")
Back to Journals » Journal of Pain Research » Volume 18
Acupotomy for Musculoskeletal Pain: Exploring Therapeutic Potential and Future Directions
Authors Hu J, Tong H , Zhang J , Jiang L
Received 21 January 2025
Accepted for publication 10 June 2025
Published 17 June 2025 Volume 2025:18 Pages 3027—3036
DOI https://doi.org/10.2147/JPR.S518705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Jiatong Hu,1,* Hongxuan Tong,2,* Jiale Zhang,2,3 Lijie Jiang2
1Guanganmen Hospital, China Academy of Chinese Medicine Sciences, Beijing, People’s Republic of China; 2Institute of Basic Theory for Chinese Medicine, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China; 3China Science and Technology Development Center for Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiale Zhang, Email [email protected] Lijie Jiang, Email [email protected]
Abstract: Musculoskeletal pain imposes a significant burden due to its high prevalence and complex pathophysiology. This perspective paper examines the current knowledge regarding the underlying mechanisms of musculoskeletal pain conditions and explores the therapeutic potential of acupotomy. Preliminary evidence suggests that acupotomy holds promise in effectively alleviating pain, improving functional outcomes, and facilitating myofascial tissue healing in individuals with musculoskeletal pain. However, further studies are warranted to elucidate the precise mechanisms through which acupotomy modulates fascia and trigger points, thus influencing pain processing. The targeted and precise nature of acupotomy in addressing specific trigger points and promoting tissue healing offers a promising approach for managing musculoskeletal pain. Nevertheless, additional research is imperative to comprehensively understand its mechanisms of action and optimize treatment protocols. This perspective paper critically contributes valuable insights into the contemporary understanding of musculoskeletal pain and underscores the potential of acupotomy as a valuable treatment modality.
Keywords: musculoskeletal pain, acupotomy, needle knife, myofascial tissue, acupuncture
Introduction
Musculoskeletal pain poses a major public health challenge. It refers to pain originating from muscles, bones, and connective tissues, presenting as either localized discomfort or widespread pain syndromes.1 According to the latest assessment of the Lancet findings,2 the prevalence of musculoskeletal disorders increased significantly from 1990 to 2020, with an estimated 494 million cases globally in 2020. Projections suggest a further increase of 115% by 2050, reaching an estimated 1060 million cases. It is associated with several conditions, including fibromyalgia and myofascial pain syndrome (MPS). Increasing evidence suggests3 that fascia, a connective tissue network enveloping and supporting various anatomical structures in the body, may contribute to generating musculoskeletal pain.4 As a supportive network enveloping muscles, tendons and bones, fascia plays an important structural and functional role. While musculoskeletal pain is highly prevalent and impactful on individuals’ health status, it remains difficult to manage effectively due to its multifactorial etiology and limited treatment options. Elucidating the role of fascia in pain mechanisms could uncover new therapeutic targets and improve current management approaches. This may enhance quality of life for patients suffering from debilitating musculoskeletal pain.5 Further research is warranted to better understand the interplay between fascia and pain generation for more targeted intervention development. Previously regarded as a passive structural component, fascia is now acknowledged as an active sensory organ involved in pain signaling and modulation.6 Furthermore, introducing the concept of musculoskeletal chains,7 considering fascia as an integrated structure, can shift the traditional perception of fascia as separate entities. This paradigm shift opens new avenues for therapeutic interventions targeting the fascia, aiming to alleviate musculoskeletal pain and improve patient outcomes.
In light of this evolving understanding of fascia’s role in musculoskeletal pain, the exploration of novel therapeutic approaches becomes particularly relevant. One such approach is acupotomy, a traditional Chinese medicine technique that involves the precise insertion and manipulation of specially designed acupuncture needles to release musculoskeletal adhesions and restore tissue function.8 To systematically assess the potential of acupotomy in managing musculoskeletal pain, this study aims to evaluate the efficacy, safety, and underlying mechanisms of action of acupotomy in treating various musculoskeletal pain conditions. By synthesizing existing evidence, this study seeks to contribute to the understanding and application of acupotomy for musculoskeletal pain, bridging the gap between fascia-oriented research and clinical practice.
Understanding Musculoskeletal Pain
Musculoskeletal pain refers to pain arising from the musculoskeletal tissues, which form a connective tissue network surrounding and supporting various body structures. It can manifest as localized discomfort or a more widespread pain syndrome. Musculoskeletal pain is often associated with conditions such as MPS and fibromyalgia.9 A clear understanding of its definition and classification is essential to manage and treat musculoskeletal pain effectively. The definition has evolved, recognizing fascia as an active sensory organ involved in pain signaling and modulation rather than solely a passive structural component.10 This paradigm shift has fostered a deeper comprehension of underlying pain mechanisms. Classification is based on anatomical location, clinical presentation, and related conditions. MPS involves trigger points within musculoskeletal tissues characterized by localized hyperalgesia and referred pain. In contrast, fibromyalgia presents as widespread pain and tenderness throughout the body, commonly accompanied by fatigue, sleep disturbances and other systemic symptoms.11
Pathophysiology of Musculoskeletal Pain
The pathophysiology of musculoskeletal pain is complex and involves multiple mechanisms. In general, fascia is now recognized as an intricate collagen-elastin network coursing throughout the body.12 It provides mechanical support, facilitates movement, and acts as a conduit for vasculature and innervation. Regarding pain generation, fascia contains specialized sensory receptors - mechanoreceptors detect mechanical stimuli like tension and compression, while nociceptors sense and transmit pain signals.13 When fascia experiences excessive or prolonged mechanical stress from trauma, inflammation or repetitive movements, it can trigger nociceptor sensitization and the emergence of pain signaling. Musculoskeletal adhesions and restrictions may also develop following trauma, surgery or immobilization. Such adhesions impair the musculoskeletal layers’ normal gliding and sliding, inducing mechanical stress and altering tissue dynamics. This perturbation of fascial mobility can instigate and perpetuate musculoskeletal pain.
Role of Fascia in Musculoskeletal Pain Generation
The role of fascia in pain generation extends beyond its structural function. Fascia contains a rich supply of sensory nerve fibers, including thinly-myelinated Aδand unmyelinated C fibers.14,15 These nerve fibers detect and transmit nociceptive signals, contributing to pain perception.16,17 Fascia also mediates neurogenic inflammation, whereby neuropeptides and inflammatory mediators released from sensory nerve fibers trigger local inflammation and sensitization in musculoskeletal tissues.18,19 Relevant studies20,21 have found that patients with fibromyalgia syndrome have higher high-sensitivity C-reactive protein (hs-CRP) levels than those in the healthy population. Higher hs-CRP levels were significantly associated with higher symptom burden and more tender points. Recent research has also highlighted the concept of musculoskeletal chains,7 emphasizing the interconnectedness and continuity of musculoskeletal structures throughout the body. The musculoskeletal chains absorb the concept of myofascial chains and emphasizes the interconnectedness and continuity of musculoskeletal structures throughout the body.22 This challenges the traditional view of fascia as separate entities and underscores the importance of considering the entire musculoskeletal network in musculoskeletal pain assessment and treatment.23 Dysfunction or imbalance in one area of the chain can potentially impact other regions, contributing to pain and dysfunction. Understanding myofascial’s role in pain generation is crucial for developing effective management strategies for musculoskeletal pain. Therapeutic interventions targeting myofascial aim to restore musculoskeletal mobility, release adhesions, and modulate pain signaling within musculoskeletal tissues. Addressing fascia dysfunction may offer an alternative treatment approach to reduce the musculoskeletal pain burden. Further research is needed to elucidate the complex interplay between fascia and nociception.
Acupotomy: An Overview
Acupotomy, also known as needle-knife therapy, involves the precise insertion and manipulation of specially designed acupuncture needles to address various musculoskeletal conditions.24 It combines elements of acupuncture and surgical principles to achieve therapeutic effects. The term “acupotomy” is derived from the combination of “acupuncture” and “tomy”, which means “to cut” (Figure 1), reflecting its dual function of stimulating meridians and mechanically releasing pathological tissues such as adhesions, scars, or compressive structures. The principles of acupotomy are based on the theory of traditional Chinese medicine, which views health as the harmonious flow of Qi, or vital energy, through the meridians or energy channels of the body. According to this theory, pain and dysfunction occur when the flow of Qi is obstructed or imbalanced.25 Acupotomy aims to restore the smooth flow of Qi by releasing adhesions, removing obstructions, and promoting the circulation of blood and energy in the targeted regions. Modern research26–29 further elucidates its mechanisms, including anti-inflammatory effects, mechanical decompression of nerves and vessels, and endogenous opioid release for analgesia. The practice of acupotomy has a long history in Chinese medicine, dating back several centuries. Its development can be traced to the ancient acupuncture and incision therapy techniques, which were used to treat various ailments. Over time, practitioners began to refine and integrate these techniques, leading to the emergence of acupotomy as a distinct therapeutic modality.
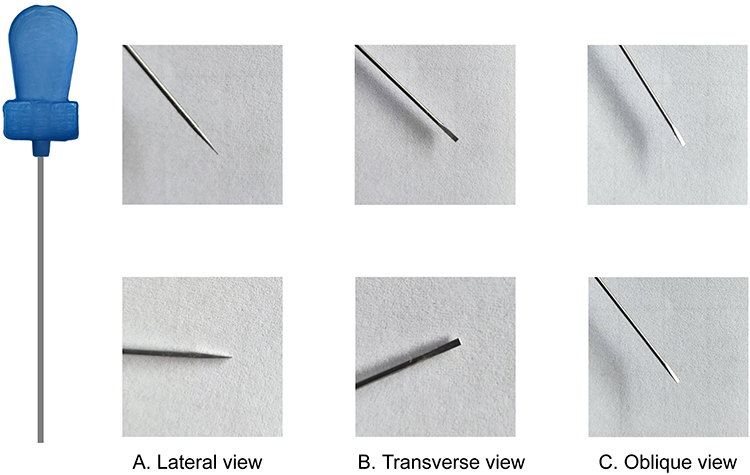 |
Figure 1 Views of the Acupotomy Needle Tip. (A). Lateral view of the acupotomy needle tip. This photograph captures the side profile of the needle tip, highlighting its shape and any distinctive characteristics along its length. (B). Transverse view of the acupotomy needle tip. This image presents a cross-sectional perspective, showcasing the structural features of the needle tip in its width dimension. (C). Oblique view of the acupotomy needle tip. This image provides an angled perspective, offering additional insight into the three-dimensional morphology of the needle tip. |
During the treatment, the acupotomist uses a specialized needle-knife instrument, typically consisting of a sharp, beveled tip and a handle. The instrument is carefully inserted into the skin and directed towards the target area. The acupotomist then performs precise and controlled movements, such as lifting, twisting, or cutting, to release adhesions, separate tissue layers, and stimulate therapeutic effects. The depth of needle insertion and the intensity of manipulation depend on factors such as the patient’s condition, the location of the affected area, and the desired therapeutic outcome.30 Acupotomy can address musculoskeletal conditions, including MPS, soft tissue injuries, joint disorders, and nerve entrapments. It is often combined with other treatment modalities,31,32 such as acupuncture, herbal medicine, and rehabilitative exercises, to enhance its therapeutic effects and promote long-term healing.
Mechanisms of Action
Neurophysiological Effects
One of the key mechanisms of action of acupuncture is its neurophysiological effects. Acupotomy as an enhanced acupuncture treatment, the precise insertion and manipulation of acupuncture needles during acupotomy stimulate nerve fibers in the skin and fascia.33 This stimulation triggers a cascade of neurochemical events, including the release of endogenous opioids, serotonin, and other neurotransmitters.34 The activation of these neurochemical substances produces analgesic effects, reducing pain perception and promoting pain relief. Additionally, the neurophysiological effects of acupotomy can modulate the transmission of pain signals in the central nervous system, helping to regulate pain processing and alleviate chronic pain conditions.
Modulation of Inflammation
Acupotomy has been found to exert modulatory effects on inflammation and the immune response. Inflammation is a common underlying factor in many musculoskeletal conditions and can contribute to pain, tissue damage, and impaired healing. Acupotomy has been shown to reduce the production of pro-inflammatory cytokines and promote the release of anti-inflammatory substances, helping to balance the inflammatory response.35 A study36 investigated the effects of acupotomy on knee osteoarthritis (KOA) and found that it improved synovial oxygen levels, suppressed inflammation and angiogenesis, and downregulated the expression of HIF-1α, VEGF, IL-1β, and TNF-α. These results suggest that acupotomy may be a promising intervention for alleviating inflammation and modulating key inflammatory markers in KOA.
Tissue Healing and Regulating Tension
Acupotomy may promote tissue healing through multiple mechanisms. Precise mechanical stimulation during acupotomy induces controlled microtrauma at target areas. This elicits a localized wound healing cascade by releasing vascular endothelial growth factor,37,38 cytokines and other biomolecules. Additionally, mechanical manipulation of myofascial during acupotomy can help restore normal tissue mobility, release adhesions and improve soft tissue39 tension in affected regions.40 Acupotomy improves the integrity of damaged muscle fibers and segments and promotes the repair of chronically injured skeletal muscles through biomechanical optimization and cellular reconstruction.41 It is worth noting that a study42 aimed to investigate the effects of acupotomy and lidocaine injection on energy crisis in rat trigger points by measuring mechanical pain thresholds and levels of various biochemical markers. The results demonstrated that compared with the model group, acupotomy and lidocaine injection could alleviate energy imbalance at trigger points, while acupotomy was more effective in decreasing AMP and increasing ATP levels. While these mechanistic pathways have been observed in clinical research, the exact molecular and physiological interactions remain under investigation.
In addition to the mechanisms described, additional studies have investigated acupotomy’s impacts from the perspective of mitochondrial autophagy. A study43 examined the effects of needle-knife intervention on mitophagy and mitochondrial function in rabbit knee cartilage. Results demonstrated that PINK1 and Parkin expression, markers of mitophagy, were significantly upregulated post-intervention alongside elevated autophagy levels. Concurrently, mitochondrial performance appeared relatively enhanced. These findings suggest PINK1 and Parkin may participate in the mechanistic pathway whereby needle-knife intervention stimulates mitophagy in chondrocytes, potentially improving mitochondrial quality control and function. Considering mitophagy modulation is important for chondrocyte homeostasis and cartilage integrity, these findings provide novel insight into how acupotomy may exert chondroprotective effects at the cellular level.44 Further molecular studies characterizing acupotomy-driven mitophagy signaling pathways could uncover additional therapeutic targets for joint tissue protection and repair.
Efficacy and Clinical Applications
While meta-analyses45,46 to date have found acupotomy to be potentially effective therapy for musculoskeletal pain, the evidence was limited by risk of bias. These newer clinical trials help bridge some of the previous methodological issues. Much of the existing research47 on fascia-related pain conditions comes from Chinese studies. However, in recent years, more high-quality randomized controlled trials (RCTs) have been published in English. To evaluate emerging evidence on fascia-related pain, we synthesized findings from recent clinical trials (2020–2025) investigating acupotomy’s efficacy for conditions such as low back pain and knee osteoarthritis (Figure 2). Through database searches and manual searches of reference lists, we identified several high-quality trials. Several clinical studies46,48 have investigated the efficacy of acupotomy for musculoskeletal pain. These studies have shown promising results, with acupotomy demonstrating effectiveness in relieving pain, improving functional outcomes, and enhancing quality of life in individuals with musculoskeletal conditions.
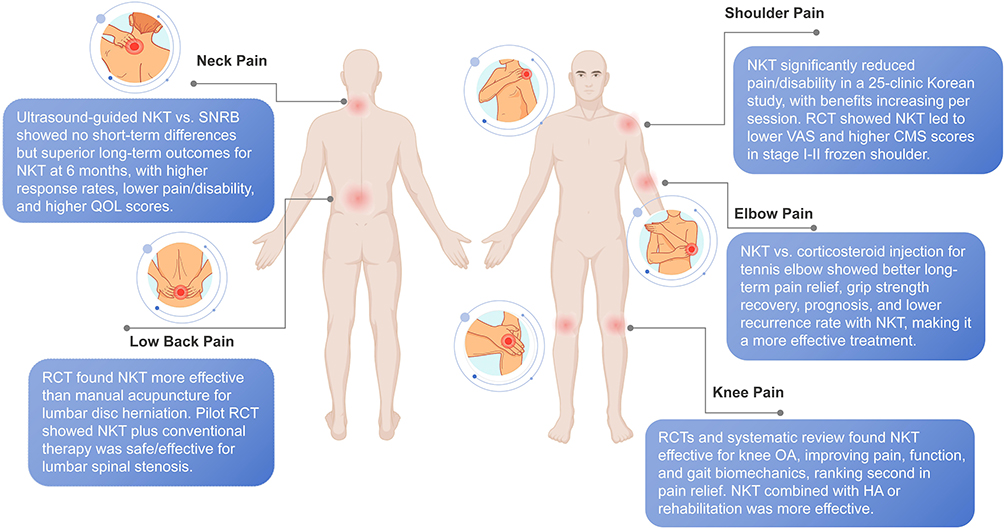 |
Figure 2 Acupotomy Treatment Sites for Various Pain. This figure illustrates the primary treatment sites for acupotomy in addressing various pain. The treatments encompass multiple anatomical regions, highlighting its versatility in managing pain. 1. Neck Pain: Acupotomy is applied to target sites in the neck region to alleviate neck pain. 2. Shoulder Pain: Treatment focuses on the shoulder area, addressing pain and improving function in shoulder conditions. 3. Low Back Pain: Acupotomy is utilized at specific lumbar sites to manage low back pain. 4. Elbow Pain (Tennis Elbow): Targeted treatment is applied to the elbow region to relieve pain associated with tennis elbow. 5. Knee Pain (Knee OA): Acupotomy is directed at the knee joint to improve pain, function, and gait biomechanics in knee osteoarthritis. Abbreviations: RCT, Randomized Controlled Trial; NKT, needle knife therapy; SNRB, selective nerve root block; VAS, Visual Analog Scale; CMS, Constant-Murley Score. |
Neck Pain
A randomized controlled trial (RCT)49 compared the short-term and long-term efficacy of ultrasound-guided injection acupotomy versus selective nerve root block for cervical spondylotic radiculopathy. Results found no differences in pain, function and quality of life scores at 30 minutes and one-month post-treatment. However, at six months, the acupotomy group demonstrated significantly higher “excellent and good” response rates and lower pain, disability and higher quality of life scores based on quantitative scales. These findings suggest ultrasound-guided injection acupotomy may offer superior long-term outcomes for cervical radiculopathy compared to selective nerve root block, supporting its potential role as a minimally invasive alternative intervention worthy of further investigation.
Shoulder Pain
Across 25 Korean clinics, A multicenter retrospective study50 provides quantitative evidence that acupotomy is an effective and safe treatment for shoulder pain. Acupotomy led to clinically significant reductions in pain levels and disability compared to baseline according to validated scales, with progressively greater benefits seen with additional treatment sessions. No serious adverse events occurred. These promising findings suggest acupotomy warrants further rigorous evaluation as a nonsurgical option for managing shoulder pain. Another RCT51 evaluated the efficacy of small needle knife therapy for stage I–II frozen shoulder. Needle knife led to greater decreases in Visual Analog Scale (VAS) scores, larger increases in Constant-Murley scores than the control group. These preliminary findings provide quantitative evidence that small needle knife may effectively manage pain and functional impairments in frozen shoulder when combined with exercise-based rehabilitation.
Low Back Pain
A RCT52 quantitatively evaluated the efficacy and safety of acupotomy versus manual acupuncture for treating back and/or leg pain in patients with lumbar disc herniation. The results demonstrated that compared to manual acupuncture, acupotomy led to significantly greater improvements in pain intensity, range of motion, and functionality as determined by various outcome measures over the 6-week study period. Moreover, acupotomy produced a higher proportion of minimally clinically significant pain reductions. While post-treatment muscle pain occurred with acupotomy, no serious adverse events were reported, indicating it is a preferable treatment to manual acupuncture for lumbar disc herniation. A pilot RCT53 evaluated the effectiveness and safety of acupotomy plus usual care compared to usual care alone for lumbar spinal stenosis. Both groups received acupuncture and interferential current therapy, with the acupotomy group receiving additional acupunctomies. The results demonstrated that while both groups had significant improvements from baseline in back pain, functionality and walking ability over 12 weeks, there were no significant between-group differences. Ultrasound-guided acupotomy (UgA) has proven to be a safe and highly effective treatment option for thoracodorsal myofascial pain syndrome, demonstrating superior outcomes in pain relief, functional improvement, and reduction of pain anxiety when compared to celecoxib.54 Notably, the therapeutic benefits of UgA persisted for three months, underscoring its potential as a promising alternative or supplementary therapy for the management of this painful condition. This provides preliminary evidence that acupotomy appears to be an effective and safe treatment for low back pain. However, larger clinical trials are still needed to validate the outcomes and compare effectiveness to standard therapies.
Elbow Pain
Furthermore, another RCT55 compared the long-term clinical effectiveness of acupotomy versus corticosteroid injection for treating different classifications of tennis elbow. The results demonstrated that while both groups saw improvements in the short term, acupotomy led to significantly greater pain relief, grip strength recovery and better prognosis over 6–48 weeks according to VAS, tenderness, grip and staging assessments. Moreover, acupotomy was associated with a lower recurrence rate than corticosteroid injections. Therefore, this study provides quantitative evidence that acupotomy is a more effective treatment than corticosteroids for managing tennis elbow, especially in the long term, regardless of the specific classification.
Knee Pain
A 2025 single-blind RCT48 compared acupotomy arthroscope with conventional arthroscopic intervention in 73 KOA patients, demonstrating that both modalities significantly improved gait biomechanics, Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores, and Knee Society Scores (P<0.01). While acupotomy arthroscope achieved superior short-term functional gains (gait cycle time, knee flexion angles), arthroscopic intervention showed greater improvements in walking speed and pain relief, highlighting context-dependent therapeutic advantages. These findings align with earlier three evidences: The first study56 found that WOMAC, VAS, structural assessments and plantar pressure demonstrated significantly improvements in knee pain, function and gait biomechanics following acupotomy compared to sham according to quantitative analyses. Beneficial effects were maintained at three-month follow-up. The second study57 demonstrated that combining acupotomy with hyaluronic acid injections led to greater pain reduction and functional improvement than injections alone based on VAS and WOMAC scores. Finally, the third pilot study58 showed small needle-knife therapy plus rehabilitation reduced pain and enhanced function to a greater extent than drugs plus the same rehab according to OKS assessments at three weeks and three months. In the present systematic review59 comparing the clinical efficacy of seven distinct non-pharmacological therapies for knee osteoarthritis, needle-knife therapy emerged as a prominent intervention for pain relief. The analysis, which integrated data from 24 RCTs involving 2582 patients, revealed that needle-knife therapy ranked second in efficacy for reducing pain, as assessed by both the VAS and the WOMAC subscale. These findings underscore the efficacy of needle-knife therapy as a non-pharmacological approach for managing pain in patients with knee osteoarthritis, warranting further investigation and consideration in clinical practice, including integration with patient education on daily care strategies (eg, ergonomic adjustments, rehabilitation protocols) as outlined in recent opinions.60–63
In conclusion, acupotomy has shown promising efficacy in clinical studies for managing musculoskeletal pain. When compared to other treatment modalities, acupotomy offers unique advantages through its targeted tissue intervention and precise manipulation. The most common adverse events64 associated with acupotomy are minor bruising, temporary soreness, and mild bleeding at the needle insertion site.65 These adverse events are typically self-limiting and resolve spontaneously without intervention. While it is generally considered safe, it is essential to receive acupotomy from qualified practitioners to minimize the risk of adverse events. Further research and well-designed clinical trials are needed to strengthen the evidence base and provide more comprehensive guidelines for the clinical application of acupotomy to manage musculoskeletal pain.
Future Directions and Considerations
Optimizing Treatment Protocols: Future research in acupotomy should focus on refining treatment protocols by investigating the selection of acupotomy points, needle insertion depths, manipulation techniques, and treatment frequency tailored to different musculoskeletal conditions. Additionally, exploring the combination of acupotomy with other modalities, such as acupuncture and rehabilitative exercises, may further enhance outcomes and provide comprehensive approaches to managing musculoskeletal disorders.66
Standardization and Guidelines: Standardizing acupotomy techniques, training, and safety guidelines is essential for ensuring consistent and high-quality care. In 2021, the consensus67 of Chinese experts on the diagnosis and treatment of myofascial pain syndrome (MPS) mentioned that acupotomy shows hope in the treatment of MPS. However, it is crucial to emphasize that the evidence supporting acupotomy, as discussed in the 2024 evidence-based guideline on treating lumbar disc herniation with traditional Chinese medicine,68 is presently deemed to be of low quality. This implies that although acupotomy may exhibit potential benefits, the current body of evidence is not sufficiently strong to definitively establish its efficacy and safety without additional research. Given the sharp tip of acupotomy instruments and the potential risks associated with the procedure, caution should be exercised when using it near major nerves, vessels, or organs. In this regard, future research should give priority to this aspect, with the development of the ACUPOtomy-related AEs CHECKlist (ACUPOCHECK) checklist through the Delphi study providing a relevant reference.69 Therefore, standardized training and protocols are still needed to optimize clinical use and minimize risks.70 Continued research exploring dosage parameters, combination therapies and long-term outcomes, and utilizing the ACUPOCHECK to establish rational safety guidelines will help ensure patient safety and establish acupotomy as an evidence-based option for MPS according to modern consensus guidelines. Furthermore, leveraging real-world data and mechanism-driven stratification (eg, genomic or imaging biomarkers) may identify novel therapeutic niches, particularly for diseases with limited treatment options, such as refractory myofascial pain or post-surgical adhesion syndromes.
Integration with multidisciplinary approaches, such as collaborating with acupuncturists, physical therapists, pain specialists, and other healthcare professionals, can enhance patient care and outcomes. By combining different modalities and addressing various aspects of musculoskeletal conditions, including pain, mobility, tissue healing, and psychosocial factors, a comprehensive and holistic approach can be achieved. Furthermore, future research should explore the cost-effectiveness of acupotomy and integration with other treatments to provide valuable information for healthcare decision-makers and promote its integration into mainstream healthcare systems.
Conclusion
Acupotomy combines acupuncture and surgery, involving the targeted insertion and manipulation of a needle-knife instrument. It shows promise in treating musculoskeletal pain by improving function, and enhancing quality of life. However, more research is needed to establish its efficacy, optimize treatment protocols, and compare it with other modalities. Acupotomy can be integrated with acupuncture and manual therapies for comprehensive care.60 Healthcare professionals should refer patients to qualified practitioners and adhere to safety protocols. The recent surge in registrations of clinical trials involving acupotomy interventions on the International Traditional Medicine Clinical Trial Registry since 2024 signifies a promising future for this ancient yet innovative treatment modality in addressing musculoskeletal pain. With trials focusing on conditions such as knee osteoarthritis, frozen shoulder, cervical spondylosis, and non-specific low back pain across diverse geographical regions, the research community is actively exploring acupotomy’s therapeutic potential. These interventional studies not only underscore the growing interest in traditional medicine but also highlight the need for rigorous scientific validation. As the evidence base expands, it is anticipated that acupotomy will gain broader recognition and integration into mainstream clinical practice, offering new therapeutic options for patients suffering from musculoskeletal disorders. The future of acupotomy research holds promise for advancing our understanding of its mechanisms of action, optimizing treatment protocols, and ultimately improving patient outcomes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Funded by Fundamental Research Funds for the Central Public Welfare Research Institutes (No: YZX-202406); Scientific and Technological Innovation Project of China Academy of Chinese Medical Sciences, NO: CI2023C060YLL.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Smith BE, Hendrick P, Bateman M, et al. Musculoskeletal pain and exercise—challenging existing paradigms and introducing new. Br J Sports Med. 2019;53(14):907–912. doi:10.1136/bjsports-2017-098983
2. Gill TK, Mittinty MM, March LM, et al. Global, regional, and national burden of other musculoskeletal disorders, 1990-2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(11):e670–e682. doi:10.1016/S2665-9913(23)00232-1
3. Langevin HM. Fascia mobility, proprioception, and myofascial pain. Life. 2021;11(7):668. doi:10.3390/life11070668
4. Tantanatip A, Chang KV. Myofascial pain syndrome. In: StatPearls. StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC; 2024.
5. Liu X, Pan F, Wang Q, Wang S, Zhang J. Traditional Chinese Rehabilitation Exercise (TCRE) for myofascial pain: current evidence and further challenges. J Pain Res. 2024;17:2801–2810. doi:10.2147/jpr.S482424
6. Barry CM, Kestell G, Gillan M, Haberberger RV, Gibbins IL. Sensory nerve fibers containing calcitonin gene-related peptide in gastrocnemius, latissimus dorsi and erector spinae muscles and thoracolumbar fascia in mice. Neuroscience. 2015;291:106–117. doi:10.1016/j.neuroscience.2015.01.062
7. Biscarini A. Dynamics of two-link musculoskeletal chains during fast movements: endpoint force, axial, and shear joint reaction forces. Bioengineering. 2023;10(2):240. doi:10.3390/bioengineering10020240
8. Kwon CY, Yoon SH, Lee B. Clinical effectiveness and safety of acupotomy: an overview of systematic reviews. Complement Ther Clin Pract. 2019;36:142–152. doi:10.1016/j.ctcp.2019.07.002
9. Shah JP, Thaker N, Heimur J, Aredo JV, Sikdar S, Gerber L. Myofascial trigger points then and now: a historical and scientific perspective. Pm r. 2015;7(7):746–761. doi:10.1016/j.pmrj.2015.01.024
10. Sikdar S, Srbely J, Shah J, et al. A model for personalized diagnostics for non-specific low back pain: the role of the myofascial unit. Front Pain Res. 2023;4:1237802. doi:10.3389/fpain.2023.1237802
11. Atzeni F, Cazzola M, Benucci M, Di Franco M, Salaffi F, Sarzi-Puttini P. Chronic widespread pain in the spectrum of rheumatological diseases. Best Pract Res Clin Rheumatol. 2011;25(2):165–171. doi:10.1016/j.berh.2010.01.011
12. Manon J, Evrard R, Maistriaux L, et al. Periosteum and fascia lata: are they so different? Front Bioeng Biotechnol. 2022;10:944828. doi:10.3389/fbioe.2022.944828
13. Sluka KA, Clauw DJ. Neurobiology of fibromyalgia and chronic widespread pain. Neuroscience. 2016;338:114–129. doi:10.1016/j.neuroscience.2016.06.006
14. Machi A, Patel A, Ottestad E. Nerve stimulation and neuromodulation for painful nerves: a narrative review. Int Orthop. 2025;49(5):989–996. doi:10.1007/s00264-025-06498-0
15. Fede C, Porzionato A, Petrelli L, et al. Fascia and soft tissues innervation in the human Hip and their possible role in post-surgical pain. J Orthop Res. 2020;38(7):1646–1654. doi:10.1002/jor.24665
16. Kondrup F, Gaudreault N, Venne G. The deep fascia and its role in chronic pain and pathological conditions: a review. Clin Anat. 2022;35(5):649–659. doi:10.1002/ca.23882
17. Schleip R, Gabbiani G, Wilke J, et al. Fascia is able to actively contract and may thereby influence musculoskeletal dynamics: a histochemical and mechanographic investigation. Front Physiol. 2019;10:336. doi:10.3389/fphys.2019.00336
18. Leicht BT, Kennedy C, Richardson C. Inflammatory biochemical mediators and their role in myofascial pain and osteopathic manipulative treatment: a literature review. Cureus. 2022;14(2):e22252. doi:10.7759/cureus.22252
19. Peck MM, Maram R, Mohamed A, et al. The influence of pro-inflammatory cytokines and genetic variants in the development of fibromyalgia: a traditional review. Cureus. 2020;12(9):e10276. doi:10.7759/cureus.10276
20. Beiner E, Brenner Miguel S, Friederich HC, Tesarz J. Elevated high sensitive C-reactive protein in fibromyalgia. Front Psychiatry. 2023;14:1237518. doi:10.3389/fpsyt.2023.1237518
21. Xiao Y, Haynes WL, Michalek JE, Russell IJ. Elevated serum high-sensitivity C-reactive protein levels in fibromyalgia syndrome patients correlate with body mass index, interleukin-6, interleukin-8, erythrocyte sedimentation rate. Rheumatol Int. 2013;33(5):1259–1264. doi:10.1007/s00296-012-2538-6
22. Wilke J, Krause F, Vogt L, Banzer W. What is evidence-based about myofascial chains: a systematic review. Arch Phys Med Rehabil. 2016;97(3):454–461. doi:10.1016/j.apmr.2015.07.023
23. Bordoni B, Myers T. A review of the theoretical fascial models: biotensegrity, fascintegrity, and myofascial chains. Cureus. 2020;12(2):e7092. doi:10.7759/cureus.7092
24. Yoon SH, Kim YS, Jo HG, Kwon CY. Current usage of terminologies related to acupotomy: a literature research and standardization suggestion. Chin J Integr Med. 2019;25(2):147–150. doi:10.1007/s11655-018-3015-1
25. Finando S, Finando D. Qi, acupuncture, and the fascia: a reconsideration of the fundamental principles of acupuncture. J Altern Complement Med. 2012;18(9):880–886. doi:10.1089/acm.2011.0599
26. Ma Y, Hu T, Liu N, et al. Acupotomy ameliorates KOA related chondrocyte premature senescence through YAP/FOXD1 pathway. J Pain Res. 2025;18:2011–2023. doi:10.2147/jpr.S475829
27. Wang J, Xiao H, Liang Y. Integration of small needle knife in treating inflammatory factors, Th17 cell function, and magnetic resonance imaging evaluation in osteoporosis complicated by compression fractures in elderly patients. Exp Gerontol. 2025;202:112719. doi:10.1016/j.exger.2025.112719
28. Xiao Y, Zhang Y, Li S, et al. Ultrasound-guided drug injection combined with mini-needle knife therapy for acute lumbar sprain: a prospective interventional study. Eur J Orthop Surg Traumatol. 2025;35(1):108. doi:10.1007/s00590-025-04234-3
29. Liu ZF, Zhang Y, Liu J, et al. Effect of traditional Chinese Non-pharmacological therapies on knee osteoarthritis: a narrative review of clinical application and mechanism. Orthop Res Rev. 2024;16:21–33. doi:10.2147/orr.S442025
30. Lu XH, Chang XL, Liu SL, Xu JY, Gou XJ. Ultrasound-guided inactivation of trigger points combined with muscle fascia stripping by liquid knife in treatment of postherpetic neuralgia complicated with abdominal myofascial pain syndrome: a prospective and controlled clinical study. Pain Res Manag. 2020;2020:4298509. doi:10.1155/2020/4298509
31. Choe G, Hwang JH. Acupotomy combined with Korean medicine treatment in a patient with acute sacroiliac pain unresponsive to conventional therapy: a case report. Explore. 2024;20(5):102999. doi:10.1016/j.explore.2024.04.003
32. Dai W, Wang X, Xie R, et al. Acupotomy combined with massage for cervical spondylotic radiculopathy: a protocol for systematic review and meta-analysis. Medicine. 2020;99(32):e21587. doi:10.1097/md.0000000000021587
33. Carlsson CP, Sundler F, Wallengren J. Cutaneous innervation before and after one treatment period of acupuncture. Br J Dermatol. 2006;155(5):970–976. doi:10.1111/j.1365-2133.2006.07450.x
34. Ahsin S, Saleem S, Bhatti AM, Iles RK, Aslam M. Clinical and endocrinological changes after electro-acupuncture treatment in patients with osteoarthritis of the knee. Pain. 2009;147(1–3):60–66. doi:10.1016/j.pain.2009.08.004
35. Wang C, Zhu JC, Zheng ZW, et al. Effects of acupotomy on partial movement gait and serum tumor necrosis factor-α, interleukin-1β in patients with knee osteoarthritis. Zhongguo Gu Shang. 2022;35(9):848–852. doi:10.12200/j.issn.1003-0034.2022.09.009
36. Guo Y, Xu Y, He M, et al. Acupotomy improves synovial hypoxia, synovitis and angiogenesis in KOA rabbits. J Pain Res. 2023;16:749–760. doi:10.2147/jpr.S396955
37. Ding Y, Shi X, Wang L, et al. Acupotomy versus sodium hyaluronate for treatment of knee osteoarthritis in rabbits. J Tradit Chin Med. 2017;37(3):404–411. doi:10.1016/S0254-6272(17)30078-X
38. Li XH, Liu NG, Guo CQ, et al. Effects of acupotomylysis on basic fibroblast growth factor and CD34 levels in rabbits with third lumbar vertebral transverse foramen syndrome. Genet Mol Res. 2015;14(3):9739–9744. doi:10.4238/2015.August.19.6
39. Li SK, Fan YX, Cao XW, Zhao J, Zhu S, Liu ZQ. Effect of administration of acupuncture stimulation combined with Gushen Zhuyu Decoction on lumbar function in patients with disc herniation. Zhen Ci Yan Jiu. 2022;47(10):907–913. doi:10.13702/j.1000-0607.20210951
40. Guo CQ, Dong FH, Li SL, et al. Effects of acupotomy lysis on local soft tissue tension in patients with the third lumbar vertebrae transverse process syndrome. Zhongguo Zhen Jiu. 2012;32(7):617–620.
41. Liu J, Lin QX, Lu LM, et al. Effect of acupotomy intervention on the morphology and ultrastructure of rectus femoris muscle in rabbits with knee osteoarthritis. Zhongguo Gu Shang. 2022;35(3):281–286. doi:10.12200/j.issn.1003-0034.2022.03.016
42. Zhang Y, Du NY, Chen C, et al. Acupotomy alleviates energy crisis at rat myofascial trigger points. Evid Based Complement Alternat Med. 2020;2020:5129562. doi:10.1155/2020/5129562
43. She ZY, Xia S, Lu M, et al. Effect of acupotomy on mitophagy mediated by PINK1/Parkin pathway in cartilage of rabbits with knee osteoarthritis. Zhen Ci Yan Jiu. 2023;48(9):898–905. doi:10.13702/j.1000-0607.20221011
44. Liu J, Zeng WQ, Lin QX, et al. Acupotomy relieves pain and improves motor function by regulating autophagy and apoptosis of cartilage in rabbits with knee osteoarthritis apoptosis. Zhen Ci Yan Jiu. 2022;47(12):1080–1087. doi:10.13702/j.1000-0607.20211184
45. Fang T, Li Q, Zhou F, et al. Effect and safety of acupotomy in treatment of knee osteoarthritis: a systematic review and Meta-analysis. J Tradit Chin Med. 2020;40(3):355–364. doi:10.19852/j.cnki.jtcm.2020.03.002
46. Sun J, Zhao Y, Zhu R, et al. Acupotomy therapy for knee osteoarthritis pain: systematic review and meta-analysis. Evid Based Complement Alternat Med. 2020;2020:2168283. doi:10.1155/2020/2168283
47. Guo YL, Gao M, Li H, et al. Current status and trend of acupuncture-moxibustion for myofascial pain syndrome: a visual analysis of knowledge graph based on CiteSpace and VOSviewer. Zhongguo Zhen Jiu. 2023;43(9):996–1005. doi:10.13703/j.0255-2930.20230119-k0002
48. Xiong Z, Cheng S, Ge C, et al. A randomized controlled trial: acupotomy Arthroscope vs. arthroscopic intervention in knee OA patients’ gait and symptoms. J Orthop. 2025;70:145–152. doi:10.1016/j.jor.2025.03.020
49. Pu J, Cao W, Chen Y, Fan Y, Cao Y. Ultrasound-guided injection acupotomy as a minimally invasive intervention therapy for cervical spondylotic radiculopathy: a randomized control trial. Ann Med. 2023;55(1):2233556. doi:10.1080/07853890.2023.2233556
50. Chae H, Chu H, Lee J, et al. Effectiveness and safety of acupotomy treatment on shoulder pain: 25 multicenter retrospective study. J Pain Res. 2023;16:1367–1380. doi:10.2147/jpr.S398711
51. Guo S, Liu D, Yang Y, Hu Z. Clinical efficacy of small needle knife therapy on stage I-II frozen shoulder. J Vis Exp. 2023;(201). doi:10.3791/65904
52. Jeong JK, Kim E, Yoon KS, et al. Acupotomy versus manual acupuncture for the treatment of back and/or leg pain in patients with lumbar disc herniation: a multicenter, randomized, controlled, assessor-blinded clinical trial. J Pain Res. 2020;13:677–687. doi:10.2147/jpr.S234761
53. Lee JH, Lee HJ, Woo SH, et al. Effectiveness and safety of acupotomy on lumbar spinal stenosis: a pragmatic, pilot, randomized controlled trial. J Pain Res. 2023;16:659–668. doi:10.2147/jpr.S399132
54. Yanling Z, Hong L, Wang C, et al. Efficacy and safety of ultrasound-guided acupotomy versus celecoxib in patients with thoracodorsal myofascial pain syndrome: a randomized controlled trial. J Integr Complement Med. 2024;30(10):986–994. doi:10.1089/jicm.2023.0490
55. Ge LP, Liu XQ, Zhang RK, Chen ZN, Cheng F. Comparison between acupotomy and corticosteroid injection for patients diagnosed with different classifications of tennis elbow: a randomized control trial. J Orthop Surg Res. 2022;17(1):433. doi:10.1186/s13018-022-03323-x
56. Xu DH, Lin YX, Wei J, et al. Tiaohe Yinyang acupotomy for knee osteoarthritis: a randomized controlled trial. Zhongguo Zhen Jiu. 2022;42(12):1351–1356. doi:10.13703/j.0255-2930.20220126-k0002
57. Chai YP, Han XQ, Cui JZ. Acupotomy combined with intra-articular injection of sodium hyaluronate in the treatment of knee osteoarthritis. Medicine. 2022;101(35):e30225. doi:10.1097/md.0000000000030225
58. Zhu J, Zheng Z, Liu Y, et al. The effects of small-needle-knife therapy on pain and mobility from knee osteoarthritis: a pilot randomized-controlled study. Clin Rehabil. 2020;34(12):1497–1505. doi:10.1177/0269215520938852
59. Cao S, Zan Q, Wang B, Fan X, Chen Z, Yan F. Efficacy of non-pharmacological treatments for knee osteoarthritis: a systematic review and network meta-analysis. Heliyon. 2024;10(17):e36682. doi:10.1016/j.heliyon.2024.e36682
60. Cho E, Yang C, Kim S. The transformation of acupuncture practice using ultrasonography: expert opinions. J Acupunct Meridian Stud. 2024;17(5):165–171. doi:10.51507/j.jams.2024.17.5.165
61. Rafiq MT, A Hamid MS, Hafiz E. Effect of progressive resistance strength training on body mass index, quality of life and functional capacity in knee osteoarthritis: a randomized controlled trial. J Multidiscip Healthc. 2021;14:2161–2168. doi:10.2147/jmdh.S317896
62. Rafiq MT, Hamid MSA, Hafiz E, Chaudhary FA, Khan MI. Feasibility and acceptability of instructions of daily care in overweight and obese knee osteoarthritis participants. Curr Rheumatol Rev. 2021;17(4):421–427. doi:10.2174/1573397117666210727095552
63. Rafiq MT, Abdul Hamid MS, Hafiz E. Effectiveness of lower limb rehabilitation protocol using mobile health on quality of life, functional strength, and functional capacity among knee osteoarthritis patients who are overweight and obese: a randomized-controlled trial. Arch Rheumatol. 2023;38(4):590–601. doi:10.46497/ArchRheumatol.2023.9018
64. Yoon SH, Kwon CY, Jo HG, et al. Safety of acupotomy in a real-world setting: a prospective pilot and feasibility study. J Integr Med. 2022;20(6):514–523. doi:10.1016/j.joim.2022.08.003
65. Jun H, Yoon S-H, Ryu M, et al. Acupotomy in Korean medicine doctors: a preliminary survey on experiences, perceptions, and clinical usage status. Healthcare. 2023;11(18):2577. doi:10.3390/healthcare11182577
66. Zhang J, Zhai X, Wang X, et al. The effect of thunder-fire moxibustion on lumbar disc herniation: study protocol for a randomized controlled trial. Front Public Health. 2022;10:930830. doi:10.3389/fpubh.2022.930830
67. Cao QW, Peng BG, Wang L, et al. Expert consensus on the diagnosis and treatment of myofascial pain syndrome. World J Clin Cases. 2021;9(9):2077–2089. doi:10.12998/wjcc.v9.i9.2077
68. Qin X, Sun K, Xu W, et al. An evidence-based guideline on treating lumbar disc herniation with traditional Chinese medicine. J Evid Based Med. 2024;17(1):187–206. doi:10.1111/jebm.12598
69. Jun H, Lee H, Yoon SH, et al. Delphi study for developing a checklist of adverse events associated with acupotomy. J Integr Med. 2024;22(5):579–587. doi:10.1016/j.joim.2024.08.003
70. Li S. Clinical application of visual minimally invasive acupotomy. Zhongguo Zhen Jiu. 2025;45(1):47–52. doi:10.13703/j.0255-2930.20240403-k0004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Percutaneous Release of the First Extensor Tendon Compartment in De Quervain’s Disease by Acupotomy with US-Guidance: A Cadaveric Study
Shen Y, Zhou Q, Sun X, Li S, Zhang W
Journal of Pain Research 2022, 15:3995-4005
Published Date: 22 December 2022
Effect of Traditional Chinese Non-Pharmacological Therapies on Knee Osteoarthritis: A Narrative Review of Clinical Application and Mechanism
Liu ZF, Zhang Y, Liu J, Wang YY, Chen M, Liu EY, Guo JM, Wang YH, Weng ZW, Liu CX, Yu CH, Wang XY
Orthopedic Research and Reviews 2024, 16:21-33
Published Date: 26 January 2024