")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Adherence to Inhalation Therapy Among COPD Patients: A Cross-Sectional Study in a Tertiary Hospital in Quito, Ecuador
Authors Izquierdo-Condoy JS , Gualpa Álvarez F, Morales-Lapo E, Arias Calvache WD, Bermúdez Moreira J, Quinga-Chiguano KM, Ortiz-Prado E
Received 15 October 2024
Accepted for publication 3 February 2025
Published 21 February 2025 Volume 2025:20 Pages 399—410
DOI https://doi.org/10.2147/COPD.S493992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Min Zhang
Juan S Izquierdo-Condoy,1 Fernando Gualpa Álvarez,2 Estefania Morales-Lapo,1 Washington David Arias Calvache,2 Jessica Bermúdez Moreira,2 Katherine M Quinga-Chiguano,2 Esteban Ortiz-Prado1
1One Health Research Group, Universidad de las Américas, Quito, Ecuador; 2Departamento de Neumología, Hospital Quito No.1 de la Policía Nacional, Quito, Ecuador
Correspondence: Juan S Izquierdo-Condoy, One Health Research Group, Universidad de las Américas, Quito, Ecuador, Email [email protected]
Background: Chronic Obstructive Pulmonary Disease (COPD), the third leading cause of death globally, poses a significant public health burden. Despite its high prevalence, underdiagnosis and poor treatment adherence remain major challenges, contributing to increased hospitalization and mortality.
Purpose: This study aimed to assess adherence to inhalation therapy among COPD patients treated at a specialty hospital in Quito, Ecuador.
Patients and Methods: A cross-sectional study was conducted on 85 patients diagnosed with COPD at a tertiary hospital in Quito. Data was collected through face-to-face surveys, utilizing the TAI-10 questionnaire to assess treatment adherence, along with demographic and clinical characteristics of the patients.
Results: Among the participants, 34.1% demonstrated good adherence to inhalation therapy, while 32.9% exhibited intermediate adherence, and 32.9% were non-adherent. The majority were older adults aged ≥ 76 years (67.1%) with a high prevalence of comorbidities (91.8%), particularly hypertension (58.8%). Non-adherence was primarily associated with forgetfulness and financial constraints. Higher BMI was significantly linked to better adherence, with obese patients showing higher odds of intermediate (OR=7.228, 95% CI 1.866– 27.996) and good adherence (OR=9.966, 95% CI 2.538– 39.139).
Conclusion: Approximately one-third of COPD patients in Ecuador demonstrate good adherence to inhalation therapy, while similar proportions show intermediate or poor adherence. Predominantly older adults and retirees with comorbidities, the population identified forgetfulness and financial constraints as key barriers. These findings emphasize the need for enhanced patient education, regular follow-ups, and tailored support for vulnerable groups.
Keywords: chronic obstructive pulmonary disease, inhaler therapy, inhaled drugs, treatment adherence, low- and middle-income countries
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a progressive condition characterized by airway inflammation and narrowing (chronic bronchitis) and alveolar destruction (emphysema), resulting in air trapping and pulmonary hyperinflation. In the small peripheral airways, key pathological changes include airway wall thickening, mucus plugging, and collapse due to the loss of alveolar attachments. These changes contribute to expiratory flow limitation (EFL), a process where small airways close or collapse during expiration, creating regional choke points within the bronchial tree. EFL exacerbates gas trapping and pulmonary hyperinflation, significantly increasing the symptom burden—particularly dyspnea—and impairing physical performance.1,2 Common symptoms include cough, dyspnea, and sputum production. The development of COPD is influenced by genetic factors, such as alpha-1 antitrypsin deficiency, and environmental exposures like tobacco smoke and pollution, which trigger the disease in susceptible individuals.3–7
According to the World Health Organization (WHO), COPD was the third leading cause of death worldwide in 2019, accounting for 3.23 million deaths, with the highest impact observed in populations from countries with limited economic resources.4,8,9 In the Americas, approximately 13.2 million people are estimated to live with COPD, primarily associated with tobacco use.10 Specifically, Colombia has reported a COPD prevalence of 8.9% among individuals over 40 years of age.11 In Ecuador, while current prevalence rates are unknown, WHO estimates from 2019 indicate that COPD was the eighth leading cause of death, with 14.8 deaths per 100,000 inhabitants, predominantly affecting individuals over 60 years old.10,12 Despite the increasing global incidence of COPD and the importance of early diagnosis, the disease often remains underdiagnosed. Additionally, many COPD patients suffer from various comorbidities, complicating disease management and hindering treatment adherence.9,13,14
Adherence to prescribed medications is vital in managing chronic diseases, including COPD, as it significantly influences disease progression, therapeutic success, and patient survival. WHO defines adherence as the extent to which a patient’s behavior aligns with medical advice, such as taking medications, following diets, and making lifestyle changes. However, adherence rates remain alarmingly low, with only about 50% of chronic disease patients adhering to prescribed regimens.15–17 Adherence to treatment, particularly inhaler therapy, is crucial for achieving optimal patient outcomes. This adherence is based on three fundamental components: initiation, implementation, and persistence, which collectively ensure the regular intake of prescribed medications and improve health outcomes.9,18
Poor treatment adherence in COPD patients has significant consequences, including increased hospitalizations due to exacerbations and a subsequent rise in morbidity and mortality rates.19 Studies have shown that adherence rates are particularly low among patients with chronic diseases, with only about 30% of COPD patients adhering to treatment under real-world conditions.20 In Latin America, the 2017 LASSYC study reported poor or low treatment adherence in 19.4% to 19.9% of COPD patients across several countries.21 Factors contributing to inadequate adherence include polypharmacy, complex dosing regimens, difficulties using inhalation devices correctly, lack of disease awareness, socioeconomic challenges, and patient age.9
In Ecuador, data regarding treatment adherence among COPD patients remains scarce. Therefore, the objective of this research was to assess treatment adherence in COPD patients at a specialty hospital in Quito, Ecuador.
Materials and Methods
Study Design
This study was a cross-sectional analysis conducted on patients diagnosed with COPD at a tertiary specialty hospital in Quito, Ecuador.
Setting and Population
Ecuador, the smallest country in the Andean Mountain region of South America, spans an area of over 283,000 km². The Ecuadorian National Health System is organized into three main sectors: social security, the private sector (self-financed and for-profit institutions), and the public sector (which provides free and open-access medical care).22
For this research, physical and in-person surveys were administered to patients diagnosed with COPD who were treated at the medical clinic of Hospital N1 in Quito. This hospital, part of the National Health System and the Comprehensive Public Health Network, is located in Quito, the capital of Ecuador, at an altitude of approximately 2,850 meters above sea level. The hospital primarily serves active and retired police officers, but also provides care to the general population as part of the Comprehensive Public Health Network.22,23
The analysis included responses from patients treated between May and July of 2024. Data were collected through non-probabilistic convenience sampling, involving all consecutively treated patients who met the selection criteria during the specified period.
Inclusion and Exclusion Criteria
Eligible participants were individuals diagnosed with COPD, aged 18 years or older, with no upper age limit, who had been using inhalation therapies for at least one year and attended outpatient medical care between May 1, 2024, and July 31, 2024. Exclusion criteria included patients under 18 years of age, those diagnosed with other respiratory or pulmonary diseases requiring inhalation therapy, and individuals with a diagnosis of COPD who were not using inhalation therapies.
Survey Development and Measures
The study utilized an anonymous 25-item online questionnaire, originally developed in Spanish, which included the TAI (Test of Adherence to Inhalers) questionnaire,24 to assess adherence to inhalation therapy among COPD patients at the hospital in Quito.
The initial version of the questionnaire was reviewed by a pulmonology expert to ensure its relevance, accuracy, and clarity. After revisions, the final questionnaire was finalized with 25 questions.
A full English version of the final survey instrument is provided in Supplementary File 1.
Variables
The questionnaire collected a range of variables to address the research objectives. Demographic variables included sex, age, occupation, educational level, and history of comorbidities. Additionally, information on lung health was collected, including tobacco use history (non-smoker, former smoker, current smoker), number of pack-years, exposure to biomass, number of COPD exacerbations per year, number of hospitalizations for COPD in the past year, number of inhaled medications, list of inhaled medications, mMRC grade, and GOLD category.
Adherence to inhalers was assessed using the TAI-10 questionnaire, which included 5 response options on a Likert scale, ranging from “always” (1) to “never” (5). Adherence was categorized based on the total score:24
- Good adherence (50 points)
- Intermediate adherence (46–49 points)
- Non-adherence (≤45 points)
Data Collection and Management
The data were collected by two pulmonologist physicians who were part of the research team. Participants completed the anonymous survey during consecutive visits to the physicians’ offices. The physicians conducted interviews with the participants and recorded their responses using the survey instrument. The survey preamble outlined the objectives of the study, assured confidentiality, and included informed consent as a mandatory requirement.
To ensure high data integrity, two team members independently reviewed all responses for errors or inconsistencies, such as implausible age ranges or systematic errors, and excluded these questionnaires from the final sample. Initially, 86 responses were collected, and after filtering, 85 valid responses were included in the analysis.
Bias
To minimize bias, the questionnaire was designed to avoid collecting identifiable information, such as IP addresses. During data analysis, two team members independently reviewed the results, and any discrepancies were resolved collaboratively to ensure the inclusion of only valid responses. These measures enhanced the reliability and credibility of our research findings.
Ethical Statement
This study adhered to the ethical standards outlined in the Declaration of Helsinki. It also complied with the ethical protocols approved by the Ethics Committee of the University of the Americas (CEISH-UDLA) under code 2023-EXC-004. Throughout the study, participant anonymity and voluntary participation were strictly maintained. No personally identifiable or sensitive information was requested or included.
Statistical Analysis
Descriptive statistics were primarily used to analyze responses for each categorical item in the questionnaire, including frequencies, percentages, means, and standard deviations for numerical variables. The Chi-square test was employed to identify relationships between categorical variables and treatment adherence.
A logistic regression model was used to estimate the association between participant characteristics and adherence to inhalers, expressed as odds ratios (OR) with 95% confidence intervals (95% CI).
All tests were two-tailed, with statistical significance set at p < 0.05. Analyses were conducted using IBM SPSS Statistics software for Windows, version 29.0 (IBM Company, Chicago, IL, USA).
Results
Sociodemographic Characteristics
Data were collected from a total of 85 patients with COPD, of whom the majority were men (64.7%, n=55) aged 76 years or older (67.1%, n=57). Most participants were retired (82.4%, n=70) and had completed school as their highest educational level (65.9%, n=56) (Table 1).
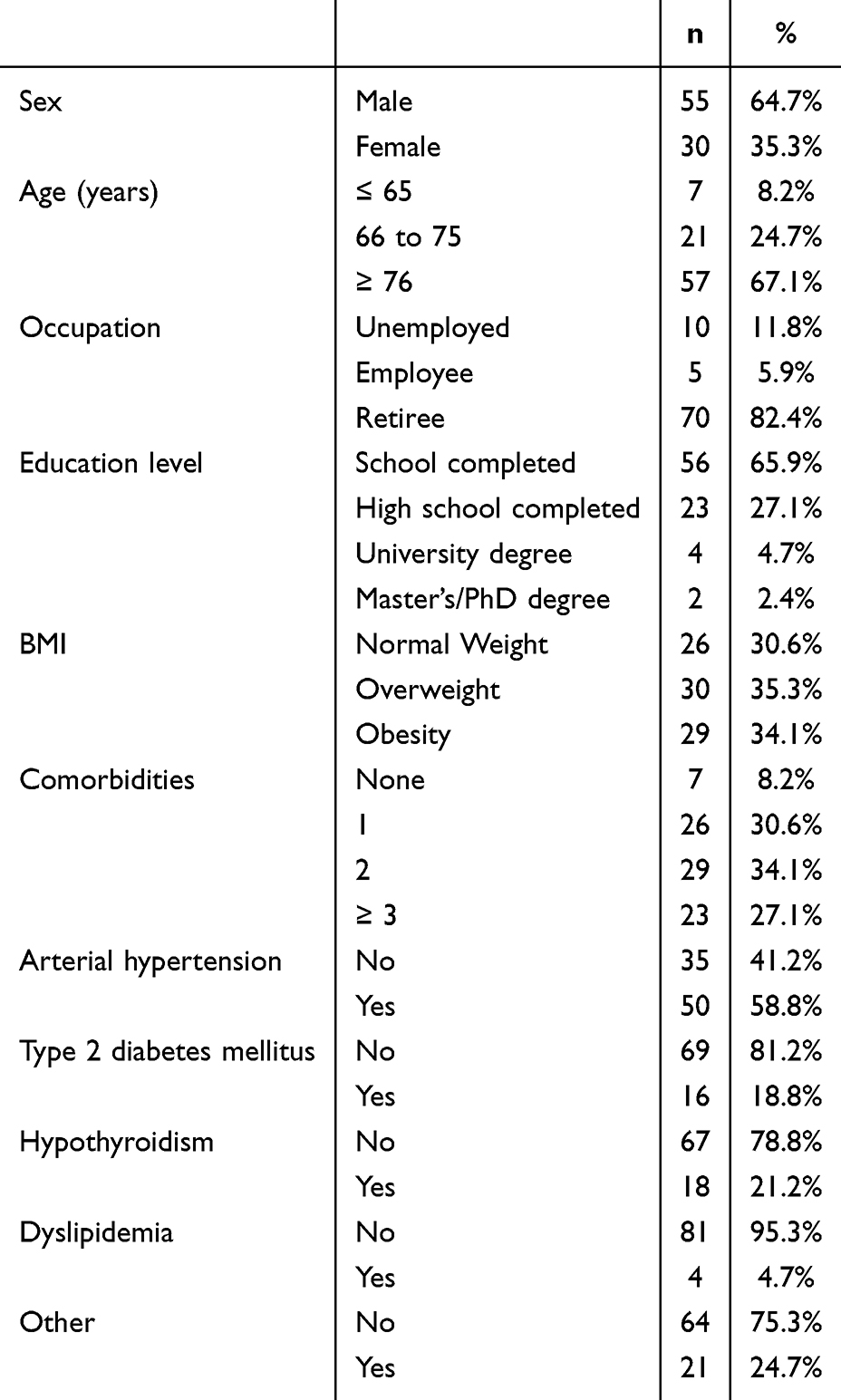 |
Table 1 Clinical and Demographic Characteristics of COPD Patients |
Clinical Characteristics
Regarding clinical characteristics, 35.3% (n=30) of patients were overweight, and 34.1% (n=29) were classified as obese. Additionally, 34.1% (n=29) reported having two comorbidities, with arterial hypertension being the most common (58.8%, n=50), followed by hypothyroidism (21.2%, n=18). Only 8.2% (n=7) reported no comorbidities (Table 1).
A significant proportion of patients were ex-smokers (52.9%, n=45), with 5.9% (n=5) being current smokers. Among the smokers, 27.1% (n=23) reported consuming fewer than 10 packs of cigarettes per year. Furthermore, 63.5% (n=54) indicated exposure to biomass for 10 years or more (Table 1).
COPD Characteristics
In terms of COPD characteristics, the majority of patients were classified under category A of the GOLD classification (52.9%, n=45), followed by category B (28.2%, n=24). Additionally, 72.9% (n=62) had an mMRC classification of less than 2. Most participants exhibited positive disease control, with 71.8% (n=61) reporting no COPD exacerbations in the past year and 81.2% (n=69) having no hospitalizations for COPD during the same period. Regarding treatment, 61.2% (n=52) of patients were using only one inhaled medication, while 38.8% (n=33) were using two or more, with tiotropium being the most commonly used (67.1%, n=57) and salmeterol the least commonly used (9.4%, n=8) (Table 2).
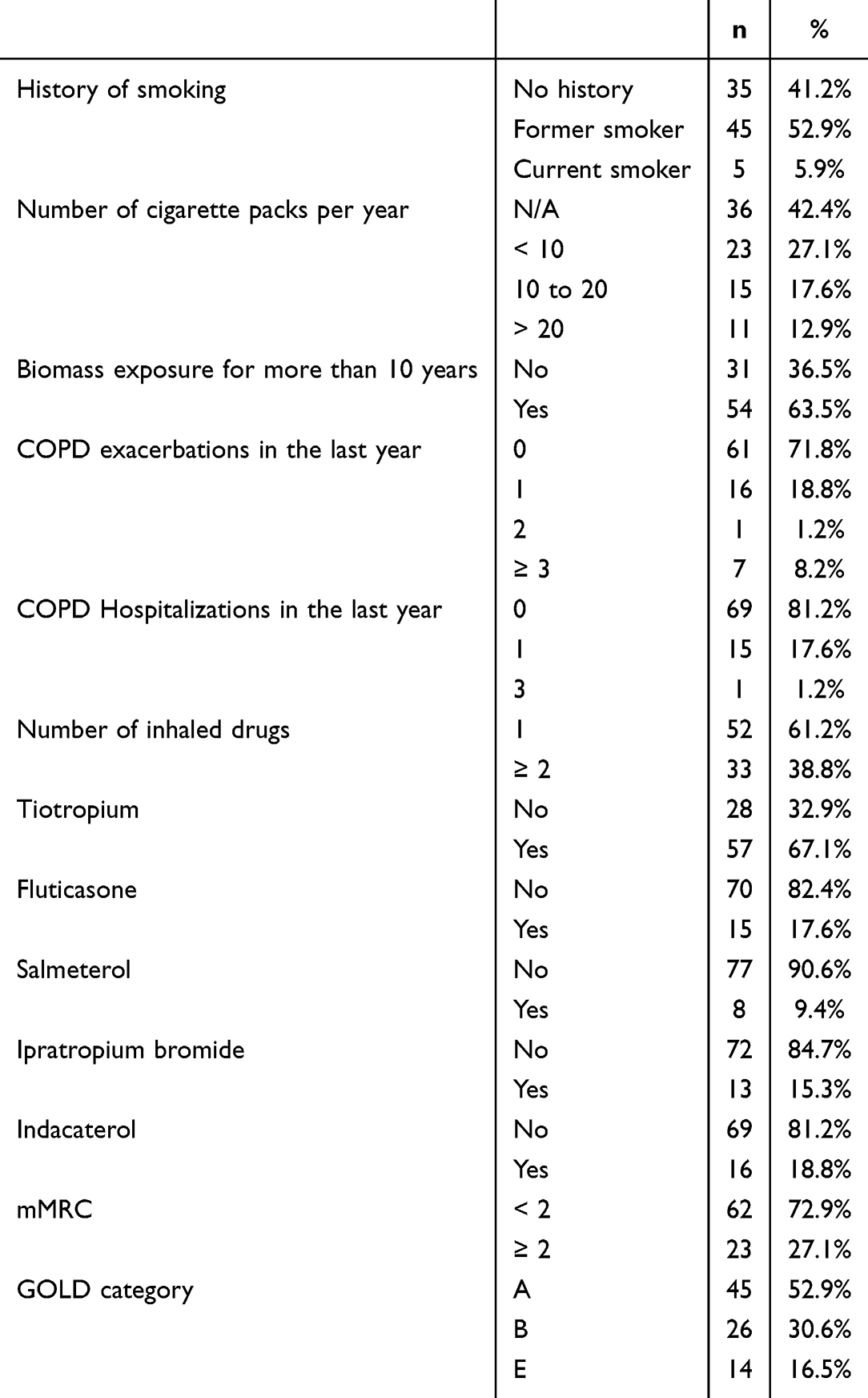 |
Table 2 Clinical Features of COPD and the Treatment of COPD Patients |
Adherence to Inhalation Therapy
Adherence to inhaled therapy, assessed using the TAI-10 questionnaire, revealed that most responses across all domains (ten questions) leaned towards the “never” option, reflecting a general trend of positive adherence to inhalers within our sample. However, domain-specific analysis highlighted notable variations. In the “erratic” non-adherence domain, 17.6% (n=15) of patients reported “sometimes” forgetting to use their inhalers. Similarly, within the “deliberate” non-adherence domain, 18.8% (n=16) of patients indicated “sometimes” discontinuing their inhaler use due to financial constraints. Figure 1 provides a detailed summary of the distribution of responses (n=85) for each of the 10 questions in the TAI questionnaire.
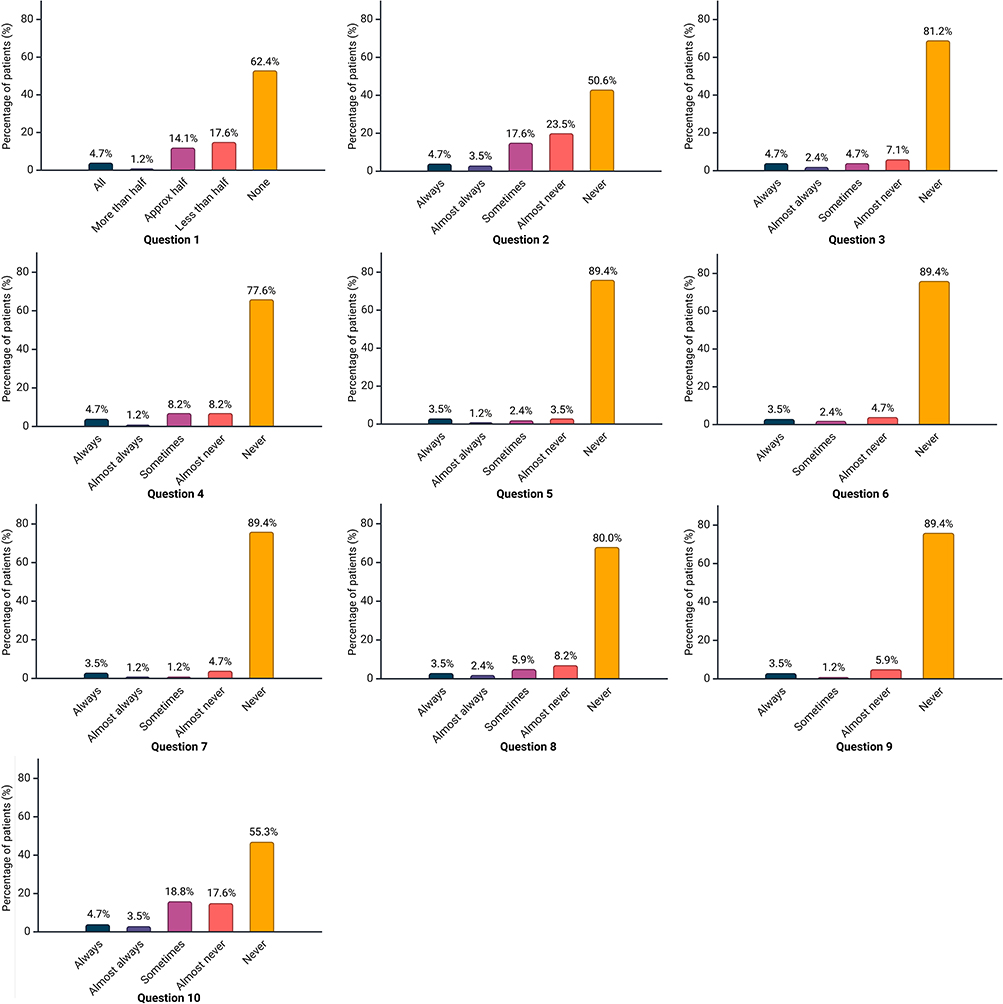 |
Figure 1 Distribution of responses to the TAI-10 questionnaire in COPD patients. |
Furthermore, an analysis of overall adherence patterns demonstrated a nearly even distribution among participants: 34.1% (n=29) exhibited good adherence, 32.9% (n=28) showed intermediate adherence, and the remaining 32.9% (n=28) reported non-adherence to inhalation therapy.
Factors Associated With Inhaled Therapy Adherence
The regression model evaluating the influence of patient characteristics on adherence revealed that higher BMI was significantly associated with better adherence. Specifically, obese patients were more likely to demonstrate intermediate adherence (OR=7.228, 95% CI 1.866–27.996), while overweight (OR=3.832, 95% CI 1.092–13.449) and obese patients (OR=9.966, 95% CI 2.538–39.139) exhibited higher odds of good adherence. Additionally, a trend was observed indicating that patients aged 65 years or younger were more likely to report good adherence (54.7%, p>0.05), as were those who were still employed (60.0%, p>0.05). However, these latter trends did not reach statistical significance (Table 3).
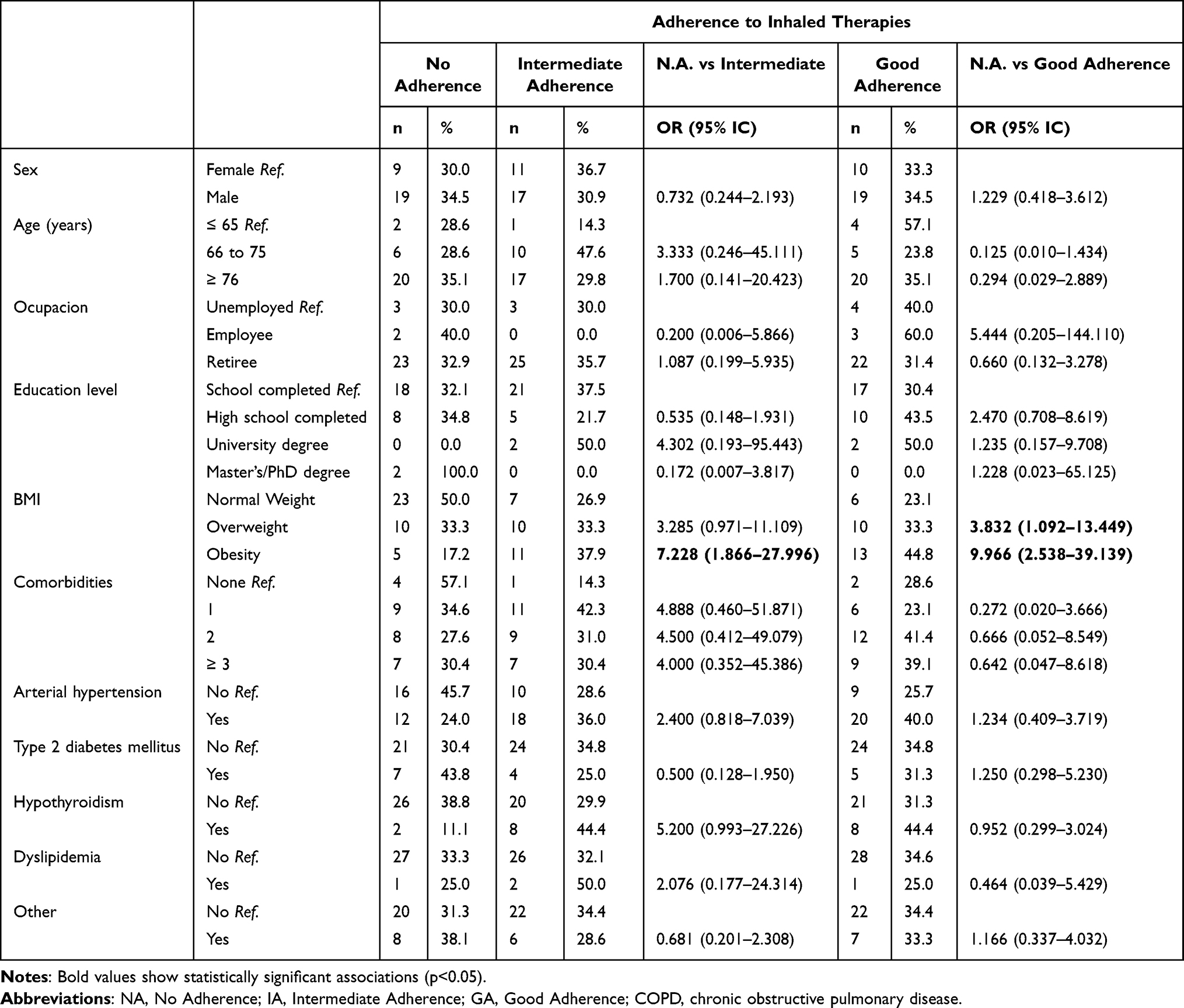 |
Table 3 Association Between demographicT and Clinical Characteristics With Adherence to Inhaled Therapy in COPD Patients |
Among COPD-related characteristics, only patients with an mMRC score of ≥2 were less likely to have good adherence compared to those with intermediate adherence (OR = 0.247, 95% CI: 0.067–0.907). Although not statistically significant, patients with a history of more than 20 pack-years of smoking were predominantly in the good adherence group (63.6%, p > 0.05), as were salmeterol users (62.5%, p > 0.05). Conversely, 100% of patients with two COPD exacerbations in the past year and 60% of current smokers were non-adherent (p > 0.05) (Table 4).
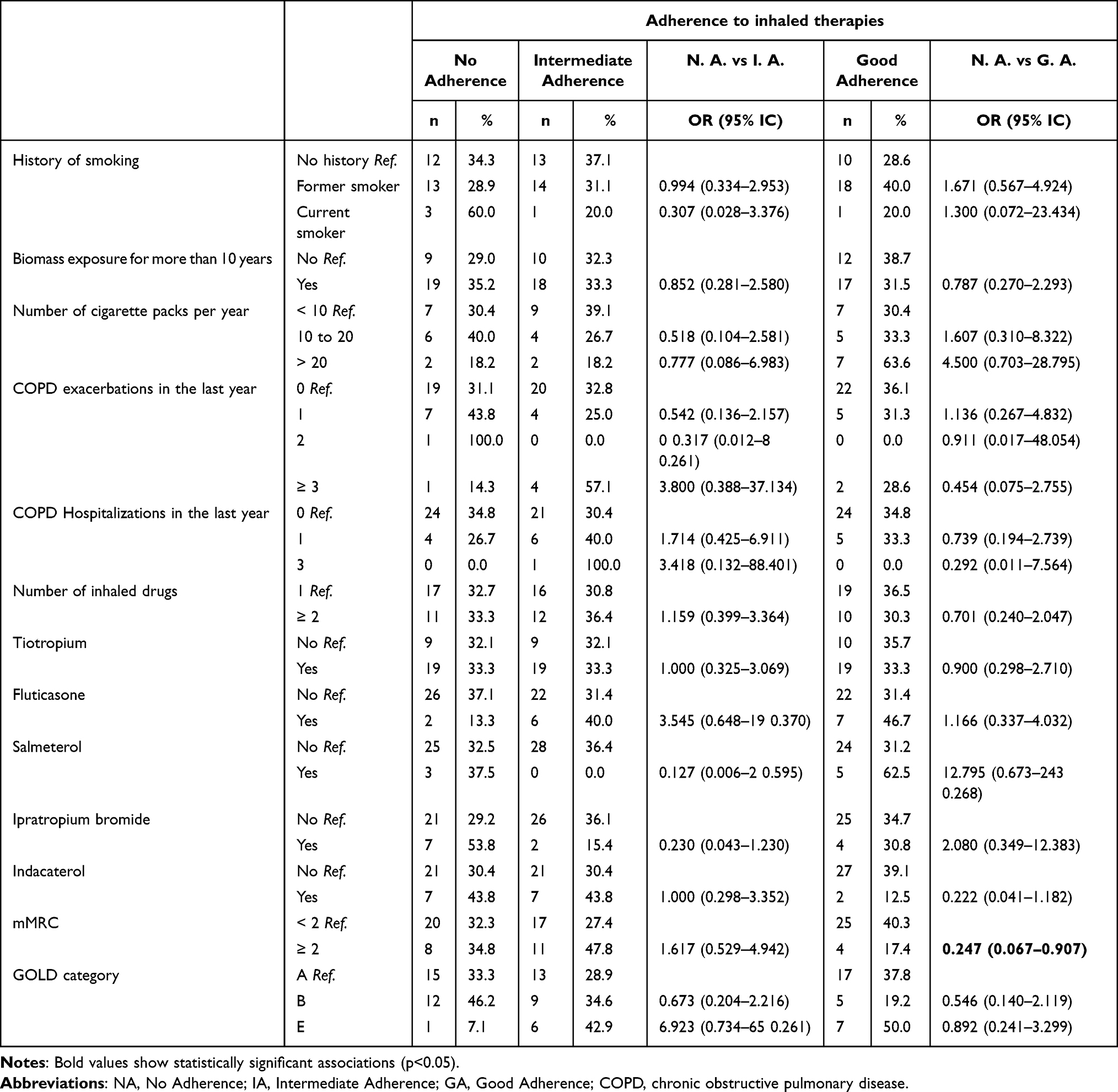 |
Table 4 Association Between Clinical Features of COPD and Adherence to Inhaled Therapy in COPD Patients |
Discussion
This research aimed to evaluate adherence to inhalation therapy among patients diagnosed with COPD treated in a specialty hospital in Quito, Ecuador. To the best of our knowledge, this is the first study of its kind conducted in Ecuador, providing essential insights into COPD adherence treatment in the country. The sample primarily consisted of men, over 75 years old, a demographic characterized by extensive health problems likely linked to advanced age. Nearly all patients (91.8%) had at least one comorbidity, with hypertension being the most prevalent. Additionally, only about one-third of the patients were of normal weight, consistent with findings from other studies on adherence in COPD patients.25,26
The status of COPD patients in this study suggested effective disease management, evidenced by the high percentage of patients without exacerbations or hospitalizations due to COPD in the past year, and with an mMRC score of less than 2 in 72.9% of cases. It was found that 34.1% of COPD patients had good adherence to inhaled medications, while 32.9% had intermediate adherence and 32.9% were non-adherent. The adherence rates observed in this study align with the variability reported in the literature, which ranges from 10% to 40% in COPD populations from countries like Austria, Ireland, Spain and Greece.25–29 In contrast, higher adherence rates have been reported in Brazil (67.3%),30 and Montes de Oca et al identified an adherence rate of 54.1% in patients from seven Latin American countries (Argentina, Chile, Colombia, Costa Rica, Guatemala, Mexico, and Uruguay).21 The non-adherence rates in our study are comparable to those reported in other research, ranging from 31.3% to 74.1% in COPD patients.26,31–34 While the non-adherent group comprised about one-third of the sample, the primary reasons for non-adherence were forgetting to take medication and lack of resources, highlighting the vulnerability of this group in Ecuador.
We observed that an increased BMI was associated with better adherence to inhaled therapy. This could be attributed to several mechanisms. Individuals with a high BMI often have comorbidities, particularly cardiovascular conditions, which lead to more frequent medical interactions. These interactions may reinforce the importance of inhaled therapy adherence.35,36 Additionally, obesity can exacerbate respiratory symptoms, such as dyspnea, making these patients more likely to experience symptomatic relief from inhaled therapies. This relief likely encourages consistent use and better adherence.37,38
Interestingly, although not statistically significant, we found a predominance of good adherence among patients aged 65 years or younger and those who were employed. This observation may reflect heightened health concerns among younger or working individuals regarding the potential deterioration of their health with age. Furthermore, patients with a history of smoking more than 20 pack-years demonstrated higher adherence to inhaled therapy. This could be due to the presence of more progressive disease and severe symptoms, which derive greater benefits from inhaled therapies.39
Tobacco smoke also impacts the efficacy of bronchodilator therapy. Chronic exposure induces airway inflammation and structural remodeling, particularly narrowing of the small airways, which increases resistance and limits smooth muscle relaxation. Tobacco smoke perpetuates inflammation through altered nicotine metabolism, weakens pulmonary immune defenses, and disrupts bacterial flora, increasing the risk of exacerbations. These changes worsen airflow limitation, lung hyperinflation, and respiratory mechanics, potentially reducing the effectiveness of bronchodilator inhalers.40,41
Previous studies, despite variability in methodologies, have associated poor adherence with factors such as age, lower educational attainment, income levels, comorbidities, smoking status, device complexity, and milder disease severity.25,42,43 Poor adherence to inhaled medications has been linked to increased risks of exacerbations, hospital admissions, and mortality.30 Conversely, good adherence has been associated with fewer severe COPD exacerbations and a reduced risk of death.44–46
Among our participants, adherence levels were relatively consistent among retirees, with similar proportions of non-adherence, intermediate adherence, and good adherence. One of the primary barriers to adherence was financial limitations, as access to inhaled medications often depends on the patient’s ability to afford them. In Ecuador, the high cost of these medications significantly restricts access.47 Notably, the high proportion of retirees (82.4%) in our sample highlights the vulnerability of this group to COPD. This is a critical finding, as previous research has demonstrated that economic inactivity can negatively impact adherence, particularly due to financial constraints that hinder access to essential medications.48,49
The non-adherence and intermediate adherence rates identified in our study are concerned, given their clinical and economic implications. Poor adherence not only leads to negative health outcomes but also imposes significant burdens on the healthcare system, primarily due to complications arising from inadequate disease management.50–52
Although no significant associations were found between the use of more than one inhaled medication, we emphasize the importance of promoting patient education and involvement in the inhaler selection process, as these have been shown to improve adherence.13 It is important to consider that specific cases, such as patients using multiple medications, may underestimate the importance of inhaled therapies, thereby jeopardizing adherence and treatment effectiveness.53 This was evident in our study, which found high percentages of comorbidities requiring pharmacological management, particularly hypertension, type 2 diabetes mellitus, and hypothyroidism.
Strategies aimed at increasing adherence in COPD patients should encompass various measures, including regular follow-ups involving multidisciplinary healthcare teams However, the implementation of such strategies is challenging in developing countries like Ecuador, where access to healthcare services and trained personnel is limited. Moreover, there is a need for improved training of healthcare providers in teaching patients the correct use of inhaled therapies.54 In addition to these factors, clinical characteristics such as age, cognitive capacity, and the patient’s spirometric profile must also be considered when developing adherence-enhancing interventions.55
Limitations
This study has several limitations that should be considered when interpreting the findings. First, the cross-sectional design limits the ability to establish causal relationships between patient characteristics and adherence to inhalation therapy. Second, the use of convenience sampling and the specific characteristics of the study sample may restrict the generalizability of the results to the wider population of COPD patients in Ecuador. Third, the reliance on self-reported data, including the TAI questionnaire, introduces the potential for recall and reporting biases, which could lead to an overestimation of adherence rates. Lastly, as the study was conducted in a single hospital, the findings may not fully reflect the variability in healthcare settings or COPD management practices across other regions of the country.
Conclusions
This study reveals that approximately one-third of COPD patients in Ecuador demonstrate good adherence to inhalation therapy, while a similar proportion exhibit intermediate or poor adherence. The study population, primarily composed of older adults and retirees with multiple comorbidities, represents a particularly vulnerable group. High rates of non-adherence, influenced by factors such as forgetfulness and financial constraints, underscore the urgent need for targeted interventions and resources to support these patients.
Improving adherence among COPD patients poses significant challenges, particularly in developing countries like Ecuador, where healthcare access and availability of trained personnel are often limited. Addressing these challenges will require a comprehensive approach that includes patient education, regular follow-ups, and the integration of multidisciplinary healthcare teams to enhance disease management and adherence to therapy.
Consent for Publication
Acceptance of voluntary participation was obtained from each of the patients. The informed consent form was completed before beginning the data collection process.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Dean J, Kolsum U, Hitchen P, Gupta V, Singh D. Clinical characteristics of COPD patients with tidal expiratory flow limitation. COPD. 2017;12:1503–1506. doi:10.2147/COPD.S137865
2. Hogg JC, Chu F, Utokaparch S, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(26):2645–2653. doi:10.1056/NEJMoa032158
3. Global Initiative for Chronic Obstructive Lung Disease. 2024 GOLD Report [Internet]. GOLD; 2024 [citado 28 de agosto de 2024]. Disponible en: https://goldcopd.org/2024-gold-report/.
4. World Health Organization. Chronic obstructive pulmonary disease (COPD) [Internet]. WHO. 2023 [citado 8 de julio de 2023]. Disponible en: https://www.who.int/news-room/fact-sheets/detail/chronic-obstructive-pulmonary-disease-(copd).
5. American Thoracic Society. Chronic obstructive pulmonary disease or COPD including chronic bronchitis, emphysema, bronchiectasis [Internet]. ATS - American Thoracic Society. 2021 [citado 28 de agosto de 2024]. Disponible en: https://www.thoracic.org/patients/patient-resources/topic-specific/copd.php.
6. Vijayan VK. Chronic obstructive pulmonary disease. Indian J Med Res. 2013;137(2):251–269.
7. Diette GB, Accinelli RA, Balmes JR, et al. Obstructive lung disease and exposure to burning biomass fuel in the indoor environment. Glob Heart. 2012;7(3):265–270. doi:10.1016/j.gheart.2012.06.016
8. Montes Cardona JA, Hincapié Erira DA, Nati-Castillo HA, Sánchez-Vallejo J, Izquierdo-Condoy JS. Characteristics of inhaler technique in COPD patients in a specialized center in Armenia, Colombia: a cross-sectional study. Patient Prefer Adherence. 2023;17:2025–2038. doi:10.2147/PPA.S417375
9. Turégano-Yedro M, Trillo-Calvo E, Navarro I Ros F, et al. Inhaler adherence in COPD: a crucial step towards the correct treatment. Int J Chron Obstruct Pulmon Dis. 2023;18:2887–2893. doi:10.2147/COPD.S431829
10. Pan American Health Organization. Chronic obstructive pulmonary disease (COPD) in the Americas [Internet]. PAHO; 2014 [citado 8 de julio de 2023]. Disponible en: https://www3.paho.org/hq/dmdocuments/2014/EPOC-Factsheet-2014-Eng-(3).pdf.
11. Caballero A, Torres-Duque CA, Jaramillo C, et al. Prevalence of COPD in five Colombian cities situated at low, medium, and high altitude (PREPOCOL study). Chest. 2008;133(2):343–349. doi:10.1378/chest.07-1361
12. World Health Organization. Ecuador [Internet]. WHO Data. 2023 [citado 28 de agosto de 2024]. Disponible en: https://data.who.int/countries/218IJGM_A_512814.
13. Kini V, Ho PM. Interventions to improve medication adherence: a review. JAMA. 2018;320(23):2461–2473. doi:10.1001/jama.2018.19271
14. Kim JA, Lim MK, Kim K, Park J, Rhee CK. Adherence to inhaled medications and its effect on healthcare utilization and costs among high-grade chronic obstructive pulmonary disease patients. Clin Drug Investig. 2018;38(4):333–340. doi:10.1007/s40261-017-0612-2
15. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
16. Hatah E, Lim KP, Ali AM, Mohamed Shah N, Islahudin F. The influence of cultural and religious orientations on social support and its potential impact on medication adherence. Patient Prefer Adherence. 2015;9:589–596. doi:10.2147/PPA.S79477
17. Burkhart PV, Sabaté E. Adherence to long-term therapies: evidence for action. J Nurs Scholarsh. 2003;35(3):207. doi:10.1111/j.1547-5069.2003.tb00001.x
18. Vrijens B, Dima AL, Van Ganse E, et al. What we mean when we talk about adherence in respiratory medicine. J Allergy Clin Immunol Pract. 2016;4(5):802–812. doi:10.1016/j.jaip.2016.05.019
19. Bischof AY, Cordier J, Vogel J, Geissler A. Medication adherence halves COPD patients’ hospitalization risk – evidence from Swiss health insurance data. NPJ Prim Care Respir Med. 2024;34:1. doi:10.1038/s41533-024-00361-2
20. Rolnick SJ, Pawloski PA, Hedblom BD, Asche SE, Bruzek RJ. Patient characteristics associated with medication adherence. Clin Med Res. 2013;11(2):54–65. doi:10.3121/cmr.2013.1113
21. Montes de Oca M, Menezes A, Wehrmeister FC, et al. Adherence to inhaled therapies of COPD patients from seven Latin American countries: the LASSYC study. PLoS One. 2017;12(11):e0186777. doi:10.1371/journal.pone.0186777
22. Instituto Nacional de Estadística y Censos. Actividades y Recursos de Salud [Internet]. Instituto Nacional de Estadística y Censos INEC. 2023 [citado 9 de abril de 2024]. Disponible en: https://www.ecuadorencifras.gob.ec/actividades-y-recursos-de-salud/.
23. Ministerio de Gobierno Ecuador C. Hospital Quito No. 1 Policia Nacional del Ecuador. Ministerio de Gobierno Ecuador. 2021.
24. Plaza V, Fernández-Rodríguez C, Melero C, et al. Validation of the “Test of the Adherence to Inhalers” (TAI) for Asthma and COPD Patients. J Aerosol Med Pulm Drug Deliv. 2016;29(2):142–152. doi:10.1089/jamp.2015.1212
25. Humenberger M, Horner A, Labek A, et al. Adherence to inhaled therapy and its impact on chronic obstructive pulmonary disease (COPD). BMC Pulm Med. 2018;18(1):163. doi:10.1186/s12890-018-0724-3
26. Ierodiakonou D, Sifaki-Pistolla D, Kampouraki M, et al. Adherence to inhalers and comorbidities in COPD patients. A cross-sectional primary care study from Greece. BMC Pulm Med. 2020;20(1):253. doi:10.1186/s12890-020-01296-3
27. Rogliani P, Calzetta L, Coppola A, et al. Optimizing drug delivery in COPD: the role of inhaler devices. Respir Med. 2017;124:6–14. doi:10.1016/j.rmed.2017.01.006
28. Sulaiman I, Cushen B, Greene G, et al. Objective assessment of adherence to inhalers by patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2017;195(10):1333–1343. doi:10.1164/rccm.201604-0733OC
29. Carpes Hernandez MJ, Cerdá B, Navarro PB, Rentero PZ. Adherencia y satisfacción del paciente con enfermedad pulmonar obstructiva crónica desde la farmacia comunitaria. Pharmaceutical Care España. 2022;24(5):13–26. doi:10.60103/phc.v24i5.781
30. Alcantara de Moreira AT, Ribeiro Pinto C, Moreira Lemos AC, Assunção-Costa L, Souza GS, Martins E. Evidence of the association between adherence to treatment and mortality among patients with COPD monitored at a public disease management program in Brazil. J Bras Pneumol. 2021;48(1):e20210120. doi:10.36416/1806-3756/e20210120
31. Duarte-de-araújo A, Teixeira P, Hespanhol V, Correia-de-sousa J. COPD: misuse of inhaler devices in clinical practice. Int J Chron Obstruct Pulmon Dis. 2019;14:1209–1217. doi:10.2147/COPD.S178040
32. Romagnoli A, Santoleri F, Costantini A. Adherence and persistence analysis after three years in real-life of inhalation therapies used in the treatment of COPD. Curr Med Res Opin. 2020;36(12):2055–2061. doi:10.1080/03007995.2020.1841617
33. Deslee G, Fabry-Vendrand C, Poccardi N, et al. Use and persistence of single and multiple inhaler triple therapy prescribed for patients with COPD in France: a retrospective study on THIN database (OPTI study). BMJ Open Respir Res. 2023;10(1):e001585. doi:10.1136/bmjresp-2022-001585
34. Santibáñez M, Rodríguez I, López-Caro JC, et al. Comparación de la adhesión terapéutica según el Test de Adherencia a Inhaladores y el registro de la retirada en farmacia de los fármacos prescritos en pacientes asmáticos. Estudio REFARMA. Open Respir Arch. 2023;5(2):100238. doi:10.1016/j.opresp.2023.100238
35. Kivimäki M, Strandberg T, Pentti J, et al. Body-mass index and risk of obesity-related complex multimorbidity: an observational multicohort study. Lancet Diabetes Endocrinol. 2022;10(4):253–263. doi:10.1016/S2213-8587(22)00033-X
36. Tuminah S, Indrawati L, Riyadina W, et al. Number of comorbidities and the risk of delay in seeking treatment for coronary heart disease: a longitudinal study in Bogor City, Indonesia. Osong Public Health Res Perspect. 2024;15(3):201–211. doi:10.24171/j.phrp.2023.0337
37. Sun Y, Zhang Y, Liu X, Liu Y, Wu F, Liu X. Association between body mass index and respiratory symptoms in US adults: a national cross-sectional study. Sci Rep. 2024;14(1):940. doi:10.1038/s41598-024-51637-z
38. Shah NM, Kaltsakas G. Respiratory complications of obesity: from early changes to respiratory failure. Breathe. 2023;19(1):220263. doi:10.1183/20734735.0263-2022
39. Vanoverschelde A, van der Wel P, Putman B, Lahousse L. Determinants of poor inhaler technique and poor therapy adherence in obstructive lung diseases: a cross-sectional study in community pharmacies. BMJ Open Respir Res. 2021;8(1):e000823. doi:10.1136/bmjresp-2020-000823
40. Pezzuto A, Ricci A, D’Ascanio M, et al. Short-term benefits of smoking cessation improve respiratory function and metabolism in smokers. COPD. 2023;18:2861–2865. doi:10.2147/COPD.S423148
41. D’Ascanio M, Viccaro F, Calabrò N, et al. Assessing static lung hyperinflation by whole-body plethysmography, helium dilution, and Impulse Oscillometry System (IOS) in patients with COPD. COPD. 2020;15:2583–2589. doi:10.2147/COPD.S264261
42. Ágh T, Inotai A, Mészáros Á. Factors associated with medication adherence in patients with chronic obstructive pulmonary disease. Respiration. 2011;82(4):328–334. doi:10.1159/000324453
43. Homętowska H, Świątoniowska-lonc N, Klekowski J, Chabowski M, Jankowska-Polańska B. Treatment adherence in patients with obstructive pulmonary diseases. Int J Environ Res Public Health. 2022;19(18):11573. doi:10.3390/ijerph191811573
44. Halpin DMG, Rothnie KJ, Banks V, et al. Comparative adherence and persistence of single- and multiple-inhaler triple therapies among patients with chronic obstructive pulmonary disease in an English real-world primary care setting. Int J Chron Obstruct Pulmon Dis. 2022;17:2417–2429. doi:10.2147/COPD.S370540
45. Alcázar-Navarrete B, Jamart L, Sánchez-Covisa J, Juárez M, Graefenhain R, Sicras-Mainar A. Clinical characteristics, treatment persistence, and outcomes among patients with COPD treated with single- or multiple-inhaler triple therapy: a retrospective analysis in Spain. Chest. 2022;162(5):1017–1029. doi:10.1016/j.chest.2022.06.033
46. Vestbo J, Anderson JA, Calverley PMA, et al. Adherence to inhaled therapy, mortality and hospital admission in COPD. Thorax. 2009;64(11):939–943. doi:10.1136/thx.2009.113662
47. Izquierdo-Condoy JS, Salazar-Santoliva C, Salazar-Duque D, et al. Challenges and opportunities in COPD management in Latin America: a review of inhalation therapies and advanced drug delivery systems. Pharmaceutics. 2024;16(10):1318. doi:10.3390/pharmaceutics16101318
48. Haynes RB, Yao X, Degani A, Kripalani S, Garg A, McDonald HP. Interventions to enhance medication adherence. Cochrane Database Syst Rev. 2005;4:CD000011.
49. Nittala A, Nahmens I, Ikuma L, Thomas D. Effects of medication adherence on healthcare services use among asthma patients. J Healthc Qual Res. 2019;34(6):301–307. doi:10.1016/j.jhqr.2019.06.007
50. van Boven JFM, Chavannes NH, van der Molen T, Rutten-van Mölken MPMH, Postma MJ, Vegter S. Clinical and economic impact of non-adherence in COPD: a systematic review. Respir Med. 2014;108(1):103–113. doi:10.1016/j.rmed.2013.08.044
51. Toy EL, Beaulieu NU, McHale JM, et al. Treatment of COPD: relationships between daily dosing frequency, adherence, resource use, and costs. Respir Med. 2011;105(3):435–441. doi:10.1016/j.rmed.2010.09.006
52. Mapel DW, Roberts MH. Management of Asthma and chronic obstructive pulmonary disease with combination inhaled corticosteroids and long-acting β-agonists: a review of comparative effectiveness research. Drugs. 2014;74(7):737–755. doi:10.1007/s40265-014-0214-8
53. Albrecht JS, Park Y, Hur P, et al. Adherence to maintenance medications among older adults with chronic obstructive pulmonary disease. The role of depression. Ann Am Thorac Soc. 2016;13(9):1497–1504. doi:10.1513/AnnalsATS.201602-136OC
54. Plaza V, Giner J, Rodrigo GJ, Dolovich MB, Sanchis J. Errors in the use of inhalers by health care professionals: a systematic review. J Allergy Clin Immunol Pract. 2018;6(3):987–995. doi:10.1016/j.jaip.2017.12.032
55. Monteiro C, Maricoto T, Prazeres F, Simões PA, Simões JA. Determining factors associated with inhaled therapy adherence on asthma and COPD: a systematic review and meta-analysis of the global literature. Respir Med. 2022;191:106724. doi:10.1016/j.rmed.2021.106724
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.