")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
A Study on the Current Situation of Stigma and Its Influencing Factors Among Chinese Patients with Port-Wine Stains
Authors Ran X, Yang X, Lin X, Yu W, Shang Y, Liang J, Shen L
Received 23 December 2024
Accepted for publication 30 April 2025
Published 26 May 2025 Volume 2025:18 Pages 1297—1308
DOI https://doi.org/10.2147/CCID.S513914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Xuehui Ran,1 Xia Yang,1 Xiaoxi Lin,2 Wenxin Yu,2 Ying Shang,3 Junyan Liang,3 Lingyue Shen1,3
1Department of Oral Maxillofacial Surgery, Shanghai Jiao Tong University School of Medicine Affiliated Ninth People’s Hospital, Shanghai, People’s Republic of China; 2Department of Plastic and Reconstructive Surgery, Shanghai Jiao Tong University School of Medicine Affiliated Ninth People’s Hospital, Shanghai, People’s Republic of China; 3Department of Laser and Aesthetic Medicine, Shanghai Jiao Tong University School of Medicine Affiliated Ninth People’s Hospital, Shanghai, People’s Republic of China
Correspondence: Lingyue Shen, Email [email protected] Junyan Liang, Email [email protected]
Background: Port-wine stains (PWS) are obvious skin lesions, most commonly located on the face and neck, which may lead to varying degrees of stigma in patients. In Chinese culture, where facial appearance is strongly tied to social identity, the stigma associated with PWS may be particularly intense. However, there is no study which examined stigma among Chinese patients with PWS yet.
Objective: This study aims to preliminarily investigate the stigma experienced by Chinese patients with facial and cervical PWS and analyze potential contributing factors.
Methods: This post-test-only one-group study included 113 adult PWS patients from Aug to Dec 2022 at Shanghai Ninth People’s Hospital. Excluding those with severe psychiatric or cognitive issues. Participants completed demographic, SSCI, SIS, and SES questionnaires. Without a control group or pre-test data, the study reflects real-world clinical settings and patient perceptions post-treatment.
Results: Statistical analyses included univariate and multiple linear regression, with Pearson correlations assessing links between stigma and self-esteem. PWS patients’ SSCI, SIS, and SES scores were 50.61± 22.2, 48.71± 15.17, and 24.75± 4.92. PWS size and income were associated with stigma; income and absence from school/work with self-esteem (P < 0.05). In multivariate analysis, only treatment number and PWS type remained significant (P < 0.05). All SSCI dimensions and SIS scores were significantly correlated with self-esteem (P < 0.01).
Conclusion: Chinese patients with port-wine stains (PWS) generally experience high levels of stigma and low levels of self-esteem. This study found that the factors influencing stigma among Chinese patients include the type of lesion (flat/thickened) and the number of treatments; an increase in the number of treatments may help alleviate patients’ feelings of stigma. The results suggest that clinical practice should emphasize patients’ emotional experiences and explore comprehensive intervention strategies to promote their mental health.
Keywords: port-wine stain, stigma, self-esteem, Chinese patients
Introduction
Port-wine stain (PWS) is a congenital capillary malformation that primarily affects the skin of the head and neck.1 Present in approximately 0.3% of newborns, PWS lesions initially appear as pink-red patches, which darken with age, potentially developing into elevated nodules prone to spontaneous bleeding.2 While PWS lesions can manifest anywhere on the body, they are most common and impactful in facial and cervical region due to their visibility and potential functional complications.
Patients with PWS often experience elevated emotional stress, as these skin lesions are associated with impaired attractiveness and social discomfort, which can negatively impact their social interactions and self-perception3. Studies have shown that individuals with PWS may face social stigma, with participants reporting concerns about unwanted attention, including staring and teasing, which, for some, may even hinder their ability to form romantic relationships.4
While medical treatments such as laser therapy can reduce the visibility of PWS lesions, their emotional impact persists, although patients report a reduced worry about their appearance after treatment and a moderate level of satisfaction with the results.5 This is partly because the standard treatment—pulse dye laser (PDL) therapy—offers limited clearance, with only about 21% of patients achieving complete lesion removal even after multiple treatments.6
Psychological studies have shown that individuals with visible skin conditions, like PWS, often struggle with issues of self-worth, anxiety, and depression, which can adversely affect their overall quality of life.7 The earlier research by M. A. M. van der Horst et al indicates that PWS has a negative impact on the mental health of adolescents and adults.8 The study population consists of patients from Amsterdam. The authors analyze how PWS affects mental health through social and cultural backgrounds as well as patients’ social needs, suggesting that different social and cultural contexts may lead to varying degrees of stigma associated with PWS.
Cultural factors play a crucial role in shaping the psychosocial impact of PWS. In Chinese society, where physical appearance can heavily influence social and professional interactions, patients with facial PWS may face unique challenges that differ from those in Western contexts. However, the specific impact of PWS on Chinese patients’ stigma has not been well-documented, highlighting a gap in the literature. Addressing this gap, this study aims to explore the psychosocial impact of facial and neck PWS on Chinese patients, examining factors such as social stigma, economic impact, and self-esteem.
Materials and Methods
This study employed a cross-sectional observational design to assess the impact of PWS on psychological state in Chinese patients with lesions on the face and/or neck. The study was a post-test-only one-group design, conducted from August 2022 to December 2022 at the Ninth People’s Hospital Affiliated with Shanghai Jiao Tong University, School of Medicine. Patients with PWS were examined by dermatology and laser aesthetics specialists at our institution to rule out other skin conditions. A total of 122 patients were selected using convenience sampling from those receiving PDL treatment at the hospital during the study period. The inclusion criteria were as follows: (1) Chinese patients with PWS located on the face and/or neck; (2) Age ≥ 18 years old; (3) Educational level of junior high school or above; (4) Ability to independently read and respond to survey questions; (5) Willing to participate in this study.
The exclusion criteria included the presence of severe systemic disease (like systemic lupus erythematosus, heart disease), other skin disorders (like vitiligo, hemangioma), previous mental illness, or any conditions that would impair understanding of the questionnaires.
Participants completed a comprehensive sociodemographic questionnaire capturing information on gender, age, educational attainment, residential status, geographical location, employment status, and monthly income. Disease characteristics such as PWS location, size, thickness, and the number of previous treatments were also documented.
Each patient completed the validated Chinese version of the Stigma Scale for Chronic Illness (SSCI), Social Impact Scale (SIS) and the Self-Esteem Scale (SES) via a networked questionnaire on their smartphone, ensuring a consistent and accessible data collection method.
SSCI: This scale includes 24 items scored on a 5-point Likert scale, with 13 items assessing intrinsic stigma and 11 items measuring extrinsic stigma. The five options of the scale were as follows: 1 point = no, 2 points = very few, 3 points = sometimes, 4 points = frequently, 5 points = always. Scores range from 24 to 120, with higher scores indicating greater perceived stigma.9 The Chinese version has been confirmed to have good reliability and validity among stroke patients in China (Deng et al, 2017).10
SIS: Comprising 24 items across four dimensions (social isolation, internal shame, social exclusion, and economic insecurity), this scale uses a 4-point Likert scoring system, with total scores ranging from 24 to 96. Higher scores reflect greater social impact due to the condition, with an internal consistency reliability (Cronbach’s α) between 0.852 and 0.903.11
SES: This scale consists of 10 items scored on a 4-point Likert scale, with positive and reverse-scored items. The total score ranges from 10 to 40, where scores between 10 and 25 indicate low self-esteem, 26 to 32 indicate moderate self-esteem, and 33 to 40 indicate high self-esteem.12,13
This study was approved by the Ethics Committee of Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine (Approval Number: SH9H-2021-T36-2). Written informed consent was obtained from each participant prior to their enrollment in the study. All procedures were conducted in accordance with the ethical principles outlined in the Declaration of Helsinki. While this design allows for preliminary exploration of associations between treatment and outcomes, the absence of a control group limits causal inference and increases the risk of confounding variables.
Statistical Analysis
Statistical analyses were performed using SPSS 25.0 software. Normally distributed data were presented as means ( ) ± standard deviations (SD), while categorical data were summarized as frequencies and percentages (%). One-way ANOVA was conducted to compare the differences in stigma and self-esteem scores across demographic groups, with Tukey’s post hoc test applied for pairwise comparisons when significant. Additionally, independent samples t-tests, χ2 tests, and Pearson’s correlation analysis were applied to explore relationships between variables. Multiple linear regression was used to analyze the possible influencing factors of SSCI, SIS, and SES. A P < 0.05 was considered statistically significant.
) ± standard deviations (SD), while categorical data were summarized as frequencies and percentages (%). One-way ANOVA was conducted to compare the differences in stigma and self-esteem scores across demographic groups, with Tukey’s post hoc test applied for pairwise comparisons when significant. Additionally, independent samples t-tests, χ2 tests, and Pearson’s correlation analysis were applied to explore relationships between variables. Multiple linear regression was used to analyze the possible influencing factors of SSCI, SIS, and SES. A P < 0.05 was considered statistically significant.
Results
Demographic Characteristics
A total of 122 questionnaires were collected, of which 113 met the inclusion criteria, resulting in an effective rate of 92.6%. Among these 113 patients, 78 (69.03%) were females, and 35 (30.97%) were males, all aged 18 years or older. Detailed demographic characteristics were provided in Table 1.
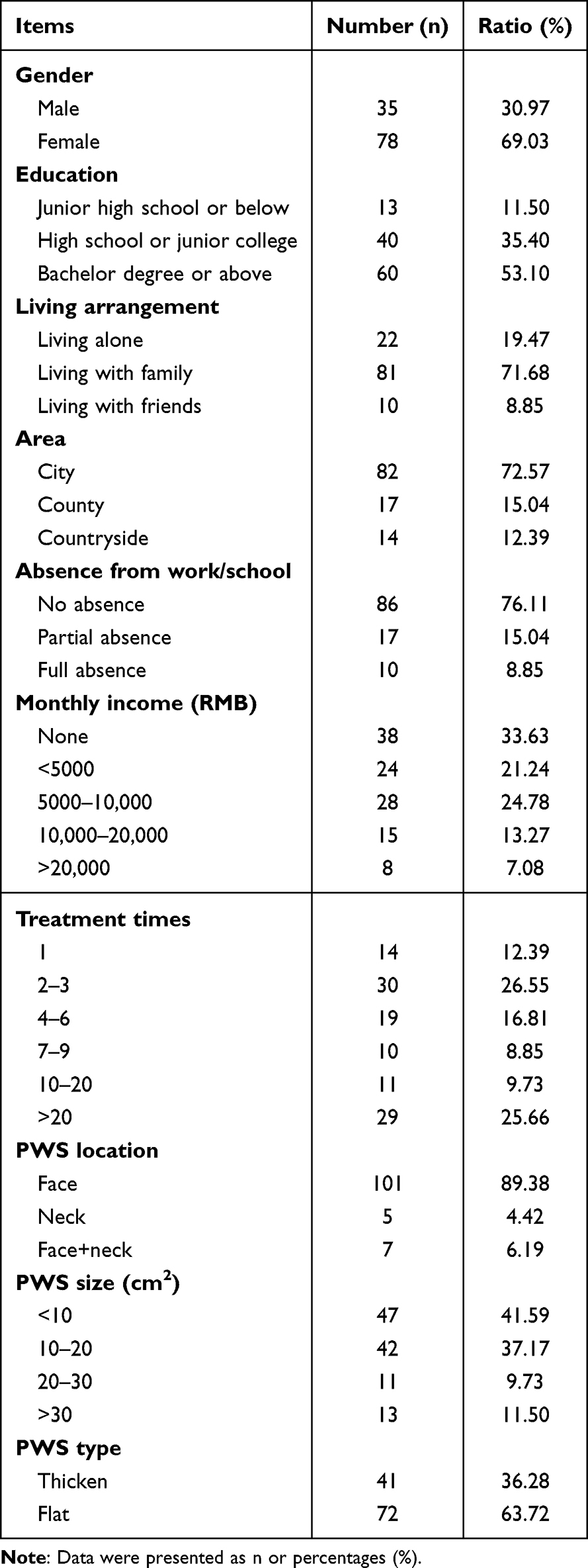 |
Table 1 Demographic Characteristics of PWS Patients |
Stigma Scale for Chronic Illness (SSCI) Scores and Influencing Factors
The reliability of the scale had been tested, and the Cronbach’s alpha was 0.974, indicating good internal consistency of the scale. To examine the construct validity of the scale, the Kaiser-Meyer-Olkin (KMO) measure and Bartlett’s test of sphericity were conducted. The KMO value was 0.941, Bartlett’s test of sphericity was significant (χ² = 2926, df = 276, p < 0.001), supporting the adequacy of the correlation matrix for factor extraction. These results confirmed the suitability of the data for further exploratory factor analysis.
The mean SSCI total score for the study population was 50.61±22.20, indicating a moderate to high level of stigma experienced by PWS patients. The intrinsic stigma subscore averaged 29.32±12.93, while the extrinsic stigma subscore was 21.29±10.22. The items with the highest score included concerns about social embarrassment and fear of others’ reactions, while the lowest score pertained to daily functional impacts (Table 2).
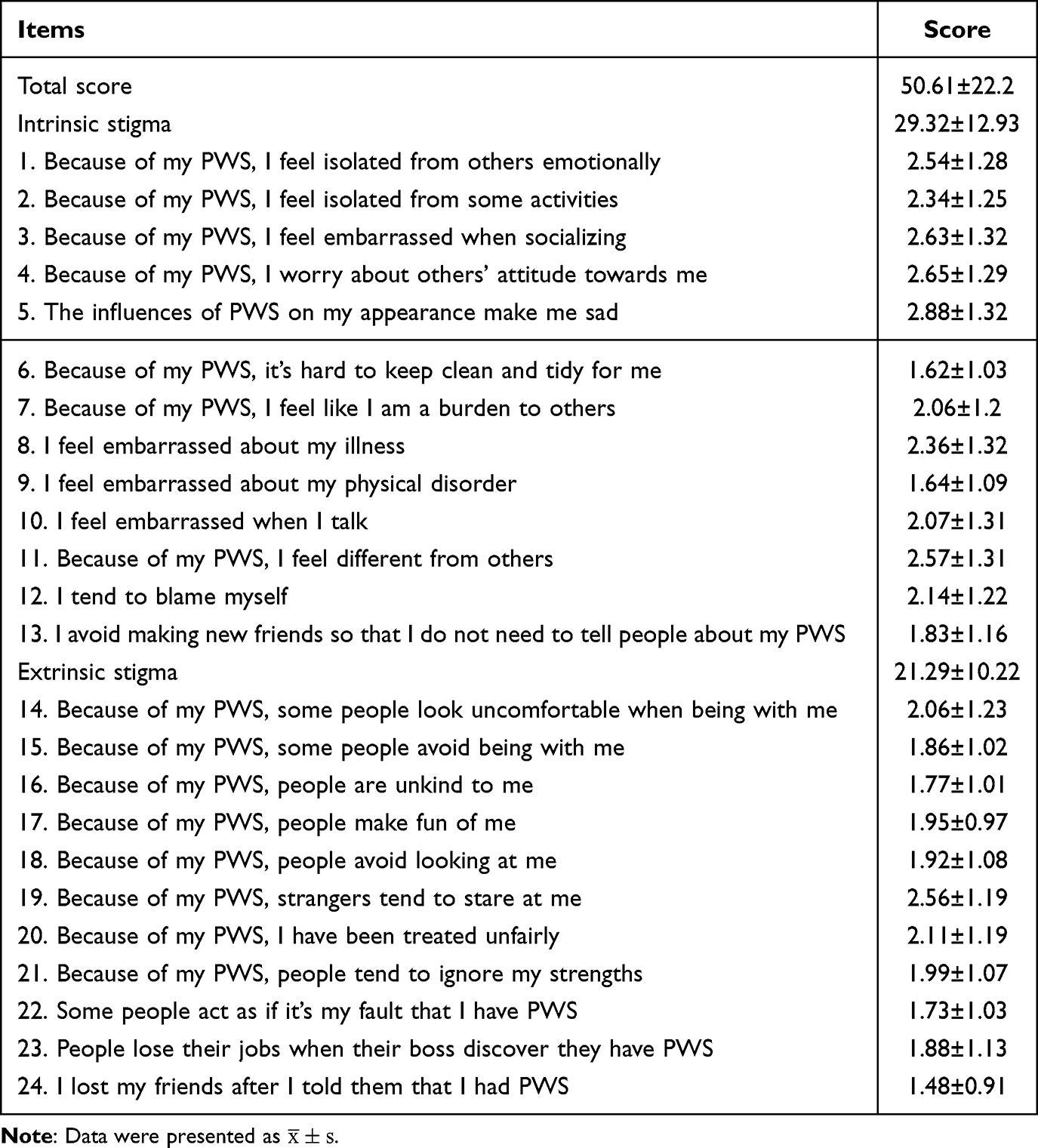 |
Table 2 Scores of Chronic Illness Stigma Dimensions in PWS Patients |
Univariate analysis revealed that monthly income and PWS lesion size were significantly associated with SSCI score (P < 0.05). Patients with lower income and larger lesion sizes reported higher levels of perceived stigma (Table 3). However, these relationships were not sustained in multivariate models (Table 4), suggesting potential confounding factors influencing the observed associations.
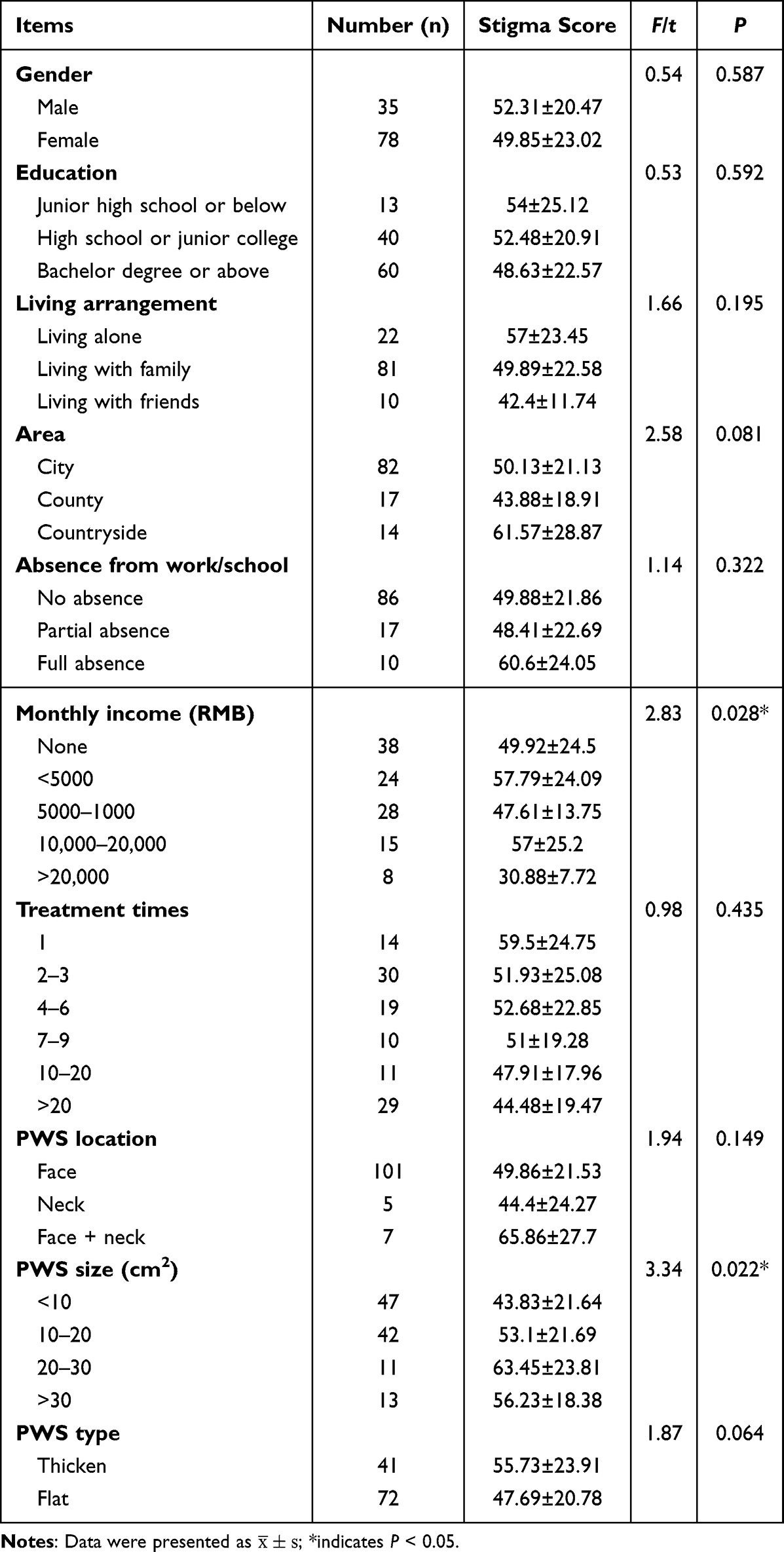 |
Table 3 Single Factor Analysis of Demographic Data on Chronic Disease Stigma |
 |
Table 4 Multiple Linear Regression Results for SSCI Scores in PWS Patients |
Social Impact Scale (SIS) Scores and Influencing Factors
The reliability of the SIS scale had been tested, and the Cronbach’s alpha was 0.971, indicating good internal consistency of the scale. The KMO value was 0.937, Bartlett’s test of sphericity was significant (χ² = 2837, df = 276, p < 0.001). The mean SIS score was 48.71±15.17, with the highest subscore for social rejection (17.46±5.66) and the lowest for financial insecurity (6.89±2.43). This indicated that PWS patients frequently faced social rejection but experienced less economic impact (Table 5).
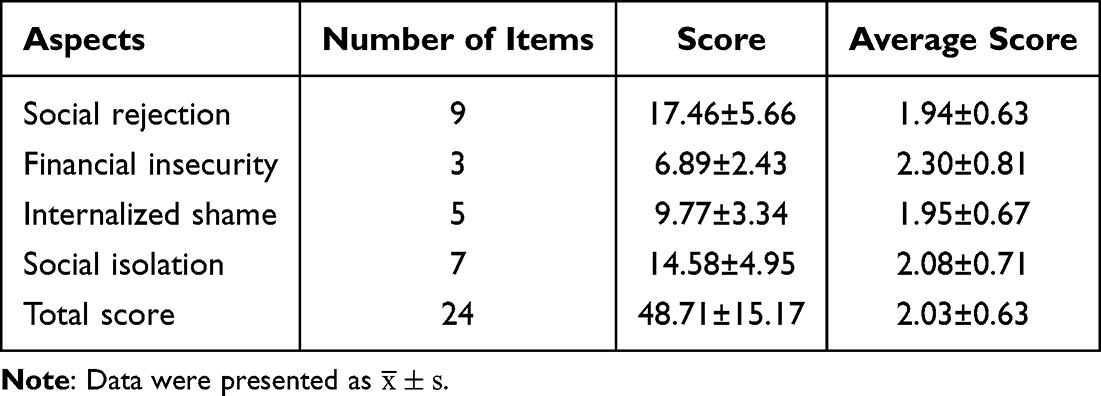 |
Table 5 Subscale Scores of SIS in PWS Patients |
Significant differences in SIS scores were observed across education level, monthly income, number of of treatment sessions, location of PWS, and lesion size of PWS (P < 0.05). For example, patients with lower educational attainment had higher scores in the “financial insecurity” dimension, while those with larger lesion sizes scored higher in “social rejection”. These results underscored the role of demographic and clinical characteristics in shaping the social impact of PWS (Table 6). Although univariate analysis identified several sociodemographic and clinical factors associated with SIS scores, these associations were not retained in multivariable models. This suggests possible intercorrelations among predictors and highlights the potential influence of unmeasured psychosocial confounders.
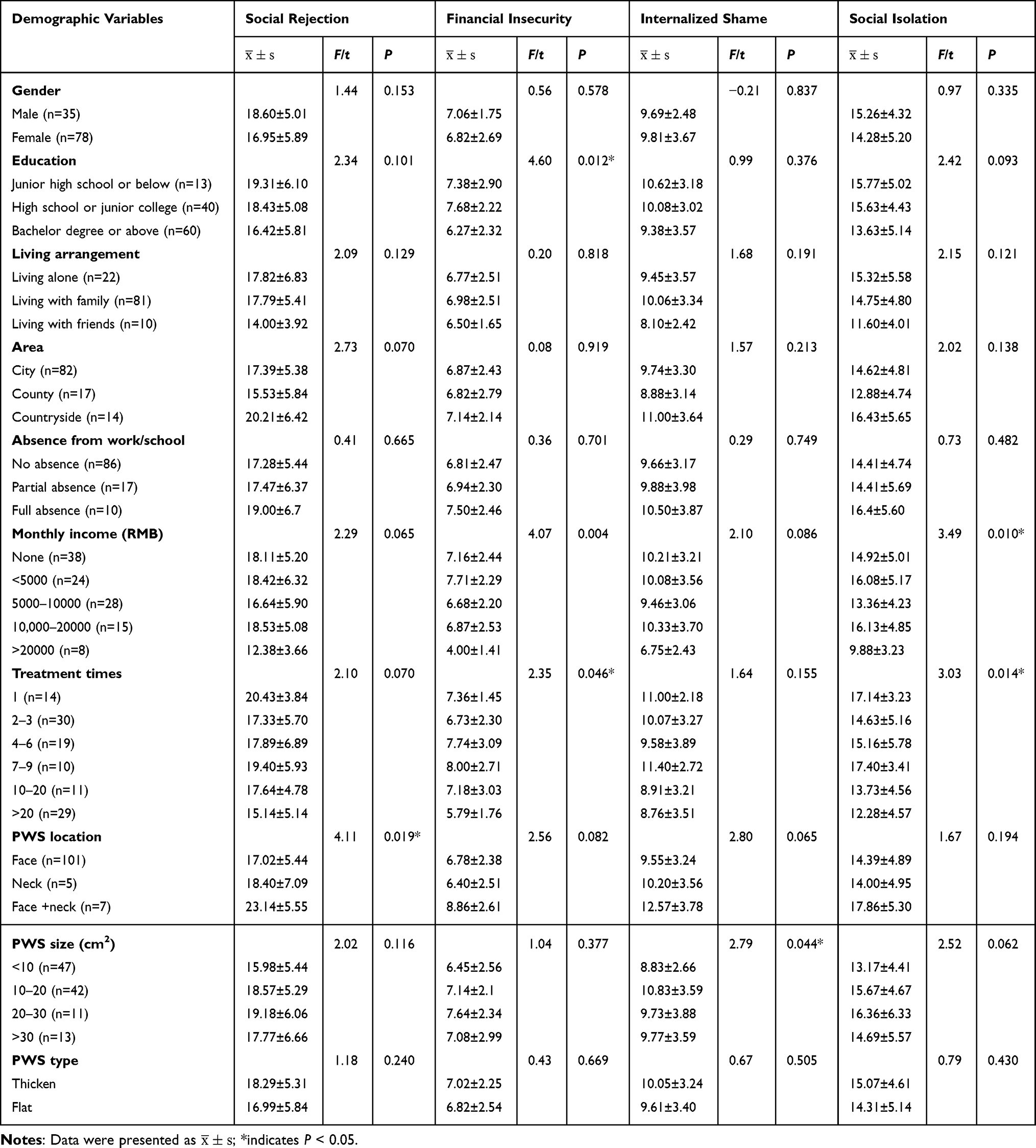 |
Table 6 Comparison of Demographic Variables Across SIS Dimensions in PWS Patients |
Self-Esteem Scale (SES) Scores
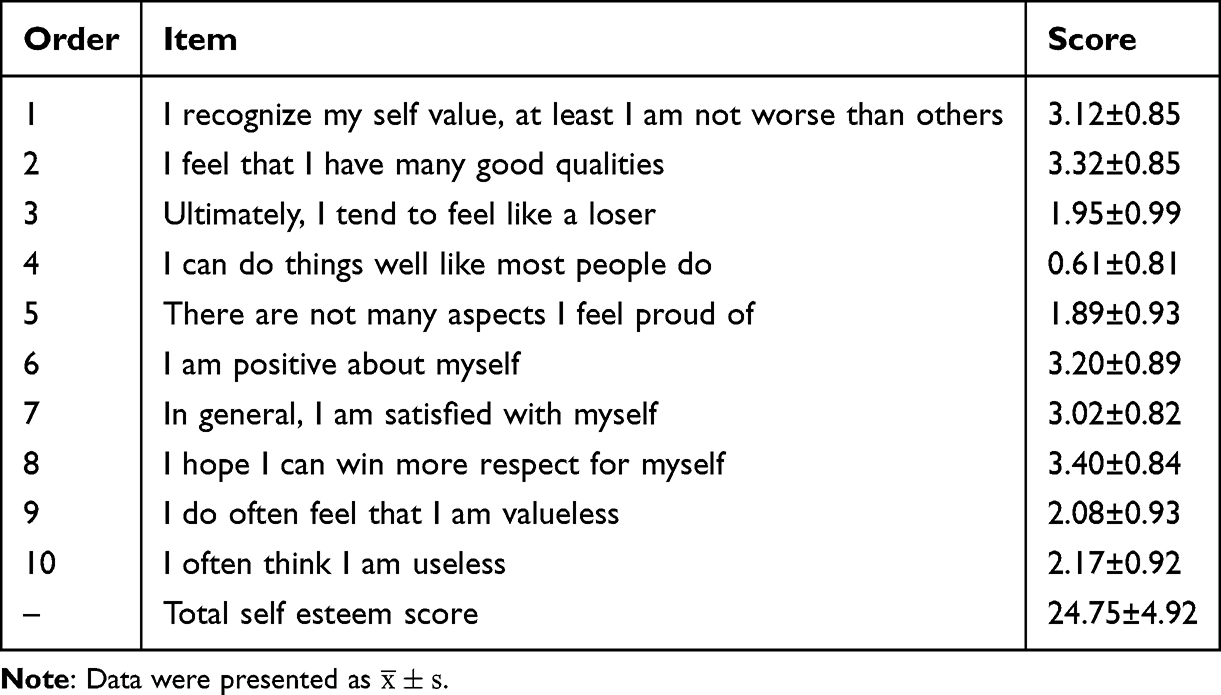
The mean SES score for the cohort was 24.75±4.92, reflecting generally low self-esteem among PWS patients. The item with the highest score was “I hope I can win more respect for myself”, indicating a strong desire among patients for greater societal acceptance and recognition. Conversely, the item with the lowest score was “I can do things well like most people do”, suggesting a pervasive sense of self-doubt regarding personal competence and abilities (Table 7). For this scale, the KMO value was 0.825, Bartlett’s test of sphericity was significant (χ² = 493, df = 45, p < 0.001). The reliability of the SES scale had been tested, and the Cronbach’s alpha was 0.572, which is below the commonly accepted threshold of 0.7, which may reflect some heterogeneity among the items or the complexity of the construct being measured. Future studies could further optimize the design of the scale to improve its internal consistency.
 |

As shown in Table 8, all 113 PWS patients fell within the “low self-esteem” category, with SES scores ranging from 10 to 27, and no participants reaching intermediate or high self-esteem levels. This result underscored the pervasive impact of PWS on self-esteem, as every participant reported a low level of self-regard, likely due to the visible nature of their condition and the societal stigma associated with facial differences.
 |
Table 8 Variations in Self-Esteem Levels Among Individuals with PWS |
As shown in Table 9, univariate analysis further revealed that employment status and monthly income were associated with SES scores (P < 0.05). Patients who were unemployed or had lower incomes tended to report lower self-esteem. However, these associations were still not sustained in multivariable models, suggesting the presence of potential confounding factors or interrelated variables that may influence self-esteem in PWS patients.
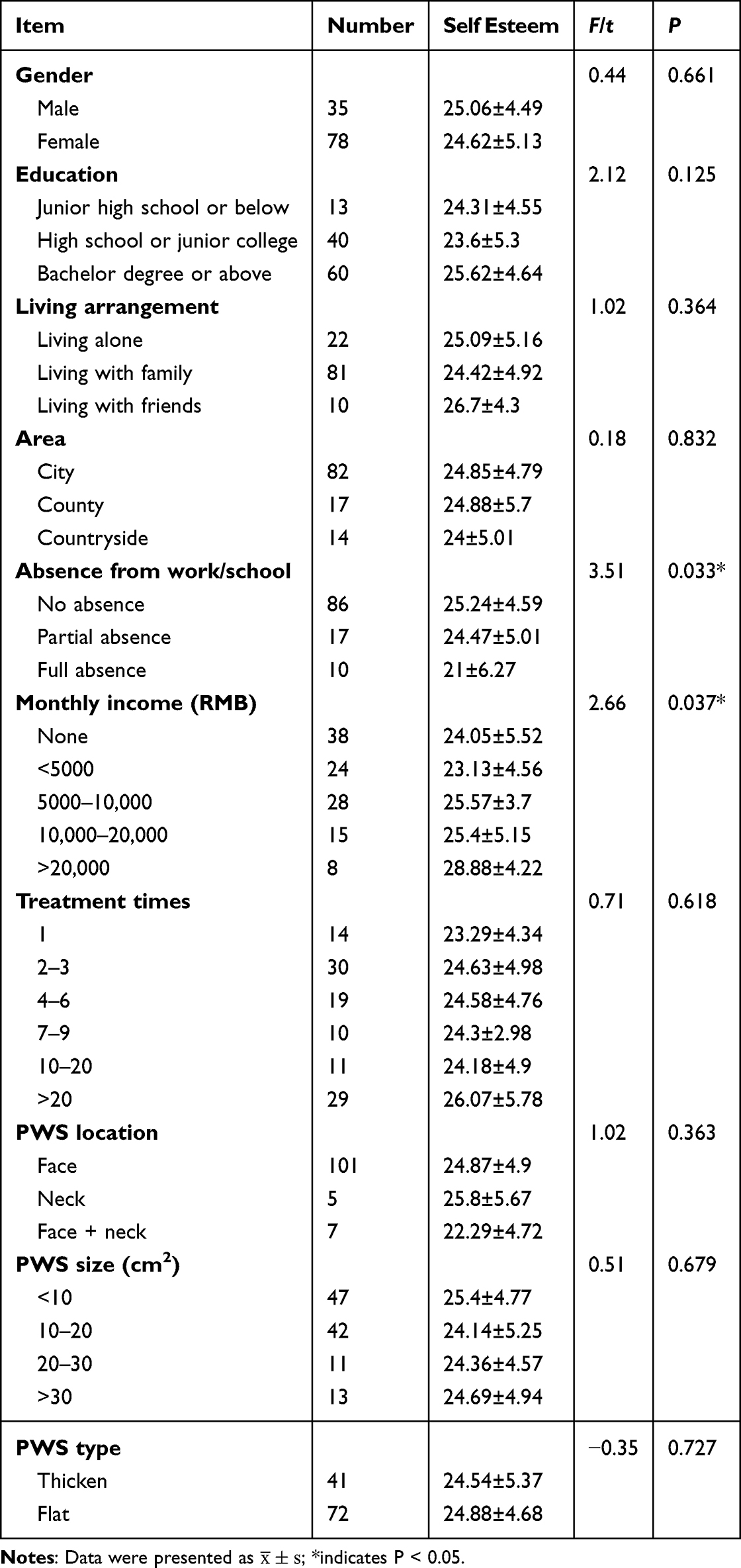 |
Table 9 A Univariate Analysis of Demographic Data Related to Self-Esteem in PWS Patients |
Correlation Between Stigma and Self-Esteem
Pearson’s correlation analysis revealed a significant negative correlation between stigma (SSCI total score) and self-esteem (SES score) (−0.497, P < 0.01), indicating that higher perceived stigma was correlated with lower self-esteem. Both intrinsic stigma (r = −0.464, P < 0.01) and extrinsic stigma (r = −0.464, P < 0.01) dimensions within the SSCI scale also showed significant negative correlations with SES scores, reinforcing the detrimental impact of stigma on self-worth.
Additionally, SIS scores were negatively correlated with SES scores (r = −0.531, P < 0.01), with each SIS subdimension (social rejection, financial insecurity, internalized shame, and social isolation) showing a similar negative association with self-esteem. These findings underscored the interrelationship between social impact, stigma, and self-esteem among patients with facial and neck PWS, suggesting that both societal and internalized forms of stigma substantially impair self-perception (Table 10). This highlighted the need for psychological and social support interventions to address the multifaceted impacts of PWS on patients’ psychological status.
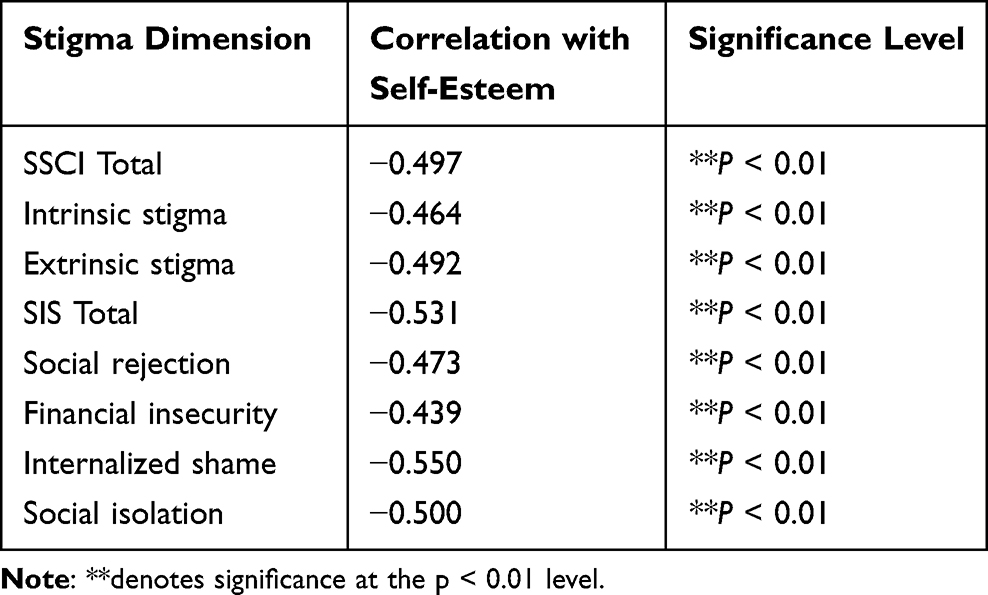 |
Table 10 Pearson Correlation Analysis Between Self-Esteem and Stigma Dimensions (SSCI and SIS) in PWS Patients |
Discussion
Prior research on PWS has primarily focused on therapeutic interventions and physiological outcomes, often overlooking the psychosocial dimensions, which are critical for understanding the broader implications of this condition on patients’ lives. Appearance, particularly when affected by visible skin conditions like PWS on the face and neck, has profound implications on self-perception, social interactions, and overall mental health. Studies indicate that PWS can significantly affect personality development and relationships, with these impacts intensifying over time as the lesions persist or become more pronounced.14 Given that 70–85% of PWS cases manifest in highly visible areas,15 this study provides valuable insights into how PWS affects social functioning and psychological well-being.
This study showed that PWS patients experience moderate levels of chronic disease-related stigma, as measured by both the SSCI and SIS. From the univariate analysis, we could tell factors including education level, monthly income, treatment frequency, and PWS characteristics such as site and size were associated with stigma. This finding aligns with prior studies suggesting that educational attainment may serve as a protective factor against stigma in chronic illness populations.16 However, when adjusted for potential confounders in the multivariable linear regression model, these associations were no longer statistically significant. Instead, we found that the type of PWS lesions and numbers of treatments were significantly associated with stigma, indicating that a flatter lesion area and a higher number of treatment sessions were associated with lower levels of stigma. It is easy to understand that flat lesions may be less noticeable and more easily hidden, which have a smaller impact on the facial appearance compared to thickened lesions. It’s also possible that thickened lesions tend to evolve from flat forms, which may mean that patients with thickened PWS lesions have lived with this condition for a longer period and therefore may be more psychologically burdened and stigmatized. Wang et al found that hypertrophic PWS were one of the main factors influencing the QoL of PWS patients,17 and our study further found that, stigma may be one of the key psychological factors faced by patients with thickened lesions, providing a more concrete psychological explanation for the decline in quality of life.
As for the number of treatments, this study found a negative correlation between the number of treatments and stigma, which is somewhat surprising, because it is generally believed that a higher number of treatments is associated with laser-resistant PWS. Does this imply that the treatment process itself may have a role in emotional regulation? Previous studies had also pointed out that after receiving laser treatment, patients with PWS experienced significant relief from emotional distress.18 This phenomenon may be partly attributed to the subjective sense of control, hope, and the psychological effects of positively coping with the condition brought about by the treatment.
This finding leads us to consider that even in cases where the disease cannot be completely eradicated, the process of repeated treatments may still provide emotional support and psychological comfort, thereby reducing the stigma associated with the illness.
It is noteworthy that the negative correlation between the number of treatments and stigma may not solely arise from the treatment effects themselves. In the actual treatment process, patients frequently contact treatment facilities multiple times and may regularly encounter other patients with port-wine stains, leading to the realization that they are not alone. This can foster a sense of “belonging” and a “normalizing” cognitive experience. As Treichler et al found that sense of belonging can protect against self-stigma.19 This sense of identification gained within the group may help weaken the stigma originally triggered by feelings of isolation.
Future treatment designs could consider incorporating patient support groups or mechanisms for group communication to further enhance the social support effects of treatment.
In examining self-esteem, this study identified a strong negative correlation between stigma and self-esteem, consistent with Corrigan’s psychological cognitive model,20 which posits that stigma is intrinsically linked to self-worth and self-perception. Patients with low self-esteem are more susceptible to internalizing societal stigma, attributing social rejection to their condition and perceiving it as a personal failing, which further exacerbates their psychological distress. Conversely, high levels of stigma erode self-esteem by reinforcing feelings of inadequacy and social exclusion, thereby creating a vicious cycle that negatively impacts mental health and social functioning.
Despite these insights, this study has several limitations. This study is a post-test-only one-group design, and the sample size is relatively limited, all coming from a single treatment center, which may affect the external validity and representativeness of the results. Future research should verify the stability of the results with multi-center studies and larger sample sizes. Additionally, since this study employs a cross-sectional design, it cannot establish causal relationships between variables. For example, the relationship between the number of treatments and stigma needs to be further explored through longitudinal tracking. The stigma assessment used a self-report questionnaire, which, despite having certain reliability, may still be influenced by subjective emotions, recall bias, and other factors. Finally, stigma, as a social-psychological response, may exhibit cultural variations. The results of this study are primarily based on Chinese patients, so caution should be exercised when generalizing to other cultural contexts.
Conclusion
In conclusion, patients with port-wine stains generally experience high levels of stigma and low levels of self-esteem, suggesting that the mental health status of current PWS patients should not be overlooked. Further analysis revealed that thickened lesions were significantly associated with stronger feelings of stigma, while more treatment sessions were linked to lower stigma levels. This may reflect the positive emotional regulation effects of the treatment itself or stem from the sense of belonging and hope that patients gain during treatment. It suggests that clinical treatment should pay more attention to the psychological state and emotional support of patients. Future intervention designs could attempt to integrate group support, psychological interventions, and the treatment itself to collectively improve stigma and promote the overall recovery of patients’ physical and mental health.
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Drooge AM, Beek JF, van der Veen JPW, et al. Hypertrophy in port-wine stains: prevalence and patient characteristics in a large patient cohort. J Am Acad Dermatol. 2012;67(6):1214–1219. doi:10.1016/j.jaad.2012.05.027
2. Ortiz AE, Nelson JS. Port-wine stain laser treatments and novel approaches. Facial Plast Surg. 2012;28(6):611–620. doi:10.1055/s-0032-1329936
3. Augustin M, Zschocke I, Wiek K, Peschen M, Vanscheidt W. Psychosocial stress of patients with port wine stains and expectations of dye laser treatment. Dermatol. 1998;197(4):353–360. doi:10.1159/000018031
4. Demellweek C, Humphris GM, Hare M, Brown J. Children’s perception of, and attitude towards, unfamiliar peers with facial port-wine stains. J Pediatr Psychol. 1997;22(4):471–485. doi:10.1093/jpepsy/22.4.471
5. Hansen K, Kreiter CD, Rosenbaum M, Whitaker DC, Arpey CJ. Long-term psychological impact and perceived efficacy of pulsed-dye laser therapy for patients with port-wine stains. Dermatol Surg. 2003;29(1):49–55. doi:10.1046/j.1524-4725.2003.29010.x
6. Lee JW, Chung HY. Capillary malformations (Portwine Stains) of the head and neck: natural history, investigations, laser, and surgical management. Otolaryngol Clin North Am. 2018;51(1):197–211. doi:10.1016/j.otc.2017.09.004
7. Masnari O, Schiestl C, Rossler J, et al. Stigmatization predicts psychological adjustment and quality of life in children and adolescents with a facial difference. J Pediatr Psychol. 2013;38(2):162–172. doi:10.1093/jpepsy/jss106
8. van der Horst CM, de Borgie CA, Knopper JL, Bossuyt PM. Psychosocial adjustment of children and adults with port wine stains. Br J Plast Surg. 1997;50(6):463–467. doi:10.1016/S0007-1226(97)90335-0
9. Rao D, Choi SW, Victorson D, et al. Measuring stigma across neurological conditions: the development of the stigma scale for chronic illness (SSCI). Qual Life Res. 2009;18(5):585–595. doi:10.1007/s11136-009-9475-1
10. Deng C, Lu Q, Zhao Y. Chinese translation and validation of the stigma scale for chronic illness in stroke patients. Chin Gen Pract. 2017;20(34):4304–4309.
11. Fife BL, Wright ER. The dimensionality of stigma: a comparison of its impact on the self of persons with HIV/AIDS and cancer. J Health Soc Behav. 2000;41(1):50–67. doi:10.2307/2676360
12. Rosenberg FR, Rosenberg M, McCord J. Self-esteem and delinquency. J Youth Adolesc. 1978;7(3):279–294. doi:10.1007/BF01537978
13. McMullen T, Resnick B. Self-esteem among nursing assistants: reliability and validity of the Rosenberg self-esteem scale. J Nurs Meas. 2013;21(2):335–344. doi:10.1891/1061-3749.21.2.335
14. Wanitphakdeedecha R, Ng JNC, Yan C, Manuskiatti W, Sudhipongpracha T, Jantarakolica T. Quality of life and psychological effects of port-wine stain: a review of literature. Clin Cosmet Invest Dermatol. 2021;14:681–690. doi:10.2147/CCID.S315804
15. Hagen SL, Grey KR, Korta DZ, et al. Quality of life in adults with facial port-wine stains. J Am Acad Dermatol. 2017;76(4):695–702. doi:10.1016/j.jaad.2016.10.039
16. Lee HJ, Choi EK, Park HB, Yang S-H. Risk and protective factors related to stigma among people with epilepsy: an integrative review. Epilepsy Behav. 2020;104(Pt A):106908. doi:10.1016/j.yebeh.2020.106908
17. Wang J, Zhu YY, Wang ZY, et al. Analysis of quality of life and influencing factors in 197 Chinese patients with port-wine stains. Med. 2017;96(51):e9446. doi:10.1097/MD.0000000000009446
18. Troilius A, Wrangsjö B, Ljunggren B. Potential psychological benefits from early treatment of port-wine stains in children. Br J Dermatol. 1998;139(1):59–65. doi:10.1046/j.1365-2133.1998.02314.x
19. Treichler EBH, Lucksted AA. The role of sense of belonging in self-stigma among people with serious mental illnesses. Psychiatr Rehabil J. 2018;41(2):149–152. doi:10.1037/prj0000281
20. Corrigan PW, Kerr AN, Knudsen L. The stigma of mental illness: explanatory models and methods for change. Appl Prev Psychol. 2005;11(3):179–190. doi:10.1016/j.appsy.2005.07.001
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Sexual Function, Self-Esteem, and Quality of Life in Infertile Couples Undergoing in vitro Fertilization: A Dyadic Approach
Wang JY, Lv XQ, Wu JM, Tang WQ, Luo GY, Liang CM, Wang DN, Hong JF, Cao YX
Psychology Research and Behavior Management 2022, 15:2449-2459
Published Date: 6 September 2022