")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Advanced Therapies in Elderly Patients With Inflammatory Bowel Disease: A Comparative Retrospective Cohort Study in Taiwan
Authors Lin SH, Chiu HY, Kuo CJ, Chen CM, Su MY, Wu RC , Chiu CT, Chang CW, Chung CS, Pan YB , Le PH
Received 19 January 2025
Accepted for publication 13 April 2025
Published 25 April 2025 Volume 2025:21 Pages 533—542
DOI https://doi.org/10.2147/TCRM.S518405
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor De Yun Wang
Shih-Hua Lin,1– 3 Horng-Yih Chiu,2 Chia-Jung Kuo,2– 6 Chien-Ming Chen,7 Ming-Yao Su,1– 3 Ren-Chin Wu,8 Cheng-Tang Chiu,2– 6 Chen-Wang Chang,3,9 Chen-Shuan Chung,3,10 Yu-Bin Pan,11 Puo-Hsien Le2– 6
1Division of Gastroenterology and Hepatology, Department of Internal Medicine, New Taipei Municipal Tucheng Hospital, Tucheng, New Taipei City, Taiwan; 2School of Medicine, Chang Gung University, Taoyuan City, Taiwan; 3Taiwan Association for the Study of Intestinal Diseases (TASID), Taoyuan City, Taiwan; 4Chang Gung Inflammatory Bowel Disease Center, Linkou, Taoyuan, Taiwan; 5Chang Gung Microbiota Therapy Center, Linkou, Taoyuan, Taiwan; 6Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 7Department of Medical Imaging and Interventions, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 8Department of Anatomic Pathology, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan; 9Department of Gastroenterology and Hepatology, Mackay Memorial Hospital, Taipei, Taiwan; 10Division of Gastroenterology and Hepatology, Department of Internal Medicine, Far Eastern Memorial Hospital, New Taipei City, Taiwan; 11Biostatistical Section, Clinical Trial Center, Chang Gung Memorial Hospital, Linkou, Taoyuan, Taiwan
Correspondence: Puo-Hsien Le, Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital Linkou Branch, 5, Fu-Hsin Street, Guei-Shan District, Taoyuan City, 33305, Taiwan, Tel +886-3-3281200 ext 8101, Fax +886-3-3272236, Email [email protected]
Purpose: Inflammatory Bowel Disease (IBD) predominantly affects younger individuals, but emerging data indicates a shift toward older populations. Elderly-onset IBD (diagnosed at 60 years or older) differs from younger-onset IBD, presenting with atypical symptoms and higher risks of infections and malignancies. However, drug persistence is underexplored in the elderly IBD group, warranting further investigation to optimize treatment strategies for this demographic.
Patients and Methods: This retrospective cohort study included IBD patients receiving advanced therapies at the Chang Gung IBD Center from October 2017 to September 2023. Patients were stratified into two groups: elderly-onset (≥ 60 years) and control (< 60 years). We compared one-year persistence of advanced therapies, opportunistic infections, IBD-related admissions, complications, surgeries, and acute flare-ups between the groups. Specifically, we analyzed the one-year persistence of various advanced therapies within the elderly-onset cohort.
Results: The study included 511 IBD patients, 107 of whom were elderly-onset. Elderly-onset patients had a higher body mass index, a higher proportion of ulcerative colitis, fewer smokers, and lower levels of white blood cells, hemoglobin, and albumin. Differences were noted in Montreal classifications and a higher use of Vedolizumab. Clinical outcomes, including steroid-free remission rates, one-year therapy persistence, infections, complications, surgeries, and flare-ups, were comparable between groups. In Crohn’s disease (CD), Infliximab and Ustekinumab exhibited higher one-year persistence. Predictors of one-year therapy persistence included Montreal L1 (OR: 6.722; 95% CI: 1.296– 34.852; P=0.023), Ustekinumab use (OR: 5.672; 95% CI: 1.138– 28.267; P=0.034), and hemoglobin level (OR: 1.612; 95% CI: 1.210– 2.147; P=0.001) with an optimal cutoff of 11.65 g/dL.
Conclusion: Elderly-onset IBD patients display unique clinical characteristics and therapy persistence, particularly in CD, highlighting the necessity for customized therapeutic strategies.
Keywords: elderly-onset inflammatory bowel disease, advanced therapies, drug persistence, clinical outcomes
Introduction
Recent epidemiological studies have highlighted the evolving global burden of inflammatory bowel diseases (IBD), including Crohn’s disease (CD) and ulcerative colitis (UC). While IBD was historically considered more prevalent in Western countries, increasing evidence suggests a rising incidence in Asian nations.1,2 This shift aligns with the four epidemiological stages of IBD evolution, reflecting changing environmental and lifestyle factors.2 Moreover, recent findings indicate that IBD in Asian populations may exhibit distinct demographic and phenotypic characteristics compared to Western cohorts.3 Additionally, the increasing diagnosis of IBD in elderly populations underscores its expanding global impact.4 As populations age, the prevalence of elderly IBD patients has surged rapidly.2,4 With aging populations, the prevalence of elderly IBD patients has increased, with approximately 25–35% now aged 60 or older.2,4–7 IBD diagnosed at this age is categorized as elderly-onset IBD.6 Notably, 10–20% of newly diagnosed IBD cases occur in this demographic, and these figures are anticipated to rise with the ongoing aging of societies.6–12 In recent decades, advanced therapies, including biologic agents and small molecule therapies, have revolutionized the treatment landscape for IBD and are now integral to managing IBD.13 The effectiveness and persistence of these advanced therapies are crucial, given the chronic nature of IBD which necessitates long-term management to alleviate symptoms and prevent disease exacerbation.14,15 However, studies focusing on drug persistence in the elderly, remain scarce. Elevated discontinuation rates of anti-TNF-α therapies have been documented in the elderly population, primarily due to lower clinical responses and increased infection-related complications, which are common reasons for therapy cessation.16–21 Additionally, older age has been identified as an independent factor influencing drug discontinuation.16,17,22 Despite these challenges, few studies have specifically investigated drug persistence and predictive factors for persistence of other advanced therapies in the elderly-onset population.
Our study aims to compare the 1-year persistence of advanced therapies between elderly-onset and control groups in both CD and UC. Additionally, we seek to identify independent predictive factors for 1-year drug persistence specifically within the elderly-onset group.
Materials and Methods
Study Population and Endpoints
This retrospective cohort study included all IBD patients who received advanced therapies and regularly followed up in the Chang Gung IBD center between October 2017 and September 2023. After enrollment, all patients were prospectively followed until either drug discontinuation or January 2024. Patients who did not receive advanced therapies or were pregnant were excluded from the study. The study population was divided into two groups: the control group (patients younger than 60 years) and the elderly group (patients aged 60 years or older), in accordance with the European Crohn’s and Colitis Organization (ECCO) Topical Review.6 Due to the national health insurance regulations, which limit the use of advanced therapies to one year, the primary objective of this study was to compare the one-year drug persistence between the control and elderly groups. Additionally, we sought to identify baseline predictors of one-year drug persistence within the elderly subgroup.
Data Collection and Definition
Patient data were collected from medical records, including the date of diagnosis, age, gender, body mass index (BMI), and disease location/extent in both CD and UC. We also recorded laboratory results at the start of biologic therapy, prior biologic agent use (adalimumab, golimumab, infliximab, vedolizumab, ustekinumab, tofacitinib), or biologic-naïve status, as well as current biologic therapy (adalimumab, infliximab, vedolizumab, ustekinumab, tofacitinib), along with the dates of the initial and final doses. Concomitant use of 5-ASA, corticosteroids, or thiopurines was noted. Corticosteroid-free remission was defined as corticosteroid discontinuation for at least 12 weeks prior to the 52nd week of therapy.23 Additional data collected included dose escalation history, drug administration intervals, IBD-related hospital admissions, opportunistic infections, IBD complications (eg, strictures, perforations, abscesses, fistulas), IBD-related surgeries, and the number of acute flare-ups. Opportunistic infections were defined to include Cytomegalovirus (CMV), Clostridioides difficile (C. difficile), Clostridium innocuum (C. innocuum), and Herpes Simplex virus (HSV) infections.24 CMV infection was identified by the presence of typical viral inclusion bodies on colonic mucosal biopsy.24,25 C. difficile infection was diagnosed via positive C. difficile toxin gene screening.24 C. innocuum infection was identified by stool culture, and HSV infection was defined by a positive serum IgM or DNA test.
Statistical Analysis
Continuous variables were presented as mean ± standard deviation (SD), depending on their distribution, and compared using the Independent Student’s t-test for normally distributed data or the Mann–Whitney U-test for non-normally distributed data. Categorical variables were presented as frequencies and percentages, with comparisons made using the Chi-square test. Fisher’s exact test was applied when more than 20% of the expected frequencies in the statistical cells were less than five. Drug persistence was assessed using Kaplan–Meier analysis and compared with the Log rank test, with a log-rank p-value < 0.05 considered statistically significant. Univariate and multivariate logistic regression analyses were employed to identify baseline predictors of drug persistence through the 52nd week in the overall cohort, as well as in the elderly subgroup. Variables with a p-value ≤ 0.05 in univariate analysis were included in the multivariate analyses. Odds ratios (OR) were calculated with 95% confidence intervals (CI). Missing data were addressed using appropriate statistical methods based on available data analysis techniques. All statistical analyses were performed using IBM SPSS Statistics 26 (SPSS Inc., Chicago, IL, USA).
Result
Patient Characteristics and Clinical Outcomes
This study included 511 patients with IBD, of whom 107 were classified as elderly-onset, while the remaining patients formed the control group (Table 1). The elderly-onset group had a higher BMI, fewer cases of CD, fewer smokers, and lower levels of white blood cells, hemoglobin, and albumin. Additionally, the elderly-onset group showed fewer cases of ileocolonic involvement and strictures in CD, but a higher incidence of UC with proctitis and extensive colitis. This group also had a higher proportion of patients using vedolizumab. Despite these differences, there were no significant disparities between the two groups in terms of steroid-free remission at 52 weeks, 1-year drug persistence, opportunistic infections, IBD-related complications, surgeries, or acute flare-ups.
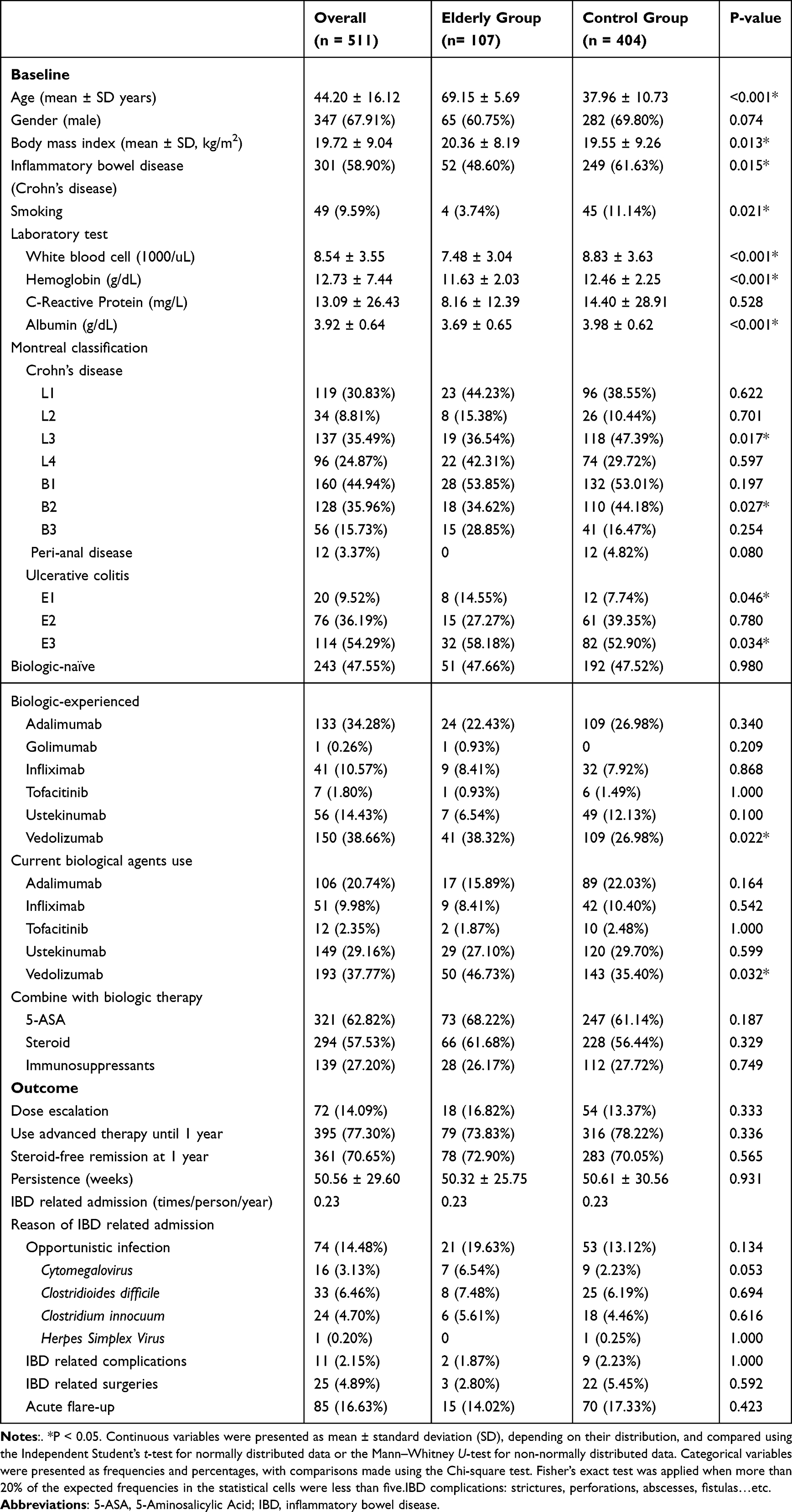 |
Table 1 Baseline Characteristics and Clinical Outcomes Between Elderly and Control Cohorts |
The Persistence of Advanced Therapies
We first compared the 1-year drug persistence of advanced therapies between the elderly-onset and control groups for both CD and UC (Figure 1). Among the 301 CD patients, 52 were in the elderly-onset group, while the remaining 249 were in the control group. A total of 245 CD patients (81.34%) used advanced therapies for at least one year, including 42 from the elderly-onset group (42/52, 80.77%) and 203 from the control group (203/249, 81.53%). Kaplan–Meier analysis showed no significant difference in 1-year drug persistence between the elderly-onset and control groups for CD (Log-rank P = 0.862, Figure 1A). In the UC cohort, 150 patients (71.43%) used advanced therapies for at least one year, including 37 patients from the elderly-onset group (37/55, 67.27%) and 113 from the control group (113/155, 72.90%). Kaplan–Meier analysis again showed no significant difference in 1-year drug persistence between the two groups for UC (Log-rank P = 0.714, Figure 1B).
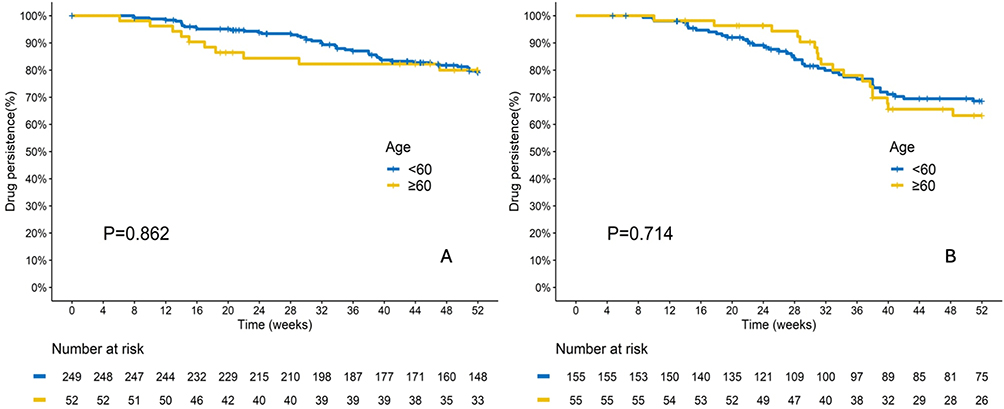 |
Figure 1 Kaplan-Meier curves comparing 1-year drug persistence between elderly-onset (≥60 years) and younger (<60 years) patients with Crohn’s disease (CD, (A) and ulcerative colitis (UC, (B) show no significant differences between age groups (P = 0.862 for CD, P = 0.714 for UC). |
Next, we assessed drug persistence for each advanced therapy within the elderly-onset group (Figure 2). In the CD subgroup, 42 patients receiving advanced therapies for at least one year (42/52, 80.77%). Among the 7 patients treated with adalimumab, 5 continued therapy for at least one year (5/7, 71.43%). All 6 patients treated with infliximab continued therapy for at least one year (6/6, 100%). Among the 20 patients treated with ustekinumab, 19 persisted for at least one year (19/20, 95.00%). Among the 19 patients treated with vedolizumab, 12 maintained therapy for at least one year (12/19, 63.16%). Kaplan–Meier analysis revealed a significant difference in drug persistence among the different therapies for CD (Log-rank P = 0.036, Figure 2A). In the UC subgroup, 37 patients persisted with advanced therapies for at least one year (37/55, 67.27%). Of the 10 patients treated with adalimumab, only 4 persisted for one year (4/10, 40.00%). Among the 3 patients who received infliximab,2 continued treatment for at least one year (2/3, 66.67%). Two patients were treated with tofacitinib, with one persisting for at least one year (1/2, 50.00%). Of the 9 patients treated with ustekinumab, and 8 patients used it for at least one year (8/9, 88.89%). Among the 31 patients treated with vedolizumab, 22 persisted for one year (22/31, 70.97%). However, Kaplan–Meier analysis showed no significant difference in drug persistence among the different therapies for UC (Log-rank P = 0.244, Figure 2B).
 |
Figure 2 Kaplan-Meier curves depicting 1-year drug persistence of advanced therapies in elderly-onset patients with Crohn’s disease (CD, (A) and ulcerative colitis (UC, (B) demonstrate a significant difference among biologic agents in CD (P = 0.036), while no significant difference is observed in UC (P = 0.244). |
Predictive Factors for the Persistence of Advanced Therapies in the Elderly-Onset Group
We conducted logistic regression to identify baseline characteristics associated with drug persistence in the elderly-onset group (Table 2). Three independent factors significantly influenced drug persistence: Montreal classification L1 (OR: 6.722; 95% CI: 1.296–34.852; P=0.023), ustekinumab use (OR: 5.672; 95% CI: 1.138–28.267; P=0.034), and hemoglobin levels (OR: 1.612; 95% CI: 1.210–2.147; P=0.001). The optimal cutoff value for hemoglobin was 11.65 g/dL (area under the ROC curve: 0.714, 95% CI: 0.610–0.818).
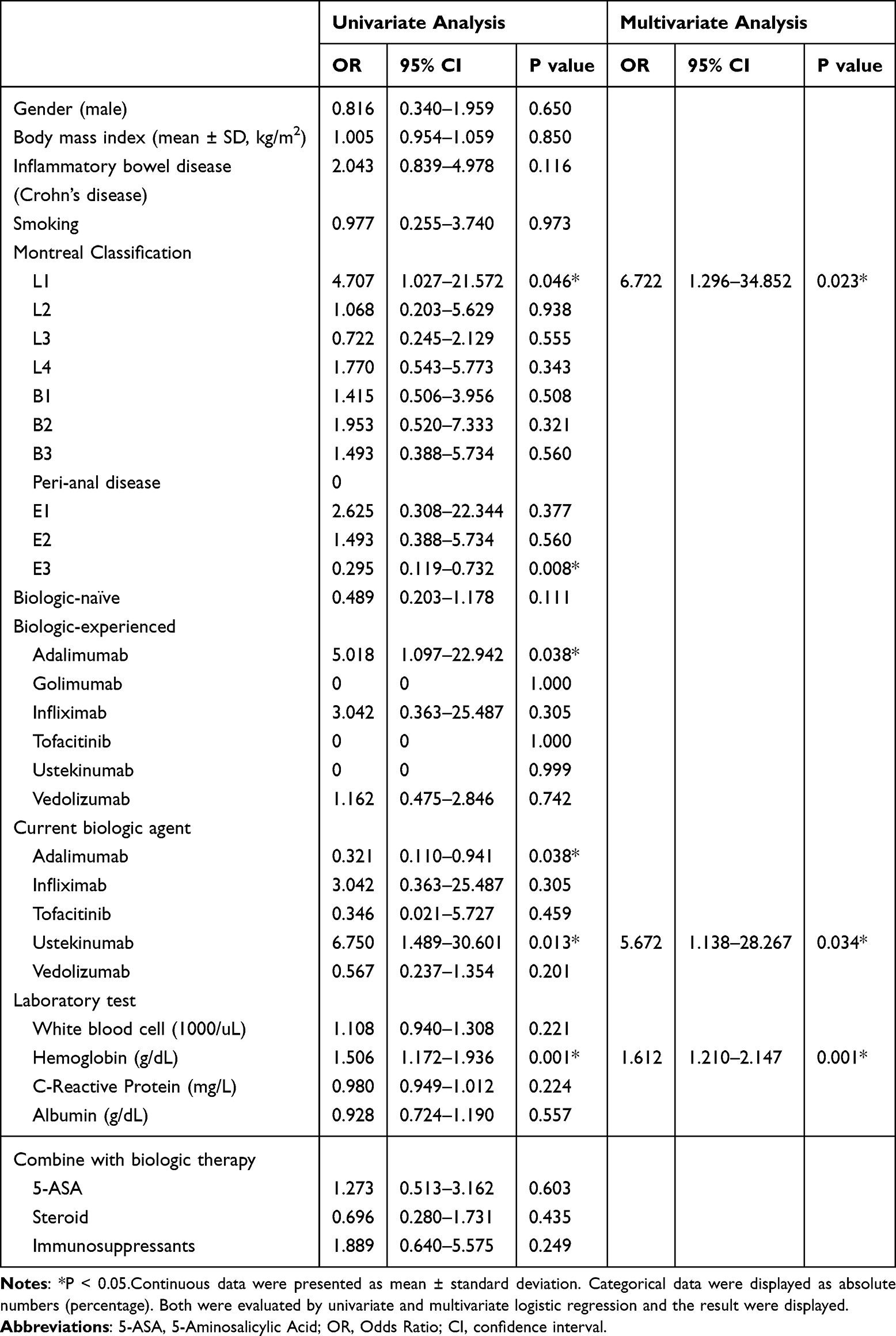 |
Table 2 Logistic Regression Analysis of 1-year Persistence in Elderly-Onset IBD Patients |
Discussion
In our study, approximately 20.94% of the IBD population had elderly-onset disease. Consistent with previous research,6,7,9,12,26–28 elderly-onset UC tended to be milder. Ileal involvement in CD (44.23%) and extensive colitis in UC (58.18%) were common findings in our elderly population. However, the extent of disease in our study differs somewhat from previous literature. In recent studies, colonic involvement in CD and left-sided colitis in UC were more common in Western populations,4,6,7,26,27,29,30 whereas ileal involvement in CD and proctitis in UC were predominant in Eastern populations.7,12,29,31 Additionally, inflammatory phenotypes in elderly-onset CD were more frequent in the West, while stricturing phenotypes were more typical in the East,7,12,29,30 Our study found a predominance of the inflammatory phenotype, suggesting a potential regional difference in disease presentation between Eastern and Western populations.
Vedolizumab, a monoclonal antibody targeting α4β7 integrin, has been shown to provide gut-selective anti-inflammatory activity.32,33 Importantly, adverse events related to vedolizumab showed no significant difference between younger and elderly patients with CD and UC,34,35 supporting its increased use in elderly-onset patients in our study.
Regarding drug persistence, our findings indicated no significant difference in 1-year drug persistence between elderly-onset and control groups in both CD and UC. This suggests that advanced therapies remain effective in elderly populations. However, ustekinumab demonstrated higher 1-year drug persistence compared to other biologic agents in the elderly-onset CD group, though no significant differences were observed in the UC cohort. Similar findings regarding ustekinumab’s favorable persistence have been reported in other studies,36,37 possibly reflecting the different efficacy profiles of therapies for managing CD and UC in elderly patients.
Older age has been identified as a predictive factor for drug persistence.17,21 In our logistic regression analysis, tㄅhree independent factors significantly influenced drug persistence in the elderly-onset group: Montreal L1, indicating isolated ileal involvement in CD, may represent a less severe disease course, which could contribute to better treatment adherence. Ustekinumab’s safety and efficacy profile likely underpin its higher persistence in this population.31,36–41 Additionally, higher hemoglobin levels were associated with better drug persistence, suggesting that patients with less severe anemia may have fewer disease complications and better overall health, allowing them to maintain treatment.42–45
Managing inflammatory bowel disease (IBD) in elderly patients requires personalized strategies due to comorbidities and increased treatment risks. Recent advancements in drug delivery systems, such as ROS-responsive nanoparticles, have enhanced therapeutic efficacy while minimizing side effects, offering promising options for improving outcomes in this population.46,47 Advanced therapies, including Infliximab and Ustekinumab, demonstrate comparable outcomes and therapy persistence to younger patients. These findings underscore the importance of identifying key predictors and tailoring treatment approaches to optimize care for elderly-onset IBD patients, ensuring more effective and safer management of their condition.
This study has several limitations. First, it was conducted at a single academic center (Linkou Chang Gung Memorial Hospital), which may introduce referral bias. Second, as a retrospective cohort study, it is subject to biases such as selection and information bias due to the reliance on existing medical records, which may contain incomplete or missing data. Third, there were only 52 elderly patients with Crohn’s disease, which may introduce statistical bias. A larger sample size is required for further analysis and research. Finally, focusing on one-year drug persistence may not fully capture long-term outcomes, as IBD management typically requires long-term treatment. Future studies with longer follow-up periods are needed to better understand the sustainability of therapeutic responses and the potential for adverse events or complications over time.
Conclusion
Elderly-onset IBD presents distinct characteristics, with ileal involvement in CD and extensive colitis in UC, and shows favorable drug persistence with treatments like infliximab and ustekinumab. Montreal L1 classification, ustekinumab use, and hemoglobin levels are key predictors of drug persistence in elderly-onset patients, underscoring the need for tailored treatment approaches in this population. However, the regional generalizability of these findings should be acknowledged, as they are based on a single-center Taiwanese cohort.
Sample Data Availability Statements
The corresponding author would share the data underlying this article upon reasonable request.
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of the Chang Gung Medical Foundation (Approval No. 202400030B0: “Diagnosis, Treatment, and Prognosis of Inflammatory Bowel Disease”). Given the retrospective nature of the study, the IRB waived the requirement for signed informed consent for the use of medical records retrieved from the electronic medical record system.
To ensure participant privacy and data confidentiality, all patient information was anonymized before analysis. No identifiable personal data were disclosed or utilized in this study, and strict measures were implemented to maintain confidentiality in compliance with ethical and regulatory standards.
Acknowledgments
We extend our gratitude to the team members of the Chang Gung IBD Center for their dedicated care of IBD patients and their invaluable support throughout this study.
This abstract of this paper was presented at the 20th congress of ECCO, Conference name “ Sustainability in IBD and beyond” as a poster presentation with interim findings. The poster’s abstract was published in ‘Poster Abstracts’ in Journal of Crohn’s and Colitis: [https://academic.oup.com/ecco-jcc/article/19/Supplement_1/i1380/7967914].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare no competing interests in this work.
References
1. Molodecky NA, Soon IS, Rabi DM, et al. Increasing incidence and prevalence of the inflammatory bowel diseases with time, based on systematic review. Gastroenterology. 2012;142(1):46–54e42. doi:10.1053/j.gastro.2011.10.001
2. Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021;18(1):56–66. doi:10.1038/s41575-020-00360-x
3. Banerjee R, Pal P, Hilmi I, et al. Emerging inflammatory bowel disease demographics, phenotype, and treatment in South Asia, South-East Asia, and Middle East: preliminary findings from the inflammatory bowel disease-emerging nations’ consortium. J Gastroenterol Hepatol. 2022;37(6):1004–1015. doi:10.1111/jgh.15801
4. Jeuring SF, van den Heuvel TR, Zeegers MP, et al. Epidemiology and long-term outcome of inflammatory bowel disease diagnosed at elderly age-an increasing distinct entity? Inflamm. Bowel Dis. 2016;22(6):1425–1434. doi:10.1097/MIB.0000000000000738
5. Nguyen GC, Sheng L, Benchimol EI. Health Care utilization in elderly onset inflammatory bowel disease: a population-based study. Inflamm. Bowel Dis. 2015;21(4):777–782. doi:10.1097/MIB.0000000000000306
6. Sturm A, Maaser C, Mendall M, et al. European crohn’s and colitis organisation topical review on IBD in the elderly. J Crohns Colitis. 2017;11(3):263–273. doi:10.1093/ecco-jcc/jjw188
7. Sousa P, Bertani L, Rodrigues C. Management of inflammatory bowel disease in the elderly: a review. Digestive Liver Dis. 2023;55(8):1001–1009. doi:10.1016/j.dld.2022.12.024
8. Gisbert JP, Chaparro M. Systematic review with meta-analysis: inflammatory bowel disease in the elderly. Aliment Pharmacol Ther. 2014;39(5):459–477. doi:10.1111/apt.12616
9. Mañosa M, Calafat M, de Francisco R, et al. Phenotype and natural history of elderly onset inflammatory bowel disease: a multicentre, case-control study. Aliment Pharmacol Ther. 2018;47(5):605–614. doi:10.1111/apt.14494
10. Å h E, Halfvarson J, Myrelid P, et al. Incidence and treatment of patients diagnosed with inflammatory bowel diseases at 60 Years or Older in Sweden. Gastroenterology. 2018;154(3):518–528.e515. doi:10.1053/j.gastro.2017.10.034
11. Rozich JJ, Dulai PS, Fumery M, Sandborn WJ, Singh S. Progression of elderly onset inflammatory bowel diseases: a systematic review and meta-analysis of population-based cohort studies. Clin Gastroenterol Hepatol. 2020;18(11):2437–2447.e2436. doi:10.1016/j.cgh.2020.02.048
12. Mak JWY, Lok Tung Ho C, Wong K, et al. Epidemiology and natural history of elderly-onset inflammatory bowel disease: results from a Territory-wide Hong Kong IBD Registry. J Crohns Colitis. 2021;15(3):401–408. doi:10.1093/ecco-jcc/jjaa181
13. Zurba Y, Gros B, Shehab M. Exploring the pipeline of novel therapies for inflammatory bowel disease; state of the art review. Biomedicines. 2023;11(3):747. doi:10.3390/biomedicines11030747
14. Wolfe F. The epidemiology of drug treatment failure in rheumatoid arthritis. Bailliere’s clin rheumatol. 1995;9(4):619–632. doi:10.1016/S0950-3579(05)80305-X
15. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
16. Cottone M, Kohn A, Daperno M, et al. Advanced age is an independent risk factor for severe infections and mortality in patients given anti-tumor necrosis factor therapy for inflammatory bowel disease. Clin Gastroenterol Hepatol. 2011;9(1):30–35. doi:10.1016/j.cgh.2010.09.026
17. Desai A, Zator ZA, de Silva P, et al. Older age is associated with higher rate of discontinuation of anti-TNF therapy in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2013;19(2):309–315. doi:10.1002/ibd.23026
18. Lobatón T, Ferrante M, Rutgeerts P, Ballet V, Van Assche G, Vermeire S. Efficacy and safety of anti-TNF therapy in elderly patients with inflammatory bowel disease. Aliment Pharmacol Ther. 2015;42(4):441–451. doi:10.1111/apt.13294
19. LeBlanc JF, Wiseman D, Lakatos PL, Bessissow T. Elderly patients with inflammatory bowel disease: updated review of the therapeutic landscape. World J Gastroenterol. 2019;25(30):4158–4171. doi:10.3748/wjg.v25.i30.4158
20. Adar T, Faleck D, Sasidharan S, et al. Comparative safety and effectiveness of tumor necrosis factor α antagonists and vedolizumab in elderly IBD patients: a multicentre study. Aliment Pharmacol Ther. 2019;49(7):873–879. doi:10.1111/apt.15177
21. Porcari S, Viola A, Orlando A, et al. Persistence on anti-tumour necrosis factor therapy in older patients with inflammatory bowel disease compared with younger patients: data from the sicilian network for inflammatory bowel diseases (SN-IBD). Drugs Aging. 2020;37(5):383–392. doi:10.1007/s40266-020-00744-3
22. Lin WC, Weng MT, Tung CC, et al. Trends and risk factors of mortality analysis in patients with inflammatory bowel disease: a Taiwanese nationwide population-based study. J Transl Med. 2019;17(1):414.
23. Ma C, Hanzel J, Panaccione R, et al. CORE-IBD: a multidisciplinary international consensus initiative to develop a core outcome set for randomized controlled trials in inflammatory bowel disease. Gastroenterology. 2022;163(4):950–964. doi:10.1053/j.gastro.2022.06.068
24. Kucharzik T, Ellul P, Greuter T, et al. ECCO guidelines on the prevention, diagnosis, and management of infections in inflammatory bowel disease. J Crohns Colitis. 2021;15(6):879–913.
25. Kandiel A, Lashner B. Cytomegalovirus colitis complicating inflammatory bowel disease. Am J Gastroenterol. 2006;101(12):2857–2865. doi:10.1111/j.1572-0241.2006.00869.x
26. Lakatos PL, David G, Pandur T, et al. IBD in the elderly population: results from a population-based study in Western Hungary, 1977-2008. J Crohns Colitis. 2011;5(1):5–13. doi:10.1016/j.crohns.2010.08.004
27. Charpentier C, Salleron J, Savoye G, et al. Natural history of elderly-onset inflammatory bowel disease: a population-based cohort study. Gut. 2014;63(3):423–432. doi:10.1136/gutjnl-2012-303864
28. Singh S, Underwood FE, Loftus EV, et al. Sa1769–worldwide incidence of older-onset inflammatory bowel diseases in the 21ST century: a systematic review of population-based studies. Gastroenterology. 2019;156(6):S–394–S–395.
29. Hwang SW, Kim JH, Im JP, et al. Influence of age at diagnosis on the clinical characteristics of Crohn’s disease in Korea: results from the CONNECT study. J Gastroenterol Hepatol. 2017;32(10):1716–1722. doi:10.1111/jgh.13775
30. Hong SJ, Katz S. The elderly IBD patient in the modern era: changing paradigms in risk stratification and therapeutic management. Ther Adv Gastroenterol. 2021;14:17562848211023399. doi:10.1177/17562848211023399
31. Park SH, Jeong SK, Lee JH, et al. Clinical characteristics and long-term prognosis of elderly-onset ulcerative colitis in a population-based Cohort in the Songpa-Kangdong District of Seoul, Korea. Gut Liver. 2021;15(5):742–751. doi:10.5009/gnl20289
32. Baumgart DC, Le Berre C. Newer biologic and small-molecule therapies for inflammatory bowel disease. N Engl J Med. 2021;385(14):1302–1315. doi:10.1056/NEJMra1907607
33. Gubatan J, Keyashian K, Rubin SJS, Wang J, Buckman CA, Sinha S. Anti-integrins for the treatment of inflammatory bowel disease: current evidence and perspectives. Clin Exp Gastroenterol. 2021;14:333–342. doi:10.2147/CEG.S293272
34. Cohen NA, Plevris N, Kopylov U, et al. Vedolizumab is effective and safe in elderly inflammatory bowel disease patients: a binational, multicenter, retrospective cohort study. United European Gastroenterol J. 2020;8(9):1076–1085. doi:10.1177/2050640620951400
35. Pugliese D, Privitera G, Crispino F, et al. Effectiveness and safety of vedolizumab in a matched cohort of elderly and nonelderly patients with inflammatory bowel disease: the IG-IBD LIVE study. Aliment Pharmacol Ther. 2022;56(1):95–109. doi:10.1111/apt.16923
36. Fiske J, Liu E, Limdi JK, et al. Safety and effectiveness of ustekinumab in elderly Crohn’s disease patients. Eur J Gastroenterol Hepatol. 2022;34(11):1132–1139. doi:10.1097/MEG.0000000000002436
37. Casas-Deza D, Lamuela-Calvo LJ, Gomollón F, et al. Effectiveness and safety of ustekinumab in elderly patients with crohn’s disease: real world evidence from the ENEIDA registry. J Crohns Colitis. 2023;17(1):83–91. doi:10.1093/ecco-jcc/jjac108
38. Sands BE, Sandborn WJ, Panaccione R, et al. Ustekinumab as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2019;381(13):1201–1214. doi:10.1056/NEJMoa1900750
39. Sandborn WJ, Rebuck R, Wang Y, et al. Five-year efficacy and safety of ustekinumab treatment in crohn’s disease: the IM-UNITI Trial. Clin Gastroenterol Hepatol. 2022;20(3):578–590.e574. doi:10.1016/j.cgh.2021.02.025
40. D’Amico F, Peyrin-Biroulet L, Danese S. Ustekinumab in crohn’s disease: new data for positioning in treatment algorithm. J Crohns Colitis. 2022;16(Supplement_2):ii30–ii41. doi:10.1093/ecco-jcc/jjac011
41. Abreu MT, Rowbotham DS, Danese S, et al. Efficacy and safety of maintenance ustekinumab for ulcerative colitis through 3 Years: UNIFI long-term extension. J Crohns Colitis. 2022;16(8):1222–1234. doi:10.1093/ecco-jcc/jjac030
42. Koutroubakis IE, Ramos-Rivers C, Regueiro M, et al. Five-year period prevalence and characteristics of anemia in a large us inflammatory bowel disease cohort. J Clin Gastroenterol. 2016;50(8):638–643. doi:10.1097/MCG.0000000000000417
43. Foteinogiannopoulou K, Karmiris K, Axiaris G, et al. The burden and management of anemia in Greek patients with inflammatory bowel disease: a retrospective, multicenter, observational study. BMC Gastroenterol. 2021;21(1):269. doi:10.1186/s12876-021-01826-1
44. Hsiao PY, Weng MT, Chang CH, et al. Anemia in inflammatory bowel disease course is associated with patients’ worse outcome. J Formos Med Assoc Taiwan yi zhi. 2023;122(7):549–556. doi:10.1016/j.jfma.2022.11.004
45. Bergamaschi G, Castiglione F, D’Incà R, et al. Follow-up evaluation and management of anemia in inflammatory bowel disease: a study by the Italian Group for Inflammatory Bowel Diseases (IG-IBD). Digestive Liver Dis. 2024;56(9):1483–1489.
46. Lei P, Yu H, Ma J, et al. Cell membrane nanomaterials composed of phospholipids and glycoproteins for drug delivery in inflammatory bowel disease: a review. Int J Biol Macromol. 2023;249:126000. doi:10.1016/j.ijbiomac.2023.126000
47. Wan X, Zhang C, Lei P, et al. Precision therapeutics for inflammatory bowel disease: advancing ROS-responsive nanoparticles for targeted and multifunctional drug delivery. J Mat Chem B. 2025;13(10):3245–3269. doi:10.1039/D4TB02868F
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.