")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 20
Adoption of Digital Therapeutics in Europe
Authors Fassbender A, Donde S, Silva M, Friganovic A, Stievano A, Costa E , Winders T, van Vugt J
Received 27 August 2024
Accepted for publication 25 November 2024
Published 27 December 2024 Volume 2024:20 Pages 939—954
DOI https://doi.org/10.2147/TCRM.S489873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Amelie Fassbender,1 Shaantanu Donde,2 Mitchell Silva,3 Adriano Friganovic,4– 6 Alessandro Stievano,7 Elisio Costa,8 Tonya Winders,9 Joris van Vugt10
1Medical Affairs DM, Viatris, Hoeilaart, Belgium; 2Medical Affairs, DM&JANZ, Viatris, Hatfield, London, UK; 3Executive Management, Esperity, Brussel, Belgium; 4University Hospital Centre, Zagreb, Croatia; 5University of Applied Health Sciences, Zagreb, Croatia; 6Faculty of Health Studies, University of Rijeka, Rijeka, Croatia; 7Department of Clinical and Experimental Medicine, University of Messina, Messina, Italy; 8Faculty of Pharmacy, CINTESIS@RISE, Competence Center on Active and Healthy Ageing (Porto4Ageing), University of Porto, Porto, Portugal; 9Board of Directors, Global Allergy & Airways Patient Platform, Vienna, Austria; 10Medical Affairs, DM&JANZ, Viatris, Amstelveen, the Netherlands
Correspondence: Amelie Fassbender, Email [email protected]
Abstract: Digital therapeutics (DTx) are an emerging medical therapy comprising evidence-based interventions that are regulatory approved for patient use, or are under development, for a variety of medical conditions, including hypertension, cancer, substance use disorders and mental disorders. DTx have significant potential to reduce the overall burden on healthcare systems and offer potential economic benefits. There is currently no specific legal regulation on DTx in the EU. Although European countries have similar approaches to digital health solutions, the adoption of DTx varies across the continent. The aim of this narrative review is to discuss the levels of adoption of DTx in Europe, and to explore possible strategies to improve adoption, with the goal of higher rates of adoption, and more consistent use of DTx across the continent. The article discusses the regulatory and reimbursement landscape across Europe; validation requirements for DTx, and the importance of co-design and an ecosystem-centric approach in the development of DTx. Also considered are drivers of adoption and prescription practices for DTx, as well as patient perspectives on these therapeutics. The article explores potential factors that may contribute to low rates of DTx adoption in Europe, including lack of harmonisation in regulatory requirements and reimbursement; sociodemographic factors; health status; ethical concerns; challenges surrounding the use and validation of AI; knowledge and awareness among healthcare professionals (HCPs) and patients, and data standards and interoperability. Efforts to improve rates of access to DTx and adoption of these therapeutics across Europe are described. Finally, a framework for improved uptake of DTx in Europe is proposed.
Keywords: digital health, regulatory, reimbursement, healthcare professionals, health inequalities
Introduction
Digital therapeutics (DTx) are an emerging medical therapy comprising evidence-based interventions, with clinically evaluated software programmes, often, but not necessarily, coupled with artificial intelligence (AI) techniques and machine learning systems,1 to prevent, manage, or treat medical conditions.2,3 DTx are a specific set of technology-enabled interventions within the broader digital health sphere intended to produce a measurable therapeutic effect.4
According to Wang et al, the use of DTx as a general medical component is ambiguous, and this ambiguity may be due in part to a lack of consensus on a definition.5 To ensure industry and global alignment, the Digital Therapeutics Alliance (DTA),1,6 a global non-profit trade association of industry leaders and stakeholders engaged in the advancement of evidence-driven DTx has adopted the definition of DTx specified by the International Organization for Standardization (ISO):7 DTx are “health software intended to treat or alleviate a disease, disorder, condition, or injury by generating and delivering a medical intervention that has a demonstrable positive therapeutic impact on a patient’s health”. As the EU Medical Device Regulation (MDR) may apply to digital health product types, such as wellness apps, and monitoring, diagnostic or medication reminder tools,6 DTx must always be classified as medical devices,8 and are held to the same standards of evidence and regulatory oversight as traditional medical treatments,1 requiring ‘rigorous’ clinical evidence,1 including data from randomised controlled clinical trials.8
Some challenges associated with real-life administration of pharmaceutical drugs and biologicals for chronic diseases (eg, medication non-adherence, adverse effects, toxicity, or inadequate efficacy) might potentially be mitigated by DTx.9 According to the DTA, DTx are essential to healthcare delivery systems and might address critical gaps in care for underserved populations, regardless of patient age, language, culture, income, disease state or geography.2 DTx fill gaps in care by increasing patient access to clinically safe and effective therapies; offering at-home convenience and privacy, thereby lowering stigma associated with the delivery of certain traditional therapies; extending clinicians’ ability to care for patients; providing therapies in different languages, and providing meaningful results and insights on personalised goals and outcomes to patients and their clinicians.2
DTx are regulatory approved for patient use, or are under development, for a variety of medical conditions, including hypertension;10–12 cancer;13–15 gastrointestinal disorders,16 such as irritable bowel syndrome17–20 and inflammatory bowel disease;21 insomnia;22,23 asthma;24,25 chronic obstructive pulmonary disease;26 substance use disorders27-30 and smoking;31 obesity and eating disorders;32–34 multiple sclerosis;35 autism;36 Alzheimer’s disease, dementia, learning disabilities, and attention deficits.1–3,9,37 Considerable research has been published on the use of DTx in diabetes, with most of this research outside Europe.38–48 DTx are also being developed for mental disorders, such as depression. Depressive disorders represent the largest proportion of mental illnesses globally, and are expected to be the leading cause of disability-adjusted life years by 2030.49 The urgency of implementing mental health services to address new barriers to care during the COVID-19 pandemic persuaded clinicians to explore DTx as potential tools for clinical intervention in patients with mental health disorders, including depression, anxiety and stress.8,50–56
DTx have significant potential to reduce the overall burden on healthcare systems, such as by preventing hospital visits by improving self-management or providing therapy remotely.57 DTx interventions also offer potential economic benefits;58 however, there are limited studies on the cost-effectiveness of DTx, with several of these from Asia12,31,58–61 and the USA.27,28,46 Furthermore, economic analyses on DTx often have important methodological shortcomings.58 Importantly, DTx can greatly impact the patient experience, and are a potential option to provide tailored interventions according to the patient’s needs.32,62,63
The aim of this narrative review is to discuss the levels of adoption of DTx in Europe, and to explore possible strategies to improve adoption, with the goal of higher rates of adoption, and more consistent use of DTx, across the continent.
Regulatory and Reimbursement Landscape Across Europe
Europe is currently uniquely positioned to be one of the pioneers for DTx clear market access pathways into the public health systems, with regulations currently in Germany, France, Belgium and Austria,64 and DTx policy pathways evolving throughout Europe.65 There is currently no specific legal regulation on DTx in the EU; national regulatory frameworks regulate the use of DTx, with country-specific regulatory standards and requirements.66 Therefore, although European countries have similar approaches to digital health solutions, there is a lack of alignment,67 hence, the regulatory and reimbursement landscape for DTx varies across the continent.37,64,67,68 The systems in place in a few example countries are described as follows.
Germany is the leading country in Europe in terms of DTx legislation, through the Digital Care Act (Digitale-Versorgung-Gesetz [DVG]), which came into force in December 2019.37,69 Germany has an active fast-track model for digital health applications (DiGA), enabling doctors to prescribe reimbursed DTx to publicly insured patients,70 and is generally recognised as a pioneer of access to and reimbursement of DTx.37,64,71
France is introducing a similar reimbursement model to Germany.72,73 The Prise en Charge Anticipée (PECAN), which includes fast-track reimbursement, has been implemented and enables quick market access and quick access to patients.64
In 2021, the INAMI-RIZIV in Belgium announced a reimbursement scheme for DTx that are CE-marked medical devices, with close alignment to the fast-track process for DTx in Germany.70 Although these regulations are in place, no DTx have reached the highest level of the mHealthBelgium validation pyramid that guarantees government funding.74
In the 2023 Digital Austria Act (DAA),75 the government parties proposed the introduction of quality approved DiGA.64
Despite the National Institute for Health and Care Excellence (NICE) evidence standards, there is no centralised reimbursement model for DTx in England, with decision making by clinical commissioning groups.70 Similarly, there are no reimbursement or financing regulations in place for DTx in the public health system in Spain.64
With regard to the widespread use of DTx, Italy has been described as “on the starting blocks” compared with other countries.37 The Parliamentary Intergroup Digital Health and Digital Therapeutics in Italy was set up in May 2023 and introduced an initial bill on DTx the following month.37
Countries such as Luxembourg and the Netherlands have no formal classification for DTx, which generally fall under the medical device category and are not subject to a distinctive product category.65
These examples clearly show the varied regulatory and reimbursement landscape in Europe.
Although there has recently been considerable progress in reimbursement schemes in Europe, particularly in Germany, Belgium and France, there remain significant barriers to reimbursement across the continent.66 Each country in Europe is unique, and the reimbursement framework must fit in with existing national systems.66 The requirements for reimbursement for DTx in a sample of European countries is shown in Figure 1.
 |
Figure 1 Requirements for reimbursement for digital therapeutics in a sample of European countries. Abbreviations: BfArM, Bundesinstitut für Arzneimittel und Medizinprodukte (Federal Institute for Drugs and Medical Devices); DiGA, digital health applications; DTx, digital therapeutics; GKV-SV, GKV-Spitzenverband; NICE, National Institute for Health and Care Excellence; PECAN, Prise en Charge Anticipée. Notes: Data collected from the official websites of national regulatory agencies. |
Validation Requirements for Digital Therapeutics
The therapeutic functionality (“active ingredient”) of DTx corresponds to the component that shows a therapeutic effect, and the efficacy of this component requires validation.76 The therapeutic effects of DTx have been evaluated through validated endpoints in conventional randomised clinical trials; however, the use of real-world data and digital endpoints is gaining interest.76,77 The user interface (“excipient”) of DTx maximises the efficacy of the therapeutic functionality,78 and should also be considered when establishing global standards for DTx.76
The DTA reports that there is a lack of frameworks for DTx defining what “good” looks like, so many healthcare decision makers have had to develop their own methods to evaluate DTx products.79 Following this observation, the DTA created an initial framework to assess DTx products, including their value and impact in real-world settings.79
A “fit-for-purpose” assessment of biometric monitoring technologies (BioMeTs) approach for DTx includes verification, analytical/statistical validation and clinical validation.80 Verification establishes whether the DTx product meets the intended purpose; analytical/statistical validation ascertains whether the DTx product accurately and reliably generates the intended output, and clinical validation determines whether the output is clinically meaningful in the defined condition.81
The Importance of Co-Design and an Ecosystem-Centric Approach in the Development of Digital Therapeutics
Many digital health interventions are failing to effectively engage patients and the public.82 One solution that has been proposed is to directly involve patients and the public in the design of these digital health interventions.82 Sanz et al describes co-design as key to delivering patient-centred care as it allows involvement of stakeholders in the development of digital health solutions.83 Co-design in the development of DTx involves engaging with, and listening to, patients and other stakeholders, including clinicians and other healthcare professionals (HCPs), carers and policy makers, to ensure that the therapeutics meet the needs and preferences of end-users and healthcare systems, as well as having a positive impact on patients’ lives.62,84 Bird et al suggest that involving individuals from the healthcare community and members of the public with personal healthcare experience into the process of designing new health systems, products or services helps to drive improvements that are useful and relevant.85 Silvola et al consider that the involvement of users is essential to provide a clear understanding of the real needs and desires of patients; however, an efficient co-design process requires patients to be provided with the tools necessary to enable them to collaborate effectively and express their opinions.86 According to O’Kelly, stakeholders who clearly see the benefits of a digital solution, including how it potentially makes their lives easier, are more likely to engage and embrace new digital models of care.84
As indicated by Mesko et al, a co-design approach could lead to a range of short-term benefits, such as improved knowledge of patient needs; original ideas from diverse perspectives and priorities; more efficient decision making, and reduced development times.87 There are also potential long-term benefits of such collaboration, including greater patient satisfaction, and increased support and enthusiasm for innovation.87
Voorheis et al noted that although there is consensus on the value of patient and public involvement in digital health design, there is little guidance on how to maximise the worth of the collaborative design work.82 Co-design has historically focused on improving the digital health product itself; however, these authors reported that patients and the public also have crucial insights on implementation planning, as well as how collaborative design can be used as its own empowering intervention.82
Adoption of Digital Therapeutics
Although there has been progress in DTx in terms of clinical validation, regulatory clarity and reimbursement, DTx innovators are now facing the challenge of bringing these therapeutics to patients at scale.88
DTx are used to successfully treat a range of clinical conditions; however, the adoption of these therapeutics in health systems in Europe remains limited,57,72,89,90 with progress in integrating DTx into access and care pathways in only a few countries.57 In addition, adherence rates are low.91–96 As there are currently few DTx approved in practice, there is resistance towards clinical acceptance and organisational change;97 therefore, the diffusion and usage of DTx are fragmented across Europe.98
Germany is a pioneer for apps on prescription;72 however, few physicians in the German healthcare system prescribe DTx.37 Furthermore, a survey conducted in Germany in 2023 showed that over 60% of participants had never heard of digital health applications,72 and around 5% of DTx prescriptions were not picked up.72 In addition, a survey of urology patients in Germany revealed that certified DTx apps were used by only 7.3% of patients aged <65 years, and 5.4% of those aged ≥65 years.99 In line with these observations, Courtet et al noted that despite the efficacy of digital interventions (in this case, for depression) demonstrated in clinical trials, many of these tools never reach real-life patients.8
In a study in France, 35.3% of patients, 30.4% of public participants, and 15.8% of HCPs reported willingness to take digital pills.100 This willingness was associated with male sex and the current use of a connected device to record health settings.100 The prospective acceptability of and willingness to take digital pills were limited by clinical and ethical concerns both at the individual and societal level.100
Drivers of Adoption of Digital Therapeutics
HCPs have a key role in prescribing and influencing uptake of DTx, as well as optimising patient care during use of DTx, and are central to DTx adoption.88 Nurses have a potentially important role in DTx adoption as they work closely with patients and gain unique insight into the patient perspective, which helps nurses to understand how patients think, what is important to them, and why they behave in certain ways.101 This knowledge enables and motivates nurses to drive change and make improvements for patients through digital technology.101 Primary research involving general practitioners (GPs) and specialists in Germany, Belgium, Sweden and the UK showed that key drivers to HCP adoption are to improve patient outcome, access and experience; to increase HCP efficiency and support organisational goals, and a personal interest in DTx.88 Further drivers of HCP adoption of DTx include the ability to continuously monitor and engage patients, adjust treatment plans remotely in real time and provide personalised care.102
If DTx are reimbursable and are prescribed, the last barrier to adoption lies with the patient.91 Price is an obvious barrier to adoption by patients – reimbursement models that require patients to pay substantial amounts for DTx will hinder adoption of these tools.91 Another driver of adoption for patients is the time-saving aspect of DTx. These tools enable data collection in real-time, thereby potentially reducing the number of face-to-face healthcare appointments needed.4 A further driver of patient adoption of DTx is the possibility to address co-morbidities of chronic disease,103 such as depression104 and fatigue,105 particularly for patients who feel that their physician does not take the time to tackle these issues.
Prescription Practices for Digital Therapeutics
Prodan et al observed that there is scarce information on DTx prescription practices as the phenomenon is rather new.97 In Germany, DiGA are prescribed on paper by primary care physicians and psychotherapists; however, these paper prescriptions complicate the general workflow of the prescription process.97 The prescription system utilises a bottom-up approach, in which developers directly target patients, who usually then ask their physicians for a prescription, or pursue direct reimbursement from the statutory health insurance companies.97 In France, physicians can prescribe DTx that are included in the List des Produits et Prestations Remboursables (LPP), and in Belgium, medical doctors are allowed to prescribe DTx to targeted broad patient groups.97 In the UK, DTx can be prescribed by GPs provided the therapeutics have been commissioned by the relevant clinical commissioning group/NHS trust group.97
Carl et al, in the US, noted that “applying the traditional prescription-based medical approval paradigm to DTx for mental health could ultimately undermine and limit the broad accessibility of these software-based innovations that have been explicitly designed to expand the accessibility of care”. 106
Patient Perspectives on Digital Therapeutics
A US study of patient perspectives on app-based digital treatments for drug use disorders showed that participants preferred to have app-related conversations incorporated into their existing healthcare appointments, rather than attending additional visits to facilitate the use of the apps.107 Nearly all participants favoured receiving support from a clinician rather than no support for using the apps, as well as follow-up support via low-burden methods, such as phone calls or secure messaging.107
In a US questionnaire-based study of older adults with hearing loss, half the participants reported that DTx helped them to adjust to their new hearing aids.108
Willingness to use (WTU) and willingness to pay (WTP) for digital health interventions are key concepts that need to be quantified and understood in the quest to expand digital healthcare in different patient populations.109–114 A study by Lee et al in Korea showed that the WTU and WTP for digital health interventions differed based on the individual’s demographics, health status and previous experience with healthcare services.114 Lupiáñez-Villanueva et al reported that recommendations for DTx by doctors was associated with an increase in both WTU and WTP in Germany and the Netherlands.110
Wang et al suggested that changes in values, culture and customs over time may change patients’ perception of the same digital content, which could lead to changes in the efficacy of DTx.5 These authors commented that DTx require periodic verification, even after approval, to address the theoretical DTx “expiration date”.5
Factors That Potentially Impact Adoption of Digital Therapeutics
DTx uptake is suboptimal even in Germany, a pioneer of DTx prescription, access and reimbursement, where there are reports of almost two-thirds of patients being unaware of DTx.72 Potential factors that may contribute to such low rates of DTx adoption include lack of harmonisation in regulatory requirements and reimbursement; sociodemographic factors; health status; ethical concerns; challenges surrounding the use and validation of AI; knowledge and awareness among HCPs and patients, and data standards and interoperability. These are described in the following sections.
Lack of Harmonisation in Regulatory Requirements and Reimbursement
There are several key challenges in adoption of DTx in Europe at country level. Although DTx are governed by the EU MDR, these regulations are interpreted differently by different countries, leading to a lack of harmonisation in regulatory requirements, evidence requirements and value assessment processes.57 Inadequate funding and the absence of standardised or specific reimbursement pathways for DTx in most countries are also likely to impact the adoption of DTx in Europe.57
The outlook for DTx is changing as these tools become more technologically advanced, and some countries are adapting their device classifications depending on specific features.73 As well as the variation in the overall reimbursement landscape, there are differences in definitions, terminology and payment approaches.73 This complex scenario demonstrates how fragmented the regulatory systems for DTx are across Europe and is expected to have a direct impact on the commercialisation of and access to DTx.73 The harmonisation of the Health Technology Assessment Regulation (HTAR), which entered into force in January 2022 and applies as of January 2025,115 might partly address the lack of harmonisation. There are joint consultation opportunities among the HTA stakeholder network in different member states that also apply for DTx that are “high risk” medical devices according to the MDR.
Sociodemographic Factors
At the societal level, not all communities or populations have the resources or infrastructure to take advantage of digital tools.116 Social factors that potentially impact adoption of DTx include the geographical location of patients, with those in rural locations likely to have less access to internet infrastructure, and slower or more unstable internet services, compared with those in urban locations.117 Patients from deprived areas may also be more likely to lack access to DTx and the internet at home.117 There is also evidence to indicate that populations who are already subject to disadvantage and worse health outcomes are also subject to digital exclusion, but the relationship is complex.117
Patient characteristics are also likely to influence DTx adoption rates. Age is an important factor, as older individuals may be less likely to own a smartphone or use the internet.117 A study in Belgium on an app to examine medication adherence highlighted age as a barrier to the uptake of digital tools, with a large subset of older patients unwilling to participate in the study or to use the app.118 Income is also an important consideration: individuals with lower income may be less likely to have a smartphone or access to the internet at home.117 There are few studies on ethnicity and digital exclusion, with differences in internet access explained by the age and income profile of the different ethnic groups.117
A snapshot of attitudes towards health digitisation among internet users selected from the general population in Germany in 2020 showed that the majority of participants expected digitisation to affect healthcare; however, the interest in and use of digital technologies for health-related purposes was not yet widespread.119 Age, education, and household income were associated with digital technology use.119 Younger, more educated and wealthier participants were more likely to use digital technologies for health-related purposes and reported higher digital literacy.119
Interim analysis results from the study of real-life acceptability of an online blended psychological treatment (deprexis)120 for patients with depression in France (DARE study)121 showed that only 33.9% of patients accepted the idea of a DTx like deprexis, with financial issues (83.3%), digital reluctancy (33.3%), and other issues, such as loneliness and lack of interest in therapy (19.9%) cited as reasons for refusal.122 Marital status, along with Patient Health Questionnaire-9 (PHQ-9)123 score, was linked to acceptability of this DTx.122 The significance of marital status in adoption of DTx challenges the impact of social context and indicates that acceptability of DTx may be influenced more by human characteristics and circumstances than clinical profile.
Health Status
An interview-based study to explore DTx-acceptance in patients with mild or moderate depression in Germany showed that patients did not perceive DTx as a substitute for face-to-face treatment, and difficult stages of depression or long-time experience of the disorder were perceived as hurdles for DTx use.124 Furthermore, recommendations for DTx by GPs were only partly relevant for patients.124
Ethical Concerns
Implementing DTx across healthcare systems raises a number of ethical concerns,1 including safety and oversight, accountability, privacy, confidentiality, data protection, transparency, consent, access, and bias and fairness.1,116,125–127 Furthermore, clinical trials to assess DTx pose new logistical, statistical and ethical challenges.1 Harnessing the full potential of DTx must be paralleled by the ethical and equitable implementation of these therapeutics.128
According to Martinez-Martin: “There will be continuing tension between the accessibility afforded by digital technology, the potential exposure of patient data through these tools, and appropriate balancing of accountability and liability concerns.” 116
Challenges Surrounding the Use and Validation of Artificial Intelligence
Challenges surrounding the use and validation of AI include lack of understanding, which impedes the development of reliable and accurate AI systems; processing power requirements, leading to high infrastructure costs; limited data availability or lack of access to the required volume or quality of data; unreliable results due to factors such as biased or incomplete datasets and algorithmic limitations; lack of trust for AI systems; unclear objectives and key performance indicators, and complexities of implementation.129 The use of AI is a relevant issue for DTx as some therapeutics are coupled with AI techniques for their functioning.1
A study conducted by Petersson et al comprising semi-structured interviews with healthcare leaders highlighted several implementation challenges in relation to AI.130 These included conditions external to the healthcare system, specifically addressing liability issues and legal information sharing; complying with standards and quality requirements, and integrating AI-relevant learning in higher education for HCPs.130 Challenges in capacity for strategic change management were also cited, including developing a systematic approach to and ascertaining resources for AI implementation; involving staff throughout the implementation of AI systems, and developing new strategies for internal and external collaboration.130 Transformation of healthcare professions and practices were also pinpointed, in terms of managing new roles in care processes and building trust for acceptance of AI systems in clinical practice.130
Knowledge and Awareness Among Healthcare Professionals and Patients
A paucity of scientific information on DTx may impact HCPs’ confidence to prescribe these therapeutics and could contribute to low adoption rates.37 In a review of studies from Europe and North America, Morita et al identified knowledge gaps and the lack of collaboration across disciplines as barriers to adoption of digital tools, stating that “Technological development dominates over the human-centric part of the equation.”131
A study in England highlighted barriers to adoption of DTx, including user perception (ie, the perception that digital is not for everyone, with older age, learning or language difficulties or lack of access to technology proposed as potential barriers), absence of formulary for digital solutions and “initiative fatigue” for HCPs.132 Issues surrounding implementation included lack of expertise among HCPs for promoting digital health and limited funding for promotional activities, as well as the absence of established models for digital implementation.132 Potential issues around adherence to DTx included the concept that, unlike medicines, there are no clearly defined points, such as the ordering of repeat prescriptions, to prompt review or indicate to the clinician that a course of treatment had been completed.132 For some patients, the resulting increased responsibility placed on them may be empowering, for others, it may lead to poor adherence to DTx.132
Data Standards and Interoperability
Interoperability in healthcare refers to timely and secure access, integration and use of electronic health data so that it can be used to optimise health outcomes for individuals and populations.133 The benefits of interoperability in healthcare include better care coordination and data-driven improvements in patient care.133 Electronic health information, including from electronic health records, is needed to develop digital health tools. The seamless flow of data and the realisation of the opportunities arising from digital health innovations require data standards and interoperability.134,135
Lehne et al discerned that most medical data currently lack interoperability, with data hidden in isolated databases, incompatible systems and proprietary software.136 This impedes data exchange, analysis and interpretation, and prevents DTx, which rely on these data, from being implemented at scale and used to their full potential.136,137
HCPs may be reluctant to adopt digital tools that are not integrated with electronic health records.138
Improving Adoption of Digital Therapeutics in Europe
The healthcare sector in Europe has been struggling to accelerate digital adoption.139 Europe would benefit from a unified market for DTx and digital health solutions in general.67 Efforts to improve access to DTx across Europe could include harmonisation of regulatory requirements; collaboration between countries to enable harmonisation of clinical evidence requirements; value assessment processes that are tailored for DTx; clear and transparent national pathways for DTx pricing and reimbursement, and explicit and budgeted funding, with no or limited financial burden on patients.57
Developers, researchers and clinicians need to consider the usability and accessibility of DTx for culturally diverse populations and marginalised groups.116,140 DTx should be evaluated on how applicable they are to diverse populations (eg, individuals from different age groups, ethnicities, linguistic backgrounds and disability statuses).116 If DTx are to fulfil the promise of increased access to healthcare, improvements are needed in infrastructure, training, and availability of clinician oversight to better serve low-income demographics.116
DTx have a potentially important role in supporting conventional medicine and reducing health inequalities across Europe;2 however, lack of access, skills and motivation for using digital technologies, ie, digital exclusion, could lead to worse health outcomes.117,141 Investment in digital inclusion, such as addressing barriers of access and skills, as well as trust and privacy concerns, and designing DTx to address the specific needs of disadvantaged groups, is essential to mitigate against widening health inequalities with the use of these therapeutics.117,141
As DTx become more popular, it is important to consider how they can be integrated into healthcare in an ethical manner.116 This requires continued attention to appropriate oversight, models of care and data protection.116 For the effective and safe proliferation of DTx, public institutions at all levels should create appropriate frameworks that ensure data privacy and protection.1,71
HCPs require complete and correct information about DTx to address knowledge gaps37,131 and to enable them to educate their patients about these tools.90 Ideally, HCPs should receive specific training on the use, value and potential limitations of DTx to inform them how to properly prescribe these therapeutics to their patients.1,64,142 Digital technologies that reduce clinician burden and are easily interpretable have been suggested to have the greatest likelihood of uptake.143 Developers of DTx should always consider how the novel technology will be introduced into the clinical workflow,144 and during which type of touchpoints with patients, as well as creating specific, informative material to facilitate onboarding of patients on these tools.
The integration of DTx into healthcare and adoption of these therapeutics by patients, requires a cooperative, interdisciplinary approach between researchers, manufacturers, governments and HCPs to ensure technologies are effective and regulated, and systems are in place to drive change management97 and overcome engagement barriers.5,57,131,145 Cripps and Scarbrough, in England, recommend shifting the focus from the DTx technology to considering the motivations of users and constraints within specific contexts.146 These practitioners advocate for a wider approach to integration of DTx that incorporates clinical and behavioural insights, process engineering and knowledge management.146
A further consideration is that clinical studies of DTx often lack rigor and inclusivity.11,76,147 Robust clinical trials with objective endpoints are needed to evaluate these interventions.11 Furthermore, improved sociodemographic representation is needed in DTx clinical trials, particularly for underserved populations typically underrepresented in clinical trials.148
The potential benefits of DTx might extend beyond improvements to the patient’s clinical condition and quality of life and into the dimension of health economics; for example, enabling the patient to return to work, and reducing the duration and cost of sick leave. Stakeholders’ needs and perspectives may differ on this point, with employers potentially more interested than payers in the ability of DTx to help a patient return to work.149 As noted by Bullard, economic evaluation of DTx is critical to payer reimbursement and provider adoption, and conducting a comprehensive and reflective economic evaluation of DTx requires a broader assessment of costs and outcomes that includes clinical and non-health benefits, as well as opportunity costs and gains.150 Development of the ideal framework for DTx to drive adoption should include consideration of the health economic aspect of these therapeutics, and how they might contribute to reduced health economic burden.
Proposed Framework for Improved Uptake of Digital Therapeutics in Europe
A proposed framework for improved uptake of DTx in Europe, showing the approach from development to launch and through follow-up of DTx, is shown in Table 1.
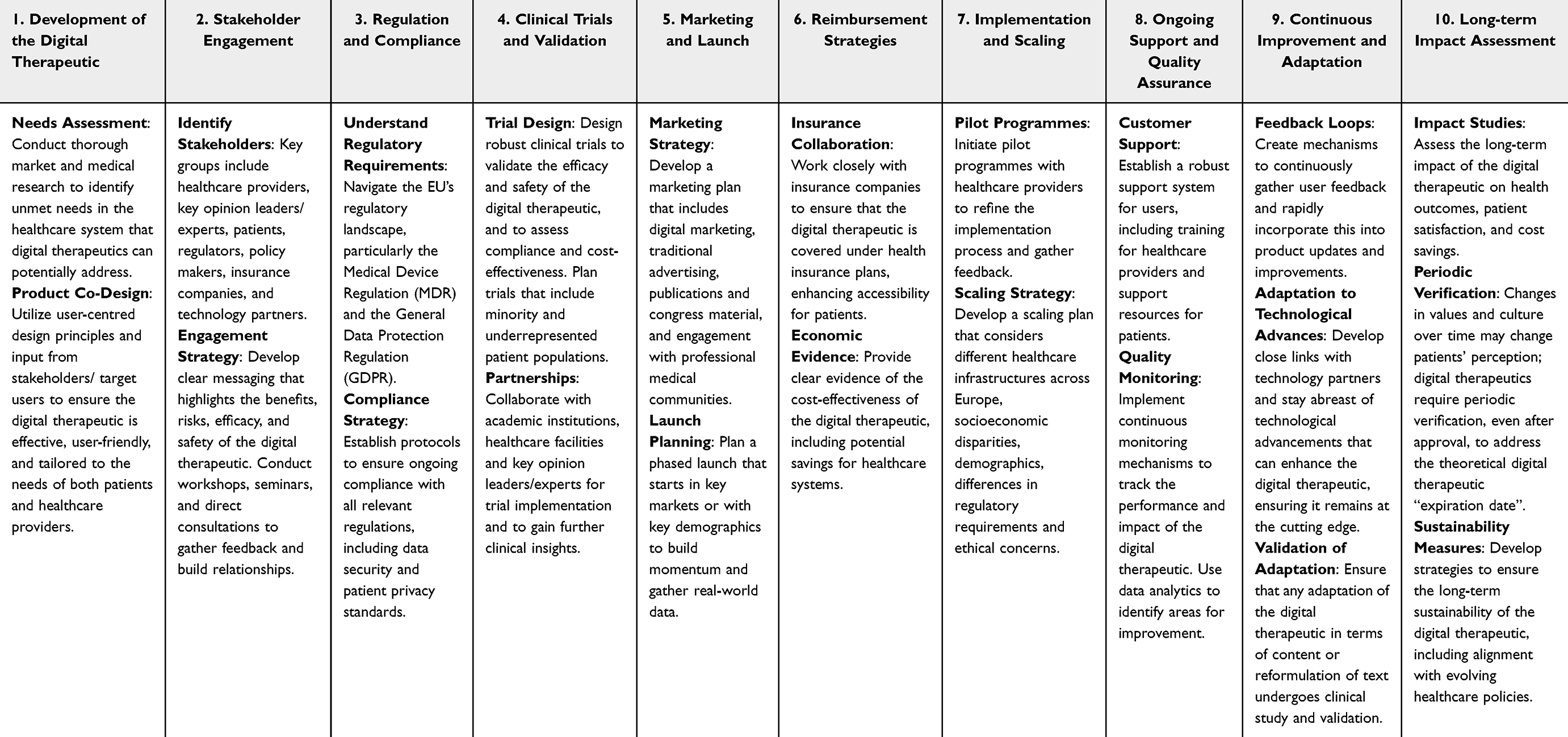 |
Table 1 Proposed Framework for Development, Launch, and Follow-Up of Digital Therapeutics in Europe |
Future Prospects and Conclusions
DTx are an evolving medical therapy that can support conventional medicine to address gaps in patient care, and potentially reduce current healthcare burden and health inequalities across Europe. Integrating DTx alongside conventional medicine into healthcare systems enables HCPs to deliver more personalised treatment for patients, thereby contributing to improved overall health outcomes. This integration requires equity, accessibility, and education of HCPs and patients on these therapeutics. The intrinsic value of DTx depends on their capacity to be safe, effective and convenient for patients and society.1 Provided access and ethical challenges can be addressed, DTx could provide innovative and equitable healthcare.116
The adoption of DTx in Europe is limited and fragmented across the continent. Potential reasons for this include the lack of regulatory alignment for DTx between countries, sociodemographic factors, such as age, education and income, and knowledge gaps among HCPs. Strategies that could improve access and adoption across Europe include harmonisation of regulatory requirements and reimbursement pathways, infrastructure and clinician oversight to better serve low-income demographics, and education and training on DTx for HCPs. Investment in digital inclusion is essential to mitigate against widening health inequalities with the use of DTx. Finally, to reduce the risk of non-adoption or abandonment of new DTx, it is critical to authentically engage HCPs and patients upfront in the design of healthcare solutions for the future.145 An ecosystem-centric approach for the development of DTx is vital to ensure holistic integration and sustainable adoption of these therapeutics within healthcare systems. This approach involves engaging a wide range of stakeholders, including healthcare providers, patients, regulators, policymakers, insurers, and technology developers, from the early stages of development through to implementation and scaling. Implementing an ecosystem-centric approach ensures that DTx are designed to meet the diverse needs of all stakeholders, facilitating smoother integration into existing healthcare workflows, improving patient outcomes, and ensuring long-term viability and acceptance.
Acknowledgments
Medical writing support was provided by Dr Brigitte Scott.
Disclosure
Dr Shaantanu Donde reports being an employee of Viatris Inc, and holds stock options of Viatris and some other pharma companies. Ms Tonya Winders reports personal fees from AstraZeneca, personal fees from Sanofi Regeneron, personal fees from GSK, personal fees from Insmed, personal fees from Chiesi, personal fees from Roche, personal fees from Novartis, personal fees from MSD, outside the submitted work; Mr Joris van Vugt reports being an employee of Viatris. The publication of this article was funded by Viatris. Dr Amelie Fassbender reports being an employee of Viatris. The authors report no other conflicts of interest in this work.
References
1. Refolo P, Sacchini D, Raimondi C, Spagnolo AG. Ethics of digital therapeutics (DTx). Eur Rev Med Pharmacol Sci. 2022;26(18):6418–6423. PMID: 36196692. doi:10.26355/eurrev_202209_29741
2. Digital Therapeutics Alliance. Understanding DTx. A New Category of Medicine. Available at: https://dtxalliance.org/understanding-dtx/.
3. Hong JS, Wasden C, Han DH. Introduction of digital therapeutics. Comput Methods Programs Biomed. 2021;209:106319. PMID: 34364181. doi:10.1016/j.cmpb.2021.106319
4. Stanojevic C, Bennett CC, Sabanovic S, et al. Conceptualizing socially-assistive robots as a digital therapeutic tool in healthcare. Front Digit Health. 2023;5:1208350. PMID: 37519896; PMCID: PMC10382135. doi:10.3389/fdgth.2023.1208350
5. Wang C, Lee C, Shin H. Digital therapeutics from bench to bedside. NPJ Digit Med. 2023;6(1):38. PMID: 36899073; PMCID: PMC10006069. doi:10.1038/s41746-023-00777-z
6. Digital Therapeutics Alliance. DTA’s adoption & interpretation of ISO’s DTx definition. June 2023. Available at: https://dtxalliance.org/wp-content/uploads/2023/06/DTA_FS_New-DTx-Definition.pdf.
7. International Organization for Standardization (ISO). ISO/TR 11147: health informatics— personalized digital health—Digital therapeutics health software systems. Available at: https://www.iso.org/standard/83767.html.
8. Courtet P, Amiot O, Baca-Garcia E, et al. Understanding the potential of digital therapies in implementing the standard of care for depression in Europe. Eur Psychiatry. 2023;66(1):e82. PMID: 37872705; PMCID: PMC10755564. doi:10.1192/j.eurpsy.2023.2453
9. Biskupiak Z, Ha VV, Rohaj A, Bulaj G. Digital therapeutics for improving effectiveness of pharmaceutical drugs and biological products: preclinical and clinical studies supporting development of drug + digital combination therapies for chronic diseases. J Clin Med. 2024;13(2):403. PMID: 38256537; PMCID: PMC10816409. doi:10.3390/jcm13020403
10. Kario K, Nomura A, Harada N, et al. A multicenter clinical trial to assess the efficacy of the digital therapeutics for essential hypertension: rationale and design of the HERB-DH1 trial. J Clin Hypertens. 2020;22(9):1713–1722. PMID: 32815648; PMCID: PMC7589405. doi:10.1111/jch.13993
11. Kario K, Harada N, Okura A. Digital Therapeutics in Hypertension: evidence and Perspectives. Hypertension. 2022;79(10):2148–2158. PMID: 35726619; PMCID: PMC9444254. doi:10.1161/HYPERTENSIONAHA.122.19414
12. Nomura A, Tanigawa T, Kario K, Igarashi A. Cost-effectiveness of digital therapeutics for essential hypertension. Hypertens Res. 2022;45(10):1538–1548. PMID: 35726085; PMCID: PMC9474296. doi:10.1038/s41440-022-00952-x
13. Wolff J, Stupin J, Olschewski J, et al. Digital therapeutic to improve cancer-related well-being: a pilot randomized controlled trial. Int J Gynecol Cancer. 2023;33(7):1118–1124. PMID: 37321673. doi:10.1136/ijgc-2023-004304
14. Boesch M, Baty F, Rassouli F, et al. Non-pharmaceutical interventions to optimize cancer immunotherapy. Oncoimmunology. 2023;12(1):2255459. PMID: 37791231; PMCID: PMC10543347. doi:10.1080/2162402X.2023.2255459
15. Payne S, Begovic D, Salifu Y, et al. Applying digital health in cancer and palliative care in Europe: Policy Recommendations from an International Expert Workshop (MyPal Project). J Palliat Med. 2024;27(2):216–223. PMID: 37738323. doi:10.1089/jpm.2023.0309
16. Kumbhare SV, Francis-Lyon PA, Kachru D, et al. Digital therapeutics care utilizing genetic and gut microbiome signals for the management of functional gastrointestinal disorders: results from a preliminary retrospective study. Front Microbiol. 2022;13:826916. PMID: 35391720; PMCID: PMC8983270. doi:10.3389/fmicb.2022.826916
17. Hasan SS, Ballou S, Keefer L, Vasant DH. Improving access to gut-directed hypnotherapy for irritable bowel syndrome in the digital therapeutics’ era: are mobile applications a “smart” solution? Neurogastroenterol Motil. 2023;35(4):e14554. PMID: 36847206. doi:10.1111/nmo.14554
18. Brenner DM, Ladewski AM, Kinsinger SW. Development and current state of digital therapeutics for irritable bowel syndrome. Clin Gastroenterol Hepatol. 2024;22(2):222–234. PMID: 37743035. doi:10.1016/j.cgh.2023.09.013
19. Saleh ZM, Chey WD, Berry SK. Behavioral health digital therapeutics for patients with irritable bowel syndrome: a primer for gastroenterologists. Am J Gastroenterol. 2023;118(8):1311–1313. PMID: 36799911. doi:10.14309/ajg.0000000000002220
20. Lackner JM. Skills over pills? A clinical gastroenterologist’s primer in cognitive behavioral therapy for irritable bowel syndrome. Expert Rev Gastroenterol Hepatol. 2020;14(7):601–618. PMID: 32510249. doi:10.1080/17474124.2020.1780118
21. Oddsson SJ, Gunnarsdottir T, Johannsdottir LG, et al. A new digital health program for patients with inflammatory bowel disease: preliminary program evaluation. JMIR Form Res. 2023;7:e39331. PMID: 37115598; PMCID: PMC10182451. doi:10.2196/39331
22. Kallestad H, Saksvik S, Vedaa Ø, et al. Digital cognitive-behavioural therapy for insomnia compared with digital patient education about insomnia in individuals referred to secondary mental health services in Norway: protocol for a multicentre randomised controlled trial. BMJ Open. 2021;11(6):e050661. PMID: 34183350; PMCID: PMC8240575. doi:10.1136/bmjopen-2021-050661
23. Digital Therapeutics Alliance. DTx Product Profile. Sleepio. 2024. Available at: https://dtxalliance.org/products/sleepio/#:~:text=Sleepio.
24. Silberman J, Sarlati S, Harris B, et al. A digital approach to asthma self-management in adults: protocol for a pragmatic randomized controlled trial. Contemp Clin Trials. 2022;122:106902. PMID: 36049674. doi:10.1016/j.cct.2022.106902
25. Zhang B, Buendia R, Iannoti N, et al. Home-based digital assessments with applied sentiment & emotion ai capture improved quality-of-life in asthma patients.
26. Spielmanns M, Boeselt T, Huber S, et al. Impact of a smartphone application (KAIA COPD app) in combination with Activity Monitoring as a maintenance prOgram following PUlmonary Rehabilitation in COPD: the protocol for the AMOPUR Study, an international, multicenter, parallel group, randomized, controlled study. Trials. 2020;21(1):636. PMID: 32653025; PMCID: PMC7353698. doi:10.1186/s13063-020-04538-1
27. Brezing CA, Brixner DI. The rise of prescription digital therapeutics in behavioral health. Adv Ther. 2022;39(12):5301–5306. PMID: 36242730; PMCID: PMC9569000. doi:10.1007/s12325-022-02320-0
28. Velez FF, Malone DC. Cost-effectiveness analysis of a prescription digital therapeutic for the treatment of opioid use disorder. J Mark Access Health Policy. 2021;9(1):1966187. PMID: 34434535; PMCID: PMC8381930. doi:10.1080/20016689.2021.1966187
29. Xiong X, Braun S, Stitzer M, et al. Evaluation of real-world outcomes associated with use of a prescription digital therapeutic to treat substance use disorders. Am J Addict. 2023;32(1):24–31. PMID: 36264211; PMCID: PMC10091717. doi:10.1111/ajad.13346
30. Luderer H, Enman N, Gerwien R, et al. A prescription digital therapeutic to support unsupervised buprenorphine initiation for patients with opioid use disorder: protocol for a proof-of-concept study. JMIR Res Protoc. 2023;12:e43122. PMID: 36662568; PMCID: PMC9898828. doi:10.2196/43122
31. Yoo SG, Kim DJ, Chun JW, Choi IY. Developing a cost-effectiveness model of digital therapeutics for smoking cessation. Stud Health Technol Inform. 2024;310:1548–1549. PMID: 38269739. doi:10.3233/SHTI231287
32. Kim M, Choi HJ. Digital therapeutics for obesity and eating-related problems. Endocrinol Metab. 2021;36(2):220–228. PMID: 33761233; PMCID: PMC8090472. doi:10.3803/EnM.2021.107
33. Carette C, Rives-Lange C, Czernichow S. Medications for the treatment of obesity. J Visc Surg. 2023;160(2S):S12–S14. PMID: 36725455. doi:10.1016/j.jviscsurg.2022.12.002
34. Moravcová K, Karbanová M, Bretschneider MP, Sovová M, Ožana J, Sovová E. Comparing digital therapeutic intervention with an intensive obesity management program: randomized controlled trial. Nutrients. 2022;14(10):2005. PMID: 35631145; PMCID: PMC9143861. doi:10.3390/nu14102005
35. Pinarello C, Elmers J, Inojosa H, Beste C, Ziemssen T. Management of multiple sclerosis fatigue in the digital age: from assessment to treatment. Front Neurosci. 2023;17:1231321. PMID: 37869507; PMCID: PMC10585158. doi:10.3389/fnins.2023.1231321
36. Wu X, Deng H, Jian S, et al. Global trends and hotspots in the digital therapeutics of autism spectrum disorders: a bibliometric analysis from 2002 to 2022. Front Psychiatry. 2023;14:1126404. PMID: 37255688; PMCID: PMC10225518. doi:10.3389/fpsyt.2023.1126404
37. Clarke O. Digital therapeutics in Europe: what is the state of play? 23, October 2023. Available at: https://www.osborneclarke.com/insights/digital-therapeutics-europe-what-state-play.
38. Wake DJ, He J, Czesak AM, Mughal F, Cunningham SG. MyDiabetesMyWay: an evolving national data driven diabetes self-management platform. J Diabetes Sci Technol. 2016;10(5):1050–1058. PMID: 27162192; PMCID: PMC5032956. doi:10.1177/1932296816648168
39. Ramakrishnan P, Yan K, Balijepalli C, Druyts E. Changing face of healthcare: digital therapeutics in the management of diabetes. Curr Med Res Opin. 2021;37(12):2089–2091. PMID: 34511002. doi:10.1080/03007995.2021.1976737
40. Fundoiano-Hershcovitz Y, Feniger E, Dar S, Ritholz M, Schorr AB, Goldstein P. Digital therapeutics for type 2 diabetes: incorporating coaching support and validating digital monitoring. J Diabetes Sci Technol. 2021;15(5):1188–1189. PMID: 34024167; PMCID: PMC8442174. doi:10.1177/19322968211017901
41. Fundoiano-Hershcovitz Y, Hirsch A, Dar S, Feniger E, Goldstein P. Role of digital engagement in diabetes care beyond measurement: retrospective cohort study. JMIR Diabetes. 2021;6(1):e24030. PMID: 33599618; PMCID: PMC7932839. doi:10.2196/24030
42. Kamat T. Digital therapeutics can improve medication adherence in diabetes. J Family Med Prim Care. 2020;9(11):5806–5807. PMID: 33532443; PMCID: PMC7842486. doi:10.4103/jfmpc.jfmpc_1252_20
43. Joshi S, Verma R, Lathia T, et al. Fitterfly diabetes CGM digital therapeutics program for glycemic control and weight management in people with type 2 diabetes mellitus: real-world effectiveness evaluation. JMIR Diabetes. 2023;8:e43292. PMID: 37133922; PMCID: PMC10193208. doi:10.2196/43292
44. Krishnakumar A, Verma R, Chawla R, et al. Evaluating glycemic control in patients of south asian origin with type 2 diabetes using a digital therapeutic platform: analysis of real-world data. J Med Internet Res. 2021;23(3):e17908. PMID: 33764306; PMCID: PMC8074838. doi:10.2196/17908
45. Verma R, Bhardwaj S, Lathia T, et al. Personalized glycemic response led digital therapeutics program improves time in range in a period of 14 days. Int J Diabetes Dev Ctries. 2023;43(3):425–432. PMID: 35892065; PMCID: PMC9303844. doi:10.1007/s13410-022-01111-1
46. Nordyke RJ, Appelbaum K, Berman MA. Estimating the impact of novel digital therapeutics in type 2 diabetes and hypertension: health economic analysis. J Med Internet Res. 2019;21(10):e15814. PMID: 31599740; PMCID: PMC6914106. doi:10.2196/15814
47. Bollyky JB, Melton ST, Xu T, Painter SL, Knox B. The effect of a cellular-enabled glucose meter on glucose control for patients with diabetes: prospective pre-post study. JMIR Diabetes. 2019;4(4):e14799. PMID: 31593545; PMCID: PMC6803884. doi:10.2196/14799
48. Wilson-Anumudu F, Quan R, Castro Sweet C, et al. Early insights from a digitally enhanced diabetes self-management education and support program: single-arm nonrandomized trial. JMIR Diabetes. 2021;6(1):e25295. PMID: 33616533; PMCID: PMC7939937. doi:10.2196/25295
49. World Health Organization. The global burden of disease: 2004 update. Geneva. 2004. Available at: https://iris.who.int/bitstream/handle/10665/43942/9789241563710_eng.pdf.
50. Torous J, Bucci S, Bell IH, et al. The growing field of digital psychiatry: current evidence and the future of apps, social media, chatbots, and virtual reality. World Psychiatry. 2021;20(3):318–335. PMID: 34505369; PMCID: PMC8429349. doi:10.1002/wps.20883
51. Elison S, Ward J, Williams C, et al. Feasibility of a UK community-based, eTherapy mental health service in Greater Manchester: repeated-measures and between-groups study of ‘living life to the full interactive’, ‘sleepio’ and ‘breaking free online’ at ‘self help services’. BMJ Open. 2017;7(7):e016392. PMID: 28729322; PMCID: PMC5541623. doi:10.1136/bmjopen-2017-016392
52. McIntyre RS, Alsuwaidan M, Baune BT, et al. Treatment-resistant depression: definition, prevalence, detection, management, and investigational interventions. World Psychiatry. 2023;22(3):394–412. PMID: 37713549; PMCID: PMC10503923. doi:10.1002/wps.21120
53. Schiller CE, Prim J, Bauer AE, et al. Efficacy of virtual care for depressive disorders: systematic review and meta-analysis. JMIR Ment Health. 2023;10:e38955. PMID: 36622747; PMCID: PMC9871881. doi:10.2196/38955
54. Karyotaki E, Efthimiou O, Miguel C, et al.,;. Internet-based cognitive behavioral therapy for depression: a systematic review and individual patient data network meta-analysis. JAMA Psychiatry. 2021;78(4):361–371. PMID: 33471111; PMCID: PMC8027916. doi:10.1001/jamapsychiatry.2020.4364
55. Digital Therapeutics Alliance. DTx Product Profile. Daylight. 2024. Available at: https://dtxalliance.org/products/daylight/.
56. Benchekroun M, Velmovitsky PE, Istrate D, Zalc V, Morita PP, Lenne D. Cross dataset analysis for generalizability of HRV-based stress detection models. Sensors. 2023;23(4):1807. PMID: 36850407; PMCID: PMC9960690. doi:10.3390/s23041807
57. European Federation of Pharmaceutical Industries and Associations (efpia). Improving access to digital therapeutics in Europe. June 2023. Available from: https://www.efpia.eu/media/677347/improving-access-to-digital-therapeutics-in-europe.pdf.
58. Sapanel Y, Tadeo X, Brenna CTA, et al. Economic evaluation associated with clinical-grade mobile app-based digital therapeutic interventions: systematic review. J Med Internet Res. 2023;25:e47094. PMID: 37526973; PMCID: PMC10427932. doi:10.2196/47094
59. Liu T, Zhan Y, Chen S, Zhang W, Jia J. Cost-effectiveness analysis of digital therapeutics for home-based cardiac rehabilitation for patients with chronic heart failure: model development and data analysis. Cost Eff Resour Alloc. 2023;21(1):82. PMID: 37932748; PMCID: PMC10626728. doi:10.1186/s12962-023-00489-x
60. Liu T, Tang Z, Cai C, et al. Cost-effectiveness analysis of digital therapeutics for home-based cardiac rehabilitation for patients with atrial fibrillation after catheter ablation. Digit Health. 2023;9:20552076231211548. PMID: 38025109; PMCID: PMC10631335. doi:10.1177/20552076231211548
61. Park C, Yi C, Choi WJ, Lim HS, Yoon HU, You SJH. Long-term effects of deep-learning digital therapeutics on pain, movement control, and preliminary cost-effectiveness in low back pain: a randomized controlled trial. Digit Health. 2023;9:20552076231217817. PMID: 38053732; PMCID: PMC10695084. doi:10.1177/20552076231217817
62. Carrera A, Manetti S, Lettieri E. Rewiring care delivery through Digital Therapeutics (DTx): a machine learning-enhanced assessment and development (M-LEAD) framework. BMC Health Serv Res. 2024;24(1):237. PMID: 38395905; PMCID: PMC10885456. doi:10.1186/s12913-024-10702-z
63. Phan P, Mitragotri S, Zhao Z. Digital therapeutics in the clinic. Bioeng Transl Med. 2023;8(4):e10536. PMID: 37476062; PMCID: PMC10354777. doi:10.1002/btm2.10536
64. Nevicky P, Baresova Z, Zaleska M, et al. A Promising Outlook for Digital Therapeutics (DTx) in Europe – how can biopharma capitalise? Deloitte. November 2023. Available at: https://www2.deloitte.com/cz/en/pages/life-sciences-and-healthcare/articles/a-promising-outlook-for-digital-therapeutics--dtx--in-europe.html.
65. Spreafico A, Coder M, Boccardo V, Lopes-Fernandes E, Milburn K DTx policy pathways: the evolving scenario in Euro pe. landscape analysis & converging trends. Digital Therapeutics Policy Report. Available at: https://3783108.fs1.hubspotusercontent-na1.net/hubfs/3783108/DTxPolicyReport/DTA-HW_DTxPolicyPathways_June23.pdf.
66. Stevovic J Digital Health Global. The main DTx reimbursement frameworks. 23, August 2022. Available at: https://www.digitalhealthglobal.com/the-main-dtx-reimbursement-frameworks/.
67. Ahlqvist J, Kalliola M. How can digital therapeutics help Europe? Sitra working paper. 2021. Available at: https://media.sitra.fi/app/uploads/2021/11/sitra-how-can-digital-therapeutics-help-europe.pdf.
68. Heese F, Offenhammer J, Bäumler T, Ph D. Digital therapeutics should take a playbook from big pharma. Available at: https://www.oliverwyman.com/our-expertise/perspectives/health/2023/july/digital-therapeutics-should-take-a-playbook-from-big-pharma.html.
69. Nomura A. Digital health, digital medicine, and digital therapeutics in cardiology: current evidence and future perspective in Japan. Hypertens Res. 2023;46(9):2126–2134. PMID: 37258624; PMCID: PMC10230462. doi:10.1038/s41440-023-01317-8
70. Kipentzoglou N, Zegaoui Y, Satherley A, Whitehouse J, Thompson A Challenges and opportunities for digital therapeutics: key requirements to demonstrate value across the EU, England and the US. Lightning Health. Available at: https://lightning.health/wp-content/uploads/2021/11/Challenges-and-opportunities-for-digital-therapeutics-key-requirements-to-demonstrate-value-across-The-EU-England-and-The-US.pdf.
71. Arcà E, Heldt D Digital therapeutics landscape in Europe: the cases of Germany and the UK. Open Health 2-16. Available at: https://f.hubspotusercontent30.net/hubfs/20088388/DigitalTherapeuticsInEurope_WP_8_31_21.pdf.
72. Telgheder M Wie oft werden DiGA verschrieben? [How often are DiGAs prescribed?]. 2023. Available at: https://www.handelsblatt.com/inside/digital-health/app-auf-rezept-wie-oft-werden-diga-verschrieben/v_detail_tab_print/29194504.html.
73. Mantovani A, Leopaldi C, Nighswander CM, Di Bidino R. Access and reimbursement pathways for digital health solutions and in vitro diagnostic devices: current scenario and challenges. Front Med Technol. 2023;5:1101476. PMID: 36891483; PMCID: PMC9986593. doi:10.3389/fmedt.2023.1101476
74. mHealth Belgium. First app in level M3 of validation pyramid. 19, April 2022. Available at: https://mhealthbelgium.be/news/persbericht-duidelijk-financieringskader-nodig-voor-doorbraak-medische-apps-in-belgie-4.
75. Digital Austria. Digital Austria Act. Available at: https://www.digitalaustria.gv.at/Strategien/Digital-Austria-Act-das-digitale-Arbeitsprogramm-der-Bundesregierung.html.
76. Huh KY, Oh J, Lee S, Yu KS. Clinical evaluation of digital therapeutics: present and future. Healthc Inform Res. 2022;28(3):188–197. PMID: 35982593; PMCID: PMC9388922. doi:10.4258/hir.2022.28.3.188
77. Rego S, Henriques AR, Serra SS, Costa T, Rodrigues AM, Nunes F. Methods for the clinical validation of digital endpoints: protocol for a scoping review abstract. JMIR Res Protoc. 2023;12:e47119. PMID: 37883152; PMCID: PMC10636620. doi:10.2196/47119
78. Recchia G, Capuano DM, Mistri N, Verna R. Digital therapeutics: what they are, what they will be. Acta Sci Med Sci. 2020;4(3):1–9.
79. Digital Therapeutics Alliance (DTA). DTx Value Assessment & Integration. Available at: https://dtxalliance.org/advancing-dtx/dtx-value-guide/.
80. Goldsack JC, Coravos A, Bakker JP, et al. Verification, analytical validation, and clinical validation (V3): the foundation of determining fit-for-purpose for Biometric Monitoring Technologies (BioMeTs). NPJ Digit Med. 2020;3:55. PMID: 32337371; PMCID: PMC7156507. doi:10.1038/s41746-020-0260-4
81. Shah SS, Gvozdanovic A. Digital health; what do we mean by clinical validation? Expert Rev Med Devices. 2021;18(sup1):5–8. PMID: 34845960. doi:10.1080/17434440.2021.2012447
82. Voorheis P, Petch J, Pham Q, Kuluski K. Maximizing the value of patient and public involvement in the digital health co-design process: a qualitative descriptive study with design leaders and patient-public partners. PLOS Digit Health. 2023;2(10):e0000213. PMID: 37878566; PMCID: PMC10599516. doi:10.1371/journal.pdig.0000213
83. Sanz MF, Acha BV, García MF. Co-design for people-centred care digital solutions: a literature review. Int J Integr Care. 2021;21(2):16. PMID: 33981193; PMCID: PMC8086727. doi:10.5334/ijic.5573
84. O’Kelly N Digitising Clinical Pathways: why is co-design so important? Spirit Health. 5, May 2022. Available at: https://www.spirit-health.co.uk/blog/why-is-co-design-important.
85. Bird M, McGillion M, Chambers EM, et al. A generative co-design framework for healthcare innovation: development and application of an end-user engagement framework. Res Involv Engagem. 2021;7(1):12. PMID: 33648588; PMCID: PMC7923456. doi:10.1186/s40900-021-00252-7
86. Silvola S, Restelli U, Bonfanti M, Croce D. Co-design as enabling factor for patient-centred healthcare: a bibliometric literature review. Clinicoecon Outcomes Res. 2023;15:333–347. PMID: 37220481; PMCID: PMC10200122. doi:10.2147/CEOR.S403243
87. Meskó B, deBronkart D. Patient design: the importance of including patients in designing health care. J Med Internet Res. 2022;24(8):e39178. PMID: 36044250; PMCID: PMC9475404. doi:10.2196/39178
88. Secker-Johnson R, Nguyen T-M, Faber S, Jolyon A Jones Digital therapeutics: what drives clinician adoption? 14, July 2022. Available at: https://www.zs.com/insights/digital-therapeutics-what-drives-clinical-adoption-europe.
89. van Kessel R, Roman-Urrestarazu A, Anderson M, et al. Mapping factors that affect the uptake of digital therapeutics within health systems: scoping review. J Med Internet Res. 2023;25:e48000. PMID: 37490322; PMCID: PMC10410406. doi:10.2196/48000
90. Dahlhausen F, Zinner M, Bieske L, Ehlers JP, Boehme P, Fehring L. There’s an app for that, but nobody’s using it: insights on improving patient access and adherence to digital therapeutics in Germany. Digit Health. 2022;8:20552076221104672. PMID: 35811758; PMCID: PMC9260569. doi:10.1177/20552076221104672
91. Bhavnani S Barriers to digital therapeutics adoption. 17, August 2021. Available at: https://www.psychiatrictimes.com/view/barriers-to-digital-therapeutics-adoption.
92. Jakob R, Rudolf AM, Harperink S, et al. Prediction and prevention of non-adherence to digital health interventions. September 2020. Available at: https://www.c4dhi.org/projects/prediction-prevention-non-adherence/.
93. Baumel A, Yom-Tov E. Predicting user adherence to behavioral eHealth interventions in the real world: examining which aspects of intervention design matter most. Transl Behav Med. 2018;8(5):793–798. PMID: 29471424. doi:10.1093/tbm/ibx037
94. Meyerowitz-Katz G, Ravi S, Arnolda L, Feng X, Maberly G, Astell-Burt T. Rates of attrition and dropout in app-based interventions for chronic disease: systematic review and meta-analysis. J Med Internet Res. 2020;22(9):e20283. PMID: 32990635. doi:10.2196/20283
95. Linardon J, Fuller-Tyszkiewicz M. Attrition and adherence in smartphone-delivered interventions for mental health problems: a systematic and meta-analytic review. J Consult Clin Psychol. 2020;88(1):1–13. PMID: 31697093. doi:10.1037/ccp0000459
96. Baumel A, Muench F, Edan S, Kane JM. Objective user engagement with mental health apps: systematic search and panel-based usage analysis. J Med Internet Res. 2019;21(9):e14567. PMID: 31573916. doi:10.2196/14567
97. Prodan A, Deimel L, Ahlqvist J, et al. Success factors for scaling up the adoption of digital therapeutics towards the realization of P5 medicine. Front Med Lausanne. 2022;9:854665. PMID: 35492346; PMCID: PMC9039393. doi:10.3389/fmed.2022.854665
98. Carrera A, Zoccarato F, Mazzeo M, et al. What drives patients’ acceptance of Digital Therapeutics? Establishing a new framework to measure the interplay between rational and institutional factors. BMC Health Serv Res. 2023;23(1):145. PMID: 36765410; PMCID: PMC9921481. doi:10.1186/s12913-023-09090-7
99. Rodler S, Kowalewski K-F, Scheibert H, et al.; Young Academic Urologists Urotechnology Group of the European Association of Urology. Digital Therapeutics in Urology: an Innovative Approach to Patient Care and Management. European Urology Open science. 2023;55:23–27. PMID: 37593208; PMCID: PMC10432164. doi:10.1016/j.euros.2023.07.003
100. Chevance A, Fortel A, Jouannin A, et al. Acceptability of and willingness to take digital pills by patients, the public, and health care professionals: qualitative content analysis of a large online survey. J Med Internet Res. 2022;24(2):e25597. PMID: 35179509; PMCID: PMC8900921. doi:10.2196/25597
101. Staff S. A nurse’s perspective: dTx is a win-win for both the patient and the healthcare system. Available at: https://www.sidekickhealth.com/news/es-a-nurses-perspective-why-dtx-is-a-win-win-for-both-The-patient-The-healthcare-system.
102. Kanagasabapathy B Digital Therapeutics: enterprise Opportunities in Virtual Healthcare. White paper. 2020. Available at: https://www.tcs.com/content/dam/global-tcs/en/pdfs/insights/whitepapers/healthcare-digital-therapeutics0.pdf#:~:text=Key%20drivers%20of%20adoption%20Changing%20medical%20protocols%2C%20alongside,reach%20USD%206.9%20billion%20for%20the%20period%202020-2025.
103. Abbadessa G, Brigo F, Clerico M, et al. Digital therapeutics in neurology. J Neurol. 2022;269(3):1209–1224. PMID: 34018047; PMCID: PMC8136262. doi:10.1007/s00415-021-10608-4
104. Gold SM, Köhler-Forsberg O, Moss-Morris R, et al. Comorbid depression in medical diseases. Nat Rev Dis Primers. 2020;6(1):69. PMID: 32820163. doi:10.1038/s41572-020-0200-2
105. Goërtz YMJ, Braamse AMJ, Spruit MA, et al. Fatigue in patients with chronic disease: results from the population-based Lifelines Cohort Study. Sci Rep. 2021;11(1):20977. PMID: 34697347; PMCID: PMC8546086. doi:10.1038/s41598-021-00337-z
106. Carl JR, Jones DJ, Lindhiem OJ, et al. Regulating digital therapeutics for mental health: opportunities, challenges, and the essential role of psychologists. Br J Clin Psychol. 2022;61(Suppl S1):130–135. PMID: 33650131. doi:10.1111/bjc.12286
107. Glass JE, Matson TE, Lim C, et al. Approaches for implementing app-based digital treatments for drug use disorders into primary care: a qualitative, user-centered design study of patient perspectives. J Med Internet Res. 2021;23(7):e25866. PMID: 34255666; PMCID: PMC8293157. doi:10.2196/25866
108. Tye-Murray N, Spehar B, Mauze E, Cardinal C. Hearing health care digital therapeutics: patient satisfaction evidence. American Journal of Audiology. 2022;31(3S):905–913. PMID: 36037482; PMCID: PMC9886161. doi:10.1044/2022_AJA-21-00236
109. Somers C, Grieve E, Lennon M, Bouamrane M, Mair FS, McIntosh E. Valuing mobile health: an open-ended contingent valuation survey of a national digital health program. JMIR mHealth uHealth. 2019;7(1):e3. doi:10.2196/mhealth.9990
110. Lupiáñez-Villanueva F, Folkvord F, Vanden Abeele M. Influence of the business revenue, recommendation, and provider models on mobile health app adoption: three-country experimental vignette study. JMIR mHealth uHealth. 2020;8(6):e17272. doi:10.2196/17272
111. Roettl J, Bidmon S, Terlutter R. What predicts patients’ willingness to undergo online treatment and pay for online treatment? Results from a web-based survey to investigate the changing patient-physician relationship. J Med Internet Res. 2016;18(2):e32. doi:10.2196/jmir.5244
112. Shariful Islam SM, Lechner A, Ferrari U, Seissler J, Holle R, Niessen LW. Mobile phone use and willingness to pay for SMS for diabetes in Bangladesh. J. Journal of Public Health. 2016;38(1):163–169. doi:10.1093/pubmed/fdv009
113. Callan A, O’Shea E. Willingness to pay for telecare programmes to support independent living: results from a contingent valuation study. Soc Sci Med. 2015;124:94–102.
114. Lee J, Oh Y, Kim M, Cho B, Shin J. Willingness to Use and Pay for Digital Health Care Services According to 4 Scenarios: results from a National Survey. JMIR mHealth and uHealth. 2023;11:e40834. PMID: 36989025; PMCID: PMC10131682. doi:10.2196/40834
115. European Commission. Regulation on health technology assessment. Available at: https://health.ec.europa.eu/health-technology-assessment/regulation-health-technology-assessment_en.
116. Martinez-Martin N Navigating the Ethical Landscape of Digital Therapeutics. August 9, 2021. Available at: https://www.psychiatrictimes.com/view/navigating-The-ethical-landscape-of-digital-therapeutics.
117. Honeyman M, Maguire D, Evans H, Davies A Digital technology and health inequalities: a scoping review. (2020). Cardiff: Public Health Wales NHS Trust. Available at: https://phw.nhs.wales/publications/publications1/digital-technology-and-health-inequalities-a-scoping-review/.
118. Desteghe L, Kluts K, Vijgen J, et al. The health buddies app as a novel tool to improve adherence and knowledge in atrial fibrillation patients: a pilot study. JMIR mHealth and uHealth. 2017;5(7):e98. PMID: 28724512; PMCID: PMC5541241. doi:10.2196/mhealth.7420
119. De Santis KK, Jahnel T, Sina E, Wienert J, Zeeb H. Digitization and health in Germany: cross-sectional nationwide survey. JMIR Public Health Surveill. 2021;7(11):e32951. PMID: 34813493; PMCID: PMC8612128. doi:10.2196/32951
120. Twomey C, O’Reilly G, Bültmann O, Meyer B. Effectiveness of a tailored, integrative Internet intervention (deprexis) for depression: updated meta-analysis. PLoS One. 2020;15(1):e0228100. PMID: 31999743; PMCID: PMC6992171. doi:10.1371/journal.pone.0228100
121. Amiot O, Clair AH, Courtet P, et al. Deprexis Acceptability study in REal life (DARE): study design. Eur Psychiatry. 2023;66(Suppl 1):S859. PMCID: PMC10479148. doi:10.1192/j.eurpsy.2023.1820
122. Amiot O, Sauvaget A, Alamome I, et al. Prospective acceptability of digital therapy for major depressive disorder in France: multicentric real-life study. JMIR Form Res. 2024. PMID: 38568139. doi:10.2196/53204
123. Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. 2002;32:509–515.
124. Posselt J, Baumann E, Dierks ML. A qualitative interview study of patients’ attitudes towards and intention to use digital interventions for depressive disorders on prescription. Front Digit Health. 2024;6:1275569. PMID: 38375490; PMCID: PMC10875127. doi:10.3389/fdgth.2024.1275569
125. Martinez-Martin N, Dasgupta I, Carter A, et al. Ethics of Digital Mental Health During COVID-19: crisis and Opportunities. JMIR Ment Health. 2020;7(12):e23776. PMID: 33156811; PMCID: PMC7758081. doi:10.2196/23776
126. Bauer M, Glenn T, Monteith S, Bauer R, Whybrow PC, Geddes J. Ethical perspectives on recommending digital technology for patients with mental illness. Int J Bipolar Disord. 2017;5(1):6. PMID: 28155206; PMCID: PMC5293713. doi:10.1186/s40345-017-0073-9
127. Torous J, Roberts LW. The ethical use of mobile health technology in clinical psychiatry. J Nerv Ment Dis. 2017;205(1):4–8. PMID: 28005647. doi:10.1097/NMD.0000000000000596
128. Wall C, Hetherington V, Godfrey A. Beyond the clinic: the rise of wearables and smartphones in decentralising healthcare. NPJ Digit Med. 2023;6(1):219. PMID: 38007554; PMCID: PMC10676376. doi:10.1038/s41746-023-00971-z
129. Çıtak E AI has many obstacles in its way. The challenges in artificial intelligence serve as a vital catalyst in shaping today’s technological landscape. 6, July 2023. Available at: https://dataconomy.com/2023/07/06/challenges-in-artificial-intelligence/.
130. Petersson L, Larsson I, Nygren JM, et al. Challenges to implementing artificial intelligence in healthcare: a qualitative interview study with healthcare leaders in Sweden. BMC Health Serv Res. 2022;22(1):850. PMID: 35778736; PMCID: PMC9250210. doi:10.1186/s12913-022-08215-8
131. Morita PP, Sahu KS, Oetomo A. Health monitoring using smart home technologies: scoping review. JMIR mHealth and uHealth. 2023;11:e37347. PMID: 37052984; PMCID: PMC10141305. doi:10.2196/37347
132. Williams MG, Stott R, Bromwich N, Oblak SK, Espie CA, Rose JB. Determinants of and barriers to adoption of digital therapeutics for mental health at scale in the NHS. BMJ Innov. 2020;6:92–98.
133. IBM. What is interoperability in healthcare? Available at: https://www.ibm.com/topics/interoperability-in-healthcare.
134. Mandl KD, Gottlieb D, Mandel JC. Integration of AI in healthcare requires an interoperable digital data ecosystem. Nat Med. 2024;30(3):631–634. PMID: 38291298. doi:10.1038/s41591-023-02783-w
135. Hodapp D, Hanelt A. Interoperability in the era of digital innovation: an information systems research agenda. J Inform Technol. 2022;37(4):407–427. doi:10.1177/02683962211064304
136. Lehne M, Sass J, Essenwanger A, Schepers J, Thun S. Why digital medicine depends on interoperability. NPJ Digit Med. 2019;2:79. PMID: 31453374; PMCID: PMC6702215. doi:10.1038/s41746-019-0158-1
137. Shull JG. Digital health and the state of interoperable electronic health records. JMIR Med Inform. 2019;7(4):e12712. PMID: 31682583; PMCID: PMC6913749. doi:10.2196/12712
138. Whitelaw S, Pellegrini DM, Mamas MA, Cowie M, Van Spall HGC. Barriers and facilitators of the uptake of digital health technology in cardiovascular care: a systematic scoping review. Eur Heart J Digit Health. 2021;2(1):62–74. PMID: 34048508; PMCID: PMC8139413. doi:10.1093/ehjdh/ztab005
139. Kyratsis Y, Scarbrough H, Begley A, Denis JL. Editorial: digital health adoption: looking beyond the role of technology. Front Digit Health. 2022;4:989003. PMID: 36419872; PMCID: PMC9677232. doi:10.3389/fdgth.2022.989003
140. Martschenko D, Martinez-Martin N. What about ethics in design bioethics? Am J Bioeth. 2021;21(6):61–63. PMID: 34036888; PMCID: PMC8281611. doi:10.1080/15265161.2021.1915415
141. van Kessel R, Hrzic R, O’Nuallain E, et al. Digital health paradox: international policy perspectives to address increased health inequalities for people living with disabilities. J Med Internet Res. 2022;24(2):e33819. PMID: 35191848; PMCID: PMC8905475. doi:10.2196/33819
142. Roberts MJ, Wilson WJ, Recugnat M, Bardy F. Barriers to adoption of digital therapeutics (DTx) into audiology clinical practice: acknowledging the challenges, adapting to the future. Semin Hear. 2023;44(3):319–327. PMID: 37484989; PMCID: PMC10361790. doi:10.1055/s-0043-1769623
143. Sterling WA, Sobolev M, Van Meter A, et al. Digital Technology in Psychiatry: survey Study of Clinicians. JMIR Form Res. 2022;6(11):e33676. PMID: 36355414; PMCID: PMC9693695. doi:10.2196/33676
144. Mogk JM, Matson TE, Caldeiro RM, et al. Implementation and workflow strategies for integrating digital therapeutics for alcohol use disorders into primary care: a qualitative study. Addict Sci Clin Pract. 2023;18(1):27. PMID: 37158931; PMCID: PMC10169300. doi:10.1186/s13722-023-00387-w
145. Ferguson C, Hickman L, Wright R, Davidson PM, Jackson D. Preparing nurses to be prescribers of digital therapeutics. Contemp Nurse. 2018;54(4–5):345–349. PMID: 29940811. doi:10.1080/10376178.2018.1486943
146. Cripps M, Scarbrough H. Making digital health “solutions” sustainable in healthcare systems: a practitioner perspective. Front Digit Health. 2022;4:727421. PMID: 35434699; PMCID: PMC9008401. doi:10.3389/fdgth.2022.727421
147. Kumar A, Ross JS, Patel NA, Rathi V, Redberg RF, Dhruva SS. Studies of prescription digital therapeutics often lack rigor and inclusivity. Health Aff. 2023;42(11):1559–1567. PMID: 37931187. doi:10.1377/hlthaff.2023.00384
148. Adu-Brimpong J, Pugh J, Darko DA, Shieh L. Examining diversity in digital therapeutics clinical trials: descriptive analysis. J Med Internet Res. 2023;25:e37447. PMID: 37531157; PMCID: PMC10433021. doi:10.2196/37447
149. Abraham J, Ambrose M, Aungst T, et al. AMCP partnership forum: digital therapeutics-what are they and where do they fit in pharmacy and medical benefits? J Manag Care Spec Pharm. 2020;26(5):674–681. PMID: 32175784; PMCID: PMC10391118. doi:10.18553/jmcp.2020.19418
150. Bullard J Evaluating The Economic Impact Of Digital Therapeutics. 28, March 2023. Available at: https://healthcare.rti.org/insights/digital-therapeutics-economic-impact.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.