")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
A Health Literate Healthcare Organization Index System for China: Based on CiteSpace and Qualitative Analysis
Authors Zhao S, Chen Y, Xia X, Zhou J, Wang X, Sun Q, Chang J, Ge J, Hu L, Lu R
Received 2 February 2025
Accepted for publication 21 May 2025
Published 1 June 2025 Volume 2025:18 Pages 3065—3090
DOI https://doi.org/10.2147/JMDH.S520366
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Shenyu Zhao,1,* Yang Chen,2,* Xiyang Xia,2 Jing Zhou,2 Xiaoyu Wang,2 Qing Sun,1 Jiaqian Chang,2 Jiaying Ge,2 Lingmin Hu,2 Renjie Lu1,3
1Changzhou Third People’s Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 2Department of Reproduction, Changzhou Maternity and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China; 3Changzhou Institute for Advanced Study of Public Health, Nanjing Medical University, Changzhou, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renjie Lu, Changzhou Third People’s Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected] Lingmin Hu, Department of Reproduction, Changzhou Maternity and Child Health Care Hospital, Changzhou Medical Center, Nanjing Medical University, Changzhou, Jiangsu, 213000, People’s Republic of China, Email [email protected]
Objective: This study aims to analyze the current status and development trends of health literate healthcare organization (HLHO) worldwide, and preliminarily construct an index system suitable for HLHO in China.
Methods: This study first utilized CiteSpace for bibliometric analysis to explore global research hotspots and trends in HLHO. Based on these findings, expert opinions were gathered through focus group interviews to preliminarily develop the index system. Finally, semi-structured interviews in primary hospitals were conducted to optimize the system, assess its adaptability, and collect feedback for refinement.
Results: CiteSpace bibliometric analysis identified high-frequency themes—including health literacy, education, service, communication, health information, digital healthcare, special populations, community, and management—as the primary indices of HLHO. Based on expert input from focus group discussions, an index system comprising 14 primary and 120 secondary indices was developed, covering key domains such as organizational management, health education, provider–patient communication, self-management, digital services, and support for vulnerable groups. Further expert interviews indicated that the system also had good local adaptability and strong potential for broader implementation in primary hospitals.
Conclusion: The index system developed in this study provides both a theoretical framework and a practical tool to support the standardized construction of health-literate healthcare organizations in China. It not only integrates cutting-edge international experience but also aligns with the practical needs of the Chinese healthcare context, demonstrating strong adaptability and relevance. The system is expected to facilitate hospital self-assessment, quality improvement, patient support, and health education efforts, thereby laying a solid foundation for enhancing healthcare service quality and improving patients’ health literacy. Moving forward, our research team will continue to optimize the index system for practical use, and initiate multicenter pilot studies and quantitative scale development to strengthen its operability and value for broader implementation.
Keywords: health literate healthcare organization, CiteSpace, focus group interviews, index system
Background
In the context of globalization, health literacy has become a key index of the advancement of a country’s healthcare system and the health level of its citizens. With a growing recognition of the importance of health literacy, there has been an increased focus on promoting this capability at the organizational level. In recent years, health literacy has expanded from an individual capability to an organizational responsibility, gradually emerging as a key indicator of the sophistication of a nation’s healthcare system. Creating health literacy-friendly medical facilities was significant for enhancing treatment outcomes, promoting changes in patient health behaviors, and improving overall population health.1 The advancement of health literacy depends not only on the cultivation of individual competencies, but also on the ability of healthcare institutions to provide supportive environments and services, driving systematic development at the organizational level. Since 2006, countries like the United States, Turkey, and Germany have proposed similar concepts such as organizational health literacy and have implemented practices to build health literacy at the organizational level.2–4 In 2012, the Institute of Medicine defined health literate healthcare organization (HLHO) as “an organization that makes it easier for people to navigate, understand, and use information and services to manage their health.1,5” Organizational support was considered essential for implementing health literacy initiatives effectively.6,7 In 2020, the United States published the “Healthy People 2030”, which emphasized incorporating a public health perspective and clarified the critical responsibilities of healthcare organizations in enhancing and promoting health literacy.8 In China, with the continued advancement of the Healthy China strategy, organizational health literacy has gradually gained traction in national policy initiatives. In 2024, China issued the Three-Year Action Plan for Improving National Health Literacy (2024–2027), emphasizing the development of health-promoting hospitals, the deep integration of health education, and the enhancement of national health literacy.9
Although a relatively systematic theoretical framework and assessment tools for HLHOs have been developed internationally—such as the Health Literacy Environment of Hospitals and Health Care (HLEHHC),2 the Ten Attributes of Health Literate Health Care Organizations,1 the ten item questionnaire of HLHO based on the ten ideal attributes (HLHO-10),10 the Health Literacy-Sensitive Communication Scale,11 and the Organizational Health Literacy Responsiveness self-assessment tool (Org-HLR tool)12 —these tools primarily focus on dimensions such as patient experience, organizational culture, and communication practices. While informative, these tools show limited alignment with the unique institutional characteristics of China’s healthcare system, including its multi-tiered management structure, uneven digital infrastructure, and the dominant role of public hospitals. Currently, the Chinese government has drafted a reference standard for evaluating health-promoting hospitals. However, most existing research in China remains centered on individual health literacy measurement or fragmented practices within select institutions,13 lacking a systematic, scalable, and localized indicator framework. This gap has hindered the advancement and evaluation of HLHO development in China and forms the central research gap addressed by the present study.
Therefore, building on international experience, this study utilized CiteSpace-based bibliometric analysis to systematically map global research hotspots and trends, while expert input was gathered through focus group interviews to inform the preliminary development of a scientific, operational, and contextually adapted HLHO index system for China. In addition, pilot field testing was conducted in primary healthcare institutions to assess contextual suitability and gather feedback, providing early evidence of the system’s applicability and potential for broader dissemination in local settings. Drawing upon the core elements of international HLHO tools, the system further introduced localized dimensions such as “online service platforms”, “support for special populations”, and “public welfare services”, highlighting organizational empowerment, digital health integration, inclusive support for vulnerable groups, and multi-context service expansion. These enhancements align with China’s healthcare realities, reinforce practical adaptability and equity orientation, and offer a reference for future empirical studies and policy implementation.
Research Methods
Data Sources
This study selected the Web of Science Core Collection in the Web of Science database, with “Science Citation Index Expanded (SCI-EXPANDED) −1975-present” and “Social Sciences Citation Index (SSCI) −1965-present” as the citation index. The first retrieval formula was “Topic = health-literate healthcare organizations or HLHO (HLHO) or health literacy health care organizations (HLHCO) or health literate health care organization or Health Literate Organization or Health-Literate Hospitals and Healthcare Organizations or Health Literate Health Care or Health-literate healthcare or Health Literate Healthcare or health literate organizations or Organizational health literacy (OHL) or health promoting hospital (HPH) or hospital health literacy (HHL) or health literacy environment (HLE) or Health Literacy Environment Review or Health Literacy Environment of Hospitals and Health Centers (HLEHHC) or literacy-friendly healthcare facility or Literacy friendly healthcare settings or Organizational Health Literacy Responsiveness self-assessment tool (Org-HLR Tool) or Communication Climate Assessment Toolkit (C‐CAT) or Pharmacy Health Literacy Assessment Tool or Health Literacy-Sensitive Communication Scale (HL-COM) or Organizational Health Literacy Responsiveness (Org-HLR) self-assessment tool and process or Patient Education Materials Assessment Tool (PEMAT) or Patient Education Materials Assessment Tool. (PEMAT)” The second retrieval formula was “Topic=health literacy or health literate or Medical Literacy AND Topic = criteria or criterion or attribute or policy or policies or guideline or recommendation AND Topi = organization or organizational or healthcare center or health care services or primary care or patient-centered care or health facilities or Medical Institution or Medical Center or Healthcare Institution or Health Care Organizations or Health Care Centers”. The publication date ranged from 1965 to 2024 (all years). A total of 3425 original articles were retrieved on January 5, 2024. The document types were limited to articles, review articles, and proceedings papers, excluding letters, conference proceedings, editorial materials, conference abstracts, book chapters, and retracted or republished documents, and a total of 3297 articles were obtained. Two authors independently searched, checked, screened, and confirmed through the resource database of their units to ensure the accuracy of the literature data. 3297 articles were added to the list of marked results. The full records and cited references were exported to plain text file, including information such as authors, research institutions, titles, publication years, keywords, abstracts, journals, references, volumes, and page numbers. The format files of full records were converted to download_xxx.txt format using the format converter of CiteSpace 6.2.R7 software. The retrieved literature data was imported into CiteSpace for deduplication, a total of 3134 original documents were obtained as analysis data samples for this study.
Index Development
Stage I: CiteSpace Bibliometric Analysis
CiteSpace primarily utilizes mathematical and statistical methods to compare, summarize, abstract, and generalize citation and co-citation phenomena of analysis objects such as scientific journals, papers, and authors. It is a scientometric research method aimed at revealing quantitative characteristics and underlying patterns. The theoretical foundation of CiteSpace draws from Thomas Kuhn’s “The Structure of Scientific Revolutions”,14 Ronald Burt’s structural holes theory,15,16 Peter Pirolli’s information foraging theory,17 Kleinberg’s burst detection18 and structural variation theory.19,20 The core functions of CiteSpace include burst detection, intermediary centrality, and heterogeneous networks, which help identify research frontiers, mark specialties, promptly detect emerging trends and mutations, and provide robust support for exploring research advances, current hotspots, frontiers, and their corresponding knowledge bases in the field of science.21 This study utilized CiteSpace 6.2 R7 software tool to deeply explore the information of co-citation networks, co-word networks, and author co-citation. When interpreting the generated networks, high frequency nodes, clustered knowledge groups, betweenness centrality nodes, and basic legends were focused on to reveal the knowledge structure and dynamic changes in the field of science. Through micro-level Author Co-Authorship, meso-level Institution Co-Authorship, and macro-level Country Co-Authorship, Co-Authorship Analysis, Co-Occurrence Analysis, and Co-Citation Analysis were conducted. In addition, Excel software was utilized to plot some data, fully revealing the collaboration model and knowledge flow in the field of science.
Evaluation Indices
In the networks generated by CiteSpace, nodes and links have different meanings. Nodes represent the objects of statistical analysis, and the size of the circles reflects the frequency of occurrences of the nodes. The width of the circles is directly proportional to the number of occurrences in the corresponding time partition, and the colors of the circles represent the citation time. By observing the colors of the circles, the distribution of citation times can be judged. Additionally, the flow of knowledge between nodes can also be observed from the time (color), from cold to warm colors. In CiteSpace, nodes with high betweenness centrality are marked with a purple outer circle, the thickness of which indicates the value of betweenness centrality. The links between nodes represent co-occurrence (or co-citation) relationships, the thickness of the lines indicates the strength of co-occurrence, and the color of the links reflects the time of the first co-citation (or co-occurrence). The color change of network links can identify the newness or oldness of the research field. These definitions will be applied to all network map analyses.
Modularity is the evaluation index of network modularization. The higher value indicates better clustering. The value range of Q is from zero to one, and Q more than 0.3 means that the network community structure obtained is significant. Silhouette is a parameter used to evaluate the clustering result by measuring the homogeneity of the network. The closer the value of Silhouette is to the range from zero to one, the higher value of Silhouette is and the better homogeneity of the network is. When the value is 0.7, a high homogeneity of the network is reflected and the clustering result has high reliability. The clustering result can be considered reasonable when the value is above 0.5.
Stage II: Qualitative Analysis – Focus Group Interviews
Focus group interviews are a qualitative research method used to refine and optimize evaluation index systems.22 By assembling a group of individuals with similar backgrounds and knowledge in an equal and pressure-free environment, specific issues are collectively discussed to gather and analyze information. Key characteristics of focus group interview23 include “Interview as research”, “Collective exploration” and “Co-construction”. To supplement the findings from the literature analysis and preliminarily validate the scientific robustness of the index dimensions, this study organized a series of focus group interviews between January 14 and February 16, 2024. Participants were selected through purposeful sampling, with priority given to experts possessing practical experience, policy insight, and a background in health literacy research. The final panel consisted of six experts (five female, one male) aged 25 to 38, all affiliated with tertiary-level hospitals and representing a range of roles, including frontline clinical staff, nursing managers, and hospital administrators. The predominance of female participants reflects the central role of women in health education, nursing, and public health within the healthcare system, and also aligns with the focus group principle of prioritizing information saturation, as the female experts demonstrated greater domain experience and willingness to express insights.
To ensure scientific rigor and methodological consistency, the focus group design adhered to the core procedures of qualitative research. Drawing on the findings from CiteSpace-based bibliometric analysis and referencing internationally recognized health literacy evaluation tools—such as HLEHHC,2 the Ten Attributes of Health Literate Health Care Organizations,1 HLHO-10,10 the Health Literacy-Sensitive Communication Scale,11 and Org-HLR tool12 —the research team developed a structured discussion guide covering 14 primary indices and 53 initial secondary indices. Prior to the interviews, the experts received the consultation guide along with the preliminary draft of the HLHO evaluation indices to facilitate deep engagement with the framework and pinpoint areas for refinement. The focus group process included three rounds of interviews. The first round was conducted in-person and emphasized inspiration and divergent thinking. Based on expert feedback from this session, the research team revised and reorganized the 53 initial indices, ultimately expanding them into 14 primary indices and 120 refined secondary indices. The subsequent two rounds were conducted via online video conferencing and focused more on supplementation, elaboration, and synthesis. Discussions evolved from open-ended exploration to more targeted deliberation on index content and structural adjustments. Informed consent was obtained from all participants prior to each session, and all interviews were audio-recorded in full. Transcripts were independently prepared by two researchers and cross-validated for accuracy. Data analysis was conducted using thematic analysis, through which key themes were extracted from the transcripts, expert insights were categorized, and the index system was iteratively revised. The final framework consisted of 14 primary indices and 120 secondary indices, demonstrating a structured and contextually relevant evaluation tool tailored to HLHO development in China.
Quality Control
This study brought together six experts in the field of health literacy, who possess good professional knowledge and practical experience, are familiar with the latest policies and standards, and provide a solid guarantee for the credibility of the research. Secondly, the host and researchers have all received training to ensure the quality of the research. Thirdly, researchers recorded the entire meeting, using standardized interviews and records to ensure the objective and complete research materials. Fourthly, two researchers analyzed the data in real time to ensure the accuracy of the results. Finally, after multiple revisions, the indices were concise and accurate, unanimously approved by experts to ensure reliable and objective results.
Stage III: Index Development
Based on the literature analysis and expert interviews, this study integrated and expanded the original indices. The constructed index system covers dimensions such as organizational management, health education, provider-patient communication, digital services, and support for vulnerable groups, with a focus on local adaptability, operability, and equity. The selection and confirmation of indices followed the principle of combining theory with practice and prioritizing expert consensus. To ensure the comprehensiveness and scientific validity of the development of the index system and to avoid the issue of “overrepresentation of tertiary hospital samples” during the development process, this study conducted semi-structured interviews24,25 in primary healthcare institutions from April 8 to 14, 2025, based on literature analysis and preliminary indicator categorization. To ensure the representativeness of the sample, four experts were selected from three grassroots healthcare institutions, including clinical frontline medical staff and hospital management (three males and one female). The experts, aged between 31 and 45 years, possess extensive clinical practice experience and managerial perspectives, enabling them to provide a comprehensive reflection of the practical needs of primary healthcare institutions. The in-depth discussions centered on three core dimensions: (1) Optimization strategies for the health literacy-based healthcare institution evaluation indicators, focusing on the addition, removal, and rewording of indicators; (2) A systematic evaluation of the preliminary indicator set, including structural validity and content coverage; (3) Primary healthcare institutions’ views on health literacy-based healthcare institutions, including the feasibility and barriers of the indicators. The entire interview process was recorded and transcribed, with strict de-identification procedures implemented to protect the privacy of the experts. Thematic analysis26 was employed in the results section of the study to systematically categorize and organize the key points from the expert interviews, thereby extracting essential information and establishing a foundation for the subsequent Delphi method-based expert consultation.
Results
CiteSpace Bibliometric Analysis
To set the corresponding analysis parameters. The Time Slicing for the study started from January 1991 and ended in January 2024. Pruning for institutions was set to pathfinder, pruning sliced networks, and pruning the merged networks. Other parameters were set as shown in Table 1.
 |
Table 1 Node and Network Characteristics |
Analysis of the Present Situation
Analysis of the Number of Published Articles
The number of published articles is one of the important indices to measure the change of research heat in a certain field of science. By analyzing the number of published articles each year, the research trends, development status, and competitive landscape in the field will be understanded. This study makes a statistic on the annual distribution for number of published articles retrieved from 1991 to 2024 (Figure 1). Since 2013, the number of published articles has been increasing every year, with a total of 2626 published articles, accounting for 83.79% of the total. This indicates that HLHOs are becoming more active in the application of international papers. Three significant increases were in 2018, 2020, and 2022. In 2018, the annual number of published articles were 213, an increase of 17.70% from 2017. In 2020, the number of published articles were 303, an increase of 35.27% from 2019. In 2022, the number of published articles were 421 articles, an increase of 19.60% from 2021.
 |
Figure 1 Annual number of published papers (1991–2024). |
It is speculated that three significant growth spurts may be closely related to changes in the external environment. The sudden increase in global scholars’ attention to issues in a certain field often stems from challenges faced by the international community. For example, in 2018, natural disasters such as hurricanes, typhoons, and volcanic eruptions occurred frequently; In 2020, the world was shrouded in the shadow of the COVID-19 pandemic; By 2022, the Russia-Ukraine conflict broke out, the world experienced extreme high temperatures, and the pandemic entered final stages. These drastic changes in the external environment may have stimulated scholars to pay more attention to health literacy and conduct research in the field of it, thereby causing a continuous increase in the number of published papers in this field.
Research Co-Authorship Analysis
In the research co-authorship network map, the size of the nodes represents the number of published papers by authors, institutions, or countries/regions, and the connections between them reflect the co-authorship and their strengths. In the node types, author, institution, and country are used for research co-authorship analysis.
Author Co-Authorship Analysis
Co-Author identity is the connection of researchers working together on a specific topic. The corresponding analysis parameters are set as follows: “Author” is selected for Node types. Author Co-Authorship network map is drawn (Figure 2). In the research field of HLHO, the top 10 authors are Wolf, Michael S (14), Osborne, Richard H (7), Creta, Massimiliano (6), Arnold, Connie L (6), Califano, Gianluigi (6), Ansmann, Lena (6), Ruvolo, Claudia (6), Celentano, Giuseppe (6), Schillinger, Dean (6), and Davis, Terry C (5). Wolf, Michael S,27 a professor of medicine at Northwestern University, is the most prolific author, with a total of 14 publications. His research covers health literacy, self-management, medication safety, and aging, significantly improving healthcare quality. According to Price’s Law “[m](m=nmax/2)”, authors with a number of publications exceeding 7 are considered core authors in the field. This includes Professor Richard H. Osborne.28 As a distinguished professor in health sciences and a health literacy advisor for the World Health Organization on non-communicable diseases, Professor Osborne has made outstanding contributions to the development of health literacy tools, many of which are widely used globally.29–31 Although there is close co-authorship among Creta, Massimiliano, Califano, Gianluigi, Ruvolo, Claudia, and Celentano, Giuseppe, there is relatively less interdisciplinary and international cooperation among other scholars. These research achievements have not only promoted the development of the health literacy field but also provided direction for the future development of HLHO within our research group.
 |
Figure 2 Network Map of Author Co-Authorship. |
Institution Co-Authorship Analysis
Institution Co-Authorship Analysis reveals the characteristics, trends, and influence of co-authorship among institutions. The corresponding analysis parameters as follows: “Institution” is selected for Node types, and the Institution Co-authorship Network Map is drawn (Figure 3). From the map, it can be observed that the top 10 institutions, including University of California System (129), University of Sydney (109), Harvard University (105), University of London (95), Johns Hopkins University (71), University of Melbourne (69), University of Toronto (64), University of California San Francisco (63), Northwestern University (59), Monash University (58), are active in health literacy institutions and constitute global research centers. These institutions are mainly concentrated in universities, highlighting the core status of universities in this field of research. In addition, considering the importance of the institutions’ positions in the network, Columbia University (0.62), University of Texas System (0.55), University of California Los Angeles (0.44), Harvard Medical School (0.30), University of North Carolina (0.24), and US Department of Veterans Affairs (0.21) play important bridging roles in the co-authorship network, indicating their strong betweenness centrality.
 |
Figure 3 Network Map of Institution Co-Authorship. |
Country Co-Authorship Analysis
Country Co-Authorship Analysis explores the cooperative relationships among countries worldwide. By quantitatively analyzing index such as the number of cooperation, the number of countries involved, and the strength of cooperation, it reveals the core countries and hotspots of co-authorship in specific fields. The corresponding analysis parameters are set as follows: “Country” is selected for Node types, in terms of the output of the countries, the United States published 1241 articles (accounting for 39.60%), with the highest betweenness centrality of 0.38, indicating the prominent position and influence of the United States in the country co-authorship network. Other high-yielding countries in order are: Australia (513), England (314), Canada (237), Germany (153), People’s Republic of China (138), Netherlands (124), India (112), Italy (69), Sweden (67). In addition, Kleinberg’s burst detection algorithm was employed to analyze the abrupt changes in node frequency in the data of country co-authorship papers, finding emerging areas of cooperation. The results showed that China’s attention to HLHO significantly increased in 2022 and collaboration between China and many countries has been abruptly growing, marking China’s gradual emergence as an important participant and contributor in this field (Figure 4).
 |
Figure 4 Network Map of Country Co-Authorship. |
Research Topics and Evolution
In the co-citation map, the size of the nodes represents the number of citations. Co-citation Analysis includes Journal Co-Citation, Reference Co-Citation, and Author Co-Citation. Co-citation analysis reveals the connection among discipline trends, core authors and journal influences.
Author Co-Citation Analysis
Author co-citation occurs when two or more authors are cited simultaneously by a third paper. This analysis reveals important authors in a discipline and their collaborative networks, reflecting the strength and status of the field. The analysis parameters are set as follows: the node type is selected as “Cited Author.” The World Health Organization (WHO) is the most frequently cited organization, with 673 citations. As a crucial promoter of global public health, the WHO has played a key role in defining and advancing health literacy.32 Following closely is Nutbeam D, with 289 citations, widely recognized for his in-depth understanding and research on health literacy, particularly in the area of health self-efficacy33,34 (Figure 5). Their research spans multiple aspects of health literacy, including intervention models, research challenges, health literacy among different populations, internet information, and digital health information. Their work provides new perspectives and insights for research in the related fields.
 |
Figure 5 Author Co-Citation Knowledge Map. |
Journal Co-Citation Analysis
When two or more journals are simultaneously cited by a third paper, there is a co-citation relationship between them. The corresponding analysis parameters are set as follows: “Cited Journal” is selected for Node types. PATIENT EDUC COUNS is the most frequently co-cited journal, followed by JAMA-J AM MED ASSOC and J GEN INTERN MED. PATIENT EDUC COUNS has the strongest betweenness centrality, indicating its significant influence on other journals (Figure 6). Among the top 11 journals, those from the United States are the most prevalent. The research areas covered by these journals include social sciences, biomedical sciences, medicine, public health, environmental health, occupational health, healthcare science and services, and medical informatics. This demonstrates the interdisciplinary nature of research in this field (Table 2).
 |
Table 2 Organizations with the Largest Number of the Literature |
 |
Figure 6 Journal Co-Citation Knowledge Map. |
Reference Co-Citation Analysis
Reference Co-Citation Analysis refers to the co-citation relationship formed when two references are cited simultaneously by a third citing reference. The corresponding analysis parameters are set as follows: “Cite reference” is selected for Node type. Tricco AC, 2018 was cited 59 times, Sorensen K, 2012 was co-cited 43 times, both showing high influence. The article Kowalski C, 2015 has the strongest betweenness centrality and had a significant influence on the academic network (Figure 7). The frequently cited references mainly involve methodological interpretations of systematic reviews, chronic disease management, the importance of health literacy, methods of information assessment, internet information quality, and the social determinants of health literacy on clinical quality and safety.
 |
Figure 7 Reference Co-Citation Knowledge Map. |
By employing Kleinberg’s Burst Detection Algorithm to identify emergent literature that has received a sudden surge in citations within a specific time frame, intense academic attention has been gained (Figure 8). Tricco AC, 2018 has a burst frequency of 22.54, indicating its significant influence in the health sciences, particularly regarding best practices and reporting standards for systematic reviews and meta-analyses.35 Paakkari L, 2020 has a burst frequency of 7.61. This study emphasized the importance of health literacy in addressing public health challenges, such as COVID-19, and suggested that health literacy education and support can improve treatment outcomes and quality of life.36 Nutbeam D, 2021 has a burst frequency of 7.37, exploring interventions to improve health literacy in clinical and community populations.37 Hong, Quan Nha, 2018 has a burst frequency of 6.8, underscoring the importance of effective assessment tools for mixed methods research. This study proved the importance of effective evaluation tools for mixed methods research, which helped medical organizations develop targeted interventions to improve patient health literacy and self-management abilities.38
 |
Figure 8 Knowledge Map of Reference Co-Citation Burst Detection Algorithm. |
Through the analysis of these four articles, this study speculated on the following construction paths for HLHO. The first step is to deeply study previous reviews to lay the foundation for the development of HLHO. The second step is to focus on the development and innovation of assessment tools to ensure the guarantee of the transformation of HLHO. The third step is to pay attention to health literacy and social factors, utilizing multi-intervention to improve patient health and service quality, and achieving transformation.
Co-Occurrence Analysis
In the co-occurrence map of paper topics, keywords, and scientific fields, the size of the nodes reflects the frequency of words, and the connections reveal the co-occurrence relationships and their strength. The trend of word frequency and centrality has been comprehensively considered to gain insights into scientific hotspots and development trends.
Keywords Co-Occurrence Analysis
Keywords Co-Occurrence Analysis is a co-occurrence analysis of keywords provided by authors and databases within the dataset. Keywords represent the core essence of articles.39 By refining and generalizing keywords, the themes and focal points of articles can be one can accurately grasped, thereby enhancing readability and search efficiency. The analysis parameters are set as follows: “Keyword” is selected for Node types, and keywords are cleaned and merged (Figure 9). High-frequency keywords included health literacy, nursing, reading and writing ability, effect, primary care, knowledge, health, influence, education, communication, with frequency of 792, 539, 346, 265, 227, 218, 213, 197, 191 and 180, respectively. As the research hotspots in this field, high-centrality keywords included service, health, public health, barrier, elderly, prevalence, community, health information, patient education, readability, with centrality of 0.11, 0.11, 0.10, 0.09, 0.09, 0.08, 0.08, 0.08, 0.07 and 0.07, respectively.
 |
Figure 9 Keywords Co-Occurrence Analysis Map. |
Focusing on high-frequency keywords, it reveals that the core of the medical service system is health literacy, and key factors include education, knowledge, and communication. The health needs of the elderly are special, and the role of nursing is significant. Reading and writing ability may affect a patient’s understanding of medical information. HLHO and public health jointly focus on the health of the population. In the context of primary care as an extension of services, promoting health literacy education at the community level can improve the health level of residents.
Keyword Clustering Analysis
Keyword clustering analysis is a commonly used method in research fields for identifying and extracting research hotspots and trends. Based on co-occurrence analysis parameters (threshold set as Top N = 50, time slicing: 2 years, pruning options including Pathfinder, pruning sliced networks, and pruning the merged networks), the LLR algorithm was employed, and keywords were selected to label the clusters. A total of 19 significant clusters were successfully identified (# represents a cluster) (Figure 10). Each cluster label was automatically generated by the system based on keyword calculations. Manual semantic review was conducted to ensure consistency between the cluster labels and the content. The clustering module value (Modularity Q = 0.7829) and the average silhouette value of the clusters (Mean Silhouette S = 0.9234) both indicate that the clustering results have high credibility and significance.
 |
Figure 10 Keyword Clustering Analysis Knowledge Map. |
Through in-depth analysis of keywords under each cluster label, it found that the keyword cluster labels were patient education, readability, primary care, health literacy, socioeconomic status, and education, jointly reflecting the basic elements of health HLHO (#0, #1, #2, #3, #4, #16). Patient education plays a key role in promoting the acquisition of disease knowledge and the improvement of self-care skills; readability ensures that medical information is easy to understand; primary care focuses on prevention and early intervention, patients are required to have health literacy; socioeconomic status affects the access to health information and services; and education is an important way to improve public health literacy and the quality of medical services. These elements together constitute the core of health literacy, providing necessary support to individuals and communities.
Represented by the keywords including prevalence, mental health, and mortality (cluster #5, #6, #9), the cluster labels reveal the health status and outcomes of individuals and groups, which are core indices for assessing the effectiveness of HLHO. Mental health affects treatment compliance and reduces the risk of disease; mortality directly reflects the effectiveness of treatment; and high prevalence rates suggest the need for increased prevention and treatment of specific diseases. These indices are crucial for improving the quality of medical services. The core of health management is characterized by keywords such as motivation, management, patient compliance, risk, risk assessment data, and health policy (cluster #11, #12, #13, #14, #15, #18). Motivation drives health behaviors; management ensures efficient services; patient compliance affects treatment outcomes; risk assessment data helps with precise interventions; and health policy guides service direction. These elements collectively enhance public health literacy and the level of healthcare. Services, qualitative research, public health, and health promotion hospitals are the keywords that collectively drive the development of HLHO (cluster #7, #8, #10, #17). Services are the core of medical organizations; and high-quality services are their basic responsibility. The modern origin of public health comes from a deep understanding of how social and environmental conditions affect health. Qualitative research can deeply understand patient needs and optimize services. Public health’s core concept is focused on the overall health of community populations; and health promotion hospitals enhance public health through education and prevention, while also supporting high-quality services and innovative research.
Through in-depth analysis of these keywords, combined with the results of co-occurrence and clustering analysis, jointly providing necessary health services and support to individuals and communities involves several key elements, including health literacy, health, patient education, public health, primary care, education, services, management, and prevalence. These are the research hotspots and cutting-edge research in the field, emphasizing their core role in improving public health literacy and the level of healthcare. At the same time, HLHO should focus on the joint education of patients and medical staff, especially caring for the elderly and vulnerable groups. By conducting in-depth research to understand their health needs, optimizing operational models and services, health literacy and public health will be promoted.
Kleinberg’s Burst Detection Analysis
Emergent word analysis contains Kleinberg’s burst detection, which reveals that keywords that change rapidly or increase sharply in quantity in a short period of time are research hotspots and cutting-edge frontiers at different time periods. The corresponding analysis parameters are set as follows: the minimum duration is set to 1 year, obtaining 86 keywords with high intensity, and the top 50 keywords are selected. The strength value of all keywords is greater than 4. Maintaining their popularity, emerging keywords include health information, perception, elderly, technology, digital health, scope review, health policy, female, health promotion, qualitative research, internet, socioeconomic status, and determinants of a healthy society, with strength value as 10.91, 7.25, 9.22, 5.21, 10.12, 9.64, 9.03, 6.99, 6.75, 7.05, 5.91, 5.71, 5.33, respectively (Figure 11).
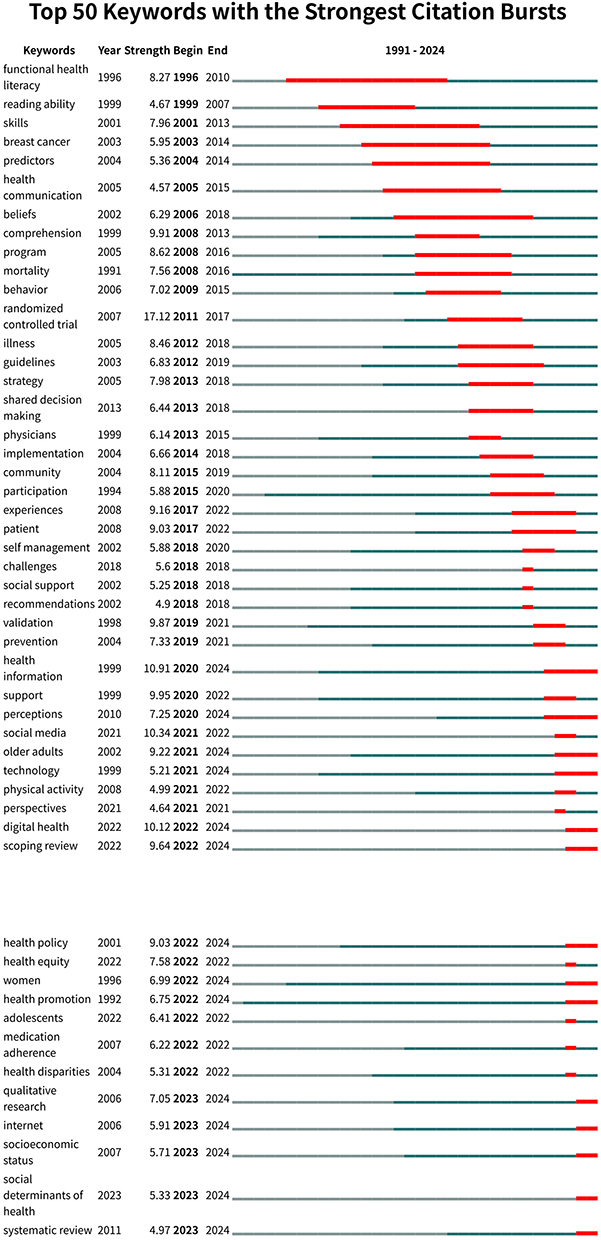 |
Figure 11 Knowledge Map of Kleinberg’s Burst Detection for Keywords. |
In recent years, the attention to health information and digital health care has significantly increased, with intensity values of 10.91 and 10.12, respectively, indicating that both are undergoing profound changes in the context of digital health care. Digital health care not only brings more efficient and precise services to medical organizations but also greatly promotes the transmission and popularization of health information, thereby enhancing the health literacy of patients. In HLHO, the health needs of specific populations such as the elderly and women are receiving special attention. As their physical functions decline and physiological characteristics change, they face more health challenges. Medical organizations need to provide personalized services to meet their needs. Therefore, the following speculations have been made. Firstly, there is close relationship among health information and perception, health policy, and health promotion, jointly affecting health concepts, behaviors, and outcomes. Secondly, key influencing factors include digital health care, technology, and socioeconomic status. Thirdly, the formulation of effective policies and strategies can enhance the role of HLHO, improve patients’ health literacy and self-management ability, and provide better protection for health.
Qualitative Analysis – Focus Group Interviews
In this qualitative analysis of the focus group interviews, experts’ opinions and suggestions were not provided in a one-to-one correspondence with each primary index, but were discussed around several highly related and overlapping themes in practical work. To more accurately reflect the key points and practical concerns of the expert discussions, this study categorized and organized the interview data using thematic analysis,26 as shown in Table 3.
 |
Table 3 Theme Classification |
Organization Management and Service Processes
Experts generally recognized the efficiency of organizational management and service processes in medical organizations. They believed that a sound management system and collaboration among departments ensured the smooth operation of medical services. However, experts also pointed out that the organizational management part of the initial 53 indices was not comprehensive. Expert 1 emphasized that organizational management should be carried out from top to bottom, including policy formulation, establishment of management departments, personnel selection, and clear goals and implementation plans. Expert 4 highlighted the importance of self-assessment and continuous improvement. Expert 2 suggested adding indices related to environmental atmosphere, reward and punishment systems, and financial and human resource support. At the same time, experts also emphasized the convenience of medical services for patients. Expert 3 proposed adding feedback mechanisms for employees and patients to better understand the effects of services. Expert 5 suggested publishing the visit process flowchart to improve the transparency of patient medical treatment. Expert 2 also believed that the rationality of the visit process should be emphasized, not just the simplification of the process. Expert 4 emphasized the importance of online platforms to enhance the patient’s medical experience.
Health Education and Public Welfare Services
Health education and public welfare services are important parts of HLHO. Experts affirmed their effectiveness and also made suggestions for improvement. Expert 1 emphasized the scientific rigor and accuracy of health education materials. Expert 3 pointed out that the materials should meet the needs of doctors and patients, ensuring accurate information dissemination. Expert 2 suggested using internet information platforms to enhance the dissemination effect of health education materials, especially for promotion in the community. Expert 6 suggested that hospitals cooperate with media and academic institutions to promote the dissemination of health information in society.
Doctor-Patient Communication and Patient Support
Doctor-patient communication is an important part of promoting health literacy. HLHO should pay attention to and create good communication conditions. According to the interview results, experts suggest strengthening communication skills training, improving service awareness, and enhancing communication feedback. Expert 1 proposed that training should cover all medical staff comprehensively, develop personalized strategies based on needs, and regularly collect feedback to optimize the communication process. Expert 2 suggested that doctor-patient communication should be bidirectional feedback, medical staff should listen to patients, encourage questions and patients’ participation in decision-making. Expert 3 emphasized the importance of communication skills and proposed that different strategies should be adopted for different groups of people, and knowledge should be transmitted in the most easily accepted way by patients. Expert 6 pointed out that doctors should avoid professional terminology, ensure that language is plain and easy to understand, moderate speech speed, and clear pronunciation.
Special Patient Group Services
Special patient groups are closely linked to HLHO, and their high dependence is due to their special needs. However, experts also suggested modifying some indices. Expert 1 proposed that medical staff should be able to identify low health literacy patients, avoiding discriminating against them and patiently helping them. Expert 2 suggested that medical staff should increase the use of written materials, videos, and other tools to help patients understand, and allocate more treatment time for them. Expert 3 proposed that medical staff should improve their communication skills, teach patients to manage their health, and use plain language. Expert 6 emphasized the need for doctors to fully explain the patient’s condition and health literacy when handing over, to ensure the continuity and safety of diagnosis and treatment.
Self-Health Management and Health Promotion
Hospitals provide comprehensive support to patients through measures such as establishing communication groups and developing follow-up plans. This is not only crucial during treatment but also indispensable in recovery and long-term management. Experts unanimously agree that medical staff have an obligation to guide patients in scientifically managing themselves during and after treatment, including aspects such as medication, exercise, and nutrition. In addition, Expert 1 particularly emphasized the importance of follow-up plans, considering them a key link in checking the effectiveness of treatment and adjusting treatment strategies. Expert 3 suggests that for patients with chronic diseases, medical staff should require them to record changes in their condition, such as blood sugar and blood pressure, as a basis for diagnosis and treatment.
During the three rounds of focus group interviews, experts provided detailed practical insights and suggestions for index revision across core dimensions, including organizational management, health education, provider–patient communication, services for special populations, and self-health management. Experts generally agreed that organizational management should integrate policies, institutional structures, and personnel levels to enhance coordination and continuous quality improvement. Service processes, they emphasized, should be patient-centered, with a focus on process transparency, feedback mechanisms, and digital support. At the same time, health education should balance scientific accuracy with ease of communication, promoting continuous improvement in staff training, communication channels, and support for vulnerable populations. In terms of patient engagement, feedback mechanisms, information accessibility, and continuity of care, indices were expected to be designed with greater operability and fairness.
In summary, based on three rounds of expert consultation, the HLHO index framework was comprehensively optimized. The research team ultimately refined 14 primary indices and added 67 new secondary indices. Following iterative revisions and screening, 28 existing secondary indices were retained, and 25 were modified, resulting in a finalized HLHO index system consisting of 14 primary and 120 secondary indices (Table 4). A comparative analysis with leading international health literacy assessment tools1,2,10–12 revealed several distinguishing features: (1) broader coverage—new dimensions such as “online healthcare service platforms”, “community welfare services”, and “continuity of care” were added, better aligning with the development of digital health and primary care systems in China; (2) emphasis on patient co-creation—multiple indices incorporated mechanisms for “joint design, evaluation, and improvement by staff and patients”, reflecting the principle of patient empowerment; (3) enhanced focus on equity and vulnerable populations—a specific cluster of indices was developed for “patients with low health literacy”, reinforcing inclusiveness and human-centered care; and (4) integration of policy orientation and international standards—the index system was aligned with key national initiatives such as the Healthy China Action and the National Health Literacy Promotion Campaign, establishing an operational framework with distinct Chinese characteristics.
 |
Table 4 HLHO Index System |
Phase III: Construction of the Index System—Semi-Structured Interviews
Optimization of the Index System
Most experts agreed that the HLHO index system developed in this study was comprehensive in content and reasonable in structure, particularly aligning well with current practice in areas such as health education, provider–patient communication, and information accessibility. For example, the participating primary healthcare institutions had already employed measures such as illustrated educational materials, optimized font usage, and streamlined clinical workflows to improve patient comprehension and engagement. Some community health centers had also collaborated with local authorities and specialist physicians to conduct health lectures, free clinics, and personalized health education services, demonstrating strong local adaptability. Meanwhile, experts emphasized the need for further strengthening of health awareness education among patients and for establishing supportive mechanisms at the societal level.
Feasibility in Primary Healthcare Institutions
All four experts indicated that although most indices were grounded in existing practices, several challenges remained in implementing the system in primary care settings. The main difficulties included: (1) delayed development of online services and continuous improvement mechanisms, limited by staffing and technological resources at the grassroots level, requiring gradual adaptation based on local conditions; (2) complex communication processes related to health insurance policies and pharmaceutical services, where information asymmetry and procurement restrictions hindered the practical implementation of certain service indices; and (3) incomplete service function structures—for instance, some community hospitals lacked inpatient departments, leading to gaps in the full service chain necessary for implementing certain indices, thus requiring differentiated adjustment based on institutional levels and functional positioning. Despite these challenges, primary care experts generally endorsed the conceptual design and structural rationality of the index system, recognizing its strong potential for promotion and adaptation.
In summary, the interview findings from primary healthcare institutions were largely consistent with the results of the focus group discussions, supporting the rationality and promotability of the HLHO index system. This study highlights that the effectiveness of health literacy initiatives depends not only on the scientific design of the indices but also on external factors such as healthcare resource allocation, organizational structure, and policy support. Therefore, during the promotion and application of the HLHO index system, it is essential to dynamically adjust and stratify implementation based on the functional positioning and actual conditions of different healthcare institutions. Moreover, primary healthcare institutions exhibit unique contextual needs and systemic shortcomings in promoting health literacy. Future implementation efforts should simultaneously strengthen capacity-building mechanisms, optimize policy support systems, and enhance intersectoral collaboration to further improve the adaptability and effectiveness of the index system.
Discussions
By integrating quantitative analysis using CiteSpace and qualitative insights from focus group interviews, this study constructed an HLHO index system that reflects China’s national characteristics while incorporating international experience. Observing from dimensions such as Author Co-Authorship, Institution Co-Authorship, and Country Co-Authorship, it was found that scholars and institutions in the United States have conducted extensive and in-depth research in this field, committed to its development for a long time, and have produced significant influence. At the same time, this study also observed that different regions have varying degrees of emphasis on improving public health literacy, as well as diverse assessment tools and intervention methods, all of which were closely related to the unique culture and medical organization systems of each country. The outbreak of COVID-19 has further highlighted the urgency of improving individual and group health literacy, highlighting the need for countries to take practical and effective measures to meet this challenge. Therefore, research in this field should actively promote deepened international cooperation and exchange, learn from the successful experiences of different countries, and jointly promote the transformation to HLHO. Research on HLHO involved multiple disciplines such as social sciences, biomedicine, interdisciplinary medicine, comprehensive and internal medicine, public health, environmental health and occupational health, health care science and services, medical informatics, and more. Current research mainly focuses on the medical discipline, with the core objective being to optimize medical institution services by improving the public’s health literacy level, thereby meeting the growing health needs of patients. In this process, interdisciplinary cooperation, information technology application, and policy system perfection play critical roles, collectively promoting breakthrough progress in health literacy services of healthcare organizations.
The construction of health-literate healthcare organizations is not a unidimensional optimization, but rather a profound transformation involving organizational culture, management mechanisms, service processes, and technological approaches. This study found that countries such as the United States have developed relatively mature pathways in areas including policy guidance, organizational leadership, and patient empowerment. In contrast, within the Chinese healthcare system, an organizational mechanism model characterized by “leadership-driven initiatives and institutional support” has demonstrated strong local adaptability. Expert interviews further confirmed that leadership commitment is the primary condition for advancing health literacy initiatives. It not only determines the level of resource investment and institutional development but also serves as the foundation for cultivating a patient-centered cultural environment. Back in 2012, the Institute of Medicine in the United States listed “management emphasis” as the primary characteristic of HLHO.1 Additionally, numerous studies have emphasized the central role of leadership in the organizational health literacy of medical centers.40,41 Borkowski’s perspective further confirmed that leaders play an indispensable role in guiding employees to adapt to change, pursue goals, and motivate actions. The findings of this study were highly consistent with the perspectives outlined above, further corroborating these conclusions, and underscoring that this level of organizational support has become a key element in driving health literacy transformation.6 Therefore, leaders of medical centers should actively create an environment that encourages employees to freely and comfortably share their insights and perspectives on organizational health literacy.42 Health literacy was incorporated as a performance index into hospitals’ medium-term and long-term development strategies. At the same time, health literacy–friendly policies and service standards were established, driving implementation through a dual approach of institutional development and cultural cultivation.
In the construction of health-literate healthcare organizations, communication and education serve as critical “interfaces” driving transformation, directly influencing the efficiency of health information transmission and the degree of patient engagement in decision-making. This study focused on dimensions such as provider–patient communication skills, the readability of health materials, diversified communication pathways, and self-health management. CiteSpace keyword analysis further revealed the frequent occurrence of terms such as readability, communication, education, and health promotion, indicating that this theme is not only a research hotspot but also a critical focus for institutional reform. In medical practice, the negative impact of poor communication on patient care and outcomes is quite common.1 On the other hand, numerous studies have confirmed that when clinical doctors communicate with patients, they should avoid presupposing the patient’s understanding, especially when dealing with complex information such as health plans and medical bills (like copayments and deductibles).1 It is crucial to use clear, layman’s terms to ensure that patients can fully understand.43,44 This patient-centered approach to communication has gradually become a priority task at all levels of healthcare organizations. Currently, an increasing number of healthcare institutions have recognized that health education, as a critical means of enhancing patient health literacy, must emphasize both precision and interactivity. The “National Action Plan to Improve Health Literacy” released by the United States in 2010 clearly pointed out that training all staff and encouraging community members to participate in organizational assessment and health literacy improvement work are effective strategies to improve health literacy.45 The study demonstrated that effective educational interventions can lead to significant improvements in patients’ health attitudes and behaviors.46 Studies found that patients who actively participate in self-health management are more likely to make scientific and reasonable health decisions and take effective measures to properly manage their chronic health conditions.42 In this process, the popularization of health knowledge is regarded as the core approach to enhancing patient health literacy.47 Secondly, the diversity of health materials and the innovation of forms are crucial for strengthening patients’ understanding and acceptance of health information, which can meet the needs of different patients.48,49 The interview results further indicated that healthcare professionals generally endorsed interactive education and two-way communication, particularly in serving vulnerable populations. Within healthcare organizations, patient engagement is one of the core components of the conceptual framework for organizational health literacy.50 The establishment of clear and effective communication has been recognized as a paramount objective.1 This has also become a key principle in the service design of healthcare institutions. Accordingly, healthcare organizations need to provide more detailed and personalized services, such as using visual aids (eg charts and images) to intuitively present information.37,43 Meanwhile, combining written information with oral communication and providing alternative written materials (such as audio-visual materials) and educational services to ensure that every patient can easily access information.1 Meanwhile, it is recommended to strengthen training in doctor-patient communication for all staff, optimize communication processes, and monitor progress to promote public health behaviors.1,51
In the process of constructing health-literate healthcare organizations, the introduction of digital technologies has been reshaping the boundaries and practices of health literacy services. With the popularity of digital health services, the consultation process has become more convenient, greatly promoting the development of personal health management.52 Digital services such as online appointment scheduling and telemedicine consultations have not only shortened patient wait times but also optimized the allocation of healthcare resources. However, the benefits brought by digitalization are not equally accessible to all groups. Keyword burst analysis revealed the frequent appearance of terms such as digital healthcare, older adults, and low health literacy, suggesting the presence of potential information gaps and equity challenges during the digital transformation process. In particular, populations with low health literacy may encounter significant barriers in navigating digital tools, understanding information, or even completing basic healthcare procedures.53 In response to these risks, this study specifically incorporated dimensions such as online healthcare service platforms and support for patients with low health literacy, reflecting a proactive approach to mitigating the potential widening of information disparities in the context of digital healthcare transformation. It emphasizes an adaptability-oriented digital health literacy concept, highlighting the need to consider population characteristics and usage barriers to ensure equitable benefits for all groups. Currently, multiple studies have confirmed that through optimizing consultation processes, providing convenient health information, services, and navigation assistance, and utilizing online medical service platforms, healthcare organizations can break through time and space limitations, providing patients with more convenient and efficient medical services.54–56 Therefore, it is recommended that healthcare institutions strengthen service processes with an adaptability-oriented approach, placing greater emphasis on improving the quality of navigation and guidance services, particularly for older adults and individuals with low health literacy, to ensure equitable service experiences.
Based on key findings in organizational development, communication, and digital services, healthcare institutions should translate the HLHO index system into actionable plans. To support this, the following implementation pathway is proposed to guide the systematic advancement of HLHO initiatives: (1) Organizational Mobilization: Integrate health literacy development into hospital priorities, with dedicated departments and budget support; (2) Baseline Assessment: Evaluate the current status using the HLHO index system to identify weaknesses and improvement areas; (3) Capacity Building: Address identified gaps through targeted training and process optimization; (4) Goal Setting: Establish phased objectives and develop operational guidelines; (5) Continuous Improvement: Build monitoring and feedback mechanisms to enable dynamic adjustments and ongoing enhancement (Table 5).
 |
Table 5 Recommended Implementation Pathway for the HLHO Index System in Healthcare Institutions |
Limitations
This study integrated CiteSpace visualization analysis and focus group interviews, combining international research hotspots with Chinese expert insights to innovatively develop an HLHO index system, demonstrating strong innovation and persuasiveness. However, the construction process may be influenced by the research team’s subjective cognition, data source limitations, and the inherent constraints of CiteSpace technology, potentially introducing bias. Additionally, qualitative methods face challenges such as interpretative openness and limited replicability, requiring further quantitative validation. Preliminary research was conducted only in a few healthcare institutions, without broader multi-center studies, thus the indices’ measurability and generalizability need further verification. To address this, the index system was translated into a scale and a survey was conducted across eight Chinese cities (Beijing, Shanghai, Guangzhou, Suzhou, Chengdu, Wuhan, Nanjing, and Xuzhou), preliminarily confirming its reliability and validity. Moreover, during the expert interviews, although purposive sampling was used to cover both managers and frontline personnel from tertiary hospitals, the sample size was limited, and the majority of experts were female. The geographical and positional distribution of the interviewed experts was relatively concentrated, posing risks of limited representativeness and expert selection bias. Furthermore, during the collection of health literacy-related information and the implementation of indicator monitoring, issues concerning patient privacy protection may arise, and healthcare institutions should strictly comply with information security and ethical review requirements.
Conclusions
This study preliminarily constructed an index system for HLHO that aligns with both international standards and China’s national context, integrating quantitative analysis from CiteSpace and qualitative insights from focus group discussions. The system includes 14 primary indices and 120 secondary indices, covering key dimensions such as organizational leadership, communication and education, patient engagement, self-health management, and digital adaptation. It provides a practical tool for healthcare institutions to conduct self-assessments, drive quality improvement, and empower patients. It also offers a structured pathway for hospital managers and policymakers to prioritize health literacy initiatives and promote the transformation toward patient-centered care models. The research team plans to further refine the index structure through the Delphi method in February 2024 and has completed a multicenter pilot study across eight cities in China (Beijing, Shanghai, Guangzhou, Suzhou, Chengdu, Wuhan, Nanjing, and Xuzhou) in March 2024, which preliminarily validated the reliability and validity of the index system. Continuous optimization efforts are underway to enhance its adaptability and applicability across different types of healthcare institutions.
Data Sharing Statement
Due to privacy restrictions, the data from this study are not publicly available. However, they can be obtained upon request from the corresponding author.
Ethical Approval and Consent to Participate
The study was approved by the ethics committee of Changzhou Third People’s Hospital (02A-A2023030). Informed consent was obtained from all participants prior to the study and written informed consent was signed, in accordance with the principles of the Helsinki Declaration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by Open Research Fund Program of Changzhou Institute for Advanced Study of Public Health, Nanjing Medical University [CPHS202303], and the 2024 Medical Quality (Evidence-Based) Management Research Project of the National Institute of Hospital Administration, National Health Commission of the People’s Republic of China [YLZLXZ24G031], and the Hospital Management Innovation Research Project of Jiangsu Hospital Association in 2023 [JSYGY-3-2023-247], and the Research Project on Policy of Traditional Chinese Medicine for Deepening Reform of Healthcare System in 2024 of the Monitoring and Statistical Research Center of the National Administration of Traditional Chinese Medicine [YGZXKT2024124], and the 2024 Hospital-level Research Project of Changzhou Third People’s Hospital [SY202433], and the Science and Technology Major Project of Changzhou Municipal Health Commission [ZD202323], and the National Natural Science Foundation of China [82471739].
Disclosure
Shenyu Zhao and Yang Chen are co-first authors for this study. The authors report no conflicts of interest in this work.
References
1. Brach C, Keller D, Hernandez LM, et al. Ten attributes of health literate health care organizations. NAM Perspectives. 2012.
2. Rudd RE, Anderson JE. The health literacy environment of hospitals and health centers. 2006.
3. Lubasch JS, Voigt-Barbarowicz M, Ernstmann N, Kowalski C, Brütt AL, Ansmann L. Organizational health literacy in a hospital—insights on the patients’ perspective. Int J Environ Res Public Health. 2021;18(23):12646. doi:10.3390/ijerph182312646
4. Hayran O, Özer O. Organizational health literacy as a determinant of patient satisfaction. Public Health. 2018;163:20–26. doi:10.1016/j.puhe.2018.06.011
5. Hernandez L. How can health care organizations become more health literate.
6. Adsul P, Wray R, Gautam K, Jupka K, Weaver N, Wilson K. Becoming a health literate organization: formative research results from healthcare organizations providing care for undeserved communities. Health Serv Manag Res. 2017;30(4):188–196. doi:10.1177/0951484817727130
7. Sipos D, Goyal R, Zapata T. Addressing burnout in the healthcare workforce: current realities and mitigation strategies. Lancet Reg Health Eur. 2024;42:100961. doi:10.1016/j.lanepe.2024.100961
8. U.S. Department of Health and Human Services. Health literacy in healthy people 2030; 2020. Available from: https://health.gov/healthypeople/priority-areas/health-literacy-healthy-people-2030.
9. The Central People’s Government of the People’s Republic of China. Notice on launching a three-year campaign to improve Health literacy for all (2024–2027); 2024. Available from: https://www.gov.cn/zhengce/zhengceku/202406/content_6955867.htm.
10. Kowalski C, Lee S-YD, Schmidt A, et al. The health literate health care organization 10 item questionnaire (HLHO-10): development and validation. BMC Health Services Research. 2015;15:1–9. doi:10.1186/s12913-015-0707-5
11. Ernstmann N, Halbach S, Kowalski C, Pfaff H, Ansmann L. Measuring attributes of health literate health care organizations from the patients’ perspective: development and validation of a questionnaire to assess health literacy-sensitive communication (HL-COM). Z Evid Fortbild Qual Gesundhwes. 2017;121:58–63. doi:10.1016/j.zefq.2016.12.008
12. Trezona A, Dodson S, Osborne RH. Development of the Organisational Health Literacy Responsiveness (Org-HLR) self-assessment tool and process. BMC Health Serv Res. 2018;18(1):694. doi:10.1186/s12913-018-3499-6
13. Tong Y, Wu Y, Han Z, et al. Development and validation of the health literacy environment scale for Chinese hospitals from patients’ perspective. Front Public Health. 2023;11:1130628. doi:10.3389/fpubh.2023.1130628
14. Kuhn T. The nature of scientific revolutions. Chicago: University of Chicago; 1970:197.
15. Burt RS. Structural Holes: The Social Structure of Competition. Harvard university press; 1992.
16. Burt RS. Structural holes and good ideas. Am J Sociol. 2004;110(2):349–399. doi:10.1086/421787
17. Pirolli P, Card S. Information foraging in information access environments.
18. Kleinberg J. Bursty and hierarchical structure in streams.
19. Chen C. Predictive effects of structural variation on citation counts. Journal of the American Society for Information Science and Technology. 2012;63(3):431–449. doi:10.1002/asi.21694
20. Chen C. The Fitness of Information: Quantitative Assessments of Critical Evidence. John Wiley & Sons; 2014.
21. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
22. Rabiee F. Focus-group interview and data analysis. Proceedings of the Nutrition Society. 2004;63(4):655–660. doi:10.1079/PNS2004399
23. Powell RA, Single HM. Focus groups. Int J Qual Health Care. 1996;8(5):499–504. doi:10.1093/intqhc/8.5.499
24. Parker LM, Rychetnik L, Carter S. Framing overdiagnosis in breast screening: a qualitative study with Australian experts. BMC Cancer. 2015;15(1):606. doi:10.1186/s12885-015-1603-4
25. Whiting LS. Semi-structured interviews: guidance for novice researchers. Nursing Standard (Royal College of Nursing. 2008;22(23):35–40. doi:10.7748/ns2008.02.22.23.35.c6420
26. Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE Guide No. 131. Med Teach. 2020;42(8):846–854. doi:10.1080/0142159x.2020.1755030
27. Wolf, MS Author profile [Internet]; 2020. Available from: https://scholar.google.com/citations?user=L_hV3AsAAAAJ&hl=zh-CN&oi=sra.
28. Osborne, RH Researcher profile [Internet]; 2021. Available from: https://www.swinburne.edu.au/research/our-research/access-our-research/find-a-researcher-or-supervisor/researcher-profile/?id=rosborne.
29. Sørensen K, Van den Broucke S, Pelikan JM, et al. Measuring health literacy in populations: illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health. 2013;13(1):948. doi:10.1186/1471-2458-13-948
30. Osborne RH, Batterham RW, Elsworth GR, Hawkins M, Buchbinder R. The grounded psychometric development and initial validation of the Health Literacy Questionnaire (HLQ). BMC Public Health. 2013;13(1):658. doi:10.1186/1471-2458-13-658
31. Busija L, Pausenberger E, Haines TP, Haymes S, Buchbinder R, Osborne RH. Adult measures of general health and health-related quality of life: medical Outcomes Study Short Form 36-Item (SF-36) and Short Form 12-Item (SF-12) Health Surveys, Nottingham Health Profile (NHP), Sickness Impact Profile (SIP), Medical Outcomes Study Short Form 6D (SF-6D), Health Utilities Index Mark 3 (HUI3), Quality of Well-Being Scale (QWB), and Assessment of Quality of Life (AQOL). Arthritis Care Res. 2011;63(S11):S383–S412. doi:10.1002/acr.20541
32. Nutbeam D. Health promotion glossary. Health Promotion Int. 1998;13(4):349–364. doi:10.1093/heapro/13.4.349
33. Nutbeam D. Evaluating health promotion—progress, problems and solutions. Health Promotion Int. 1998;13(1):27–44. doi:10.1093/heapro/13.1.27
34. Nutbeam D. Health literacy as a public health goal: a challenge for contemporary health education and communication strategies into the 21st century. Health Promotion Int. 2000;15(3):259–267. doi:10.1093/heapro/15.3.259
35. Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. doi:10.7326/m18-0850
36. Paakkari L, Okan O. COVID-19: health literacy is an underestimated problem. Lancet Public Health. 2020;5(5):e249–e250. doi:10.1016/s2468-2667(20)30086-4
37. Nutbeam D, Lloyd JE. Understanding and responding to health literacy as a social determinant of health. Ann Rev Public Health. 2021;42(Volume 42, 2021):159–173. doi:10.1146/annurev-publhealth-090419-102529
38. Hong QN, Fàbregues S, Bartlett G, et al. The Mixed Methods Appraisal Tool (MMAT) version 2018 for information professionals and researchers. Educ Inf. 2018;34(4):285–291. doi:10.3233/EFI-180221
39. Chen S, Lu Q, Bai J, Deng C, Wang Y, Zhao Y. Global publications on stigma between 1998–2018: a bibliometric analysis. J Affect Disord. 2020;274:363–371. doi:10.1016/j.jad.2020.05.006
40. Eslami V, Tavakkoli-Sani S, Ghavami V, Peyman N. The relationship of health literacy with preventive behaviors of urinary tract infection in pregnant women. J Health Lit. 2022;6(4):22–31.
41. Mahdifar M, Tavakoly Sany SB, Ghavami V, Vahedian-Shahroodi M. Health literacy and body image concern among healthcare employees in Binaloud, Iran. J Health Lit. 2021;6(1):31–40.
42. Nancy Borkowski D, Meese KA. Organizational Behavior in Health Care. Sudbury, ON, Canada: Jones and Bartlett Publishers; 2011.
43. Hersh L, Salzman B, Snyderman D. Health literacy in primary care practice. Am Fam Physician. 2015;92(2):118–124.
44. Chinn D. Review of interventions to enhance the health communication of people with intellectual disabilities: a communicative health literacy perspective. J Appl Res Intellect Disabil. 2017;30(2):345–359. doi:10.1111/jar.12246
45. Baur C. The National Action Plan to Improve Health Literacy. US Department of Health and Human Services, Office of Disease Prevention and Health Promotion; 2010:19.
46. Singh T. Health education: concepts and strategies. J Indian Med Assoc. 1996;94(3):112–114.
47. Howe CJ, Adame T, Lewis B, Wagner T. Original research: assessing organizational focus on health literacy in north Texas hospitals. Am J Nurs. 2020;120(12):24–33. doi:10.1097/01.NAJ.0000723424.47838.4d
48. Hogan A, Hughes L, Coyne E. Understanding nursing assessment of health literacy in a hospital context: a qualitative study. J Clin Nurs. 2023;32(19–20):7495–7508. doi:10.1111/jocn.16809
49. Pignone M, DeWalt DA, Sheridan S, Berkman N, Lohr KN. Interventions to improve health outcomes for patients with low literacy. A systematic review. J Gen Intern Med. 2005;20(2):185–192. doi:10.1111/j.1525-1497.2005.40208.x
50. Cormier CM, Kotrlik JW. Health literacy knowledge and experiences of senior baccalaureate nursing students. J Nurs Educ. 2009;48(5):237–248. doi:10.3928/01484834-20090416-02
51. Wu T, Deng Z, Feng Z, Gaskin DJ, Zhang D, Wang R. The effect of doctor-consumer interaction on social media on consumers’ health behaviors: cross-sectional study. J Med Internet Res. 2018;20(2):e73. doi:10.2196/jmir.9003
52. Smith B, Magnani JW. New technologies, new disparities: the intersection of electronic health and digital health literacy. Int J Cardiol. 2019;292:280–282. doi:10.1016/j.ijcard.2019.05.066
53. Paasche-Orlow MK, Wolf MS. The causal pathways linking health literacy to health outcomes. Am J Health Behav. 2007;31 Suppl 1:S19–S26. doi:10.5555/ajhb.2007.31.supp.S19
54. Bremer D, Klockmann I, Jaß L, Härter M, von Dem Knesebeck O, Lüdecke D. Which criteria characterize a health literate health care organization? - a scoping review on organizational health literacy. BMC Health Serv Res. 2021;21(1):664. doi:10.1186/s12913-021-06604-z
55. Rathmann K, Salewski L, Vockert T, Lutz J, Spatzier D, Dadaczynski K. Tools to strengthen organizational health literacy in the health care sector. Z Evid Fortbild Qual Gesundhwes. 2022;170:21–28. doi:10.1016/j.zefq.2022.02.004
56. Brach C. The journey to become a health literate organization: a snapshot of health system improvement. Stud Health Technol Inform. 2017;240:203–237. doi:10.1093/intqhc/mzr024
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.