")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
A Randomized Controlled Study of Efficacy and Cognitive Function Improvement of Vortioxetine and Escitalopram in Patients with Depression in Chinese Han Nationality
Authors Ye X, Xu P, Jiao J, Zhao H, Jin K, Zhang S, Pan F, Chen J, Jiang H, Hu J, Huang M
Received 16 August 2024
Accepted for publication 21 November 2024
Published 5 December 2024 Volume 2024:20 Pages 2363—2374
DOI https://doi.org/10.2147/NDT.S491768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Xinyi Ye,1– 4,* Pengfeng Xu,1– 4,* Jianping Jiao,1– 4 Haoyang Zhao,1– 4 Kangyu Jin,1– 5 Shiyi Zhang,1– 4 Fen Pan,1– 4 Jingkai Chen,1– 4 Hao Jiang,1– 4 Jianbo Hu,1– 4 Manli Huang1– 4
1Department of Psychiatry, The First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China; 2Zhejiang Key Laboratory of Precision psychiatry, Hangzhou, 310003, People’s Republic of China; 3Brain Research Institute of Zhejiang University, Hangzhou, 31003, People’s Republic of China; 4Zhejiang Engineering Center for Mathematical Mental Health, Hangzhou, 310003, People’s Republic of China; 5Institute of Translational Medicine, Zhejiang University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Manli Huang, Department of Psychiatry, the First Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310003, People’s Republic of China, Email [email protected]
Objective: To assess the efficacy and safety of Vortioxetine and Escitalopram in improving cognition in patients with major depressive disorder (MDD).
Methods: At baseline, 131 MDD patients and 70 healthy controls completed the Hamilton Depression Scale (HAMD-17), Hamilton Anxiety Scale (HAMA), Snaith-Hamilton Pleasure Scale (SHAPS) and MATRICS Consensus Cognitive Battery (MCCB). Patients with MDD were randomly divided into Vortioxetine (n = 62) and Escitalopram (n = 69) groups with an 8-week follow-up research. ANOVA for repeated measurement was utilized to compare the efficacy of Vortioxetine and Escitalopram.
Results: The total scores of HAMD-17, HAMA and SHAPS scales had statistical difference between MDD cases and healthy controls (P < 0.001) at baseline. After 8 weeks of treatment, the scale scores of the HAMD-17, HAMA and SHAPS had lowered in both groups, with no statistical difference between two groups (P > 0.05). At baseline, MDD patients had defects in Speed of Processing, Attention Vigilance, Verbal Learning, Visual Learning, Reasoning and Problem Solving, and Social Cognition, compared with healthy controls. After 8 weeks of treatment with Vortioxetine or Escitalopram, the patients had improved in the aspects of cognitive functions above except Social Cognition. Numerical improvements of MCCB scale were found in the two groups, P > 0.05. Most adverse events were mild or moderate, with nausea being the most common adverse event.
Conclusion: Both Vortioxetine and Escitalopram can improve the mental status and cognitive functions in MDD patients, with mild or moderate adverse events.
Trial Registration: www.chictr.org.cn, identifier: ChiCTR1900024858.
Keywords: vortioxetine, escitalopram, major depressive disorder, randomized controlled trial, efficacy
Introduction
Major Depression disorder (MDD), a common mental disorder, features high prevalence, high relapse rate, high suicide rate, and heavy economic burden. The latest epidemiological studies show that the lifetime prevalence of MDD is 3.4% in China.1 The DALY rate of MDD is 409.7 per 100,000 people in China in 2017.2 The treatment of MDD is faced with the dilemma of low remission rate and residual symptoms. According to STAR*D trial, most MDD participants received citalopram and other antidepressants. However, after 12 weeks of treatment with 4 different antidepressants in 1 year, only 67% of patients finally achieved clinically remission.3 MDD patients recover slowly due to residual cognitive symptoms during remission; thus, remission may not be achieved after multiple interventions.4 MDD patients have lower remission rates due to cognitive impairment.5 Evidence suggests that MDD patients show clinical deficits in five cognitive domains: attention, response inhibition, verbal memory, decision speed, and information processing. Even if the depressive symptoms are significantly alleviated, the cognitive symptoms still lack corresponding improvement.6
Previous findings suggest that escitalopram and vortioxetine have inherently greater efficacy and acceptability than other antidepressants.7 Studies demonstrate that Escitalopram, one of the most selective SSRI, has great efficacy in relieving the symptoms of MDD in China.8 Furthermore, latest meta-analyses have showed that Escitalopram and other SSRIs have modest positive effect on recovery of cognition.9
Vortioxetine was approved for MDD treatment by the Federal Drug Administration in 2013 and approved for clinical use in China in 2017. Unlike Escitalopram, Vortioxetine is a multimodal antidepressant, acting on six pharmacological targets through two different modes of action, including inhibiting the reuptake of the 5-HT transporter (SERT), antagonizing 5-HT3, 5-HT7 and 5-HT1D, agonizing 5-HT1A and partially agonizing 5-HT1B.10 Studies found that Vortioxetine enhances LTP and long-lasting changes in hippocampal synaptic functions; it also stimulates neurogenesis, increases dendritic length, and promotes neuronal neurotransmission and synaptic neuroplasticity in this brain region.11 Behavioral studies indicate that Vortioxetine has antipsychotic and antidepressant activity in different animal models.12 It has also been shown to promote memory, cognition and executive functions in a variety of animal models.13,14 Clinical studies in many countries have reported the clinical effects of Vortioxetine on cognitive function in patients with depression.15–18 A Single-Arm RELIEVE China Study demonstrates short- and long-term effectiveness and tolerability of Vortioxetine for patients with MDD in China.19 Meanwhile, a network meta-analysis shows that Vortioxetine provides statistically significant improvements in cognitive function compared with other antidepressants, possibly due to its unique pharmacological profile.20
The clinical efficacy and safety of Vortioxetine have been confirmed in Asian countries, and some studies suggest that Vortioxetine is better tolerated than other antidepressants.7,21 However, there is currently a lack of head-to-head comparative study in the Chinese population.
Therefore, this randomized, head-to-head, 8-week study is aimed to evaluate the efficacy and the cognitive function benefit of Vortioxetine compared with Escitalopram in MDD patients in China.
Methods
Participants
Patients who meet the diagnostic criteria for MDD according to the Diagnostic and Statistical Manual of Mental Disorders, Five Edition (DSM-5)22 were recruited from the Department of Psychiatry at the First Affiliated Hospital, College of Medicine, Zhejiang.
The inclusion criteria used in this study for patient selection were : (1) patients aging from 18 to 45; (2) patients with MDD meeting the diagnostic criteria of DSM-5;22 MDD diagnosed for the first time without any treatment, or relapsed depression without treatment; (4) the total score of Hamilton Depression Scale (HAMD-17) ≥17; (5) Han-nationality, right-handed; and (6) junior high school education or above.
The exclusion criteria were as follows: (1) patients who received the use of antidepressants or other psychiatric drugs, or other antidepressive treatments such as transcranial magnetic stimulation (TMS) and electroshock; (2) comorbidities or a history of other mental disorders;22 (3) a first-degree relative with a history of mental disorder; (4) secondary mental disorders caused by drugs or organic factors; (5) a history of major neurological diseases (eg epilepsy, stroke), physical diseases (eg heart disease, hypertension, liver disease), and endocrine diseases (eg diabetes); (6) a history of alcohol or drug abuse or dependence; (7) contraindications for magnetic resonance imaging (MRI) (eg metal implants, claustrophobia).
This study was approved by the Ethics Review Committee of the First Affiliated Hospital of Zhejiang University School of Medicine (approval number: No. 2019(1014)) and was registered at China Clinical Trial Registry (www.chictr.org.cn, registration number: ChiCTR1900024858). All subjects had signed the informed consent before the study.
Healthy Controls
The health controls (n=70) underwent free psychological tests. Healthy controls and MDD patients were matched by age, sex, and years of education. Exclusion criteria were the same as for patients with MDD.
Study Design, Medications, Randomization, and Blinding
The study consisted of an initial screening and psychological test of patients and healthy controls, starting from 06/02/2020, followed by a randomized, 8-week and active controlled treatment.
All eligible patients were then randomly assigned to either of two groups: Vortioxetine or Escitalopram group based on a computer-generated randomization scheme stratified by the center.
Vortioxetine: The patients took 5 mg orally after supper for the first 2 days, and 10 mg orally on the third day. If the 4-week decrease rate of HAMD-17 score was less than 50%, the dosage could be gradually increased to 15–20 mg per day. Vortioxetine was continuously used for 8 weeks.
Escitalopram: Took 5mg orally after supper for the first 2 days and changed to 10mg orally after supper on the third day. If the 4-week decrease rate of HAMD-17 score was less than 50%, the dose could be gradually increased to 15–20 mg per day. Escitalopram was continuously used for 8 weeks.
The efficacy and safety assessments were performed by trained practitioners who were blind to the treatment that the patients were receiving.
Concomitant Medication
Benzodiazepines and propranolol tablets can be used together. However, benzodiazepines should not be administered within 6 hours before a predetermined efficacy or safety rating. Other antidepressants and any prescription drugs, illicit mood-altering drugs, or over-The-counter drugs with psychotherapeutic properties were not permitted.
Assessments
Primary Outcome: Efficacy Assessments
The primary efficacy variable was the change in HAMD-17 total score from baseline to endpoint (week 8). Secondary efficacy variables included changes from baseline to endpoint in Hamilton Anxiety Rating Scale (HAMA) and Snaith-Hamilton Pleasure Scale (SHAPS) scores. Trained assessors with relevant clinical expertise performed all efficacy assessments. Where possible, scale administration was conducted by the same rater at all scheduled visits from baseline to final assessment (weeks 2, 4, and 8 or at early withdrawal).
Secondary Outcome: Cognitive Function Assessments
MATRICS Consensus Cognitive Battery (MCCB) was conducted at baseline and week 8 to assess cognitive function. The MCCB has seven factors in total, assessing cognitive function from aspects such as Speed of Processing, Attention Vigilance, Working Memory, Verbal Learning, Visual Learning, Reasoning and Problem Solving, and Social Cognition.
Safety Assessments
Treatment-emergent adverse events (TEAEs) were evaluated and recorded from baseline to final assessment (weeks 2, 4, and 8 or at early withdrawal).
Statistical Analysis
The intention-to-treat (ITT) analysis set included all randomized patients who received at least one dose of study drug at baseline and had at least one HAMD-17 total score assessment after baseline. The analysis set for each protocol included all randomized patients who completed the study without major protocol deviations. Efficacy variables, including HAMD-17 total score using the last observation carried forward (LOCF) method, were analyzed primarily in the ITT set. The safety analysis set included all patients who received at least one dose of study drug. The continuous variables were described using the mean standard deviation (SD). For repeated measures, we used a mixed-effect model. The mixing procedure was used to provide an overall assessment of the effect of treatment group (GROUP), treatment time (TIME), and the interaction between GROUP and TIME. The comparison statement is used to compare the average levels of each variable between GROUP/TIME after controlling the impact of TIME/GROUP. Statistical analysis was performed using SPSS 21.0 (IBM Institute Inc).
Results
Subject Disposition, Baseline Demographics, and Clinical Characteristics
A total of 210 people met the inclusion criteria, 70 healthy controls and 140 patients with depression, 9 of whom refused to sign the informed consent form, and 131 MDD patients were finally enrolled. MDD patients were randomly divided into 2 groups, 62 in the Vortioxetine group and 69 in the Escitalopram group. After 2 weeks, 4 weeks, and 8 weeks of treatment, the numbers of patients in the Vortioxetine group were 55, 50, and 31, respectively, and the numbers in the Escitalopram group were 56, 50, and 47, respectively (Figure 1). The ITT analysis set included 55 patients in the Vortioxetine group and 56 in the Escitalopram group, and these populations were used for the analysis of efficacy-related measures. Due to the attrition rate and limited time points of cognitive assessment, the per-protocol (PP) analysis set were used in efficacy analysis and the comparison of Vortioxetine and Escitalopram between baseline and 8 weeks of MCCB, including 31 patients in the Vortioxetine group and 47 patients in the Escitalopram group who completed the entire study period. The safety analysis includes all 131 patients that underwent randomization.
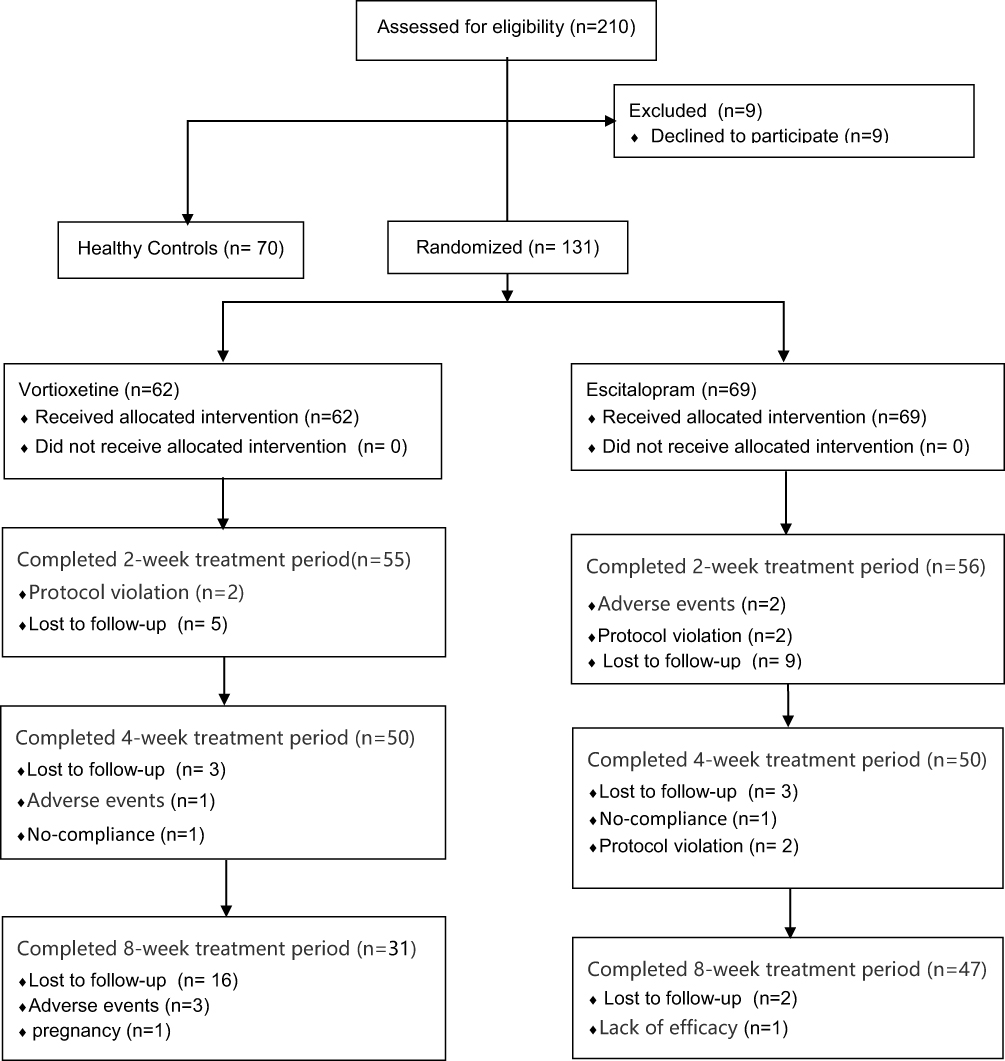 |
Figure 1 CONSORT diagram of participants through the trial. |
The demographic and clinical characteristics of MDD patients and healthy controls are shown in Table 1. There was no statistical difference in general information regarding age, gender and years of education, with all P > 0.05. There were statistically significant differences in the total scores of HAMD-17, HAMA and SHAPS scales between MDD cases and healthy controls (P <0.001). There were also differences in MCCB scores including Speed of Processing, Attention Vigilance, Working Memory, Verbal Learning, Visual Learning, Reasoning and Problem Solving, and Social Cognition between the two groups, with all P < 0.05. The demographic and clinical characteristics of patients in Vortioxetine and Escitalopram groups are also shown in Table 1. There was no statistical difference in characteristic information and the total scores of HAMD-17, HAMA, SHAPS and the other MCCB scales between two study groups, except that the scores of Working Memory in MCCB were significantly different, with P <0.01.
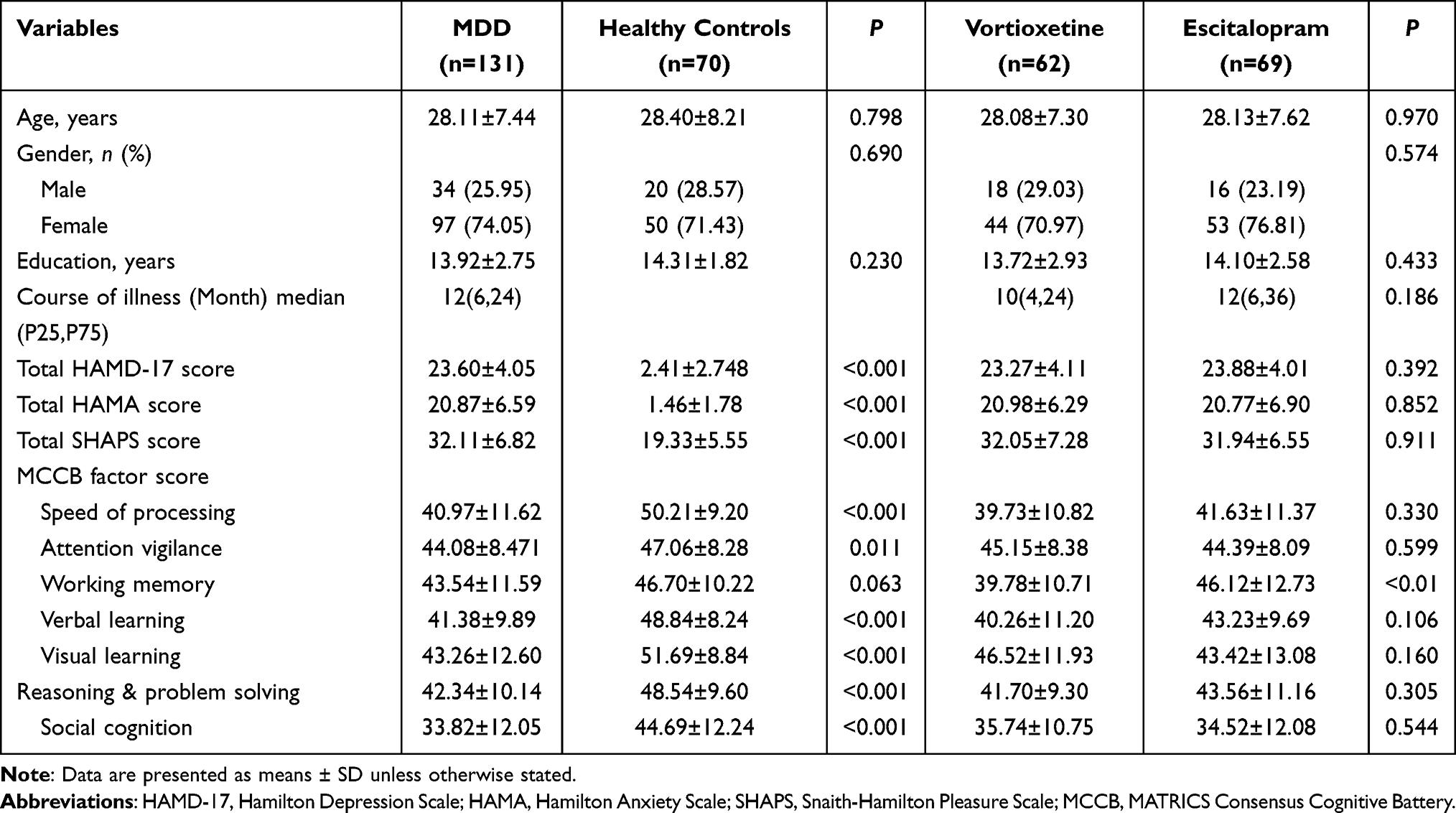 |
Table 1 Demographic and Clinical Characteristics of Comparison Groups at Baseline (Mean ± SD) |
Primary Outcome: Treatment Effect
The changes of the total HAMD-17, HAMA and SHAPS scores in the two groups were listed in Table 2. There was no statistical difference in the total scores of HAMD-17, HAMA and SHAPS between the Vortioxetine and Escitalopram groups at baseline, 2-, 4- and 8-week treatments, with all P > 0.05. In addition, we found that the total HAMD-17 (F = 209.638, P < 0.001), HAMA (F = 122.323, P < 0.001) and SHAPS (F = 13.907, P < 0.001) scores at different follow-up points were significantly different compared with baseline, and the mean scores of these scales gradually decreased over time after the use of antidepressants (Figure 2), but there was no difference between the scales of the two groups (P > 0.05). No interaction between drug and follow-up time was found in the three scales (P > 0.05). The results obtained by ITT and PP analysis methods were basically consistent as listed in Table 2 and Supplement Table 1.
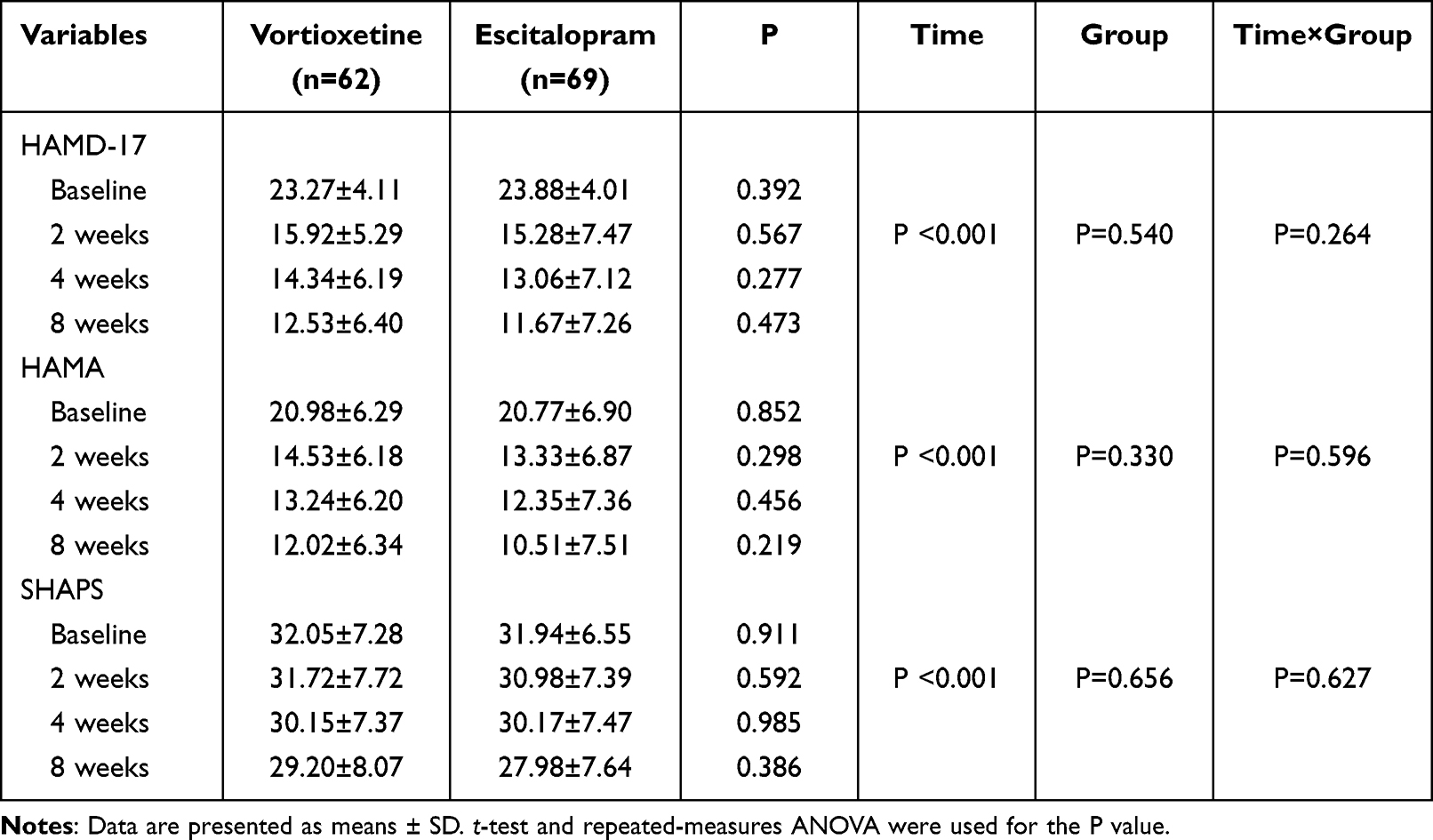 |
Table 2 Comparison of Clinical Scales at Baseline and After Treatment Using ITT Analysis |
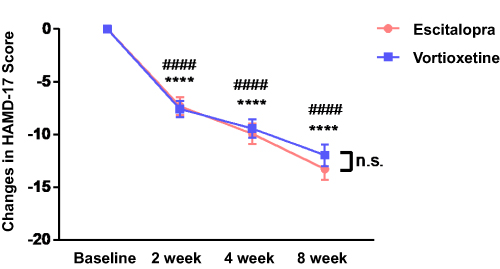 |
Figure 2 HAMD-17 scores were significantly improved after the 8 weeks use of Escitalopram and Vortioxetine. ####P < 0.0001 in Vortioxetine group. ****P < 0.0001 in Escitalopram group. n.s.P > 0.05. |
Cognitive Function Between the Two Groups
The changes of MCCB scores between the Vortioxetine and Escitalopram groups are listed in Table 3. The significant improvements of Attention Vigilance (45.15 vs 50.31), Speed of Processing (39.73 vs 47.65), Working Memory (39.78 vs 45.22), Verbal Learning (40.26 vs 47.19), and Reasoning and Problem Solving (41.70 vs 48.67) were discovered in the Vortioxetine group after the 8-week treatment (P1 < 0.05). Escitalopram had improved cognition regarding Speed of Processing (41.63 vs 48.77), Attention Vigilance (44.39 vs 47.84), Verbal Learning (43.23 vs 50.00), Visual Learning (43.42 vs 49.63) and Reasoning and Problem Solving (43.56 vs 49.07), with statistical differences (P2 < 0.05). Compared with before treatment, there were no differences in the scores of seven factors in MCCB between the two groups after 8 weeks of treatment, with all P3 > 0.05.
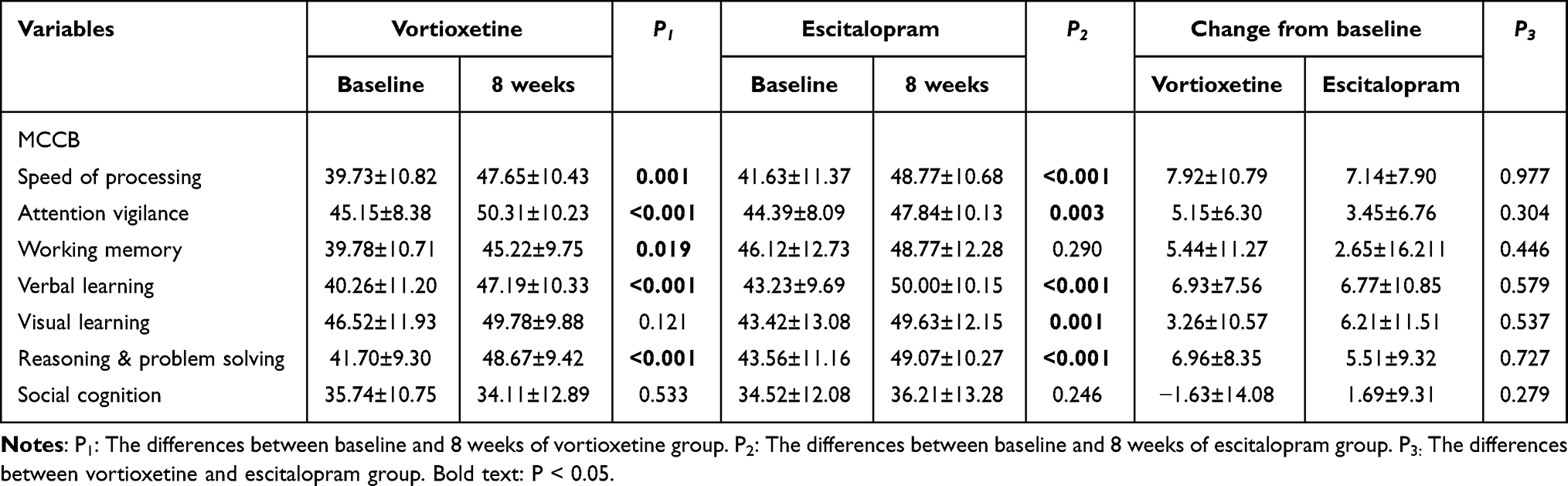 |
Table 3 Comparison of Vortioxetine and Escitalopram Between Baseline and 8 weeks of MCCB Using PP Analysis |
Safety Findings
The adverse reactions of MDD cases treated with Vortioxetine or Escitalopram within 8 weeks are shown in Table 4. There were 58 cases of treatment-emergent adverse events (TEAEs), 33 (53.2%) in the Vortioxetine group and 25 (36.2%) in the Escitalopram group. Most adverse events were mild or moderate, with nausea in 22 cases (35.5%) of Vortioxetine group and 13 (18.8%) of Escitalopram group being the most common adverse event. No deaths or serious adverse events occurred during the study.
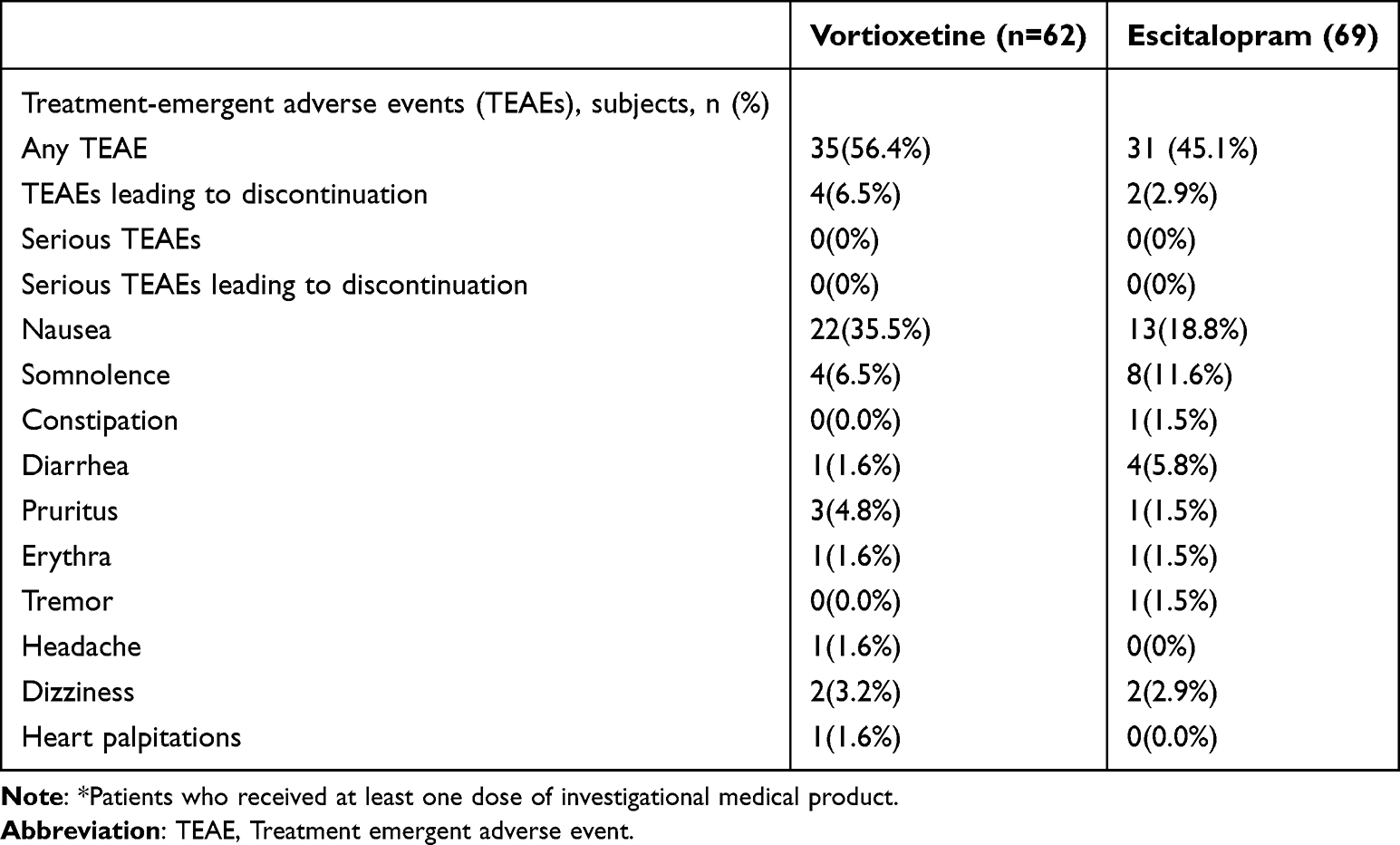 |
Table 4 Summary of TEAEs in the 8-Week Treatment Period (All Patients Treated*) |
Discussion
Vortioxetine was launched in China in 2017, and there are few relevant head-to-head comparative trials in China. In contrast, there are many clinical studies of Escitalopram in the treatment of MDD patients. The remission rate of Escitalopram in the treatment of MDD in China has reached 72.8% at week 8 in the intention-to-treat group.23 Escitalopram is the most recommended prescription antidepressant due to its high remission rate. In our study, after 8 weeks of treatment, there was no statistical difference in the efficacy between the Vortioxetine group and the Escitalopram group (Table 2). Our results reveal that the efficacy of Vortioxetine is essentially the same as that of Escitalopram in Chinese population. Considering the status of Escitalopram as one of the most widely used antidepressants, Vortioxetine, with a different mechanism of action, may be a promising option for patients who derive optimal benefit from first-line antidepressant therapy.
Cognitive dysfunction is increasingly recognized as an important symptom of MDD and an important dimension in antidepressant treatment. Research suggests that cognitive dysfunction in MDD includes psychomotor processing, declarative memory, working memory, executive functions, and attention.24,25 In previous clinical studies, cognitive assessment tools such as Digit Symbol Substitution Test (DSST), Wisconsin Card Sorting Test (WCST), Stroop Test, Rey Auditory Verbal Learning Test (RAVLT) and Trail Making Test (TMT) have been used.26 However, different tests have limitations in assessing cognitive function. Likewise, the various tools used in clinical trials can lead to heterogeneous results. In comparison, MCCB provides more multidimensional parameters and therefore is more closely related to the multiple symptoms of mental illness, which could assess the severity of the symptoms more comprehensively and serve as a potentially sensitive cognitive marker to identify the early pathological state changes of psychosis.27 Studies have showed that MCCB has been widely used to assess cognitive functions in clinical trials and shown stable internal consistency and reliability in Chinese patients with MDD of different ages.28–32
In our study, MDD patients showed cognitive impairments compared with healthy individuals, including: Speed of Processing, Attention Vigilance, Verbal Learning, Visual Learning, Reasoning and Problem Solving, and Social Cognition (Table 1). Previous review mentioned that in addition to common cognitive symptoms such as inattention and psychomotor slowdown, MDD also has response inhibition, cognitive flexibility, semantic verbal fluency, and executive function compared with healthy people.25 These cognitive impairments severely impact the prognosis and social function of patients.
Meanwhile, our study found that after 8 weeks of treatment, both Vortioxetine and Escitalopram could improve cognitive symptoms, but there was no statistical difference between the two antidepressants. Our results are similar to those published by Vieta E in 2018: at week 8, Digit Symbol Substitution Test (DSST) and the University of San Diego Performance-based Skills Assessment-Brief (UPSA-B) performance had improved in Vortioxetine group and Escitalopram group, with no statistically significant treatment difference.33 A study of a larger scale comparing the effects of antidepressants on cognitive function measured by DSST demonstrated that Vortioxetine was more efficacious than Escitalopram and other antidepressants.20
In terms of safety, the most common adverse event of the two drugs in our study was nausea, which was a mild-to-moderate reaction and was acceptable to patients. The incidence rate is similar to that of previous clinical studies at around 30%.17,34 The incidence of nausea was slightly higher with Vortioxetine than with Escitalopram, which was consistent with the results of Vieta E.33
Notably, cognitive dysfunction has been identified and emphasized in MDD patients and significantly contribute to social functional disabilities.35 In the treatment of MDD, multiple antidepressants could effectively improve the core symptoms, while the cognitive function impairment still lacks targeted management.36 Recent studies have shown that even with adequate treatment of conventional selective serotonin reuptake inhibitors (SSRIs), a significant proportion of MDD patients still have residual symptoms of cognitive function impairment,37,38 or even be negatively affected in terms of cognitive ability.39,40 In addition to the antidepressant effects, the multimodal antidepressants like Vortioxetine have an independent effect on improving cognition,41 thus to provide an overall improvement of patients’ symptoms and social functioning. Vortioxetine works as a 5-HT3, 5-HT7 and 5-HT1D receptor antagonist, a partial 5-HT1B receptor agonist, a 5-HT1A receptor agonist, and a 5-hydroxytryptamine transporter (SERT) inhibitor, combining the 5-HT reuptake inhibition with modulations of other key 5-HT receptors.42 Its blockage of the 5-HT3 receptors would improve the glutamatergic and serotoninergic transmission and also the firing of pyramidal neurons in prefrontal cortex, which plays a key role in the cognitive improvement.43 Likewise, it could block the 5-HT7 receptor prominently expressed in the limbic areas, which are the key brain regions associated with anhedonia, cognition dysfunction and many other symptoms.44 Besides, Vortioxetine has been shown to enhance cognition in MDD patients by affecting brain metabolites, including altering neurobiochemical metabolites levels in the frontal lobe-thalamus-cingulate gyrus loop.32 Therefore, Vortioxetine may have advantages in targeting cognitive dysfunction compared to traditional SSRIs. Although our study showed no significant difference between Vortioxetine and Escitalopram in improving cognitive function in MDD patients, it still needs to be studied and demonstrated in a larger population sample in the future. Clinical biochemical measures and pre-clinical studies are urgently required to further investigate mechanisms of Vortioxetine in cognition improvement.
It is worth mentioning that some promising drugs and neuromodulation technology have emerged, providing more actionable clinical recommendations for the treatment of MDD and other mental disorders. Novel pharmacological interventions, such as Ketamine/Esketamine and Psilocybin, have shown significant antidepressant effect and work faster compared with traditional antidepressants. Single or multiple infusions of Ketamine are both effective and safe in the treatment of MDD45 and multiple infusions of Ketamine show a long-lasting antidepressant effect.46 Esketamine provides an even more ultra-rapid and long-lasting antidepressant effect for MDD and its adjunctive intranasal administration brings convenience to the treatment mode.47 However, the remission rate of Esketamine might not be better than that of intravenous ketamine48 and the relatively high price limits the patient accessibility. Neither Ketamine nor Esketamine has showed cognition improvement independent of antidepressant effect30,46,49 or any significant difference between treatment-resistant depression (TRD) and non-TRD.48 The long-term therapeutic effect and safety of Ketamine/Esketamine and their benefits in combination with other antidepressants need further clarification in large-scale randomized clinical trials. Psilocybin also has a rapid onset of antidepressant effect50 similar to Ketamine/Esketamine, mainly improving the depression and anxiety symptoms in MDD.51,52 Psilocybin shows the ability to increase brain network integration globally which has not been observed in Escitalopram, implying the mechanism of its antidepressant action in TRD.53 On the other hand, adverse events and suicidal behaviour occurred more frequently with the use of Psilocybin.54 Larger and longer trials are required to determine the long-term efficacy, safety, and tolerability of Psilocybin in MDD. Neuromodulation technology using non-invasive physical stimulus, such as nonconvulsive electrotherapy (NET) and stanford neuromodulation therapy (SNT), has greatly enriched the treatment of MDD. The antidepressant efficacy of NET on depression is similar to that of electroconvulsive therapy (ECT) with significantly fewer neurocognitive impairments.55 Compared with the pharmacological treatments in MDD, NET has limited patient acceptance and shows no significant improvement in cognitive impairment, but works well as an effective treatment for TRD.56,57 In addition to the electrical stimulation, repetitive transcranial magnetic stimulation (rTMS) is also a clinically mature intervention for MDD. SNT is a faster and more efficient form of rTMS, enhancing antidepressant effect through acceleration, interval stimulation, higher total pulse doses and individualized targeting, and has greatly improved the response rate and remission rate of treatment for TRD, with barely any adverse events.58 Taken together, SNT may lead to better outcomes as a promising therapeutic innovation for patients who lack benefits from previous treatments. Future studies in this area should further investigate treatment parameters, widespread application in larger patient groups and clinical benefit of combination therapy.
Several explanations may account for our results that failed to replicate previous findings regarding cognitive symptom outcomes. First, a total of 131 MDD patients were recruited in this study with a relatively high attrition rate, as the small sample size could have affected the significance of the results. The possible reason is that people were prohibited from going out due to COVID-19. The medication was available in provincial capital cities but hardly accessible in small cities, thus many patients stopped taking Vortioxetine due to the difficulty in obtaining medicines, but Escitalopram is available in most hospitals, which made the dropout rate of the Escitalopram group in this study lower than the Vortioxetine group. Also, the price of Vortioxetine is much higher than that of Escitalopram, which may result in the higher dropout rate of Vortioxetine group. Second, we chose HAMD-17, HAMA and SHAPS to evaluate depressive symptoms and MCCB to evaluate the cognitive function of patients with MDD. The lack of significant differences between the two groups may be due to the low sensitivity of the selected scales. Third, the relatively short duration of eight-week treatment period might not fully reflect the long-term effects of symptoms and cognition improvement achieved by Vortioxetine and Escitalopram. The potential advantages long-term benefits of both medications could be further evaluated in prospective trials with a prolonged period. Meanwhile, sufficient biomarkers such as plasma factors, intestinal flora and magnetic resonance imaging were not included in this study, which could help detect possible pathological mechanisms of MDD and different pharmacological mechanisms of Vortioxetine and Escitalopram. We have also collected blood, feces, and functional magnetic resonance data, and will further analyze the biological mechanisms in the future.
Conclusions
Both Vortioxetine and Escitalopram can improve the mental status and cognitive functions in MDD patients, with mild or moderate adverse events. There is no significant difference in the efficacy and the cognitive function benefit between Vortioxetine and Escitalopram. Further verification in a large sample population is needed in the future. Some promising drugs, physical therapy and psychotherapy should be jointly explored as well in order to bring up more advanced clinical guidance.
Significant Outcomes
- Both Vortioxetine and Escitalopram can improve the mental status and cognitive function, with mild or moderate adverse events.
Limitations
- The small sample size and attrition rate could have affected the significance of the results.
- Long-term trials and widespread patients population are required to verificate the efficacy and cognition improvements of Vortioxetine and Escitalopram.
- More comprehensive parameters need to be introduced for clinical evaluation of Vortioxetine and Escitalopram.
Data Sharing Statement
The data that support the findings of this study are available on request from the corresponding author, Manli Huang, upon reasonable request.
Ethical Standards
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2008.
Funding
This research was supported by the National Natural Science Foundation of China (No. 82271562 to MH), the Key Research and Development Program of Zhejiang Province of China (No. 2023C03077 to MH).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: a cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
2. Ren X, Yu S, Dong W, Yin P, Xu X, Zhou M. Burden of depression in China, 1990–2017: findings from the global burden of disease study 2017. J Affect Disord. 2020;268:95–101. doi:10.1016/j.jad.2020.03.011
3. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905–1917. doi:10.1176/ajp.2006.163.11.1905
4. Saragoussi D, Touya M, Haro JM, et al. Factors associated with failure to achieve remission and with relapse after remission in patients with major depressive disorder in the PERFORM study. Neuropsychiatr Dis Treat. 2017;13:2151–2165. doi:10.2147/NDT.S136343
5. Sheehan DV, Harnett-Sheehan K, Spann ME, Thompson HF, Prakash A. Assessing remission in major depressive disorder and generalized anxiety disorder clinical trials with the discan metric of the Sheehan disability scale. Int Clin Psychopharmacol. 2011;26(2):75–83. doi:10.1097/YIC.0b013e328341bb5f
6. Shilyansky C, Williams LM, Gyurak A, Harris A, Usherwood T, Etkin A. Effect of antidepressant treatment on cognitive impairments associated with depression: a randomised longitudinal study. Lancet Psychiatry. 2016;3(5):425–435. doi:10.1016/S2215-0366(16)00012-2
7. Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
8. Wang X, Fan Y, Li G, Li H. The efficacy of escitalopram in major depressive disorder: a multicenter randomized, placebo-controlled double-blind study. Int Clin Psychopharmacol. 2021;36(3):133–139. doi:10.1097/YIC.0000000000000350
9. Prado CE, Watt S, Crowe SF. A meta-analysis of the effects of antidepressants on cognitive functioning in depressed and non-depressed samples. Neuropsychol Rev. 2018;28(1):32–72. doi:10.1007/s11065-018-9369-5
10. Sanchez C, Asin KE, Artigas F. Vortioxetine, a novel antidepressant with multimodal activity: review of preclinical and clinical data. Pharmacol Ther. 2015;145:43–57. doi:10.1016/j.pharmthera.2014.07.001
11. Betry C, Etievant A, Pehrson A, Sanchez C, Haddjeri N. Effect of the multimodal acting antidepressant vortioxetine on rat hippocampal plasticity and recognition memory. Prog Neuropsychopharmacol Biol Psychiatry. 2015;58:38–46. doi:10.1016/j.pnpbp.2014.12.002
12. Jin K, Zhang S, Jiang C, et al. The role of reelin in the pathological mechanism of depression from clinical to rodents. Psychiatry Res. 2022;317:114838. doi:10.1016/j.psychres.2022.114838
13. du Jardin KG, Jensen JB, Sanchez C, Pehrson AL. Vortioxetine dose-dependently reverses 5-HT depletion-induced deficits in spatial working and object recognition memory: a potential role for 5-HT1A receptor agonism and 5-HT3 receptor antagonism. Eur Neuropsychopharmacol. 2014;24(1):160–171. doi:10.1016/j.euroneuro.2013.07.001
14. Jensen JB, du Jardin KG, Song D, et al. Vortioxetine, but not escitalopram or duloxetine, reverses memory impairment induced by central 5-HT depletion in rats: evidence for direct 5-HT receptor modulation. Eur Neuropsychopharmacol. 2014;24(1):148–159. doi:10.1016/j.euroneuro.2013.10.011
15. Mahableshwarkar AR, Zajecka J, Jacobson W, Chen Y, Keefe RS. A randomized, placebo-controlled, active-reference, double-blind, flexible-dose study of the efficacy of vortioxetine on cognitive function in major depressive disorder. Neuropsychopharmacology. 2016;41(12):2961. doi:10.1038/npp.2016.181
16. Mahableshwarkar AR, Jacobsen PL, Serenko M, Chen Y, Trivedi MH. A randomized, double-blind, placebo-controlled study of the efficacy and safety of 2 doses of vortioxetine in adults with major depressive disorder. J Clin Psychiatry. 2015;76(5):583–591. doi:10.4088/JCP.14m09337
17. Mahableshwarkar AR, Jacobsen PL, Chen Y, Serenko M, Trivedi MH. A randomized, double-blind, duloxetine-referenced study comparing efficacy and tolerability of 2 fixed doses of vortioxetine in the acute treatment of adults with MDD. Psychopharmacology. 2015;232(12):2061–2070. doi:10.1007/s00213-014-3839-0
18. Jain R, Mahableshwarkar AR, Jacobsen PL, Chen Y, Thase ME. A randomized, double-blind, placebo-controlled 6-wk trial of the efficacy and tolerability of 5 mg vortioxetine in adults with major depressive disorder. Int J Neuropsychopharmacol. 2013;16(2):313–321. doi:10.1017/S1461145712000727
19. Wang G, Xiao L, Ren H, et al. Effectiveness and safety of vortioxetine for major depressive disorder in real-world clinical practice: results from the single-arm RELIEVE China study. Neuropsychiatr Dis Treat. 2022;18:1939–1950. doi:10.2147/NDT.S358253
20. Baune BT, Brignone M, Larsen KG. A network meta-analysis comparing effects of various antidepressant classes on the Digit Symbol Substitution Test (DSST) as a measure of cognitive dysfunction in patients with major depressive disorder. Int J Neuropsychopharmacol. 2018;21(2):97–107. doi:10.1093/ijnp/pyx070
21. Inoue T, Sasai K, Kitagawa T, Nishimura A. Inada I: randomized, double-blind, placebo-controlled study to assess the efficacy and safety of vortioxetine in Japanese patients with major depressive disorder. Psychiatry Clin Neurosci. 2020;74(2):140–148. doi:10.1111/pcn.12956
22. Nuechterlein KH, Green MF, Kern RS, et al. The MATRICS consensus cognitive battery, part 1: test selection, reliability, and validity. Am J Psychiatry. 2008;165(2):203–213. doi:10.1176/appi.ajp.2007.07010042
23. Si T, Wang G, Yang F, et al. Efficacy and safety of escitalopram in treatment of severe depression in Chinese population. Metab Brain Dis. 2017;32(3):891–901. doi:10.1007/s11011-017-9992-5
24. Beblo T, Sinnamon G, Baune BT. Specifying the neuropsychology of affective disorders: clinical, demographic and neurobiological factors. Neuropsychol Rev. 2011;21(4):337–359. doi:10.1007/s11065-011-9171-0
25. Papakostas GI. Cognitive symptoms in patients with major depressive disorder and their implications for clinical practice. J Clin Psychiatry. 2014;75(1):8–14. doi:10.4088/JCP.13r08710
26. Lim J, Oh IK, Han C, et al. Sensitivity of cognitive tests in four cognitive domains in discriminating MDD patients from healthy controls: a meta-analysis. Int Psychogeriatr. 2013;25(9):1543–1557. doi:10.1017/S1041610213000689
27. Ding Y, Hou W, Wang C, et al. Longitudinal changes in cognitive function in early psychosis: a meta-analysis with the MATRICS consensus cognitive battery (MCCB). Schizophr Res. 2024;270:349–357. doi:10.1016/j.schres.2024.06.048
28. Liang S, Yu W, Ma X, et al. Psychometric properties of the MATRICS Consensus Cognitive Battery (MCCB) in Chinese patients with major depressive disorder. J Affect Disord. 2020;265:132–138. doi:10.1016/j.jad.2020.01.052
29. Lai S, Zhong S, Wang Y, et al. The prevalence and characteristics of MCCB cognitive impairment in unmedicated patients with bipolar II depression and major depressive disorder. J Affect Disord. 2022;310:369–376. doi:10.1016/j.jad.2022.04.153
30. Lan X, Wang C, Zhang F, et al. Short-term cognitive effects of repeated-dose esketamine in adolescents with major depressive disorder and suicidal ideation: a randomized controlled trial. Child Adolesc Psychiatry Ment Health. 2023;17(1):108. doi:10.1186/s13034-023-00647-2
31. Wang Y, Li J, Bian W, et al. Latent classes of symptom trajectories among major depressive disorder patients in China. J Affect Disord. 2024;350:746–754. doi:10.1016/j.jad.2024.01.144
32. Zhang Y, Lai S, Zhang J, et al. The effectiveness of vortioxetine on neurobiochemical metabolites and cognitive of major depressive disorders patients: a 8-week follow-up study. J Affect Disord. 2024;351:799–807. doi:10.1016/j.jad.2024.01.272
33. Vieta E, Sluth LB, Olsen CK. The effects of vortioxetine on cognitive dysfunction in patients with inadequate response to current antidepressants in major depressive disorder: a short-term, randomized, double-blind, exploratory study versus escitalopram. J Affect Disord. 2018;227:803–809. doi:10.1016/j.jad.2017.11.053
34. Alvarez E, Perez V, Dragheim M, Loft H, Artigas F. A double-blind, randomized, placebo-controlled, active reference study of Lu AA21004 in patients with major depressive disorder. Int J Neuropsychopharmacol. 2012;15(5):589–600. doi:10.1017/S1461145711001027
35. Pan Z, Park C, Brietzke E, et al. Cognitive impairment in major depressive disorder. CNS Spectr. 2019;24(1):22–29. doi:10.1017/S1092852918001207
36. Bortolato B, Miskowiak KW, Köhler CA, et al. Cognitive remission: a novel objective for the treatment of major depression? BMC Med. 2016;14:9. doi:10.1186/s12916-016-0560-3
37. Myklebost SB, Gjestad R, Inal Y, Hammar Å, Nordgreen T. Predictors of treatment response to an internet-delivered intervention targeting residual cognitive symptoms after major depressive disorder. Front Psychiatry. 2022;13:795698. doi:10.3389/fpsyt.2022.795698
38. Iancu SC, Wong YM, Rhebergen D, van Balkom AJLM, Batelaan NM. Long-term disability in major depressive disorder: a 6-year follow-up study. Psychol Med. 2020;50(10):1644–1652. doi:10.1017/S0033291719001612
39. Knight MJ, Baune BT. Cognitive dysfunction in major depressive disorder. Curr Opin Psychiatry. 2018;31(1):26–31. doi:10.1097/YCO.0000000000000378
40. MacQueen GM, Memedovich KA. Cognitive dysfunction in major depression and bipolar disorder: assessment and treatment options. Psychiatry Clin Neurosci. 2017;71(1):18–27. doi:10.1111/pcn.12463
41. Frampton JE. Vortioxetine: a review in cognitive dysfunction in depression. Drugs. 2016;76(17):1675–1682. doi:10.1007/s40265-016-0655-3
42. De Diego-Adeliño J, Crespo JM, Mora F, et al. Vortioxetine in major depressive disorder: from mechanisms of action to clinical studies. An updated review. Expert Opin Drug Saf. 2022;21(5):673–690. doi:10.1080/14740338.2022.2019705
43. Pehrson AL, Sanchez C. Serotonergic modulation of glutamate neurotransmission as a strategy for treating depression and cognitive dysfunction. CNS Spectr. 2014;19(2):121–133. doi:10.1017/S1092852913000540
44. Okada M, Matsumoto R, Yamamoto Y, Fukuyama K. Effects of subchronic administrations of vortioxetine, lurasidone, and escitalopram on thalamocortical glutamatergic transmission associated with serotonin 5-HT7 receptor. Int J Mol Sci. 2021;22(3). doi:10.3390/ijms22031351
45. Zheng W, Zhou Y-L, Liu W-J, et al. Rapid and longer-term antidepressant effects of repeated-dose intravenous ketamine for patients with unipolar and bipolar depression. J Psychiatr Res. 2018;106:61–68. doi:10.1016/j.jpsychires.2018.09.013
46. Zhou Y, Zheng W, Liu W, et al. Neurocognitive effects of six ketamine infusions and the association with antidepressant response in patients with unipolar and bipolar depression. J Psychopharmacol. 2018;32(10):1118–1126. doi:10.1177/0269881118798614
47. Zheng W, Cai D-B, Xiang Y-Q, et al. Adjunctive intranasal esketamine for major depressive disorder: a systematic review of randomized double-blind controlled-placebo studies. J Affect Disord. 2020;265:63–70. doi:10.1016/j.jad.2020.01.002
48. Bahji A, Vazquez GH, Zarate CA. Comparative efficacy of racemic ketamine and esketamine for depression: a systematic review and meta-analysis. J Affect Disord. 2021;278:542–555. doi:10.1016/j.jad.2020.09.071
49. Zheng W, Zhou Y-L, Liu W-J, et al. Neurocognitive performance and repeated-dose intravenous ketamine in major depressive disorder. J Affect Disord. 2019;246:241–247. doi:10.1016/j.jad.2018.12.005
50. von Rotz R, Schindowski EM, Jungwirth J, et al. Single-dose psilocybin-assisted therapy in major depressive disorder: a placebo-controlled, double-blind, randomised clinical trial. EClinicalMedicine. 2023;56:101809. doi:10.1016/j.eclinm.2022.101809
51. Wang S-M, Kim S, Choi W-S, et al. Current understanding on psilocybin for major depressive disorder: a review focusing on clinical trials. Clin Psychopharmacol Neurosci. 2024;22(2):222–231. doi:10.9758/cpn.23.1134
52. Li L-J, Mo Y, Shi Z-M, et al. Psilocybin for major depressive disorder: a systematic review of randomized controlled studies. Front Psychiatry. 2024;15:1416420. doi:10.3389/fpsyt.2024.1416420
53. Daws RE, Timmermann C, Giribaldi B, et al. Increased global integration in the brain after psilocybin therapy for depression. Nat Med. 2022;28(4):844–851. doi:10.1038/s41591-022-01744-z
54. Goodwin GM, Aaronson ST, Alvarez O, et al. Single-dose psilocybin for a treatment-resistant episode of major depression. N Engl J Med. 2022;387(18):1637–1648. doi:10.1056/NEJMoa2206443
55. Cai D-B, Zhou H-R, Liang W-N, et al. Adjunctive nonconvulsive electrotherapy for patients with depression: a systematic review. Psychiatr Q. 2021;92(4):1645–1656. doi:10.1007/s11126-021-09936-5
56. Zhang M, Wei X, Li S-Y, et al. Sex differences in the antidepressant and neurocognitive effects of nonconvulsive electrotherapy in patients with treatment-refractory depression. Alpha Psychiatry. 2024;25(1):68–74. doi:10.5152/alphapsychiatry.2024.231402
57. Zheng W, Jiang M-L, He H-B, et al. A preliminary study of adjunctive nonconvulsive electrotherapy for treatment-refractory depression. Psychiatr Q. 2021;92(1):311–320. doi:10.1007/s11126-020-09798-3
58. Lan X-J, Cai D-B, Liu Q-M, et al. Stanford neuromodulation therapy for treatment-resistant depression: a systematic review. Front Psychiatry. 2023;14:1290364. doi:10.3389/fpsyt.2023.1290364
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice in Italy: Results from the RELIEVE Study
De Filippis S, Pugliese A, Christensen MC, Rosso G, Di Nicola M, Simonsen K, Ren H
Neuropsychiatric Disease and Treatment 2022, 18:1665-1677
Published Date: 9 August 2022
Effectiveness and Safety of Vortioxetine for Major Depressive Disorder in Real-World Clinical Practice: Results from the Single-Arm RELIEVE China Study
Wang G, Xiao L, Ren H, Simonsen K, Ma J, Xu X, Guo P, Wang Z, Bai L, Heldbo Reines E, Hammer-Helmich L
Neuropsychiatric Disease and Treatment 2022, 18:1939-1950
Published Date: 30 August 2022
Effectiveness of Vortioxetine in Patients with Major Depressive Disorder in Real-World Clinical Practice: French Cohort Results from the Global RELIEVE Study
Polosan M, Rabbani M, Christensen MC, Simonsen K, Ren H
Neuropsychiatric Disease and Treatment 2022, 18:1963-1974
Published Date: 31 August 2022
Assessing Reliability and Validity of the Oxford Depression Questionnaire (ODQ) in a Japanese Clinical Population
Kato M, Kikuchi T, Watanabe K, Sumiyoshi T, Moriguchi Y, Åström DO, Christensen MC
Neuropsychiatric Disease and Treatment 2023, 19:2401-2412
Published Date: 8 November 2023
Goal Attainment Scaling for Depression: Validation of the Japanese GAS-D Tool in Patients with Major Depressive Disorder
Kato M, Kikuchi T, Watanabe K, Sumiyoshi T, Moriguchi Y, Oudin Åström D, Christensen MC
Neuropsychiatric Disease and Treatment 2024, 20:49-60
Published Date: 16 January 2024