")
Back to Journals » International Journal of Women's Health » Volume 17
Acupuncture and Herbal Medicine for Nausea and Vomiting in Pregnancy: An Overview and Quality Assessment of Systematic Reviews
Authors Choi SJ , Choi S , Kim DI
Received 6 January 2025
Accepted for publication 8 April 2025
Published 11 May 2025 Volume 2025:17 Pages 1343—1361
DOI https://doi.org/10.2147/IJWH.S512247
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Vinay Kumar
Su-Ji Choi,1 Seoyoon Choi,2 Dong-Il Kim2
1Department of Obstetrics & Gynecology, College of Korean Medicine, Dong-eui University, Busan, Republic of Korea; 2Department of Obstetrics & Gynecology, College of Korean Medicine, Dongguk University, Goyang-si, Republic of Korea
Correspondence: Dong-Il Kim, Department of Obstetrics & Gynecology, College of Korean Medicine, Dongguk University, 27 Dongguk-ro, Ilsandong-gu, Goyang-si, Gyeonggi-do, 10326, Republic of Korea, Email [email protected]
Background: Up to 85% of pregnant women experience nausea and vomiting in pregnancy (NVP), which can impact both the pregnant woman and developing fetus. Traditional East Asian Medicine (TEAM) including acupuncture and herbal medicine has been used to treat NVP; however, its effectiveness remains under debate. This study aimed to systematically review the existing evidence from systematic reviews on the effectiveness of TEAM for NVP and to critically evaluate the quality of these reviews.
Methods: Nine databases were searched from their inception until January 2024. Search terms included, “Hyperemesis gravidarum”, “Nausea”, “Vomiting”, “acupuncture” and “herbal medicine”. Systematic reviews (SRs) that evaluated the effect of TEAM treatment for NVP were included. We evaluated methodological quality, reporting quality, and risk of bias using the AMSTAR-2, ROBIS tool, and PRISMA guidelines.
Results: In total, 20,121 publications were retrieved from the databases. Twenty-five SRs met the inclusion criteria, indicating that acupuncture and related techniques, and herbal medicines are effective in alleviating NVP. Various methods including traditional acupuncture, acupressure, acupoint injection, electroacupuncture, herbal acupoint patching, and herbal decoctions were used. Herbs like ginger and additional aromatherapies such as lemon and cardamom have also shown beneficial effects. However, there are controversies regarding the consistency of results and the quality of methodologies. Despite low risk of bias across reviews, all were deemed low or critically low in methodological quality, with none fully adhering to PRISMA guidelines.
Conclusion: This comprehensive review underscores the potential of TEAM in managing NVP but highlights significant gaps in research quality and reporting. Future studies of higher methodological quality are essential to validate these findings and guide clinical practice.
Keywords: systematic review, complementary therapies, morning sickness, acupuncture, herbal medicine
Introduction
Nausea and vomiting in pregnancy (NVP) is a common medical condition experienced by pregnant women, with approximately 70–85% suffering from nausea and up to 50% from vomiting.1,2 Severe symptoms such as hyperemesis gravidarum (HG; the severe form of NVP) occur in 0.3–2% of all pregnancies and can have significant negative impacts on both the pregnant woman and developing fetus.
The immediate effects of this condition include significant ketones in urine, rapid weight reduction, nutritional deficiencies, fluid loss, and imbalanced electrolytes.3 When ketone levels in urine become excessive, they can overwhelm kidney function, negatively impacting pregnancy. This makes ketone measurement in urine a crucial parameter for evaluating the severity of hyperemesis gravidarum.4 Without prompt intervention, severe cases may progress to symptoms like jaundice, oliguria, and neurological complications.5 Long-term, women who experience this condition face higher risks of psychological issues including depression and pregnancy avoidance.6,7 Moreover, approximately 10% of pregnant women suffering from hyperemesis gravidarum terminate their pregnancies due to unbearable symptoms and complications.8 Therefore, it’s vital to manage nausea and vomiting during pregnancy and prevent hyperemesis gravidarum from worsening during crucial pregnancy stages to avoid hospitalization, intensive treatment requirements, and negative outcomes for mothers, developing fetuses, and birth results.3
Currently, the etiology of nausea and vomiting during pregnancy (NVP) are not fully understood, but several theories suggest factors such as hormonal changes, gastrointestinal dysmotility, and psychological factors could play a role.9 Despite the availability of pharmacological interventions for NVP, the therapeutic management of this condition remains challenging. Antiemetics may not completely alleviate symptoms, and potential teratogenic effects of medication on the fetus may also decrease medication compliance.10 Concerns about potential adverse effects of pharmacological interventions often lead pregnant women to explore alternative approaches. Among these, Traditional East Asian Medicine (TEAM), including acupuncture, moxibustion, cupping, herbal medicines, and manual therapies, has gained attention for its holistic and noninvasive options.11,12 TEAM is believed to alleviate symptoms primarily through improving digestive function, regulating gastrointestinal motility, providing antiemetic effects, and modulating the autonomic nervous system.13–15
TEAM is one of the most popular CAM practices in the world as well as in East Asian countries. TEAM includes traditional medical systems from China, Korea, Japan, and surrounding regions. According to the cross-national survey conducted in East Asian countries, 34% of the respondents in China, 27% in Japan, 44% in Korea and 34% in Taiwan have used TEAM in the past year.16 In the “equalization” system in Korea and Taiwan and in the “unification” system in China, TEAM is recognized as legitimate medical practices that are equivalent to biomedicine. As a result, medical education, licensing, and health insurance systems in these three countries have established a separate category of TEAM doctors who have rights over all treatment modalities within TEAM, such as acupuncture/moxibustion, herbal medicine and manual therapies.17 Therefore, in these East Asian countries, TEAM is widely utilized within mainstream healthcare systems and is actively employed to manage conditions such as NVP.
Considering such clinical realities, several international guidelines on the treatment of NVP have recommended acupuncture related techniques and ginger as possible options to manage this condition.9,18,19 Numerous clinical researches and reviews have investigated TEAM interventions for NVP. However, comprehensive reviews of overall TEAM interventions for NVP are insufficient,10 leaving the safety and efficacy of TEAM interventions for NVP unclear.9 Additionally, conflicting findings form existing studies make it difficult for healthcare professionals to draw definitive conclusions. The abundance of Systematic reviews (SRs) further complicates the synthesis and effective use of the evidence.20
This study seeks to address these challenges by summarizing the evidence from SRs on the effects of TEAM for NVP and critically evaluating the scientific quality of these reviews. Specifically, we aim to identify consistent findings, clarify uncertainties, and highlight research gaps to guide future studies and improve decision-making in this field. The findings of this study are expected to provide clinicians, researchers, and policymakers with essential information for understanding the evidence base for TEAM in treating NVP and HG and developing effective and safe treatment strategies.
Materials and Methods
Protocol and Registration
The protocol of this review was prospectively registered at the Research Registry (review registry 1678). This overview adheres to the guidelines for overview of SRs in the field of traditional and complementary medicine.20
Eligibility Criteria
Type of Studies
This study included SRs of randomized controlled trials (RCTs) on patients with NVP, including HG. Repeat publications and graduate theses were excluded.
Interventions
This study included SRs of TEAM therapies, including acupuncture-related techniques (eg, acupuncture, acupressure, moxibustion, and cupping), herbal medicines, and manual therapies. Furthermore, studies on TEAM or TEAM plus conventional therapy as an intervention for NVP were included. The following treatments were used in the control group: placebo, sham, no treatment, and conventional treatments.
Outcome
SRs had to include at least one clear outcome in assessing the symptoms of NVP. Examples of such outcomes include the proportion of nausea and vomiting, effective rate, urine ketone levels, blood potassium and sodium level, recurrence rate, termination of pregnancy rate, and prevalence and severity of nausea and vomiting symptoms.
Data Sources and Search Strategy
Nine electronic databases (PubMed, Cochrane Library, EMBASE, CNKI, CiNii, OASIS, ScienceON, KISS, and KMBASE) were searched for potential SRs from their inception until October 08, 2022, and an updated search was conducted on January 8, 2024, to provide an up-to-date comprehensive evidence. No language restrictions were applied. Supplement 1 presents the search strategies applied in each database.
Data Management and Extraction
The following information was extracted from the final study using a data extraction form in Microsoft Excel 2016: the first author’s name, publication year, country, language, number of the included clinical studies, total sample size, details of the participants, interventions of the treatment and control groups, quality assessments tool, whether a meta-analysis was conducted, and main results. All articles were evaluated by two independent investigators, and disagreements between the two investigators were resolved through discussions with a third person.
Quality Assessment
Two independent investigators assessed the methodological quality, reporting quality, risk of bias, and evidence quality using Assessing the Methodological Quality of Systematic Reviews 2 (AMSTAR-2),21 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA)22, Risk of Bias in Systematic Reviews (ROBIS),23 and Grading of Recommendations, Assessments, Development, and Evaluation (GRADE).24 Disagreements between the two investigators were resolved through discussion with a third person.
Umbrella Review Synthesis Methods
The overlap in component RCTs that were included across all eligible reviews was assessed using the Corrected Covered Area (CCA) method.25 A CCA of 100% indicates that every review included in our umbrella review comprised the same component RCTs, while a CCA of 0% indicates that every review in our umbrella review included entirely unique RCTs. The following cut-offs were used to quantify the CCA: 0%–5%=“slight overlap”; 6%–10%=“moderate”; 11%–15%=“high” and >15%=“very high” overlap.25
Results
Results on Literature Search and Selection
In total, 20,121 publications were retrieved from the nine databases. After removing duplicates and screening the titles/abstracts, 82 publications were retrieved for full-text assessment. Examination of these full-text publications resulted in the exclusion of 57 articles. Ultimately, 24 publications were included. The screening and selection procedures are presented in Figure 1. They included 221 unique (component) RCTs and the CCA was 2.96%, indicating slight overlap (Supplement 2). This low overlap is likely due to the diversity of TEAM interventions evaluated.
 |
Figure 1 The flowchart of the literature selection. Abbreviations: SR, Systematic review; NVP, Nausea and vomiting in pregnancy; TEAM, Traditional East Asian Medicine. |
Description of Characteristics
The summarized data extracted from the 24 SRs/MAs are listed in Table 1. These included SRs/MAs published between 2005 and 2024. Six of these articles were written in Chinese,26–31 one32 in Korean, and the remaining ones in English. The number of trials ranged from 4 to 33, and sample size ranged from 504 to 8,986. The intervention in the included studies were largely acupuncture related techniques and herbal medicines. Fifteen studies2,26,27,29–31,33–41 reported the effects of acupuncture-related techniques on NVP and 122,28,32,34,36,37,42–47 reported the effects of herbal medicines. There were no studies on manual therapies. Any interventions that excluded TEAM were included in the control group. In terms of the quality assessment scales, seven studies26,29,30,36,37,42,48 used Jadad, one39 used the Quality of Reports of Meta-analysis of Randomized Controlled Trials (QUOROM) guidelines, another one43 used CASP tool and the remaining ones used the Cochrane Risk of Bias criteria.
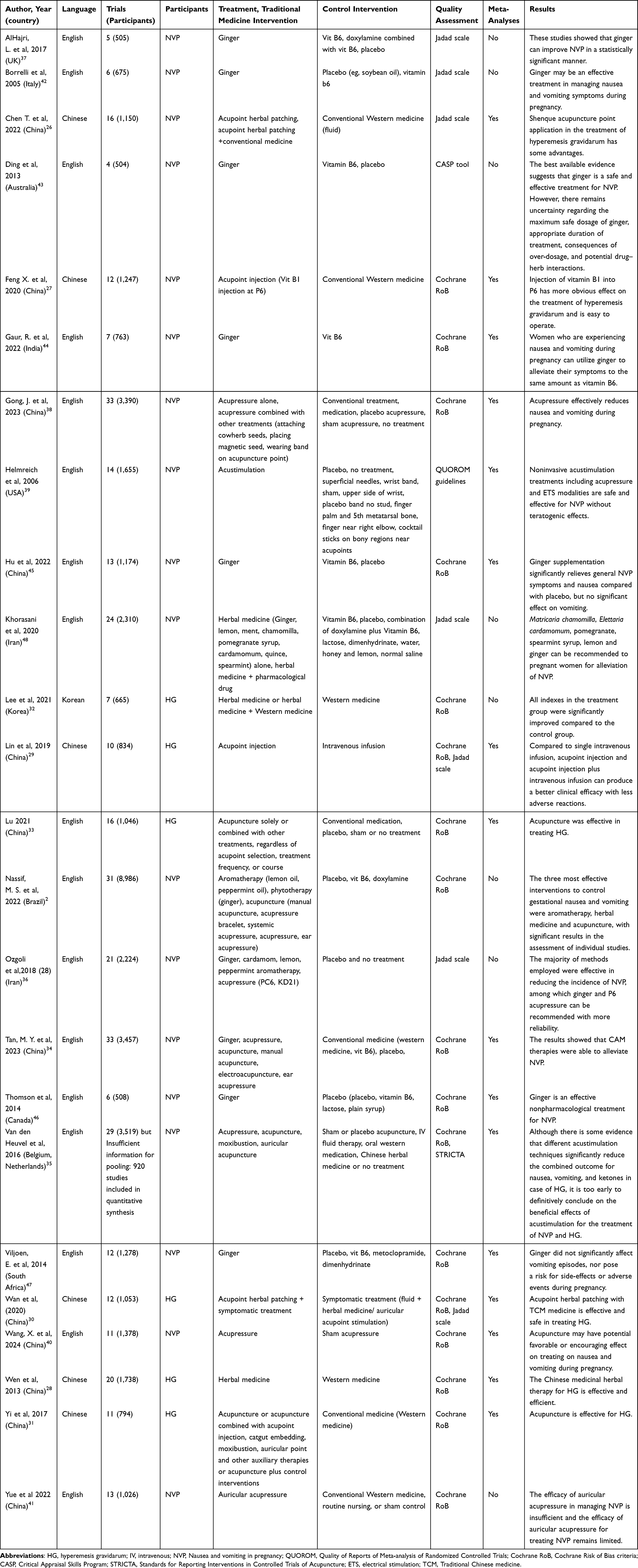 |
Table 1 Main Characteristics of the Included Reviews |
Results of the Methodological Quality
In terms of methodological quality, three trials were regarded as low-quality, and others as critically low-quality. Quality was critically low when more than one critical item was unmet in the included SRs and SRs with just one critical flaw were of low quality. The critical items considered as methodological limitations were as follows: Q 2 (five SRs registered the protocol), Q 4 (only two SRs provided a complete search strategy), Q 7 (two of the SRs provided an excluded studies’ list), Q 9 (five SRs did not conduct an adequate quality assessment), Q 13 (four SRs did not account for the risk of bias when interpreting the results of the review), and Q 11 and 15 (six SRs did not conduct a meta-analysis). These details are presented in Table 2.
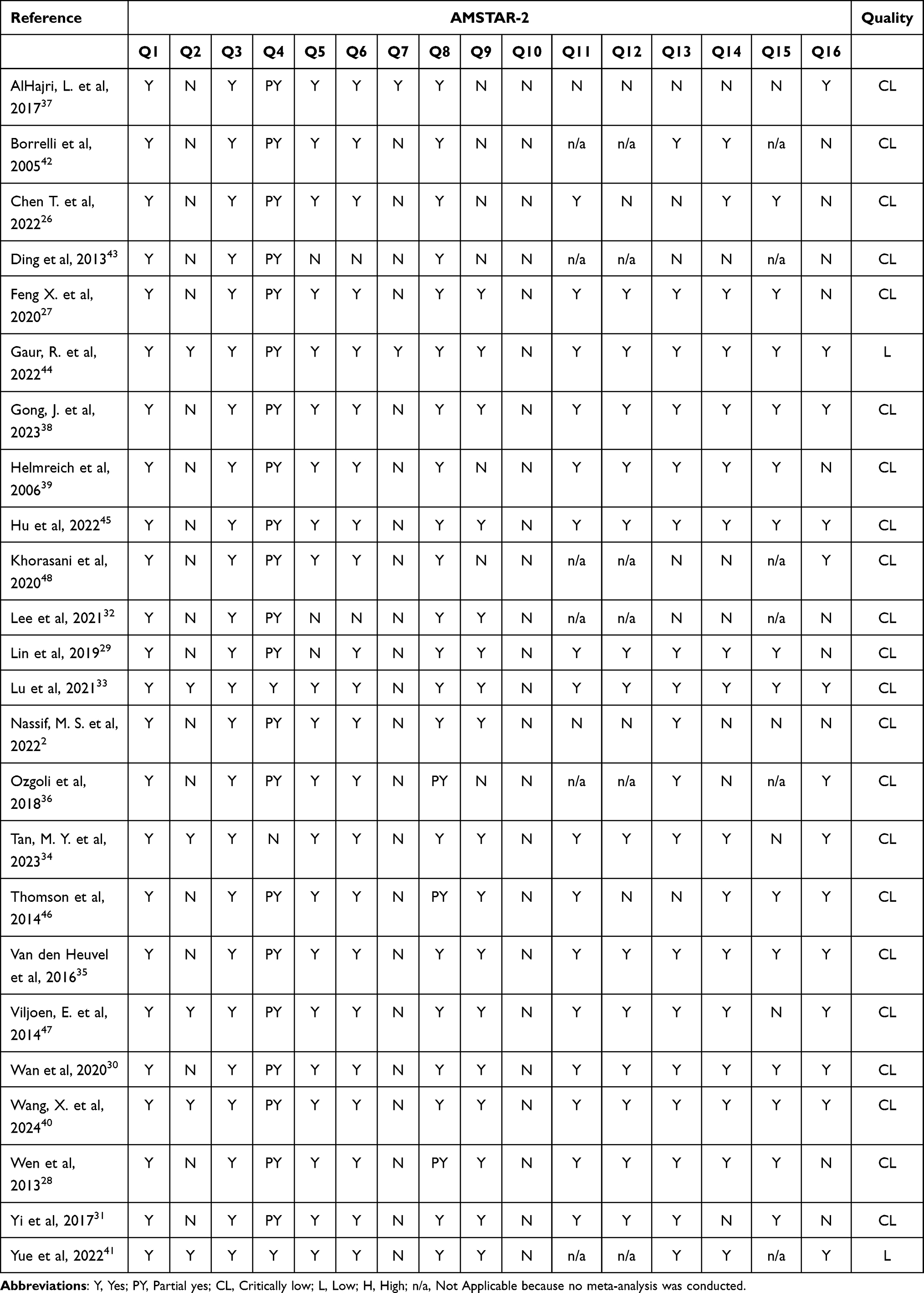 |
Table 2 Results of the AMSTAR-2 Assessment |
Results of the Reporting Quality
We used the 27-item checklist from the PRISMA Statement.22 The aim of the PRISMA Statement is to help authors improve the reporting of systematic reviews and meta-analyses. It may also be useful for the critical appraisal of published systematic reviews.22 An overview of PRISMA assessment for the included SRs is presented in Table 3. Generally, none of the SRs reported all items required for PRISMA. The results showed that seven items were reported in 100% of the SRs (yes or partially yes). When assessing the items of PRISMA, if at least one criterion was not met, it was regarded as “partially yes”, even though most criteria were met. Less than 50% of the included studies reported the items of Protocol and registration, Search, Risk of bias across studies, and Additional analysis in the Methods section; Risk of bias across studies and Additional analysis in the Results section; and the Funding section. Further details are provided in Table 3.
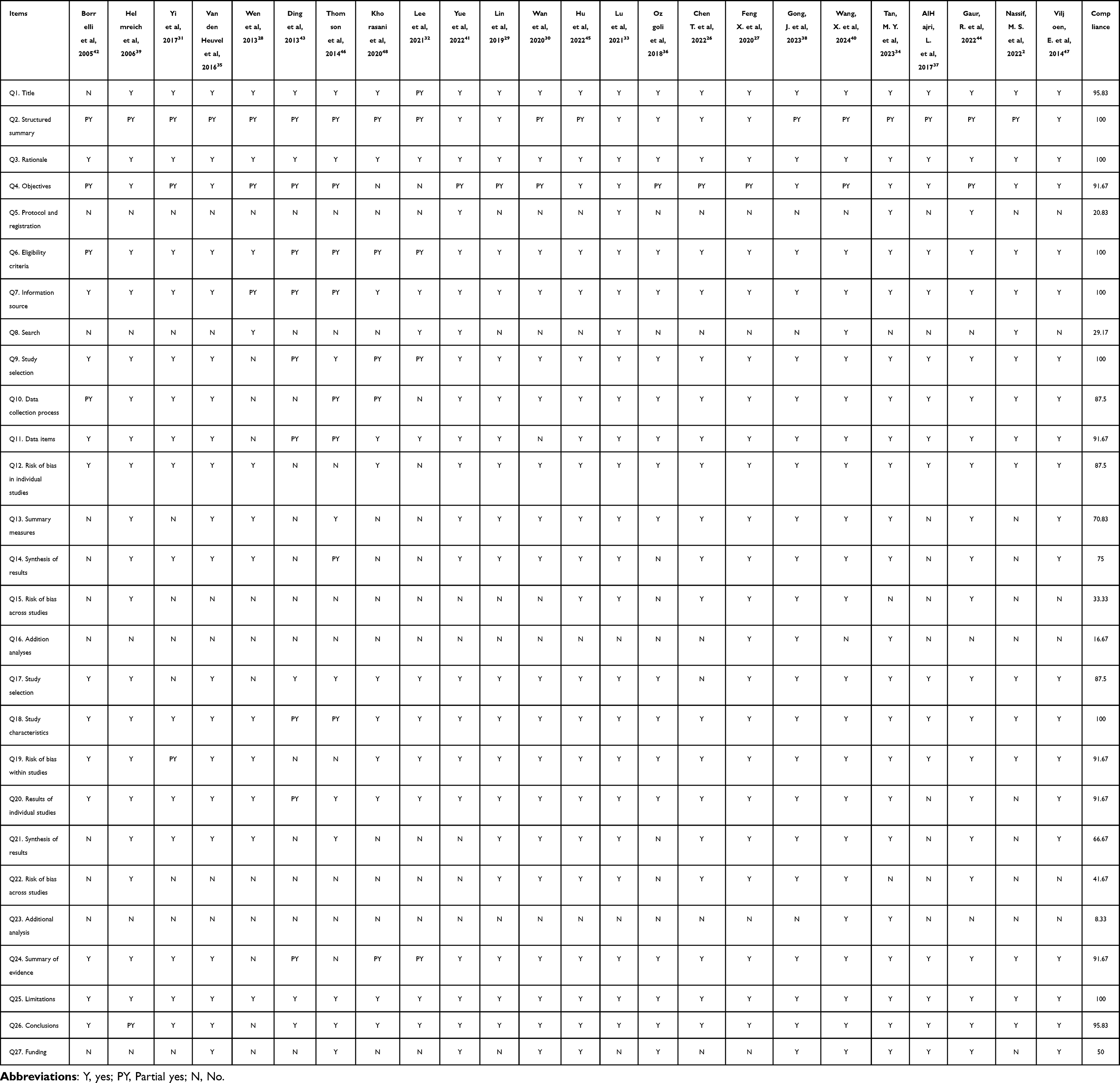 |
Table 3 Results of the PRISMA |
Results of ROBIS Evaluation
In Phase I of the ROBIS, which assesses the relevance of the research topic, all SRs/MAs were rated as low-risk. Domain 1 assessed the study eligibility criteria, and all SRs/MAs except for one were rated as having a low risk of bias. Domain 2 assessed the identification and selection of studies, and 16 SRs/MAs had a low risk of bias. Domain 3 assessed collection and study appraisal, and 17 SRs/MAs had a low risk of bias. Domain 4 assessed the synthesis and findings. Regarding Domain 4, 8 SRs/MAs could not be evaluated because of the lack of data synthesis, and 9 out of 16 SRs/MAs were rated as having a low risk of bias. Phase 3 considered the overall risk of bias in the reviews, and 14 SRs/MAs had a low risk of bias. Additional details are provided in Table 4.
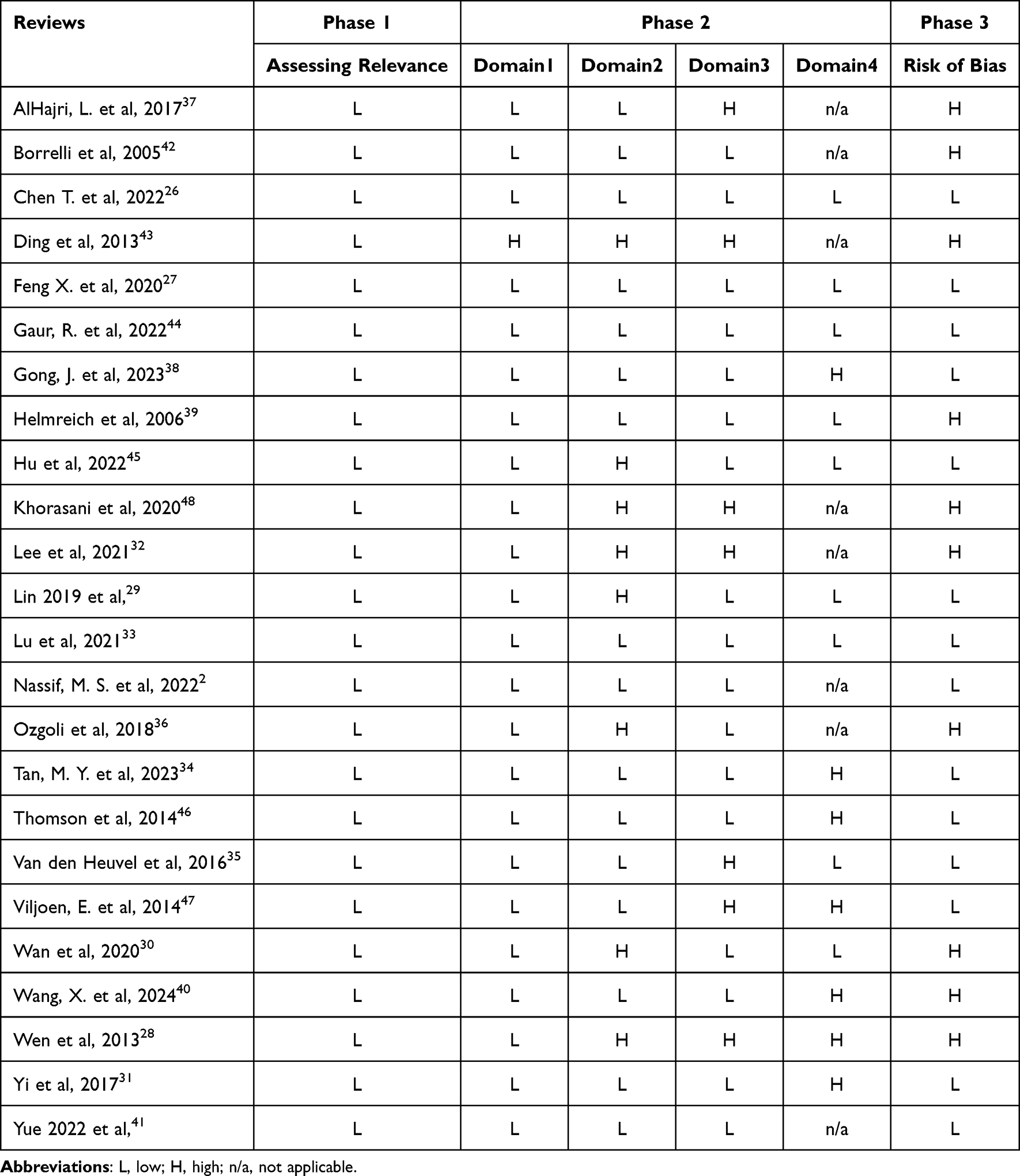 |
Table 4 Results of ROBIS Evaluation |
Evidence Quality
Seventeen out of the 24 SRs/MAs conducted a meta-analysis; 112 outcomes in the 16 SRs/MAs included were evaluated using the GRADE system. The evidence was downgraded owing to limitations within the RCTs, inconsistency, indirectness, imprecision, and publication bias. Details are provided in the Supplement 3.
Effect Evaluation
Acupuncture-Related Techniques
Fifteen studies2,26,27,29–31,33–41 reported the effects of acupuncture-related techniques on NVP. Acupressure, acupuncture, acupoint injection, electroacupuncture, moxibustion, auricular acupuncture or acupressure, acupoint herbal patching, and catgut embedding acupuncture were used as interventions. Proportion of nausea and vomiting, effective rate, urine ketone levels, blood potassium and sodium level, recurrence rate, termination of pregnancy rate, and prevalence and severity of nausea and vomiting symptoms were used as outcome indicators.
Most studies reported that acupuncture-related techniques were effective in NVP, but the effect of these techniques were controversial. According to one review,35 the overall effect of different acustimulation techniques showed a significant reduction in the combined outcome for NVP or HG in pregnancy as a dichotomous variable; however, studies that used continuous outcome measures for nausea, vomiting, and the combined outcome did not show any evidence for acupuncture-related techniques in relieving symptoms of NVP and HG.35
Some studies reported adverse events; however, only one study33 conducted meta-analysis on the safety of the acupuncture-related approaches. One study33 reported that compared with the control set, the random-effects model suggested that the incidence of adverse events in the acupuncture group was lower. Since there were significant differences between the groups (p=0.04).33
One study34 reported that some articles mentioned adverse events of acupressure, including fatigue, sleep disturbance, arm heaviness, vomiting, flatulence, dreaming, and a feeling of coldness, but there were no significant differences between the acupuncture group and control group. Adverse effects of wristbands were reported in some reviews, including pain, numbness, hand swelling, itching, or other allergic reactions.38,39
Most studies reported that they were not able to include the safety results in the analysis because of insufficient data. All these studies suggest that larger sample sizes or high-quality studies are required. Because of the small number of included studies and low quality of the evidence, further studies on the safety of acupuncture treatment are needed in the future.
Traditional Acupuncture
In many studies,2,31,33–35,39 traditional acupuncture points were used, primarily the points that were believed to alleviate nausea and vomiting during pregnancy. Most studies2,31,33–35 generally found traditional acupuncture to be effective in reducing the severity of nausea and frequency of vomiting when compared to placebo or conventional treatment. However, one study39 reported that acupuncture was not effective in reducing NVP and there was a placebo effect on reducing nausea and vomiting compared with controls.
Acupressure
Eight studies2,34–36,38–41 reported that acupressure was beneficial in reducing nausea symptoms among pregnant women. Acupressure with hand and other devices such as wearable band were analyzed together, and acupressure was effective in women with nausea and vomiting during pregnancy.2,34–36,38–41 One study41 analyzed auricular acupoint acupressure alone, and there was a significant difference in effect rate between the treatment and control groups.
Acupoint Injection
Two studies27,29 reported the acupoint injection showed a higher effectiveness rate in controlling severe nausea and vomiting compared to control groups receiving conventional treatment. In one study,27 the use of Vitamin B1 at acupuncture points was specifically highlighted for its effect in providing relief of hyperemesis gravidarum symptoms. One study29 compared the acupoint injection with intravenous infusion, suggesting that acupoint injection and acupoint injection with intravenous infusion can produce a better clinical effect with less adverse reactions compared to single intravenous infusion.
Electroacupuncture
It was difficult to find studies evaluating the effect of electroacupuncture alone. One study34 assessed the effectiveness of electroacupuncture by combining it with other studies with acupuncture interventions, and confirmed that its effect was significantly higher compared to conventional medicine (P = 0.042).
Acupoint Herbal Patching
Two studies26,30 reported that acupoint herbal patching showed a higher effectiveness rate compared to the treatment used in the control group. One study26 analyzed the herbal patching on CV8, and another one30 did not specify the acupuncture points used. Acupuncture patch therapy is relatively safe compared to other methods because it can be applied without oral medication. However, further analysis of acupuncture points and herbs used is needed.
Herbal Medicine
Herbal Medicine Decoction
Two studies28,32 investigated the effects of Traditional herbal medicine decoctions on NVP. In both studies, the herbal medicine group showed a higher effect rate and lower recurrence rate than the western medicine group.
Ginger
Twelve studies2,34,36,37,42–49 reported the effect of ginger on NVP. Various main outcome methods such as the Rhodes Index, Visual Analogue Scale, and Pregnancy Unique Quantification of Emesis Score were used. Across several studies, ginger has been consistently shown to reduce the severity of nausea and frequency of vomiting in pregnancy. Most studies compared ginger to placebo and some to vitamin B6, with ginger often performing comparably or better in reducing symptoms. Some studies compared the effects of Western medications (doxylamine, metoclopramide, and dimenhydrinate) with those of ginger, with no significant differences in reducing NVP. Most clinical trials used ginger in daily doses ranging from 750 mg to 1.5 g, typically administered in capsule form. The duration of the studies varied, generally spanning from a few days to several weeks. Ginger was generally well-tolerated with mild side effects. Common side effects were minor, such as stomachaches and heartburns. Some studies noted no significant adverse effects from ginger use. However, ginger should be used with caution in patients taking medications that affect blood clotting or in those on anti-arrhythmic or central nervous system depressants. High doses of ginger may interact with these medications, potentially leading to increased risks of bleeding or other pharmacological interactions43.
Ginger was found to be as effective as vitamin B6 in many cases. However, some meta-analyses suggest that while both treatments are effective, vitamin B6 might be slightly more effective in reducing overall NVP scores44. Nevertheless, ginger provided relief from nausea and vomiting in early pregnancy more effectively than some conventional medicines without the risk of severe side effects, making it a viable non-pharmacological alternative.
Additional Herbs
One study36 included cardamom, lemon, and peppermint aromatherapies. Lemon aromatherapy led to a significant reduction in NVP compared to the placebo, and cardamom powder significantly reduced the severity of NVP; however, aromatherapy with peppermint oil caused no significant reduction in NVP compared to the placebo.
One study48 reviewed various herbal remedies for treating nausea and vomiting in pregnancy (NVP), highlighting their effectiveness and usage. The study showed that herbal medicines such as matricaria chamomilla, Elettaria cardamomum, pomegranate and spearmint syrup, lemon provide safe and effective medical alternatives for treating pregnant women with mild to moderate NVP. Cardamom was effective for treating NVP compared to placebo (p<0.001). There was significant difference in NVP between lemon and placebo (p<0.049). Inhalation of peppermint oil did not show a significant difference in vomiting and nausea scores compared to placebo, and the use of mint oil also demonstrated identical effects to placebo in improving symptoms before and after treatment. Matricaria chamomilla showed significantly better effects than placebo (p<0.05); however, there was no significant difference between pomegranate and spearmint syrup plus vitamin B, and alone vitamin B.
One study2 included aromatherapy with lemon or peppermint oil. Aromatherapy using lemon essential oil has been shown to effectively reduce gestational nausea and vomiting. In comparison with placebo treatments, aromatherapy demonstrated superior results in about 67% of the studies where it was used, particularly in combination with lemon essential oil. Aromatherapy was generally well tolerated. Less than half of the studies reported adverse effects, which were predominantly mild and transient.
Discussion
Our review of the SRs on TEAM treatment strategies for NVP showed that they could be divided into acupuncture-related techniques and herbal medicine. The overall quality of the SRs was low, with many failing to meet key criteria such as protocol registration and the performance of meta-analyses. These methodological limitations likely contributed to inconsistencies in the reported effects of TEAM interventions. Ginger demonstrated consistent short-term effectiveness, while acupuncture-related techniques showed mixed results due to variations in methodologies and study quality. The low quality of evidence and lack of long-term safety data further underscore the need for rigorous future research.
Among the herbal medicine treatments for NVP, ginger has been studied extensively and shown to be effective in treating NVP symptoms. Ginger is considered both an herbal medicine and a food, making it a viable treatment option for patients hesitant to take conventional medication. Although ginger appears safe and effective for short-term use, there are limited data on its long-term safety and effectiveness. Future research should focus on long-term outcomes and more detailed safety profiles of ginger, especially concerning its dosages above 2 g per day and interactions with other medications. There is a need for standardization in the dosages used in trials to better compare effectiveness and safety outcomes across studies. Furthermore, further research is required to determine the safety of complex herbal medicines involving several components.
Acupuncture-related techniques included auricular acupressure, acupuncture, electroacupuncture, ear acupuncture, acupoint herbal patching, acustimulation band, acupoint injection, and thread embedding acupuncture. However, due to low or critically low quality, more high-quality studies are required to establish the effect of acupuncture-related techniques in the management of NVP. In the case of acupuncture treatment, various methods are often combined; therefore, analysis of each specific method of use seems necessary. In the case of acupuncture, it can be easily employed in clinical settings because this treatment method can be used even in cases where oral medication is difficult due to severe nausea and vomiting. Indeed, it can be applied in patients who have difficulty taking oral medication due to severe vomiting.
According to previous studies,50 herbal medicine and acupuncture are the most widely used TEAM interventions for NVP or HG, but cupping, moxibustion, and pharmacopuncture are also widely used. Cupping and moxibustion are non-drug-based interventions and acupuncture-related techniques that stimulate acupuncture points, which can be safely performed, but owing to the lack of related studies the need for clinical research has been confirmed. Moxibustion is also a widely used intervention, but because it provides thermal stimulation, its safety needs to be evaluated. Pharmacopuncture is a novel intervention that is still evolving and is widely used in clinical practice.51 Pharmacopuncture therapy combines acupuncture and herbal medicine, with the injection of herbal extracts into acupoints.52 The two included reviews27,29 evaluated acupoint injection; however, this approach differs from pharmacopuncture which involves the injection of traditional herbal medicines, because it involves the injection of western medications. Although there are some RCTs53–59 on the treatment of NVP by injecting vitamin B6 into acupuncture points, there are no RCTs on pharmacopuncture. Therefore, it is necessary to actively conduct clinical research on pharmacopuncture treatment and update the SR.
This study provides a comprehensive reference to clinical practice, providing an overview of TEAM treatments for NVP. Different studies used varying intervention techniques and outcome measures, making it difficult to draw uniform conclusions about the effect of TEAM interventions. Additionally, there was a lack of clear criteria for the severity of NVP in the included SRs, and in Korean and Chinese language studies, NVP was often encompassed within HG. Future analyses should consider the severity of the condition for more precise evaluations. There were also limited long-term outcome data. Long-term data are important because NVP can be associated with fetal growth and development over time. Many studies lacked long-term follow-up, making it difficult to assess the sustained effect and safety of TEAM interventions for NVP.
Our study also has some limitations. Many of the included SRs were of low or critically low quality according to AMSTAR-2 assessments, which limits the reliability of the conclusions drawn. None of the SRs fully complied with the PRISMA guidelines, indicating potential issues with reporting completeness and transparency. Although the ROBIS tool suggested low risk of bias overall, some domains within individual SRs indicated potential biases that were not fully accounted for. This review included studies published in Chinese, Korean, and English, potentially excluding relevant SRs published in other languages.
We strived to utilize transparent and reproducible methods throughout our study. However, the substantial variation in interventions, designs, execution, and data presentation across the included reviews necessitated the use of judgment in appraising the quality of these systematic reviews and in articulating the standards and criteria employed. Additionally, the process of quality evaluation can be subjective, as different researchers might assess the same factors differently, leading to potential variations in findings across studies. This subjectivity could influence the assessment of study quality. Moreover, inconsistencies in reporting results and a lack of long-term outcome data challenge the robustness of the review’s conclusions, highlighting the need for more comprehensive future research to solidify the evidence base.
Conclusions
This study provides a comprehensive overview of TEAM treatments for NVP, highlighting both acupuncture-related techniques and herbal medicine. Several herbal medicines, particularly ginger, and acupuncture have emerged as promising complementary therapies for alleviating NVP symptoms. However, the reliability of these findings is limited due to methodological weaknesses and inadequate reporting quality observed in existing systematic reviews. Critical gaps include inadequate long-term follow-up assessments and insufficient safety monitoring protocols, which preclude definitive judgments regarding the safety profile of TEAM interventions. Thus, our overview confirms the necessity for future research that rigorously adheres to established methodological guidelines, clearly reports study procedures, and includes comprehensive evaluations of long-term clinical outcomes and safety profiles of TEAM therapies.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Acknowledgments
We thank Sung-Wook Kim, Sumin Jung, Jisoo Kim for their help with data collection or analysis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by both the Traditional Korean Medicine R&D Program funded by the Ministry of Health & Welfare through the Korea Health Industry Development Institute (HF22C0120) and Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (RS-2022-NR074852).
Disclosure
The authors declare no competing interests in this work.
References
1. Piwko C, Ungar WJ, Einarson TR, Wolpin J, Koren G. The weekly cost of nausea and vomiting of pregnancy for women calling the Toronto Motherisk Program. Curr Med Res Opin. 2007;23:833–840. doi:10.1185/030079907x178739
2. Nassif MS, Costa ICP, Ribeiro PM, CdC M, PEd O. Integrative and complementary practices to control nausea and vomiting in pregnant women: a systematic review. Revista da Escola de Enfermagem da USP. 2022;56:e20210515. doi:10.1590/1980-220X-REEUSP-2021-0515en
3. Fejzo MS, Trovik J, Grooten IJ, et al. Nausea and vomiting of pregnancy and hyperemesis gravidarum. Nat Rev Dis Primers. 2019;5(1):62. doi:10.1038/s41572-019-0110-3
4. Boelig RC, Barton SJ, Saccone G, Kelly AJ, Edwards SJ, Berghella V. Interventions for treating hyperemesis gravidarum: a Cochrane systematic review and meta-analysis. J Matern Fetal Neonatal Med. 2018;31(18):2492–2505. doi:10.1080/14767058.2017.1342805
5. McCullough DC, McKinney JA, Patel J, Best K, Wiggins JM, Sanchez-Ramos L. Nausea and vomiting during pregnancy leading to nystagmus, ataxia, and maternal brain injury. Am J Clin Exp Obstet Gynecol. 2022;227(2):327–328. doi:10.1016/j.ajog.2022.03.061
6. McCarthy FP, Khashan AS, North RA, et al. A prospective cohort study investigating associations between hyperemesis gravidarum and cognitive, behavioural and emotional well-being in pregnancy. PLoS One. 2011;6(11):e27678. doi:10.1371/journal.pone.0027678
7. Christodoulou-Smith J, Gold JI, Romero R, et al. Posttraumatic stress symptoms following pregnancy complicated by hyperemesis gravidarum. J Matern Fetal Neonatal Med. 2011;24(11):1307–1311. doi:10.3109/14767058.2011.582904
8. Poursharif B, Korst LM, MacGibbon KW, Fejzo MS, Romero R, Goodwin TM. Elective pregnancy termination in a large cohort of women with hyperemesis gravidarum. Contraception. 2007;76(6):451–455. doi:10.1016/j.contraception.2007.08.009
9. Erick M, Cox JT, Mogensen KM. ACOG practice bulletin 189: nausea and vomiting of pregnancy. Obstet Gynecol. 2018;131:935. doi:10.1097/AOG.0000000000002604
10. Niebyl JR, Goodwin TM. Overview of nausea and vomiting of pregnancy with an emphasis on vitamins and ginger. Am J Clin Exp Obstet Gynecol. 2002;186(5):S253–S255. doi:10.1067/mob.2002.122595
11. Cheung F. TCM: made in China. Nature. 2011;480:S82–3. doi:10.1038/480S82a
12. Kim Y, Lee D, Lim E. Reviewing gravid patients in dept. Gynecology clinic of hospital, college of oriental medicine, Kyung-won Univ. The J Korean Obstet Gynecol. 2001;14:380–392.
13. Li S, Lei Y, Chen JD. Chemotherapy-induced pica in rats reduced by electroacupuncture. Neuromodulation. 2018;21(3):254–260. doi:10.1111/ner.12712
14. Li H, He T, Xu Q, et al. Acupuncture and regulation of gastrointestinal function. World J Gastroenterol. 2015;21(27):8304–8313. doi:10.3748/wjg.v21.i27.8304
15. Lu M-J, Yu Z, He Y, Yin Y, Xu B. Electroacupuncture at ST36 modulates gastric motility via vagovagal and sympathetic reflexes in rats. World J Gastroenterol. 2019;25(19):2315–2326. doi:10.3748/wjg.v25.i19.2315
16. Shim J-M. The relationship between the use of complementary and alternative medicine and the use of biomedical services: evidence from East Asian medical systems. Asia Pac J Public Health. 2016;28(1):51–60. doi:10.1177/1010539515613411
17. Shim J-M, Kim J. Cross-national differences in the holistic use of traditional East Asian medicine in East Asia. Health Promotion Int. 2018;33(3):536–544. doi:10.1093/heapro/daw089
18. National Guideline Alliane (UK). Management of Nausea and Vomiting in Pregnancy. London: National Institute for Health and Care Excellence (NICE); 2021.
19. Tsakiridis I, Mamopoulos A, Athanasiadis A, Dagklis T. The management of nausea and vomiting of pregnancy: synthesis of national guidelines. Obstet Gynecol Surv. 2019;74:161–169. doi:10.1097/OGX.0000000000000654
20. Kim T-H, Tian Z-Y, Liao X, Robinson N. Essential elements required for conducting and structuring an overview of systematic reviews in the field of traditional and complementary medicine. Eur J Int Med. 2022;49:101605. doi:10.1016/j.eujim.2021.101605
21. Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ. 2017;358:j4008. doi:10.1136/bmj.j4008
22. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg. 2010;8:336–341. doi:10.1016/j.ijsu.2010.02.007
23. Whiting P, Savović J, Higgins JP, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. 2016;69:225–234. doi:10.1016/j.jclinepi.2015.06.005
24. Guyatt G, Oxman AD, Akl EA, et al. GRADE guidelines: 1. Introduction—GRADE evidence profiles and summary of findings tables. J Clin Epidemiol. 2011;64(4):383–394. doi:10.1016/j.jclinepi.2010.04.026
25. Pieper D, Antoine S-L, Mathes T, Neugebauer EA, Eikermann M. Systematic review finds overlapping reviews were not mentioned in every other overview. J Clin Epidemiol. 2014;67(4):368–375. doi:10.1016/j.jclinepi.2013.11.007
26. Chen Tingting SJ. Meta analysis of clinical effect of shenque acupoint application on hyperemesis gravidarum. Chin J Ethnomed Ethnopharm. 2022;31(9):83–89.
27. Xin F, Zhongbo X, Lin Y, Shuping Z. meta-analysis and sequential analysis of the efficacy of vitamin B1 injection in treating hyperemesis gravidarum neiguan point (P6). Chin Med Herald. 2020;17(9):87–102.
28. Wen X, Yao Z. Meta-analysis of internal TCM on hyperemesis gravidarum. J Liaoning Univ TCM. 2013;15:163–165.
29. Lin X, Shen Q, Zhuang L. Clinical efficacy of acupoint injection in treating hyperemesis gravidarum: a meta analysis. J Clin Acupunct Moxibustion. 2019;35:62–67.
30. Wan Q, Ou Y, Wang B. A meta-analysis of treating hyperemesis gravidarum by acupoint application. Clin J Chin Med. 2020;12:135–139.
31. Yi L, Yirong W, Chunri L, Zhixing Z. A systematic review and meta-analysis of domestic acupuncture for treatment of hyperemesis gravidarum. J Liaoning Univ TCM. 2017;19:150–152.
32. Lee J-W, Ahn S-Y, Kim D-C. A review of randomized controlled trials on the treatment effects of herbal medicine for hyperemesis gravidarum. The J Korean Obstet Gynecol. 2021;34:62–77. doi:10.15204/jkobgy.2021.34.4.062
33. Lu H, Zheng C, Zhong Y, Cheng L, Zhou Y. Effectiveness of acupuncture in the treatment of hyperemesis gravidarum: a systematic review and meta-analysis. Evid Based Complement Alternat Med. 2021;2731446. doi:10.1155/2021/2731446
34. Tan M-Y, Shu S-H, Liu R-L, Zhao Q. The efficacy and safety of complementary and alternative medicine in the treatment of nausea and vomiting during pregnancy: a systematic review and meta-analysis. Front Public Health. 2023;11:1108756. doi:10.3389/fpubh.2023.1108756
35. Van den Heuvel E, Goossens M, Vanderhaegen H, Sun HX, Buntinx F. Effect of acustimulation on nausea and vomiting and on hyperemesis in pregnancy: a systematic review of Western and Chinese literature. BMC Complement Altern Med. 2016;16:13. doi:10.1186/s12906-016-0985-4
36. Ozgoli G, Saei Ghare Naz M. Effects of complementary medicine on nausea and vomiting in pregnancy: a systematic review. Int J Prev Med. 2018;9:75. doi:10.4103/ijpvm.IJPVM_430_16
37. AlHajri L, AlFalasi M, Abdelrahim M, AlKaabi R. The efficacy of ginger for pregnancy-induced nausea and vomiting: a systematic review. J Nat Remedies. 2017:48–56. doi:10.18311/jnr/2017/18012
38. Gong J, Gu D, Wang H, et al. Effect of acupressure in nausea and vomiting treatment during pregnancy: a meta-analysis. EXPLORE. 2023;20:17–26. doi:10.1016/j.explore.2023.06.015
39. Helmreich RJ, Sypk S, Dune LS. Meta-analysis of acustimulation effects on nausea and vomiting in pregnant women. Explore. 2006;2:412–421. doi:10.1016/j.explore.2006.06.002
40. Wang X, Yang G, Li K, Yang F, Liang X, Wu S. Efficacy and safety of acupressure in nausea and vomiting during pregnancy: a systematic review and meta-analysis of randomized controlled trials. Arch Gynecol Obstetrics. 2024;309(4):1237–1248. doi:10.1007/s00404-023-07313-0
41. Yue SW, Huang YY, Huang CR, Huang WP, Ouyang YQ. Effect of auriculotherapy on nausea and vomiting during pregnancy: a systematic review. Eur J Integr Med. 2022;53:102130. doi:10.1016/j.eujim.2022.102130
42. Borrelli F, Capasso R, Aviello G, Pittler MH, Izzo AA. Effectiveness and safety of ginger in the treatment of pregnancy-induced nausea and vomiting. Obstet Gynecol. 2005;105:849–856. doi:10.1097/01.AOG.0000154890.47642.23
43. Ding M, Leach M, Bradley H. The effectiveness and safety of ginger for pregnancy-induced nausea and vomiting: a systematic review. Women Birth. 2013;26:e26–30. doi:10.1016/j.wombi.2012.08.001
44. Gaur R, Mudgal SK, Kalyani V, et al. Ginger vs vitamin B6 for treating nausea and vomiting during pregnancy: a systematic review and meta-analysis. J South Asian Fed Obstet Gynecol. 2022;14(2):210–217. doi:10.5005/jp-journals-10006-2040
45. Hu Y, Amoah AN, Zhang H, et al. Effect of ginger in the treatment of nausea and vomiting compared with vitamin B6 and placebo during pregnancy: a meta-analysis. J Matern Fetal Neonatal Med. 2022;35:187–196. doi:10.1080/14767058.2020.1712714
46. Thomson M, Corbin R, Leung L. Effects of ginger for nausea and vomiting in early pregnancy: a meta-analysis. J Am Board Fam Med. 2014;27:115–122. doi:10.3122/jabfm.2014.01.130167
47. Viljoen E, Visser J, Koen N, Musekiwa A. A systematic review and meta-analysis of the effect and safety of ginger in the treatment of pregnancy-associated nausea and vomiting. Nutr J. 2014;13:1–14. doi:10.1186/1475-2891-13-20
48. Khorasani F, Aryan H, Sobhi A, et al. A systematic review of the efficacy of alternative medicine in the treatment of nausea and vomiting of pregnancy. J Obstet Gynaecol. 2020;40:10–19. doi:10.1080/01443615.2019.1587392
49. Matthews A, Haas DM, O’Mathúna DP, Dowswell T. Interventions for nausea and vomiting in early pregnancy. Cochrane Database Syst Rev. 2015;2015:CD007575. doi:10.1002/14651858.CD007575.pub4
50. Jung H-J, Choi S-J, Kim D-I. A survey on general public’s experience and perception of Korean medicine treatment for developing clinical practice guideline of nausea and vomiting of pregnancy. J Korean Obstet Gynecol. 2023;36(2):69–84. doi:10.15204/jkobgy.2023.36.2.069
51. Choi S-J, Kim D-I. The review on trend of clinical studies of hominis placenta pharmacopuncture on obstetrics & gynecology diseases. The J Korean Obstet Gynecol. 2019;32:15–25. doi:10.15204/jkobgy.2018.32.1.015
52. Park J, Lee H, Shin B-C, Lee MS, Kim B, Kim J-I. Pharmacopuncture in Korea: a systematic review and meta-analysis of randomized controlled trials. Evid Based Complement Alternat Med. 2016.
53. Mei QX. Clinical observation of acupoint injection therapy in the treatment of severe vomiting in pregnancy in 30 cases. Chin J Ind Med. 2009;26:171. doi:10.13586/j.cnki.yjyx1984.2009.02.00
54. Huijuan Z, Xiaoping W, Guanghong L. Treatment of 73 cases of nausea and vomiting in pregnancy with acupoint injection therapy. J Shandong Univ Trad Chin Med. 1996;8.
55. Jie C, Baixue Z, Xiuxia Y. Clinical experience of acupoint injection with vitamin B1 for the treatment of severe nausea and vomiting in pregnancy. Strait Pharm J. 1997.
56. Jufen X. Acupoint injection for the treatment of 58 cases of pregnancy vomiting: a therapeutic observation. Traffic Med. 1997;11:229.
57. Guanghua Z, Lan D, Chengwen J. Acupoint injection of vitamin B1 at Neiguan for the treatment of 35 cases of severe vomiting in pregnancy. Shaanxi J Trad Chin Med. 2005;26:1089–1090.
58. Yuzhen S, Hongying S. Therapeutic observation of vitamin B1 acupoint blockage treatment for severe vomiting during pregnancy. J Guangdong Med Coll. 2002;20:363.
59. Caixia Y. Analysis of 68 cases of severe vomiting in pregnancy treated by acupoint injection at Neiguan and Zusanli acupoints. J Prim Health Care. 2008;12:732–733.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Acupuncture for Post-Stroke Cognitive Impairment: An Overview of Systematic Reviews
Li L, Yang L, Luo B, Deng L, Zhong Y, Gan D, Wu X, Feng P, Zhu F
International Journal of General Medicine 2022, 15:7249-7264
Published Date: 13 September 2022
The Efficacy and Safety of Acupuncture for Tinnitus-Associated Insomnia: A Protocol for a Systematic Review and Meta-Analysis
Fan L, Gao Y, Zhou J, Hu H, Gao H
Journal of Pain Research 2022, 15:2957-2965
Published Date: 21 September 2022
The Efficacy of Herbs as Complementary and Alternative Therapy in Recovery and Clinical Outcome Among People with COVID-19: A Systematic Review, Meta-Analysis, and Meta-Regression
Komariah M, Amirah S, Maulana S, Abdurrahman MF, Ibrahim K, Platini H, Lele JAJMN, Kohar K, Rahayuwati L, Firdaus MKZH
Therapeutics and Clinical Risk Management 2023, 19:611-627
Published Date: 18 July 2023
The Analgesic Effect and Potential Mechanisms of Acupuncture for Migraine Rats: A Systematic Review and Meta-Analysis
Sun S, Liu L, Zhou M, Liu Y, Sun M, Zhao L
Journal of Pain Research 2023, 16:2525-2542
Published Date: 24 July 2023
Efficacy of Acupuncture-Related Therapy for Migraine: A Systematic Review and Network Meta-Analysis
Liu Y, Wang Y, Mi C, Wang Z, Han Y, Qi X, Ding X
Journal of Pain Research 2024, 17:1107-1132
Published Date: 15 March 2024