")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
An Effectiveness Trial of an Exercise Physiologist Service to Improve Quality of Life in Adults with Severe Mental Illness: Protocol for the MOVEMENT Study
Authors Chapman JJ , Siskind D, Yung AR, Lee YY, Arnautovska U , Scott JG, Burke K, Malacova E, Korman N , Wyder M, Doohan MA, Keating SE , Parker S, Walker ME, Hu D , O'Brien J , Lau G , Pratt GF, Rosenbaum S, Curtis J, Chatterton ML, Simmons L, Wheeler AJ
Received 27 March 2025
Accepted for publication 3 July 2025
Published 11 July 2025 Volume 2025:21 Pages 1399—1408
DOI https://doi.org/10.2147/NDT.S530837
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Taro Kishi
Justin J Chapman,1– 3 Dan Siskind,2,4,5 Alison R Yung,6 Yong Yi Lee,5,7,8 Urska Arnautovska,2,5 James G Scott,4,9,10 Kylie Burke,11– 13 Eva Malacova,14 Nicole Korman,2,4,5 Marianne Wyder,2 Meg A Doohan,1 Shelley E Keating,15 Stephen Parker,4,13 Max E Walker,1 Di Hu,1 Jake O’Brien,16 Geoffrey Lau,2 Gregory F Pratt,17 Simon Rosenbaum,18 Jackie Curtis,18,19 Mary Lou Chatterton,7 Lisa Simmons,20 Amanda J Wheeler1,3,21
1School of Pharmacy and Medical Sciences, Centre for Mental Health, Griffith University, Southport, QLD, Australia; 2Addictions and Mental Health Service, Metro South Health, Brisbane, QLD, Australia; 3ALIVE National Centre for Mental Health Research, University of Melbourne, Parkville, VIC, Australia; 4School of Medicine, The University of Queensland, Herston, QLD, Australia; 5Queensland Centre for Mental Health Research, Brisbane, QLD, Australia; 6School of Medicine, Deakin University, Geelong, VIC, Australia; 7School of Public Health and Preventive Medicine, Monash University, Melbourne, VIC, Australia; 8School of Public Health, The University of Queensland, Herston, QLD, Australia; 9Child and Youth Mental Health Service, Children’s Health Queensland, Brisbane QLD, Australia; 10Child Health Research Centre, The University of Queensland, Brisbane, QLD, Australia; 11Parenting and Family Support Centre, School of Psychology, The University of Queensland, St Lucia, QLD, Australia; 12Australian Government through the Australian Research Council’s Centre of Excellence for Children and Families over the Life Course, The University of Queensland, Brisbane, QLD, Australia; 13Metro North Mental Health Service, Metro North Health, Herston, QLD, Australia; 14QIMR Berghofer Medical Research Institute, Herston, QLD, Australia; 15School of Human Movement and Nutrition Science, The University of Queensland, St Lucia, QLD, Australia; 16Department of Gastroenterology and Hepatology, Metro South Health, Brisbane, QLD, Australia; 17Mental Health and Genomics, Central Queensland University, Brisbane, QLD, Australia; 18Discipline of Psychiatry and Mental Health, School of Clinical Medicine, University of New South Wales, Sydney, NSW, Australia; 19Mindgardens Neuroscience Network, Sydney, NSW, Australia; 20Australian Institute of Tropical Health & Medicine, James Cook University, Townsville, QLD, Australia; 21Faculty of Medical and Health Sciences, Auckland University, Auckland, New Zealand
Correspondence: Justin J Chapman, Griffith University Centre for Mental Health 170 Kessels road Nathan, Brisbane, Queensland, 4111, Tel +61432 299 240, Email [email protected]
Introduction: Exercise can improve the quality of life (QoL) of people with severe mental illness (SMI); however, many experience practical, psychosocial, and socioeconomic barriers to commencing and maintaining exercise. This protocol describes a study aiming to assess the effectiveness of an Accredited Exercise Physiologist (AEP) service for improving QoL in adults with SMI.
Methods and Analysis: This is a prospective non-randomised effectiveness trial to evaluate the effectiveness and cost-effectiveness of an AEP service within mental healthcare settings. Participants will be adults (18+ years) with SMI recruited from public mental health services and community organizations. The primary outcome is QoL assessed using the Recovering Quality of Life questionnaire (ReQoL) assessed at baseline, 3-month and 6-month follow-up. Participants will be invited to a study in which they may self-select to access an AEP service for six months. Self-reported health, demographic and psychosocial influences will be measured and incorporated in analyses as covariates. This is a pragmatic observational approach to evaluating effectiveness, in which participants who attend the AEP service will be compared with those who decline. Reasons for non-participation will be explored, and rates of recruitment and adherence will be examined. Findings will provide insight into implementing AEP services in mental health settings.
Ethics and Dissemination: Ethics approval has been obtained from the Metro South Health Human Research Ethics Committee (HREC/2024/QMS/109698). We plan to submit a manuscript of the results to a peer-reviewed journal. Results will be presented at conferences, community and consumer forums and hospital grand rounds.
Trial Registration: The trial is registered under the Australian and New Zealand Clinical Trial Registry (ACTRN12624001148561).
Keywords: physical activity, implementation, mental health, health services, recovery, lifestyle intervention
Introduction
Severe mental illnesses (SMIs), such as major depression, bipolar disorder, and psychotic disorders, are characterised by persistent symptoms and functional challenges. Symptoms can fluctuate in severity over time, and include positive symptoms (eg, hallucinations, mania) and negative symptoms (eg, avolition, depressed mood). Depending upon the phase of illness,1 people with SMI may require support from clinical and non-clinical services across acute inpatient, intensive rehabilitation, and community settings. People with SMI also experience psychosocial disadvantages, such as social isolation, housing instability, low engagement in the workforce, and unhealthy lifestyle behaviours such as poor nutritional intake, low physical activity, and high rates of smoking and alcohol consumption.2 These factors lead to a heightened risk of preventable chronic disease such as diabetes,2 which further contributes to psychological distress and lower quality of life (QoL) of this group.3 Interventions to improve QoL and reduce the risk of chronic disease are needed to complement existing clinical mental healthcare for people SMI.
Physical activity (PA) and exercise intervention can improve QoL in people with mental illnesses.4–6 People with SMI have low levels of PA,7 but if supported appropriately, adherence to exercise interventions for this group is comparable with the general population (~70% completion rates).8 Meta-analyses indicate that exercise interventions can also reduce the positive and negative symptoms of psychosis and improve functioning and metabolic health in people with SMI.4,9,10 Exercise is an evidence-based therapy for improving health outcomes in people with a range of mental illnesses, and internationally adopted best-practice guidelines recommend lifestyle support for people with metabolic risks, including exercise intervention.11 Further, exercise delivered by qualified exercise professionals may improve adherence, cardiorespiratory fitness, and cognition for people with SMI compared with other providers such as mental health staff.4,8,12
Accredited Exercise Physiologists (AEPs) are qualified exercise professionals who specialise in rehabilitative exercise therapy, and professional consensus statements advocate for their role in mental health services.13–15 Because exercise intervention is generally outside the scope and role of mental health professionals, AEP involvement in mental health teams is highly valued by both participants and staff alike.16,17 Pioneering examples of service models incorporating AEPs within mental healthcare exist in Australia: the Keeping the Body in Mind program has operated since 2013 and evidenced improved health outcomes for young people and adults with psychotic disorders.18,19 Evaluations of AEP services for people with SMI have been conducted across inpatient, residential and community mental health settings, with sample sizes ranging from n=16 to 55. These studies demonstrated the feasibility and acceptability of AEP services,18–25 and promising indications for preventing cardiometabolic abnormalities18,19 and improving motivation, physical activity and fitness, sleep quality and negative symptoms.18–25 One study examined QoL outcomes for a 12-week AEP intervention, reporting improvements in total QoL scores (d=0.61), independent living (d=0.8), mental health (d=0.67) and coping (d=0.76) dimensions for 17 young people (aged 14–25 years) with early psychosis.25 However, the effectiveness and cost-effectiveness of AEP services for improving QoL in people with SMI remains unclear. Therefore, the overarching aim of this study is to evaluate the effectiveness, cost-effectiveness and implementation process of an AEP service implemented within routine mental health care settings.
Materials and Methods
Study Design and Aims
The MOVEMENT study (“iMproving quality Of life in people with seVEre MENTal illness”) is a non-randomised effectiveness trial evaluating implementation of an AEP service as an adjunct to mental healthcare across public mental health services and non-government organizations (NGOs). The primary aim is to evaluate the effectiveness of the AEP service for improving QoL in people with SMI by comparing those who accept the service with those who decline. A secondary aim is to assess the cost-effectiveness of the service. Tertiary aims are to evaluate the implementation process, including reasons for recruitment and attrition rates, reasons for accepting or declining the AEP service, and experiences of staff and participants. It is acknowledged that a cluster randomised trial would be a more robust design to address the study aims; however, a non-randomised design was chosen to support evaluation of the implementation of the AEP service within trial resource restraints.
Patient and Public Involvement
This project was developed with the support and input of a broad collaboration of service providers and mental health sector leaders. Partner organizations include NGOs: Communify Queensland, Stride, Neami National, Richmond Fellowship Queensland; public hospital and health services (HHSs): Metro South Addictions and Mental Health Service, Metro North Mental Health Service; Primary Health Networks (PHNs): Brisbane South and Brisbane North PHNs; and Psychosis Australia, a national advocacy body in the mental health and research sector.
The research question and the intervention content were developed based on community programs developed collaboratively with people with lived experience of mental illness. These programs have been implemented and iteratively improved based on participant feedback since 2015. Representatives from the partner organizations, including people with lived experience of mental illness, will form a Steering Committee overseeing the study’s implementation. The results of this study will be disseminated to participants through presentations at consumer and community forums.
Setting and Participants
Participants will be recruited from community and residential rehabilitation services of partnering HHSs and NGOs in Brisbane, Australia. These services provide specialist treatment for approximately two million residents of a catchment encompassing inner city, suburban, and regional areas. The study will be implemented at five sites corresponding with areas serviced by relevant teams within partner organizations. The study will be promoted across team meetings, and staff will be asked to refer interested individuals. Individuals will be eligible if they are current consumers of mental health services for people with SMI provided by partnering organizations, aged 18–65 years, sufficiently fluent in English to complete consent and study procedures, and willing to provide consent to study participation.
Participants will be informed that study participation requires them to complete assessments at three timepoints, each three-months apart, and they will be offered a $50 gift card for completing each assessment session. They will also be informed that they can access an optional exercise program as part of their involvement in the study, and data collected will be used to evaluate the effectiveness of the program. After completing baseline assessments, participants will be asked if they would like to participate in the AEP service. Accepting or declining the AEP service will not impact their involvement in the study.
If they agree, an appointment will be made with the AEP at the community exercise venue for an induction and initial assessment. The initial assessment will involve medical screening using the Adult Pre-exercise Screening System (APSS);26 participants will be unable to participate in the exercise service if contraindicating factors are identified as per the American College of Sports Medicine absolute contraindications to exercise (9th edition, page 53); however, this will not exclude them from remaining in the study and completing follow-up assessments. The anticipated participant flow diagram is provided in Figure 1. Assumptions for the flow diagram are based on pilot community implementation which indicates roughly 50% completion rates; however, it is acknowledged that the final recruitment and completion rates may differ.
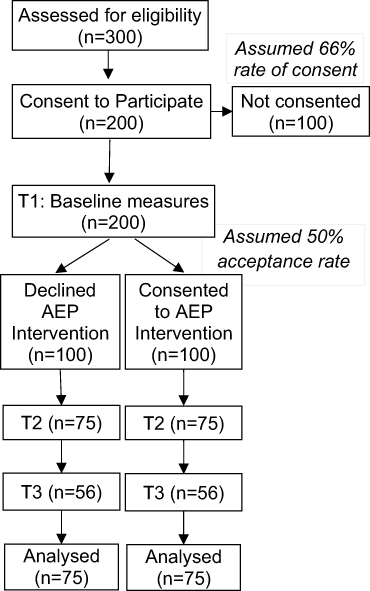 |
Figure 1 Anticipated participant flow diagram. A total of 150 participants with at least two timepoints are needed to adequately power primary analyses. Accounting for a dropout rate of 25% and assumed rate of declining vs accepting the Accredited Exercise Physiologist (AEP) service of 50%, we anticipate recruiting 200 participants. |
Exercise Service Structure
The exercise service will involve an AEP working with participants according to their scope of practice.27 Participants will be asked to complete at least one group-based exercise session/week at a community gym in groups of up to 10 participants, involving 60-minutes of exercise in the gym and a 60-minute health literacy session covering a range of topics. The AEP will engage participants in individual goal setting, and exercise prescriptions will be tailored to individual preferences and abilities and include a variety of aerobic and resistance exercises and physically active recreation (eg, sports, active groups). Participants will have access to the AEP service for six months, and exercise sessions will be delivered in blocks (10–12 weeks) separated by interim assessments. Participants will be sent weekly text message reminders about the group session times, with phone follow-up if sessions are missed without explanation. There will be no restrictions on participating in other therapies or programs outside the intervention.
Data Collection
The schedule of assessments is provided in Table 1. Assessments include 12 self-report questionnaires with a total of 87 items, and physical measures described in Table 2. Questionnaires will cover the following domains: quality of life, psychological distress, health service utilisation, resource use, sense of belonging, self-efficacy, health literacy, social connection, alcohol intake, nutritional intake, physical activity, and sleep quality. Physical health assessments will include blood pressure and waist circumference. These outcomes were chosen because of their potential influence on QoL, and usefulness in describing what psychosocial and lifestyle factors may have changed over the course of the 6-month intervention. Measures were chosen based on their validity and brevity for minimising participant burden. Initial piloting indicates that these measures are generally completed within a 60-minute assessment session.
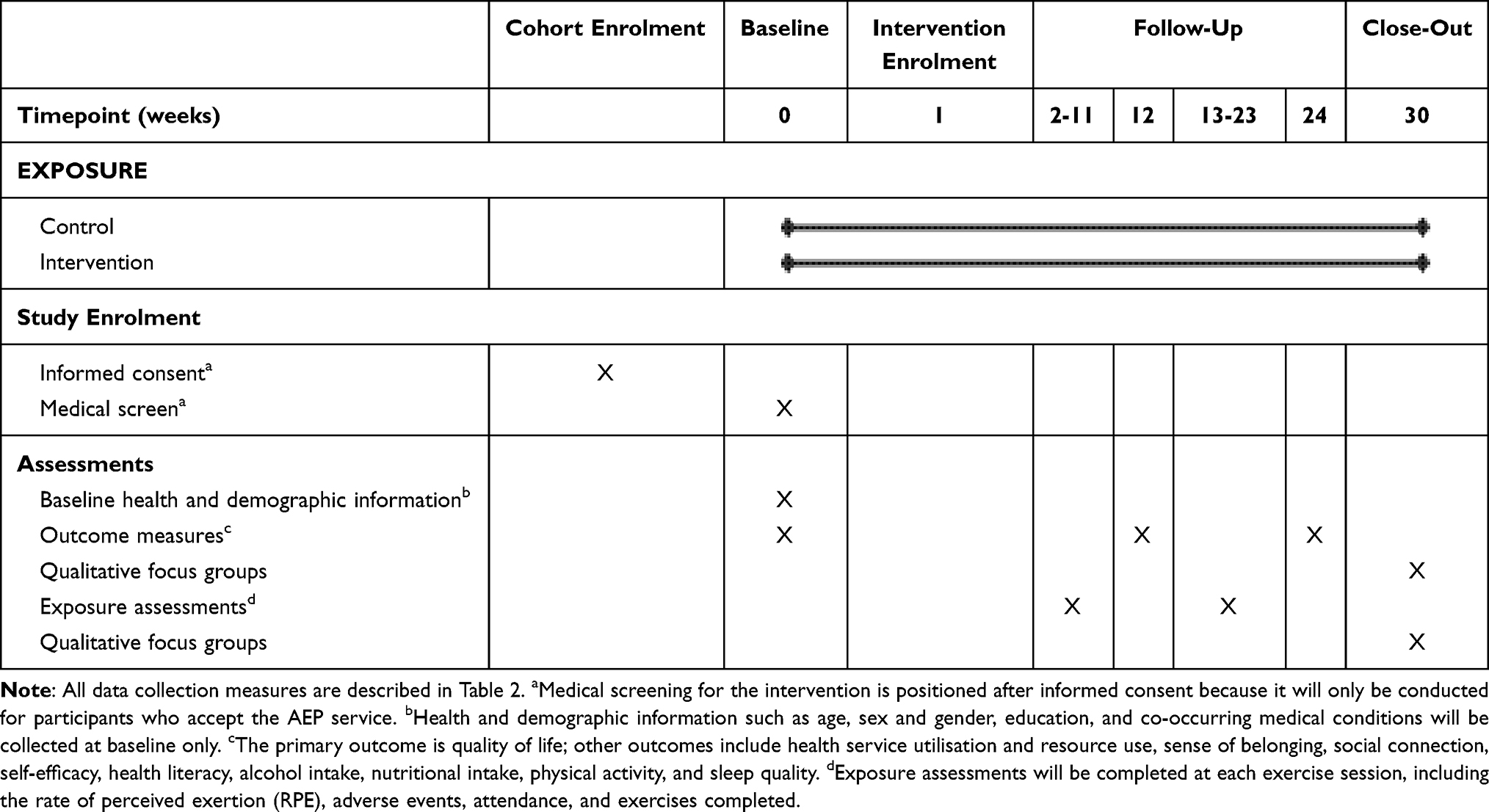 |
Table 1 SPIRIT Figure for Schedule of Assessments |
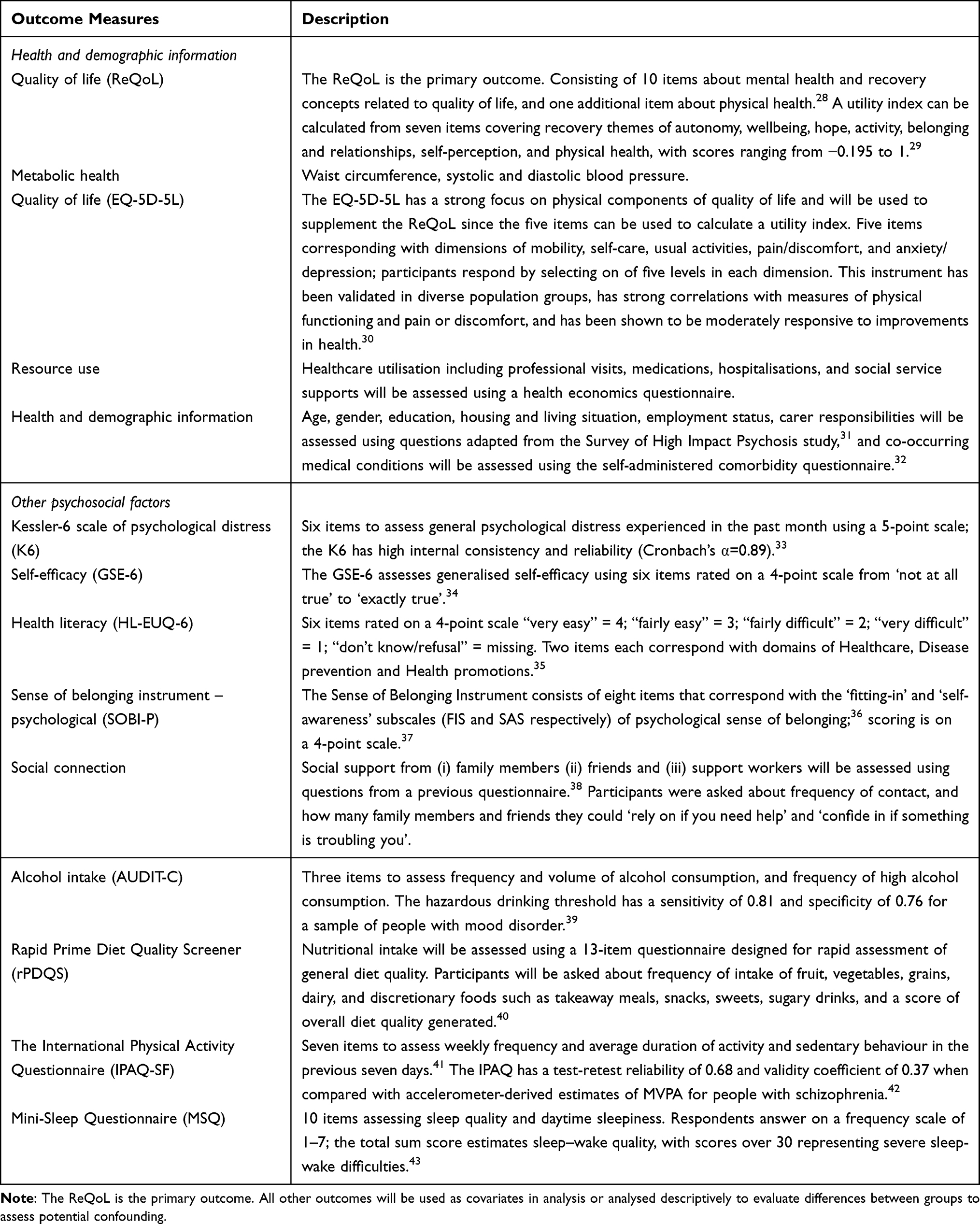 |
Table 2 Prospective Data Collection |
Participants may elect to complete self-report questionnaires online; however, it is anticipated the participants will complete most assessments with the assistance of researchers in-person. Participants will be offered $50AUD gift cards for completing assessments at each timepoint. Additional data collection for participants of the AEP service will include medical screening, attendance at the exercise sessions, rate of perceived exertion and exercise completed each session, adverse events, and qualitative interviews about their experiences with the service.
Adverse Event Reporting
Participants will be asked to report pain or injuries from the previous week at each session; any adverse events will be reported to the Steering Committee and Metro South Health Human Research Ethics Committee. Participants experiencing pain related to exercise, pre-existing conditions, or unrelated injury may be required to discontinue the intervention until medical clearance can be obtained. Hospital re-admissions for psychiatric reasons will also be reported, and participants permitted to re-enter the intervention when they return to community or residential mental healthcare settings.
Data Management and Analyses
Questionnaires will be administered electronically using the online survey platform REDcap; data will be exported into SPSS version 23 (SPSS Inc, Chicago, Illinois) and STATA 15 (College Station, TX: StataCorp LLC) for analysis.
Primary Analysis
Linear mixed-effects models for repeated measures (repeated measurements nested within individuals) will be used to compare outcomes between participants who consent to the exercise intervention with those who decline. The most suitable auto-regressive covariance structure will be tested and implemented to account for relations of measurements over time. We will adjust for potential confounders, such as implementation site, changes to medications, other treatments (eg, Allied Health), and baseline health status. Analysis will be conducted on the intention-to-treat basis (ITT), and missing data will be handled using multiple imputation with chained equations where appropriate. Because participants self-select to the intervention, potential selection bias and confounding will be approached descriptively by examining standardised mean differences and confidence intervals between groups on psychosocial outcomes, and by comparing participant characteristics with a random sample of de-identified routine care data from the whole service cohort.
Economic Evaluation
All relevant costs and participant health outcomes will be compared in a cost-utility analysis using both health sector and partial societal perspectives. Costs will include the exercise intervention plus additional health and social support resource use data. Total incremental costs will be compared between each group using generalised linear models (GLMs). The total quality-adjusted life years (QALYs) occurring in each group will be derived from health utility scores using area-under-the-curve methods. Incremental QALYs between groups will, in turn, be analysed using mixed-effects (eg, linear, gamma family, log link) GLMs. The “incremental cost per QALY gain” ratio will be estimated by dividing the difference in mean costs between participants who accept the exercise service vs those who decline against the corresponding difference in mean outcomes. Uncertainty and sensitivity analyses will be conducted to evaluate the impact of parameter uncertainty around the cost-effectiveness findings.
Tertiary Aims
The Consolidated Framework for Implementation Research (CFIR) will inform evaluation of the implementation process,44 and the Behaviour Change Wheel and COM-B framework will inform the evaluation of the implementation and participant experiences.45 CFIR will be used to examine barriers and enablers to implementation in five domains (inner and outer setting, people involved, implementation process, and intervention content). COM-B will be used to frame qualitative data from participants about their capability, opportunity and motivation to engage in the AEP service.
To ensure that a range of views are represented, participants from three different experience groups (those who: (i) declined the exercise service; (ii) accepted but did not continue; and (iii) had high attendance to the sessions) will be invited to interviews. A framework approach will be employed for qualitative analysis which provides a structure for coding and categorising data.46 Both deductive and inductive logic will be used to reduce and synthesise data using COM-B as a frame; coding will be conducted by one researcher. Recruitment and participation rates and the resourcing required to conduct the study will be examined.
Sample Size
Previous research has estimated mean baseline ReQoL scores of 21.99 (SD=10.26) for a sample of people with mental health difficulties, and that a change of five points or more on the ReQoL is reliable for detecting clinical changes.28 Using Power Analysis and Sample Size software (PASS) 2020 for a repeated measures design with a first-order autoregressive covariance structure, we estimate that 75 participants would be required in each condition to provide at least 90% power to detect a clinically significant increase of five points on the ReQoL questionnaire, assuming a correlation between three time points of 0.6 and a statistical significance level set at 5%. Accounting for dropout, we will aim to recruit a total of 200 participants over two-years.
Ethics and Dissemination
The authors assert that all procedures contributing to this work comply with the ethical standards of the relevant national and institutional committees on human experimentation and with the Helsinki Declaration of 1975, as revised in 2013. All procedures involving human subjects/patients are approved by the Metro South Health Human Research Ethics Committee (HREC/2024/QMS/109698). The trial will be subject to random auditing by the HREC independently from the researchers. Results from the trial will be available to participants, published in a peer-reviewed journal, and presented at conferences, community and consumer forums and hospital grand rounds. The final dataset will be deidentified and published on an open access repository; confidentiality will be protected in all dissemination activities. The trial is registered under the Australian and New Zealand Clinical Trial Registry (ACTRN12624001148561). Any protocol modifications will be reported to the HREC and ACTRN and reported in the subsequent publication.
Discussion
A pragmatic approach has been taken in the design: inclusion criteria are broad and specific to services that provide care for people with SMI to enhance generalisability to similar service settings. To further enhance applicability to routine service settings, participation in the study is not contingent on involvement with the AEP service. Describing potential differences between participants who adopt or decline the AEP service is pertinent to informing implementation in routine care. For example, the difference in outcomes between participants who accessed the service and those who could not attend because of participation barriers may elucidate how the implementation could be adapted to improve the accessibility of exercise among people living with SMI.
However, because participants will not be randomly allocated to conditions, the comparison group must be drawn from participants who decline involvement with the AEP service. It is acknowledged that participant groups (ie, control and intervention) will likely differ on important characteristics, and unmeasured confounding may compromise internal validity. Representativeness of the sample will be evaluated by comparing demographic information with a random selection of routine care data from the whole service cohort.
We anticipate that these findings will inform future implementation of AEP services within mental healthcare settings, and how AEP interventions could be designed to address the barriers to engagement experienced by people with SMI. Because of differences in healthcare systems, we anticipate that the findings will be most relevant to Australian mental healthcare settings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the protocol conception or study design; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is funded by a grant from the Medical Research Futures Fund (App ID:2023060). This work is also funded by contribution from the Brisbane North Primary Health Network.
Disclosure
Dr Nicole Korman reports financial support to convene an educational conference from Otsuka, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Morgan V, McGrath J, Jablensky A, et al. Psychosis prevalence and physical, metabolic and cognitive co-morbidity: data from the second Australian national survey of psychosis. Psychol Med. 2014;44(10):2163–2176. doi:10.1017/S0033291713002973
2. Firth J, Siddiqi N, Koyanagi A, et al. The Lancet Psychiatry Commission: a blueprint for protecting physical health in people with mental illness. Lancet Psychiatry. 2019;6(8):675–712. doi:10.1016/S2215-0366(19)30132-4
3. Barnes AL, Murphy ME, Fowler CA, Rempfer MV. Health-related quality of life and overall life satisfaction in people with serious mental illness. Schizophr Res Treatment. 2012;2012:1–6. doi:10.1155/2012/245103
4. Firth J, Stubbs B, Rosenbaum S, et al. Aerobic exercise improves cognitive functioning in people with schizophrenia: a systematic review and meta-analysis. Schizophr Bull. 2017;43(3):546–556. doi:10.1093/schbul/sbw115
5. Rosenbaum S, Tiedemann A, Sherrington C, Curtis J, Ward PB. Physical activity interventions for people with mental illness: a systematic review and meta-analysis. J Clin Psychiatr. 2014;75.
6. Firth J, Solmi M, Wootton RE, et al. A meta‐review of “lifestyle psychiatry”: the role of exercise, smoking, diet and sleep in the prevention and treatment of mental disorders. World Psychiatry. 2020;19(3):360–380. doi:10.1002/wps.20773
7. Stubbs B, Firth J, Berry A, et al. How much physical activity do people with schizophrenia engage in? A systematic review, comparative meta-analysis and meta-regression. Schizophr Res. 2016;176(2–3):431–440. doi:10.1016/j.schres.2016.05.017
8. Vancampfort D, Rosenbaum S, Schuch FB, Ward PB, Probst M, Stubbs B. Prevalence and predictors of treatment dropout from physical activity interventions in schizophrenia: a meta-analysis. Gen Hosp Psychiatry. 2016;39:15–23. doi:10.1016/j.genhosppsych.2015.11.008
9. Korman N, Stanton R, Vecchio A, et al. The effect of exercise on global, social, daily living and occupational functioning in people living with schizophrenia: a systematic review and meta-analysis. Schizophr Res. 2023;256:98–111. doi:10.1016/j.schres.2023.04.012
10. Samaras K, Shiers D, Chen R, Holt RI, Curtis J. Keeping the body in mind: scientific effort in advocating the best outcomes for people living with severe mental illness. Front Endocrinol. 2021;12:831933. doi:10.3389/fendo.2021.831933
11. Curtis J, Newall HD, Samaras K. The heart of the matter: cardiometabolic care in youth with psychosis. Early Interv Psychiatry. 2012;6(3):347–353. doi:10.1111/j.1751-7893.2011.00315.x
12. Vancampfort D, Rosenbaum S, Schuch F, et al. cardiorespiratory fitness in severe mental illness: a systematic review and meta-analysis. Sports Med. 2017;47(2):343–352. doi:10.1007/s40279-016-0574-1
13. Fibbins H, Lederman O, Morell R, Furzer B, Wright K, Stanton R. Incorporating exercise professionals in mental health settings: an Australian perspective. J Clin Exerc Physiol. 2019;8(1):21–25. doi:10.31189/2165-6193-8.1.21
14. Lederman O, Grainger K, Stanton R, et al. Consensus statement on the role of accredited exercise physiologists within the treatment of mental disorders: a guide for mental health professionals. Australas Psychiatry. 2016;24(4):347–351. doi:10.1177/1039856216632400
15. Morgan AJ, Parker AG, Alvarez-Jimenez M, Jorm AF. Exercise and mental health: an exercise and sports science Australia commissioned review. J Exercise Physiol Online. 2013;16(4).
16. Austin F, Wright KE, Jackson B, Budden T, McMahen C, Furzer BJ. Experiences of exercise services for individuals with severe mental illness: a qualitative approach. Psychol Sport Exercise. 2025;78:102826. doi:10.1016/j.psychsport.2025.102826
17. Fibbins H, Ward PB, Stanton R, et al. Embedding an exercise professional within an inpatient mental health service: a qualitative study. Ment Health Phys Act. 2019;17:100300. doi:10.1016/j.mhpa.2019.100300
18. Curtis J, Watkins A, Rosenbaum S, et al. Evaluating an individualized lifestyle and life skills intervention to prevent antipsychotic‐induced weight gain in first‐episode psychosis. Early Interv Psychiatry. 2016;10(3):267–276. doi:10.1111/eip.12230
19. Curtis J, Teasdale SB, Morell R, et al. Implementation of a lifestyle and life‐skills intervention to prevent weight‐gain and cardiometabolic abnormalities in young people with first‐episode psychosis as part of routine care: the keeping the body in mind program. Early Interv Psychiatry. 2024;18:731–738. doi:10.1111/eip.13508
20. Seymour J, Pratt G, Patterson S, et al. Changes in self-determined motivation for exercise in people with mental illness participating in a community-based exercise service in Australia. Health Soc Care Community. 2021;30:e1611–e1624. doi:10.1111/hsc.13588
21. Korman N, Fox H, Skinner T, et al. Feasibility and acceptability of a student-led lifestyle (Diet and Exercise) Intervention Within a Residential rehabilitation setting for people with severe mental illness, GO HEART (Group Occupation, Health, Exercise And Rehabilitation Treatment). Front Psychiatry. 2020;11:319. doi:10.3389/fpsyt.2020.00319
22. Furzer BJ, Wright KE, Edoo A, Maiorana A. Move your mind: embedding accredited exercise physiology services within a hospital-based mental health service. Australas Psychiatry. 2021;29(1):52–56. doi:10.1177/1039856220943030
23. Fibbins H, Edwards L, Morell R, Lederman O, Ward P, Curtis J. Implementing an exercise physiology clinic for consumers within a community mental health service: a real-world evaluation. Front Psychiatry. 2021;12:791125. doi:10.3389/fpsyt.2021.791125
24. Pearce M, Foote L, Brown E, O’donoghue B. Evaluation of an exercise physiology service in a youth mental health service. Ir J Psychol Med. 2021;38(1):56–61. doi:10.1017/ipm.2020.91
25. Lederman O, Ward PB, Rosenbaum S, et al. Stepping up early treatment for help-seeking youth with at-risk mental states: feasibility and acceptability of a real-world exercise program. Early Interv Psychiatry. 2020;14(4):450–462. doi:10.1111/eip.12871
26. Norton K, Coombes J, Hobson-Powell A, et al. Adult Pre-Exercise Screening System (APSS). Exercise and Sports Science Australia; 2012.
27. ESSA. Scopes of practice. exercise and sports science Australia. Available from: https://www.essa.org.au/Public/Public/Professional_Standards/ESSA_Scope_of_Practice_documents.aspx.
28. Keetharuth AD, Brazier J, Connell J, et al. Recovering Quality of Life (ReQoL): a new generic self-reported outcome measure for use with people experiencing mental health difficulties. Br J Psychiatry. 2018;212(1):42–49. doi:10.1192/bjp.2017.10
29. Keetharuth AD, Rowen D, Bjorner JB, Brazier J. Estimating a preference-based index for mental health from the recovering quality of life measure: valuation of recovering quality of life utility index. Value Health. 2021;24(2):281–290. doi:10.1016/j.jval.2020.10.012
30. Feng Y-S, Kohlmann T, Janssen MF, Buchholz I. Psychometric properties of the EQ-5D-5L: a systematic review of the literature. Qual Life Res. 2021;30:647–673. doi:10.1007/s11136-020-02688-y
31. Morgan VA, Waterreus A, Jablensky A, et al. People living with psychotic illness 2010. Report on the second Australian national survey. In: Department of Health and Ageing. Canberra; 2011.
32. Sangha O, Stucki G, Liang MH, Fossel AH, Katz JN. The Self‐Administered Comorbidity Questionnaire: a new method to assess comorbidity for clinical and health services research. Arthritis Care Res. 2003;49(2):156–163. doi:10.1002/art.10993
33. Kessler RC, Barker PR, Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. 2003;60(2):184. doi:10.1001/archpsyc.60.2.184
34. Romppel M, Herrmann-Lingen C, Wachter R, et al. A short form of the General Self-Efficacy Scale (GSE-6): development, psychometric properties and validity in an intercultural non-clinical sample and a sample of patients at risk for heart failure. Psychosoc Med. 2013;10.
35. Lorini C, Lastrucci V, Vettori V, et al. Measuring health literacy in Italy: a validation study of the HLS-EU-Q16 and of the HLS-EU-Q6 in Italian language, conducted in Florence and its surroundings. Ann Ist Super Sanita. 2019;55(1):10–18. doi:10.4415/ANN_19_01_04
36. Allen K-A, Arslan G, Craig H, Arefi S, Yaghoobzadeh A, Sharif Nia H. The psychometric evaluation of the sense of belonging instrument (SOBI) with Iranian older adults. BMC Geriatr. 2021;21:1–8. doi:10.1186/s12877-021-02115-y
37. Hagerty BM, Patusky K. Developing a measure of sense of belonging. Nurs Res. 1995;44(1):9–13. doi:10.1097/00006199-199501000-00003
38. Saha S, Scott J, Varghese D, McGrath J. Social support and delusional-like experiences: a nationwide population-based study. Epidemiol Psychiatr Sci. 2012;21(2):203–212. doi:10.1017/S2045796011000862
39. Reinert DF, Allen JP. The alcohol use disorders identification test: an update of research findings. Alcohol Clin Exp Res. 2007;31(2):185–199. doi:10.1111/j.1530-0277.2006.00295.x
40. Kronsteiner-Gicevic S, Tello M, Lincoln LE, et al. Validation of the rapid prime diet quality score screener (rPDQS), a brief dietary assessment tool with simple traffic light scoring. J Acad Nutr Diet. 2023;123(11):1541–1554.e1547. doi:10.1016/j.jand.2023.05.023
41. Craig CL, Marshall AL, Sjöström M, et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003;35(8):1381–1395. doi:10.1249/01.MSS.0000078924.61453.FB
42. Faulkner G, Cohn T, Remington G. Validation of a physical activity assessment tool for individuals with schizophrenia. Schizophr Res. 2006;82(2–3):225–231. doi:10.1016/j.schres.2005.10.020
43. Natale V, Fabbri M, Tonetti L, Martoni M. Psychometric goodness of the mini sleep questionnaire. Psychiatry Clin Neurosci. 2014;68(7):568–573. doi:10.1111/pcn.12161
44. Damschroder LJ, Reardon CM, Widerquist MAO, Lowery J. The updated Consolidated Framework for Implementation Research based on user feedback. Implement Sci. 2022;17(1):1–16. doi:10.1186/s13012-022-01245-0
45. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implement Sci. 2011;6:1–12. doi:10.1186/1748-5908-6-42
46. Ritchie J, Spencer L. Qualitative data analysis for applied policy research. Qualitative Res Companion. 2002;573:305–329.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Is It Important to Increase Physical Activity Among University Students During the Second-Wave COVID-19 Pandemic in Asian Countries? A Cross-Sectional Study of the Knowledge, Attitudes, and Practices in Asian Countries

Sari DK, Mani S, Fadli M, Ihksan R, Machrina Y, Arrasyid NK, Siregar KB, Sunarno A
Journal of Multidisciplinary Healthcare 2022, 15:1559-1571
Published Date: 21 July 2022
Influence of Coaching on Effectiveness, Participation, and Safety of an Exercise Program for Postmenopausal Women with Osteoporosis: A Randomized Trial
Bragonzoni L, Barone G, Benvenuti F, Ripamonti C, Lisi L, Benedetti MG, Marini S, Dallolio L, Maietta Latessa P, Zinno R, Audino G, Kemmler W, Pinelli E
Clinical Interventions in Aging 2023, 18:143-155
Published Date: 5 February 2023
Obstacles to the Early Diagnosis and Management of Sarcopenia: Current Perspectives
Ooi H, Welch C
Clinical Interventions in Aging 2024, 19:323-332
Published Date: 20 February 2024