")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
A Pilot Study of Remote Ischemic Conditioning in Preventing Post-Stroke Depression
Authors Li W, Qin Y, Wang J, Li L, Gao J, Xu X, Wu Z, Ji X, Wang Y, Gao K, Ren M, Shao X
Received 8 September 2024
Accepted for publication 8 March 2025
Published 19 March 2025 Volume 2025:21 Pages 611—619
DOI https://doi.org/10.2147/NDT.S495215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Wanyan Li,1 Yankun Qin,1 Jinglei Wang,1 Lin Li,1 Junfeng Gao,1 Xiaowei Xu,1 Zhaohua Wu,1 Xunming Ji,2 Yanhong Wang,3 Keming Gao,4,5 Ming Ren,6 Xiangzhong Shao1
1Department of Neurology, Affiliated Haian Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China; 2Department of Neurology, Beijing Xuanwu Hospital, Beijing, People’s Republic of China; 3Department of Neurology, Shanghai Municipal Hospital of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 4Department of Psychiatry, University Hospitals Cleveland Medical Center, Cleveland, OH, USA; 5Case Western Reserve University School of Medicine, Cleveland, OH, USA; 6Department of Neurology, Shanghai Blue Cross Brain Hospital, Shanghai, People’s Republic of China
Correspondence: Xiangzhong Shao; Ming Ren, Email [email protected]; [email protected]
Background: Post-stroke depression (PSD) constitutes a significant complication that influences both patient survival and functional recovery following a stroke. Despite its prevalence, PSD still lacks a long-term, safe and effective treatment measure. Remote ischemic conditioning (RIC) is a simple and noninvasive procedure that exert neuroprotective effects. This pilot study aims to investigate the efficacy, safety, and feasibility of RIC as a preventive measure against PSD.
Methods: Acute ischemic stroke patients within 15 days post-event were considered eligible for study enrollment. Fifty participants were recruited and underwent daily RIC treatments for a 12-month period. Depressive symptoms were assessed utilizing the Patient Health Questionnaire-9 (PHQ-9) and the Hamilton Depression Rating Scale (HAMD) at baseline, as well as at 1, 3, 6, and 12-months post-intervention.
Results: The study found a gradual improvement in depressive symptoms among the 50 patients who completed the study over the 12-month treatment period, as evidenced by a consistent decline in pertinent scores. Moreover, merely two patients experienced mild adverse reactions.
Conclusion: The study’s outcomes indicate that RIC is safe, well-tolerated, and feasible as a preventive measure for PSD. Consequently, it is advisable to conduct a comprehensive randomized controlled trial to further evaluate the effectiveness and safety of RIC in preventing PSD.
Keywords: ischemic stroke, post stroke depression, remote ischemic conditioning, prevention
Introduction
Post-stroke depression (PSD) represents a prevalent complication following stroke, which is acknowledged in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5) as one of a few conditions that can “directly” cause depression. Approximately 17 million incidences of stroke occurred worldwide in 20101 and half of these patients survived with chronic disability.2 Prior research has demonstrated that at least 25% of stroke patients developed depressive symptoms within the first year following an acute stroke.3–5 The highest risk period for PSD was the initial few months after stroke. Prevalence of PSD ranges from 18% to 33%.6–9 The impact of PSD includes the risk of reducing rehabilitation progress and quality of life while increasing likelihood of recurrence of stroke.10 However, over half of PSD patients remain undiagnosed or untreated.11
Risk factors for PSD include female gender, history of psychiatric disorders, social isolation, large and multiple strokes within one-year post-stroke, strokes localized in anterior/frontal lobes and basal ganglia, and higher levels of disability associated with stroke.7–9,12–15 The pathogenesis of PSD is likely multifactorial, associated with decreased levels of monoamines and BDNF, abnormal neurotrophic response, increased inflammation, hypothalamic-pituitary-adrenal dysregulation, and glutamate-mediated excitotoxicity.16–19 The management strategies for PSD encompass psychosocial intervention, pharmacotherapy eg selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs), stroke-focused treatment, and neuromodulation techniques such as repetitive transcranial magnetic stimulation (rTMS) and electroconvulsive therapy (ECT).15,20,21 Despite these interventions potentially reducing PSD severity and improving quality of life, no large, high-quality studies have assessed the efficacy and safety of each intervention in patients with PSD.
In contrast to the traditional treatments of PSD, prevention could be more cost-effective. Interventions targeting decreased monoamine levels related to PSD, such as antidepressants, have yielded inconsistent and controversial results.22,23 Additionally, SSRIs may increase the risk of intracranial hemorrhage shortly after stroke due to their platelet aggregation inhibitory effect.24 Although rTMS has demonstrated efficacy in PSD treatment,25 the requirement of five days per week for at least four to six weeks in a clinical setting renders determining its efficacy and safety in prevention of PSD shortly after stroke as a major challenge, if not impossible.
Remote ischemic conditioning (RIC), recognized for its ease of application and the possibility of being performed at home, has shown promise in managing acute stroke and in the prevention of recurrent ischemic strokes, with minimal side effects, as highlighted in studies.26,27 The exploration of RIC in the context of Post-Stroke Depression (PSD) is still in its infancy. However, the potential impact of RIC in preventing PSD has been proposed by Wenbo Zhao et al in their 2017 study.
The exact mechanisms through which RIC offers neuroprotection after a stroke are not entirely clear. However, it’s believed that its influence on anti-inflammation, neuroplasticity, the monoamine system, and the hypothalamic-pituitary-adrenal axis (HPA-axis) are key factors. The protective effects of RIC on the heart and other organs lend further support to this hypothesis.28 In a single-arm trial focusing on the use of RIC for treating major depressive disorder (MDD),29 RIC proved to be safe and effective in reducing depressive symptoms. This study was conducted to determine whether RIC can prevent the occurrence of PSD.
Methods
Study Design
This study is a single-arm, open-label, prospective, and single-center trial investigating RIC in PSD. The study protocol was approved by the Institutional Review Board of Haian People’s Hospital (Nantong, Jiangsu, China) and registered in the Chinese Branch of WHO registration website (http://www.chictr.org.cn) for clinical trials with a registration number of ChiCTR-OPC-17012871.The study complies with the Declaration of Helsinki.
The trial adhered to the guidelines set forth by the Declaration of the Institutional Review Board of Haian People’s Hospital. Informed consent was obtained from each participant before any study-related procedures were performed. Acute ischemic stroke management was carried out in accordance with the Chinese acute ischemic stroke diagnosis and management guidelines (2018).
Patients
All subjects were recruited from the patients with ischemic stroke hospitalized in Department of Neurology at Haian People’s Hospital of Nantong, Jiangsu Province. The study took place from January 2020 to January 2022. Enrollment criteria included: 1) age between 18 and 80 years; 2) acute ischemic stroke confirmed via head CT (Computed Tomography) or brain MRI (Magnetic Resonance Imaging); 3) enrollment completed within 15 days post-ischemic stroke onset, with standard care; 4) patient mRS (modified Rankin Scale) score ≤ 3; and 5) capacity to provide informed consent. The mRS scores range from 0 to 6: a score of 0 indicates “no symptoms” 1 signifies “no clinically significant disability” 2 represents “slight disability” (able to manage own affairs without assistance but unable to perform all previous activities), 3 denotes “moderate disability” (requires some help but can walk unassisted), 4 implies “moderately severe disability” (unable to attend to bodily needs or walk), 5 signifies “severe disability” (receiving constant nursing care and attention), and 6 indicates “death.”
Patients were excluded if they had any of the following: 1) history of psychiatric disorders (eg, schizophrenia, bipolar disorder, major depressive disorder); 2) other intracranial diseases such as infection, tumor, or bleeding, as confirmed by head CT or MRI; 3) coagulation disorders or platelet counts <100 * 109/L, history of retinal and visceral hemorrhage, or on thrombolytic drugs; 4) uncontrolled high blood pressure (systolic pressure >180 mmHg or diastolic pressure >110 mmHg) that could not be managed with antihypertensive medications; 5) severe renal failure with a creatinine clearance rate <0.6 mL/s or serum creatinine level >265 μmol/l; 6) severe hepatic failure, defined as serum alanine aminotransferase (ALT) or aspartate aminotransferase (AST) at least three times the upper limit of normal; 7) history of coronary artery disease; 8) peripheral vascular disease of the upper extremity, such as severe subclavian artery stenosis; or 9) recent upper extremity fracture, soft tissue damage, or vascular injury.
Remote Ischemic Conditioning (RIC) Treatment
RIC was performed using the IPC-906 device obtained from Beijing Renqiao Cardio-cerebrovascular Disease Prevention Research Nantong Co., Ltd, China. The device features two electric-control cuffs that generate 200 mmHg of pressure for ischemic conditioning. By applying pressure to both upper arms, simultaneous ischemic conditioning of the bilateral forearms was induced. Five cycles of arterial and venous blood flow blockage to the forearms were executed. Each ischemic phase lasted for 5 minutes, followed by a 5-minute reperfusion period.30 Enrolled patients underwent RIC once daily for 12 months. RIC was the only treatment modality used in patients at risk for PSD and the RIC procedure could be stopped at any time if the patient experienced intolerable discomfort or other adverse reactions.
Safety Monitoring
Treatment-emergent adverse events (TEAEs), such as skin or neurovascular injuries resulting from the RIC procedure, were assessed and documented at each treatment session by the investigator, who determined the severity of the adverse event (AE). Reporting of AEs and serious adverse events (SAEs) was conducted in accordance with the requirements of the Institutional Review Board of Haian People’s Hospital (Nantong, Jiangsu, China). Additionally, laboratory tests, including a comprehensive metabolic panel, urine pregnancy test (if applicable), ECG (Electrocardiography), and complete blood count, were performed at baseline and one week after initiating RIC. The results showed that these indicators were basically normal. Patient treatment adherence was assessed by counting the number of missed sessions for each patient. The number of missed sessions equaled 5 times the number of follow-up weeks minus the recorded sessions from the IPC-906 device. The average missed sessions were calculated as: the number of missed RIC treatment sessions / total RIC treatment number × 100%.
Assessments
We needed several standardized tools to comprehensively assess the evaluation of neurologic deficit severity and depression in ischemic stroke patients. The National Institutes of Health Stroke Scale (NIHSS) is a widely recognized tool for assessing the severity of a stroke, providing a standardized measure of a patient’s neurologic deficit. The modified Rankin Scale (mRS) is undoubtedly the most frequent assessment of functional prognosis after stroke. However, evaluating depression is a challenging process, especially if the subject is elderly and co-existed with stroke. A lot of questionnaires are utilized to measure depression. At the beginning of the research, we chose Self-Rating Depression Scale (SDS) which was commonly used due to its simplicity. But it does not cover all symptoms of depression and it has more items compared to the Patient Health Questionnaire-9 (PHQ-9). The PHQ-9 is a self-administered scale for depression, based on the nine items of the DSM-IV diagnostic criteria. It is known for its effectiveness, strong reliability and validity in diagnosing depression and evaluating symptom severity. Finally, we used the PHQ-9 in initial screening of depressed patients, and then the Hamilton Rating Scale for Depression - 17 items (HAMD-17) was applied for more accurate assessment of depression.
Initially, at baseline, and subsequently at the first, third, sixth, and twelfth month post-stroke, patients were evaluated using the NIHSS, mRS, PHQ-9 and the HAMD-17. These evaluations were conducted in-person by investigators and research coordinators at the study site. To ensure the accuracy and reliability of these assessments, all raters underwent specialized training in NIHSS, mRS, PHQ-9, and HAMD. They received certifications from international neurologists and experienced psychiatrists affiliated with Haian People’s Hospital of Nantong University and University Hospitals Cleveland Medical Center. Moreover, M, YK, and KM, recognized experts in their fields, oversaw the process to guarantee the reliability of these assessments.
Statistical Analysis
Demographic, clinical characteristics, and adverse events (AEs) were analyzed using descriptive statistics (Table 1). The safety profile included all patients who received at least one RIC treatment. Baseline to endpoint NIHSS, mRS, PHQ-9, and HAMD scores were analyzed using the paired t-test (Table 2). Any depression was calculated as the number of patients with depression / total number of patients × 100%. All statistical analyses were performed using R software (version 4.0.3). The criterion for statistical significance was set at 0.05.
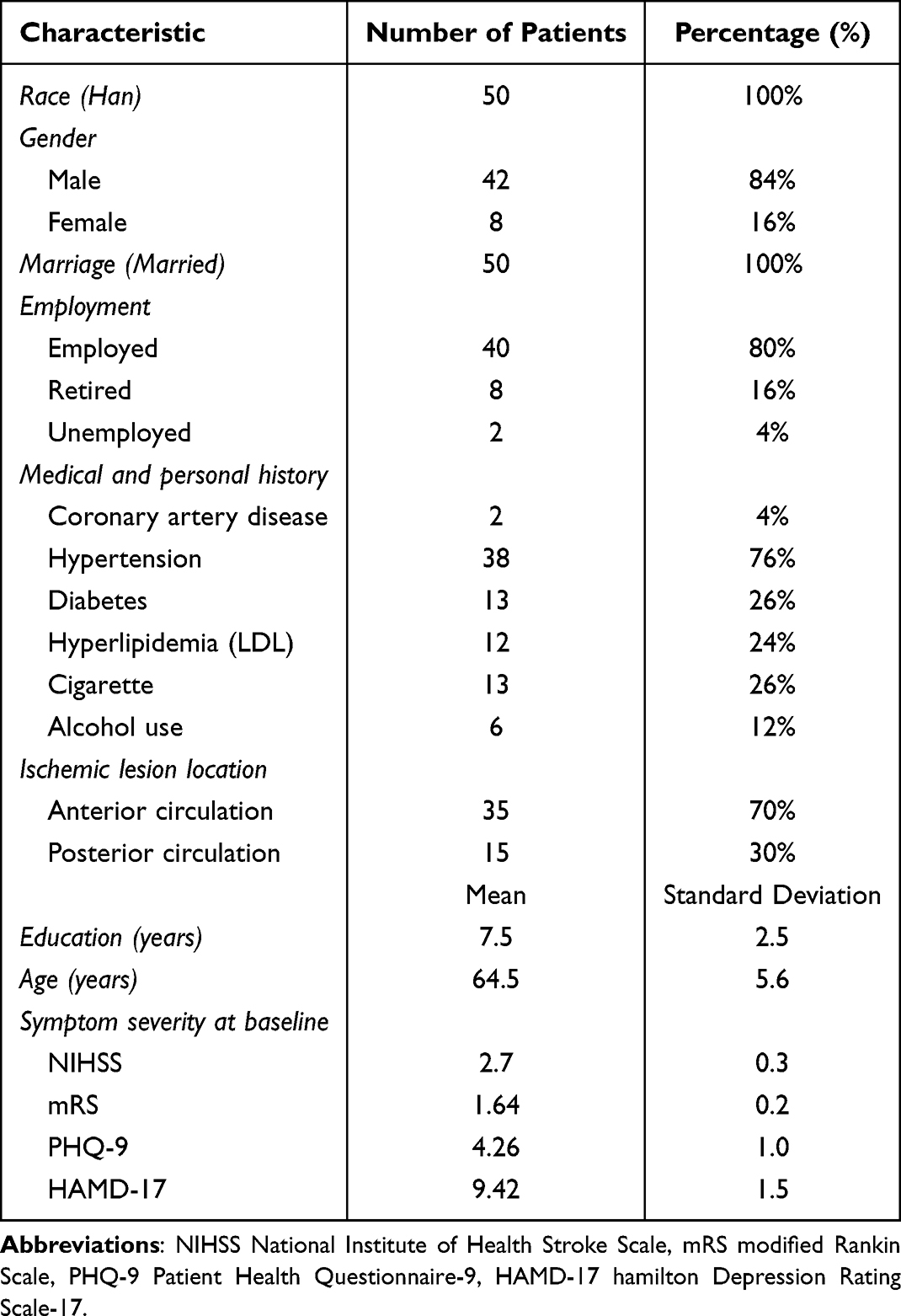 |
Table 1 Demographics and Clinical Characteristics of Enrolled Patients with Ischemic Stroke |
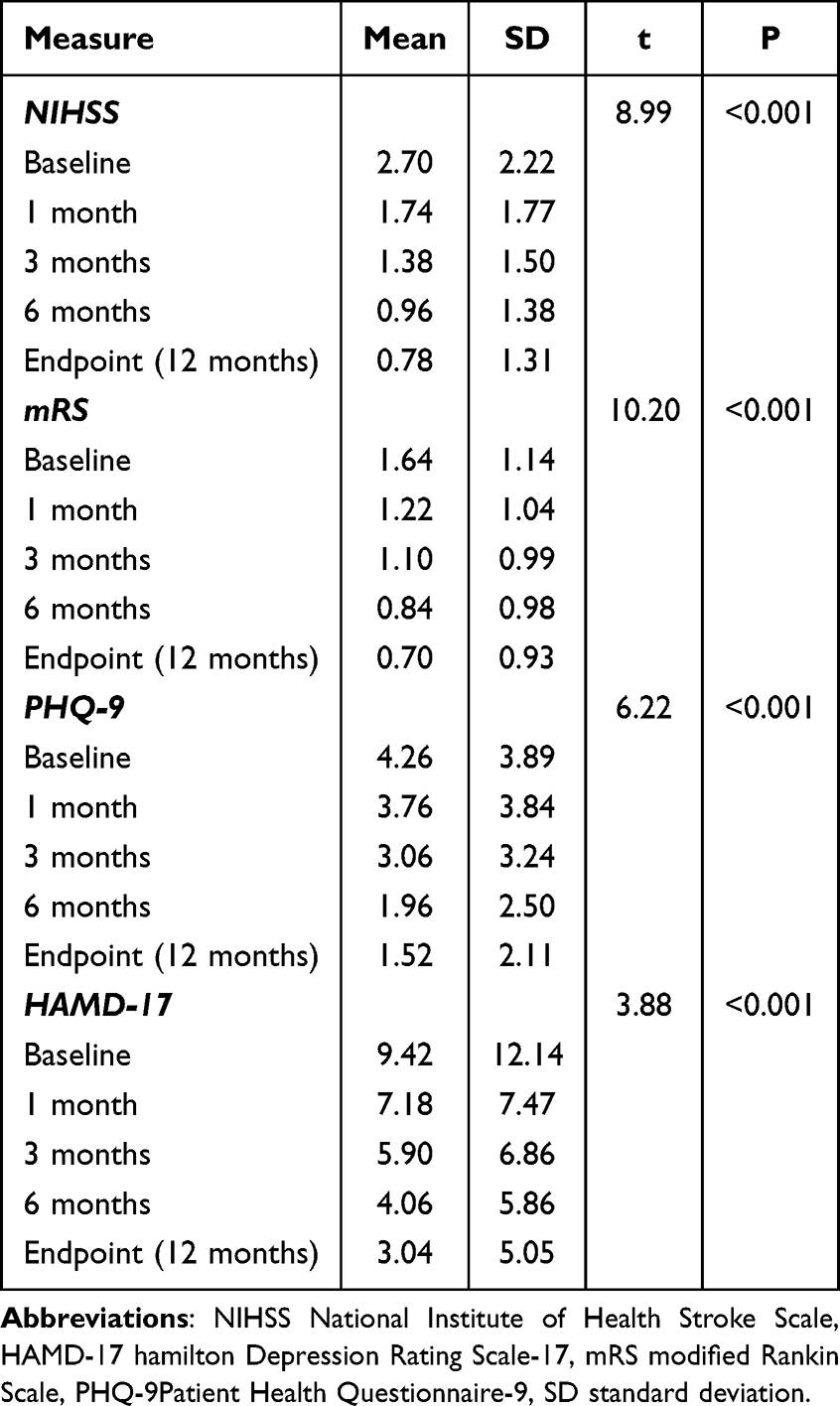 |
Table 2 Efficacy Outcomes of Remote Limb Ischemic Preconditioning |
Results
Demographics and Baseline Clinical Characteristics
Fifty patients with ischemic stroke who met the inclusion criteria and none of the exclusion criteria were enrolled in this study. All 50 patients completed the remote ischemic conditioning procedure and were included in the analysis. Demographics, including race, gender, age, marital status, education, employment, medical and personal history, ischemic lesion, and baseline scores of NIHSS (National Institute of Health Stroke Scale), mRS, PHQ-9 (Patient Health Questionnaire-9), and HAMD-17 (Hamilton Depression Rating Scale −17) at study entry are presented in Table 1.
Adverse Events and Adherence
Out of the 50 patients enrolled, two experienced mild limb numbness that resolved within three days after initiating RIC. One patient developed petechiae of the skin under the pressure cuff area during the first week of RIC. No patients had severe adverse events. In terms of adherence, missed sessions for all patients averaged at 23%. Furthermore, all 50 participants in this study received RIC in at least 281 of the 365 treatment sessions (77% average adherence rate).
Efficacy Analysis
A significant reduction in both National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores was observed from the baseline to the endpoint (12 months), shifting from 2.70 ± 2.22 to 0.78 ± 1.31 (P <0.001) and 1.64 ± 1.14 to 0.70 ± 0.93 (P <0.001), respectively (Table 2). The Patient Health Questionnaire-9 (PHQ-9) and Hamilton Depression Rating Scale-17 (HAMD-17) scores also saw a significant decrement from baseline to the endpoint, altering from 4.26 ± 3.89 to 1.52 ±2.11 for PHQ-9 and 9.42 ± 12.14 to 3.04 ± 5.05 for HAMD-17 (refer to Table 2). A comprehensive visual representation of the significant reduction from baseline to the endpoint in NIHSS score, mRS score, PHQ-9, and HAMD-17 scores is presented (Figures 1 and 2).
 |
Figure 1 NIHSS and mRS scores in patients (N = 50) post ischemic stroke in 1, 3, 6, and 12 months. The results showed that scores of NIHSS and mRS at baseline, 1, 3, 6, and 12 months were treading down, with NIHSS dropping from 2.70 to 0.78 and mRS from 1.64 to 0.70. |
 |
Figure 2 HAMD-17 and PHQ-9 scores in patients (N = 50) post ischemic stroke in 1, 3, 6, and 12 months. The results showed that scores of HAMD-17 and PHQ-9 at baseline, 1, 3, 6, and 12 months were treading down with HAMD-17 dropping from 9.42 to 3.04, and PHQ-9 dropping from 4.26 to 1.52. |
Rates of Depression Based on PHQ-9 and HAMD-17 Scores
Among the 50 patients evaluated using the PHQ-9, the number and percentage of patients with various degrees of depression, from none or minimal to severe, were calculated at baseline, 1, 3, 6, and 12 months. At baseline, 32 (64%) did not have depression, 12 (24%) had mild depression, 5 (10%) had moderate depression, 1(2%) had moderate severe depression, and none had severe depression (Table 3). The proportion of patients with no or minimal depression was 70% at 1 month, 76% at 3 months, 84% at 6 months, and 88% at 12 months (Table 3). All 50 patients were also assessed with the HAMD-17 rating scale. The numbers and percentages of patients with no, mild, moderate, and severe depression at baseline, 1, 3, 6, and 12 months were calculated (Table 4). At baseline, 28 (56%) patients were not depressed (score ≤6), 10 (20%) had mild depression (score:7–16), 10 (20%) had moderate depression score:18–24, and 2 (4%) had severe depression (score: ≥25). The proportion of patients without depression was 62% at 1 month, 72% at 3 months, 76% at 6 months, and 84% at 12 months (Table 4).
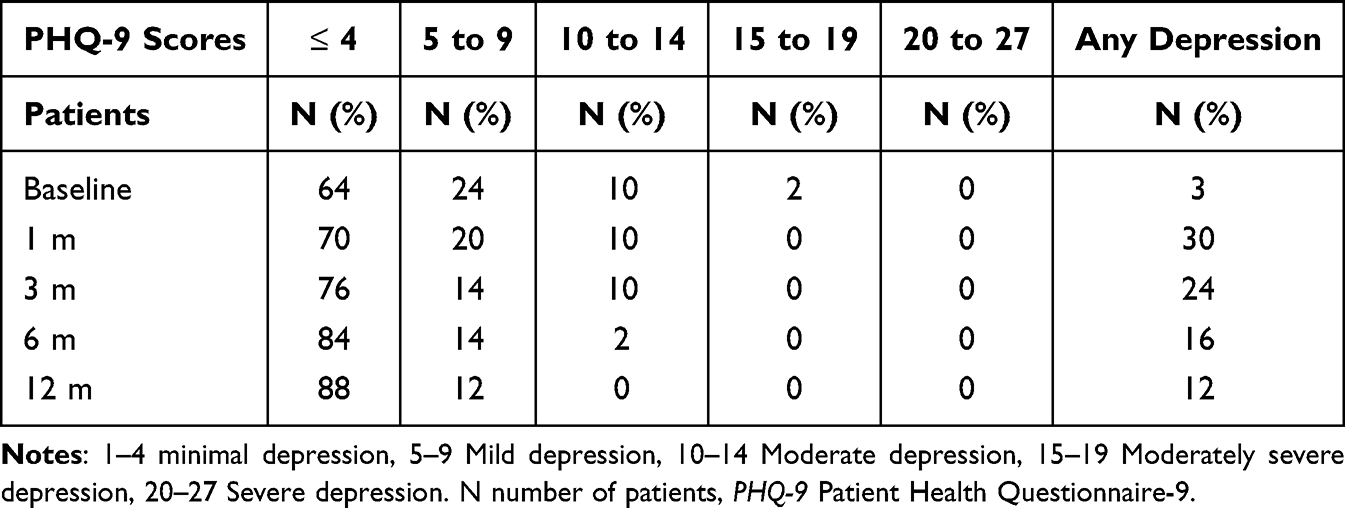 |
Table 3 PHQ-9 Score in Ischemic Stroke Patients Before and After Treatment with Remote Ischemic Conditioning (N = 50) |
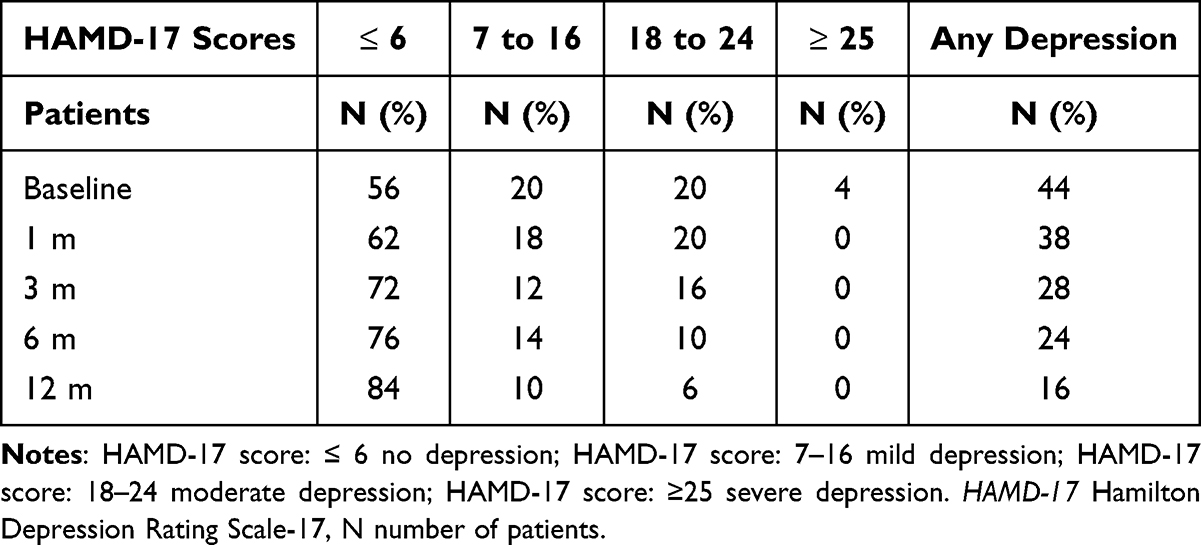 |
Table 4 HAMD-17 Score in Patients with Ischemic Stroke Before and After Treatment with Remote Ischemic Conditioning (N = 50) |
Discussion
In this single-arm clinical trial, we recruited 50 patients within 15 days following an acute ischemic stroke. Each patient received daily Remote Ischemic Conditioning (RIC) for a period of 12 months. The depressive symptoms of the patients were assessed with PHQ-9 and HAMD-17 at baseline, and subsequently at the first, third, sixth, and twelfth month after the ischemic stroke. Throughout the 12-month follow-up period, we observed a consistent downward trend in both PHQ-9 and HAMD-17 scores. Broadly, the prevalence of post-stroke depression symptoms saw a considerable reduction, from 46% at baseline to 12% at the end of the 12 months, as per PHQ-9 data. According to the HAMD-17 scores, the proportion of patients experiencing moderate to severe depression decreased from 24% to 6%, while the percentage of patients exhibiting no depression increased from 56% to 84%. These outcomes suggest a strong potential of RIC in preventing post-stroke depression.
The findings of this study could be attributed to several factors: 1) natural evolution of the patient’s mood following a severe physical illness; 2) selection bias due to the limited sample size; and 3) the potential protective effect of RIC against post-stroke depression.
Patient safety is paramount in clinical practice. Prior studies have evidenced the safety of long-term RIC in patients with severe carotid artery stenosis (CAS) and intracranial arterial stenosis (ICAS).27,30,31 Furthermore, RIC exhibited no significant impact on the mean blood flow velocity, oxygenation index, and heart rate in ICAS patients and healthy volunteers. Our investigation corroborates these findings and demonstrates that RIC is safe and well-tolerated in patients with acute ischemic stroke. In our study, only two patients reported mild limb numbness and distal red flecks on the skin beneath the RIC cuffs. Importantly, no patient ceased the RIC treatment or withdrew from the study due to adverse effects, which is a significant improvement over previous studies involving CAS patients.26
At present, psychotherapy, neurostimulation treatments, and pharmacotherapy are the most prevalent strategies for managing Post-Stroke Depression (PSD) but these methods have sparked debates over their adherence and efficacy. As per existing data, about 20% of patients in outpatient clinics may not comply with prescribed antidepressants. Additionally, roughly one-third of patients with depression may discontinue short-term treatments such as transcranial direct current stimulation (tDCS) and repetitive transcranial magnetic stimulation (rTMS). Thus, it has been estimated that conventional treatments are successful in managing approximately 30–40% of all cases of PSD.15,32 Yet, it must be acknowledged that these existing therapies may prove insufficient for a substantial portion of PSD patients. However, our research suggests that RIC might possess an advantage in terms of treatment adherence and effectiveness.33
Moreover, the practicality of implementing RIC is underscored as a significant advantage in our study. The simplicity of RIC not only facilitates its understanding but also its application, thereby enhancing its accessibility. Importantly, it does not necessitate a dedicated space for its execution, which implies that this treatment can be administered without the requirement for any additional resources.
In summary, we observed that the treatment resulted in improvements in depressive symptoms over a 12-month treatment period. RIC may play a positive role in preventing post-stroke depression.
Limitations
The limitations of this study include a small sample size, a single-arm design, and an open-label approach. These factors may pose challenges in definitively establishing the preventive effects of RIC against post-stroke depression (PSD). The small sample size may introduce biases in evaluating the safety and efficacy of RIC in PSD, potentially either inflating or deflating its effects. The single-arm design precludes direct comparisons with a control group, making it difficult to ascertain the true efficacy of RIC in preventing PSD. Nonetheless, it is possible to indirectly compare our results with those from previous studies that did not involve RIC and focused on PSD. Additionally, the open-label design may contribute to an increased “placebo” effect. Given these limitations, larger, randomized, double-blind, sham-controlled trials are essential to definitively verify both the efficacy and safety of RIC as a preventive measure for PSD in patients with acute ischemic stroke.
Conclusions
RIC, as a simple, easy-to-use and noninvasive therapy, is safe and well-tolerated in patients with acute ischemic stroke. This pilot study suggests that RIC is effective in preventing PSD. We expect further research about RIC in PSD.
Data Sharing Statement
Anonymized data not published within this article will be made available by request from Wanyan Li ([email protected]).
Ethical Approval
This research was approved by the Medical Ethics Committee of Haian People’s Hospital, approval GJZ16126-8.
Informed Consent
Informed consent requirement was waived by the Institutional Review Board (minimal risk). All data analyzed were collected as part of routine diagnosis and treatment.
Funding
No funding has been received for this paper.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Feigin V, Forouzanfar M, Krishnamurthi R, et al. Global and regional burden of stroke during 1990-2010: findings from the global burden of disease study. Lancet. 2014;383:245–254. doi:10.1016/s0140-6736(13)61953-4
2. Donkor ES. Stroke in the 21(st) century: a snapshot of the burden, epidemiology, and quality of life. Stroke Res Treat. 2018;2018:3238165. doi:10.1155/2018/3238165
3. House A, Dennis M, Mogridge L, Warlow C, Hawton K, Jones L. Mood disorders in the year after first stroke. Br J Psychiatry. 1991;158:83–92. doi:10.1192/bjp.158.1.83
4. Kapoor A, Si K, Yu A, et al. Younger age and depressive symptoms predict high risk of generalized anxiety after stroke and transient ischemic attack. Stroke. 2019;50(9):2359–2363. doi:10.1161/strokeaha.119.025464
5. Dong L, Sánchez B, Skolarus L, Stulberg E, Morgenstern L, Lisabeth L. Sex difference in prevalence of depression after stroke. Neurology. 2020;94(19):e1973–e83. doi:10.1212/wnl.0000000000009394
6. Mitchell A, Sheth B, Gill J, et al. Prevalence and predictors of post-stroke mood disorders: a meta-analysis and meta-regression of depression, anxiety and adjustment disorder. Gen Hosp Psychiatry. 2017;47:48–60. doi:10.1016/j.genhosppsych.2017.04.001
7. Jørgensen TS, Wium-Andersen IK, Wium-Andersen MK, et al. Incidence of depression after stroke, and associated risk factors and mortality outcomes, in a large cohort of Danish patients. JAMA Psychiatry. 2016;73(10):1032–1040. doi:10.1001/jamapsychiatry.2016.1932
8. Hackett M, Pickles K. Part I: frequency of depression after stroke: an updated systematic review and meta-analysis of observational studies. Int J Stroke. 2014;9(8):1017–1025. doi:10.1111/ijs.12357
9. Ayerbe L, Ayis S, Wolfe CD, Rudd AG. Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis. Br J Psychiatry. 2013;202(1):14–21. doi:10.1192/bjp.bp.111.107664
10. Alghwiri A. The correlation between depression, balance, and physical functioning post stroke. J Stroke Cerebrovasc Dis. 2016;25(2):475–479. doi:10.1016/j.jstrokecerebrovasdis.2015.10.022
11. Espárrago Llorca G, Castilla-Guerra L, Fernández Moreno M, Ruiz Doblado S, Jiménez Hernández M. Post-stroke depression: an update. Neurologia. 2015;30:23–31. doi:10.1016/j.nrl.2012.06.008
12. Robinson RG, Jorge RE. Post-stroke depression: a review. Am J Psychiatry. 2016;173(3):221–231. doi:10.1176/appi.ajp.2015.15030363
13. Zhang T, Jing X, Zhao X, et al. A prospective cohort study of lesion location and its relation to post-stroke depression among Chinese patients. J Affective Disorders. 2012;136:e83–e7. doi:10.1016/j.jad.2011.06.014
14. Ku HL, Chen CH, Yang YT, et al. Association between cerebral lesions and emotional changes in acute ischemic stroke patients. J Nerv Ment Dis. 2013;201(5):400–406. doi:10.1097/NMD.0b013e31828e0fe9
15. Medeiros GC, Roy D, Kontos N, Beach SR. Post-stroke depression: a 2020 updated review. Gen Hosp Psychiatry. 2020;66:70–80. doi:10.1016/j.genhosppsych.2020.06.011
16. Dongqing J, Xiaoli H, Xiao G, et al. Sun Xiaodong. Astrocytes in post-stroke depression: roles in inflammation, neurotransmission, and neurotrophin signaling. Cell mol Neurobiol. 2023;43(7):3301–3313. doi:10.1007/s10571-023-01386-w
17. Loubinoux I, Kronenberg G, Endres M, et al. Post-stroke depression: mechanisms, translation and therapy. J Cell & Mol Med. 2012;16(9):1961–1969. doi:10.1111/j.1582-4934.2012.01555.x
18. Whyte EM, Mulsant BH. Post stroke depression: epidemiology, pathophysiology, and biological treatment. Biol Psychiatry. 2002;52(3):253–264. doi:10.1016/s0006-3223(02)01424-5
19. Roberson AM, Castro VM, Cagan A, Perlis RH. Antidepressant nonadherence in routine clinical settings determined from discarded blood samples. J Clin Psychiatry. 2016;77(3):359–362. doi:10.4088/JCP.14m09612
20. Lincoln NB, Flannaghan T. Cognitive behavioral psychotherapy for depression following stroke: a randomized controlled trial. Stroke. 2003;34(1):111–115. doi:10.1161/01.str.0000044167.44670.55
21. Legg LA, Rudberg AS, Hua X, et al. Selective serotonin reuptake inhibitors (SSRIs) for stroke recovery. Cochrane Database Syst Rev. 2021;11(11):Cd009286. doi:10.1002/14651858.CD009286.pub4
22. Gu J, Huang H, Chen K, Huang G, Huang Y, Xu H. Are they necessary? preventive therapies for post-stroke depression: a meta-analysis of RCTs. Psychiatry Res. 2020;284:112670. doi:10.1016/j.psychres.2019.112670
23. Kim JS. Management of post-stroke mood and emotional disturbances. Expert Rev Neurother. 2017;17(12):1179–1188. doi:10.1080/14737175.2017.1395281
24. Hackam DG, Mrkobrada M. Selective serotonin reuptake inhibitors and brain hemorrhage: a meta-analysis. Neurology. 2012;79(18):1862–1865. doi:10.1212/WNL.0b013e318271f848
25. Duan H, Yan X, Meng S, et al. Effectiveness evaluation of repetitive transcranial magnetic stimulation therapy combined with mindfulness-based stress reduction for people with post-stroke depression: a randomized controlled trial. Int J Environ Res Public Health. 2023;20(2):930. doi:10.3390/ijerph20020930
26. Meng R, Asmaro K, Meng L, et al. Upper limb ischemic preconditioning prevents recurrent stroke in intracranial arterial stenosis. Neurology. 2012;79(18):1853–1861. doi:10.1212/WNL.0b013e318271f76a
27. An J, Cheng Y, Guo Y, et al. Safety and efficacy of remote ischemic postconditioning after thrombolysis in patients with stroke. Neurology. 2020;95(24):e3355–e63. doi:10.1212/wnl.0000000000010884
28. Hausenloy DJ, Yellon DM. Remote ischaemic preconditioning: underlying mechanisms and clinical application. Cardiovasc Res. 2008;79(3):377–386. doi:10.1093/cvr/cvn114
29. Wang Z, Li X, Li N, et al. Safety and tolerability of both arm ischemic conditioning in patients with major depression: a proof of concept study. Frontiers in Psychiatry. 2020;11:570. doi:10.3389/fpsyt.2020.00570
30. Zhao W, Meng R, Ma C, et al. Safety and efficacy of remote ischemic preconditioning in patients with severe carotid artery stenosis before carotid artery stenting: a proof-of-concept, randomized controlled trial. Circulation. 2017;135(14):1325–1335. doi:10.1161/circulationaha.116.024807
31. Sijie L, Wenbo Z, Guiyou L, et al. Chronic remote ischemic conditioning for symptomatic internal carotid or middle cerebral artery occlusion: a prospective cohort study. CNS Neurosci Ther. 2022;28(9):1365–1371. doi:10.1111/cns.13874
32. Thibaut A, O’Brien A, Fregni F. Strategies for replacing non-invasive brain stimulation sessions: recommendations for designing neurostimulation clinical trials. Expert Rev Med Devices. 2017;14(8):633–649. doi:10.1080/17434440.2017.1352470
33. Frank D, Gruenbaum B, Zlotnik A, Semyonov M, Frenkel A, Boyko M. Pathophysiology and current drug treatments for post-stroke depression: a review. Int J mol Sci. 2022;23(23). doi:10.3390/ijms232315114
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.