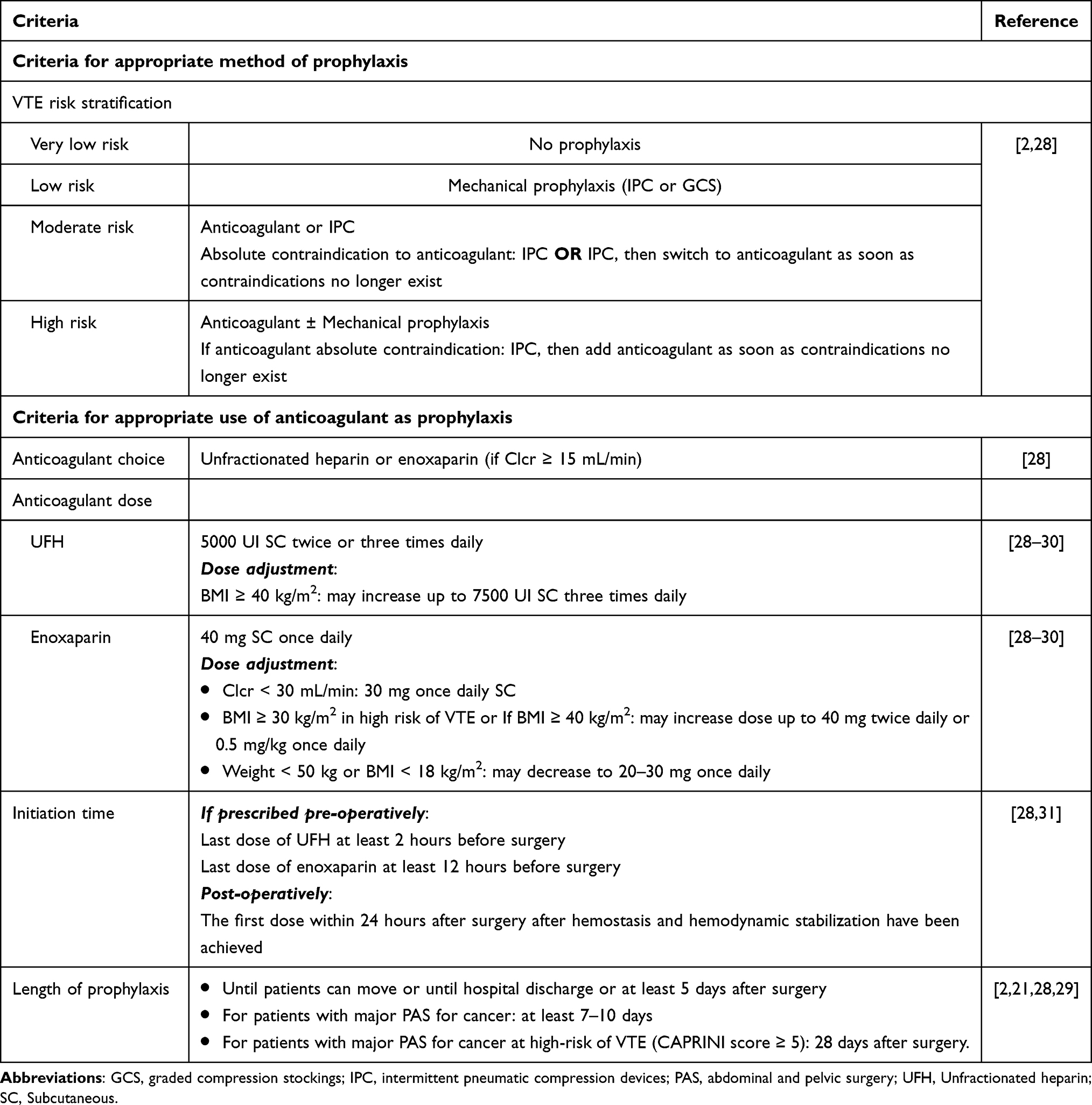 |
Table 1 Criteria for Evaluating the Appropriateness of VTE Prevention Practice for PAS Patients |
Data Analysis
Data was analyzed using descriptive statistics. Means and standard deviations were reported for continuous variables where the data were normally distributed, while medians and interquartile ranges (IQR) were used to report non-normally distributed data. Categorical variables are reported as numbers and percentages.
Phase 2: Qualitative Data
Semi-structured, 1-on-1 interviews with surgeons were conducted to identify the barriers and facilitators influencing surgeons’ practice of VTE prophylaxis in compliance with standard guidelines.
Participants
All physicians who provided care for patients with PAS were eligible to participate, aiming to capture a diversity of relevant perspectives and beliefs. The necessity of interviewing all doctors stemmed from the quantitative data indicating suboptimal compliance practices among all doctors. Participants were recruited through an in-person announcement and a direct invitation by the lead author. Interested surgeons responded directly to the invitation, provided verbal permission, and were contacted to organize interviews.
Theoretical Framework
The Theoretical Domains Framework (TDF) guided interview guide development, data collection, and analysis.32 Although numerous psychological theories have been utilized to explain health care providers’ behavior,33,34 the TDF framework is a validated framework specifically designed for application in health care settings to investigate the barriers and facilitators influencing healthcare professionals’ behavior and to guide interventions aimed at modifying their practices regarding the implementation of evidence-based practices.23,32,34–39 It consists of 14 theoretical domains derived from 128 theoretical constructs from 33 theories of behavior and behavior change relevant to the determinants of behavior and intervention development in health care. The domains were derived through a systematic expert consensus process and provided a basis for understanding the broad set of factors that may influence behavior. The 14 domains included knowledge, skills, social/professional roles and identity, beliefs about capabilities, optimism, beliefs about consequences, reinforcement, intentions, goals, memory, attention and decision processes, environmental context and resources, social influences, emotion, and behavioral regulation.
Interview Guide
The semi-structured interview guide included open-ended questions based on the 14 theoretical domains of the TDF to elicit beliefs about each domain and identify the role of the domain in influencing the behavior of physicians. Each domain was linked to a set of questions used to explore the target behavior “conducting VTE risk assessment and ordering the recommended venous thromboembolism prophylaxis”. The interview guide was pilot tested with two surgeons to provide feedback on the clarity of the questions and accordingly revise the wording of several questions. The guide was iteratively revised throughout the interview process to better capture new themes introduced by participants and to remove or rephrase questions that participants had difficulty answering, as per best practices in qualitative research.
Data Collection
The interviews lasted 15 to 30 minutes and were conducted in person by a research associate with experience in interviewing and applying qualitative methods who did not work with the participants. Prior to conducting each interview, written informed consent was obtained from all participants. The interviews were then conducted and recorded in a private space in the hospital selected by the participants. Before ending the interview, demographic information (eg, age, sex, years of experience, and academic title) was collected from the participant. No repeat interviews were conducted, and transcripts were not returned to the participants for comments, although they were available if requested.
Data Analysis
The interviews were audio-recorded, transcribed verbatim, and anonymized. This was followed by manual cleaning to remove identifying information and ensure accuracy before analysis. Deductive directed content analysis was conducted by two research team members using TDF as the coding framework. To establish consistency between the coders, three interviews were coded independently, after which the two coders reviewed their coding, resolved discrepancies, and determined a coding strategy. The remaining interview transcripts were then divided equally between the two coders and coded using an agreed-upon coding scheme. Coders frequently triangulated the data and maintained their reliability. After the data were coded into the TDF domains, the data units (ie, several lines of text) were labelled with codes according to the key concept represented within the data unit by one coder. These codes were refined, and similar codes were grouped into larger themes within each TDF domain. These themes were also classified as facilitators or barriers to VTE prevention. TDF domains were classified as relevant to VTE prevention practices (ie, more likely to influence VTE prevention practices) based on the frequency of specific beliefs across interviews (four or more clinicians identified the belief in their interview), the number of beliefs in each domain (more than two), the presence of conflicting beliefs signaling variations in beliefs and attitudes, and evidence of strong beliefs that could directly influence teamwork performance.32
Ethics Approval
The study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Ethical Committee in Biomedical Research of 108 Military Central Hospital, Vietnam (the approval number 3527/GCN-BV). For the quantitative research phase, the Ethical Committee in Biomedical Research of 108 Military Central Hospital granted a waiver for consent as this phase was conducted retrospectively, posed no more than minimal risks to the patients, used anonymized data, and data confidentiality was maintained in accordance with national and international guidelines. For the qualitative research phase, all physicians provided their informed consent for inclusion prior to participating in the study and the participants’ informed consent included publication of anonymized responses/direct quotes.
Results
Quantitative Phase
Patients’ Characteristics
Patient characteristics are shown in Table 2. A total of 240 eligible patients (median age, 61 years; 63.3% male) were included in the audit. The mean hospitalization duration was 8 days for the overall population. Five (2.1%) patients experienced severe kidney failure.
 |
Table 2 General Characteristics of the Surgical Patient (n = 240) |
VTE Risk and Bleeding Risk Stratification
The results of the VTE risk and bleeding risk stratification are shown in Table 3. Of the 240 patients, 35 (14.6%) were at low risk, 80 (33.3%) were at moderate risk, and 125 (52.1%) were at high risk of developing VTE (Table 3). Major surgery and malignancy comorbidity were the two most frequent VTE risk factors (87.9% and 46.3%, respectively). Among these patients, 40.8% had at least one risk factor for serious bleeding. The most common risk factors for bleeding were lumbar puncture and epidural or spinal anesthesia within the previous 4h or next 12h, accounting for 39.6%.
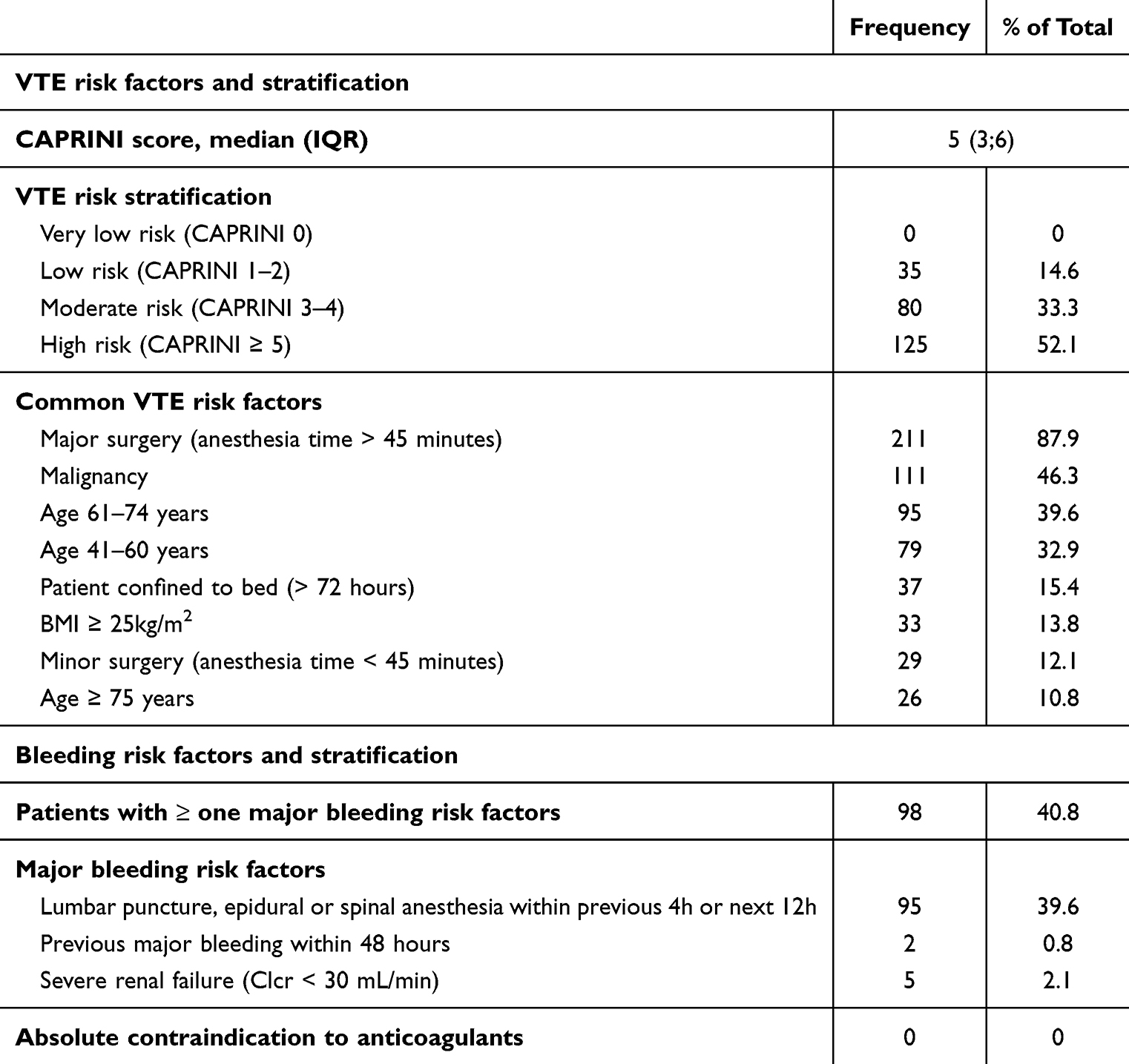 |
Table 3 VTE and Bleeding Risk Stratification |
Characteristics of Prescribed VTE Prophylaxis Methods
As shown in Table 4 and Figure 1, VTE prophylaxis was administered to 29 (12.1%) patients, including 26 who underwent PAS for cancer. In the subgroup of patients at high risk of VTE and those with PAS for cancer, the rates of prescribing thromboprophylaxis were low, at 20% and 30.2%, respectively.
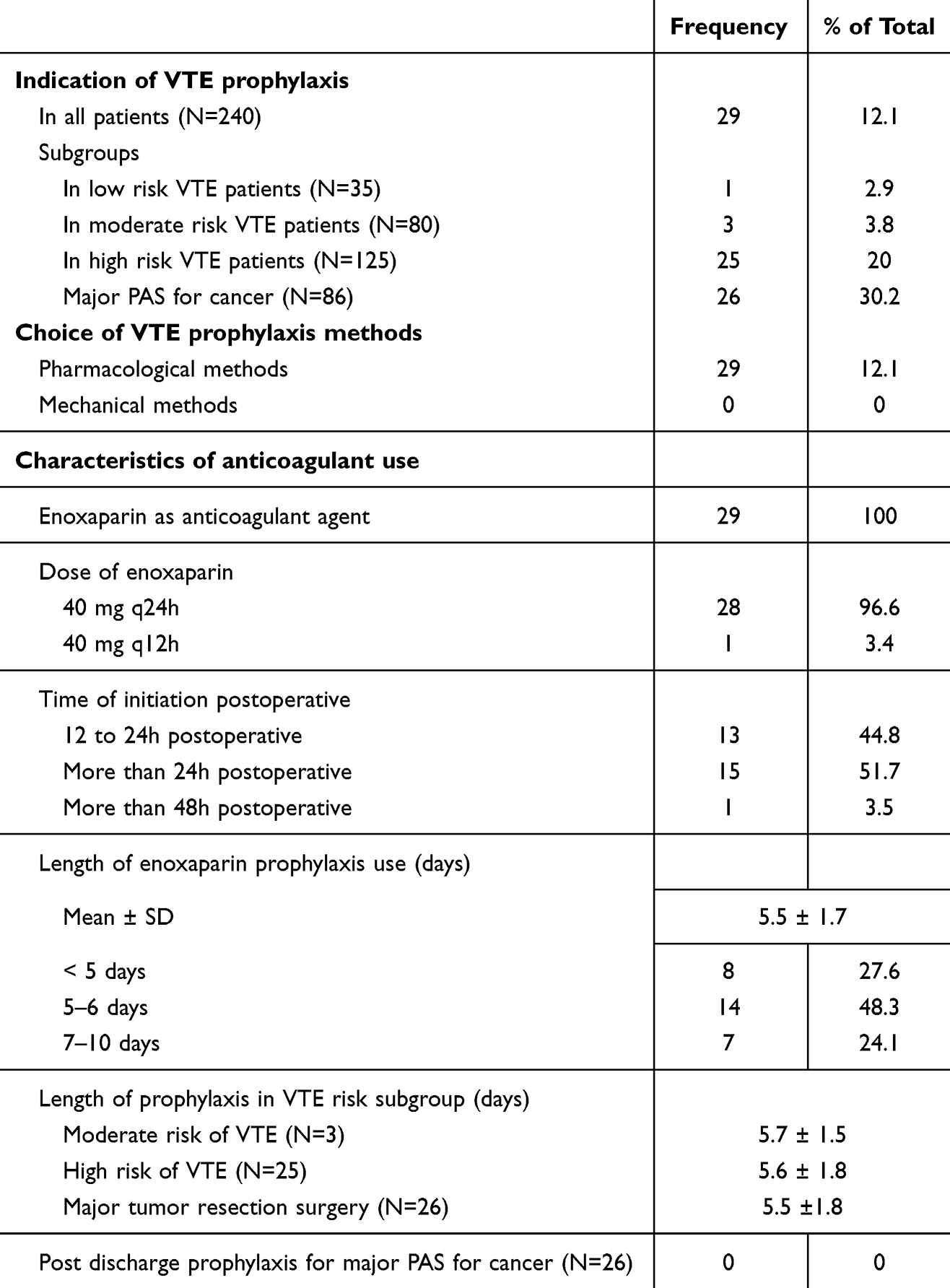 |
Table 4 Characteristics of Prescribed VTE Prophylaxis Methods |
 |
Figure 1 VTE risk stratification and adoption of prophylaxis in PAS patients. |
The only prescribed type of VTE prophylaxis was the pharmacological method (ie enoxaparin). Enoxaparin administered at a dose of 40 mg/day was the most common. Only 44.8% of the patients had enoxaparin initiated between 12 and 24 hours postoperatively. On average, the patients received 5.5 days of prophylaxis, of which only 24.1 patients received 7–10 days of enoxaparin. Notably, none of the patients were prescribed anticoagulants at discharge.
Audit of VTE Prevention Practice
Table 5 presents the appropriateness rate of thromboprophylaxis practice. Table 6 provides further details on the reasons for inappropriateness for each aspect of prophylaxis.
 |
Table 5 Audit of VTE Prophylaxis Practice |
 |
Table 6 Reasons for Inappropriate VTE Prophylaxis for Each Aspect |
The proportion of patients who were prescribed the recommended preventive measures based on their VTE risk level was very low (11.7% in the general population, 30.2% in the subgroup of cancer patients, and 20% in the high-risk VTE subgroup). A total of 87.9% of patients were classified as underuse of venous thromboembolism prevention.
For patients who were prescribed anticoagulants, while the concordance rate was high for the aspects of anticoagulant choice and dosing regimen (100% and 89.3%, respectively), the initiation time postoperatively and length of prevention poorly adhered to the guidelines. Specifically, only 50% of the patients had anticoagulation initiated at the appropriate time, and only 28.6% had an appropriate length of VTE prophylaxis.
Specifically, 50% of patients were started on anticoagulants at the appropriate time, while the remainder commenced prophylaxis later than recommended. 28.6% received VTE prophylaxis for the appropriate duration, while the remainder received prophylaxis for a shorter duration than recommended. Notably, among cancer patients, no patient received adequate prophylaxis as all were used it for a shorter duration than recommended.
Qualitative Phase
Participant Characteristics
In total, 16 surgeons from three departments of the Institute of Digestive Surgery were interviewed. The median age of the participants was 40 years and 100% were male (Table 7). More than 80% of the participants had at least ten years of experience in practice. The median interview time was 19.5 minutes. Relevant domains and the most frequently coded theoretical domains were presented in Table 8.
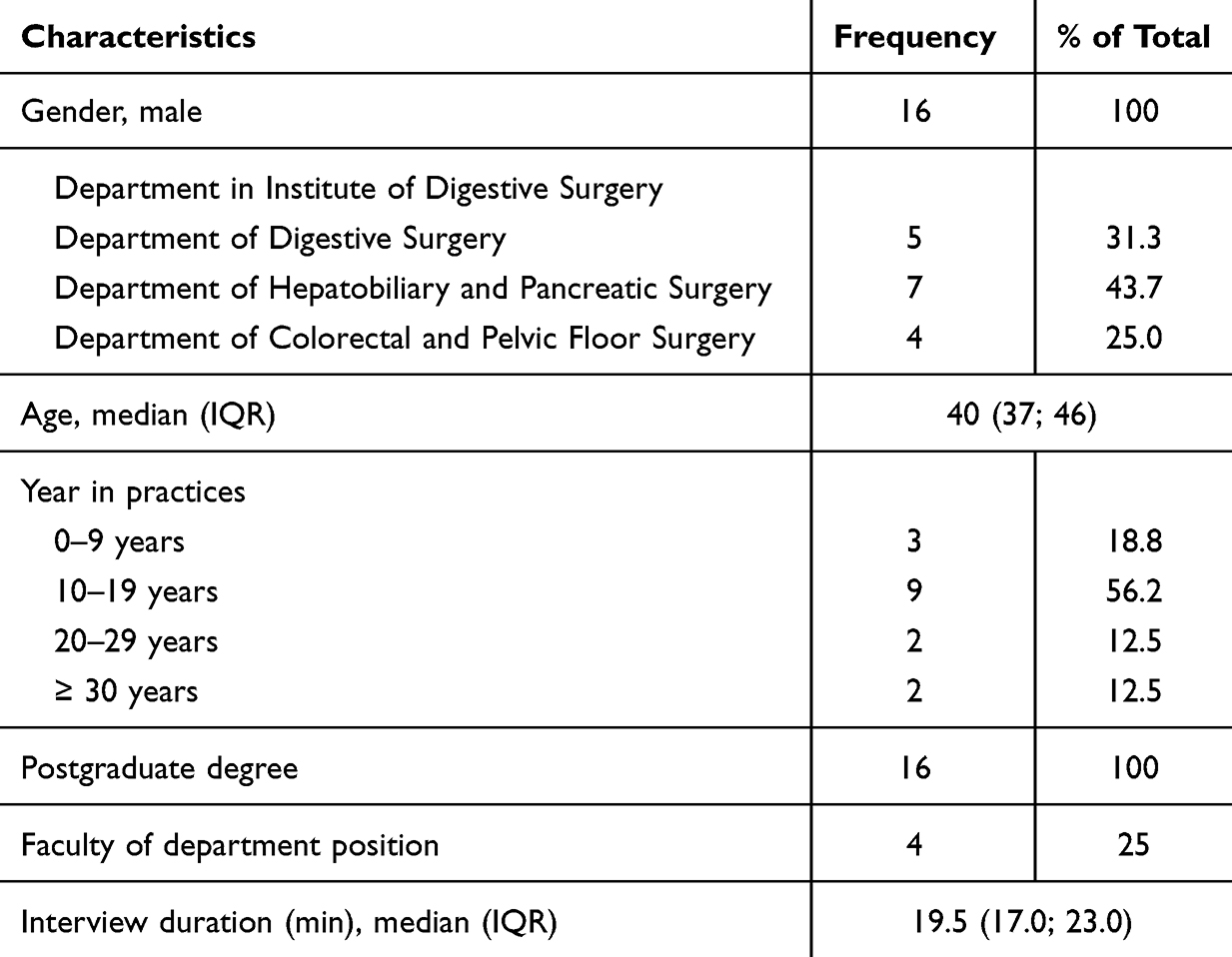 |
Table 7 Participants’ Characteristics (n=16) |
 |
Table 8 The Coding Frequencies of 12 Relevant Domains of the Theoretical Domains Framework |
As illustrated in Table 8, 12 out of the 14 theoretical domains were identified as relevant to the target behavior among surgeons (ie, VTE risk assessment and ordering recommended thromboprophylaxis practice). However, seven out of the 12 domains stood out: environmental context and resources, beliefs about consequences, Knowledge, Social/professional role and identify, social influence, Goals and Behavior regulation, which were identified as the prominent enablers of and barriers to VTE prevention practice and will thus be the focus of the following detailed analysis. These seven prominent domains represented 86.0% of the emerging themes.
Barriers and Enablers to Implementation of VTE Prevention Practice Among Surgeons
Figure 2 summarizes the barriers and enablers identified by participants across the 12 domains.
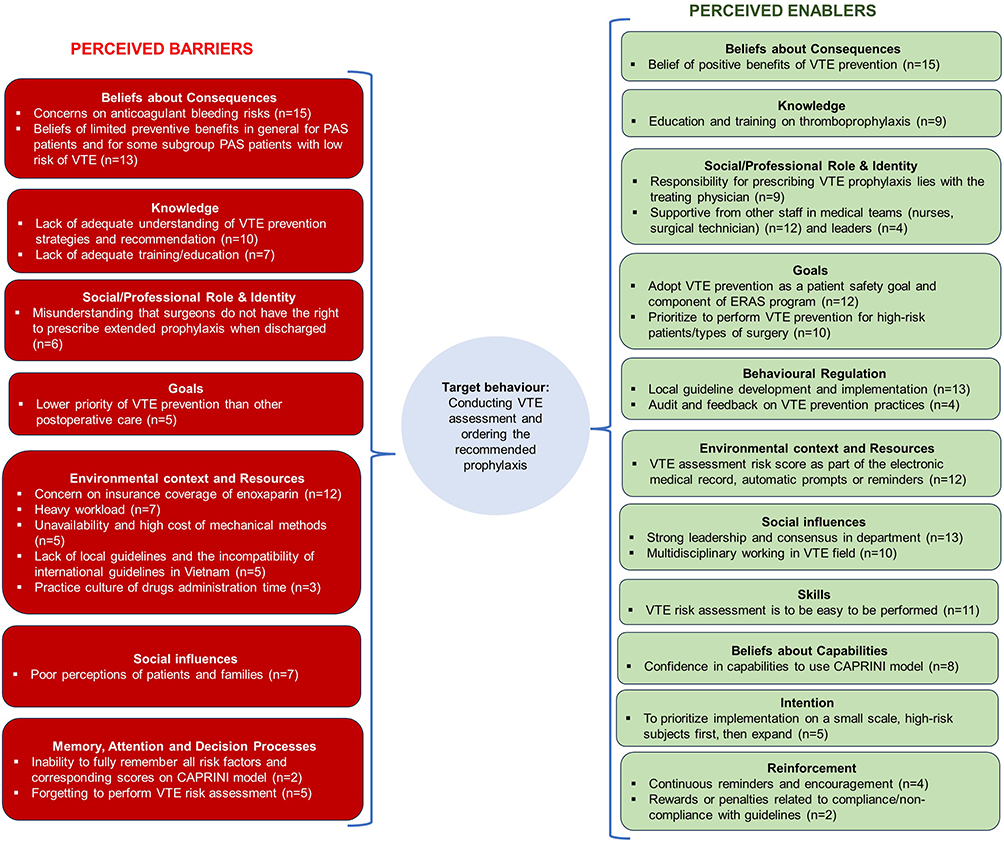 |
Figure 2 Barriers and enablers to VTE prevention practices reported by surgeons. |
Detailed Analysis of Themes and Quotes for the Most Frequently Coded Theoretical Domains
Intrapersonal Factors That Influence Physicians’ Practice of VTE Prophylaxis for PAS Patients
Beliefs About Consequences
All participants identified several different benefits and risks associated with anticoagulant use that could potentially influence VTE prevention practice.
Among the perceived benefits, almost all participants believed that the implementation of VTE prevention practices would generally reduce the development of DVT and PE, morbidity, and mortality. Moreover, it would decrease the financial burden on both the hospital and the patient, protect doctors and hospital reputation, and reduce hospitalization days and management. Their beliefs were also strengthened by the fact that they have faced serious cases of pulmonary embolism in the absence of thromboprophylaxis, their experience of a good safety profile for postoperative enoxaparin use, and the advancement of surgical techniques that also help reduce postoperative bleeding complications.
…prevention complications of deep vein thrombosis and even pulmonary embolism and even risk of death. And there is a high rate of these complications in major abdominal surgery and especially cancer surgery. (BS2)
…reduce costs for hospital. Treating a case of pulmonary infarction costs a lot of money. (BS3)
In addition to the benefits, most participants also believed that the indication for thromboprophylaxis may be negatively affected by surgeons’ concerns regarding the bleeding risks of anticoagulants. Doctors mentioned that they often start anticoagulation later than recommended (usually after 24 h) to ensure adequate monitoring to eliminate the patients’ risk of bleeding as much as possible. In addition, doctors were also concerned about the serious consequences of bleeding in outpatients; therefore, they ignored extended anticoagulants for major cancer surgery patients.
We usually let the hemodynamics stabilize, we can usually start anticoagulant after 6 - 12 hours, depending on the patient. We usually let it start after 24 hours. (BS3)
Having an out-of-hospital complication due to anticoagulants is very complicated. (BS2)
Some participants also expressed their beliefs about the limited benefits of thromboprophylaxis for some types of surgery, such as gall bladder resection, gallstone removal, hemorrhoidectomy, or fistulotomy. Many surgeons mentioned that they have reported very few cases of thrombosis associated with abdominopelvic surgery in the past few years. Hence, they expressed their desire to provide data on the local incidence of an event. Furthermore, to increase the number of patients receiving extended prophylaxis, it is necessary to provide information about whether the benefits are worth the required resources (costs and risks of anticoagulant use).
Currently, although the high risk VTE group in my department accounts for about 50%, actually I rarely see its complication [VTE] in practice. (BS16)
Now we don’t give thromboprophylaxis, but everything seems to be fine. So, we need to understand comprehensively the reason why we must apply it. (BS4)
Knowledge
Most surgeons have a certain level of knowledge regarding VTE prevention guidelines and thromboprophylaxis strategies for patients with PAS. They listed enoxaparin as a prophylactic pharmacological option.
ESMO, NCCN or even in our country also give recommendations on anticoagulant prophylaxis in major abdominal surgery and cancer. (BS2)
In-depth interviews also showed that the majority of doctors seemed to lack in-depth understanding of VTE prevention strategies. Only about 1/3 of the participants could list the names or detailed contents of the guidelines and VTE risk assessment model. They could not name the recommendations/guidelines or the commonly used scoring scales to assess the risk of VTE. Some doctors explained that, because they were surgical doctors and the issue of thromboprophylaxis was not their specialty, they did not thoroughly exploit the VTE prevention guidelines.
Basically, I’m not in that major…I don’t go in-depth. Just follow and learn from others’ experiences. (BS1)
However, nearly half of the doctors said that their current education and training on this topic was inadequate. Hence, most surgeons mentioned that education and information about the importance of VTE recommendations, preferably by highly experienced specialist doctors, will improve VTE prevention practices.
There hasn’t been much formal training. (BS12)
Social/Professional Role and Identity
Most participants identified VTE prevention as part of their professional roles and jobs. In addition, many doctors mentioned the role of other medical staff in providing important patient information to support their decision-making regarding thromboprophylaxis. Specifically, surgical technicians should note the complexity of the procedure and the risk of bleeding to the treating physician, and nurses should collect factors in the risk assessment model at the time of patient admission.
The responsibility is still to be the treating doctors (BS2)
The nurse can collect VTE risk factors when patients admitted to department. (BS6)
Notably, more than one-third of the doctors expressed ambiguity about their responsibility in prescribing extended anticoagulants after discharge from the hospital. They believe that they are surgeons, so prescribing extended thromboprophylaxis is not their responsibility; instead, the person who can prescribe it is an internal medicine doctor, or there must be coordination between surgeons and cardiologists.
We are surgeons, prescribing outpatient anticoagulation may cause legal problems, requiring coordination with a cardiology specialist. (BS1)
Goals
The vast majority of participants evaluated that performing VTE practice would support the common healthcare goal of improving the safety of surgical patients. Some doctors have mentioned VTE practice as a mandatory component of the early recovery after surgery (ERAS) program, which is being vigorously conducted at the hospital. However, a small number of physicians emphasized that thromboprophylaxis, although important, is a lower priority than other post-operative care; therefore, doctors’ time and attention towards this practice are sometimes limited.
promoting preventive medicine, meaning prevention is better than cure. (BS7)
VTE prevention is important, but it still has to come after other post operative care. (BS6)
Two-thirds believed that thromboprophylaxis programs need to prioritize prevention for high-risk patients who benefit the most from this practice.
I will select patients with high risk factors, e.g. in our department colorectal cancer…As for those with hemorrhoids or appendicitis, I don’t use prevention. (BS6)
For example, pancreaticoduodenectomy, gastrectomy, colon resection surgery can be offered VTE prevention practice on a regular basis. (BS7)
Behavioral Regulation
The interviewed participants identified various suggestions on how to regulate and influence physicians to perform VTE assessment and order the recommended prophylaxis.
Almost all physicians highlighted that the development and implementation of local VTE guidelines would facilitate VTE prevention practice. Furthermore, it would protect them from legal problems if adverse events associated with anticoagulant use occurred. Moreover, as per the many participants, making VTE guidelines mandatory would support the target behavior.
When you follow the prophylaxis regimen that was agreed upon in the hospital, if any problem occurs, you will have legal protection. (BS11)
Monitoring compliance with VTE guidelines and sharing or feedback on the results would encourage the implementation of VTE guidelines.
Whenever deploying something, there needs to audit and feedback. (BS4)
The Environmental Factors That Influence Physicians’ Practice of VTE Prophylaxis for PAS Patients
Environmental Context and Resources
Almost all the participants referred to various environmental factors that affected their thromboprophylaxis practices. The vast majority of surgeons expressed uncertainty about health insurance coverage for enoxaparin prescriptions. Having to explain and ask the patient’s caregiver to pay for drugs not covered by insurance also makes it possible for doctors to ignore preventive anticoagulant.
Another problem is that the health insurance does not pay [for Lovenox]. Prescribing enoxaparin carries not only the fear of non-reimbursement but also an extra task of surgeons to explain and ask patients’ caregivers to pay by themselves. (BS3)
In addition, a third stated that mechanical prophylaxis was necessary for patients, but the inadequate availability of mechanical devices in the department and the associated additional treatment costs for the patients negatively affected their decision to order appropriate prophylaxis.
I know [mechanical prophylactic measures] but the problem is where to get the money to use it, shouldn’t I force the patient to buy it? (BS15)
Many participants identified a heavy workload, including the number of patients and the other post operative tasks they had to care for, leading to their omission of conducting VTE risk assessment or sometimes the assessment was still done but not thorough enough. In addition, a few doctors reported that nurses often administer medication to patients at relatively fixed times, making it difficult for individuals to ensure the correct time for anticoagulant initiation. This may explain why a certain proportion of the patients started VTE prophylaxis later than recommended.
It’s not that we don’t know about VTE prevention, we’re busy, we don’t remember, we forget what needs to be done. (BS8)
Nearly one-third of doctors believed that there was currently a lack of local guidelines and policies that stated that it is mandatory to carry out VTE risk assessment and prescribe VTE prophylaxis for all surgical patients in the hospital. In addition, some doctors were concerned about the incompatibility of international guidelines in Vietnam, owing to different patient characteristics and patient management systems. They gave an example that the recommendation of extended prophylaxis for high-risk cancer patients up to 28 days post-discharge is difficult to apply in the Vietnamese in the context that the management of outpatients, especially those taking high-risk medications such as anticoagulants, is not synchronized. This caused a tendency toward suboptimal VTE prevention practices.
The most important thing is to obtain consensus on implementing this practice at the hospital, and must provide specific, detailed protocol, guidance. (BS6)
In addition, most participants indicated that having the VTE assessment risk score as part of the electronic medical record, automatic prompts, or reminders would facilitate implementation of the guidelines.
Going into the hospital software, you will immediately see the score [of VTE risk], and then it will be displayed whether or not you should prescribe VTE prevention, it saves time. (BS4)
The Interpersonal Factors That Influence Physicians’ Practice of VTE Prophylaxis for PAS Patients
Social Influences
Apart from the physical environment, social environment is another major determinant of VTE prevention practices. The social influences domain identifies whether leaders, other members of the medical team, and patients or their relatives may influence physicians’ decisions to order the recommended prophylaxis. In-depth interviews showed that a substantial portion of surgeons mentioned the great influence of department leaders on their practice of VTE, with roles including issuance of mandatory regulations on VTE risk assessment, ordering thromboprophylaxis among doctors, promoting implementation progress, and reminders on implementation.
If the department wants to implement a protocol on thromboprophylaxis, it must be firstly approved by the department leader. (BS1)
Professional consensus among physicians also plays an important role in promoting VTE prevention practices. Specifically, despite the unavailability of a VTE prevention protocol in the hospital and the irregularity in VTE risk assessments using the CAPRINI score, two-thirds mentioned that doctors in their departments had discussions and agreed on several specific characteristics of high-risk VTE, including patient and procedural factors, to consider routine VTE prophylaxis for these patients.
In our department, most major surgeries are performed on cancer patients. By default, for patients undergoing surgery for liver cancer or pancreatic cancer, we will use prophylactic anticoagulants, and for minor surgeries, we will not use anticoagulants. (BS8)
Half of the participants indicated that they had discussed VTE recommendations with team members. In addition, multi-specialty coordination in implementing systematic VTE practice, for example, with cardiologists or pharmacists, was also emphasized by half of the doctors. Moreover, participants stated that they sought the opinions of experts in the field.
We must discuss with each surgeon whether there are any special issues during surgery that need caution when using prophylaxis anticoagulant postoperatively…They will advise the treating doctor whether to start anticoagulants within the first 24 hours, after 24 hours, or delay further. (BS9)
Furthermore, just under half of the participants stated that their decision was affected by the patient and family’s level of awareness about VTE risks and refusal of prophylaxis treatment.
But implementing extended prophylaxis…letting patients self-inject anticoagulants on an outpatient basis is very difficult. Because patients with chronic diabetes may not be able to inject insulin subcutaneously correctly. (BS7)
The problem is that we may indicate anticoagulants or mechanical devices for prophylaxis, but patients say nothing is wrong with them, so why do I ask them to self-pay for those things. (BS9)
Discussion
There is a growing body of evidence that indicates suboptimal utilization of VTE prophylaxis in at-risk surgical patients, particularly non orthopedic procedures.6 Implementing interventions to improve thromboprophylaxis practices for at-risk patients is an important focus of anticoagulant stewardship and quality improvement programs in hospitals.5,13 The urgency of these actions is heightened in underdeveloped and developing nations, where the adoption rate of standardized preventative measures is markedly inferior to that in resource-abundant countries.6–8 It is necessary to report the adherence rate to evidence-based recommendations, accompanied by a comprehensive understanding of the influencing factors, to inform the most likely successful interventions locally.5,12 In this study, we adopted an explanatory sequential mixed-method research design to address this research question in a tertiary care hospital in Vietnam.
The Quantitative Phase
The audit results indicated a distinct mismatch between the guidelines and the actual VTE prevention practices, highlighting a potential area for future enhancement. Two significant deficiencies in thromboprophylaxis were the underuse of prophylactic measures and insufficient duration of pharmacological prophylaxis. Hence, we focus the subsequent discussion on these two issues.
Underuse of Prophylaxis
A very low proportion of PAS patients (11.7%) received appropriate VTE prophylaxis. In comparison, a similar figure of 11.8% of appropriate prophylaxis was recorded in the DissolVE-2 study which was conducted in 60 urban, tertiary Chinese hospitals.40 In a multicenter study in Lebanese and Jordanian hospitals, there is also a substantial underuse of thromboprophylaxis among hospitalized patients; in which less than half of at-risk surgical patients received their recommended thromboprophylaxis.41 The proportion of VTE prophylaxis in our study was far lower than in many previous observations, such as 58.5% in the ENDORSE study,6 73.9% in cancer PAS patients,18 80% in surgical patients.42 Lower rates of appropriate thromboprophylaxis in Asian country than in other regions have been revealed in a meta-analysis by Gabor Forgo.7,8
The lack of adequate prophylaxis was an emerging issue in our study, when nearly all inappropriate cases (87.9%) were classified as underuse of prophylaxis. Overuse of prophylaxis was not a significant issue in this study, contrasting with Hajj’s study, when 66.9% of the surgical patients who were ineligible for VTE prophylaxis were administered prophylactic agents.41
We would like to underscore the issue of underutilization of VTE prophylaxis in cancer PAS patients as standard pharmacological prophylaxis is advised for all patients undergoing major cancer surgery unless contraindicated.21,28 In our study, although there were 86 patients undergoing major abdominal and pelvic surgery for cancer, only 30.2% received recommended postoperative thromboprophylaxis, which was lower than the expected rate of 100%. This figure is also lower than the high concordance rate recorded in previous studies on patients with major abdominal pelvic cancer, at 40.4% (by Krell et al), 73.9% (by Geahchan et al), and as high as 98.1% (by Logan et al).18,43–45 Without prophylaxis, the risk of VTE in cancer patients undergoing surgery has been estimated to be as high as 50%, and VTE is found to be the most common cause of death in this group of patients at 30 days after surgery.46 Thus, enhanced initiatives are necessary to close the gap between existing VTE prevention practice and standard recommendations for patients undergoing abdominal or pelvic surgery for cancer.
Inadequate Length of Thromboprophylaxis
In 28 cases where enoxaparin indication was appropriate, only 28.6% were evaluated as adherent to the recommendation on the minimum length of prophylaxis. Thromboprophylaxis was classified as shorter than the recommended duration in all remaining cases (71.4%).
It is established that in patients undergoing abdominal or pelvic surgery for cancer, extended duration of thromboprophylaxis is associated with a significant reduction in the incidence of clinical VTE without a significant increase in clinically relevant bleeding.47 Hence, extended prophylaxis with LMWH is widely recommended in numerous national as well as international guidelines.48 Despite these recommendations, adoption of extended thromboprophylaxis in clinical practice remains low and clinical equipoise seems to persist.48 Our study revealed that in a tertiary care hospital in Vietnam, no cancer PAS patient was prescribed anticoagulation at discharge to achieve optimal prophylaxis duration up to 28 days. In comparison, previous studies also reported a low rate of outpatient ordering of chemoprophylaxis after major cancer surgery, with rates ranging from 1% to 30%.8,43,49 Notably, several studies also report very low rates of extended prophylaxis, similar to our finding, such as 0% in Vázquez et al,50 2.9% in Laureano et al.51 In a cohort study using VASQIP data reported by 101 VHA hospitals nationwide, while inpatient chemoprophylaxis was ordered for a high rate of cancer surgery patients (80.4%), only 10.5% received discharge chemoprophylaxis.43 The inadequate execution of recommendations for extended prophylaxis in cancer PAS patients is a concern not just in Vietnam but also in other international hospitals. These challenges require further investigation of their underlying rationale to inform quality improvement interventions.
The Qualitative Phase and Associated Interpretation With Key Quantitative Data Results
This study identified a set of beliefs that are facilitators or barriers to VTE guideline implementation among surgical physicians using the TDF Framework. Seven out of 12 TDF domains stood out, and focusing on these seven prominent domains, which represented 86.0% of the emerging themes, is likely to reveal key insights that can shape important future interventions. The influencing factors identified from these key domains are discussed in more detail, and the corresponding quantitative results are also discussed. Based on our research findings, we also discuss what interventions can be effective in the tertiary care context, which is best carried out within the framework of a quality improvement program or an anticoagulant stewardship program.
The Barriers to Implementation of VTE Prevention Practice
The Intrapersonal Barriers
Almost all surgeons recognized the risk of bleeding as an important barrier to anticoagulant prescribing, similar to previous studies.37,52–54 This concern also explained the quantitative data, in which 50% of the PAS patients were initiated anticoagulants later than recommended. Additionally, the low adherence rate regarding the length of VTE prophylaxis could be partly explained by this concern. Indeed, our study was conducted in a tertiary hospital in Vietnam, where patients have not been managed synchronously in the health system. This context led to the surgeons’ special concern that timely monitoring and management of complications of high-risk medications, such as anticoagulants, in outpatients is very challenging.
Some healthcare professionals expressed low trust in the benefits of thromboprophylaxis because they had seen very few cases of thrombosis associated with abdominal pelvic surgery. These results are consistent with the findings of Gaston et al.22 This barrier explained that although 52.1% of patients were at a high risk of VTE, a very low proportion (11.7%) received their recommended prophylaxis. Our participants were also ambiguous about the benefits of extended VTE prophylaxis post-discharge and wondered whether extended prophylaxis provides benefits commensurate with the expended resources and the associated risks for the patients. We believe that physicians might have underestimated the risk and incidence of VTE when they relied only on events observed during a patient’s very short hospital stay. Actually, VTE complications, including fatal PE, may occur up to 30 days after discharge.55 Their underestimation is likely to be biased and might have led to misdirected practice. Providing more well-established evidence to doctors about the incidence of events and the effectiveness of extended prophylaxis is therefore extremely necessary to strengthen their beliefs about preventive benefits. Similarly, in a study conducted in Iran, the majority of participants underestimates the prevalence and consequences of VTE in daily practice, probably due to low levels of awareness of presence and content of VTE guidelines and the authors also suggested that programs should be designed to uphold the levels of information of DVT prophylaxis guidelines.56
In-depth interviews also showed that two-thirds of the doctors were not fully aware of VTE risk assessment and prevention strategies. Our findings are similar to those described in the literature.22,37 A survey of medical staff at a tertiary hospital in China also concludes that medical institutions should improve staff training regarding VTE prophylaxis, and that medical staff should be encouraged to actively engage in VTE prophylaxis, stemming from the results showing that healthcare workers’ knowledge about thrombosis prevention is still poor.57
We also identified another important barrier that contributed to the fact that patients undergoing surgery for abdominal and pelvic tumors at high risk of VTE were not prescribed enoxaparin for up to 28 days after surgery. There was a misconception among surgeons that the responsibility for prescribing anticoagulation therapy upon discharge belonged to the cardiologist and not their professional responsibility. Therefore, in the future, when developing a procedure for preventing VTE at the hospital, there should be specific regulations on the responsibilities of surgeons regarding outpatient anticoagulant prophylaxis prescription.
Environmental Factors
Repeatedly, the workload pressure on admitting physicians was highlighted as one of the barriers preventing physicians from implementing appropriate VTE prevention practices. A common situation in such public hospitals in Vietnam is that one doctor needs to manage and monitor a large number of patients, so they are generally more focused on treating immediate health care problems that precipitate hospital admission than on preventing future complications. A high workload might prevent them from completing the VTE risk assessment, ordering necessary measures, and administering appropriate thromboprophylaxis in a suitable manner for all patients. This barrier agrees with the previous findings.22,37 VTE prevention and management was reported as not being the highest on their list of actions to take in relation to surgical patient care. Healthcare professionals often stated they were too busy to add this to their practice, or they simply forgot to complete the requirements for VTE care. Surgeons were more focused on treating the immediate health care problem precipitating hospital admission than on preventing future complications.58 Patients who do not initiate VTE prophylaxis early may be missed during the whole remaining hospital stay.
Lack of system support was also seen as a barrier when there were no developed guidelines for VTE within the health service and no risk assessment tools to use.22 This barrier was also stated in our study.
Additionally, some surgeons were ambiguous whether enoxaparin was covered by health insurance in Vietnam. According to Vietnamese regulations, drugs are currently covered by insurance when used according to drug labels, national formularies, or national guidelines from the Ministry of Health. All three sources support the use of enoxaparin as surgical prophylaxis in moderate-to high-risk patients. Hence, providing this information to clinicians will be helpful in promoting the target behavior. Furthermore, anti-embolic stockings and intermittent pneumatic compression were reported to have cost restrictions and were unavailable in the ward. This finding is similar to the key findings of Gaston et al.22
The Interpersonal Factors
Interpersonal factors and the social environment were key determinants of VTE prevention practice. In-depth interviews showed that just under half of the participants stated that their decision was affected by the patient and family’s level of awareness and attitude towards VTE risk and VTE prophylaxis treatment, which is similar to Cabana’s finding.23 The inability to reconcile patient preferences with guideline recommendations was a barrier to adherence.37 Previous work concludes that better information for patients on the risks and benefits of prophylaxis might decrease the refusal rate and increase compliance with VTE prophylaxis.59
The Facilitators to the Implementation of VTE Prevention Practice
Although there was a quality gap in the current VTE prophylaxis practice, it could be clearly seen from the quantitative data that physicians had adopted VTE guidelines for a certain group of patients. This is explained by the qualitative findings that surgeons tend to prioritize VTE prevention for high-risk VTE patients or high-risk VTE surgery. The perceived benefits of VTE guideline implementation by our participants are similar to the findings of Abboud et al.37 VTE prevention practices were also believed by doctors to be further adopted in the near future as a patient safety goal and an important component of the ERAS program, which is beginning to be implemented in hospitals. Therefore, in the context of no protocol or policy issued at the facility, the development and official issuance of VTE guidelines are necessary.60 Having a mandatory VTE policy would also support wider VTE implementation.5,12,37
Our surgeons identified a range of strategies to facilitate improvements in VTE prevention practice. Education and training in VTE guidelines, preferably by highly experienced specialist doctors, will improve VTE prevention practice. Monitoring compliance with VTE guidelines through audits and feedback, where clinical audits were deployed at regular intervals and the results were reported back to clinicians, was identified as one of the facilitators to reinforce the target behavior. Audit and feedback strategies are among the main interventions followed in several studies and provide guidance to support the implementation of VTE guidelines.22,37,60
However, participants highlighted that integrating the VTE risk assessment tool into electronic medical records and the development of a computer-based clinical decision support system would facilitate VTE practices. This would overcome barriers such as large workloads, lack of attention, forgetfulness of risk assessment, and difficulty in remembering the CAPRINI scale and would also act as a reminder. This is similar to other studies and can provide support for clinicians by providing prompts and guiding practice through clinical support decision instructions.22,37,61,62 Moreover, computer alerts are associated with higher proportions of patients who received VTE prophylaxis.63 Implementation of a multifaceted intervention consisting of clinical decision support software significantly increases guideline adherence.5,64
The practice culture was strongly evident in the interviews and was determined by senior physicians’ impact, especially the leader of the department. Thus, leader physicians are key to influencing the target behavior and introducing changes. This is similar to the previous literature, where participants indicated that the seniors from the clinical team had an impact on their behavior and they might change their prophylaxis order based on the discussion with the senior.37 The authors conclude that senior clinicians are the key enablers for VTE prophylaxis practice change. They need to be convinced that guideline compliance adds value to their patient care, and with the support of systems, they will drive practice changes in their teams.37,65
The Urgent Need for Anticoagulant Stewardship Implementation
Our study clearly demonstrates the “implementation gap” between evidence-based best practices and real world practices in VTE prophylaxis for non-orthopedic surgery patients in tertiary care in Vietnam. We believe that the study results not only reflect the circumstances at our facility but may also represent the typical features of hospitals of comparable sizes and levels of care in Vietnam. The low percentage of high-risk PAS patients receiving sufficient VTE prophylaxis necessitates prompt attention. Simultaneously, the qualitative results indicated the concurrent presence and intricate interrelations of numerous influencing factors, particularly barrier factors. Therefore, the execution of multifaceted interventions incorporated within the anticoagulant stewardship program framework is the most suitable solution for tackling these complex practice challenges.5,12,13,64 In contrast to developed countries, where anticoagulant stewardship programs have been extensively established and widely implemented as a priority within health systems, Vietnam currently lacks legal documentation and standards for the implementation of these activities.13 This policy gap also needs to be addressed at both national and grassroots levels to facilitate sustained practice improvement. Our institution should implement hospital-based management programs to promptly enhance existing suboptimal practices, guaranteeing that patients undergoing non-orthopedic surgery, especially major abdominal and pelvic surgery, receive optimal VTE prevention according to current best practices.
Conclusion
Our quantitative analysis indicated that although a considerable proportion of abdominal and pelvic surgical patients are at risk of developing VTE postoperatively, there is a low rate of appropriate thromboprophylaxis. Two significant gaps in VTE prophylaxis practice for PAS patients were underuse of VTE prophylaxis and shorter-than-recommended prophylaxis. The application of the Theoretical Domain Framework has revealed the facilitators and barriers that influenced VTE preventative practice. Implementation of quality improvement initiatives, optimally conducted within the framework of an anticoagulant stewardship program, is urgently needed.
Acknowledgments
We gratefully acknowledge the participants who took valuable time to participate in this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Henke PK, Kahn SR, Pannucci CJ, et al. Call to action to prevent venous thromboembolism in hospitalized patients: a policy statement from the American heart association. Circulation. 2020;141(24):e914–e931. doi:10.1161/CIR.0000000000000769
2. Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis, 9th ed: American college of chest physicians evidence-based clinical practice guidelines. Chest. 2012;141(2 Suppl):e227S–e277S. doi:10.1378/chest.11-2297
3. Merkow RP, Ju MH, Chung JW, et al. Underlying reasons associated with hospital readmission following surgery in the United States. JAMA. 2015;313(5):483–495. doi:10.1001/jama.2014.18614
4. Anderson FA Jr, Zayaruzny M, Heit JA, Fidan D, Cohen AT. Estimated annual numbers of US acute-care hospital patients at risk for venous thromboembolism. Am J Hematol 2007;82(9):777–782. doi:10.1002/ajh.20983
5. Agency for Healthcare Research and Quality (AHRQ). Preventing Hospital-Associated Venous Thromboembolism a Guide for Effective Quality Improvement; 2019.
6. Cohen AT, Tapson VF, Bergmann J-F, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet. 2008;371(9610):387–394. doi:10.1016/S0140-6736(08)60202-0
7. Forgo G, Micieli E, Ageno W, et al. An update on the global use of risk assessment models and thromboprophylaxis in hospitalized patients with medical illnesses from the World Thrombosis Day steering committee: systematic review and meta-analysis. J Thrombosis Haemostasis. 2022;20(2):409–421. doi:10.1111/jth.15607
8. Merkow RP, Bilimoria KY, McCarter MD, et al. Post-discharge venous thromboembolism after cancer surgery: extending the case for extended prophylaxis. Ann Surg. 2011;254(1):131–137. doi:10.1097/SLA.0b013e31821b98da
9. Anderson DR, Morgano GP, Bennett C, et al. American Society of Hematology 2019 guidelines for management of venous thromboembolism: prevention of venous thromboembolism in surgical hospitalized patients. Blood Adv. 2019;3(23):3898–3944. doi:10.1182/bloodadvances.2019000975
10. Thrombosis Canada. Thromboprophylaxis After Non-Orthopedic Surgery; 2022.
11. Lyman GH, Carrier M, Ay C, et al. American Society of Hematology 2021 guidelines for management of venous thromboembolism: prevention and treatment in patients with cancer. Blood Adv. 2021;5(4):927–974. doi:10.1182/bloodadvances.2020003442
12. Australian Commission on Safety and Quality in Health Care. Implementation guide venous thromboembolism prevention clinical care standard. 2020.
13. Anticoagulation forum. Core Elements of Anticoagulation Stewardship Programs; 2019.
14. Manoucheri R, Javad M. Adherence to venous thromboprophylaxis guidelines for medical and surgical inpatients of teaching hospitals, Shiraz-Iran. Tanaffos. 2015;14(1):17–26.
15. Randelli F, Cimminiello C, Capozzi M, Bosco M, Cerulli G. Real life thromboprophylaxis in orthopedic surgery in Italy. Results of the GIOTTO study. Thrombosis Res. 2016;137:103–107. doi:10.1016/j.thromres.2015.11.007
16. Hương Giang L. Study on the current status of using drugs to prevent venous thromboembolism in patients undergoing major orthopedic surgery. J 108 - Clin Med Pham. 2022;17(3):1.
17. Badge H, Churches T, Naylor JM, et al. Compliance with Australian orthopaedic association guidelines does not reduce the risk of venous thromboembolism after total hip and knee arthroplasty. Sci Rep. 2024;14(1):5955. doi:10.1038/s41598-024-54916-x
18. Geahchan N, Basile M, Tohmeh M. Venous thromboembolism prophylaxis in patients undergoing abdominal and pelvic cancer surgery: adherence and compliance to ACCP guidelines in DIONYS registry. SpringerPlus. 2016;5(1):1541. doi:10.1186/s40064-016-3057-9
19. McAlpine K, Breau R, Carrier M, et al. Thromboprophylaxis practice patterns and beliefs among physicians treating patients with abdominopelvic cancers at a Canadian centre. Can J Surg J Canadien de Chirurgie. 2020;63(6):E562–e568. doi:10.1503/cjs.015219
20. Streiff MB, Holmstrom B, Ashrani A, et al. Cancer-associated venous thromboembolic disease, version 1.2015. J Nat Comprehensive Cancer Network. 2015;13(9):1079–1095. doi:10.6004/jnccn.2015.0133
21. Key NS, Khorana AA, Kuderer NM, et al. Venous thromboembolism prophylaxis and treatment in patients with cancer: ASCO guideline update. J Clin Oncol. 2023;41(16):3063–3071. doi:10.1200/JCO.23.00294
22. Gaston S, White S. Systematic review of barriers and facilitators to venous thromboembolism clinical practice guideline compliance by healthcare professionals in acute care. Int J Cardiovasc Cerebrovasc Dis. 2013;1:1–9. doi:10.13189/ijccd.2013.010101
23. Cabana MD, Rand CS, Powe NR, et al. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA. 1999;282(15):1458–1465. doi:10.1001/jama.282.15.1458
24. Michie S, van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:42. doi:10.1186/1748-5908-6-42
25. Tariq S, Woodman J. Using mixed methods in health research. JRSM Short Rep. 2013;4(6):2042533313479197. doi:10.1177/2042533313479197
26. Fischer F, Lange K, Klose K, Greiner W, Kraemer A. Barriers and strategies in guideline implementation—A scoping review. InHealthcare. 2016;4(3):36. doi:10.3390/healthcare4030036
27. Leung FH, Savithiri R. Spotlight on focus groups. Cana Family Physician Med Famille Canadien. 2009;55(2):218–219.
28. Vietnam National Heart Association. Recommendations on the Diagnosis, Treatment and Prevention of Venous Thromboembolism; 2022.
29. Queensland Health. Guideline for the Prevention of Venous Thromboembolism (VTE) in Adult Hospitalised Patients; 2018.
30. Streiff MB, Holmstrom B, Angelini D, et al. Cancer-associated venous thromboembolic disease, version 2.2021, NCCN clinical practice guidelines in oncology. J Nat Comprehensive Cancer Network. 2021;19(10):1181–1201. doi:10.6004/jnccn.2021.0047
31. Menaka Pai M, Douketis JD. Prevention of venous thromboembolic disease in adult nonorthopedic surgical patients. UpToDate. 2022;2022:1.
32. Atkins L, Francis J, Islam R, et al. A guide to using the theoretical domains framework of behaviour change to investigate implementation problems. Implement Sci. 2017;12(1):77. doi:10.1186/s13012-017-0605-9
33. Nazar Z, Naseralallah LM, Stewart D, Paudyal V, Shafei L, Weidmann A. Application of behavioural theories, models, and frameworks in pharmacy practice research based on published evidence: a scoping review. Int J Clin Pharm. 2024;46(3):559–573. doi:10.1007/s11096-023-01674-x
34. Stewart D, Al Hail M, Al-Shaibi S, et al. A scoping review of theories used to investigate clinician adherence to clinical practice guidelines. Int J Clin Pharm. 2023;45(1):52–63. doi:10.1007/s11096-022-01490-9
35. Cowdell F, Dyson J. How is the theoretical domains framework applied to developing health behaviour interventions? A systematic search and narrative synthesis. BMC Public Health. 2019;19(1):1180. doi:10.1186/s12889-019-7442-5
36. Cane J, O’Connor D, Michie S. Validation of the theoretical domains framework for use in behaviour change and implementation research. Implement Sci. 2012;7:37. doi:10.1186/1748-5908-7-37
37. Abboud J, Rahman AA, Shaikh N, Dempster M, Adair P. Physicians’ perceptions and preferences for implementing venous thromboembolism (VTE) clinical practice guidelines: a qualitative study using the Theoretical Domains Framework (TDF). Arch Public Health. 2022;80(1):52. doi:10.1186/s13690-022-00820-7
38. Debono D, Taylor N, Lipworth W, et al. Applying the theoretical domains framework to identify barriers and targeted interventions to enhance nurses’ use of electronic medication management systems in two Australian hospitals. Implement Sci. 2017;12(1):42. doi:10.1186/s13012-017-0572-1
39. Hallsworth K, Dombrowski SU, McPherson S, Anstee QM, Avery L. Using the theoretical domains framework to identify barriers and enabling factors to implementation of guidance for the diagnosis and management of nonalcoholic fatty liver disease: a qualitative study. Transl Behav Med. 2020;10(4):1016–1030. doi:10.1093/tbm/ibz080
40. Zhai Z, Kan Q, Li W, et al. VTE risk profiles and prophylaxis in medical and surgical inpatients: the identification of Chinese hospitalized patients’ risk profile for venous thromboembolism (DissolVE-2)-A cross-sectional study. Chest. 2019;155(1):114–122. doi:10.1016/j.chest.2018.09.020
41. Hajj I, Al-Masri M, Bashaireh K, et al. A cross-sectional, multicenter, observational study to assess the prophylaxis of venous thromboembolism in Lebanese and Jordanian hospitals. Thromb J. 2021;19(1):9. doi:10.1186/s12959-021-00261-2
42. Ismail A, Jadawji N, Adebayo P, et al. Evaluation of venous thromboembolism (VTE) risk assessment and thrombo-prophylaxis practices in hospitalized medical and surgical patients at Aga Khan Hospital Dar es Salaam: single-centre retrospective study. Pan Afr Med J. 2022;42:160. doi:10.11604/pamj.2022.42.160.28278
43. Logan CD, Hudnall MT, Schlick CJR, et al. Venous thromboembolism chemoprophylaxis adherence rates after major cancer surgery. JAMA Network Open. 2023;6(9):e2335311. doi:10.1001/jamanetworkopen.2023.35311
44. Ramanathan R, Lee N, Duane TM, et al. Correlation of venous thromboembolism prophylaxis and electronic medical record alerts with incidence among surgical patients. Surgery. 2016;160(5):1202–1210. doi:10.1016/j.surg.2016.04.029
45. Yang AD, Hewitt DB, Blay E Jr, et al. Multi-institution evaluation of adherence to comprehensive postoperative VTE chemoprophylaxis. Ann Surg. 2020;271(6):1072–1079. doi:10.1097/SLA.0000000000003124
46. Bhagya Rao B, Kalayarasan R, Kate V, Ananthakrishnan N. Venous thromboembolism in cancer patients undergoing major abdominal surgery: prevention and management. ISRN Vasc Med. 2012;2012:783214. doi:10.5402/2012/783214
47. Knoll W, Fergusson N, Ivankovic V, et al. Extended thromboprophylaxis following major abdominal/pelvic cancer-related surgery: a systematic review and meta-analysis of the literature. Thrombosis Res. 2021;204:114–122. doi:10.1016/j.thromres.2021.06.010
48. Noureldin A, Ivankovic V, Delisle M, Wang TF, Auer RC, Carrier M. Extended-duration thromboprophylaxis following major abdominopelvic surgery – for everyone or selected cases only? Thrombosis Res. 2024;235:175–180. doi:10.1016/j.thromres.2024.01.026
49. Mavros MN, Johnson LA, Schootman M, Orcutt ST, Peng C, Martin BC. Adherence to extended venous thromboembolism prophylaxis and outcomes after complex gastrointestinal oncologic surgery. Ann Surg Oncol. 2023;30(9):5522–5531. doi:10.1245/s10434-023-13677-z
50. Vázquez FJ, Bilbao MS, Saimovici J, Vaccaro C. Improving adherence rate of extended prophylaxis for venous thromboembolic disease after abdominal and pelvic oncologic surgery: a pilot educational study. Clin Appl Thrombosis/Hemostasis. 2015;21(8):750–754. doi:10.1177/1076029615583348
51. Laureano M, Ebraheem M, Crowther M. Extended venous thromboembolism prophylaxis after abdominopelvic cancer surgery: a retrospective review. Current Oncol. 2019;26(1):e106–e110. doi:10.3747/co.26.4339
52. Gaston S, White S, Misan G. Venous thromboembolism (VTE) risk assessment and prophylaxis: a comprehensive systematic review of the facilitators and barriers to healthcare worker compliance with clinical practice guidelines in the acute care setting. JBI Lib Syst Rev. 2012;10(57):3812–3893. doi:10.11124/jbisrir-2012-12
53. Kahn SR, Morrison DR, Cohen JM, et al.Interventions for implementation of thromboprophylaxis in hospitalized medical and surgical patients at risk for venous thromboembolism. Cochrane Database Syst Rev. 2013;(7):CD008201. doi:10.1002/14651858.CD008201.pub2
54. Ekwere T, Ino-Ekanem BM, Ekanem A. Venous thromboembolism: awareness and practice of thromboprophylaxis among physicians in a tertiary-care hospital. Int J Med Biomed Res. 2015;4:14–20. doi:10.14194/ijmbr.4.1.3
55. Van Hemelrijck M, Garmo H, Holmberg L, et al. Thromboembolic events following surgery for prostate cancer. Europ Urol. 2013;63(2):354–363. doi:10.1016/j.eururo.2012.09.041
56. Ebrahimpur M, Gohari Moghadam K, Pejman Sani M, Knowledge NZ. Attitudes and practices of internal medicine residents towards deep vein thrombosis prophylaxis in a university hospital in Tehran. Shiraz E-Med J2016;17(12):e39038.
57. Feng S, Li M, Wang K, et al. Knowledge, attitudes, and practices regarding venous thromboembolism prophylaxis: a survey of medical staff at a tertiary hospital in China. Medicine. 2021;100(49):e28016. doi:10.1097/MD.0000000000028016
58. Cook D, Tkaczyk A, Lutz K, McMullin J, Haynes RB, Douketis J. Thromboprophylaxis for hospitalized medical patients: a multicenter qualitative study. J hosp med. 2009;4(5):269–275. doi:10.1002/jhm.461
59. Popoola VO, Lau BD, Shihab HM, et al. Patient preferences for receiving education on venous thromboembolism prevention - A survey of stakeholder organizations. PLoS One. 2016;11(3):e0152084. doi:10.1371/journal.pone.0152084
60. Anticoagulation forum. Core Elements of Anticoagulation Stewardship Programs Administrative Oversight Gap Analysis: Hospitals and Skilled Nursing Facilities; 2019.
61. Adams P, Riggio JM, Thomson L, Brandell-Marino R, Merli G. Clinical decision support systems to improve utilization of thromboprophylaxis: a review of the literature and experience with implementation of a computerized physician order entry program. Hosp Pract. 2012;40(3):27–39. doi:10.3810/hp.2012.08.987
62. Janus E, Bassi A, Jackson D, Nandurkar H, Yates M. Thromboprophylaxis use in medical and surgical inpatients and the impact of an electronic risk assessment tool as part of a multi-factorial intervention. A report on behalf of the elVis study investigators. J Thromb Thrombolysis. 2011;32(3):279–287. doi:10.1007/s11239-011-0602-9
63. Kahn SR, Morrison DR, Diendéré G, et al. Interventions for implementation of thromboprophylaxis in hospitalized patients at risk for venous thromboembolism. Cochrane Database Syst Rev. 2018;4(4):Cd008201. doi:10.1002/14651858.CD008201.pub3
64. Jaspers T, Duisenberg-van Essenberg M, Maat B, Durian M, van den Berg R, van den Bemt P. A multifaceted clinical decision support intervention to improve adherence to thromboprophylaxis guidelines. Int J Clin Pharm. 2021;43(5):1327–1336. doi:10.1007/s11096-021-01254-x
65. Chapman NH, Lazar SP, Fry M, Lassere MN, Chong BH. Clinicians adopting evidence based guidelines: a case study with thromboprophylaxis. BMC Health Serv Res. 2011;11(1):240. doi:10.1186/1472-6963-11-240
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.