")
Back to Journals » Journal of Pain Research » Volume 18
Analgesic and Hemodynamic Effects of Dexmedetomidine–Ketamine vs Fentanyl–Ketamine in Healthy Volunteers: A Randomized Trial
Authors Green M, Hayley AC , Downey LA, Keane M, Kenneally ME, Chakravarthy K, Shehabi Y
Received 21 January 2025
Accepted for publication 13 May 2025
Published 16 May 2025 Volume 2025:18 Pages 2483—2496
DOI https://doi.org/10.2147/JPR.S514277
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Dawood Sayed
Maja Green,1,2 Amie C Hayley,3,4 Luke A Downey,3,4 Michael Keane,4,5 Michaela Elise Kenneally,6 Krishnan Chakravarthy,1,2 Yahya Shehabi5,7
1NXTSTIM, Department of Pain Medicine, San Diego, CA, USA; 2Soalris Research Institute, Temecula, CA, USA; 3Institute for Breathing and Sleep, Austin Hospital, Melbourne, Victoria, Australia; 4Centre for Human Psychopharmacology, Swinburne University of Technology, Hawthorn, Australia; 5Critical Care and Anaesthesia, School of Clinical Sciences, Monash University, Melbourne, Victoria, Australia; 6Forensic Science, Adelaide, South Australia, Australia; 7Clinical School of Medicine, University of New South Wales, Sydney, New South Wales, Australia
Correspondence: Maja Green, NXTSTIM Inc., Department of Pain Medicine, San Diego, CA, 92130, USA, Email [email protected]
Background: Dexmedetomidine is an α 2-agonist sedative with opioid-sparing properties, is limited by dose-dependent hypotension and bradycardia. Ketamine, an NMDA receptor antagonist, has sympathomimetic effects and may attenuate these cardiovascular effects while contributing analgesia. Whether low-dose ketamine can stabilize dexmedetomidine-induced hemodynamic changes and provide comparable analgesia to an opioid-based regimen is uncertain.
Methods: In this open-label trial, we enrolled 41 healthy volunteers aged 18 to 45 years. All participants received a ketamine infusion (0.3 mg/kg bolus, then 0.15 mg/kg/hour for 3 hours). At 90 minutes, participants were randomized to receive either dexmedetomidine (0.7 μg/kg/hour for 90 minutes, KET/DEX group) or fentanyl (three 25 μg boluses, KET/FENT group). The primary outcomes were change in blood pressure and pain tolerance (measured by pressure algometry). Secondary outcomes included heart rate, subjective mood and sedation, and adverse events. Data were analyzed using mixed-effects models and Fisher’s exact tests.
Results: Of 41 randomized participants, 39 completed the protocol (KET/DEX, 19; KET/FENT, 20). KET/DEX resulted in greater reductions in systolic blood pressure (mean decrease 35– 40 mm Hg; ~25– 30%) compared to KET/FENT (mean change minimal; between-group P< 0.001). Heart rate declined modestly with KET/DEX but did not differ significantly between groups. Both regimens increased pain tolerance to a similar degree (mean threshold rise ~30– 50 kPa; between-group P=0.80). Participants in the KET/DEX group reported greater sedation and transient negative mood effects (eg, disinterest), while KET/FENT was associated with mild nausea in a minority. Clinically significant hypotension occurred in 4 participants (21%) in the KET/DEX group and in none of the KET/FENT group (P=0.047). All events were transient and responsive to fluid boluses. No respiratory depression occurred in either group.
Conclusion: Ketamine plus dexmedetomidine produced analgesia equivalent to ketamine plus fentanyl but with more pronounced hypotension and deeper sedation. The hemodynamic effects of dexmedetomidine were not fully offset by low-dose ketamine. These findings suggest that while ketamine–dexmedetomidine may offer an opioid-sparing alternative, careful dose selection and monitoring are required to ensure tolerability. (Funded by Monash University and Monash Health; ACTRN12617000787381).
Clinical Trial Number and Registry Url: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=372916.
Keywords: ketamine, dexmedetomidine, fentanyl, sedation, haemodynamic changes
Introduction
Opioid analgesics remain central to acute pain management but are increasingly scrutinized due to their adverse effects and potential for long-term dependence. Even short-term perioperative opioid use in previously opioid-naïve patients has been associated with prolonged use in 6 to 10% of cases.1–4 In both surgical and critical care settings, opioid exposure is linked to respiratory depression, nausea, constipation, and paradoxical opioid-induced hyperalgesia. These limitations have driven interest in opioid-sparing strategies that incorporate non-opioid analgesics with distinct mechanisms of action. Ketamine and dexmedetomidine have emerged as attractive components of multimodal analgesia. Ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, reduces central sensitization and provides dose-dependent analgesia.1,2 It also exerts sympathomimetic effects through norepinephrine reuptake inhibition, often increasing blood pressure and heart rate. However, at higher doses, ketamine may induce dissociative or psychotomimetic symptoms. Dexmedetomidine, a selective α2-adrenoceptor agonist, produces sedation and analgesia by inhibiting central sympathetic outflow. Unlike opioids, dexmedetomidine does not cause respiratory depression and can reduce anesthetic and opioid requirements, but it is associated with bradycardia and hypotension due to its sympatholytic action.5–8 Theoretically, combining ketamine and dexmedetomidine may yield synergistic benefits: ketamine’s sympathetic stimulation could offset dexmedetomidine’s hemodynamic effects, while dexmedetomidine’s sedation may reduce ketamine-related psychotropic side effects.9 Such combinations have been used in perioperative protocols and intensive care sedation, with reports suggesting effective analgesia, opioid-sparing potential, and improved ventilator weaning times.10–12 However, the cardiovascular interactions of these drugs remain incompletely understood. In particular, it is unclear whether low-dose ketamine can reliably prevent dexmedetomidine-induced hypotension and bradycardia. Much of the current evidence comes from heterogeneous patient populations, where surgical stress and comorbidities may confound the pharmacodynamic profile.13,14
To isolate the direct pharmacodynamic effects of ketamine and dexmedetomidine, a randomized trial was conducted in healthy volunteers comparing a ketamine–dexmedetomidine regimen with a ketamine–fentanyl regimen, the latter serving as a standard opioid-based comparator. Fentanyl was selected as the comparator adjunct because opioid–ketamine combinations are widely used in clinical practice and provide a well-established reference for multimodal analgesia. This approach enabled comparison of the ketamine–dexmedetomidine regimen against a standard-of-care framework. A dexmedetomidine-only or placebo arm was not included, as neither would offer a clinically meaningful comparator: dexmedetomidine lacks the analgesic potency of ketamine, and placebo would not provide active sedation or analgesia, limiting interpretability of the findings.
The primary objective was to evaluate the hemodynamic consequences of co-administration, with additional assessment of analgesic efficacy, sedation, mood alterations, and adverse events. It was anticipated that low-dose ketamine would provide only partial attenuation of dexmedetomidine’s cardiovascular effects, while offering analgesia comparable to that of the ketamine–fentanyl combination. Data from this controlled model may inform safer dosing practices and guide the clinical application of ketamine–dexmedetomidine protocols in opioid-sparing analgesia.
Notably, this investigation was conducted in healthy volunteers. Studying drug effects in a healthy population permits isolation of the direct pharmacodynamic response to the ketamine–dexmedetomidine combination, without confounding factors such as surgical stress, general anesthesia, or critical illness. This controlled design provides a clear safety and physiological profile that can inform subsequent studies in clinical settings. While our ultimate aim is to improve real-world pain management strategies, this model offers foundational insight necessary to support future patient-based research.
Methods
Study Design and Participants
This single-center, open-label, randomized trial was conducted at the Clinical Trials Centre of the Monash Health Translation Precinct in Melbourne, Australia. The study protocol was approved by the Monash Health Human Research Ethics Committee (HREC/17/MonH/230) and registered with the Australian New Zealand Clinical Trials Registry (ACTRN12617000787381). This study adhered to the Declaration of Helsinki. Written informed consent was obtained from all participants before enrollment.
Eligible participants were healthy adults aged 18 to 45 years, with no history of cardiovascular, respiratory, neurologic, or psychiatric conditions, substance use disorder, or known hypersensitivity to ketamine, dexmedetomidine, or fentanyl. To minimize risk to healthy volunteers, the upper age limit for participant eligibility was lowered from 45 to 40 years prior to recruitment. To minimize external influences on physiological parameters, participants were instructed to abstain from alcohol, caffeine, and non-prescribed medications for at least 48 hours prior to the study visit. A total of 41 participants were enrolled and randomly assigned in a 1:1 ratio to receive either ketamine with dexmedetomidine (KET/DEX) or ketamine with fentanyl (KET/FENT). Randomization was stratified by sex and performed using permuted blocks of four. Due to the sedative profile of dexmedetomidine, blinding of participants and investigators was not feasible; however, primary outcomes, including vital signs and pain thresholds, were assessed using objective measures to minimize bias.
Two participants were excluded prior to analysis: one in the KET/FENT group for protocol nonadherence and one in the KET/DEX group due to detectable pre-study ketamine use. Both were replaced to maintain target sample size. The final analysis included 39 participants; 19 in the KET/DEX group and 20 in the KET/FENT group, all of whom completed the intervention protocol. A CONSORT diagram depicting participant flow is available in Supplementary Figure 1.
Baseline demographic and clinical characteristics were similar between the two groups (Table 1). The mean age of the study population was 28.4 years (±5.8), with 74% identifying as male and a mean body weight of 78 kg (±16). No significant differences were observed in resting blood pressure or heart rate at baseline.
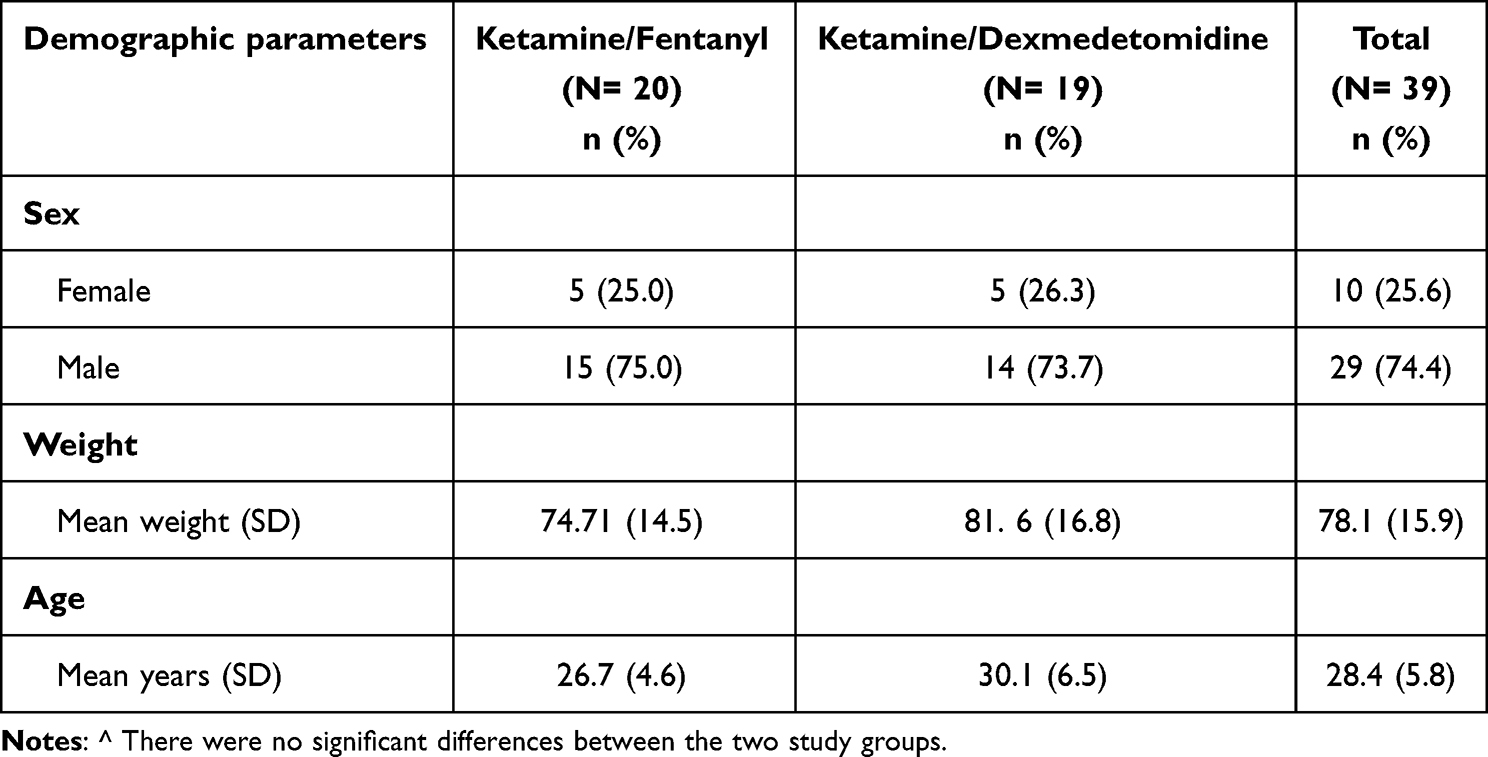 |
Table 1 Demographic and Lifestyle Characteristics According to Study Group (Ketamine/Dexmedetomidine and Ketamine/Fentanyl) and for the Total Sample^ |
Interventions and Study Procedure
All experimental sessions were conducted in a controlled clinical research unit under continuous monitoring. Upon arrival, an intravenous cannula was inserted for drug administration, and baseline assessments were performed. Participants remained semirecumbent at a 45-degree angle for the duration of the study to ensure comfort and consistency in measurement conditions. Initial evaluations included recording of baseline vital signs, pressure pain threshold testing, and completion of mood assessments.
All participants received ketamine as a low-dose infusion. A loading dose of S(+)-ketamine (0.3 mg per kilogram of body weight) was administered intravenously over 2 to 3 minutes, followed by a continuous infusion at 0.15 mg/kg/hour for 3 hours. Ketamine was prepared in 0.9% saline (2 mg/mL concentration) and delivered via an infusion pump. The S(+) enantiomer was used, consistent with institutional formulary, and is referred to as “ketamine” throughout. The dosing regimen was selected to achieve subanesthetic, analgesic plasma levels while minimizing psychotropic effects, in accordance with prior clinical studies.
For the first 90 minutes of the infusion (ketamine-only phase), no additional medications were administered. At 90 minutes, participants entered the co-administration phase according to randomization.
- Ketamine–Dexmedetomidine Group (KET/DEX): A second intravenous line was inserted for dexmedetomidine delivery. The drug was infused at a rate of 0.7 µg/kg/hour over 90 minutes using a syringe pump, without a loading dose. The solution was prepared such that 1 mL/hour delivered 0.1 µg/kg/hour. The selected dose, considered moderate, was anticipated to produce measurable sympatholytic and sedative effects. No other medications or flushes were administered through this line during infusion.
- Ketamine–Fentanyl Group (KET/FENT): Participants received three intravenous fentanyl boluses (25 µg each) at 30-minute intervals, beginning at 90 minutes, in addition to the ongoing ketamine infusion. Fentanyl was diluted to a concentration of 25 µg/mL in normal saline and administered as 1 mL boluses, followed by a 10 mL saline flush. The total fentanyl dose (75 µg) was selected to reflect low-dose clinical practice, minimizing risk of respiratory or hemodynamic compromise in healthy volunteers.
Ketamine infusion continued throughout the 90-minute co-administration period in both groups. At the 3-hour mark, all study infusions were discontinued, and participants entered a monitored recovery phase.
Vital signs, including noninvasive systolic and diastolic blood pressure and heart rate, were recorded at baseline and every 30 minutes during the 3-hour infusion (ie, at 30, 60, and 90 minutes during ketamine-only administration and at 120, 150, and 180 minutes during co-administration). Following drug discontinuation, vital signs were recorded hourly for an additional 4 hours (ie, at 4, 5, 6, and 7 hours after study initiation). Continuous monitoring of oxygen saturation and respiratory rate was maintained throughout the study. No respiratory complications occurred. A physician and research nurse were present throughout the procedure to ensure participant safety and intervene as required.
Outcomes and Assessments
The co-primary outcomes were (1) change in systolic and diastolic blood pressure from baseline during ketamine–dexmedetomidine and ketamine–fentanyl administration, and (2) pain tolerance measured by pressure algometry during treatment. Key secondary outcomes included changes in heart rate, subjective pain ratings, sedation and mood effects, and the incidence of predefined adverse events, including hypotension, bradycardia, nausea, vomiting, and psychotropic symptoms.
Hemodynamic Measurements
Noninvasive systolic and diastolic blood pressure and heart rate were recorded at baseline and at 30-minute intervals throughout the 3-hour infusion period. Measurements continued hourly during the 4-hour post-infusion recovery phase to evaluate resolution of drug effects. The primary hemodynamic endpoint was the lowest systolic blood pressure (nadir) observed during the infusion, along with between-group differences at each time point. Hypotension was defined a priori as systolic blood pressure below 90 mm Hg or a reduction exceeding 30% from baseline. Bradycardia was defined as heart rate less than 50 beats per minute. If hypotension occurred, the protocol specified administration of 250 to 500 mL of intravenous normal saline, repeatable as needed. Persistent hypotension unresponsive to fluid resuscitation triggered preparedness for vasopressor use (phenylephrine or ephedrine). In cases of bradycardia with hemodynamic compromise (heart rate <45 beats per minute with symptoms or <40 beats per minute irrespective of symptoms), intravenous atropine was indicated. These thresholds were established prospectively to standardize management of adverse events.
Pain Tolerance and Analgesic Effect
Mechanical pain tolerance was assessed using a handheld digital pressure algometer applied to the nondominant forearm. The algometer probe (1 cm² contact surface) was applied perpendicularly to the muscle surface, and pressure was increased gradually until the participant indicated the onset of pain. The peak pressure at which pain was first perceived (in kilopascals, kPa) was recorded. This threshold was measured at four time points: at baseline, at 90 minutes (prior to randomization), at 180 minutes (end of treatment), and again 2 hours after drug discontinuation. Each test consisted of three trials, and the highest value was recorded as the pain threshold for that session. Subjective pain intensity was evaluated using a 100-mm visual analog scale (VAS) immediately following each algometer test, with anchors ranging from “no pain” (0 mm) to “worst imaginable pain” (100 mm). Because participants did not have ongoing clinical pain, these measures represented induced pressure pain only. Analgesic effect was defined by increases in pain pressure threshold and/or reductions in VAS pain ratings during treatment relative to baseline.
Sedation and Mood
Subjective mood and sedation effects were evaluated using validated 100-mm VAS items adapted from the Cambridge Neuropsychological Test Automated Battery (CANTAB). Each VAS presented bipolar adjectives (eg, “alert–drowsy”, “calm–agitated”, “content–discontent”), with participants marking their perceived state. The domains assessed included calmness, relaxation, energy level, openness, amicability, and engagement. Assessments were conducted at baseline, at 90 minutes (prior to randomization), at 180 minutes (end of infusion), and at 2 hours post-treatment. Each scale was scored in millimeters from the negative end, with higher values reflecting the more positive affective state (except for inverted domains such as drowsiness). Sedation was inferred primarily from low energy ratings and increased scores on “drowsiness.” Objective sedation scales, such as the Richmond Agitation–Sedation Scale (RASS), were not used in this study, which is acknowledged as a limitation. All sedation and mood measures were self-reported, and no behavioral or EEG-based assessments were performed.
Cognitive and Psychomotor Testing
As part of a broader trial protocol, participants completed computerized neurocognitive assessments and a simulated driving task at baseline and during the treatment period. These data were collected for a separate planned analysis and are not reported in the present study. Cognitive tasks were scheduled to avoid interfering with core hemodynamic and pain assessments; for example, testing occurred during defined windows between drug infusions, typically between the 90-minute and 120-minute marks and after the 180-minute assessment.
Adverse Events
Adverse events were continuously monitored throughout the infusion and recovery phases by a study physician and nurse. Prespecified events of interest included hypotension, bradycardia, respiratory depression (defined as oxygen saturation <94% or respiratory rate <8 breaths per minute), nausea, vomiting, dizziness, emergence reactions (eg, hallucinations, agitation), and any other serious or unexpected reactions. Events were categorized by system (eg, cardiovascular, gastrointestinal, neurologic) and recorded with associated severity, duration, and management. Safety intervention thresholds were specified a priori, and infusion discontinuation criteria were predefined. No serious adverse events occurred, and no participant met criteria for premature study termination.
Statistical Analysis
All analyses were performed on data from the 39 participants who completed the study per protocol. No interim analyses were conducted. Continuous outcome variables, including vital signs, pain thresholds, and visual analog scale (VAS) scores, were analyzed using repeated-measures models to assess changes over time within groups and to compare trajectories between groups.
Linear mixed-effects models were fitted with fixed effects for treatment group (KET/DEX vs KET/FENT), time (assessment points), and their interaction. Either an unstructured or compound symmetry covariance matrix was used, selected based on model fit, to account for within-subject correlations. The primary outcomes; change in systolic and diastolic blood pressure and change in pressure pain threshold, were evaluated based on both within-group changes over time and group-by-time interactions. If the interaction term or main effect of time reached statistical significance, post hoc pairwise comparisons were performed with Bonferroni correction to control for multiple comparisons.
Between-group comparisons at individual time points, including comparisons of nadir systolic blood pressure and end-of-infusion pain thresholds, were performed using two-sample t-tests. These comparisons were prespecified and are presented with unadjusted p-values. Categorical outcomes, including incidence of hypotension, bradycardia, and nausea or vomiting, were compared using Fisher’s exact test, chosen for its robustness in small samples.
All tests were two-tailed, with a significance threshold of α = 0.05. No imputation was performed; all participants had complete data for primary endpoints, and the mixed-model approach accommodated any sporadic missing values in secondary measures.
Data are presented as means ± standard deviation unless otherwise specified. Analyses were conducted using SPSS Statistics version 24 (IBM Corp). and GraphPad Prism version 9.0. Although the trial was exploratory and not powered to detect a prespecified primary endpoint, a post hoc analysis indicated that the sample size provided greater than 80% power to detect a 15 mm Hg difference in systolic blood pressure between groups, assuming a standard deviation of 12 mm Hg.
Results
Participant Flow and Baseline Characteristics
A total of 41 healthy volunteers were enrolled and randomly assigned to receive either ketamine–dexmedetomidine (KET/DEX) or ketamine–fentanyl (KET/FENT). Two participants were excluded and replaced prior to analysis: one in the KET/FENT group for protocol nonadherence and one in the KET/DEX group due to undisclosed pre-study ketamine exposure, identified via baseline plasma screening. The final analysis included 39 participants: 19 in the KET/DEX group and 20 in the KET/FENT group, all of whom completed the study per protocol. The trial profile is presented in Supplementary Figure 1.
Baseline demographic and clinical characteristics were similar between groups (Table 1). The mean age of the overall cohort was 28.4 ± 5.8 years, and 74% of participants were male. Mean body weight was 78.0 ± 16.2 kg. Resting blood pressure and heart rate at baseline were within normal limits across all participants (mean supine blood pressure approximately 118/75 mm Hg; heart rate ~70 beats per minute), with no statistically significant differences observed between the treatment groups before drug administration.
Hemodynamic Responses
Blood Pressure
Hemodynamic profiles during the infusion and recovery periods are shown in Figure 1. During the initial 90-minute ketamine-only phase, systolic and diastolic blood pressure increased transiently by approximately 10 to 15 mm Hg, likely reflecting ketamine’s sympathomimetic properties, and then stabilized. No significant differences were observed between the two groups during this phase, as all participants were receiving the same regimen.
 |
Figure 1 (A) Mean [standard error (±SE)] (i) systolic and (ii) diastolic blood pressure (mmHg) at baseline, during the treatment period and recovery period for the KET/DEX and KET/FENT group. Time interval 1 represents baseline, and intervals 2–7 present measurement of the variables every 30 minutes from baseline and intervals 8–12 present measurement recorded every hour thereafter (post-treatment). Interval 1 denotes baseline assessments, intervals 2–4 denote the time of the S(+)-ketamine only infusion (0.3mg/kg + 0.15mg/kg/hr ketamine, 0–90 min), and intervals 5–7 indicate the time of co-administration (0.15mg/kg/hr ketamine infusion + 0.7µg/kg/hr infusion of dexmedetomidine OR three 25µg fentanyl injections, 90–180 minutes). Intervals 8–12 denote post-treatment assessments. *Significantly different from baseline (p <0.05). **Significantly different from baseline (p<0.0001). #Significantly different from the corresponding value for group (ie KET/DEX vs KET/FENT systolic) (p < 0.05). ##Significantly different from the corresponding value for group (p < 0.0001). (B) Individual plotted [standard error (±SE)] systolic blood pressure (mmHg) at baseline, during the treatment period and recovery period for the KET/DEX and KET/FENT group. Time interval 1 represents baseline, and intervals 2–7 present measurement of the variables every 30 minutes from baseline and intervals 8–12 present measurement recorded every hour thereafter (post-treatment). Interval 1 denotes baseline assessments, intervals 2–4 denote the time of the S(+)-ketamine only infusion (0.3mg/kg + 0.15mg/kg/hr ketamine, 0–90 min), and intervals 5–7 indicate the time of co-administration (0.15mg/kg/hr ketamine infusion + 0.7µg/kg/hr infusion of dexmedetomidine OR three 25µg fentanyl injections, 90–180 minutes). Intervals 8–12 denote post-treatment assessments. (C) Individual plotted [standard error (±SE)] diastolic blood pressure (mmHg) at baseline, during the treatment period and recovery period for the KET/DEX and KET/FENT group. Time interval 1 represents baseline, and intervals 2–7 present measurement of the variables every 30 minutes from baseline and intervals 8–12 present measurement recorded every hour thereafter (post-treatment). Interval 1 denotes baseline assessments, intervals 2–4 denote the time of the S(+)-ketamine only infusion (0.3mg/kg + 0.15mg/kg/hr ketamine, 0–90 min), and intervals 5–7 indicate the time of co-administration (0.15mg/kg/hr ketamine infusion + 0.7µg/kg/hr infusion of dexmedetomidine OR three 25µg fentanyl injections, 90–180 minutes). Intervals 8–12 denote post-treatment assessments. |
Following initiation of the co-administration phase at 90 minutes, blood pressure trajectories diverged significantly. In the ketamine–dexmedetomidine group (KET/DEX), systolic pressure declined to a mean of 100 ± 8 mm Hg by the end of infusion (180 minutes), representing a 29% decrease from baseline (p<0.0001 for within-group time effect). Diastolic pressure in the same group decreased in parallel, from approximately 80 mm Hg to 55 mm Hg (p<0.0001). In contrast, blood pressure in the ketamine–fentanyl group (KET/FENT) remained stable throughout the co-administration phase. At 180 minutes, mean systolic pressure in the KET/FENT group was 116 ± 10 mm Hg, not significantly different from baseline (p=0.60). The between-group difference in systolic pressure at 180 minutes was 16 mm Hg (p<0.001). The lowest recorded systolic pressures (nadir values) occurred near the end of the infusion in most participants, averaging 98 mm Hg in KET/DEX versus 115 mm Hg in KET/FENT.
The hypotensive effect of dexmedetomidine persisted into early recovery. One hour after drug cessation, mean systolic pressure in KET/DEX remained 10 to 15 mm Hg below baseline and significantly lower than in KET/FENT (p<0.05). By 4 hours post-treatment, pressures in both groups had returned to baseline and no longer differed.
During the co-administration phase, four participants in the KET/DEX group experienced clinically significant hypotension, defined as symptomatic dizziness or systolic pressure below 90 mm Hg. Nadir systolic pressures in these cases ranged from 85 to 88 mm Hg. All events were transient and managed with intravenous fluid boluses (500–1000 mL normal saline); no participants required vasopressors. In contrast, no participant in the KET/FENT group experienced systolic pressure below 100 mm Hg at any time. The incidence of hypotension was significantly higher in KET/DEX than in KET/FENT (21% vs 0%; p=0.047 by Fisher’s exact test). There were no hypertensive episodes in either group beyond the transient ketamine-induced elevations during the initial infusion phase. Adverse event frequencies are summarized in Table 2.
 |
Table 2 Total (n, %) and Group Distribution (Ketamine/Dexmedetomidine Vs Ketamine/Fentanyl) of Adverse Events |
Heart Rate
Heart rate changes mirrored the differential autonomic effects of the two regimens (Figure 2). During the ketamine-only phase, heart rate increased modestly in both groups by approximately 5 to 7 beats per minute, peaking between 30 and 60 minutes. Following administration of dexmedetomidine, heart rate in the KET/DEX group declined from approximately 75 bpm at 90 minutes to 68 ± 10 bpm at 180 minutes, a 10% decrease from baseline (p<0.05 within-group). In contrast, heart rate in the KET/FENT group remained stable throughout, averaging 74 ± 12 bpm at 180 minutes (p=0.90 within-group).
 |
Figure 2 (A) Mean [standard error (±SE)] heart rate at baseline, during the treatment period and recovery period for the KET/DEX and KET/FENT group. Time interval 1 represents baseline, and intervals 2–7 present measurement of the variables every 30 minutes from baseline and intervals 8–12 present measurement recorded every hour thereafter. Interval 1 denotes baseline assessments, intervals 2–4 denote the time of the S(+)-ketamine only infusion (0.3mg/kg + 0.15mg/kg/hr ketamine, 0–90 min), and intervals 5–7 indicate the time of co-administration (0.15mg/kg/hr ketamine infusion + 0.7µg/kg/hr infusion of dexmedetomidine OR three 25µg fentanyl injections, 90–180 minutes). Intervals 8–12 denote post-treatment assessments. (B) Individual plotted [standard error (±SE)] heart rate at baseline, during the treatment period and recovery period for the KET/DEX and KET/FENT group. Time interval 1 represents baseline, and intervals 2–7 present measurement of the variables every 30 minutes from baseline and intervals 8–12 present measurement recorded every hour thereafter. Interval 1 denotes baseline assessments, intervals 2–4 denote the time of the S(+)-ketamine only infusion (0.3mg/kg + 0.15mg/kg/hr ketamine, 0–90 min), and intervals 5–7 indicate the time of co-administration (0.15mg/kg/hr ketamine infusion + 0.7µg/kg/hr infusion of dexmedetomidine OR three 25µg fentanyl injections, 90–180 minutes). Intervals 8–12 denote post-treatment assessments. |
Despite the within-group decline in KET/DEX, between-group comparisons of heart rate at individual time points did not reach statistical significance. At 180 minutes, the difference between groups was 6 bpm (68 vs 74 bpm; p=0.15), and no significant differences were observed at other time points (all p>0.1). The modest bradycardia in KET/DEX appeared to be offset by ketamine’s sympathomimetic effects, resulting in similar net heart rates between groups. One participant in KET/DEX recorded a transient heart rate of 45 bpm but remained asymptomatic and did not require intervention. No participant in the KET/FENT group exhibited a heart rate below 60 bpm at any point. Heart rates in both groups returned to baseline by 4 hours post-infusion.
These findings indicate that while dexmedetomidine induced a modest bradycardic trend, concurrent ketamine administration attenuated this effect, resulting in heart rate profiles not significantly different from those observed with ketamine–fentanyl.
Analgesic Outcomes
Pain Threshold (Pressure Algometry)
Both treatment regimens were associated with increases in mechanical pain tolerance, as measured by pressure algometry (Figure 3). At baseline, mean pain thresholds were similar between the two groups (approximately 250–260 kPa), with no significant differences. Following 90 minutes of ketamine infusion (prior to co-administration), participants in the ketamine–dexmedetomidine group (KET/DEX) exhibited a significant increase in pain threshold from baseline (mean increase of approximately 20 kPa; p<0.0001, within-group), whereas the ketamine–fentanyl group (KET/FENT) showed a smaller, non-significant increase at the same time point.
 |
Figure 3 Box plot for the distributions of the Algometer scores across each assessment phase for the ketamine/dexmedetomidine treatment group. The box plot displays 10th, 25th, median, 75th, and 90th percentiles of values. **Significantly different from baseline (p<0.0001). Higher scores indicate higher pain tolerance. ^Co-administration refers to treatment group: KET/DEX; 0.15mg/kg/hr ketamine infusion + 0.7µg/kg/hr infusion of dexmedetomidine or KET/FENT; 0.15mg/kg/hr ketamine infusion + three 25µg fentanyl injections. **Significantly different from baseline (p < 0.0001). Significantly different from ketamine only to co-administration^. |
During the 90-minute co-administration phase, further increases in pressure tolerance were observed in both groups. At the end of treatment (180 minutes), mean thresholds reached approximately 300 kPa in KET/DEX and 310 kPa in KET/FENT (from ~250 kPa at baseline), with both increases statistically significant compared to baseline (p<0.0001, within-group). The incremental gain in pain tolerance during co-administration appeared slightly greater in the KET/FENT group, consistent with the additional analgesic contribution of fentanyl during this period. However, no statistically significant difference was observed between the two groups at the end of the infusion (mean difference <5 kPa; p=0.78), indicating comparable analgesic efficacy between regimens.
At the final post-treatment assessment, conducted approximately two hours after infusion cessation (5 hours from initiation), pain thresholds in both groups had returned toward baseline. Minor residual elevation was observed in some participants but was not statistically significant and did not differ between groups.
Of note, the KET/DEX group demonstrated a significant analgesic response during the ketamine-only phase, prior to dexmedetomidine administration. This early effect is consistent with ketamine’s known analgesic properties and may have been augmented by sedation-related modulation of pain perception. By contrast, the KET/FENT group exhibited a more pronounced analgesic response only after the introduction of fentanyl. Nevertheless, by the end of the study, both groups achieved similar levels of increased pressure pain tolerance, supporting the interpretation that dexmedetomidine contributed a comparable analgesic effect to fentanyl in the context of low-dose ketamine.
Pain Intensity Ratings
Despite objective increases in pressure pain thresholds, subjective ratings of pain intensity remained low throughout the study. Participants consistently rated the pain induced by algometry at threshold as mild, both at baseline and during treatment (mean VAS scores ~5–15 mm on a 100-mm scale). No significant changes in pain intensity ratings were observed over time in either group and no between-group differences were detected at any time point (all p>0.5).
The dissociation between increased objective pain thresholds and unchanged subjective intensity ratings likely reflects a ceiling effect, as participants were asked to identify the first sensation of pain. Alternatively, sedation or altered affective processing, particularly with dexmedetomidine, may have influenced subjective pain appraisal. These findings underscore the importance of using both objective and subjective measures when evaluating analgesic effects in controlled experimental settings.
Sedation and Mood Effects
Both treatment regimens were associated with measurable sedative and mood-altering effects, consistent with the known psychotropic profiles of ketamine and its adjunct agents. However, the quality and trajectory of these effects differed between groups, particularly following the addition of dexmedetomidine or fentanyl.
During the ketamine-only phase (0 to 90 minutes), participants in both groups reported increased calmness and mild reductions in alertness, without significant dysphoria. No significant between-group differences were noted across most mood domains at this stage, with the exception of the calmness rating. Participants later assigned to the ketamine–dexmedetomidine group (KET/DEX) reported higher calmness scores at 90 minutes compared to those in the ketamine–fentanyl group (KET/FENT) (p<0.05), a finding that may reflect random variation or psychological expectation due to the unblinded design.
Following initiation of the adjunctive agents (90 to 180 minutes), sedation deepened in both groups, but the degree and associated mood effects diverged. Participants in the KET/DEX group reported significantly lower energy levels and reduced engagement with their surroundings compared to both their own baseline and to the KET/FENT group (p<0.01). Qualitative observations included descriptions of somnolence, detachment, and withdrawal. Conversely, the KET/FENT group reported increased calmness and relaxation without significant negative affect. Although reductions in energy were also noted in this group, they were less pronounced than in KET/DEX (p<0.05 between groups). On the contentment scale, KET/DEX participants tended toward discontent or apathy, whereas KET/FENT participants remained neutral or mildly positive (p<0.05 between groups).
Despite these differences in mood profiles, both regimens were well tolerated. No significant differences were observed in self-rated overall comfort or analgesic satisfaction. Importantly, no emergence reactions, hallucinations, or severe agitation occurred in either group. The deeper sedative effect of dexmedetomidine likely mitigated ketamine-associated psychotropic effects. Some participants in KET/DEX retrospectively described the infusion period as “dreamy” or “foggy”, though not distressing.
By two hours post-treatment (five hours after ketamine initiation), most mood effects had resolved. Group differences in VAS scores for calmness, contentment, and alertness were no longer statistically significant. By four hours post-infusion, all participants were fully alert and ambulatory. No delayed psychological adverse effects were reported on follow-up.
These findings indicate that the ketamine–dexmedetomidine combination produces a deeper sedative state with transient negative mood features, such as withdrawal and disengagement, whereas the ketamine–fentanyl regimen is associated with milder sedation characterized predominantly by relaxation. These subjective differences may have implications for patient experience and tolerability in clinical applications.
Adverse Events
Adverse events are summarized in Table 2. Of the 39 participants included in the analysis, 9 (23.1%) experienced at least one adverse event, while the remaining 30 (76.9%) completed the study without incident aside from expected sedation. The type and frequency of events varied between treatment groups and reflected the pharmacologic profiles of the administered agents.
Cardiovascular Events
In the KET/DEX group, the mean nadir systolic blood pressure was 92 mm Hg, with the largest observed drop being 36 mm Hg in a single participant (from 135 mm Hg to 99 mm Hg). Hypotension, defined a priori as systolic pressure below 100 mm Hg or symptomatic low blood pressure, occurred in 4 of 19 participants (21%). Each episode was transient, typically lasting 5 to 10 minutes. Per protocol, all cases were managed with intravenous crystalloid boluses: three participants received 500 mL, and one required 1000 mL of normal saline. Blood pressure stabilized promptly following fluid administration in all cases. No participant required vasopressor support, and all hypotensive episodes resolved within 15 minutes. No arrhythmias were observed on cardiac monitoring. One participant in KET/DEX exhibited a transient heart rate of 45 beats per minute without associated symptoms or clinical intervention. No bradycardia or hypotension was recorded in the KET/FENT group, where blood pressure and heart rate remained stable throughout. The differential incidence of hypotension between groups underscores the need for hemodynamic vigilance when administering dexmedetomidine, even at moderate doses, particularly in ambulatory or unsedated populations.
Respiratory Events
No episodes of respiratory depression occurred in either group. Oxygen saturation remained ≥96% in all participants while breathing room air, and respiratory rates were maintained above 12 breaths per minute. The combination of low-dose fentanyl with ketamine did not result in observable respiratory compromise, and dexmedetomidine was similarly well tolerated in this respect. No participant exhibited signs of airway obstruction or required respiratory support.
Psychotropic and Neurologic Events
No participant experienced hallucinations, agitation, or other severe emergence phenomena. Mild euphoria or a “floating” sensation was reported by a few participants in the KET/FENT group during ketamine infusion. In the KET/DEX group, some participants reported transient dream-like states or internal dialogue, which were not distressing. Two participants in KET/DEX experienced brief disorientation upon awakening, resolving spontaneously within minutes and not classified as adverse events. These findings are consistent with the sedative effects of dexmedetomidine and suggest that its co-administration may attenuate the dysphoric and psychotomimetic effects typically associated with ketamine.
Gastrointestinal Events
Gastrointestinal symptoms were more frequent in the KET/FENT group. Nausea was reported by three participants (15%) in KET/FENT, with one instance of vomiting during the recovery period. In the KET/DEX group, one participant (5%) reported mild nausea without emesis. Although numerically higher in KET/FENT, the difference in nausea/emesis incidence between groups was not statistically significant (p = 0.32). All affected participants responded to antiemetic treatment (ondansetron 8 mg intravenously or oral meclizine 10 mg), and no additional interventions were required. The greater frequency of nausea in the fentanyl group is consistent with the known emetogenic profile of opioids, whereas dexmedetomidine may exert antiemetic effects via sympathetic modulation.
Other Adverse Events
No allergic reactions or injection site complications were observed. Transient dizziness or light-headedness was reported by participants in the KET/DEX group and was associated with hypotension. One participant in KET/FENT reported a mild headache during recovery, which resolved without intervention and was not attributed to study medication. No cases of dry mouth or urinary retention were reported.
No serious adverse events occurred. All participants were discharged on the same day without medical sequelae. Follow-up on the day after study completion revealed no delayed adverse effects.
These findings indicate that the ketamine–dexmedetomidine regimen is associated with a higher incidence of transient, fluid-responsive hypotension, while the ketamine–fentanyl combination demonstrates a greater tendency toward mild gastrointestinal symptoms. Both regimens were otherwise well tolerated in a closely monitored research setting.
Discussion
In this randomized trial involving healthy volunteers, the cardiovascular and analgesic effects of a ketamine–dexmedetomidine regimen were compared with those of a ketamine–fentanyl combination, with the aim of evaluating the tolerability and potential clinical utility of dexmedetomidine as an opioid-sparing adjunct. The two regimens produced similar analgesic effects, but with distinct safety and side effect profiles. The ketamine–dexmedetomidine combination was associated with greater reductions in blood pressure and a higher incidence of hypotension requiring intervention, whereas the ketamine–fentanyl regimen was associated with a higher incidence of mild gastrointestinal symptoms. Mood effects also differed, with dexmedetomidine producing deeper sedation and transient withdrawal-like states. These findings underscore the trade-offs inherent in opioid-sparing analgesic strategies and highlight the need for careful dose selection and hemodynamic monitoring.
Hemodynamic Effects
Administration of dexmedetomidine in combination with ketamine resulted in significant reductions in systolic and diastolic blood pressure, with a mean decrease of approximately 25–30% from baseline, despite concurrent low-dose ketamine. These findings are consistent with dexmedetomidine’s known sympatholytic effects, which may override ketamine’s modest pressor activity at the doses used. Although heart rate also decreased in the dexmedetomidine group, the reduction was modest, and between-group differences were not statistically significant, suggesting partial attenuation of dexmedetomidine-induced bradycardia by ketamine.
Four participants in the dexmedetomidine group required fluid boluses to manage hypotension, although none required vasopressors. In contrast, no participants in the fentanyl group met criteria for intervention. These findings support previous reports that ketamine may blunt but does not fully prevent the hypotensive effects of dexmedetomidine. In clinical contexts, particularly in patients with compromised cardiovascular function, a reduced dexmedetomidine dose or prophylactic fluid loading may be warranted. While this study used an infusion rate of 0.7 µg/kg/hr, doses of 0.3 to 0.4 µg/kg/hr may offer more favorable hemodynamic profiles, a hypothesis that requires formal evaluation in future studies.
Our findings underscore the need for dose optimization of dexmedetomidine when used in combination with ketamine. It is possible that a lower dexmedetomidine dose or slower titration could achieve comparable analgesic effects with a reduced risk of hypotension. Additionally, incorporating routine fluid administration or anticipatory vasopressor support into clinical protocols may improve the safety profile of this regimen. These strategies warrant prospective evaluation in future studies.
Analgesic and Sedative Effects
Both regimens produced a significant increase in pressure pain thresholds compared to baseline, with no statistically significant differences in peak pain tolerance between groups. These findings suggest that dexmedetomidine provided analgesic efficacy comparable to fentanyl when combined with low-dose ketamine. Dexmedetomidine’s analgesic effects are believed to involve α2-adrenergic receptor activation in the spinal cord and brainstem, which inhibits nociceptive transmission and may contribute to the observed outcomes.
Subjective pain intensity ratings remained low throughout the study and did not differ between groups, reflecting either the threshold-based nature of the pain assessment or sedation-associated reductions in the affective component of pain. The early increase in pain tolerance observed in the dexmedetomidine group during the ketamine-only phase may reflect anticipatory effects or variability in sensitivity, though both groups converged at similar endpoints. Together, these data support the potential role of dexmedetomidine as an effective opioid-sparing adjunct in multimodal analgesia.
Mood and Psychotropic Effects
Participants in the dexmedetomidine group reported greater sedation, reduced energy, and decreased engagement with their surroundings compared to those in the fentanyl group. These transient mood changes, which resolved during the recovery phase, may be attributable to dexmedetomidine’s profound sedative effects and altered central arousal states. In contrast, participants receiving ketamine with fentanyl reported calmness and relaxation without disengagement or dysphoria.
Importantly, no participants experienced hallucinations or severe psychotomimetic symptoms, and no serious neuropsychiatric adverse events were reported. The absence of emergence phenomena in the dexmedetomidine group suggests that this agent may mitigate the dissociative effects of ketamine, providing a more tolerable psychological profile. However, in conscious or lightly sedated patients, the reduction in affective responsiveness and engagement associated with dexmedetomidine may impact patient satisfaction or comfort, particularly in procedural or outpatient settings.
Safety and Clinical Implications
Overall, the ketamine–dexmedetomidine combination was associated with a greater incidence of transient hypotension, while the ketamine–fentanyl regimen was more frequently associated with mild nausea and emesis. No respiratory depression or airway compromise occurred in either group. These findings suggest that each regimen presents distinct but manageable safety considerations.
In clinical practice, the choice between these regimens may depend on individual patient characteristics, including cardiovascular status and sensitivity to opioid-related side effects. Dexmedetomidine’s opioid-sparing potential may be particularly useful in patients at high risk for opioid-related complications, provided that adequate hemodynamic monitoring is available. In contrast, the ketamine–fentanyl regimen may offer greater cardiovascular stability in patients with limited physiologic reserve.
This trial involved the administration of sedative and analgesic agents to healthy volunteers. To ensure participant safety, continuous monitoring and predefined intervention thresholds for hypotension, bradycardia, and other adverse events were implemented throughout the study. No serious adverse events occurred, and all side effects were managed successfully with protocol-specified measures. Establishing the safety profile of the ketamine–dexmedetomidine combination in a healthy population was an essential prerequisite before extending investigation to clinical populations. This controlled approach formed part of the study’s rationale and received prior approval from the institutional ethics committee.
From a clinical standpoint, the two regimens present distinct supportive care considerations. KET/DEX was associated with transient hypotension requiring fluid resuscitation, suggesting that clinicians using this combination should be prepared to manage hemodynamic instability, potentially through fluid preloading or vasopressor support. In contrast, KET/FENT was associated with a higher incidence of nausea and vomiting, reinforcing the need for anticipatory antiemetic prophylaxis. These findings underscore the importance of regimen-specific monitoring and supportive strategies when employing either approach in clinical practice.
Study Limitations and Future Directions
Several limitations of the study should be acknowledged. First, the use of healthy, pain-free volunteers limits generalizability to clinical populations. Hemodynamic responses may differ in patients with comorbidities or acute pain, and the analgesic efficacy observed in an experimental model may not translate directly to perioperative or intensive care settings. Second, the trial design did not include dexmedetomidine-only or ketamine-only arms, precluding isolated attribution of effects to individual agents. The study compared two active regimens to reflect real-world alternatives but limits conclusions about drug-specific interactions. Third, the open-label design may have introduced bias in subjective measures such as mood and sedation. Blinded designs with active placebos may help mitigate expectation effects in future trials. Fourth, no objective sedation scale (eg, RASS or BIS index) was used, limiting the ability to quantify and compare sedation levels rigorously. Fifth, the study evaluated only single-dose effects; longer-term administration may yield different safety or efficacy profiles. Dose-finding studies are needed to identify the optimal balance between analgesia and hemodynamic stability.
Further research should evaluate the use of ketamine–dexmedetomidine in clinical populations, including patients with acute or chronic pain, those undergoing surgery, and those receiving prolonged sedation. Studies comparing multiple dexmedetomidine infusion rates or testing adjunctive strategies to mitigate hypotension (eg, fluid loading, adrenergic agents) would be valuable. Investigation of physiological biomarkers (eg, heart rate variability, catecholamine levels) may improve understanding of autonomic modulation under combined regimens. Finally, long-term outcome studies assessing opioid use, recovery trajectories, and patient-reported outcomes will be essential to fully characterize the clinical relevance of this opioid-sparing strategy.
The combination of ketamine and dexmedetomidine demonstrated effective analgesia but was associated with more pronounced hemodynamic effects and deeper sedation than ketamine plus fentanyl. These results highlight the potential utility of ketamine–dexmedetomidine as an opioid-sparing analgesic strategy, contingent upon appropriate cardiovascular monitoring and management. Careful dose titration and patient selection will be essential to ensure safe and effective clinical application.
Conclusion
The combination of ketamine and dexmedetomidine offers a feasible opioid-sparing analgesic strategy, providing pain relief comparable to a ketamine–fentanyl regimen while exhibiting a distinct adverse effect profile. Dexmedetomidine was associated with significant hypotension and bradycardia, only partially mitigated by ketamine, reinforcing the need for close hemodynamic monitoring when using this combination. Despite these effects, the regimen achieved effective analgesia without opioids and was associated with fewer opioid-related adverse events, including nausea, and no evidence of respiratory depression. Participants receiving ketamine–dexmedetomidine experienced deeper sedation and transient mood alterations, in addition to hemodynamic shifts, whereas those receiving ketamine–fentanyl maintained cardiovascular stability but reported more frequent gastrointestinal symptoms. These findings suggest that ketamine–dexmedetomidine may serve as a useful adjunct in multimodal analgesia, particularly in opioid-tolerant patients or those at risk for opioid-related complications. To enhance tolerability, dose adjustments, such as reducing the dexmedetomidine infusion rate to approximately 0.4 µg/kg/hour and proactive cardiovascular support may be beneficial.15 Further clinical research is needed to confirm these findings in patient populations and to assess the long-term safety and efficacy of this opioid-sparing approach across various care settings.
Data Sharing Statement
The authors intend to share individual de-identified participant data (including clinical and outcome data) from this study upon reasonable request. The study protocol and statistical analysis plan will also be available. Data can be obtained by contacting the corresponding author (email provided above). These data will be made available immediately following publication and will remain available for 5 years post-publication.
Disclosure
Amie Hayley is supported by a National Health and Medical Council (NHMRC) Peter Doherty Biomedical Early Career Research Fellowship (GNT:1119960). Luke Downey is supported by an NHMRC R.D. Wright Biomedical Career Development Fellowship (GNT:1122577). Michael Keane reports Medical Advisory Committee from Cannvalate. Institutional departmental funds were used to reimburse participants. The authors report no other conflicts of interest in this work.
References
1. Suzuki M. Role of N-methyl-D-aspartate receptor antagonists in postoperative pain management. Curr Opin Anaesthesiol. 2009;22(5):618–622. doi:10.1097/ACO.0b013e32832e7af6
2. Grider JS, Ackerman WE. Opioid-induced hyperalgesia and tolerance: understanding opioid side effects. Expert Rev Clin Pharmacol. 2008;1(2):291–297. doi:10.1586/17512433.1.2.291
3. Khademi H, Kamangar F, Brennan P, Malekzadeh R. Opioid therapy and its side effects: a review. Arch Iran Med. 2016;19(12):870–876.
4. Clarke H, Soneji N, Ko DT, Yun L, Wijeysundera DN. Rates and risk factors for prolonged opioid use after major surgery: population based cohort study. BMJ. 2014;348:g1251. doi:10.1136/bmj.g1251
5. Kurdi MS, Theerth KA, Deva RS. Ketamine: current applications in anesthesia, pain, and critical care. Anesth Essays Res. 2014;8(3):283–290. doi:10.4103/0259-1162.143110
6. Imboden TJ, Pownall WR, Rubin S, Spadavecchia C, Schollhorn B, Rohrbach H. Determination of a safe sedative combination of dexmedetomidine, ketamine and butorphanol for minor procedures in dogs by use of a stepwise optimization method. Acta Vet Scand. 2023;65(1):41. doi:10.1186/s13028-023-00697-8
7. Ferreira R, Telo M, Figueiredo J. Ketamine and dexmedetomidine combination for the management of the pediatric difficult airway. Cureus. 2023;15(12):e50473. doi:10.7759/cureus.50473
8. Elsaeidy AS, Ahmad AHM, Kohaf NA, et al. Efficacy and safety of ketamine-dexmedetomidine versus ketamine-propofol combination for periprocedural sedation: a systematic review and meta-analysis. Curr Pain Headache Rep. 2024;28(4):211–227. doi:10.1007/s11916-023-01208-0
9. Kehlet H, Dahl JB. The value of “multimodal” or “balanced analgesia” in postoperative pain treatment. Anesth Analg. 1993;77(5):1048–1056. doi:10.1213/00000539-199311000-00030
10. Schwenk ES, Viscusi ER, Buvanendran A, et al. Consensus guidelines on the use of intravenous ketamine infusions for acute pain management from the American Society of Regional Anesthesia and Pain Medicine, the American Academy of Pain Medicine, and the American Society of Anesthesiologists. Reg Anesth Pain Med. 2018;43(5):456–466. doi:10.1097/AAP.0000000000000806
11. Bell RF, Dahl JB, Moore RA, Kalso E. Peri-operative ketamine for acute post-operative pain: a quantitative and qualitative systematic review (Cochrane review). Acta Anaesthesiol Scand. 2005;49(10):1405–1428. doi:10.1111/j.1399-6576.2005.00814.x
12. Gottschalk A, Smith DS. New concepts in acute pain therapy: preemptive analgesia. Am Fam Physician. 2001;63(10):1979–1984.
13. Shehabi Y, Howe BD, Bellomo R, et al. Early sedation with dexmedetomidine in critically ill patients. N Engl J Med. 2019;380(26):2506–2517. doi:10.1056/NEJMoa1904710
14. Tan JA, Ho KM. Use of dexmedetomidine as a sedative and analgesic agent in critically ill adult patients: a meta-analysis. Intensive Care Med. 2010;36(6):926–939. doi:10.1007/s00134-010-1877-6
15. Sangkum L, Termpornlert S, Tunprasit C, Rathanasutthajohn C, Komonhirun R, Dusitkasem S. Effect of low-dose dexmedetomidine to prolong spinal anesthesia in elderly patients: a prospective randomized controlled study. BMC Anesthesiol. 2024;24(1):427. doi:10.1186/s12871-024-02815-z
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Successful Use of Low-Dose Combination Propofol and Fentanyl in Cataract Surgery Phacoemulsification
Irawati D, Adli M, Yadi DF
Clinical Ophthalmology 2023, 17:1929-1937
Published Date: 5 July 2023