")
Back to Journals » Journal of Pain Research » Volume 18
A Systematic Review and Meta-Analysis of Randomized Controlled Trials for Electroacupuncture Treatment of Migraine
Received 21 January 2025
Accepted for publication 23 April 2025
Published 6 May 2025 Volume 2025:18 Pages 2321—2333
DOI https://doi.org/10.2147/JPR.S518294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
ShiWei Song,1 Hao Chen2
1Department of Traditional Chinese Medicine, Sichuan Taikang Hospital, Chengdu, Sichuan, People’s Republic of China; 2Chengdu University of Traditional Chinese Medicine CN, Chengdu, Sichuan, People’s Republic of China
Correspondence: ShiWei Song, Sichuan Taikang Hospital, No. 881 Xianghe 1st Street, Huayang Community, Tianfu New Area, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Purpose: Numerous clinical studies have shown that patients with migraine can benefit from electroacupuncture treatment. However, there are no published systematic reviews and meta-analyses of pure electroacupuncture for migraine. Therefore, we conducted a meta-analysis to evaluate the efficacy of pure electroacupuncture as a standalone treatment for migraine patients.
Patients and Methods: We searched Six electronic databases. All from the inception to August 1st, 2024. In the literature, clinical investigators evaluated the efficacy and safety of electroacupuncture as the primary treatment for migraine. Researchers assessed the quality of the studies using the Cochrane Handbook for Systematic Reviews of Interventions. The Review Manager 5.4 software was used to perform statistical analysis.
Results: Ten randomized controlled trials involving 1161 people were included. The meta-analysis yielded a substantial result: the application of pure electroacupuncture significantly improved the effective rate compared to the control group. In the visual analogue scale score, the present study found no significant difference between electroacupuncture and Western medicine as standalone treatments. Regarding migraine-associated symptom scores, the experimental group exhibited no superiority in comparison to the control group. Moreover, following the intervention, several significant changes were observed in the secondary outcome indicators between the two groups, including cerebral arterial blood flow velocity, the migraine attack days, the lasting time of headache remission, mean time of the headache attack, duration of the headache attack, and the migraine-specific quality of life questionnaire score, with the results proving to be statistically significant.
Conclusion: The results of the analysis suggested that pure electroacupuncture is beneficial for migraine patients, but it remains difficult to obtain comprehensive data. Our study is supported by evidence of low to moderate quality. It is necessary to further confirm the efficacy of pure electroacupuncture for migraine with higher-quality clinical research.
Keywords: electroacupuncture, migraine, meta-analysis, randomized controlled trials, systematic review
Introduction
Migraine is one of the ten most serious chronic dysfunction diseases in the world. The worldwide prevalence of migraine is around 11.6%.1,2 It is estimated that more than one billion people worldwide are affected by migraine.3 The majority of patients are under the age of 50, with a higher prevalence observed among women compared to men.4 Compared with developed countries, in China, evidence from an epidemiological study of migraine shows that the prevalence of the disease is 9.33%, 5.0% to 6.9% for men and 11.5% to 14.1% for women, and is estimated to cost more than 300 billion Yuan on an annual basis.5 As a common and frequently occurring disease in the clinic, migraine is easy to repeat, prolonged, and difficult to cure, which may have a serious impact on the patient’s work life and family, and may cause certain disability in severe cases, which will bring huge economic burden and survival pressure to the country and even the whole society.6 Migraine is a neurological disease mainly caused by vasomotor dysfunction, often manifested as unilateral or bilateral pulsatile headache.7 The disease is characterized by periodic, recurrent attacks, and severe attacks are often accompanied by nausea, dizziness, sweating, vomiting, palpitations, and other unpleasant symptoms.8 While these conventional treatments can provide temporary symptomatic relief, it is important to note that they are associated with certain side effects.9 Consequently, there has been an increasing tendency to utilize complementary and alternative therapies, with electroacupuncture representing a salient example.10
Through numerous clinical trials, researchers have found that electroacupuncture has a significant advantage in the treatment of migraine.11,12 Electroacupuncture has been widely used in the clinical treatment of migraine and has shown clear efficacy in a series of studies. Electroacupuncture has a good analgesic effect.13 In recent years, electroacupuncture treatment of migraine has been accepted by the masses for its advantages of economy, effectiveness, and little side-effects.14 However, electroacupuncture is regarded as an independent treatment method, so far, there are no systematic reviews and meta-analyses that address the application of pure electroacupuncture for treating migraine. Therefore, we conducted this meta-analysis to evaluate the efficacy of electroacupuncture in alleviating migraine. Our goal is to provide strong support for the clinical practice of migraine treatment.
Materials and Methods
This meta-analysis strictly adheres to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-analysis. A comprehensive protocol for the study has been meticulously registered at PROSPERO (No. CRD42024575485).
Inclusion Criteria
- Patient: Patients included in the literature must be older than 18 years. Patients diagnosed with migraine according to the International Classification of Headache Disorders released by the International Headache Society, regardless of gender, race, color of skin, and source of the patients.
- Intervention: The experimental group only received electroacupuncture treatment.
- Comparison: The control group received Western treatments for migraine.
- Outcome: Main outcome measures: The effective rate; The visual analogue scale score.
Secondary outcome assessment indicators: migraine-associated symptom score; Cerebral arterial blood flow velocity; The migraine attack days; The lasting time of headache remission; mean time of the headache attack; duration of the headache attack; The Migraine - Specific Quality of Life Questionnaire score.
- Study design: The type of literature is a randomized controlled trial of the independent use of electroacupuncture for the treatment of migraine. The language of publication was limited to English and Chinese.
Exclusion Criteria
- Studies without diagnostic criteria for migraine.
- (The treatment group received electroacupuncture in combination with other treatment methods.
- Research on animal experiments, case reports, letters, reviews, comments, and personal experience.
- Repeatedly published literature.
- Defective literature data.
- Incomplete full text and outcomes.
- Nonclinical randomized controlled trials.
- Studies for which data could not be extracted.
Search Strategy
A full schematic and protocol of this study have been registered at PROSPERO (No. CRD42024575485). The following databases were the Wan-Fang database, the China National Knowledge Infrastructure, VIP database, Embase, PubMed, and Cochrane Library. All from the inception to August 1st, 2024. In addition, to avoid missing studies, grey literature and reference lists were also searched. The main search terms and keywords included “migraine”, “migraine disorders”, “hemicrania”, “headache”, “electroacupuncture”, “acupuncture”, “Pharmacopuncture”, “acupuncture treatment”, “acupuncture therapy”, “needling therapy”, “needling”, “randomized controlled trial” and “clinical trials”. As an example, Table 1 shows the study selection process of PubMed.
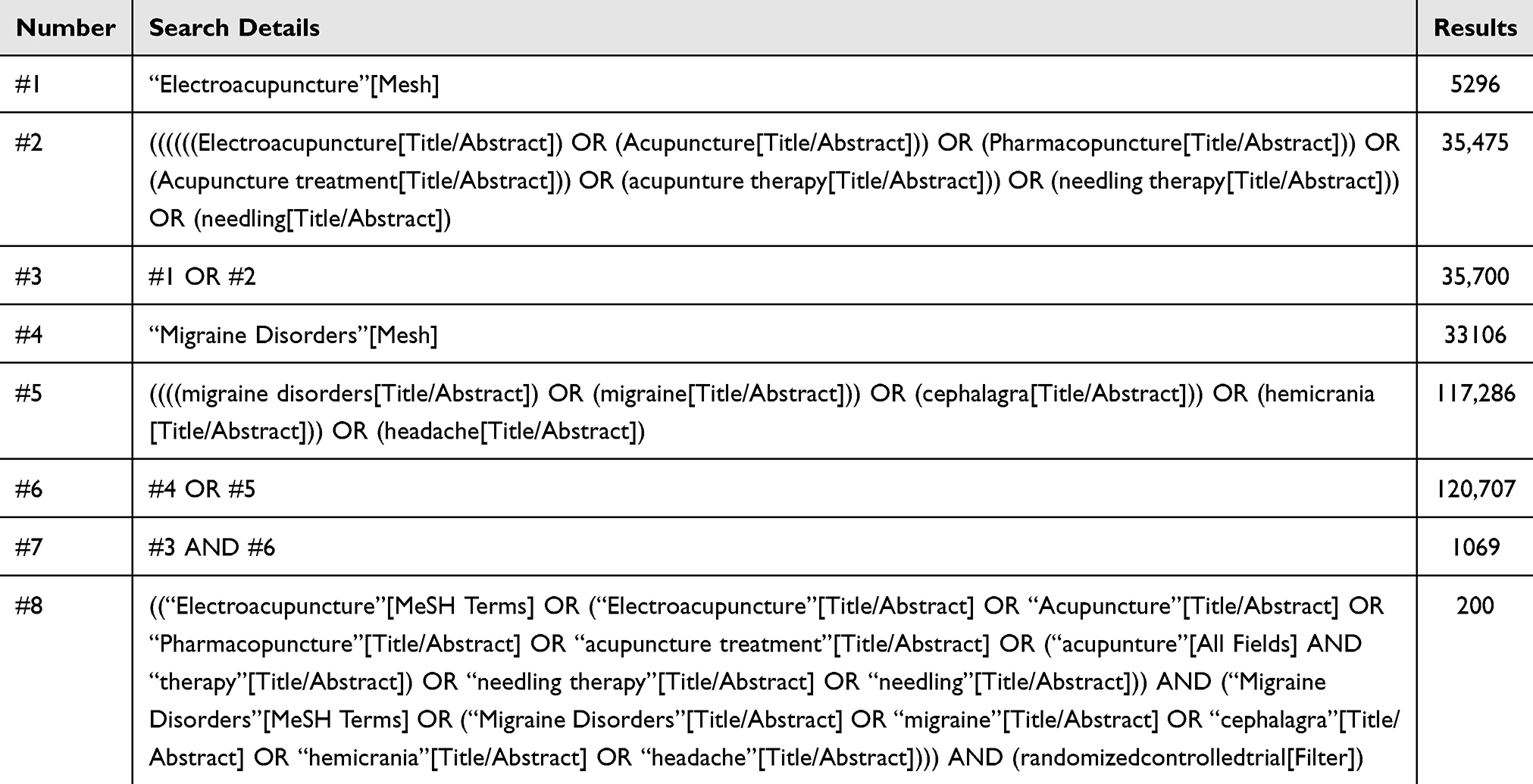 |
Table 1 PubMed: Session Results |
Outcome Assessment Indicators
Main outcome measures: The effective rate; The visual analogue scale score.
Secondary outcome assessment indicators: migraine-associated symptom score; Cerebral arterial blood flow velocity; The migraine attack days; The lasting time of headache remission; mean time of the headache attack; duration of the headache attack; The Migraine - Specific Quality of Life Questionnaire score.15
Literature Screening and Data Extraction
All the collected submissions, including those from various databases and manually retrieved studies, were entered into EndNoteX9, Once the duplicate literature had been eliminated using the re-checking function, two researchers carried out the preliminary screening of the literature according to the inclusion and exclusion criteria. After the preliminary screening of literature by two researchers independently, the substandard literature was excluded. Then re-screen by reading the full text. In cases of divergence, discrepancies were resolved through collaborative discussion, with the pursuit of unified agreement guiding the resolution process. Finally, the selected literature that meets the requirements is classified. Excel was used to make a statistical analysis of the basic data of the study.
Risk Bias and Quality Assessment
Two reviewers independently used the ReviewManager5.4 software risk bias assessment tool provided by the Cochrane Collaboration RCT risk of bias assessment tool. The quality of the literature was evaluated by low risk, unknown risk, and high risk. Evaluation indicators include: l) Random scheme generation; 2) allocation concealment; 3) blinding of patients; 4) blinding of outcome measurements; 5) incomplete outcome data; 6) selective reporting; 7) other bias.
Statistical Analysis
The Review Manager 5.4 software was used to perform statistical analysis. Continuous outcomes were assessed using the mean difference, and the odds ratio was selected as the analysis measure for dichotomous variable data.95% Confidence Intervals (95% CIs) are selected to quantify the precision. If there was no heterogeneity, the fixed effects model was used (P≥ 0.1, I²≤50%). The random effects model is used when there is statistical heterogeneity between studies (P < 0.1, I² > 50%). The Forest plot shows the result. It was assumed (P < 0.05) that this represented a statistically significant difference. When heterogeneity was high, sensitivity analyses were performed to test the stability of the results, if necessary.
Results
Literature Search Results
Per the search strategy, a total of 5024 articles were searched. Following the exclusion of 540 duplicate references, 4372 articles deemed irrelevant on initial review were excluded. This process was conducted by reading the title and abstract, resulting in the retrieval of 112 articles for further evaluation. A total of 102 articles excluded included the following literature: graduation thesis (n=3), conference (n=16), reviews (n=5); inappropriate interventions (n=29), not human (n =5), patients younger than 18 years (n=16), combined with other treatments (n=23), and concurrent with other diseases (n=5). Following a comprehensive review of the pertinent literature, a total of 10 studies were selected for inclusion in the meta-analysis (Figure 1).
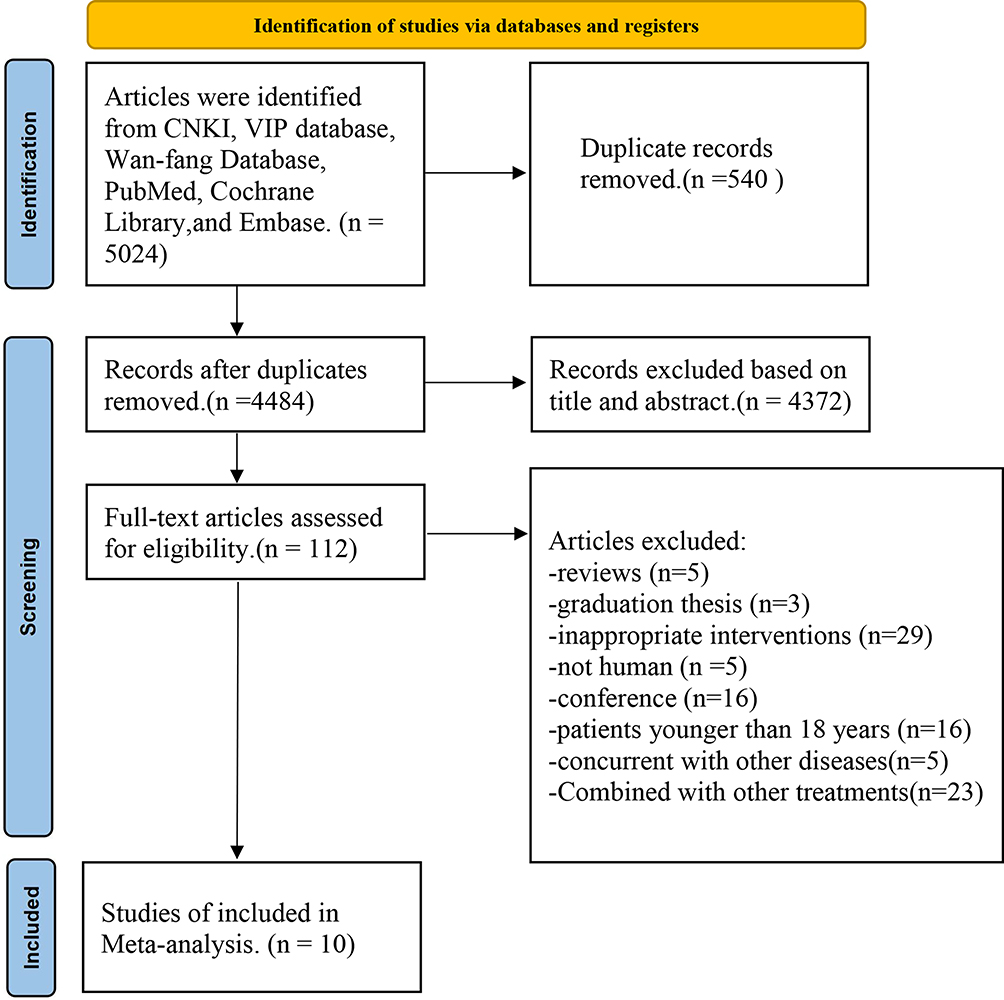 |
Figure 1 The process of literature search. |
The general information and characteristics of 10 studies are shown in Table 2.16–25 The publication period under consideration is from 2007 to 2022. The total number of patients enrolled in the study was 1,161, with 566 patients allocated to the control group and 595 patients allocated to the treatment group. The number of cases ranged from 40 to 286. In the 10 studies, the experimental groups were administered pure electroacupuncture in the treatment of patients with migraine, while the control group was treated exclusively with Western medicine. The duration of the treatment period in the ten studies ranged from 20 to 90 days. Basic information about the literature included: the first author`s name; year of publication; the number of cases; sample size; gender; average age; duration of disorder; treatment period; outcome; adverse reaction; and follow-up duration.
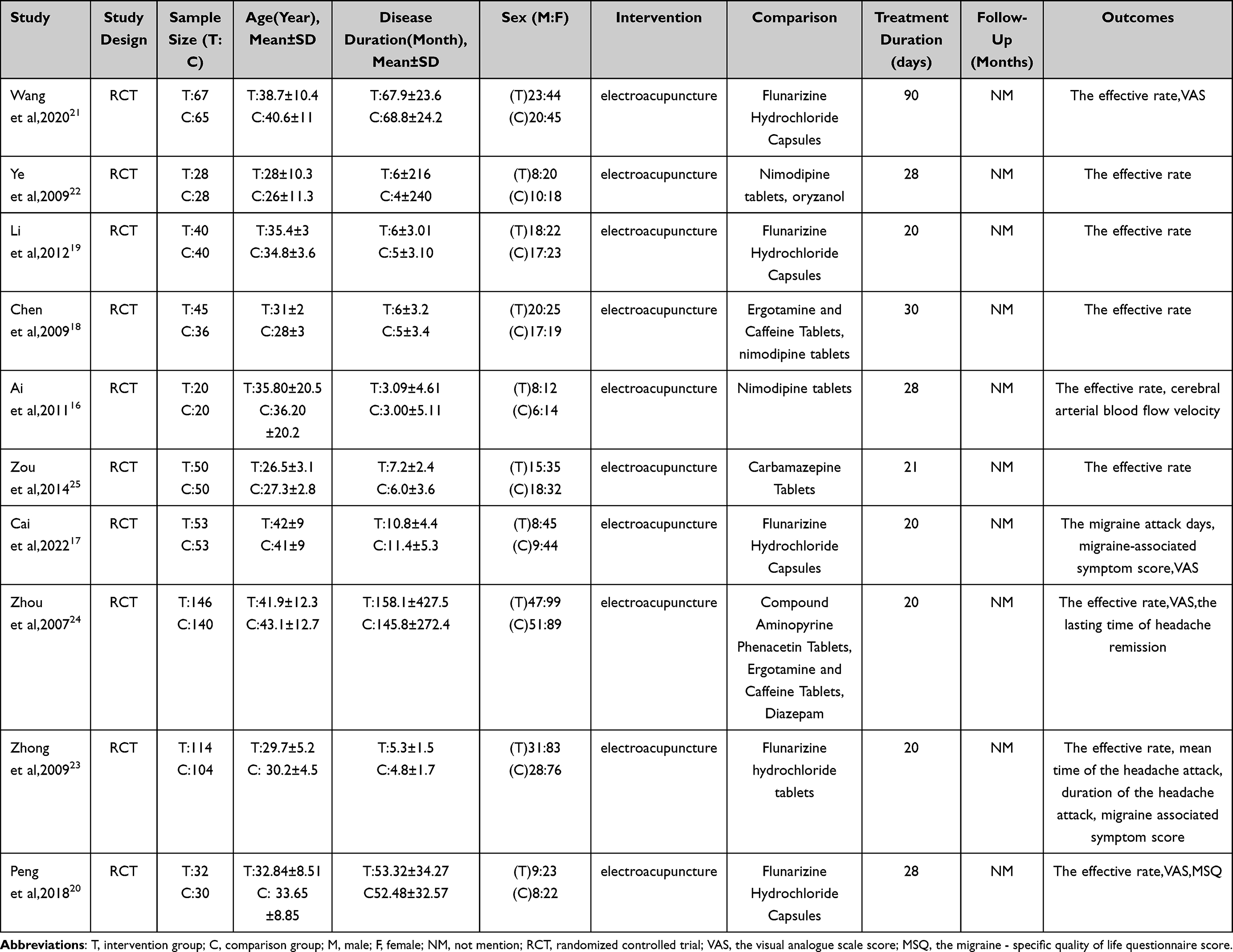 |
Table 2 Characteristics of 10 Studies |
Where 9 studies assessed the effective rate of treatment, 4 articles analyzed the visual analogue scale score, 2 articles measured migraine-associated symptom score, 1 article analyzed cerebral arterial blood flow velocity,1 article reported the migraine attack day,1 article measured the lasting time of headache remission, In addition, one article each examined the duration of the headache attack, mean time of the headache attack, and the migraine-specific quality of life questionnaire score.
Methodological and Reporting Quality
The included literature was analyzed according to the risk assessment tool. 7 studies used random number tables which are at low risk in terms of random sequence generation. In terms of allocation program concealment, half of the studies described whether the studies implemented allocation concealment or specific schemes. Concerning the presence or absence of blinding amongst investigators and patients, the following observations can be made: Four studies described how the researchers or subjects were blinded. About the evaluation of outcomes in the absence of knowledge regarding the allocation of interventions, six articles were found to be at low risk. In terms of the completeness of outcome data, six studies were found to be at low risk. In the risk assessment for reporting bias, only 1 study was at unknown risk. With a view to other biases, seven articles were categorized as being at unknown risk. As demonstrated in Figures 2 and 3, the specific risk of bias is illustrated.
 |
Figure 2 Assessment of the risk of bias of ten articles. |
 |
Figure 3 The overall risk bias assessments of this study.16–25 |
The Effective Rate
9 studies reported the effective rate of electroacupuncture in the treatment of migraine.16–25 A heterogeneity analysis of the effectiveness rate was conducted, which revealed the absence of heterogeneity within the extant literature. Consequently, a fixed-effects model was selected for the analysis (I2=0%; P=0.71). Regarding the effective rate, the efficacy of electroacupuncture in treating migraine was better than that of the control group (OR:3.13; 95% CI:2.16–4.54; P<0.00001, Figure 4).
 |
Figure 4 Forest plot of electroacupuncture efficiency for migraine.16,18–25 |
Visual Analogue Scale Score
In the included studies, a total of 4 studies recorded visual analogue scale scores.17,20,21,24 The existence of significant heterogeneity among the studies necessitated the implementation of a random-effects model in this meta-analysis (I2=93%; P<0.00001). The findings indicated that there was no statistically significant discrepancy in the visual analogue scale score between the two groups (MD: −0.67; 95% CI: −2.15–0.80; P=0.37, Figure 5).
 |
Figure 5 Forest plot of meta-analysis on visual analogue scale score for migraine.17,20,21,24 |
Migraine-Associated Symptom Score
Only two types of research with 324 patients evaluated migraine-associated symptom scores.17,23 The analysis adopted random-effects model analysis, no homogeneity among studies (P<0.0001, I2 = 95%) was operated. The results of the study indicated that, in comparison with Western medicine, electroacupuncture alone exhibited no substantial benefits in terms of reducing migraine-associated symptom score (MD: −1.74; 95% CI: −3.56–0.08; P=0.06, Figure 6).
 |
Figure 6 Forest plot of migraine-associated symptom score with electroacupuncture treatment.17,23 |
Other Secondary Outcome Assessment Indicators
1 article reported cerebral arterial blood flow velocity,16 and there was a statistical difference between the electroacupuncture group and the control group (P < 0.05).1 article reported the migraine attack days,17 and the migraine attack days in the two groups were decreased compared with before treatment (P<0.05). One article measured the lasting time of headache remission,24 with the treatment group being significantly longer than that of the control group (P < 0.01). Additionally, one article each examined the duration of the headache attack, and the mean time of the headache attack,23 following the administration of treatment, a marked improvement was observed in both groups (P < 0.01). However, electroacupuncture treatment exhibited superior efficacy in comparison to the Western medicine group (P < 0.05). A research reported the improvement of migraine-specific quality of life questionnaire score was better in the treatment group than in the control group (P<0.05).20
Adverse Events Assessment
Among the 10 studies, 7 mentioned no adverse reactions between the experimental group and the control group, and 3 mentioned adverse reactions: Wang:21 control group: gastrointestinal reactions (3 cases) (23.07%), and drowsiness (6 cases) (46.15%). Cai17 reported one case of a subcutaneous hematoma in the treatment group (7.69%), one case of gastrointestinal reactions (7.69%), and one case of drowsiness in the control group (7.69%). Zhong23 showed that in the Western medicine group, one patient experienced drowsiness, fatigue, and lower limb edema (7.69%), which improved after discontinuing the medication.
Sensitivity Analysis
Sensitivity analyses of the visual analogue scale score and migraine-associated symptom score with greater heterogeneity were performed separately using the method of excluding individual studies. Heterogeneity did not change significantly after excluding each study, suggesting that the source of heterogeneity may be due to the small number of relevant outcome indicators included in the literature, as well as due to differences in electroacupuncture frequency, acupoint selection, depth of needling, and patients’ subjective feelings in the test groups.
Publication Bias
In this study, the number of articles on all outcome indicators was less than 10, which did not meet the criteria for making a funnel plot. Consequently, the funnel plot bias test was not utilized, and the efficacy of the research results in terms of testing efficiency may be deemed to be inadequate.
Discussion
Summary of Main Results
This systematic review and meta-analysis were the first to focus on randomized controlled trials examining the efficacy of pure electroacupuncture for migraine treatment. The present analysis encompassed a total of ten articles, which collectively comprised 1,161 patients diagnosed with migraine. The study evaluated the primary outcomes of electroacupuncture as a standalone treatment, including the effective rate, the visual analogue scale score, migraine associated symptom score; cerebral arterial blood flow velocity; the migraine attack days; the lasting time of headache remission; mean time of the headache attack; duration of the headache attack; and the migraine-specific quality of life questionnaire score. A statistically significant difference in the effective rate after treatment was observed between the treatment group and the Western medicine group. Regarding cerebral arterial blood flow velocity and the migraine attack days, there is a significant difference. One research reported that p-values had had statistical significance in duration of the headache attack and mean time of the headache attack. The lasting time of headache remission were changed significantly after intervention in both groups. An article reported that the migraine - specific quality of life questionnaire score was better in the treatment group than in the control group. Despite there were no significant differences were observed in the visual analogue scale score and migraine-associated symptom score between the two groups. The results suggested that electroacupuncture can achieve a beneficial effect in the treatment of migraine. Naturally, there are a few indicators where electroacupuncture does not significantly improve the corresponding symptoms. Nevertheless, it should be pointed out that in our meta-analysis, there are indeed some parameters that do not show significant correlation with the main efficacy indicators. This may be due to differences in the design, sample size, and measurement methods of the included studies, which lead to an inconspicuous association between some secondary indicators and the main indicators. We recommend that future clinical studies further explore the potential links between these parameters and include a sham-injection control group to verify the direct impact of electroacupuncture on the vascular tone of the cranial district.
So far, migraine is the second most common cause of disability, accounting for 16.3% of neurological symptoms all over the world.26 Migraine has become a major public health problem and has a significant impact on activities of daily living. The etiology of migraine is a subject that is not yet fully elucidated, contemporary clinical research has demonstrated a correlation with cerebral cerebrovascular diseases, genetic factors, mental tension, menstruation, endocrine factors, and other variables.27 Of course, it does not exclude the influence of living habits, psychological factors, or social environment. Currently, the exact pathogenesis of migraine remains elusive in Western medical science, although there is a broad consensus that the principal triggers are likely related to the dysfunction of cerebral vasodilatation and vasoconstriction.28 Despite earlier beliefs, vasodilation is only a secondary phenomenon and vasoconstriction is not essential for antimigraine efficacy.29 The pathogenesis hypothesis of migraine mainly includes vascular theory, trigeminal vascular theory, cortical diffusion inhibition theory, inflammatory mediator theory, and genetic theory.30 At present, the main Western treatment options for migraine are non-steroidal anti-inflammatories, the 5-HT1F receptor, and calcitonin gene-related peptide.9,31 In terms of the progress of non-drug treatment of migraine, there are mainly nerve block treatment, nerve stimulation treatment, etc. These treatments can relieve migraine to varying degrees, but their safety and sustainability still need further research.32,33 However, there has been a paucity of efficacious pharmacotherapy for migraine. Moreover, conventional Western medicine has been shown to have both adverse side effects and clear limitations in its approach to the treatment of migraine. Some patients are prone to nausea, vomiting, fatigue, and somnolence, and may even suffer from liver and kidney dysfunction. Therefore, it is necessary to explore the need for alternative or complementary comprehensive treatment of migraine. On the basis of these findings, it can be concluded that electroacupuncture has the potential for further development and expansion. In recent years, the clinical research and pathological mechanism of electroacupuncture treatment of migraine have gradually increased.34 Researchers have found that the mechanism of electroacupuncture therapy for migraine mainly focuses on improving cerebral blood flow, regulating vasoactive neuropeptides, regulating inflammatory cytokines, and regulating the endocannabinoid receptor system.35 A substantial corpus of clinical studies and animal experiments has demonstrated that electroacupuncture can enhance the body’s immune system and alleviate migraine pain.
Limitations
Our study has several limitations. In the first instance, the meta-analysis was constrained by the inclusion of a mere ten literature sources, which were all from China. A secondary issue that was identified pertained to the overall quality of the extant literature on the subject, which was found to be low. Moreover, the subsequent data from the relevant studies was incomplete, and the outcome indicators were not exhaustive, with key parameters such as healthcare costs and duration of follow-up omitted. A fourth finding was that the selection of electroacupuncture points differed between the treatment and control groups. Furthermore, the types and dosages of Western drugs selected by the control group were inconsistent, which was not conducive to a comprehensive, objective, and accurate evaluation of efficacy. Additionally, the frequency and depth of electroacupuncture are subjective, which may engender variability in treatment efficacy across different practitioners.
Conclusion
Electroacupuncture is an effective treatment for migraine patients, with a notable enhancement in the efficacy of the treatment. However, in the pursuit of advancing the scientific understanding of electroacupuncture treatment for migraine, there is a necessity for rigorous clinical study design and the execution of multi-center, large-sample, randomized controlled trials that encompass sufficient follow-up time. At the same time, due to the subjective nature of electroacupuncture treatment points, it is important to increase research on real-world electroacupuncture as a primary treatment for migraine in future studies and to include trials with the same electroacupuncture frequency and similar courses of treatment as much as possible, to obtain better results and to provide a certain amount of literature for the treatment of migraine with electroacupuncture.
Abbreviations
CNKI, China National Knowledge Infrastructure; OR, Odds Ratio; MD, Mean Difference; CI, Confidence Interval; RCT, randomized controlled trial; T, intervention group; C, comparison group; NM, not mention; VAS, the visual analogue scale score; MSQ, the migraine - specific quality of life questionnaire score.
Data Sharing Statement
The study’s original contributions can be found in this article. If necessary, please contact the corresponding authors.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that there are no conflicts of interest regarding the publication of this paper.
References
1. Stovner LJ, Andree C. Prevalence of headache in Europe: a review for the Eurolight project. J Headache Pain. 2010;11(4):289–299. doi:10.1007/s10194-010-0217-0
2. Woldeamanuel YW, Cowan RP. Migraine affects 1 in 10 people worldwide featuring recent rise: a systematic review and meta-analysis of community-based studies involving 6 million participants. J Neurol Sci. 2017;372(1878–5883 (Electronic)):307–315. doi:10.1016/j.jns.2016.11.071
3. Ashina M, Katsarava Z, Do TP, et al. Migraine: epidemiology and systems of care. Lancet. 2021;397(10283):1485–1495. doi:10.1016/S0140-6736(20)32160-7
4. Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017;16(1):76–87. doi:10.1016/S1474-4422(16)30293-9
5. Yu S, Liu R, Zhao G, et al. The prevalence and burden of primary headaches in China: a population-based door-to-door survey. Headache. 2012;52(4):582–591. doi:10.1111/j.1526-4610.2011.02061.x
6. Underwood M, Achana F, Carnes D, et al. Supportive self-management program for people with chronic headaches and migraine: a randomized controlled trial and economic evaluation. Neurology. 2023;100(13):e1339–e1352. doi:10.1212/WNL.0000000000201518
7. Silberstein SD. Migraine. Lancet. 2004;363(9406):381–391. doi:10.1016/S0140-6736(04)15440-8
8. Burch R. Migraine and tension-type headache: diagnosis and treatment. Med Clin North Am. 2019;103(2):215–233. doi:10.1016/j.mcna.2018.10.003
9. Blech B, Starling AJ. Noninvasive neuromodulation in migraine. Curr Pain Headache Rep. 2020;24(12):78. doi:10.1007/s11916-020-00914-3
10. Urits I, Patel M, Putz ME, et al. Acupuncture and its role in the treatment of migraine headaches. Neurol Ther. 2020;9(2):375–394. doi:10.1007/s40120-020-00216-1
11. Zheng S, Cui H. Acupuncture for migraine: a meta analysis. Chin J Inf Traditional Chin Med. 2012;19(06):20–23.
12. Linde K, Allais G, Fau - Brinkhaus B, et al. Acupuncture for migraine prophylaxis. Cochrane Database Syst Rev. 2009;
13. Gao X, Wang B, Song Y, Qi H, Rong Z, Wang H. Systematic review and meta-analysis of acupuncture for migraine treatment. Chin J Clin Pharmacol Ther. 2011;16(05):530–537.
14. Zhang F, Kong LL, Zhang YY, Li SC. Evaluation of impact on health-related quality of life and cost effectiveness of Traditional Chinese Medicine: a systematic review of randomized clinical trials. J AlternComplementary Med. 2012;18(12):1108–1120. doi:10.1089/acm.2011.0315
15. Martin BC, Pathak DS, Sharfman MI, et al. Validity and reliability of the migraine-specific quality of life questionnaire (MSQ Version 2.1). Headache. 2000;40(3):204–215. doi:10.1046/j.1526-4610.2000.00030.x
16. Ai M, Chang Y, Zhang Y, et al. Observation of the therapeutic effect of acupuncture at bilateral Sun and Fengchi acupoints on migraine. J Clin Acupuncture Moxibustion. 2011;27(9):9–10. doi:10.3969/j.issn.1005-0779.2011.09.003
17. Cai Y, Pei J, Fu Q, et al. Electroacupuncture at Siguan points for migraine of liver yang hyperactivity: a randomized controlled trial. Chin Acupuncture Moxibustion. 2022;42(05):498–502. doi:10.13703/j.0255-2930.20210403-0001
18. Chen H, Yang G, Tang Y. Observation on the therapeutic effect of electroacupuncture on migraine. Shanghai J Acupuncture Moxibustion. 2009;28(06):353–354.
19. Li J, Wang X. Observation of the therapeutic effect of electroacupuncture on 40 cases of migraine. Yunnan J Trad Chin Med Mater Med. 2012;33(03):46–47. doi:10.16254/j.cnki.53-1120/r.2012.03.011
20. Peng Y, Zhou J. Observation on the therapeutic effect of electroacupuncture in Qiuxu combined with Shaoyang meridian acupuncture on 32 cases of migraine. Zhejiang J Trad Chin Med. 2018;53(02):134–135. doi:10.13633/j.cnki.zjtcm.2018.02.042
21. Wang Y, Jin H, Li X, Lan J, Zheng Z, Ye Q. A randomized clinical trial about the effect of electro-acupuncture for migraine prophylaxis. Chin Health Stand Manag. 2020;11(02):85–89.
22. Ye G, Ma J. Acupuncture at points of lesser Yang meridians for treatment of migraine. J Liaoning Univ Traditional Chin Med. 2009;11(12):134–135. doi:10.13194/j.jlunivtcm.2009.12.136.yegx.058
23. Zhong G, Li W, Luo Y, et al. Acupuncture at points of the liver and gallbladder meridians for treatment of migraine; a multi- center randomized and controlled study. Chin Acupuncture Moxibustion. 2009;29(04):259–263.
24. Zhou J, Li J, Li N, et al. Transient analgesic effect of electroacupuncture at Taiyang (EX-HN 5) for treatment of migraine with hyperactivity of the liver-yang. Chin Acupuncture Moxibustion. 2007;(03):159–163.
25. Zou S. Observation on the clinical efficacy of eleacupuncture in treating 50 cases of migraine. Chin J Ethnomed Ethnopharm. 2014;(12):51–52. doi:10.3969/j.issn.1007-8517.2014.12.zgmzmjyyzz201412034
26. Amiri P, Kazeminasab S, Nejadghaderi SA, et al. Migraine: a review on its history, global epidemiology, risk factors, and comorbidities. Front Neurol. 2021;12(1664–2295 (Print)):800605. doi:10.3389/fneur.2021.800605
27. Agostoni E, Rigamonti A. Migraine and cerebrovascular disease. Neurol Sci. 2007;
28. Khan J, Asoom LIA, Sunni AA, et al. Genetics, pathophysiology, diagnosis, treatment, management, and prevention of migraine. Biomed Pharmacother. 2021;139(1950–6007 (Electronic)):111557. doi:10.1016/j.biopha.2021.111557
29. Ashina M, Hansen JM, Do TP, Melo-Carrillo A, Burstein R, Moskowitz MA. Migraine and the trigeminovascular system-40 years and counting. Lancet Neurol. 2019;18(8):795–804. doi:10.1016/S1474-4422(19)30185-1
30. Ye S, Wang X, Zhang Y. Research progress in pathogenesis of migraine. Med Recapitulate. 2020;26(06):1086–1091.
31. Ferrari MD, Goadsby PA-O, Burstein R, et al. Migraine. Nat Rev Dis Primers. 2022;8(2056–676X (Electronic)):2. doi:10.1038/s41572-021-00328-4
32. Chen X, Wang X. Advances in non-pharmacological treatments for migraine. Chin J Pain Med. 2015;21(12):928–930.
33. Escher CM, Paracka L, Dressler D, Kollewe K. Botulinum toxin in the management of chronic migraine: clinical evidence and experience. Ther Adv Neurol Disord. 2017;10(2):127–135. doi:10.1177/1756285616677005
34. Gu T, Lin L, Jiang Y, et al. Acupuncture therapy in treating migraine: results of a magnetic resonance spectroscopy imaging study. J Pain Res. 2018;11(1178–7090 (Print)):889–900. doi:10.2147/JPR.S162696
35. Liang Y, Yang L, Mai S, Liu Y, Zhu Y, Chen R. Review on the mechanism of electroacupuncture in the treatment of migraine. Info Trad Chin Med. 2024;41(05):87–91. doi:10.19656/j.cnki.1002-2406.20240515
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.