")
Back to Journals » Journal of Pain Research » Volume 18
Acupuncture as an Adjunctive Therapy to Etoricoxib for Patients with Acute Gouty Arthritis: Protocol for a Multicenter Randomized Controlled Trial
Authors Wang YR, Liu CZ, Cong Y, Xi YW, Xu YY, Li B, Zhou Y, Tu JF , Fu YM, Chen W, Wang LQ, Shi GX
Received 19 February 2025
Accepted for publication 22 May 2025
Published 9 June 2025 Volume 2025:18 Pages 2889—2900
DOI https://doi.org/10.2147/JPR.S523657
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Yi-Ran Wang,1 Cun-Zhi Liu,1 Yan Cong,2 Ya-Wei Xi,3 Ying-Ying Xu,4 Bo Li,5 Yi Zhou,6 Jian-Feng Tu,1 Yi-Ming Fu,1 Wen Chen,1 Li-Qiong Wang,1 Guang-Xia Shi1
1International Acupuncture and Moxibustion Innovation Institute, School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Department of Rheumatology and Immunology, Lianyungang Affiliated Hospital of Nanjing University of Chinese Medicine, Lianyungang, People’s Republic of China; 3Acupuncture-Moxibustion Department, Liangxiang Hospital of Beijing Fangshan District, Beijing, People’s Republic of China; 4Endocrine Department, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Hangzhou, People’s Republic of China; 5Department of Traditional Chinese Medicine, The First Affiliated Hospital of Xiamen University, School of Medicine, Xiamen University, Xiamen, People’s Republic of China; 6Endocrine Department, Xiamen Hospital of Traditional Chinese Medicine, Xiamen, People’s Republic of China
Correspondence: Guang-Xia Shi, International Acupuncture and Moxibustion Innovation Institute, School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, No. 11, Bei San Huan Dong Lu, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Purpose: Acute gouty arthritis (AGA) is often managed with non-steroidal anti-inflammatory drugs. However, patients still tolerate severe pain before the analgesic takes effect. Early adjuvant analgesia is necessary in the pharmacological management of AGA. Acupuncture has the advantage of quick analgesia; nevertheless, the evidence to support the use of early-acupuncture as an adjunctive therapy for AGA is limited. This study aims to assess the efficacy of acupuncture compared with sham acupuncture on pain relief among AGA patients who are concurrently receiving etoricoxib.
Patients and methods: In this multicenter, randomized, controlled trial, total 160 eligible patients with AGA will be randomly allocated into acupuncture group and sham acupuncture group in a 1:1 ratio. All patients will receive oral etoricoxib followed by 30-minute acupuncture or sham acupuncture for 1 session. The primary outcome is the change in pain intensity (Visual Analogue Scale) after the 30-minute acupuncture treatment from baseline. The secondary outcomes include tenderness of study joint, swelling of study joint, rescue medicine, credibility and expectation evaluation and blinding assessment. Adverse events will be recorded during the trial. All the patients who are randomized in this study will be included in the intention-to-treat analysis.
Conclusion: The results of this study will provide evidence for acupuncture used in the treatment of acute gouty arthritis and promote clinical decisions to physicians and patients.
Trial Registration: The protocol has been approved by the Medical Ethical Committee of Beijing University of Chinese Medicine (2023BZYLL0103) and registered at International Traditional Medicine Clinical Trial Registry (ITMCTR2024000218; http://itmctr.ccebtcm.org.cn/zh-CN/UserPlatform/ProjectView?pid=1749b951-b101-418f-8f82-77be3c72ea00).
Keywords: acupuncture, complementary medicine, pain management, acute gouty arthritis
Introduction
Acute gouty arthritis (AGA) is a common and treatable form of inflammatory arthritis. It is caused by excessive precipitation of monosodium urate crystals in articular and non-articular structures. The incidence and prevalence of AGA are on the rise annually.1 Intense acute joint pain, most frequently affecting the first phalangeal joint, is the typical presentation of AGA.2 The pain could be described as stabbing, gnawing or burning.3 Time of the gout flare pain from onset to peak intensity is short, and the pain is always unbearable.4 Gout flares are usually self-limiting over a period of 7–14 days.5 The acute pain associated with AGA results in impaired physical function, restricted social participation and unhealthy psychological state contributing to work absenteeism and low quality of life.6 Moreover, there may be an elevated risk of cardiovascular disease (CVD)7 and venous thromboembolism (VTE).8
Acute pain management is the main expectation of patients suffering from AGA. According to the 2020 American College of Rheumatology Guideline for the Management of Gout recommendations, non-steroidal anti-inflammatory drugs (NSAIDs) are recommended as the first-line analgesic to alleviate acute joint pain of AGA.9 Although pharmacotherapy exhibits significant analgesic efficacy,10,11 it has a relatively slow onset time. These medications typically demand a minimum of 24 hours to achieve adequate pain relief.12,13 Patients still tolerated acute pain until it took effect; only 22% of etoricoxib recipients reported no or mild pain within 4 hours of initial administration.14 Similar results of NSAIDs for AGA have been reported in other clinical trials.15,16 Developing additional therapeutic methods with faster onset and analgesic effect is necessary.
Acupuncture has the advantage of quick analgesia affirmed in research on a range of acute conditions such as renal colic, migraine, low back pain, dental pain and ankle sprain.17–20 Acupuncture has been recommended to be incorporated into the management of acute pain in emergency department.21 Our pilot study found that acupuncture had a rapid analgesic effect among patients with AGA. Pain intensity, measured on a 100-mm Visual Analogue Scale (VAS), was decreased by approximately 10 mm immediately after the acupuncture treatment. The results were consistent with another study exploring the immediate analgesic effect of electroacupuncture combined with diclofenac sodium on AGA.22 Meta-analysis has suggested that acupuncture can offer advantages in treating AGA; however, the quality of the evidence is low.23,24 There are several limitations present in the trials such as methodological deficiency, small sample sizes, absence of sham acupuncture controls and single-center designs. Most clinical trials fail to adequately report the acupuncture intervention details, blinding assessment, randomization methods and allocation concealment. A proportion of trials have small sample sizes and fail to report the calculation methodologies. The absence of sham acupuncture controls, making the blinding of participants impossible and failing to account for placebo effects of acupuncture. Furthermore, the design of single-center trials limits the generalizability of findings. Considering the shortage of previous trials, we designed this trial to investigate whether acupuncture as an adjunctive therapy to etoricoxib could provide immediate analgesic effect for patients with AGA.
Methods
Study Design
This is a multicenter, parallel, two-arm, randomized, controlled trial to testify the efficacy of the combination of acupuncture and drug for patients with AGA. This trial will took place at five study centers in China: The First Affiliated Hospital of Xiamen University, The Third Affiliated Hospital of Zhejiang Chinese Medical University, Lianyungang Affiliated Hospital of Nanjing University of Chinese Medicine, Xiamen Hospital of Traditional Chinese Medicine, Liangxiang Hospital of Beijing Fangshan District. A total of 160 eligible patients with AGA will be included in our study and assigned randomly into two groups: the acupuncture group and the sham acupuncture group in a 1:1 ratio. The total observation period is 1 day. Patients will receive acupuncture or sham acupuncture for 1 session on the day of screening, meanwhile they will be required to take etoricoxib. The SPIRIT schedule is shown in Table 1 and the flow diagram is presented in Figure 1. The protocol will be reported in accordance with the Standard Protocol Items: Recommendations for Interventional Trials guidelines.25
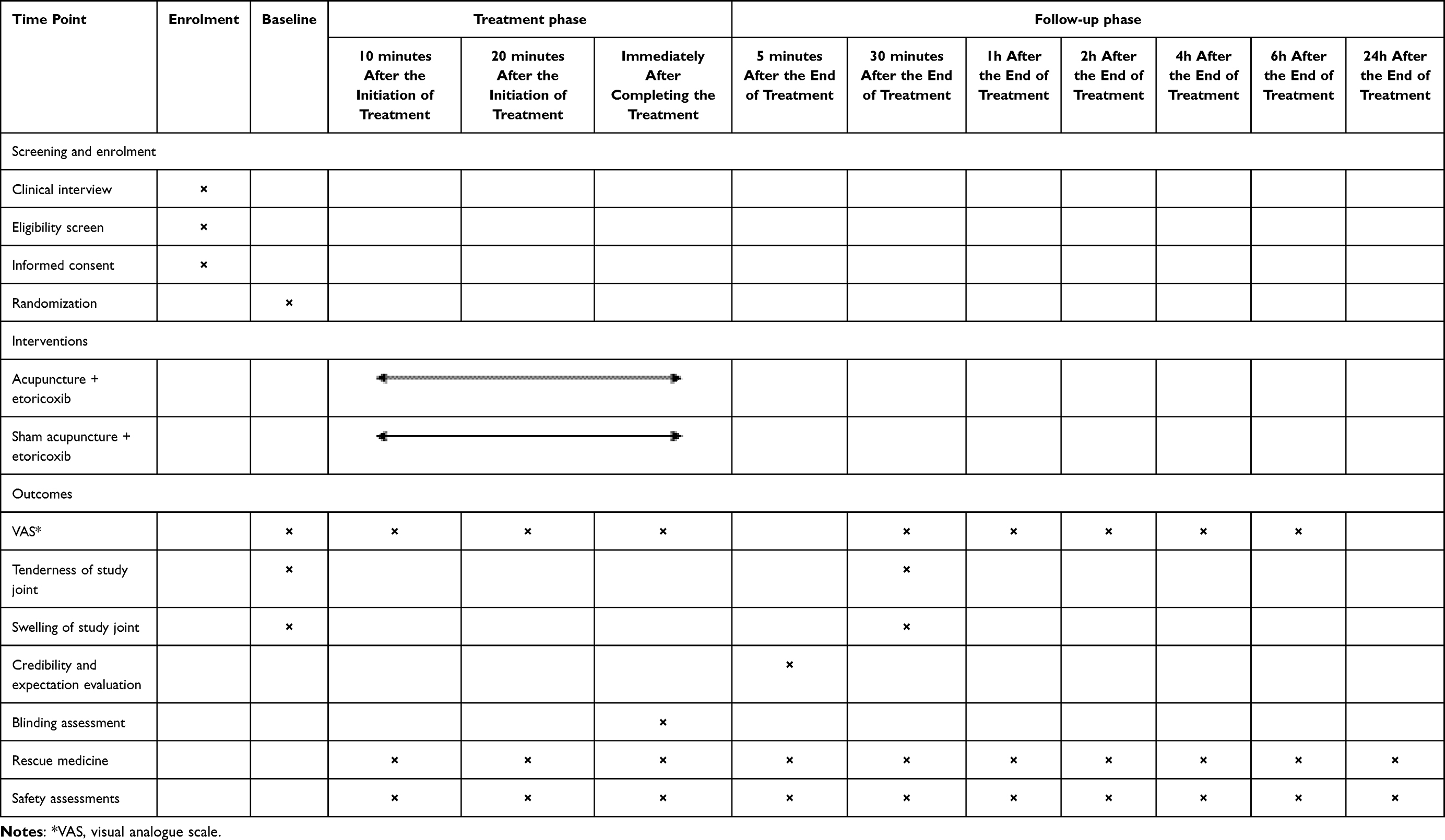 |
Table 1 SPIRIT Schedule |
 |
Figure 1 Flow chart of the trial procedure. |
Recruitment
Patients with AGA will be recruited through emergency departments, rheumatology outpatient clinics, advertisements and other forms in five hospitals. Interested patients will be referred by outpatient physicians to clinical recruiters who will subsequently inform them of the study details. After the screening process based on inclusion and exclusion criteria, eligible patients will participate in this study after signing the written informed consent form. Confidentiality measures will be taken to protect the privacy of patients.
Participants
Inclusion Criteria
- Patients who meet the American College of Rheumatology 1977 preliminary criteria for the classification of AGA and the American College of Rheumatology/European League Against Rheumatism 2015 classification criteria of gout.26,27
- Male or female patients aged between 18 and 75 years.
- Patients who suffer from AGA within 48 hours.
- Patients with pain intensity ≥60 mm on a 100-mm VAS.
- Patients whose unilateral first metatarsophalangeal joint or unilateral ankle joint is affected.
Exclusion Criteria
- Patients who are suspected of infectious arthritis or other joint disease.
- Patients who plan to undergo surgical intervention for gouty tophus or joint correction surgery during the study.
- Patients with active peptic ulcer/gastrointestinal bleeding or history of peptic ulcer/gastrointestinal bleeding.
- Patients with severe acute or chronic organic diseases.
- Patients with history contraindicating the use of drug in the trial (allergy, severe peptic ulcer, hypertension and so on).
- Patients with metal allergy, blood coagulation disorders and severe skin damage at body regions of acupuncture.
- Women who are pregnant, lactating or preparing for pregnancy.
- Patients who have received acupuncture treatment in the last 3 months.
- Patients with history of using glucocorticoid in the last 1 month or using anti-inflammatory and analgesic drugs in the last 24 hours (eg nonsteroidal anti-inflammatory drugs or colchicine).
- Patients who are currently participating in other clinical trials.
Randomization and Blinding
Eligible patients with AGA will be randomly assigned to two groups: the acupuncture group and the sham acupuncture group. The randomization sequence will be generated by the statistician who do not involve in the treatment or the efficacy assessment, using SAS V.9.3 software. The central stratified block randomization approach will be employed, considering the center as the stratification factor. Acupuncturists will obtain the allocation of patients independently through the central randomization system (Electronic Data Capture system, EDC system). The randomization sequence will be hidden in the EDC system until the end of this study. The group assignments information will be blinded to patients, outcome assessors, and statistical analysts. During this trial, blinding assessment of patients will be performed to assess the quality of blinding. However, because of the nature of acupuncture, it is difficult to achieve masking in acupuncturists.
Interventions
Patients will undergo either acupuncture or sham acupuncture treatment for 1 session, which lasts 30 minutes on the day of screening. Meanwhile, they will administer 60 mg etoricoxib (QILU PHARMACEUTICAL CO., LTD) orally that is dispensed by the researchers. Patients especially in different groups will be isolated from each other during the conduct of the trial to minimize their communication. In cases where the pain is severe and intolerable, the rescue drug prednisone acetate (ZHEJIANG XIANJU PHARMACEUTICAL CO., LTD) will be utilized. The details of medication use will be strictly recorded in the EDC system. Certified acupuncturists who have at least 3 years of experience in acupuncture received the operation training of intervention prior to the commencement of the trial.
Acupuncture Group
The acupuncture prescription is determined based on clinical experience and literature.23 The essential acupoints include unilateral zusanli (ST36), sanyinjiao (SP6), yinlingquan (SP9), fenglong (ST40), taichong (LR3) and neiting (ST44). If the affected joint is the first metatarsophalangeal joint, unilateral taibai (SP3) will be selected additionally. While the ankle joint is affected, unilateral qiuxu (GB40) will be added into the acupuncture prescription. The locations of acupoints refer to the 2021 national standard of the People’s Republic of China (GB/T12346-2021) and are presented in Table 2 and Figure 2A. Before inserting needles, the acupuncture sites and the hands of the acupuncturists will be strictly disinfected with 75% alcohol. After pasting disposable sterile foam pads on the acupoints, single-use aseptic needles (length: 25–50mm, diameter: 0.30mm, Hwato, Suzhou, China) will be used and manually stimulated (twirling, lifting and thrusting) to achieve the sensation of “De Qi”. It is defined as the feeling of soreness, numbness, distention or heaviness. The acupuncture manipulation procedure is illustrated in Figure 3A. Acupuncture treatment will consist of 1 session and the needles will be retained for 30 minutes. In the meantime, patients should take 60 mg etoricoxib orally.
 |
Table 2 Acupoints Used in the Acupuncture Group |
 |
Figure 2 (A) is the locations of acupoints. Red points are the essential acupoints used in the acupuncture group; blue points are the adjunct acupoints used in the acupuncture group. (B) is the locations of non-acupoints. Black points are the non-acupoints used in the sham acupuncture group. |
 |
Figure 3 (A) is the schematic diagram of acupuncture manipulation. (B) is the schematic diagram of sham acupuncture manipulation. |
Sham Acupuncture Group
Patients in sham acupuncture group will receive non-penetrating acupuncture at non-acupoints for 30 minutes. After rigorous disinfection and affixing of disposable sterile foam pads that are same to the acupuncture group, the acupuncturist will use disposable sterile blunt-tipped needles to pierce into the foam pads rather than the skin with no manipulation. There will be no “De Qi” sensation. The sham acupuncture manipulation procedure is illustrated in Figure 3B. All details of the locations of non-acupoints are referred to Table 3 and Figure 2B. The remaining procedures are in accordance with those in the acupuncture group.
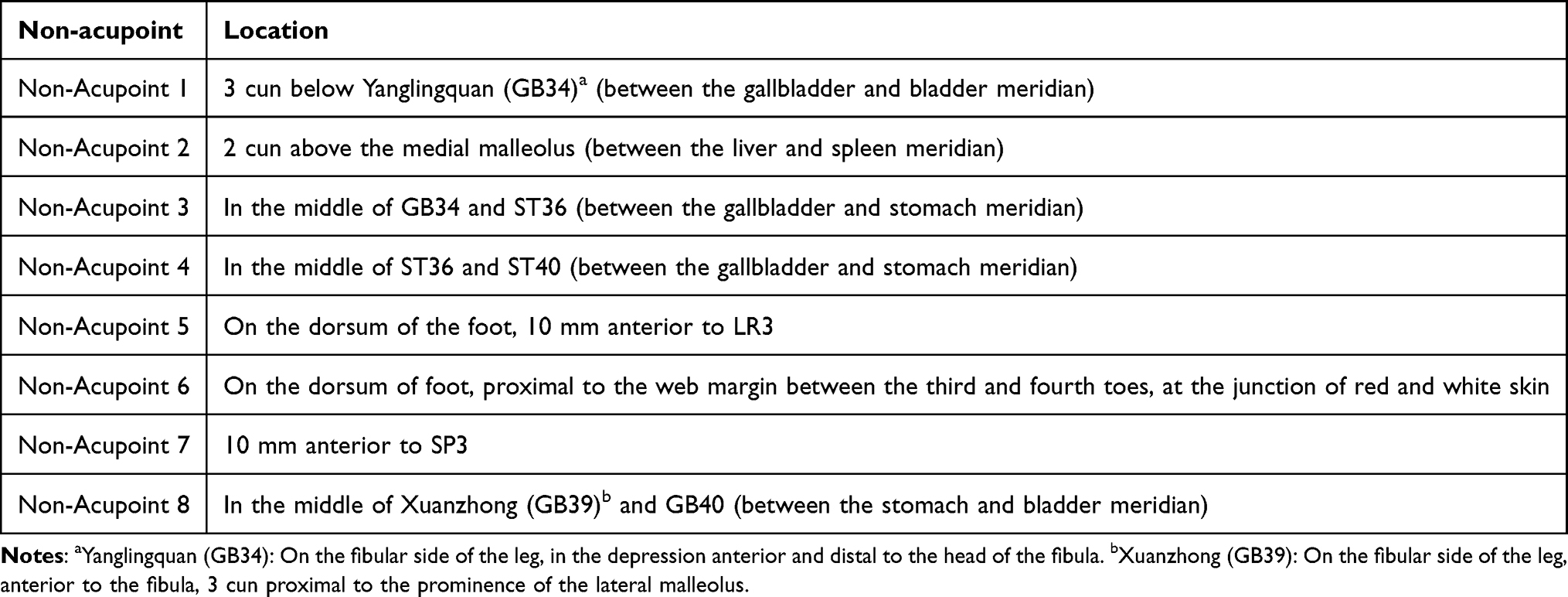 |
Table 3 Non-Acupoints Used in the Sham Acupuncture Group |
Outcomes
Primary Outcome
The primary outcome is the change in pain intensity from baseline to the end of the acupuncture treatment. The VAS scale from 0 to 100 mm in length, which is widely utilized in the assessment of pain, will be employed. The extremes are defined as “no pain” (0) and “unbearable severe pain” (100) without any intermediate points on the line.28 Immediately after completing the treatment, the outcome assessors will inquire about the pain intensity of patients. Subsequently, they will be requested to select an appropriate position to mark on this line, the length of which will be measured by the outcome assessors to represent their pain intensity at this instant.
Secondary outcomes
Change in Pain Intensity at Other Time Points from Baseline
The scores of VAS scale will be recorded at 10, 20 minutes after the initiation of acupuncture or sham acupuncture treatment and 30 minutes, 1h, 2h, 4h, 6h after the end of acupuncture or sham acupuncture treatment (Figure 4). They will be used to calculate the values of change from baseline respectively.
 |
Figure 4 Time points of assessing the pain intensity. |
Tenderness of Study Joint
At baseline and 30 minutes after the end of acupuncture or sham acupuncture treatment, the evaluation of joint tenderness will be assessed by outcome assessors on the basis of palpation. It is scored using a 4-point scale: 0 = no tenderness, 1 = patient complained of tenderness, 2 = patient complained of tenderness and cowering, and 3 = patient complained of tenderness and avoidance. This scale is frequently employed in clinical trials to evaluate symptoms of the affected joint in AGA.14,29–31 High face validity is attributed to its ability to capture the extent of tenderness in the involved joint.28
Swelling of Study Joint
Outcome assessors will assess the joint swelling at baseline and 30 minutes after the end of acupuncture or sham acupuncture treatment. It is a 4-point scale: 0 = no swelling, 1 = palpable swelling, 2 = visible swelling, and 3 = swelling beyond the scope of the joint. This scale has no specialist equipment required which is handy to use in clinical practice.14,29–32 It is high face validity, high acceptance and particularly relevant to AGA which frequently presents as a monoarthritis.28
Credibility and Expectation Evaluation
Five minutes after the end of acupuncture treatment, patients will finish the credibility and expectancy questionnaire of acupuncture. It is a simple-to-administer scale that assesses the impact of expectancy and rationale credibility for use on outcomes.33 This questionnaire includes six items to ask about patients’ perception of therapeutic effect and views on acupuncture treatment.
Blinding Assessment
Prior to the initiation of the trial, patients will be informed that they have an equal chance of being assigned to the two treatment groups. Immediately upon the end of treatment, outcome assessors will determine whether the blinding is successful by querying patients to conjecture, which treatment they have undergone. The James blinding index will be used to assess blinding.
Rescue Medicine
Prednisone acetate will be utilized if the pain is severe and intolerable. Any administration of prednisone acetate within 24 hours will be strictly documented, encompassing the time, the dose and so on.
Safety Assessments
For any adverse events that occur during the trial, researchers are required to document the time of occurrence, classification, severity, implemented measurements, and final resolution in detail. Researchers should upload them to EDC system promptly. In the event of serious adverse events, it is necessary to be reported to the principal investigator within 24 hours. And the patients should be directed to proceed to the treatments by researchers upon receiving instructions from superiors. Adverse events mainly encompassed disease progression, dizziness, subcutaneous hematoma, persistent pain after acupuncture treatment, and so on. All adverse events will be followed up until final resolution.
Sample Size
A pilot study was carried out to assess the feasibility and efficacy of acupuncture combined with etoricoxib in the treatment of AGA (unpublished data). Based on the pilot study and relevant literature researches,34 it is assumed that the difference of the primary outcome between acupuncture group and sham acupuncture group is 10mm with the standard deviation of 21.8mm. The sample size of 76 patients will be required per group to provide 80% power in a 1:1 ratio with a two-tailed α level of 0.05. Due to the short duration of this trial, a dropout rate of 5% is considered. A total of 160 patients (80 patients in each group) needs to be recruited.
Statistical Analysis
An independent statistician, who remains unaware of the group assignments, will conduct the statistical analysis. A p-value of less than 0.05 will be deemed indicative of a statistically significant difference in a two-sided test. Quantitative data that conforms to normal distribution will be presented as mean ± standard deviation (M ± SD). Conversely, if normality is violated, such data will be represented by median (interquartile range). Qualitative data will be described in terms of frequency, constituent ratio, and percentage. All the patients who are randomized in this study will be included in intention-to-treat analysis (ITT) population. Per-protocol analysis will be conducted on patients who complete 1 session of acupuncture or sham acupuncture treatment and provide evaluable data for the primary outcome. Missing data will be addressed through multiple imputation techniques. For the primary outcome, two independent-sample t-test will be employed for comparisons among the two groups if the data are normally distributed. Mixed-effects model with repeated measure, two independent-sample t-test, rank sum test, chi-square test, or Fisher’s test will be used in secondary outcome measures. The Blinding Index will be used to assess blinding.
Data Management
All researchers, including outcome evaluators and inspectors, received comprehensive training in data recording and management prior to the commencement of the trial. The trail data will be recorded in both paper and electronic documents. Researchers responsible for data monitoring at each center will regularly assess the quality of data entry in both paper materials and EDC system. They will identify any existing issues and request relevant researchers in charge to address these concerns promptly. All paper documents will be securely stored in designated lockers by outcome evaluators. The data in EDC system will be safeguarded on a password protected computer. All study-related data will be retained for a minimum of 5 years after the publication of the article. Readers and reviewers can contact the corresponding author to request access to the original data if they have any questions about our published data. Patients’ private information, including names, telephone numbers, and medical conditions, will be maintained with strict confidentiality as permitted by law.
Quality Control
The trial protocol was meticulously reviewed and revised by experts in gout, acupuncture and methodology, who established the standard operating procedures for all aspects of the trial. The study protocol will be submitted to the ethics committee for approval before modification. Prior to the start of the trial, researchers underwent training based on these procedures, which encompassed the objectives of the trial, diagnostic criteria, inclusion and exclusion criteria, randomization processes, acupuncture techniques, evaluation forms, and other relevant components to ensure standardized operations among researchers. Patients will be included strictly in accordance with diagnostic, inclusion and exclusion criteria. If patients do not complete the cycles of treatment and observation as specified in the protocol, researchers should contact them as much as possible to inquire about the reason and to complete the evaluation items. In this study, a combination of paper materials and electronic documents will be employed to collect data objectively. Any issues arising during the trial will be recorded accurately. Patients, outcome assessors, and statisticians will be strictly blinded. Regular monitoring will be carried out by the main center, focusing primarily on the operational procedures and the quality of data within the trial. The data monitoring committee (DMC) will not be established.
Discussion
Pharmacotherapy is recommended as the primary treatment modality, but there still remains a challenge in achieving satisfactory pain relief. Although the administration of first-line drugs provides the relatively consistent analgesic effect, patients still have to endure severe pain until the analgesic takes effect after the initial administration. Acupuncture, with its rapid analgesic effect, has the potential to offer pain relief for patients with AGA during this period. Acupuncture has been already used in acute pain conditions.35,36 A previous clinical trial on the management of acute pain in the emergency department has shown that resolution time of pain was about 15 minutes in acupuncture group.37 Furthermore, acupuncture decreased pain scores by 50% within half the time taken by morphine (14 versus 28 minutes) in a study for acute renal colic.38 Similar results about analgesia have been reported in a trial for symptomatic irreversible pulpitis.39
Multiple centers enhance the representativeness of patients and the generalizability of results. This trial ensures a sufficient sample size, which is calculated based on the pilot study and relevant literature reviews. We chose non-penetrating needles and non-acupoints as controls to reduce the physiological effects of sham acupuncture. Additionally, the researchers received unified standardized training to guarantee adherence to regulated trial procedures. With these rigorous methodologic designs, we believe that the results of this trial will add new evidence of acupuncture effects in AGA.
This study has certain limitations. First, due to the specific nature of acupuncture procedures, it is not feasible for acupuncturists to be blinded. But both patients and outcome assessors will be blinded strictly. Secondly, the treatment cycle is short. Patients receive acupuncture treatment and etoricoxib for 1 session in this trial. Given that NSAIDs require time to take effect upon initial administration, acupuncture can be utilized during this period, leveraging its advantage of rapid analgesia. After the onset of pharmacological action, the analgesic effect of NSAIDs is stable and prolonged. Therefore, acupuncture may not be essential as an adjuvant therapy. Based on these considerations, we design a short treatment period in this trial. Finally, the assessment of primary outcome is relied on subjective indicators, with no objective measures being assessed. Given that pain is inherently a subjective experience, patient self-report remains the gold standard and it is difficult to measure or quantify pain directly.40
Conclusion
This study could evaluate the potential of acupuncture to rapid analgesia during the early management of AGA. The results of this trial are expected to provide evidence for acupuncture to enhance therapeutic efficacy of AGA and improve the life quality of patients. The findings also might improve guidance for protocolized analgesia and offer a new option of adjuvant therapy for patients to alleviate pain. Furthermore, the analgesic effects of acupuncture could potentially reduce dependence on pharmacological analgesics, thereby minimizing drug-related adverse effects and lowering healthcare costs to alleviate the burden on patients.
Data Sharing Statement
All relevant data from this study will be made available upon study completion. Data and material from this trial are available upon reasonable request and approved by the corresponding author.
Ethics Statements
The trial will be carried out in compliance with the ethical principles of the Declaration of Helsinki. This protocol has been approved by the Medical Ethical Committee of Beijing University of Chinese Medicine (2023BZYLL0103) on January 7, 2023, and registered on International Traditional Medicine Clinical Trial Registry (ITMCTR2024000218). During the dissemination phase, the personal information of the patients shall not be disclosed. The results of this study will be published in a peer-reviewed journal and presented at conferences.
Trial Status
This trial is under way. Recruitment of this trial started on August 2024.
Acknowledgments
The authors would like to appreciate the contributions of all the staff that participate in this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas: took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the National Key R&D Program of China(2022YFC3500605).
Disclosure
The authors have declared that no competing interests exist.
References
1. Gill TK, Mittinty MM, March LM; GBD 2021 Other Musculoskeletal Disorders Collaborators. Global, regional, and national burden of other musculoskeletal disorders, 1990-2020, and projections to 2050: a systematic analysis of the global burden of disease study 2021. Lancet Rheumatol. 2023;5(11):e670–e682. doi:10.1016/S2665-9913(23)00232-1
2. Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet. 2021;397(10287):1843–1855. doi:10.1016/S0140-6736(21)00569-9
3. Qaseem A, Harris RP, Forciea MA, et al. Management of acute and recurrent gout: a clinical practice guideline from the American college of physicians. Ann Intern Med. 2017;166(1):58–68. doi:10.7326/M16-0570
4. Taylor WJ, Fransen J, Jansen TL, et al. Study for updated gout classification criteria: identification of features to classify gout. Arthritis Care Res. 2015;67(9):1304–1315. doi:10.1002/acr.22585
5. Dalbeth N, Choi HK, Joosten L, et al. Gout. Nat Rev Dis Primers. 2019;5(1):69. doi:10.1038/s41572-019-0115-y
6. Choi HK, Zhang Y, Dalbeth N. When underlying biology threatens the randomization principle - initial gout flares of urate-lowering therapy. Nat Rev Rheumatol. 2022;18(9):543–549. doi:10.1038/s41584-022-00804-5
7. Cipolletta E, Tata LJ, Nakafero G, Avery AJ, Mamas MA, Abhishek A. Association between gout flare and subsequent cardiovascular events among patients with gout. JAMA. 2022;328(5):440–450. doi:10.1001/jama.2022.11390
8. Cipolletta E, Tata LJ, Nakafero G, Avery AJ, Mamas MA, Abhishek A. Risk of venous thromboembolism with gout flares. Arthritis Rheumatol. 2023;75(9):1638–1647. doi:10.1002/art.42480
9. FitzGerald JD, Dalbeth N, Mikuls T, et al. 2020 American college of rheumatology guideline for the management of gout. Arthritis Care Res. 2020;72(6):744–760. doi:10.1002/acr.24180
10. McKenzie BJ, Wechalekar MD, Johnston RV, Schlesinger N, Buchbinder R. Colchicine for acute gout. Cochrane Database Syst Rev. 2021;8(8):CD006190. PMID: 34438469. doi:10.1002/14651858.CD006190.pub3
11. van Durme CM, Wechalekar MD, Landewé RB, et al. Non-steroidal anti-inflammatory drugs for acute gout. Cochrane Database Syst Rev. 2021;12(12):CD010120. PMID: 34882311. doi:10.1002/14651858.CD010120.pub3
12. Schlesinger N. Difficult-to-treat gouty arthritis: a disease warranting better management. Drugs. 2011;71(11):1413–1439. PMID: 21812506. doi:10.2165/11592290-000000000-00000
13. Dalbeth N, Choi HK, Terkeltaub R. Review: gout: a roadmap to approaches for improving global outcomes. Arthritis Rheumatol. 2017;69(1):22–34. doi:10.1002/art.39799
14. Schumacher HR, Boice JA, Daikh DI, et al. Randomised double blind trial of etoricoxib and indometacin in treatment of acute gouty arthritis. BMJ. 2002;324(7352):1488–1492. doi:10.1136/bmj.324.7352.1488
15. Janssens HJ, Janssen M, van de Lisdonk EH, van Riel PL, van Weel C. Use of oral prednisolone or naproxen for the treatment of gout arthritis: a double-blind, randomised equivalence trial. Lancet. 2008;371(9627):1854–1860. PMID: 18514729. doi:10.1016/S0140-6736(08)60799-0
16. Man CY, Cheung IT, Cameron PA, Rainer TH. Comparison of oral prednisolone/paracetamol and oral indomethacin/paracetamol combination therapy in the treatment of acute goutlike arthritis: a double-blind, randomized, controlled trial. Ann Emerg Med. 2007;49(5):670–677. PMID: 17276548. doi:10.1016/j.annemergmed.2006.11.014
17. Wang Y, Du R, Cui H, Zhang L, Yuan H, Zheng S. Acupuncture for acute migraine attacks in adults: a systematic review and meta-analysis. BMJ Evid Based Med. 2023;28(4):228–240. doi:10.1136/bmjebm-2022-112135
18. Cohen MM, Smit V, Andrianopoulos N, et al. Acupuncture for analgesia in the emergency department: a multicentre, randomised, equivalence and non-inferiority trial. Med J Aust. 2017;206(11):494–499. doi:10.5694/mja16.00771
19. Müller M, Schmucker C, Naumann J, Schlueter N, Huber R, Lederer AK. Acupuncture in management of acute dental pain - A systematic review and meta-analysis. Jpn Dent Sci Rev. 2023;59:114–128. doi:10.1016/j.jdsr.2023.02.005
20. Tu JF, Cao Y, Wang LQ, et al. Effect of adjunctive acupuncture on pain relief among emergency department patients with acute renal colic due to urolithiasis: a randomized clinical trial. JAMA Network Open. 2022;5(8):e2225735. doi:10.1001/jamanetworkopen.2022.25735
21. Fan AY, Miller DW, Bolash B, et al. Acupuncture’s role in solving the opioid epidemic: evidence, cost-effectiveness, and care availability for acupuncture as a primary, non-pharmacologic method for pain relief and management-white paper 2017. J Integr Med. 2017;15(6):411–425. doi:10.1016/S2095-4964(17)60378-9
22. Liu LM, Yin P, Hu JW, Chen YL. Immediate analgesic effect of electroacupuncture combined with diclofenac sodium on acute gouty arthritis: a randomized controlled trial. Zhongguo Zhen Jiu. 2023;43(7):766–770. PMID: 37429655. doi:10.13703/j.0255-2930.20220907-k0001
23. Ni Z, Xiao Q, Xia Z, Kuang K, Yin B, Peng D. Electroacupuncture for acute gouty arthritis: a systematic review and meta-analysis of randomized controlled trials. Front Immunol. 2023;14:1295154. doi:10.3389/fimmu.2023.1295154
24. Fan Y, Zhu C, Ji Y, et al. Comparison of efficacy of acupuncture-related therapies in treating acute gouty arthritis: a network meta-analysis of randomized controlled trials. Heliyon. 2024;10(7):e28122. doi:10.1016/j.heliyon.2024.e28122
25. Chan AW, Tetzlaff JM, Altman DG, et al. SPIRIT 2013 statement: defining standard protocol items for clinical trials. Ann Intern Med. 2013;158(3):200–207. doi:10.7326/0003-4819-158-3-201302050-00583
26. Neogi T, Jansen TL, Dalbeth N, et al. 2015 gout classification criteria: an American college of rheumatology/European league against rheumatism collaborative initiative. Ann Rheum Dis. 2015;74(10):1789–1798. doi:10.1136/annrheumdis-2015-208237
27. Wallace SL, Robinson H, Masi AT, Decker JL, McCarty DJ, Yü TF. Preliminary criteria for the classification of the acute arthritis of primary gout. Arthritis Rheum. 1977;20(3):895–900. doi:10.1002/art.1780200320
28. Dalbeth N, Zhong CS, Grainger R, et al. Outcome measures in acute gout: a systematic literature review. J Rheumatol. 2014;41(3):558–568. doi:10.3899/jrheum.131244
29. Li T, Chen SL, Dai Q, et al. Etoricoxib versus indometacin in the treatment of Chinese patients with acute gouty arthritis: a randomized double-blind trial. Chin Med J. 2013;126(10):1867–1871. doi:10.3760/cma.j.issn.0366-6999.20122892
30. Shu C, Yang F, Zhu F, Hua D. Effect of external use of Qingluo San on clinical efficacy in patients with acute gouty arthritis. Eur J Med Res. 2022;27(1):245. doi:10.1186/s40001-022-00872-z
31. Wang H, Chen ST, Ding XJ, et al. Efficacy and safety of Huzhang Granule, a compound Chinese herbal medicine, for acute gouty arthritis: a double-blind, randomized controlled trial. J Integr Med. 2024;22(3):270–278. doi:10.1016/j.joim.2024.03.008
32. Schlesinger N, Alten RE, Bardin T, et al. Canakinumab for acute gouty arthritis in patients with limited treatment options: results from two randomised, multicentre, active-controlled, double-blind trials and their initial extensions. Ann Rheum Dis. 2012;71(11):1839–1848. doi:10.1136/annrheumdis-2011-200908
33. Devilly GJ, Borkovec TD. Psychometric properties of the credibility/expectancy questionnaire. J Behav Ther Exp Psychiatry. 2000;31(2):73–86. doi:10.1016/S0005-7916(00)00012-4
34. Madsen MV, Gøtzsche PC, Hróbjartsson A. Acupuncture treatment for pain: systematic review of randomised clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ. 2009;338(jan27 2):a3115. doi:10.1136/bmj.a3115
35. Kelly RB, Willis J. Acupuncture for pain. Am Fam Physician. 2019;100(2):89–96.
36. Han JS. Acupuncture analgesia: areas of consensus and controversy. Pain. 2011;152(3 Suppl):S41–S48. doi:10.1016/j.pain.2010.10.012
37. Grissa MH, Baccouche H, Boubaker H, et al. Acupuncture vs intravenous morphine in the management of acute pain in the ED. Am J Emerg Med. 2016;34(11):2112–2116. doi:10.1016/j.ajem.2016.07.028
38. Beltaief K, Grissa MH, Msolli MA, et al. Acupuncture versus titrated morphine in acute renal colic: a randomized controlled trial. J Pain Res. 2018;11:335–341. doi:10.2147/JPR.S136299
39. Murugesan H, Venkatappan S, Renganathan SK, Narasimhan S, Sekar M. Comparison of acupuncture with ibuprofen for pain management in patients with symptomatic irreversible pulpitis: a randomized double-blind clinical trial. J Acupunct Meridian Stud. 2017;10(6):396–401. doi:10.1016/j.jams.2017.09.002
40. Tracey I, Woolf CJ, Andrews NA. Composite pain biomarker signatures for objective assessment and effective treatment. Neuron. 2019;101(5):783–800. doi:10.1016/j.neuron.2019.02.019
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.