")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 18
Adverse Events Associated with Apremilast and Deucravacitinib for Psoriasis: A Pharmacovigilance Study Based on the FAERS Database
Authors Xu Y , Liu X , Guo L , Jiang X
Received 23 February 2025
Accepted for publication 12 April 2025
Published 5 May 2025 Volume 2025:18 Pages 1121—1135
DOI https://doi.org/10.2147/CCID.S439643
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yuanyuan Xu,1,2,* Xinjin Liu,1,2,* Linghong Guo,1,2 Xian Jiang1,2
1Department of Dermatology, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China; 2Laboratory of Dermatology, Clinical Institute of Inflammation and Immunology, Frontiers Science Center for Disease-Related Molecular Network, West China Hospital, Sichuan University, Chengdu, 610041, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Linghong Guo, Email [email protected] Xian Jiang, Email [email protected]
Introduction: Apremilast and deucravacitinib are oral small-molecule inhibitors approved for the treatment of psoriasis, each with the potential to fill unmet needs among psoriasis patients. Investigating their adverse event (AE) profiles with post-marketing data is essential for optimizing patient care.
Methods: We analyzed AE reports from the FDA Adverse Event Reporting System (FAERS) database during Q1 2014 to Q4 2023. Disproportionality and Bayesian analyses were utilized to compare safety signals.
Results: A total of 95,524 and 754 AE reports associated with apremilast and deucravacitinib were retrieved, respectively. Apremilast was more prevalent to cause gastrointestinal AEs such as diarrhea and nausea, as well as psoriasis recurrence and nervous system disorders like headache. Deucravacitinib showed stronger associations with cutaneous AEs, including acne, folliculitis, pruritus, rash, and erythema, along with oral conditions. AEs not previously documented on drug labels, such as sinus headache and multiple allergies for apremilast, and acneiform dermatitis and rosacea for deucravacitinib, were identified. Female patients were exposed to a higher risk for skin-related AEs when using deucravacitinib.
Conclusion: Our study offers valuable real-world insights into the safety profiles of apremilast and deucravacitinib. The observed sex differences in adverse events associated with apremilast and deucravacitinib require further investigation in real-world and clinical settings.
Keywords: apremilast, deucravacitinib, pharmacovigilance analysis, safety signals, adverse events, psoriasis
Introduction
Psoriasis is a chronic, immune-mediated, inflammatory cutaneous disease, affecting over 100 million adults and children worldwide.1,2 Plaque psoriasis (PsO), characterized by erythematous scaly patches and plaques, is the most common phenotype of psoriasis.3 Involving the peripheral joints, spine, tendon insertions, and fingers, psoriatic arthritis (PsA) is another major phenotype which occurs in up to 30% of the psoriasis patients.4 PsO and PsA can significantly impair patients’ physical and psychological conditions, which leads to declined health-related quality of life.5,6 Moreover, psoriasis is related to increased risk of comorbidities, such as cardiovascular diseases, metabolic syndromes, and malignancies, resulting in substantial burdens on patients and society.7
Current treatment options for psoriasis, including traditional systemic agents and biologics, offer patients a broad range of choices, while there remain unmet needs due to problems such as high costs, insufficient efficacy and inconvenience caused by injections. Oral small-molecule inhibitors have emerged as a major therapeutic advancement for patients and physicians in treating psoriasis.8 Apremilast is an orally administrated small-molecule inhibitor of phosphodiesterase 4 (PDE4), which modulates the immune system by increasing the intracellular levels of cyclic adenosine monophosphate (cAMP), thereby reducing inflammatory cytokine production.9 Apremilast is approved by the US Food and Drug Administration (FDA) for indications of plaque psoriasis, psoriatic arthritis and oral ulcers of Behcet’s Disease.10 On the other hand, deucravacitinib is a new oral, selective, allosteric tyrosine kinase 2 (TYK2) Inhibitor. TYK2 is a member of the Janus Kinase family that mediates cytokine signaling, including IL-12, IL-23, and type I interferons, which were crucial in psoriasis pathogenesis.11 Deucravacitinib specifically targets the pseudokinase domain of TYK2, potentially enhancing efficacy and safety while limiting its impact on JAK1/2/3.12,13 Deucravacitinib was recently FDA-approved for moderate-to-severe plaque psoriasis and is showing promising potential in clinical trials for psoriatic arthritis.14,15
As with all drug treatments, the use of apremilast and deucravacitinib can carry the risk of adverse reactions.16,17 Deucravacitinib and Apremilast may result in different adverse effects because they target distinct enzymes and modulate different signaling pathways. However, most studies comparing the safety and tolerability of these two drugs for treating psoriasis derived from clinical trials, with limited evidence from real-world data and post-market surveillance.18,19 Uncovering the differences in adverse events (AEs) of both medications in real-world settings can help clinicians make appropriate treatment decisions based on patients’ baseline characteristics.20 The FDA Adverse Event Reporting System (FAERS) is a public database with millions of spontaneous AE and medication error reports. This study aims to characterize and compare the AE profiles of two oral small-molecule agents, apremilast and deucravacitinib, in treating psoriasis in real-world and post-market settings by using the FAERS database.
Methods
Search Strategies and Data Sources
Adverse event reports (AERs) were extracted from the FAERS database using American Standard Code for Information Interchange (ASCII) files. The search terms included both trade names and generic names of apremilast and deucravacitinib, such as “Otezla”, “apremilast”, “CC-10004”, “Sotyktu”, and “deucravacitinib”. The search timeframe spanned from the second quarter of 2014 to the last quarter of 2023, aligning with the market introduction timelines of apremilast and deucravacitinib. Only AERs where these drugs were listed as the primary suspect (PS) for the AEs were included. The indication was limited to “psoriasis”. As the FAERS database is updated quarterly, duplicates from previous reports were removed by retaining only the most recent report for cases with the same case ID in the DEMO table The original data were imported into R software (Version 4.4.1), and the faersR package was utilized for data searching, extraction, and analysis.
Data Extraction and Identification Process
To establish relationships between datasets, the primary ID field was used, and the Medex_UIMA_1.8.3 system was employed to standardize drug names. The dataset included patient demographic and administrative information, such as age, gender, reporting date, and region. For AEs and medication errors, preferred terms (PTs) with at least three counts were selected. The Medical Dictionary for Regulatory Activities (MedDRA) terminology was used to encode, categorize, and localize signals, allowing analysis of the specific system organ classes (SOCs) involved in AE signals.
Data Analysis
Three algorithms were used to quantify the adverse drug event (ADE) signals associated with apremilast and deucravacitinib: the Reporting Odds Ratio (ROR), Proportional Reporting Ratio (PRR), and Bayesian Confidence Propagation Neural Network (BCPNN). While ROR and PRR are based on frequentist statistics, BCPNN applies Bayesian statistics. ROR is useful for adjusting minor biases associated with low-frequency events, PRR offers greater specificity, and BCPNN can integrate multi-source data and perform cross-validation. The use of multiple algorithms enabled a more comprehensive and reliable analysis of AE signals for both drugs. Details of the 2×2 contingency table and formulas for all algorithms are provided in Supplementary Tables 1 and 2.
Results
Descriptive Analysis of Safety Signals for Apremilast and Deucravacitinib
From Q2 2014 to Q4 2023, a total of 12,732,564 AE reports (AER) were retrieved from the FAERS databases after the removal of duplication. Of these, 95,524 reports were associated with apremilast and 754 with deucravacitinib. As shown in Figure 1, the number of AE reports for apremilast increased gradually over time, reaching a peak of 4,852 AERs in a single quarter in 2020. Deucravacitinib, introduced in 2022, exhibited a rapid rise in AE reports, suggesting growing clinical use and awareness.
 |
Figure 1 The number of adverse events reported quarterly after the marketing of apremilast and deucravacitinib. |
The median age of patients reporting AEs was 56 years for apremilast and 55 years for deucravacitinib, indicating a similar age distribution among the affected populations of both drugs. Females accounted for a higher proportion of reports, comprising 63.65% of the apremilast cases and 59.81% of the deucravacitinib cases. Geographically, most of the AERs were from the United States, with 96.75% for apremilast and 96.29% for deucravacitinib. Canada and Japan also contributed to apremilast reports, representing 1.04% and 0.50%, respectively, while 3.71% of deucravacitinib reports came from countries outside of the United States. Serious outcomes were reported in association with both drugs, and hospitalization was the most prevalent one among them (Table 1). While death, disability and other life-threatening conditions were reported, their occurrence was relatively rare.
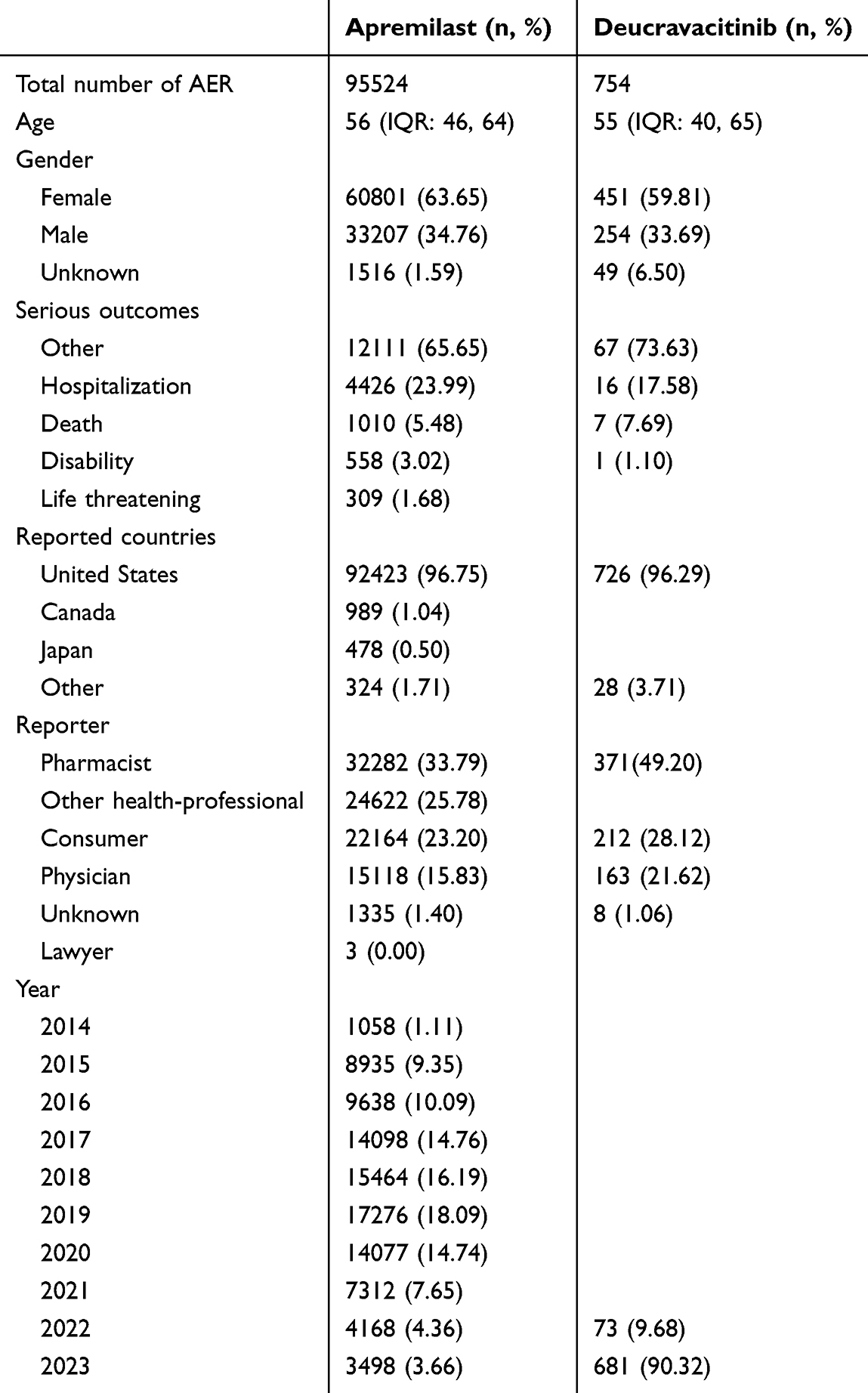 |
Table 1 Characteristics of Reports Associated with Apremilast and Deucravacitinib from Q2 of 2014 to Q4 of 2023 |
AEs that met the signal generation criteria and formulas were categorized by SOCs and ranked by case number. After screening, certain AEs were excluded from the SOCs, such as “injury, poisoning and procedural complications”, “neoplasms benign, malignant and unspecified”, and “pregnancy, puerperium and perinatal conditions”. For apremilast, the recurrence or exacerbation of psoriasis and diarrhea were the most frequently reported AEs, while acne and pruritus were the leading AEs for deucravacitinib. The top 10 AEs for both drugs are listed in Table 2.
 |
Table 2 Top 10 in the Number of Adverse Events Reports of Apremilast and Deucravacitinib |
Disproportionality Analysis of Safety Signals for Apremilast and Deucravacitinib
In this disproportionality analysis, we documented the AEs with over 100 cases for apremilast and over 5 cases for deucravacitinib. In total, 34 AEs related to apremilast and 35 AEs related to deucravacitinib were ranked by the number of case reports in different SOCs (Table 3). Among the AEs associated with apremilast, psoriasis was the most frequently reported with 17,193 cases, alongside signaling a significant disproportionality [ROR 50.12, PRR 45.63, information component(IC) 5.21]. Gastrointestinal disorders were predominant for apremilast, including diarrhea (16,673 cases, ROR 8.75, PRR 8.06, IC 2.96), nausea (14,770 cases, ROR 6.58, PRR 6.14, IC 2.58), and abdominal discomfort (4,319 cases, ROR 7.77, PRR 7.61, IC 2.88). Nervous system disorders were also common, especially headache (11,483 cases, ROR 6.05, PRR 5.75, IC 2.49). These findings were consistent with the label of apremilast, suggesting that the main safety concerns for apremilast were concentrated in the gastrointestinal, nervous systems and disease recurrence or exacerbation. However, we also found several AEs that did not appear in the label of apremilast but showed high safety signals, such as sinus headache (100 cases, ROR 6.75, PRR 6.74, IC 2.71), multiple allergies (125 cases, ROR 4.92, PRR 4.92, IC 2.27), and gallbladder disorder (118 cases, ROR 3.01, PRR 3.00, IC 1.57).
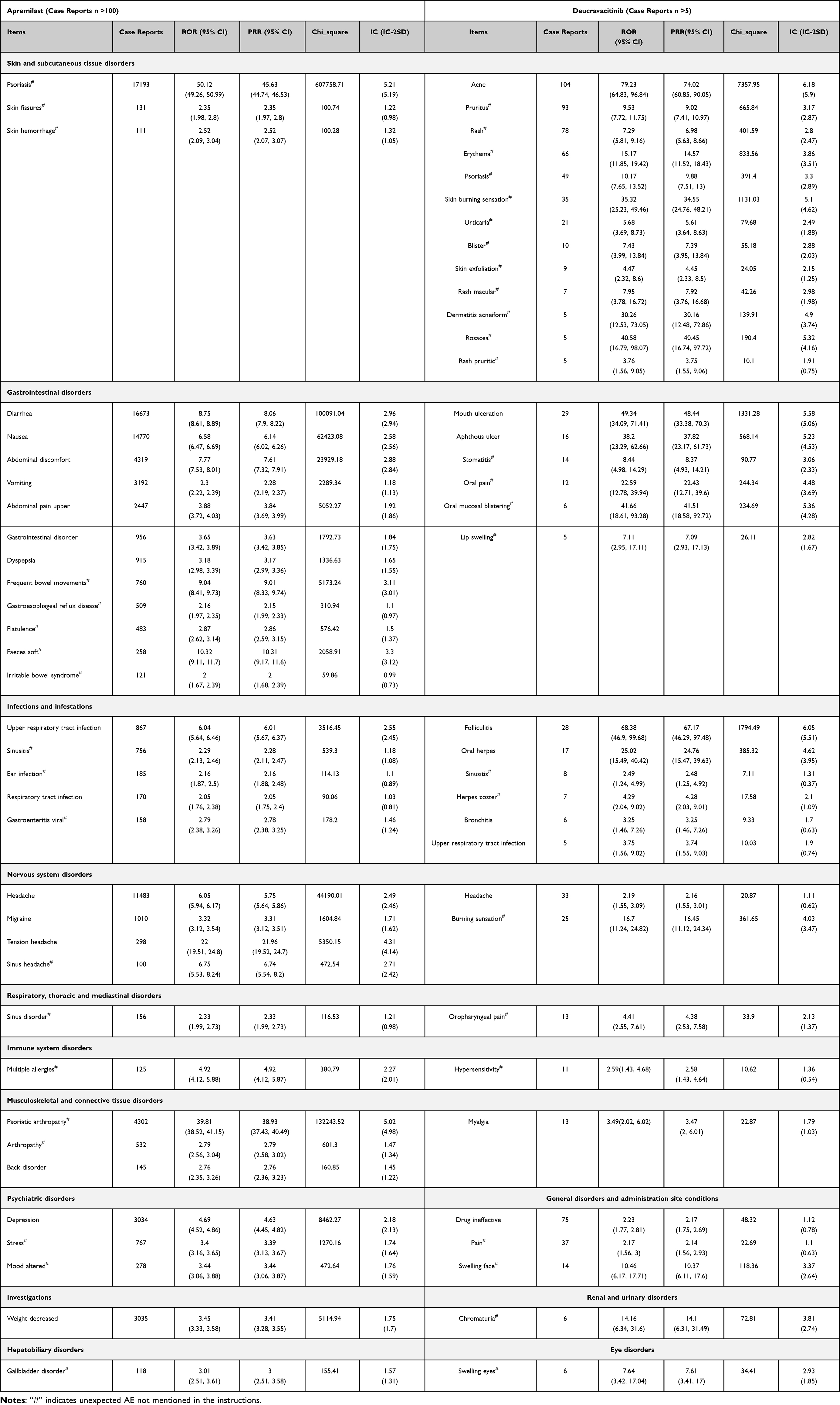 |
Table 3 Comparison of Adverse Event Signals Between Apremilast and Deucravacitinib in Various System Organ Classes |
In contrast, deucravacitinib exhibited higher disproportionality in AEs related to the skin, oral, and infection categories. Our findings highlighted significantly higher signals for cutaneous AEs, including acne (104 cases, ROR 79.23, PRR 74.02, IC 6.18), folliculitis (28 cases, ROR 68.38, PRR 67.17, IC 6.05), skin burning sensation (35 cases, ROR 35.32, PRR 34.55, IC 5.1), acneiform dermatitis (5 cases, ROR 30.26, PRR 30.16, IC 4.9), and rosacea (5 cases, ROR 40.58, PRR 40.45, IC 5.32). Oral conditions, including mouth ulceration (29 cases, ROR 49.34, PRR 48.44, IC 5.58), aphthous ulcer (16 cases, ROR 38.2, PRR 37.82, IC 5.23), oral pain (12 cases, ROR 22.59, PRR 22.43, IC 4.48), oral mucosal blistering (6 cases, ROR 41.66, PRR 41.51, IC 5.36), and oral herpes (17 cases, ROR 25.02, PRR 24.76, IC 4.62), also displayed strong safety signals. Infections related to deucravacitinb, including herpes zoster (7 cases, ROR 4.29, PRR 4.28, IC 2.1), upper respiratory tract infection (URTI) (5 cases, ROR 3.75, PRR 3.74, IC 1.9), and sinusitis (16 cases, ROR 2.49, PRR 2.48, IC 1.31) also occurred, but not as prevalent as the aforementioned conditions. This analysis also revealed additional AEs not listed in the deucravacitinib label, mainly related to skin reactions. Significant signals for acneiform dermatitis, rosacea, burning sensation, and chromaturia (6 cases, ROR 14.16, PRR 14.1, IC 3.81) suggested potential underreported risks.
Temporal Analysis of Safety Signals for Apremilast and Deucravacitinib
To better understand the temporal trends of safety signals for both drugs, time scans were generated for key AEs associated with apremilast and deucravacitinib, focusing on diarrhea, acne, pruritus, nausea, upper respiratory tract infection (URTI) and headache. The safety signals for apremilast, including diarrhea, nausea, and URTI remained stable throughout the observation period, as evidenced by consistent IC values and steady reporting patterns (Figure 2). These stable trends suggested that the risks associated with these AEs are predictable and inherent to apremilast, supporting effective long-term risk management.
 |
Figure 2 The information component (IC) value and its 95% credibility interval (CI) over time for apremilast and deucravacitinib-associated adverse events. (A) the IC value and 95% CI of diarrhoea; (B) the IC value and 95% CI of nausea; (C) the IC value and 95% CI of upper respiratory tract infection; (D) the IC value and 95% CI of headache; (E) the IC value and 95% CI of pruritus; (F) the IC value and 95% CI of acne. |
In contrast, safety signals for deucravacitinib began to emerge after its market entry in 2022. Since then, signals for deucravacitinib-related acne, pruritus, and headache have stabilized, with IC values remaining above zero and confidence intervals gradually narrowing over time. However, Figure 2 indicated fluctuating IC values for diarrhea between 2022 and 2023, as well as a wider confidence interval for URTI, which was based solely on 2023 data. These findings highlighted the need for additional data to further validate the risk associations for diarrhea and URTI with deucravacitinib use.
Comparison of Safety Signals Across System Organ Classes and Sex Differences for Apremilast and Deucravacitinib
The comparison of safety signals across four SOCs revealed distinct AE characteristics for apremilast and deucravacitinib, respectively (Figure 3). In the skin and subcutaneous tissue disorders category, psoriasis and rebound psoriasis emerged as the strongest signals for apremilast, with both high ROR and Chi-square values. This may align with the immunomodulatory effects of apremilast and the recurrent nature of psoriasis. In contrast, deucravacitinib exhibited a wider range of skin-related AEs, including acne, skin burning sensation, erythema, pruritus, and rash, suggesting a more complex dermatological risk profile. This diversity of cutaneous AEs for deucravacitinib underscored the need for enhanced monitoring and management of skin during clinical use. In the gastrointestinal disorders category, apremilast demonstrated significant signals for gastrointestinal AEs, particularly diarrhea, nausea, abdominal discomfort, frequent bowel movements, and upper abdominal pain. These findings suggested that apremilast has a more concentrated and severe impact on the gastrointestinal system, warranting close monitoring and appropriate symptomatic management during clinical practice. In contrast, deucravacitinib did not exhibit significant gastrointestinal AE signals, implying a lower gastrointestinal risk profile. In the infections category, URTI and sinusitis were more prevalent for apremilast, while folliculitis and oral herpes were the primary infectious AE for deucravacitinib, revealing a different pattern of infection-related risks between the two drugs. Lastly, in the nervous system disorders category, headache was a significant AE for both drugs, but apremilast displayed stronger signals than deucravacitinib. Burning sensation was more frequently associated with deucravacitinib, whereas tension headache, sinus headache, and migraine were more related to apremilast.
 |
Figure 3 Comparison of four system organ classes safety signals between apremilast and deucravacitinib. (A) the safety signals of skin and subcutaneous system; (B) the safety signals of gastrointestinal system; (C) the safety signals of infections; (D)the safety signals of nervous system. |
We also compared sex differences in AEs associated with apremilast and deucravacitinib (Figure 4). Notable skin-related AEs, such as acne, erythema, pruritus, and rash, seemed to be more pronounced in females taking deucravacitinib than in males. For apremilast, AEs such as recurrence of psoriasis, psoriatic arthritis, and therapy non-responder were distributed almost equally between males and females. However, AEs like tension headache and soft faeces appeared to exhibit a sex-related pattern, suggesting potential differences that may warrant further investigation.
 |
Figure 4 Comparison of sex differences in safety signals between apremilast and deucravacitinib. (A) the safety signals for deucravacitinib between sexes; (B) the safety signals for apremilast between sexes. |
Discussion
Given the widespread clinical use of apremilast and the potential of deucravacitinib as a newly approved drug for psoriasis treatment, evaluating their safety profiles has become a crucial area of research.21,22 Previous research comparing the safety of deucravacitinib and apremilast has have primarily relied on data from clinical trials.18,21,23–26 However, there is a limited but crucial need for comprehensive safety analyses of these two drugs in post-marketing and real-world settings, as such studies may reveal safety characteristics distinct from those observed in clinical trials.27 This is a pharmacovigilance study focusing on the real-world safety of two oral small-molecule drugs, namely apremilast and deucravacitinib, in the treatment of psoriasis, providing clinicians with valuable evidence to monitor and manage adverse events, thereby optimizing treatment strategies.
In our study, the characteristics of AEs at the SOC level indicated that apremilast is more likely to cause gastrointestinal and nervous system AEs, as well as disease recurrence, while deucravacitinib poses a higher risk of cutaneous and oral AEs. The different patterns in AEs between apremilast and deucravacitinib may be closely linked to the drugs’ mechanism of action.28 Apremilast enhances intracellular cyclic adenosine monophosphate (cAMP) levels and modulate the production of pro-inflammatory and anti-inflammatory mediators.11,30 This mechanism broadly affects multiple inflammatory signaling pathways. Deucravacitinib is a highly selective TYK2 inhibitor that binds allosterically to the pseudokinase JH2 (regulatory) domain of TYK2, thus inhibiting the signaling of pro-inflammatory cytokines such as IL-12, IL-23, and IFN-α. This unique mechanism may enhance its selectivity and reduce the risk of adverse events associated with other JAK isoforms.31–33
Regarding gastrointestinal system disorders, apremilast is significantly more prevalent to cause AEs like diarrhea, nausea, and vomiting, whereas deucravacitinib mainly causes milder and non-significant gastrointestinal discomfort. As mentioned above, the elevated cAMP by PDE4 inhibition can activate the cystic fibrosis transmembrane conductance regulator (CFTR), which is a chloride ion channel in intestinal epithelial cells, thus leading to excessive fluid secretion and secretory diarrhea.34 This process can further exacerbate as elevated cAMP can also enhance intestinal smooth muscle motility.35,36 The increase in vomiting and nausea associated with PDE4 inhibition is not fully understood, but it may be result from both central and peripheral mechanisms.37 A previous study revealed that cAMP signaling alterations may contribute to the emetic effects of PDE4 inhibitors within the human brainstem.38 In the skin and subcutaneous tissues, the main AE of apremilast is psoriasis recurrence, while deucravacitinib is more frequently associated with various skin-related AEs, including acne, pruritus, rash, and erythema. This is consistent with a previous meta-analysis, which demonstrated a significant increase in incidence of acne associated with deucravacitinib.39 In addition, although the case report number is limited, the safety signals for acneiform dermatitis and rosacea following deucravacitinib use were also notable. The specific mechanism of higher risk for skin-related AEs during deucravacitinib treatment is complex and demands further in-depth investigations, as prior studies have identified the involvement of the JAK-STAT pathway in chronic cutaneous inflammatory conditions, such as rosacea and acne.40,41 Although theoretically inhibiting the JAK-STAT pathway may be beneficial for certain skin inflammatory diseases, in practical applications it may paradoxically lead to unexpected AEs, paralleling similar observations with other treatments like oral corticosteroids.42 Regarding infections, deucravacitinib and apremilast exhibit different patterns, with deucravacitinib showing higher disproportionality in certain infection-related AEs, including folliculitis and oral herpes. TYK2 has multiple immunological roles and mediates both pro-inflammatory and antiviral cytokine responses, which may partially explain the differences in infection-related AEs between the two drugs.43,44 Regarding nervous system disorders, both drugs exhibit significant risk for headache, with apremilast showing stronger signals than deucravacitinb, suggesting that the risk of headache may differ between the two drugs.
Although the major adverse events (AEs) of apremilast and deucravacitinib align with their respective drug labels, our analyses identified additional AEs not documented in the instructions.10,45 In previous Phase 2 and 3 trials of apremilast, common AEs included diarrhea, nausea, URTI, nasopharyngitis, tension-type headaches, and headaches, findings that correspond with our study.25,26 However, we also observed AEs absent from the label, such as sinus headaches, multiple allergies, and gallbladder disease. Notably, existing studies suggest insufficient evidence regarding the safety of long-term use, potentially explaining the discrepancy.46 This may indicate that certain AEs manifest over prolonged treatment periods and are thus not captured in clinical trials, underscoring the necessity for clinicians to consider long-term drug impacts when managing chronic diseases like psoriasis. Similarly, the clinical trials of deucravacitinib have reported AEs such as nasopharyngitis, URTI, acne, headaches, and diarrhea.18,21,24 Our findings revealed additional AEs primarily involving cutaneous and oral reactions, including pruritus, rashes, erythema, skin burning sensations, urticaria, oral pain, and oral mucosal blistering. Of particular interest is the emergence of rare but significant safety signals for acneiform dermatitis and rosacea. While acne is listed on the drug label, the observed severity of acneiform dermatitis and rosacea exceeds that of typical acne, warranting increased vigilance from both patients and healthcare providers. Given that deucravacitinib has been on the market for only one year, many reported AEs—including fluctuating signals for URTI, diarrhea, and unlisted skin-related reactions—are based on limited data. Therefore, further studies are essential to validate the post-marketing safety profile of deucravacitinib.
Our analyses also found some sex differences in AE patterns of apremilast and deucravacitinib. Firstly, females reported significantly more AERs than males, with rates of 63.65% vs. 34.76% for apremilast and 59.81% vs 33.69% for deucravacitinib. This may be partly due to a slightly higher number of female psoriasis patients compared to males.47–49 Additionally, women with psoriasis often experience a greater disease burden, including poorer quality of life (QoL), more severe pruritus, more frequent fatigue, and increased work disability.50–54 These factors could contribute to a higher likelihood of drug use among female patients. Furthermore, female patients were more likely to experience specific AEs than male patients, such as skin-related reactions with deucravacitinib and tension headaches with apremilast. Women often have higher drug concentrations and longer elimination times, possibly due to physiological differences, which could influence AE rates.55 These observations suggest that sex-related factors may be associated with the AE patterns of apremilast and deucravacitinib.
Although our findings offer valuable insights for managing AEs related to apremilast and deucravacitinib, there are several limitations. Firstly, this pharmacovigilance study is based on FAERS database, which is a spontaneous reporting system that might have variable quality and potential bias due to incomplete and inaccurate data from various sources. The occurrence of AEs can be influenced by different confounders and factors, such as concomitant drug use, drug dosage, duration of drug use, and baseline comorbidities. Additionally, the time intervals for AE reports were not uniform between the two drugs due to data availability. Thus, healthcare professionals should continue to closely monitor adverse events in clinical practice to ensure timely intervention. Moreover, the causal relationship between apremilast or deucravacitinib and AEs cannot be established by this disproportionality analysis, as it only indicates signal strength without confirming causality. To address this, more in-depth investigations that focus on the mechanism of action of drugs and the underlying causes of side effects are needed to establish the causal relationship between drug use and AEs, distinguishing them from those resulting from the natural progression of the disease.
Conclusion
This FAERS-based study systematically and comprehensively identified the safety signals of apremilast and deucravacitinib, offering valuable real-world insights into the safety profiles of these two drugs. Our finding showed that apremilast was closely associated with AEs such as psoriasis relapse, gastrointestinal, and nervous system disorders. Deucravacitinib, on the other hand, shows a more complex risk profile of skin and oral AEs, with skin-related AEs being more prevalent among females.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Exemption Statement
This study exclusively uses publicly available data from the FDA Adverse Event Reporting System (FAERS). No new human participants were recruited, and no personally identifiable information was involved. According to Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Subjects (February 18, 2023, China), research that does not cause harm to individuals, does not involve sensitive personal information or commercial interests, and falls into the following categories is exempt from ethics review to reduce unnecessary burdens on researchers and promote life science and medical research: (1) Research using legally obtained public data or data generated through the observation of public behavior without interference; (2) Research using anonymized data. As this study meets these criteria, it is exempt from additional ethics review.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The abstract of this paper was presented as a poster at the 2024 Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) Annual Meeting and Trainee Symposium with interim findings. The poster is available online at: https://grappa-ac24.performedia.com/wp-content/uploads/2024/06/NEW-POSTER-2024-GRAPPA-%E5%89%AF%E6%9C%AC.pdf.
The authors report no conflicts of interest in this work.
References
1. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983–994. doi:10.1016/S0140-6736(14)61909-7
2. Michalek IM, Loring B, John SM. WHO Global report on psoriasis. World Health Organization; 2016.
3. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis: a review. JAMA. 2020;323(19):1945–1960. doi:10.1001/jama.2020.4006
4. Ritchlin CT, Colbert RA, Gladman DD. Psoriatic Arthritis. N Engl J Med. 2017;376(10):957–970. doi:10.1056/NEJMra1505557
5. Moraes FA, da Silva MRR, Dos Santos JBR, et al. Health-related quality of life in psoriatic arthritis: findings and implications. Value Health Reg Issues. 2021;26:135–141. doi:10.1016/j.vhri.2021.06.003
6. Varni JW, Globe DR, Gandra SR, Harrison DJ, Hooper M, Baumgartner S. Health-related quality of life of pediatric patients with moderate to severe plaque psoriasis: comparisons to four common chronic diseases. Eur J Pediatr. 2012;171(3):485–492. doi:10.1007/s00431-011-1587-2
7. Takeshita J, Grewal S, Langan SM, et al. Psoriasis and comorbid diseases: epidemiology. J Am Acad Dermatol. 2017;76(3):377–390. doi:10.1016/j.jaad.2016.07.064
8. Xu Y, Li Z, Wu S, Guo L, Jiang X. Oral small-molecule tyrosine kinase 2 and phosphodiesterase 4 inhibitors in plaque psoriasis: a network meta-analysis. Front Immunol. 2023;14:1180170. doi:10.3389/fimmu.2023.1180170
9. Schafer PH, Parton A, Gandhi AK, et al. Apremilast, a cAMP phosphodiesterase-4 inhibitor, demonstrates anti-inflammatory activity in vitro and in a model of psoriasis. Br J Pharmacol. 2010;159(4):842–855. doi:10.1111/j.1476-5381.2009.00559.x
10. Corporation C. Otezla (apremilast) [package insert]. U.S. Food and Drug Administration; 2023.
11. Estevinho T, Lé AM, Torres T. Deucravacitinib in the treatment of psoriasis. J Dermatolog Treat. 2023;34(1):2154122. doi:10.1080/09546634.2022.2154122
12. Wrobleski ST, Moslin R, Lin S, et al. Highly selective inhibition of tyrosine kinase 2 (TYK2) for the treatment of autoimmune diseases: discovery of the allosteric inhibitor BMS-986165. J Med Chem. 2019;62(20):8973–8995. doi:10.1021/acs.jmedchem.9b00444
13. Thaçi D, Strober B, Gordon KB, et al. Deucravacitinib in moderate to severe psoriasis: clinical and quality-of-life outcomes in a phase 2 trial. Dermatol Ther. 2022;12(2):495–510. doi:10.1007/s13555-021-00649-y
14. Hoy SM. Deucravacitinib: first Approval. Drugs. 2022;82(17):1671–1679. doi:10.1007/s40265-022-01796-y
15. Mease PJ, Deodhar AA, van der Heijde D, et al. Efficacy and safety of selective TYK2 inhibitor, deucravacitinib, in a Phase II trial in psoriatic arthritis. Ann Rheum Dis. 2022;81(6):815–822. doi:10.1136/annrheumdis-2021-221664
16. Daudén Tello E, Alonso Suárez J, Beltrán Catalán E, et al. Multidisciplinary management of the adverse effects of apremilast. Actas Dermosifiliogr. 2021;112(2):134–141. doi:10.1016/j.ad.2020.08.007
17. Hu C, Han X, Cui Y, Zhang Y, Cheng Y. Safety and efficacy of deucravacitinib for moderate to severe plaque psoriasis: a meta-analysis. Skin Res Technol. 2024;30(8):e13855. doi:10.1111/srt.13855
18. Strober B, Blauvelt A, Warren RB, et al. Deucravacitinib in moderate-to-severe plaque psoriasis: pooled safety and tolerability over 52 weeks from two Phase 3 trials (POETYK PSO-1 and PSO-2). J Eur Acad Dermatol Venereol. 2024;38(8):1543–1554. doi:10.1111/jdv.19925
19. Potestio L, Tommasino N, Lauletta G, et al. Efficacy and safety of deucravacitinib for the management of psoriasis: a drug safety evaluation. Expert Opin Drug Saf. 2024;23(6):677–685. doi:10.1080/14740338.2024.2351462
20. Lee EB, Amin M, Egeberg A, Wu JJ. Adverse events associated with apremilast use and withdrawal for psoriasis in a real-world setting. J Eur Acad Dermatol Venereol. 2018;32(10):e393–e4. doi:10.1111/jdv.15061
21. Lebwohl M, Warren RB, Sofen H, et al. Deucravacitinib in plaque psoriasis: 2-year safety and efficacy results from the Phase III POETYK trials. Br J Dermatol. 2024;190(5):668–679. doi:10.1093/bjd/ljae014
22. Mease PJ, Hatemi G, Paris M, et al. Apremilast long-term safety up to 5 years from 15 pooled randomized, placebo-controlled studies of psoriasis, psoriatic arthritis, and Behçet’s syndrome. Am J Clin Dermatol. 2023;24(5):809–820. doi:10.1007/s40257-023-00783-7
23. Crowley J, Thaçi D, Joly P, et al. Long-term safety and tolerability of apremilast in patients with psoriasis: pooled safety analysis for ≥156 weeks from 2 phase 3, randomized, controlled trials (ESTEEM 1 and 2). J Am Acad Dermatol. 2017;77(2):310–7.e1. doi:10.1016/j.jaad.2017.01.052
24. Imafuku S, Okubo Y, Tada Y, et al. Deucravacitinib, an oral, selective, allosteric tyrosine kinase 2 inhibitor, in Japanese patients with moderate to severe plaque, erythrodermic, or generalized pustular psoriasis: efficacy and safety results from an open-label, phase 3 trial. J Dermatol. 2024;51(3):365–379. doi:10.1111/1346-8138.17074
25. Ohtsuki M, Okubo Y, Komine M, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in the treatment of Japanese patients with moderate to severe plaque psoriasis: efficacy, safety and tolerability results from a phase 2b randomized controlled trial. J Dermatol. 2017;44(8):873–884. doi:10.1111/1346-8138.13829
26. Rich P, Gooderham M, Bachelez H, et al. Apremilast, an oral phosphodiesterase 4 inhibitor, in patients with difficult-to-treat nail and scalp psoriasis: results of 2 phase III randomized, controlled trials (ESTEEM 1 and ESTEEM 2). J Am Acad Dermatol. 2016;74(1):134–142. doi:10.1016/j.jaad.2015.09.001
27. Martin K, Bégaud B, Latry P, Miremont-Salamé G, Fourrier A, Moore N. Differences between clinical trials and postmarketing use. Br J Clin Pharmacol. 2004;57(1):86–92. doi:10.1046/j.1365-2125.2003.01953.x
28. Chen X, Wang Y, Wang P, et al. Systematic analysis of the associations between adverse drug reactions and pathways. Biomed Res Int. 2015;2015:670949. doi:10.1155/2015/670949
29. Drakos A, Torres T, Vender R. Emerging oral therapies for the treatment of psoriasis: a review of pipeline agents. Pharmaceutics. 2024;16(1):111. doi:10.3390/pharmaceutics16010111
30. Gooderham M, Papp K. Selective phosphodiesterase inhibitors for psoriasis: focus on apremilast. BioDrugs. 2015;29(5):327–339. doi:10.1007/s40259-015-0144-3
31. Lé AM, Puig L, Torres T. Deucravacitinib for the treatment of psoriatic disease. Am J Clin Dermatol. 2022;23(6):813–822. doi:10.1007/s40257-022-00720-0
32. Chimalakonda A, Burke J, Cheng L, et al. Selectivity profile of the tyrosine kinase 2 inhibitor deucravacitinib compared with Janus kinase 1/2/3 inhibitors. Dermatol Ther. 2021;11(5):1763–1776. doi:10.1007/s13555-021-00596-8
33. Rusiñol L, Puig L. Tyk2 Targeting in Immune-Mediated Inflammatory Diseases. Int J mol Sci. 2023;24(4):3391. doi:10.3390/ijms24043391
34. Blauvelt A, Langley RG, Gordon KB, et al. Next Generation PDE4 Inhibitors that Selectively Target PDE4B/D Subtypes: a Narrative Review. Dermatol Ther. 2023;13(12):3031–3042. doi:10.1007/s13555-023-01054-3
35. Tanahashi Y, Komori S, Matsuyama H, Kitazawa T, Unno T. Functions of muscarinic receptor subtypes in gastrointestinal smooth muscle: a review of studies with receptor-knockout mice. Int J mol Sci. 2021;22(2).
36. Prissadova N, Argirova MD, Krastev AD, Turiiski VI, Ardasheva RI. Participation of cAMP in tacrine-induced gastric smooth muscle relaxation. Central European Journal of Biology. 2011:16–22.
37. Robichaud A, Tattersall FD, Choudhury I, Rodger IW. Emesis induced by inhibitors of type IV cyclic nucleotide phosphodiesterase (PDE IV) in the ferret. Neuropharmacology. 1999;38(2):289–297. doi:10.1016/S0028-3908(98)00190-7
38. Mori F, Pérez-Torres S, De Caro R, et al. The human area postrema and other nuclei related to the emetic reflex express cAMP phosphodiesterases 4B and 4D. J Chem Neuroanat. 2010;40(1):36–42.
39. Martinez J, Manjaly C, Manjaly P, et al. Janus kinase inhibitors and adverse events of acne: a systematic review and meta-analysis. JAMA Dermatol. 2023;159(12):1339–1345.
40. Li T, Zeng Q, Chen X, et al. The therapeutic effect of artesunate on rosacea through the inhibition of the JAK/STAT signaling pathway. Mol Med Rep. 2018;17(6):8385–8390. doi:10.3892/mmr.2018.8887
41. Awad SM, Tawfik YM, El-Mokhtar MA, El-Gazzar AF, Abdel Motaleb AA. Activation of Janus kinase signaling pathway in acne lesions. Dermatol Ther. 2021;34(1):e14563. doi:10.1111/dth.14563
42. Kazandjieva J, Tsankov N. Drug-induced acne. Clin Dermatol. 2017;35(2):156–162.
43. Schwartz DM, Kanno Y, Villarino A, Ward M, Gadina M, O’Shea JJ. JAK inhibition as a therapeutic strategy for immune and inflammatory diseases. Nat Rev Drug Discov. 2017;16(12):843–862.
44. Shaw MH, Freeman GJ, Scott MF, et al. Tyk2 negatively regulates adaptive Th1 immunity by mediating IL-10 signaling and promoting IFN-gamma-dependent IL-10 reactivation. J Immunol. 2006;176(12):7263–7271.
45. Administration USFAD. SOTYKTU™ (deucravacitinib) tablets, for oral use Initial U.S. Approval: 2022: u.S. Food and Drug Administration; 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/214958s000lbl.pdf.
46. Yuan C, Ryan PB, Ta CN, Kim JH, Li Z, Weng C. From clinical trials to clinical practice: how long are drugs tested and then used by patients? J Am Med Inform Assoc. 2021;28(11):2456–2460. doi:10.1093/jamia/ocab164
47. AlQassimi S, AlBrashdi S, Galadari H, Hashim MJ. Global burden of psoriasis - comparison of regional and global epidemiology, 1990 to 2017. Int J Dermatol. 2020;59(5):566–571. doi:10.1111/ijd.14864
48. Mehrmal S, Uppal P, Nedley N, Giesey RL, Delost GR. The global, regional, and national burden of psoriasis in 195 countries and territories, 1990 to 2017: a systematic analysis from the Global Burden of Disease Study 2017. J Am Acad Dermatol. 2021;84(1):46–52. doi:10.1016/j.jaad.2020.04.139
49. Peng C, Xu X, Chen W, et al. Epidemiological variations in the global burden of psoriasis, an analysis with trends from 1990 to 2017. Front Med. 2021;8:585634. doi:10.3389/fmed.2021.585634
50. Napolitano M, Mastroeni S, Fania L, et al. Sex- and gender-associated clinical and psychosocial characteristics of patients with psoriasis. Clin Exp Dermatol. 2020;45(6):705–711. doi:10.1111/ced.14218
51. Mabuchi T, Yamaoka H, Kojima T, Ikoma N, Akasaka E, Ozawa A. Psoriasis affects patient’s quality of life more seriously in female than in male in Japan. Tokai J Exp Clin Med. 2012;37(3):84–88.
52. Youn SW, Lee JH, Yu DY, et al. The relationship between clinical characteristics including presence of exposed lesions and health-related quality of life (HRQoL) in patients with psoriasis: analysis from the nationwide epidemiologic study for psoriasis in Korea (EPI-PSODE study). J Eur Acad Dermatol Venereol. 2018;32(9):1499–1506. doi:10.1111/jdv.14865
53. Murer C, Sgier D, Mettler SK, et al. Gender differences in psoriasis: a Swiss online psoriasis survey. Arch Dermatol Res. 2021;313(2):89–94. doi:10.1007/s00403-020-02066-1
54. Damiani G, Cazzaniga S, Conic RR, Naldi L. Pruritus characteristics in a large Italian cohort of psoriatic patients. J Eur Acad Dermatol Venereol. 2019;33(7):1316–1324. doi:10.1111/jdv.15539
55. Zucker I, Prendergast BJ. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biol Sex Differ. 2020;11(1):32. doi:10.1186/s13293-020-00308-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Effectiveness and Safety of Deucravacitinib for the Management of Psoriasis: A Review of the Current Literature
Potestio L, Ruggiero A, Fabbrocini G, Martora F, Megna M
Psoriasis: Targets and Therapy 2023, 13:19-26
Published Date: 4 May 2023
Clinical Utility of Deucravacitinib for the Management of Moderate to Severe Plaque Psoriasis
Jin JQ, Spencer RK, Reddy V, Bhutani T, Liao W
Therapeutics and Clinical Risk Management 2023, 19:413-423
Published Date: 18 May 2023
Safety of Biologics for Psoriatic Patients with Latent Tuberculosis
Yuan L, Li Y, Lin J, Lin X, Yang B, Man MQ, Wang X
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2333-2336
Published Date: 28 August 2023