")
Back to Journals » Infection and Drug Resistance » Volume 18
AIDS-Associated Talaromyces marneffei Infection with Thoracic Spinal Cord Involvement Leading to Paraplegia: A Case Report and Literature Review
Authors Guo Y , Song Y, Peng X, Zhou X, Zhou H, Xu L , Zhu B
Received 28 September 2024
Accepted for publication 25 February 2025
Published 4 March 2025 Volume 2025:18 Pages 1263—1269
DOI https://doi.org/10.2147/IDR.S495568
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sandip Patil
Yongzheng Guo,1 Ying Song,2 Xiaorong Peng,1 Xiaotang Zhou,1 Hengjun Zhou,3 Lijun Xu,1 Biao Zhu1
1The Department of Infectious Diseases, State Key Laboratory for Diagnosis and Treatment of Infectious Diseases, National Clinical Research Center for Infectious Diseases, Collaborative Innovation Center for Diagnosis and Treatment of Infectious Diseases, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China; 2The Department of Infectious Diseases, The Third People’s Hospital of Shenzhen and The Second Affiliated Hospital of Southern University of Science and Technology, Shenzhen, Guangdong, People’s Republic of China; 3Department of Neurosurgery, the First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang, People’s Republic of China
Correspondence: Biao Zhu, Email [email protected]
Background: Talaromyces marneffei is a common opportunistic infection in patients with acquired immune deficiency syndrome (AIDS) in South China. Spinal cord abscesses caused by T. marneffei are exceptionally rare and present with non-specific symptoms, which may result in delayed diagnosis and heightened adverse prognoses.
Case Presentation: We report a case of a spinal cord abscess in a 30-year-old patient with AIDS that was caused by T. marneffei infection. The patient initially presented with T. marneffei septicemia and pleurisy. After initial antifungal treatment and combined antiretroviral therapy (cART), the patient’s condition temporarily improved. However, he discontinued the antifungal treatment against medical advice and subsequently developed paraplegia, T. marneffei meningitis, and related intracranial and thoracic spinal cord lesions. Neurosurgical resection of the spinal cord lesion, combined with continued cART and antifungal treatment, resulted in the intracranial mass in the cerebellum resolving on MRI, but the patient remained non-ambulatory and incontinent during the last follow-up in August 2024.
Conclusion: In patients with spinal cord abscesses and a history of disseminated T. marneffei infection, especially those with AIDS, talaromycosis should be considered as a potential differential diagnosis. Comprehensive management, encompassing adherence to treatment plans and effective follow-up, is crucial for improving prognosis.
Keywords: Talaromyces marneffei, HIV, fungi, abscess, spinal cord
Background
Talaromyces marneffei is a thermally dimorphic opportunistic fungus that causes talaromycosis. It is categorized as one of the 19 fungal pathogens featured on the World Health Organization’s Fungal Priority Pathogens List (WHO FPPL).1 Even though T. marneffei infection is placed in the “medium priority” category on the FPPL, it notably ranks as the third most common opportunistic infection, surpassed only by tuberculosis and cryptococcosis, among patients with acquired immune deficiency syndrome (AIDS) residing in tropical and subtropical regions of Asia.1–3
T. marneffei can cause disseminated life‐threatening infections in patients with HIV/AIDS.2 The common manifestations of T. marneffei infection, including fever, respiratory signs, lymphadenopathy, hepatomegaly, and splenomegaly, lack diagnostic specificity.4 Involvement of the central nervous system (CNS) is exceptionally rare (<1%) and primarily manifests as non-specific meningitis or meningoencephalitis, with spinal cord infections being even rarer.5–8 With prompt diagnosis and appropriate treatment, patients with HIV/AIDS and T. marneffei infection can achieve similar outcomes to patients without HIV/AIDS.9 Nevertheless, the insidious and atypical symptoms of spinal cord infections exacerbate its complexity and lead to delayed diagnosis and treatment, which might be fatal. Talaromycosis mortality doubles from 24% to 50% when the diagnosis is delayed and approaches 100% when the diagnosis is missed.2,10 Initiation of combination antiretroviral therapy (cART) within 2 weeks helps to reduce the mortality due to talaromycosis.11 However, the activation of latent T. marneffei infections or the recurrence of persistent infection foci, despite effective antifungal treatment, during the immune reconstitution phase following early cART, significantly heightens the challenges associated with achieving accurate and early diagnosis.12
We describe here a case of spinal cord lesion due to disseminated T. marneffei infection in a patient with AIDS. Based on our knowledge and search of relevant databases, such a case has not been reported before. We also review similar cases to enhance the clinical understanding of this rare condition.
Case Presentation
In June 2023, a 30-year-old office worker was admitted to a local hospital due to chills, fever, fatigue, anorexia, dry cough, and chest pain. He had lived in Shanxi (North China) for a long time before he moved to Shenzhen (South China) 9 years ago. He had a history of homosexual activity for 5 years. He was diagnosed with a multitude of health conditions, including HIV infection, T. marneffei septicemia, and pleurisy. HIV infection was definitively confirmed through the detection of HIV antibodies and HIV RNA. His CD4+ T-cell count was 26 cells/µL, and HIV viral load was 3.71×107 copies/mL (Table 1). T. marneffei was positively identified through blood and pleural fluid cultures. His white blood cell (WBC) count was 2.23 × 109/L, and C-reactive protein level was 48.7 mg/L (Table 1). The results of the blood galactomannan (GM) test, cryptococcal capsular polysaccharide antigen (CrAg) test, and T-SPOT.TB test were negative (Table 1). Metagenomic next-generation sequencing (mNGS) of pleural fluid was employed to investigate other opportunistic infections and revealed 16,242 reads of T. marneffei and 59 reads of Epstein–Barr virus (EBV). The results of pleural fluid acid-fast stain, GeneXpert test, T-SPOT.TB test, and mycobacterial cultures were negative. The patient was initially administered two weeks of amphotericin B deoxycholate (AmBd, 25 mg/d, intravenously). According to the treatment plan, this was to be followed by oral itraconazole (ITR) at a dosage of 200 mg every 12 hours for 10 weeks, then adjusted to 200 mg daily until the CD4+ T-cell counts exceeded 100 cells/µL, for a minimum of 6 months. Concurrently, cART was initiated with dolutegravir/lamivudine (DTG/3TC) after the two-week AmBd treatment. The patient reported excellent adherence to cART throughout the treatment period. However, in December 2023, he discontinued the antifungal treatment without medical consultation, citing perceived improvement in his condition, and thus did not complete the planned ITR regimen.
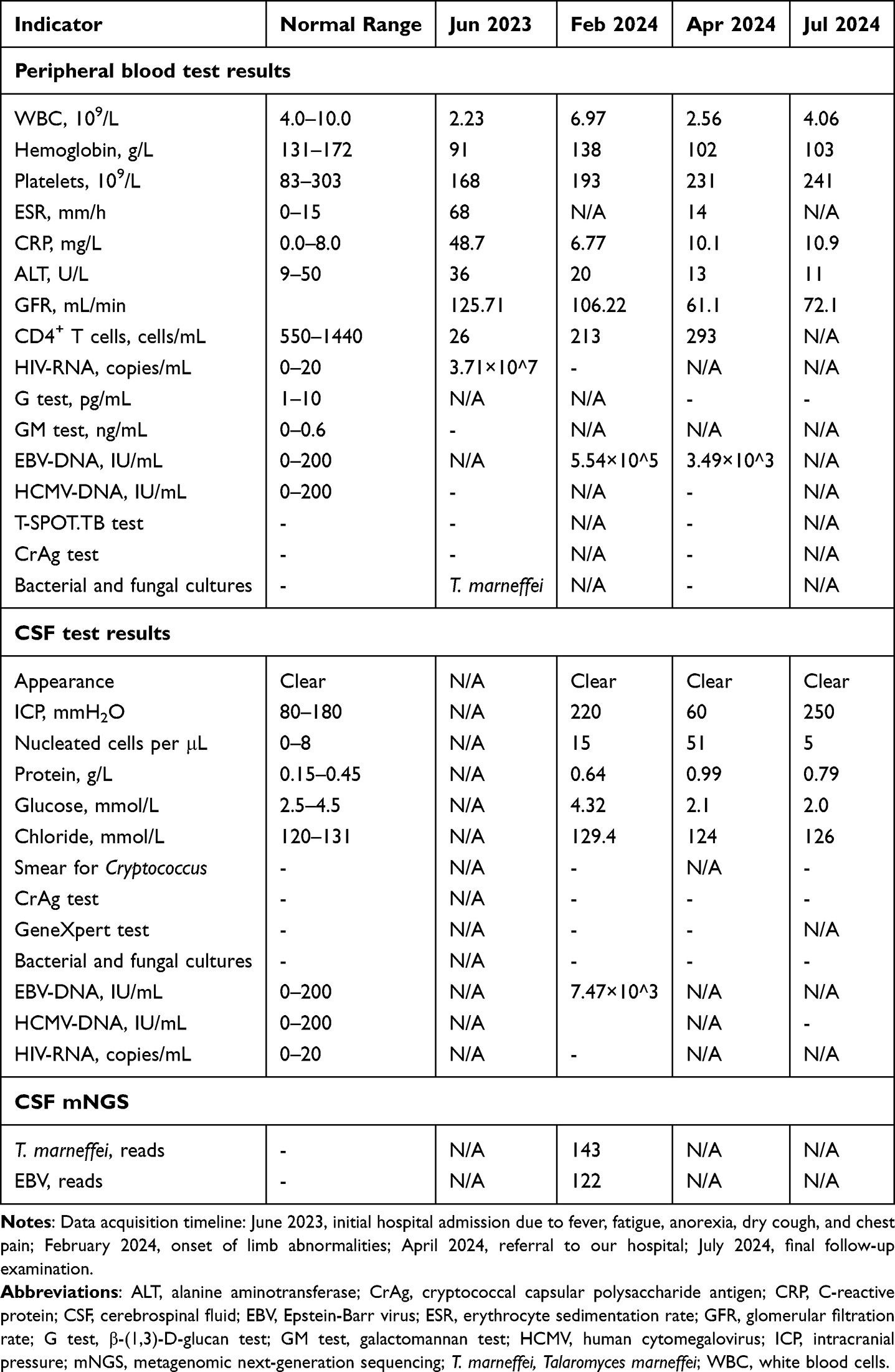 |
Table 1 Changes in Peripheral Blood & CSF Parameters |
On February, 2024, the patient presented with sudden bilateral lower limb muscle weakness and sensory loss, without symptoms such as fever, respiratory issues, dizziness, headache, and altered consciousness. He had grade 1 muscle strength in both lower limbs and sensory impairment below thoracic vertebra (T)12. Spinal MRI revealed a 1.1-cm nodular abnormality in the spinal cord at T6. His blood WBC count was 6.97 × 109/L, and the CD4+ T-cell count had increased to 213 cells/µL (Table 1). Moreover, the HIV viral load had decreased to less than 20 copies/mL, and the EBV-DNA concentration was 5.54×105 IU/mL (Table 1). Lumbar puncture revealed an intracranial pressure (ICP) of 220 mmH2O, and cerebrospinal fluid (CSF) analysis showed a nucleated cell count of 15 cells/μL, a protein concentration of 0.64 g/L, and a glucose concentration of 4.32 mmol/L (Table 1). Bacterial and fungal cultures of CSF were negative (Table 1). Additionally, the CSF test results indicated the presence of EBV-DNA at a concentration of 7.47×103 IU/mL, while the results of tests for HIV-RNA, human cytomegalovirus (HCMV)-DNA, GeneXpert, and CrAg were all negative (Table 1). T. marneffei (143 reads) and EBV (122 reads) was detected by CSF analysis using mNGS (Table 1). AmBd was administered intravenously at a dose of 25 mg daily for 10 days. Subsequently, voriconazole (VOR) was prescribed orally at a loading dose of 400 mg every 12 h on the first day, followed by a maintenance dose of 200 mg every 12 h. The patient exhibited fluctuating declines in sensation and muscle strength.
On April 22, 2024, the patient was referred to our hospital with numbness and weakness in both lower limbs for more than 2 months. The patient presented with fecal and urinary incontinence, significant sensory impairment below T8, a muscle strength of 0 in both lower limbs, and a positive Babinski sign on the right side. His blood tests showed a WBC count of 2.56 × 109/L, a CD4+ T cell count of 293 cells/mL, and an EBV-DNA concentration of 3.49×103 IU/mL. The results of the β-(1,3)-d-glucan (G) test, Mp1p antigen detection, T-SPOT.TB test, CrAg test, and HCMV-DNA test were all negative (Table 1). ICP was 60 mmH2O, and CSF analysis revealed a nucleated cell count of 51 cells/μL, a protein concentration of 0.99 g/L, and a glucose concentration of 2.1 mmol/L. Bacterial and fungal cultures of CSF, as well as the results of the GeneXpert test and CrAg test, were all negative (Table 1). MRI showed an enlarged thoracic cord lesion and an enhanced nodule in the right cerebellar hemisphere (Figure 1). We speculated that the patient might have disseminated T. marneffei meningitis and intracranial abscess.
 |
Figure 1 Comparison of MRI findings: pre-surgery versus 2 months post-treatment. Pre-surgery MRI: A 0.8-cm nodule in the right cerebellar hemisphere (A and B) and a 2.1-cm mass in the thoracic spinal cord (C and D). Follow-up MRI at 2 months after surgical resection of the spinal cord mass and antifungal treatment: Resolution of the cerebellar lesion (E and F) and improvement in the thoracic spinal cord lesion, despite residual slight thickening and patchy long T2 signals (G and H).The white arrows in panels A, B, C, D, G, and H indicate the locations of the lesions. |
On May 6, 2024, neurosurgeons resected the intramedullary lesion at the T6 level of the thoracic cord and uncovered an abscess measuring 2 cm × 1.5 cm × 1.5 cm. Due to the relatively small volume of samples, only mNGS testing and pathological examination were carried out. Both fungal immunofluorescence and periodic acid-Schiff staining yielded positive results (Supplementary Figure 1). The in situ hybridization technique also showed scattered mildly positive EBV-encoded RNA. mNGS of the resected tissue confirmed the presence of T. marneffei (3202 reads) and EBV (21 reads). Due to the patient’s decreased glomerular filtration rate (61.1 mL/min), AmBd was administered intravenously at a dosage of 15 mg/day, in addition to the oral VOR regimen. Upon discharge, the patient continued with the oral VOR regimen.
During the follow-up in July 2024, MRI revealed that the lesion in the right cerebellar hemisphere had disappeared (Figure 1). This was indicative of a T. marneffei infection, even though biopsy and other examinations were not performed. The patient then returned to his hometown in Shanxi Province. A phone follow-up was carried out in August. The patient reported that he had adhered well to both cART and antifungal therapy and reported slight improvements in muscle strength and sensation in his lower limbs. However, the patient remained non-ambulatory and incontinent. In November 2024, we could not reach the patient and have been unable to contact him since.
Discussion and Conclusion
Invasive T. marneffei infections are generally associated with severe cellular immune dysfunction and are more likely to disseminate hematogenously and involve the CNS in patients with HIV than in those without HIV.5 Despite this, CNS involvement is non-specific and uncommon, with spinal cord involvement being even rarer, making the present case exceptionally unique.5
A search of PubMed, Embase, and Web of Science (published in the last 15 years, until Nov 2024) for “marneffei” and “spinal cord” (filtered for English language) yielded only one case report.6 This report describes an immune-competent patient without HIV infection who presented with multiple T. marneffei lesions in the brain, spinal cord, and lungs.6 The patient was treated with AmBd and ITR, which resulted in gradual resolution of lower limb weakness within a month.6
The detection of T. marneffei in CSF signifies an increased risk of intracranial infection. It was difficult to determine the sequential order of infection in the meninges and brain parenchyma. It has been established that the fungus, through inducing M2 macrophage polarization, can disseminate and eventually traverse the blood–brain barrier and blood-CSF barrier to establish latent infections within the CNS.13 In patients with HIV/AIDS who are infected with T. marneffei and achieve a good immunological response to cART, relapse is rare, as long as antifungal treatment is maintained.14 Initially, the underlying cause of thoracic spinal cord lesions was uncertain, primarily due to the rarity of T. marneffei infections in this specific region. Furthermore, in this severely immunocompromised patient, discontinuation of antifungal therapy during immune reconstitution following cART triggered T. marneffei-associated immune reconstitution inflammatory syndrome (IRIS), which presented as nonspecific neurological dysfunction. IRIS, a common complication in patients with HIV/AIDS and T. marneffei infection, is associated with extended hospital stays and increased readmission rates, as well as exacerbating both the financial and disease burden for patients.12 Moreover, besides T. marneffei-associated IRIS, the differential diagnosis of intramedullary rim-enhancing lesion of the spinal cord includes other conditions, such as various intramedullary tumors and lymphomas, inflammatory diseases of the spinal cord (such as sarcoidosis), hemorrhages or infarctions within the spinal cord, syringomyelia, and spinal cord opportunistic infections caused by mycobacteria, fungi, and viruses. These factors further complicate the diagnosis of thoracic spinal cord intramedullary space-occupying lesions in patients with HIV/AIDS and T. marneffei infection.15 Consequently, there is a pressing need for further research on T. marneffei-associated IRIS to enable early diagnosis.
Culture, the current primary diagnostic method, has limited sensitivity and is time consuming.2,16 Microscopic tissue analysis offers quicker presumptive diagnosis of talaromycosis compared to culture-based methods.13,16 However, it requires skilled personnel to validate the findings.13,16 mNGS has both high efficiency and remarkable accuracy in mixed infection, with sensitivity and specificity reaching 100% and 98.7%, respectively.13,16 The most rapid presumptive diagnostic methods are serological antigen or antibody detection methods. For example, the G test holds potential for travelers to non-endemic areas.13,17 Additionally, the GM test demonstrates high specificity, especially in endemic regions, although it may have cross-reactivity with other fungi.13,18 Notably, our patient, who lived in southern China—an area with the highest incidence of T. marneffei infection—tested negative for GM in the blood in June 2023. With regard to other detection methods, immunoassays for T. marneffei Mp1p and 4D1 demonstrate high specificity and sensitivity.13 Both methods align well with blood cultures and may, thereby, facilitate early treatment decisions, although further validation is required.13
Antifungal medication concentrations vary in blood, CSF, and brain parenchyma. Therapeutic drug monitoring boosts treatment success and minimizes adverse reactions, but direct measurement in CSF and brain parenchyma is clinically impractical.19 Thus, a currently clinically feasible approach is to use antifungal agents with robust CNS penetration for ongoing maintenance therapy, coupled with strict adherence to the prescribed regimen and rigorous monitoring of adverse drug reactions. This is crucial to avert relapses of T. marneffei infections. In cases of advanced HIV infection with talaromycosis abscesses in the CNS, there is currently no consensus on the optimal antifungal treatment duration. Surgery, continued cART, and a prolonged course of antifungal therapy may well constitute a reasonable treatment approach.8,20 The duration of antifungal therapy should be based on CD4+ T cell counts and clinical/imaging improvement.20
Approximately 95% of adults are infected with EBV.12 In patients with HIV, immune suppression leads to EBV persistence and reactivation. Severe immune suppression in these patients increases the risk of high EBV-DNA loads and invasive T. marneffei infections, both associated with immune dysfunction and suggesting a potential association between EBV and T. marneffei. Importantly, EBV co-infection is an independent risk factor for mortality related to T. marneffei infection.9 Previous studies have established a strong link between EBV and the development of lymphoma in patients with HIV. The coexistence of T. marneffei and lymphoma has been reported in three case reports, with one case describing a brain abscess combined with T. marneffei infection and B-cell non-Hodgkin lymphoma.15,21,22 In our case, EBV was detected at multiple sites. With regard to last contact with the patient, no evidence of tumor has been found. However, if conditions permit, regular follow-up remains essential for monitoring the development of lymphoma.
The multifaceted health challenges posed by immunodeficiency disorders underscore the need for a comprehensive, multi-disciplinary treatment approach. As patients with HIV/AIDS live longer as a result of improved management strategies, the likelihood of complications is increasing. This is likely to lead to escalated demand for such integrated care models. To meet these growing needs, future initiatives must prioritize enhancing capabilities for diagnosing and treating HIV-related complications, as well as for fostering deeper cooperation between infectious disease hospitals and comprehensive medical centers.
Based on the present findings, spinal cord abscess caused by T. marneffei infection should be considered as a differential diagnosis in patients with a history of disseminated T. marneffei infection who exhibit limb movement or sensory abnormalities. The comprehensive application of various diagnostic techniques, surgical intervention, cART, antifungal treatment, and interdisciplinary collaboration, along with a high level of adherence to medical care, is crucial for achieving a better prognosis in cases of talaromycosis abscesses. However, maintaining patients’ adherence through effective follow-up management necessitates further commitment and endeavor.
Data Sharing Statement
The patient data utilized in this study are partially presented in the table. The remaining data are available upon reasonable request by contacting the corresponding author.
Ethics Approval and Consent to Participate
Ethical approval for this case report (Approval Number: IIT20240838A) was obtained from the Ethics Committee of the First Affiliated Hospital of Zhejiang University School of Medicine. Written informed consent was obtained from the patient for publication.
Acknowledgments
We would like to express our gratitude to the patient and his family for their cooperation and to all frontline healthcare workers involved in direct diagnosis, treatment, and care of patients.
Funding
This work was supported by the National Major Scientific and Technological Special Project for “Significant New Drugs Development” during the Thirteenth Five-Year Plan Period (grant number 2017ZX09303004-001). The funding organization had no involvement in the study or in the decision to submit the article for publication.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. WHO. Fungal priority pathogens list to guide research, development, and public health action. 2022. Available from: https://www.who.int/publications/i/item/9789240060241.
2. Jiang J, Meng S, Huang S, et al. Effects of Talaromyces marneffei infection on mortality of HIV/AIDS patients in southern China: a retrospective cohort study. Clin Microbiol Infect. 2019;25(2):233–241. doi:10.1016/j.cmi.2018.04.018
3. Le T, Wolbers M, Chi NH, et al. Epidemiology, seasonality, and predictors of outcome of AIDS-associated Penicillium marneffei infection in Ho Chi Minh City. Viet Nam Clin Infect Dis. 2011;52(7):945–952. doi:10.1093/cid/cir028
4. Limper AH, Adenis A, Le T, et al. Fungal infections in HIV/AIDS. Lancet Infect Dis. 2017;17(11):e334–e43. doi:10.1016/S1473-3099(17)30303-1
5. Lino R, Guimaraes AR, Sousa E, et al. Emerging fungal infections of the central nervous system in the past decade: a literature review. Infect Dis Rep. 2024;16(5):952–976. doi:10.3390/idr16050076
6. Zhu YM, Ai JW, Xu B, et al. Rapid and precise diagnosis of disseminated T. marneffei infection assisted by high-throughput sequencing of multifarious specimens in a HIV-negative patient: a case report. BMC Infect Dis. 2018;18(1):379. doi:10.1186/s12879-018-3276-5
7. Le T, Huu Chi N, Kim Cuc NT, et al. AIDS-associated Penicillium marneffei infection of the central nervous system. Clin Infect Dis. 2010;51(12):1458–1462. doi:10.1086/657400
8. Li YY, Dong RJ, Shrestha S, et al. AIDS-associated Talaromyces marneffei central nervous system infection in patients of southwestern China. AIDS Res Ther. 2020;17(1):26. doi:10.1186/s12981-020-00281-4
9. Wang Y, Mo X, Zhang J, et al. Clinical features of Talaromyces marneffei infection in HIV-positive and HIV-negative individuals: a retrospective study in southern China. Med Mycol. 2023;61(8). doi:10.1093/mmy/myad083
10. Hu Y, Zhang J, Li X, et al. Penicillium marneffei infection: an emerging disease in mainland China. Mycopathologia. 2013;175(1–2):57–67. doi:10.1007/s11046-012-9577-0
11. Qin Y, Zhou Y, Liu S, et al. HIV-associated talaromycosis: does timing of antiretroviral therapy matter? J Infect. 2022;84(3):410–417. doi:10.1016/j.jinf.2021.12.032
12. Zhang Q, Zhang H, Guo P, et al. Clinical characteristics and prognosis of Talaromycosis marneffei associated immune reconstitution inflammatory syndrome in AIDS patients. PLoS Negl Trop Dis. 2024;18(10):e0012609. doi:10.1371/journal.pntd.0012609
13. Zaongo SD, Zhang F, Chen Y. An overview of diagnostic and management strategies for talaromycosis, an underrated disease. J Fungi. 2023;9(6):647. doi:10.3390/jof9060647
14. Qiu Y, Zhang J, Liu G, et al. Retrospective analysis of 14 cases of disseminated Penicillium marneffei infection with osteolytic lesions. BMC Infect Dis. 2015;15:47. doi:10.1186/s12879-015-0782-6
15. Liu X, Xing H, Lin J, et al. Coexisting of primary central nervous system lymphoma and talaromyces marneffei brain abscess in an AIDS Patient, a case report and review of the literature. Infect Drug Resist. 2024;17:709–718. doi:10.2147/IDR.S432697
16. Liu L, Sun B, Ying W, et al. Rapid diagnosis of Talaromyces marneffei infection by metagenomic next-generation sequencing technology in a Chinese cohort of inborn errors of immunity. Front Cell Infect Microbiol. 2022;12:987692. doi:10.3389/fcimb.2022.987692
17. Karageorgopoulos DE, Vouloumanou EK, Ntziora F, et al. beta-D-glucan assay for the diagnosis of invasive fungal infections: a meta-analysis. Clin Infect Dis. 2011;52(6):750–770. doi:10.1093/cid/ciq206
18. Huang YT, Hung CC, Liao CH, et al. Detection of circulating galactomannan in serum samples for diagnosis of Penicillium marneffei infection and cryptococcosis among patients infected with human immunodeficiency virus. J Clin Microbiol. 2007;45(9):2858–2862. doi:10.1128/JCM.00050-07
19. Ashley ED. Antifungal drugs: special problems treating central nervous system infections. J Fungi. 2019;5(4):97. doi:10.3390/jof5040097
20. WHO. Guidelines for diagnosing, preventing, and managing cryptococcal disease among adults, adolescents, and children living with HIV. 2022. Available from https://www.who.int/publications/i/item/9789240052178/.
21. Wanzhen L, Weihua P, Xuefei HU, et al. AIDS combinated with penicilliosis marneffei and malignant lymphoma: the first case report. Chin J Nosocomiol. 2008;18(7):1038–1040. doi:10.3321/j.issn:1005-4529.2008.07.051
22. Yang Z, Zeng W, Qiu Y, et al. Nodular sclerosing Hodgkin lymphoma combined with disseminated talaromyces marneffei infection: a case report. Infect Drug Resist. 2021;14:5671–5678. doi:10.2147/IDR.S340192
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Talaromyces marneffei is the Persistent Overwhelming Bloodstream Infection Pathogen Among HIV Inpatients in Fujian, China
Lai J, Liu Y, Ye H, Chen Y
Infection and Drug Resistance 2022, 15:5207-5214
Published Date: 5 September 2022
Disseminated Combined Talaromyces marneffei and Enterococcus faecium Bloodstream Infection Presenting as Gastrointestinal Perforation in a Patient with CARD9 Gene Mutation
Liang H, Duan X, Li T, Hu L, Guo J
Infection and Drug Resistance 2024, 17:4783-4790
Published Date: 31 October 2024