")
Back to Journals » Infection and Drug Resistance » Volume 18
Analysis of Manifestations and Associated Factors of HIV-1 Associated Thrombocytopenia in a General Teaching Hospital in Western China
Authors Tang Z, Wang Z, Wang T, Li D , Li J, Liu C, Tao C
Received 24 January 2025
Accepted for publication 10 April 2025
Published 17 April 2025 Volume 2025:18 Pages 1913—1921
DOI https://doi.org/10.2147/IDR.S517427
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Zhuoyun Tang, Zhonghao Wang, Tingting Wang, Dongdong Li, Jingyi Li, Chaonan Liu, Chuanmin Tao
Department of Laboratory Medicine, Clinical Laboratory Medicine Research Center, West China Hospital, Sichuan University, Sichuan Clinical Research Center for Laboratory Medicine, Chengdu, 610041, People’s Republic of China
Correspondence: Chuanmin Tao, Email [email protected]
Background: Thrombocytopenia frequently occurs with HIV-1 infection and plays a vital role in the deterioration of the Blood-Brain Barrier (BBB) and the development of neuroinflammation. This study aims to assess the prevalence and risk factors for HIV-1 associated thrombocytopenia (HAT) and summarize the characteristics of HAT-related neuroinflammation.
Methods: A retrospective study of HAT patients was conducted in a general teaching hospital from January 2017 to December 2021. Clinical and laboratory data from HIS and LIS were analyzed to determine the prevalence and risk factors for HAT and manifestations of HAT with neuroinflammation.
Results: The prevalence of HAT was 11.06%, with a majority of male patients (76.92%), individuals aged 50 and older (55.21%), and 63.80% experiencing mild thrombocytopenia. Significant differences were observed in CD4+ T cell count, platelet crit (PCT), and the proportion of large platelets (P-LCR) between the HAT and control groups (P< 0.001, P< 0.001, P=0.002). A CD4+ T cell count < 200 cells/μL (P=0.001) was identified as a significant risk factor for HAT, while advanced age and high viral load were closely associated with HAT occurrence. HAT Patients with neuroinflammation were predominantly male (X2=10.066, P=0.007), had higher viral loads (X2=12.297, P=0.006), advanced age (X2=11.721, P=0.02), neuropsychiatric symptoms, and elevated levels of inflammatory factors such as IL-6 and proteins in cerebrospinal fluid (CSF).
Conclusion: In HIV-1 infection, the activation of monocytes, macrophages, and microglia leads to thrombocytopenia and neuroinflammation, highlighting the importance of recognizing HAT and HAT with neuroinflammation. Advanced age, lower CD4+ T cell count, and high viral load are closely linked to their occurrence.
Keywords: HIV-1, thrombocytopenia, neuroinflammation, prevalence
Introduction
Human Immunodeficiency Virus-1 (HIV-1) disrupts the human immune system, increasing the risk of cancers and various opportunistic infections. Hematologic complications such as anemia, leukopenia, and thrombocytopenia often accompany HIV-1 infection and AIDS.1 The prevalence of HIV-1 associated thrombocytopenia (HAT) can range from 5.9% to 40% and may manifest at any stage of the infection.2–4 Thrombocytopenia can be the initial clinical sign in asymptomatic HIV-1-infected individuals and may worsen over time, potentially leading to severe bleeding.5 Besides, HIV-1 and its proteins, including Tat, can compromise the integrity of the Blood-Brain Barrier (BBB), enabling them to enter the central nervous system and induce neuroinflammation.6,7 Although the exact causes of HAT remain uncertain so far, factors such as age, viral load, CD4+ T cell counts, and others may be linked to its occurrence. Meanwhile, several studies have emphasized the critical role of HIV-1 and platelet interaction in BBB degradation.8 In this study, we have consolidated data from a large general teaching hospital in China with 4300 beds to assess the prevalence and risk factors associated with HAT, as well as the manifestations of HAT with neuroinflammation.
Materials and Methods
Study Population
A retrospective study was conducted in a general teaching hospital in Sichuan, China, with 4300 beds, serving a catchment population of approximately 16.33 million. The study encompassed 221 HAT samples obtained from both inpatients and outpatients between January 2017 and December 2021.
Study-Outcome Definitions
HIV-1 infected patients were identified in accordance with the guidelines for the diagnosis and treatment of HIV/AIDS in China (2021 edition). HIV infection was screened by electrochemiluminescence assay (Elecsys® HIV Duo assay, Elecsys® HIV combi PT assay, Roche Diagnostics) and all initially positive (cut‐off index [COI] > 1.0) or borderline (0.9 ≤ COI ≤ 1.0) specimens were retested by Anti-HIV Colloidal gold kit (Zhuhai Livzon Diagnostics Inc). All initially positive samples were confirmed by Western Blot assay (HIV Blot 2.2 assay, MP Diagnostics) and the positive results were defined as the presence of at least two bands, including two env bands, or one env band plus p24 band.
All patients enrolled in this study were newly diagnosed HIV infection and collected the platelet (PLT) count within one week after or before the HIV screening test. HAT patients were defined as individuals with HIV-1 infection who exhibited thrombocytopenia, which was characterized by a PLT count of <100 × 109/L. Mild thrombocytopenia was categorized as a PLT count between 99 × 109/L and 50 × 109/L. Moderate thrombocytopenia was defined as a PLT count between 30 × 109/L and 49 × 109/L, while severe thrombocytopenia was denoted by a PLT count <30 × 109/L. HAT with neuroinflammation was diagnosed when neuroinflammation symptoms, such as headache, dizziness, and consciousness disorders, were observed in HAT patients. The control group, consisting of HIV-1-infected individuals without thrombocytopenia, was used for assessing viral load, CD4+ T cell counts, platelet crit (PCT), the proportion of large platelets (P-LCR), and platelet distribution width (PDW). The groups were matched in a 1:2 ratio, and no significant differences in sex and age were noted between the disease and control groups (P>0.05).
Data Collection
The following clinical and laboratory data were extracted from the electronic medical record system: sex, age, patient source, lymphocyte count, COI of the screening test, viral load, CD4+ T cell count, PCT, P-LCR, and PDW. For HAT with neuroinflammation, medical records were also reviewed, encompassing cerebrospinal fluid (CSF) protein levels (reference range: 0.15–0.45), serum IL-6 levels (reference range: 0–7.00), and clinical diagnoses, in addition to the indicators mentioned earlier.
Statistical Analysis
Data were recorded using Excel and analyzed through SPSS 23.0 and Origin 2022. Quantitative data were presented as the median and interquartile range (IQR). Non-categorical variables were subjected to t-tests, while categorical variables were examined using the chi-square test or Fisher’s exact probability test. Univariate and multivariate logistic regression analyses were conducted to assess the impact of risk factors on the prevalence of HAT. The results were presented as adjusted odds ratios (OR) along with their corresponding 95% confidence intervals (CI). Statistical significance was defined as a P-value ≤ 0.05.
Results
The Clinical and Laboratory Characteristics of HAT
A total of 1998 samples were confirmed as positive by Western Blot between 2017 and 2021, and among them, 221 were ultimately diagnosed with HAT, resulting in a prevalence of 11.06% (221/1998). The prevalence showed a consistent increase from 10.90% in 2017 to 18.67% in 2021. The clinical and laboratory characteristics of these 221 HAT cases were summarized in Table 1. The majority of patients were male (76.92%) and aged 50 or older (55.21%). The median COI value, which was 350.85 (173.30, 724.25), indicated a high COI value, and 63.80% of patients exhibited mild thrombocytopenia. Additionally, there was a significant difference in prevalence between patients under 50 years old and those above 50 years old (X2=458.00, P<0.001). Most HAT patients (71.95%) had low lymphocyte counts, suggesting low CD4+ T cell counts.
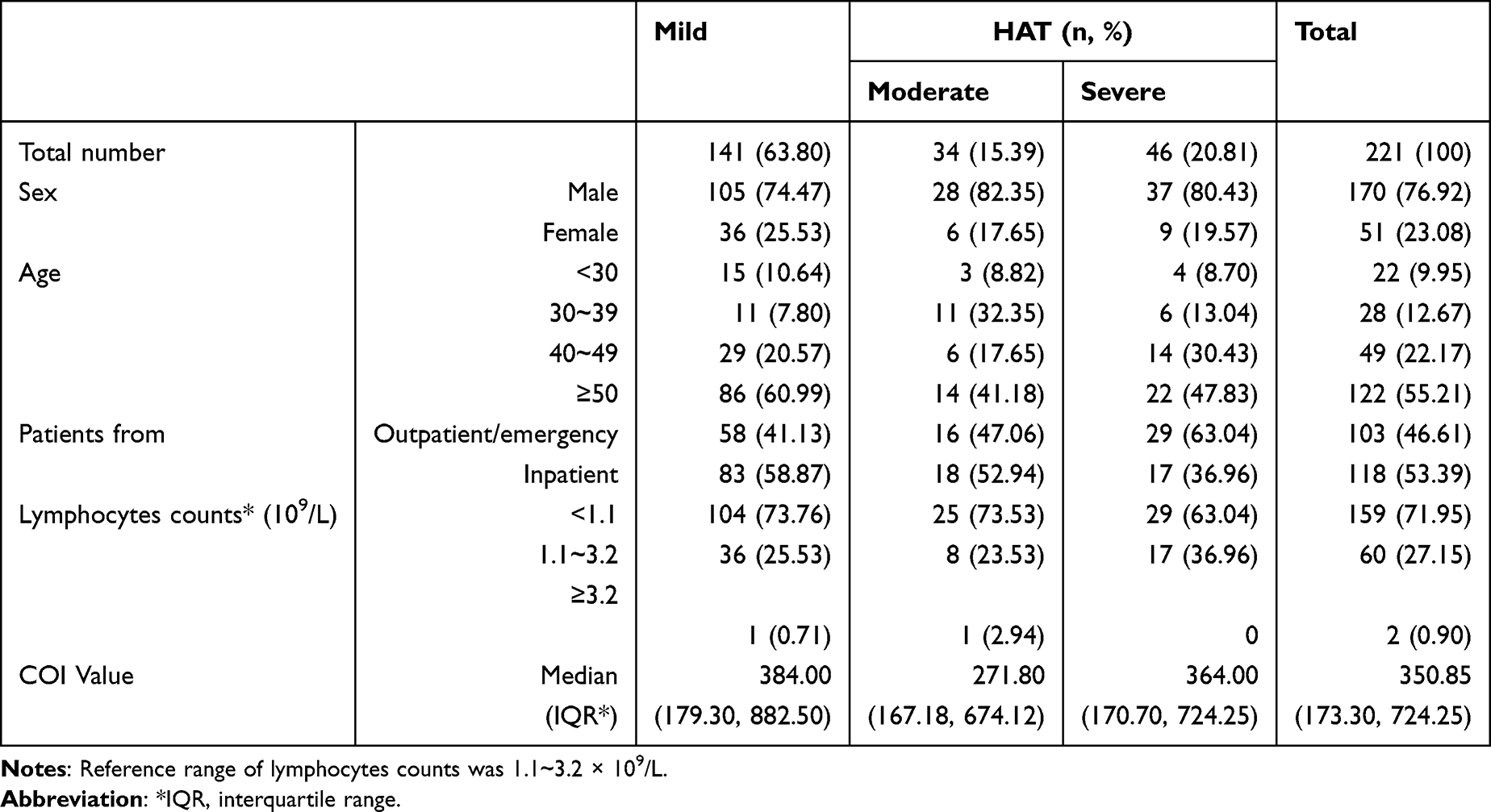 |
Table 1 Clinical and Laboratory Characteristics of 221 HAT Cases |
Platelet Parameters and Risk Factors of HAT
RNA testing was conducted for 116 HAT patients, CD4+ T cell count data was available for 120 HAT patients, and PCT, P-LCR, and PDW results were obtained for 25 HAT patients. Among HAT patients, the majority (64.66%) had a viral load ≥105 cp/mL, 77.5% had a CD4+ T cell count of <200 cell/μL, and 92.00% exhibited low PCT (<0.19). The average CD4+ T cell count for HAT patients was 123.11 cell/μL, significantly lower than that of the control group (t=3.565, P<0.001). Significant differences were also observed in PCT and P-LCR values between the HAT and control group (t=5.372, P<0.001; t=3.274, P=0.002). However, there were no discernible variations in viral load (t=1.540, P=0.125) and PDW values (t=1.150, P=0.254) between the two groups. These differences were illustrated in Figure 1.
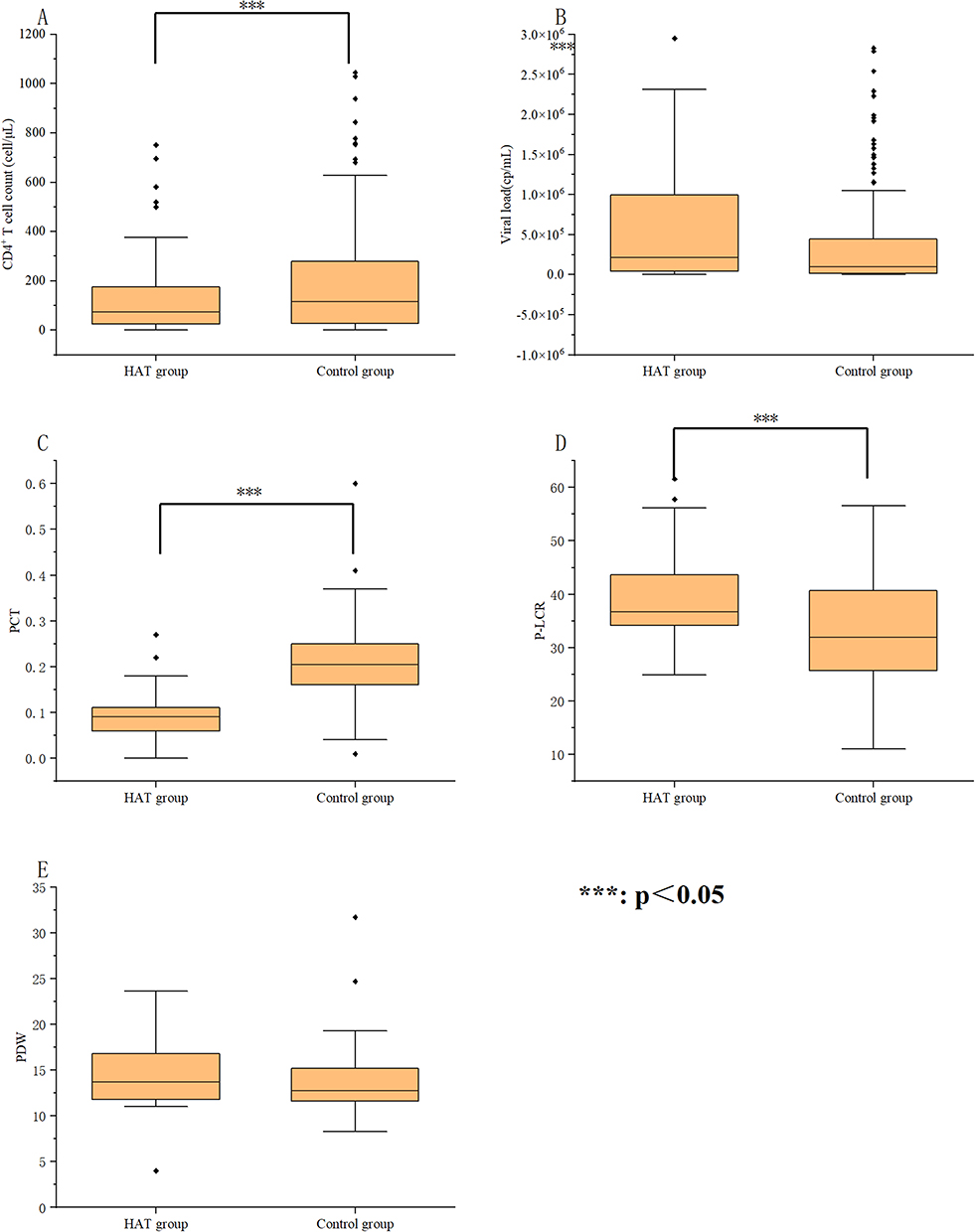 |
Figure 1 CD4+ T cell count, VL, platelets, and related parameters of 221 HAT samples and the control group. (A) CD4+ T cell count. (B) Viral load. (C) Platelet crit. (D) The rate of large platelets. (E) Platelet distribution width. |
Regarding the prevalence of HAT in different groups, significant differences were noted between CD4+ T cell count <200 cell/μL and ≥200 cell/μL (X2=248.00, P=0.019) and between viral load <105 cps/mL and ≥105 cps/mL (X2=119.00, P<0.001) as depicted in Figure 2.
 |
Figure 2 VL and CD4+ T cell count of mild, moderate, and severe HAT samples. (A) VL in different HAT samples. (B) CD4+ T cell count in different HAT samples. |
Both univariate and multivariate logistic regression analyses indicated that CD4+ T cell count <200 cell/μL (OR=1.003, 95% CI=1.001–1.005, P=0.001) was a significant risk factor for the occurrence of HAT. Although high viral load (P=0.200) showed an association with HAT occurrence, it did not reach statistical significance, consistent with the earlier findings. Notably, a majority of patients with advanced age (70.49%), high viral load (65.33%), and low CD4+ T cell count (64.52%) were observed in the mild thrombocytopenia group.
The Clinical and Laboratory Characteristics of HAT with Neuroinflammation
Among the 1998 patients, 22 individuals experienced HAT with neuroinflammation, resulting in a prevalence of 1.10% (22/1998). The majority of these patients sought medical attention from the emergency department (63.64%, 14/22). Neuropsychiatric symptoms were the predominant newly diagnosed symptoms, including headache (27.27%, 6/22), dizziness (22.73%, 5/22), disturbance of consciousness (18.18%, 4/22), and intracranial infection (18.18%, 4/22). Regarding laboratory characteristics, 15 patients underwent CSF biochemical testing, and 13 patients had serum IL-6 results. Among these, 73.33% (11/15) exhibited elevated levels of total trace protein beyond normal, and 84.62% (11/13) showed elevated levels of IL-6 exceeding normal ranges. In comparison to HAT patients without neuroinflammation, HAT with neuroinflammation were predominantly male (X2=10.066, P=0.007), had higher viral loads (X2=12.297, P=0.006), and were of advanced age (X2=11.721, P=0.02). Although there was no statistically significant difference in CD4+ T cell count, the results indicated lower CD4+ T cell counts in HAT with neuroinflammation patients. Table 2 and Figure 3 provided a detailed comparison between HAT with and without neuroinflammation.
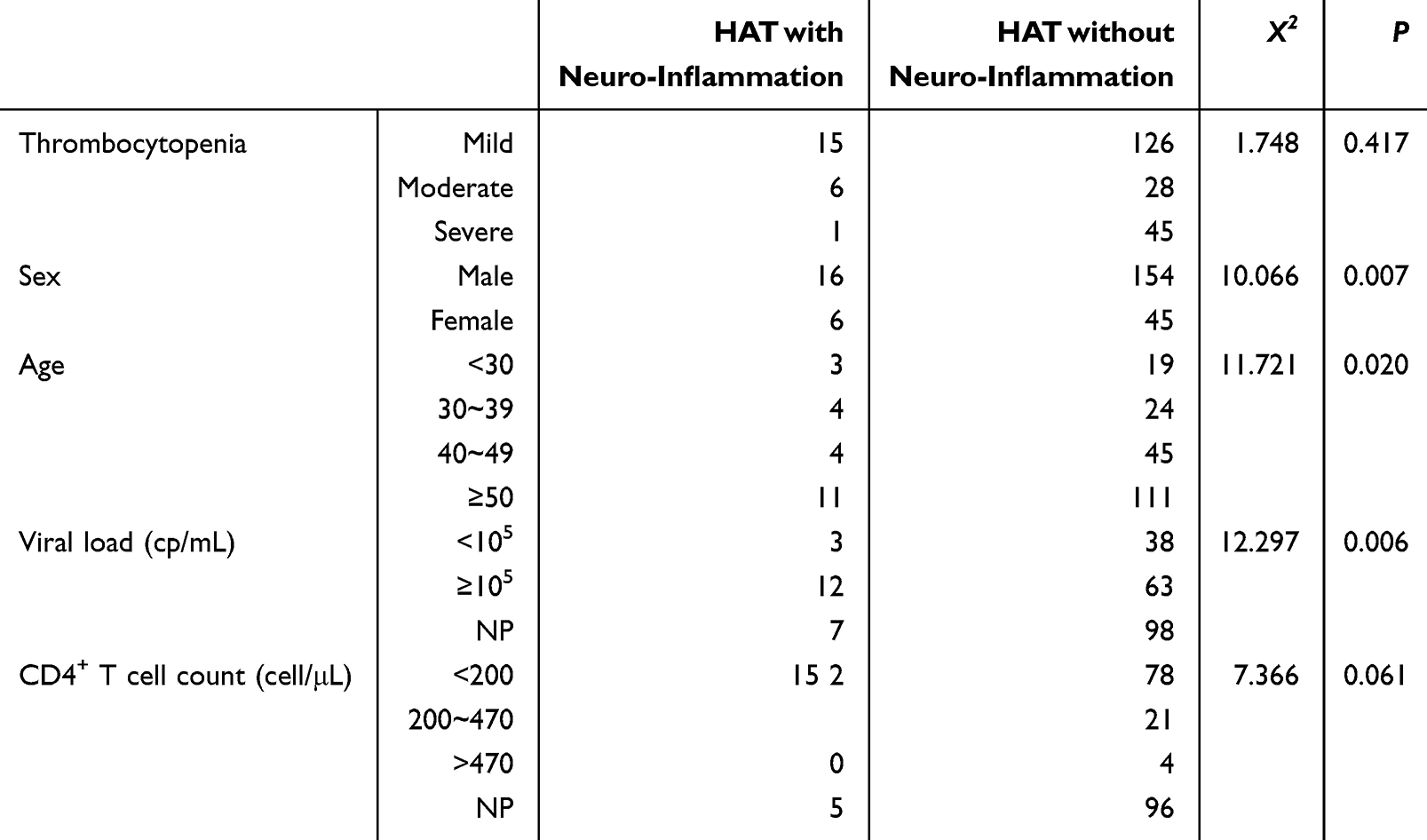 |
Table 2 Comparison Between HAT with and without Neuroinflammation |
 |
Figure 3 Comparison between HAT with and without neuroinflammation. (A) Comparison in age. (B) Comparison in viral load. (C) Comparison in CD4+ T cell count. |
Discussion
Sichuan province is recognized for having one of the highest rates of HIV-1 infection in China, coupled with a notably high incidence of thrombocytopenia.9,10 Thrombocytopenia, a prevalent hematological disorder, can often manifest as the initial clinical indication in individuals with HIV-1 infection. This study revealed an HAT prevalence of 11.06%, which agrees with findings in other publications ranging from 10.00% to 30.00%,11–16 including China. The prevalence observed in our study was similar to that of HIV-1-associated tumors and HIV-1-associated fungal infections but lower than that of HIV-1-associated tuberculosis.17–20 These results underscore that thrombocytopenia occurs more frequently in HIV-1-infected individuals, particularly before commencing antiretroviral therapy, when compared to the general population.1 The majority of HAT patients were male, elderly, and exhibited high COI values. In the context of HAT, males constituted the demographic with the highest prevalence of HIV-1 infection.21,22 Elderly patients often present with more severe illnesses and underlying health issues, which can contribute to various HIV-1 infection-related complications, including HAT.23 Elevated COI levels likely signify an early stage of infection and rapid viral replication, leading to abnormal megakaryocyte differentiation, viral-induced inhibition of hematopoietic stem cell proliferation, and cytokine imbalances.24
The results demonstrated significant differences in CD4+ T cell count, PCT, and P-LCR between the HAT group and the control group. PLT, PCT, P-LCR, and PDW, which respectively represent platelet quantity, size, degree of variation, and the proportion of large platelets, are recognized as markers of platelet activation.25 PCT serves as an indicator of platelet activation, and a simultaneous decrease in PLT and PCT indicates excessive platelet consumption.26 Furthermore, elevated P-LCR levels suggest an increase in newly formed or relatively immature platelets characterized by larger volumes, denser particles, and heightened activity that respond vigorously to inflammatory mediators or pro-inflammatory chemokines.27 Therefore, our findings indicated that viral infection led to reductions in PLT and PCT, prompting increased platelet activation and production, resulting in elevated P-LCR.
As observed in our study, a significantly low CD4+ T cell count (<200 cell/μL) emerged as a key factor driving HAT. Lower CD4+ T cell counts have been associated with an elevated risk of thrombocytopenia in prior research.3,28,29 One study found that among homosexual males, a decline in PLT count was indicative of a sharp drop in CD4+ T cell counts.3 Additionally, advanced age and high viral load closely correlated with the occurrence of HAT, consistent with previous investigations.3,28,29 High viral load suggests active viral replication, while a low CD4+ T cell count signals immune system deterioration. A decline in platelets and blood cells signifies a rapid deterioration in the patient’s condition, heightening the risk of infection by bacteria, fungi, and viruses, among other pathogens.
Furthermore, this study delved into HAT with neuroinflammation, primarily characterized by clinical symptoms such as headaches, dizziness, and disturbances in consciousness, among others. HIV-1-associated neurocognitive disorders (HAND) are significant complications representing end-organ manifestations of HIV-1 infection. Neuroinflammation serves as a precursor phenotype for HAND and can be challenging to diagnose, warranting attention. When compared to HAT cases without neuroinflammation, HAT with neuroinflammation patients shared common traits, including advanced age and higher viral load. Additionally, it was observed that HAT with neuroinflammation patients had lower CD4+ T cell counts and elevated levels of proteins in CSF and IL-6 in serum. The elevation of CSF protein levels is particularly concerning, especially considering that some studies have indicated that elevated β2-microglobulin levels in CSF are significant predictors of AIDS-related dementia.30,31 According to several pieces of research, HIV-1 does not directly harm neurons but can infect peripheral blood monocytes, traverse the BBB, and enter brain tissue. Moreover, platelets can influence the integrity and permeability of the BBB in vitro, exacerbating its breakdown.32–35 Subsequently, HIV-1 expresses neurotoxic compounds such as gp120, Tat, and Nef proteins to enhance neurotoxicity and induce neuroinflammation, resulting in increased levels of inflammatory factors like TNF-α and IL-6.34,36–39 Furthermore, one of the mechanisms through which HIV-1 exerts neurotoxicity involves the interaction between HIV-1 and monocyte-platelet aggregates, leading to abnormal platelet activation and thrombocytopenia.40,41
Our study has certain limitations due to its retrospective design. Firstly, being a single-center study, it may not provide a comprehensive representation of the epidemiology of HAT and HAT with neuroinflammation. Secondly, some data, such as viral load, CD4+ T cell count, and platelet parameters, were partially missing.
Conclusions
In conclusion, the presence of HAT and HAT with neuroinflammation should not be overlooked in HIV-1 infection. Thrombocytopenia can be attributed to abnormal platelet activation, leading to reduced PCT and elevated P-LCR. Elevated levels of inflammatory substances and proteins induced by HIV-1’s neurotoxicity contribute to neuroinflammation-related symptoms and a more unfavorable prognosis. Therefore, for HAT patient, it is necessary to be vigilant about the virus’s damage to the BBB, which can develop into neuroinflammation. Conversely, patients with thrombocytopenia accompanied by neuroinflammation can be further screened for HIV infection. Therefore, this research offers valuable insights into the condition and its diagnosis. Furthermore, diagnostic methods and pathogenesis warrant further investigation.
Ethics Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of West China Hospital of Sichuan University (approval number: 2020742). The study involved only clinically remaining samples, and it was difficult to contact the subjects. After review by the ethics committee, it was considered that the study was not greater than the minimum risk, and it was agreed to waive informed consent.
Acknowledgments
This work was supported by the National Natural Science Foundation of China (82102485, Z.W.).
Disclosure
The authors declare that there is no conflict of interest of the research reported. This paper has been uploaded to Biorxiv as a preprint: https://www.biorxiv.org/content/biorxiv/early/2022/11/10/2022.11.09.515900.full.pdf.
References
1. Li B, Zhang L, Liu Y, et al. Manifestations and related risk factors of thrombocyte abnormalities in HIV-positive patients before and after the initiation of ART. Infect Drug Resist. 2021;14:4809–4819. doi:10.2147/IDR.S334046
2. Shen Y, Wang J, Wang Z, et al. A cross-sectional study of leukopenia and thrombocytopenia among Chinese adults with newly diagnosed HIV/AIDS. Biosci Trends. 2015;9(2):91–96. doi:10.5582/bst.2015.01024
3. Fan HW, Guo FP, Li YJ, et al. Prevalence of thrombocytopenia among Chinese adult antiretroviral-naïve HIV-positive patients. Chin Med J. 2015;128(4):459–464. doi:10.4103/0366-6999.151078
4. Ambler KL, Vickars LM, Leger CS, et al. Clinical features, treatment, and outcome of HIV-associated immune thrombocytopenia in the HAART era. Adv Hematol. 2012;2012:910954. doi:10.1155/2012/910954
5. Raadsen M, Du Toit J, Langerak T, et al. Thrombocytopenia in virus infections. J Clin Med. 2021;10(4):877. doi:10.3390/jcm10040877
6. Zhang YL, Ouyang YB, Liu LG, et al. Blood-brain barrier and neuro-AIDS. Eur Rev Med Pharmacol Sci. 2015;19(24):4927–4939.
7. Rom S, Gajghate S, Winfield M, et al. Combination of HIV-1 and diabetes enhances blood brain barrier injury via effects on brain endothelium and pericytes. Int J Mol Sci. 2020;21(13):4663. doi:10.3390/ijms21134663
8. Fernandes N, Pulliam L. Inflammatory mechanisms and cascades contributing to neurocognitive impairment in HIV/AIDS. Curr Top Behav Neurosci. 2021;50:77–103. doi:10.1007/7854_2019_100
9. Zhou Q, Wu W, Yi M, et al. HIV knowledge, sexual practices, condom use and its associated factors among international students in one province of China: a cross-sectional study. BMJ Open. 2022;12(8):e058108. doi:10.1136/bmjopen-2021-058108
10. Zhou C, Liang S, Li Y, et al. Characterization of HIV-1 molecular epidemiology and transmitted drug-resistance in newly diagnosed HIV-infected patients in Sichuan, China. BMC Infect Dis. 2022;22(1):602. doi:10.1186/s12879-022-07576-z
11. Akdag D, Knudsen AD, Thudium RF, et al. Increased risk of anemia, neutropenia, and thrombocytopenia in people with human immunodeficiency virus and well-controlled viral replication. J Infect Dis. 2019;220(11):1834–1842. doi:10.1093/infdis/jiz394
12. Bisetegn H, Ebrahim H. The prevalence of thrombocytopenia and leucopenia among people living with HIV/AIDS in Ethiopia: a systematic review and meta-analysis. PLoS One. 2021;16(9):e0257630. doi:10.1371/journal.pone.0257630
13. Getawa S, Aynalem M, Bayleyegn B, et al. The global prevalence of thrombocytopenia among HIV-infected adults: a systematic review and meta-analysis. Int J Infect Dis. 2021;105:495–504. doi:10.1016/j.ijid.2021.02.118
14. Durandt C, Potgieter JC, Mellet J, et al. HIV and haematopoiesis. S Afr Med J. 2019;109(8b):40–45. doi:10.7196/SAMJ.2019.v109i8b.13829
15. Deressa T, Damtie D, Workineh M, et al. Anemia and thrombocytopenia in the cohort of HIV-infected adults in northwest Ethiopia: a facility-based cross-sectional study. EJIFCC. 2018;29(1):36–47.
16. Woldeamanuel GG, Wondimu DH. Prevalence of thrombocytopenia before and after initiation of HAART among HIV infected patients at black lion specialized hospital, Addis Ababa, Ethiopia: a cross sectional study. BMC Hematol. 2018;18:9. doi:10.1186/s12878-018-0103-6
17. Atallah-Yunes SA, Murphy DJ, Noy A. HIV-associated Burkitt lymphoma. Lancet Haematol. 2020;7(8):e594–e600. doi:10.1016/S2352-3026(20)30126-5
18. Carbone A, Vaccher E, Gloghini A. Hematologic cancers in individuals infected by HIV. Blood. 2022;139(7):995–1012. doi:10.1182/blood.2020005469
19. Ying RS, Le T, Cai WP, et al. Clinical epidemiology and outcome of HIV-associated talaromycosis in Guangdong, China, during 2011–2017. HIV Med. 2020;21(11):729–738. doi:10.1111/hiv.13024
20. Martino RJ, Chirenda J, Mujuru HA, et al. Characteristics indicative of tuberculosis/HIV coinfection in a high-burden setting: lessons from 13,802 incident tuberculosis cases in Harare, Zimbabwe. Am J Trop Med Hyg. 2020;103(1):214–220. doi:10.4269/ajtmh.19-0856
21. Sharma AL, Singh TR, Devi KR, et al. Molecular epidemiology of HIV-1 among the HIV infected people of Manipur, Northeastern India: emergence of unique recombinant forms. J Med Virol. 2017;89(6):989–999. doi:10.1002/jmv.24738
22. McCutchan FE. Global epidemiology of HIV. J Med Virol. 2006;78(Suppl 1):S7–S12. doi:10.1002/jmv.20599
23. Shamu T, Chimbetete C, Egger M, et al. Treatment outcomes in HIV infected patients older than 50 years attending an HIV clinic in Harare, Zimbabwe: a cohort study. PLoS One. 2021;16(6):e0253000. doi:10.1371/journal.pone.0253000
24. Pretorius E. Platelets in HIV: a guardian of host defence or transient reservoir of the virus? Front Immunol. 2021;12:649465. doi:10.3389/fimmu.2021.649465
25. Wysokiński A, Szczepocka E. Platelet parameters (PLT, MPV, P-LCR) in patients with schizophrenia, unipolar depression and bipolar disorder. Psychiatry Res. 2016;237:238–245. doi:10.1016/j.psychres
26. Zhang S, Cui YL, Diao MY, et al. Use of platelet indices for determining illness severity and predicting prognosis in critically ill patients. Chin Med J. 2015;128(15):2012–2018. doi:10.4103/0366-6999.161346
27. Chen Q, Chen Y, Zhang Y, et al. Prognostic impact of platelet-large cell ratio in myelodysplastic syndromes. Front Oncol. 2022;1(12):846044. doi:10.3389/fonc.2022.846044
28. Nka AD, Sosso SM, Fokam J, et al. Thrombocytopenia according to antiretroviral drug combinations, viremia and CD4 lymphocytes among HIV-infected patients in Cameroon: a snapshot from the City of Yaoundé. BMC Res Notes. 2019;12(1):632. doi:10.1186/s13104-019-4664-7
29. Talargia F, Getacher L. Thrombocytopenia and associated factors among HIV infected patients in pre- and post-anti-retroviral therapy, North East Ethiopia. J Blood Med. 2021;12:741–748. doi:10.2147/JBM.S323086
30. Gomez D, Power C, Gill MJ, et al. Empiric neurocognitive performance profile discovery and interpretation in HIV infection. J Neurovirol. 2019;25(1):72–84. doi:10.1007/s13365-018-0685-6
31. Landi C, Santinelli L, Bianchi L, et al. Cognitive impairment and CSF proteome modification after oral bacteriotherapy in HIV patients. J Neurovirol. 2020;26(1):95–106. doi:10.1007/s13365-019-00801-7
32. Nair M, Maria JM, Agudelo M, et al. Platelets contribute to BBB disruption induced by HIV and alcohol. J Alcohol Drug Depend. 2015;3(1):182. doi:10.4172/2329-6488.1000182
33. Sweeney MD, Sagare AP, Zlokovic BV. Blood-brain barrier breakdown in Alzheimer disease and other neurodegenerative disorders. Nat Rev Neurol. 2018;14(3):133–150. doi:10.1038/nrneurol.2017.188
34. McRae M. HIV and viral protein effects on the blood brain barrier. Tissue Barriers. 2016;4(1):e1143543. doi:10.1080/21688370.2016.1143543
35. Barker CT, Vaidya NK. Modeling HIV-1 infection in the brain. PLoS Comput Biol. 2020;16(11):e1008305. doi:10.1371/journal.pcbi.1008305
36. Huang J, Zhang R, Wang S, et al. Methamphetamine and HIV-Tat protein synergistically induce oxidative stress and blood-brain barrier damage via transient receptor potential melastatin 2 channel. Front Pharmacol. 2021;12:619436. doi:10.3389/fphar.2021.619436
37. Karampoor S, Zahednasab H, Bokharaei-Salim F, et al. HIV-1 Tat protein attenuates the clinical course of experimental autoimmune encephalomyelitis (EAE). Int Immunopharmacol. 2020;78:105943. doi:10.1016/j.intimp.2019.105943
38. Louboutin JP, Strayer DS. Blood-brain barrier abnormalities caused by HIV-1 gp120: mechanistic and therapeutic implications. Sci World J. 2012;2012:482575. doi:10.1100/2012/482575
39. Bhargavan B, Kanmogne GD. Toll-like receptor-3 mediates HIV-1-induced interleukin-6 expression in the human brain endothelium via TAK1 and JNK pathways: implications for viral neuropathogenesis. Mol Neurobiol. 2018;55(7):5976–5992. doi:10.1007/s12035-017-0816-8
40. Dahal S, Chitti SV, Nair MP, et al. Interactive effects of cocaine on HIV infection: implication in HIV-associated neurocognitive disorder and neuroAIDS. Front Microbiol. 2015;6:931. doi:10.3389/fmicb.2015.00931
41. Singh MV, Davidson DC, Jackson JW, et al. Characterization of platelet-monocyte complexes in HIV-1-infected individuals: possible role in HIV-associated neuroinflammation. J Immunol. 2014;192(10):4674–4684. doi:10.4049/jimmunol.1302318
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prevalence, Clinical Manifestations, Treatment, and Clinical Course of Chronic Urticaria in Elderly: A Systematic Review
Kulthanan K, Rujitharanawong C, Munprom K, Trakanwittayarak S, Phumariyapong P, Prasertsook S, Ungprasert P
Journal of Asthma and Allergy 2022, 15:1455-1490
Published Date: 20 October 2022