")
Back to Journals » Drug Design, Development and Therapy » Volume 19
Analysis of Menopausal Hormone Therapy to Chinese Patients with Menopausal Syndrome: A Real-World Retrospective Study from Chinese Hospitals
Authors Zhu Z, Shi A, Liu L, Jin G, Wang X
Received 24 January 2025
Accepted for publication 29 May 2025
Published 4 June 2025 Volume 2025:19 Pages 4861—4873
DOI https://doi.org/10.2147/DDDT.S517420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Muzammal Hussain
Zhenling Zhu,1 Aiping Shi,1 Lanhua Liu,2 Guixiu Jin,2 Xianli Wang3
1Department of Pharmacy, Taixing People’s Hospital Affiliated to Yangzhou University, Jiangsu, Taixing, 225400, People’s Republic of China; 2Department of Obstetrics and Gynecology, Taixing People’s Hospital Affiliated to Yangzhou University, Jiangsu, Taixing, 225400, People’s Republic of China; 3Department of Pharmacy, Obstetrics and Gynecology Hospital of Fudan University, Shanghai, 200011, People’s Republic of China
Correspondence: Xianli Wang, Obstetrics and Gynecology Hospital of Fudan University, 419 Fangxie Road, Huangpu District, Shanghai, 200011, People’s Republic of China, Email [email protected]
Purpose: To investigate and analyse the changing trends in the use of menopausal hormone therapy (MHT) for patients with menopausal syndrome (MPS) in hospitals in nine Chinese cities from 2019 to 2023 and to provide an evidence base for the rational clinical use of MHT.
Methods: Data on the use of MHT by patients with menopausal syndrome were collected and a trend analysis was conducted, including trends in the number of prescriptions, patient age, total prescription amount, average prescription amount, defined daily doses (DDDs), defined daily cost (DDC), and drug rank ratio (B/A).
Results: From 2019 to 2023, the prescriptions of MPS patient were concentrated in East China and North China, with an average age of 48.22± 5.94 years. In a span of five years, the number of prescriptions increased by 86.08%, the total prescription amount increased by 126.58%, and the average prescription amount increased by 21.76%. The B/A ratios for estradiol/estradiol dydrogesterone and tibolone were both determined to be 1, thus indicating that the sales amounts and DDDs of these two drugs were in good agreement and that the drug costs are reasonable.
Conclusion: From 2019 to 2023, the number of MPS patients and the total number of treatment drug prescriptions in nine cities throughout the country demonstrated an increasing trend. The estradiol/estradiol dydrogesterone and tibolone were the main sex hormone drugs that were used to treat MPS. The state’s abolition of the drug price addition policy and the organization of centralized drug procurement in some areas had alleviated the financial burdens on patients to a certain extent.
Keywords: menopausal syndrome, menopausal hormone therapy, estradiol/estradiol dydrogesterone, tibolone
Introduction
Menopause syndrome (MPS) refers to a series of clinical symptoms triggered by hormonal fluctuations due to ovarian function failure in women around the period of menopause.1,2 During the menopausal transition, approximately 50%–75% of women typically present with vasomotor symptoms such as hot flashes and night sweats,3 while more than 50% develop genitourinary symptoms. Postmenopausal manifestations potentially emerging 10–15 years after menopause, including Alzheimer’s disease, obesity, metabolic syndrome, and osteoporosis,4 collectively impose severe impacts on women’s physical and psychological well-being. The average life expectancy for Chinese women has exceeded 80 years, with projections indicating it will surpass 85 years by 2035. This demographic shift implies that women will spend approximately one-third of their lifespan in the postmenopausal phase. Improving the quality of life of menopausal women has been indicated as one of the three major health issues in the 21st century. It is imperative to alleviate symptoms and address psychological burdens experienced by patients during this critical period.5–7
MHT not only provides rapid and effective relief of menopausal symptoms but also confers long-term health benefits.8 However, in China, there are significant differences in the allocation of medical resources in different regions, and there are gaps in healthcare knowledge and practices regarding menopausal care among medical professionals,9–11 social media institutions have various levels of publicity for menopausal treatment,12 patients undergoing treatment are concerned about the side effects of sex hormone therapy and the potential risk of cancer, in less economically developed regions, self-paying cost are a financial burden for patients (self-paying cost means that the patient pay the full cost of treatment),13,14 all of which lead to a low rate of visits by patients with MPS and a low rate of acceptance of MHT treatment. In developed countries across Europe and North America, the prevalence of MHT use among the general population is as high as 30–40%. Sex hormone therapy remains the primary approach for alleviating the most common menopausal symptoms, as supported by extensive clinical evidence.15,16 In contrast, current research in China predominantly focuses on the prevalence of menopausal syndrome, clinician-patient awareness dynamics, treatment-related attitudes, and medication adherence.17,18 There is limited data on the real-world utilization of MHT to patients with MPS in China. To address this gap and provide a basis for policy management, this study aims to evaluate the trends and patterns of MHT use across nine major cities in China from 2019 to 2023.
Materials and Methods
Data Sources
The research data originated from the “Hospital Prescription Analysis Cooperation Project” of the Hospital Pharmacy Committee of the Chinese Pharmaceutical Association. This project is a collaborative effort involving 104 hospitals across nine cities (Beijing, Shanghai, Guangzhou, Harbin, Shenyang, Chengdu, Hangzhou, Tianjin, and Zhengzhou), encompassing both urban and rural healthcare institutions. The participating hospitals include 3 primary hospitals, 9 secondary hospitals, and 92 tertiary hospitals. According to the Chinese medical technology level, primary hospitals, including community health centers and township hospitals, deliver essential medical services directly to local communities, acting as the closest healthcare providers to residents. Secondary hospitals serve as regional medical facilities providing comprehensive healthcare to multiple communities. Tertiary hospitals are specialized institutions providing advanced medical services, often serving patients across provincial or even national regions.19 Additionally, the hospitals were divided into 14 specialized hospitals and 90 comprehensive hospitals according to their scope of treatment. Prescription data for 10 working days (40 working days for 4 quarters, 240 working days for 5 years) were randomly collected from each hospital information system in each quarter. The electronic information on outpatient prescriptions for 10 working days in each quarter was aggregated and included in the prescription database of the “Hospital Prescription Analysis Cooperation Project”.
Survey Method
Prescription data of female outpatients diagnoses including “premature ovarian failure” or “premature ovarian insufficiency” or “ovarian dysfunction” or “menopause” or “POF” or “POI” in the database from January 1, 2019, to December 31, 2023, were extracted. According to the Stages of Reproductive Aging Workshop +10 (STRAW+10) criteria, perimenopause begins with the transition period (early transition) and ends 1 year after menopause,20 the Chinese guidelines point out that symptoms of menopause require vigilance for premature low estrogen condition such as POI.1 MHT is not recommended in principle for women over 60 years of age or for those who have been menopausal for more than 10 years.16 Therefore, this study included a patient population aged 35–60 years. The extracted data included region, time, patient code, department name, reimbursement category, sex, age, original diagnostic drug code, generic name, trade name, specification, quantity, unit price, usage and dosage, and prescription amount. Missing data, inconsistencies, and prescriptions not containing sex hormone medications were excluded from this study. The clinician has ruled out MHT contraindications before prescribing, and the prescription included in this study does not contain MHT contraindications.
Research Indicators and Methods
The ATC/DDD, which was compiled by the Center for Drug Statistics of the World Health Organization (WHO), was adopted. It classifies drugs based on different tissues or systems, as well as drug treatments, pharmacology, and chemical properties.21 DDD is a standardized unit of measurement that represents the average value, which refers to the average daily dose of a drug that is used for the main therapeutic purpose in adults. According to the 2020 edition of the Chinese Pharmacopeia Guidelines for Clinical Drug Use, data from the WHO website and the provisions of the drug instructions, the frequency of drug prescriptions, and the amounts of the prescribed drugs are counted according to the generic names of the drugs. The defined daily doses (DDDs), defined daily cost (DDC), and drug rank ratio (B/A) are subsequently calculated and analysed.
DDDs is calculated as the annual total prescription dosage/DDD value of the drug, with a higher value indicating a greater clinical preference for the drug. DDC is calculated as the annual total prescription amount of the drug/DDDs of the drug, thus indicating the average daily cost of the drug, which represents the price level of the drug. A higher DDC value corresponds to a higher price of the medicine and a greater financial burden on the patient. B/A = the sales amount ranking (B) / DDDs ranking (A). B/A value closer to 1 indicates better synchronism between the sales amount and DDDs of the drug, thus indicating a more reasonable drug costs. Moreover, a higher B/A ratio indicates a lower price, which corresponds to a higher usage rate; conversely, a lower B/A ratio indicates a higher price, which corresponds to a lower usage rate.
Statistical Methods
Microsoft Excel 2019 was used to perform the subgroup analysis of MPS patients based on age, city, and drug classification, among other factors. Statistical analysis focused on the prescription mode of the therapeutic drugs. The results are expressed as either several cases or percentages (n, %).
Results
Demographic Characteristics of the Patients
The average age of the individuals seeking medical treatment was 48.22±5.94 years, with the age distribution mainly concentrated in the 46–50 years age group (30.07%) and the 51–55 years age group (27.31%), followed by the 41–45 years age group (19.13%). The proportions of individuals aged 35–40 years and 56–60 years were similar (Figure 1). The use of MHT in patients of different ages demonstrates specific characteristics. The estradiol/estradiol dydrogesterone was most frequently prescribed in the 35–50-year-old age group, whereas tibolone was most frequently prescribed in the 51–60-year-old age group (Table 1).
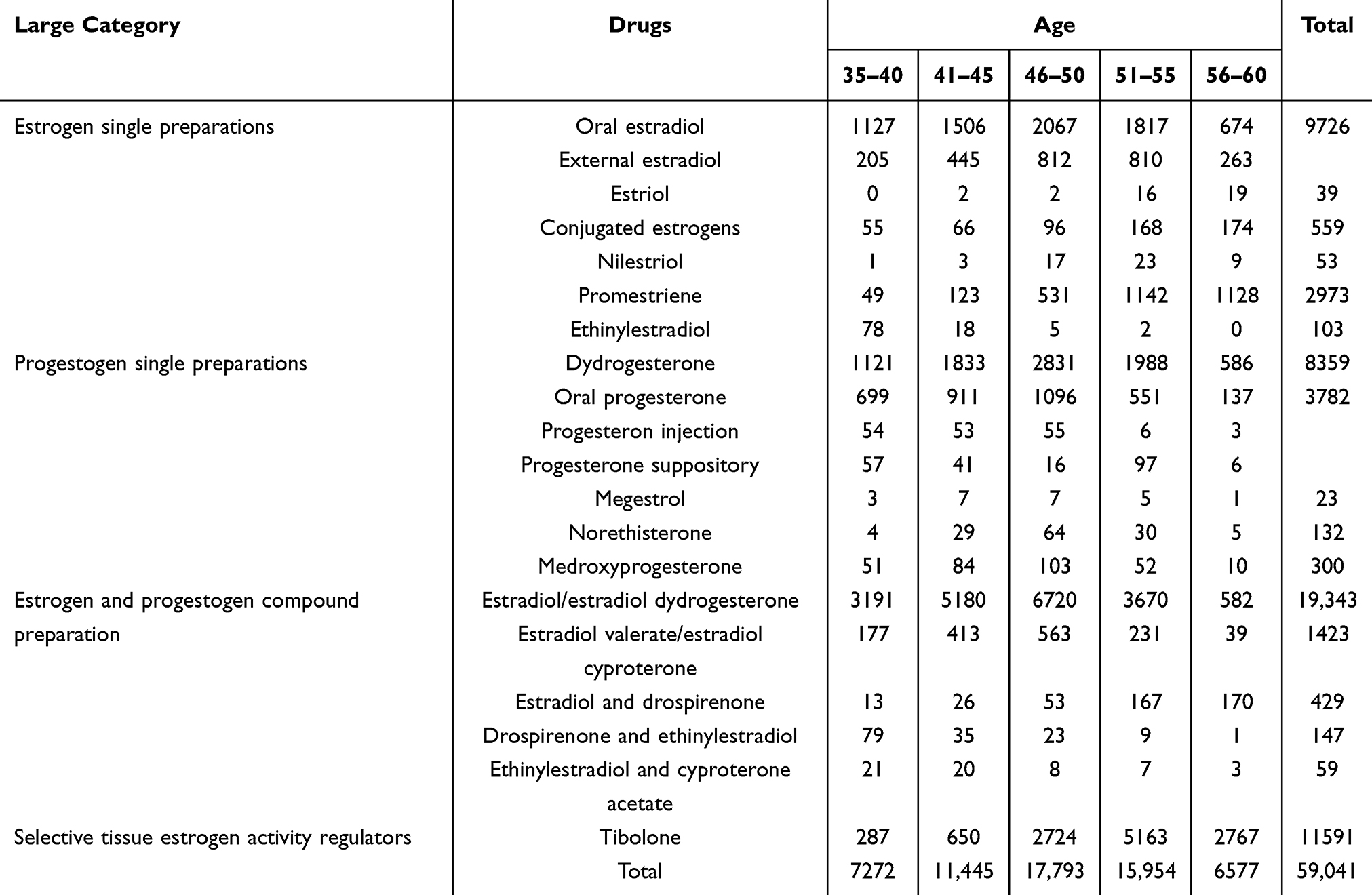 |
Table 1 Age Distribution of Patients with Menopausal Syndrome Using MHT from 2019 to 2023 |
 |
Figure 1 Age distribution of patients with menopausal syndrome from 2019 to 2023. |
The nine cities that were involved in the study belong to six geographical regions in China: East China (Hangzhou, Shanghai), South China (Guangzhou), Central China (Zhengzhou), North China (Beijing, Tianjin), Southwest China (Chengdu), and Northeast China (Shenyang, Harbin). The number of sampled hospitals for this study originated from East China (27), South China (11), Central China (11), North China (22), Southwest China (8), and Northeast China (25). The distribution of the prescriptions in each region was as follows: East China (38.53%), South China (17.08%), Central China (4.27%), North China (27.48%), Southwest China (7.67%), and Northeast China (4.97%). The sampled prescriptions were mainly concentrated in East China, followed by North China (Figure 2).
 |
Figure 2 Regional distribution of patients with menopausal syndrome from 2019 to 2023. |
Prescription Patterns of MHT
From 2019 to 2023, there was a total of four major types of MHT prescribed for menopausal syndrome patients in nine cities throughout the country: estrogen single preparations (oral estradiol, external estradiol, estriol, conjugated estrogens, nilestriol, promestriene, and ethinylestradiol), progestogen single preparations (dydrogesterone, oral progesterone, progesterone injection, progesterone suppository, megestrol, norethisterone, and medroxyprogesterone), estrogen and progestogen compound preparations (estradiol/estradiol dydrogesterone, estradiol valerate/estradiol cyproterone, estradiol and drospirenone, drospirenone and ethinylestradiol, and ethinylestradiol and cyproterone acetate), and selective tissue estrogen activity regulators (tibolone). Among all of the therapeutic drugs, estrogen and progestogen compound preparations were most frequently prescribed (36.25%), followed by estrogen single preparations (22.79%), progestogen single preparations (21.33%), selective tissue estrogen activity regulators (19.63%). The estradiol/estradiol dydrogesterone, tibolone, estradiol, dydrogesterone and progesterone were deemed to be high for single drugs. Among these drugs, the prescription frequency of the estradiol/estradiol dydrogesterone has ranked first since 2019 (Table 2).
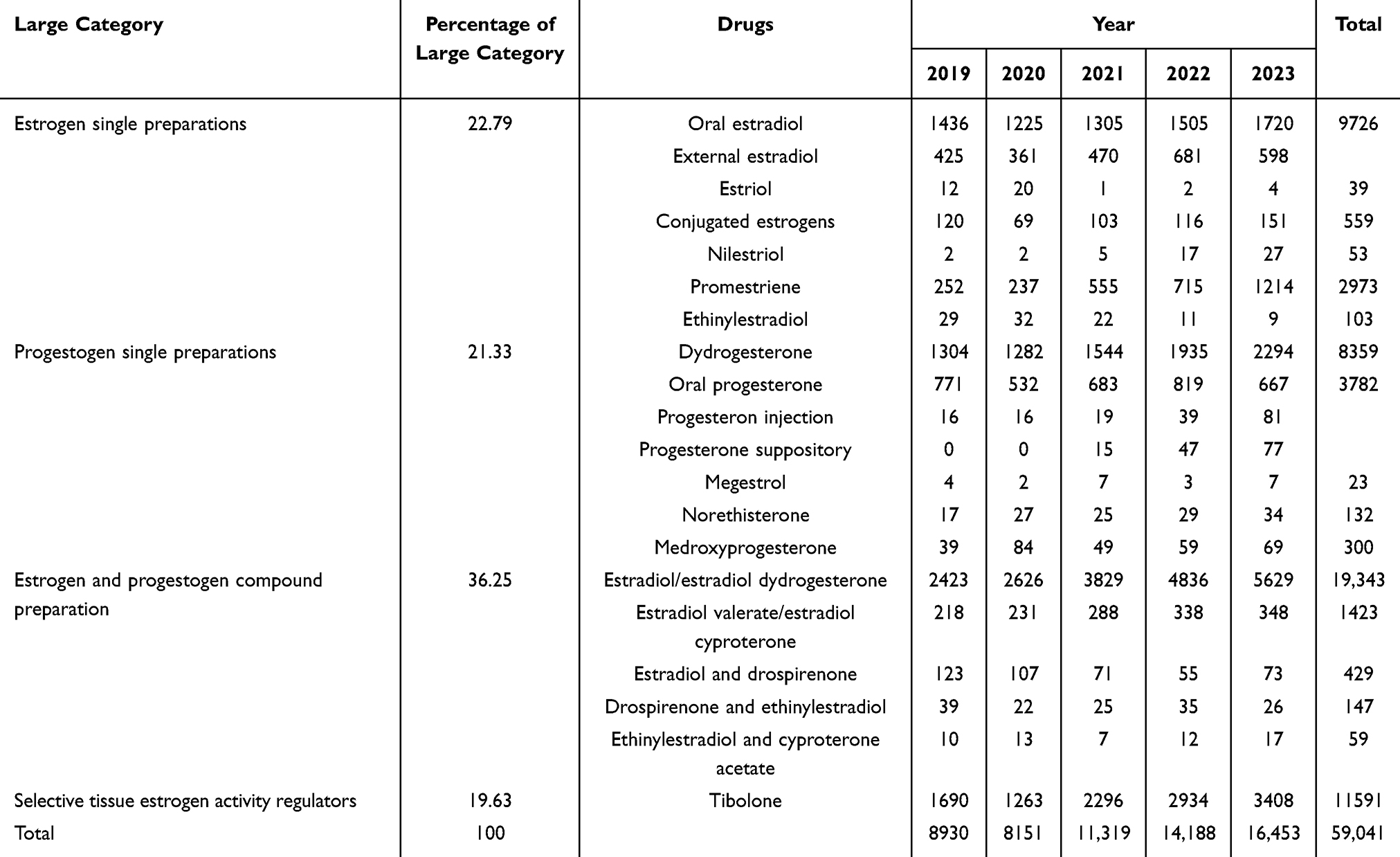 |
Table 2 Classification and Proportion of MHT for Patients with Menopausal Syndrome from 2019 to 2023 |
Analysis of Trends in the Number of Prescriptions, Total Prescription Amounts, and Average Prescription Amounts of MHT
After excluding prescriptions lacking treatment with MHT, the total number of prescriptions for MHT in nine cities throughout the country from 2019 to 2023 was 49,346, which represented an increase of 86.08% over the five years. Compared with that in 2019, the number of prescriptions in 2020 decreased by 8.36%, and the number of prescriptions in 2021 increased by 27.83% (Table 3).
 |
Table 3 Number of Prescriptions, Annual Total Prescription Amount, and Average Annual Prescription Amount of MHT for Patients with Menopausal Syndrome from 2019 to 2023 |
The annual total prescription amount demonstrated a fluctuating upward trend, whereby it increased from CNY 0.9193 million in 2019 to CNY 2.0829 million in 2023, which represented an increase of 126.58% over five years. The average annual prescription amount began to significantly decline in 2022, with a decrease of 1.71% compared with that in 2021; afterwards, it rebounded in 2023, with a total increase of 21.76% indicated over five years (Table 3).
DDDs Values of MHT
Among the MHT that were used in nine cities throughout the country from 2019 to 2023, estrogen and progestogen compound preparations ranked first in DDDs, followed by estrogen single preparations. The estradiol/estradiol dydrogesterone, tibolone, dydrogesterone, estradiol, and progesterone was deemed to be high for single drugs. The specific results are shown in Table 4.
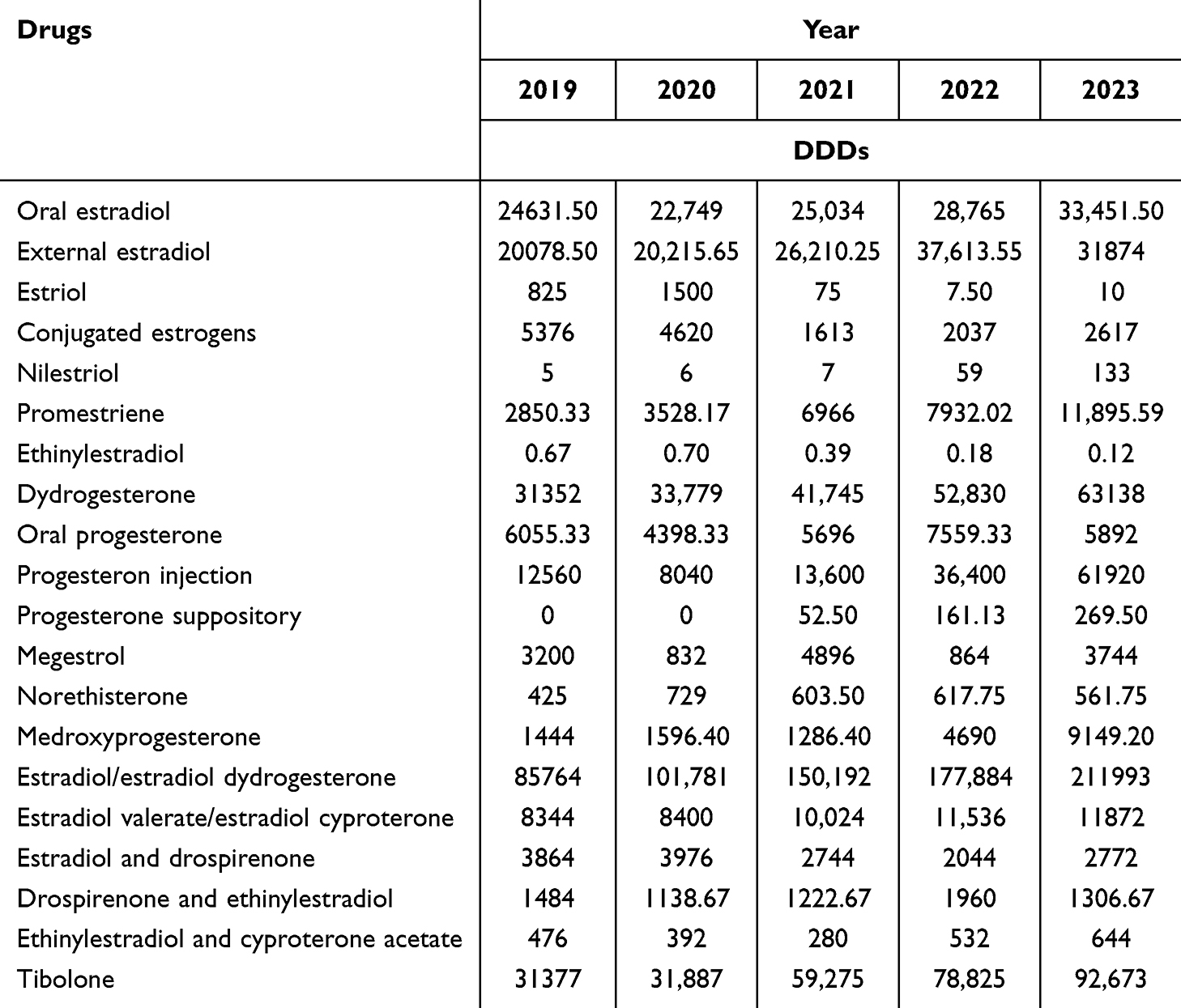 |
Table 4 DDDs of MHT for Patients with Menopausal Syndrome from 2019 to 2023 |
The Top 10 Sex Hormone Drugs by Amount of Drug Consumed, DDC Values, and B/A
From 2019 to 2023, among the MHT that were used in nine cities throughout China, the consumption of these nine drugs consistently ranked in the top ten of most consumed drugs, including estradiol/estradiol dydrogesterone, tibolone, dydrogesterone, external estradiol, oral estradiol, oral progesterone, estradiol valerate/estradiol cyproterone, and estradiol and drospirenone. Tibolone has increased from fourth place to second place with respect to ranking, and the estradiol/estradiol dydrogesterone has been ranked in first place for five years, thus indicating stability. The specific results are shown in Table 5.
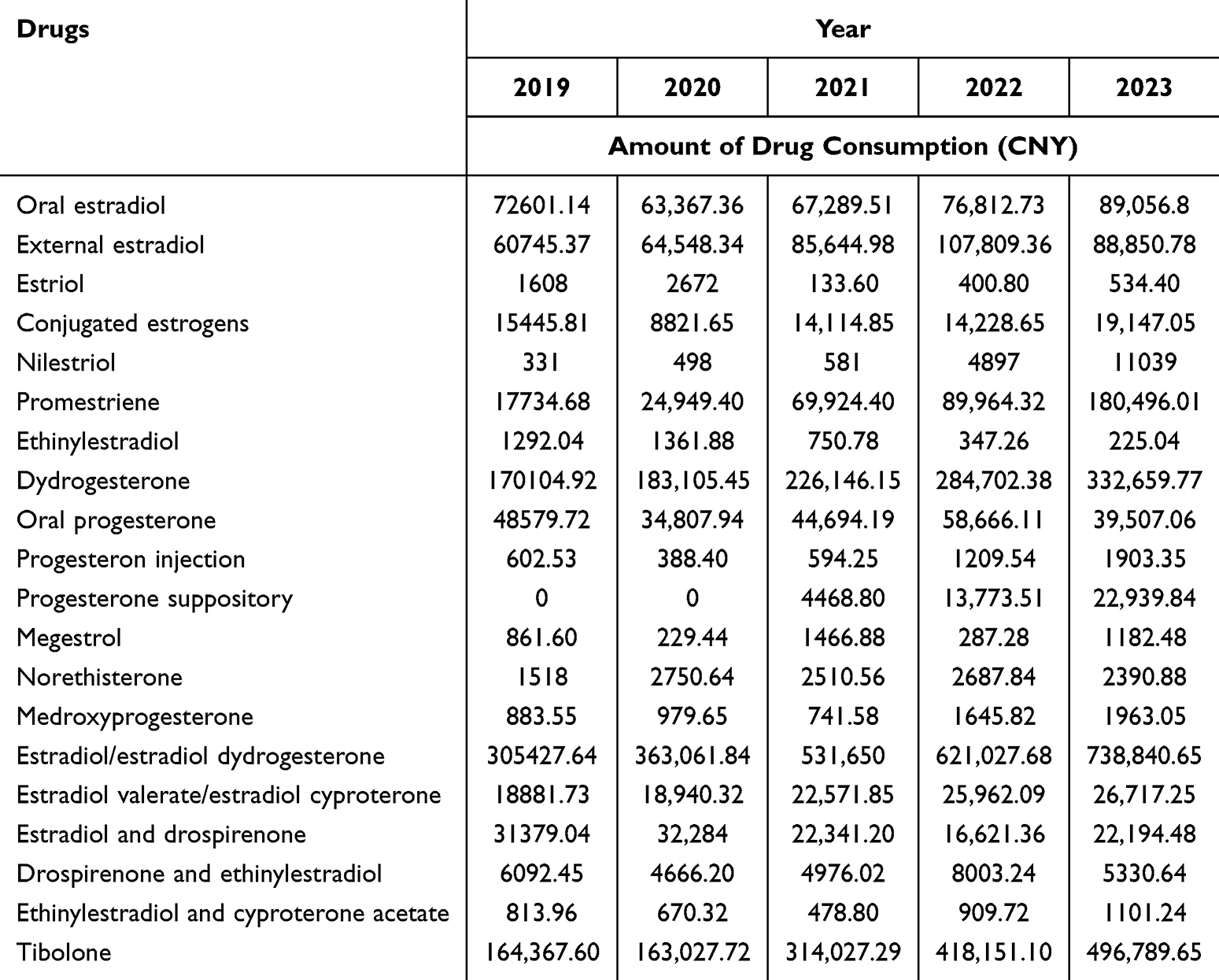 |
Table 5 Consumption Amount of MHT for Patients with Menopausal Syndrome from 2019 to 2023 |
Among all of the sex hormone drugs, the DDC of estradiol/estradiol dydrogesterone was approximately CNY 3.4 per day, and the B/A=1. The DDC of tibolone was approximately CNY 5.2 per day, and the B/A=1 after 2021, thus indicating that the sales amounts and DDDs of the two drugs are in good agreement and that the drug costs are reasonable. The B/A ratios of most of the other drugs were greater than 1, thus indicating that the drugs are relatively inexpensive and are frequently used. Among them, the DDC value of estradiol valerate/estradiol cyproterone was the lowest at approximately 2.25 yuan per day. The specific results are shown in Tables 6 and 7.
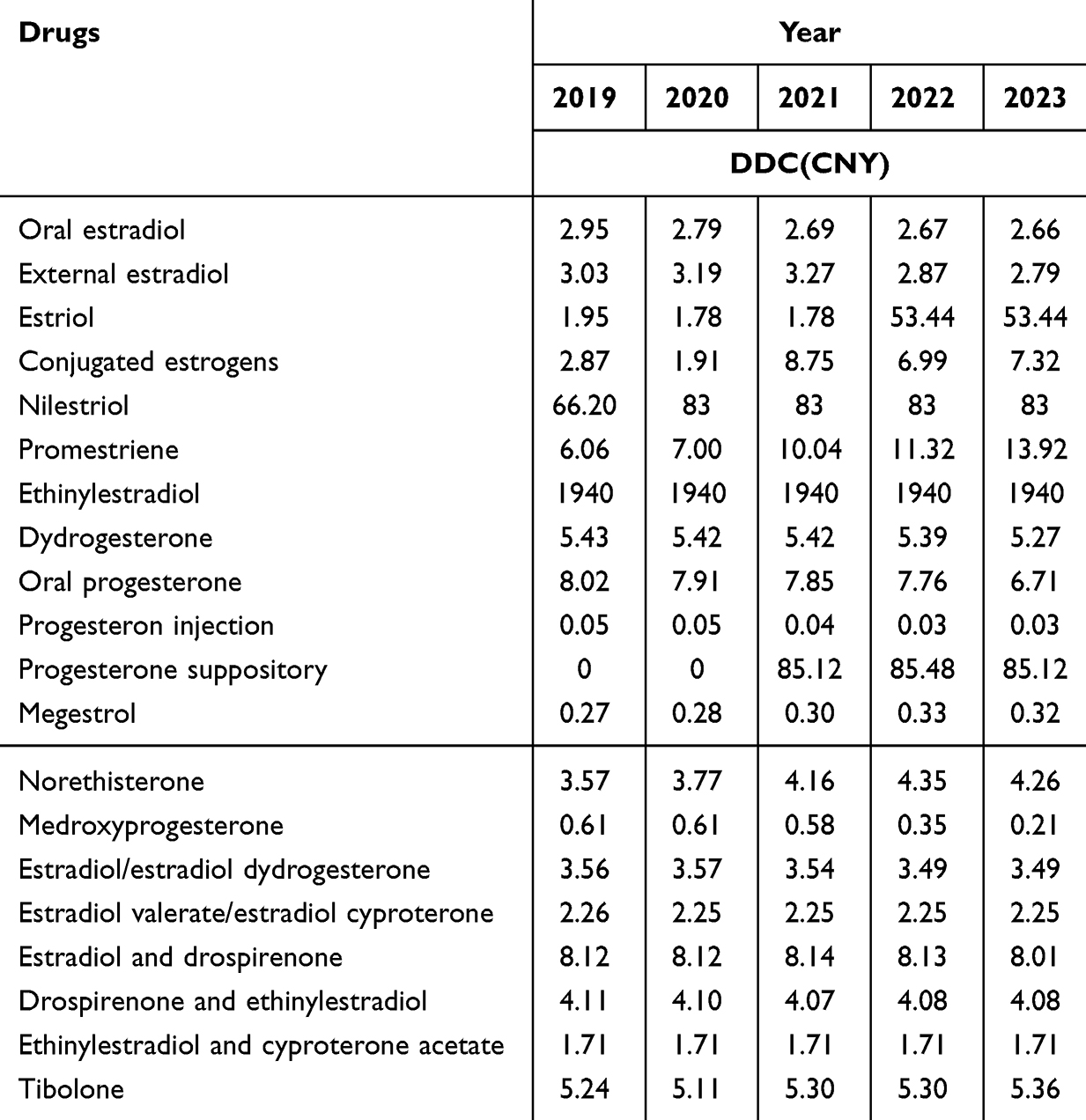 |
Table 6 DDC of MHT for Patients with Menopausal Syndrome from 2019 to 2023 |
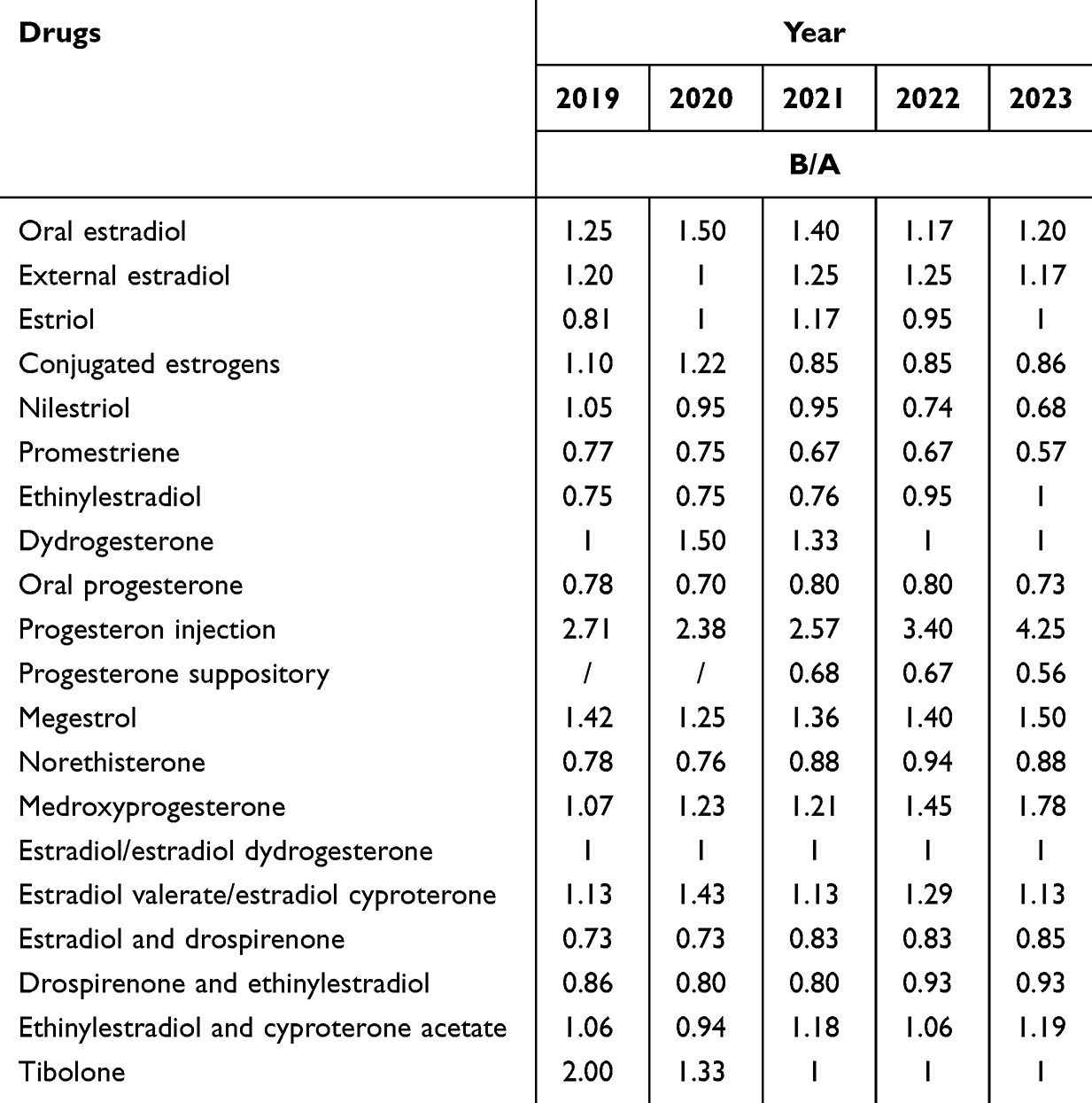 |
Table 7 B/A of MHT for Patients with Menopausal Syndrome from 2019 to 2023 |
Discussion
According to the background of population ageing, an improvement in the quality of life of MPS patients, as well as reductions in the incidence of MPS, are public health problems that cannot be ignored in China. In this study, the utilized outpatient prescription data encompassed hospitals in China with different levels of medical technology and scopes of treatment; this scenario can reflect the current treatment development level of MPS patients in different regions of China (to some extent).
Demographic Characteristics of the Patients
The number of hospital prescriptions from 2019 to 2023 generally increased, however in 2020, it decreased by 8.36% compared with that in 2019. Considerations include the global spread of the COVID-19 pandemic in 2020, the fear of menopausal women about the unknown of the new coronavirus infection, and China’s implementation of precise containment, control, and other measures,22 which led to a significant decline in the rate of clinical visits with respect to MPS.
Patients aged 46–55 years with MPS constitute the main group seeking sex hormone drugs. In this survey, the average age of the patients with menopausal syndrome was 48.22±5.94 years. The results of a previous study revealed that the average age of natural menopause throughout the world is 48.8 years,23 and China also follows this pattern. Menopause occurring within 10 years of this time interval or <60 years represents the “window period”. If a patient does not have contraindications (such as a history of breast cancer, elderly coronary heart disease, previous venous thrombosis events/stroke or active liver disease), MHT can be safely used. If the “window period” for MHT is missed, it is possible that the patient will be prevented from experiencing the benefits of sex hormone therapy.1 The age of MPS patients at the time of diagnosis was mainly concentrated in the 46–50 years age group, followed by the 51–55 years age group, both of which were within the “window period”. When considering that hormone levels fluctuate greatly in patients in this age group, a series of problems, such as hot flashes, night sweats, insomnia, urogenital atrophy symptoms, and osteoporosis, can increase the frequency of hospital visits by patients in this age group.24 Patients aged 35–40 years accounted for 11.92% of the sample. Patients who were included in this group mainly experienced the occurrence of menopausal syndrome caused by decreased ovarian reserve or premature ovarian failure.25
The outpatient visit rates in North China and East China are higher than those in Northeast China and Central China. The low outpatient visit rates in Central China may be due to the fact that only 11 hospitals in one city in Zhengzhou were selected for analysis. However, there was no significant difference in the number of cases sampled from 25 hospitals in Northeast China compared to those in East and North China; moreover, when considering that North China and East China are more economically developed than Northeast China and that the proportion of highly educated women is greater in these regions, these women have more avenues for receiving information and knowledge, as well as a stronger awareness of health care. In addition, mental concentration is associated with greater mental pressure and greater work intensity. Therefore, patients with menopausal syndrome who are in a high-pressure environment are more sensitive to physical and psychological changes, and the nature of their work requires a high degree of mental concentration. Therefore, these patients are more inclined to visit the hospital to address this discomfort.26 In addition, the income from jobs requiring mental concentration is greater than income from jobs requiring physical activity in China; moreover, a good economic foundation is also a major reason as to why these individuals prefer to seek medical treatment.
Prescription Patterns of MHT
Menopause is a stage of significant biological-psychological-social changes.7 The estrogen and progestogen compound preparation ranked first for five years, thus indicating that it is the most commonly used drug type for the clinical treatment of MPS in China. Estrogen and progestogen compound preparations can be used in sequential estrogen and progesterone treatment, which is suitable for women with a complete uterus who still experience menstrual-like bleeding.27 A study of sex hormone interventions in patients with a uterus revealed that the risk of endometrial hyperplasia increased by 34% in patients receiving estrogen single preparations, whereas the risk in women receiving combined therapy was only 1%.28,29 The total prescription frequency of the estradiol/estradiol dydrogesterone accounts for 32.76% of the total prescription frequency of sex hormone drugs, and its DDDs value has also ranked first for five years. It is most commonly prescribed to individuals aged 46–50 years, followed by those aged 41–45 and 35–40 years. A previous study showed that low-dose estradiol/estradiol dydrogesterone is more effective at improving vasomotor symptoms in menopausal women in Europe and China and that withdrawal bleeding occurs after discontinuation30,31. Furthermore, it is suitable for patients who have just entered into menopause and still hope for the occurrence of menstrual-like bleeding, thus providing patients with a transition period to accept the onset of menopause.
Tibolone is a selective tissue estrogen activity regulator that can produce estrogen, progestogen, and weak androgen activity in different tissues.32 It is suitable for women who have been menopausal for more than one year and who do not want to experience menstruation-like bleeding or receive medication.1 For five years, tibolone has consistently ranked first in terms of the frequency of prescriptions among individuals aged 51–60 years, with a steady increase in DDDs and amounts of drug consumption being observed. In particular, the frequency of prescriptions and DDDs ranked second from 2021 onwards, which may be related to China’s entry into a moderately ageing society. Studies have shown that menopausal hormone therapy can prevent osteoporosis and fractures in women aged 50–60 years. Tibolone can also significantly improve the symptoms of bone density and urogenital atrophy and has positive effects on sex desire and emotion.33,34
The prescription frequency of progestogen single preparations was found to be 21.33%, which is suitable for patients with abnormal uterine bleeding due to ovarian function decline (AUB-O) who do not exhibit low estrogen symptoms in the early menopausal transition period. AUB-O is characterized by heavy and irregular uterine bleeding due to anovulation and a lack of luteal formation.1 Progestogens alone are used to treat withdrawal bleeding by preventing endometrial growth and transforming estrogen to stimulate the endometrium. The DDDs of dydrogesterone ranked first from 2019–2020. Dydrogesterone is an orally active reverse progestogen with a similar structure to that of natural progesterone. Its retro-conjugated structure endows dydrogesterone with highly selective properties for binding to progesterone receptors. A previous Chinese study showed that dydrogesterone is effective in treating AUB-O.35,36 From 2022 onwards, the incidence of progesterone DDDs increased to first place, which may have led to an increase in clinical use due to the decrease in the price of progesterone collection. One study revealed that natural progestogens and similar natural progestogens have inhibitory effects on breast cancer cell lines. Specifically, the risk of breast cancer after the use of progesterone and dydrogesterone is lower than that after the use of other synthetic progestogens.37
The prescription frequency of estrogen single preparations accounts for 22.79%, which is suitable for women with hysterectomy. According to relevant statistical data in China, from 2005 to 2016, the number of patients who needed total hysterectomy in hospitals at all levels increased from more than 1 million to more than 2.8 million.38 Patients who undergo hysterectomy may experience iatrogenic loss of ovarian function and menopause, as well as a series of menopausal symptoms, such as vasomotor symptoms, urogenital symptoms, bone loss, and osteoporosis,39 therefore, estrogen alone can relieve menopausal symptoms. The frequency of estradiol prescription and DDDs accounted for the highest proportion. A study on the effectiveness and safety of oral and transdermal estradiol in relieving menopausal symptoms revealed no significant difference between the two modes of delivery.40 Compared with third-ranked conjugated estrogens, estradiol has a lower risk of ischaemic stroke.41 Notably, beginning in 2021, the prescription frequency and DDDs ranking of promestriene increased to second place, especially among individuals aged 56–60 years, which may be related to menopausal urogenital syndrome (GSM). GSM is common in aged females. Promestriene vaginal soft capsules are a type of local vaginal estrogen therapy. Studies have shown that the local use of estrogen in the vagina can effectively improve the blood supply of blood vessels around the vaginal wall, thus improving the symptoms of the urogenital tract; additionally, it is highly safe for use.42
The North American Menopause Society states that hormone therapy is the most effective treatment for VMS and genitourinary GSM.8 Non-hormonal treatments and non-drug therapies are available for patients with contraindications to hormone use or based on personal preferences. For the management of VMS, several non-hormonal medications can be considered, including selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), black cohosh extract, gabapentin, and clonidine. These options provide alternative approaches to alleviate symptoms when hormone therapy is not suitable or desired. In May 2023, Fezolinetant was officially approved by the US Food and Drug Administration for the treatment of moderate to severe VMS in menopausal women, lifestyle changes can also be selected as first-line therapy for VMS.43,44 For GSM, studies have shown that non-ablative dual wavelength diode laser therapy or the use of lubricants and vaginal moisturizers can improve urogenital symptoms.1,45
Economic Evaluation of MHT
The results of this survey revealed that the annual total prescription amount in 2020 was the same as that in 2019 and that the number of prescriptions decreased by 8.36%; however, the average annual prescription amount increased by 15.27%, which may have been due to the outbreak of the COVID-19 epidemic in early 2020. The demand for medical treatment from the public could not be met because of the impact of the pandemic. In response, the general office of the National Health Commission issued the “Notice on Strengthening the Management of Medical Services during the Epidemic to Meet the Basic Medical Needs of the Public”. For outpatients with chronic diseases, the prescription amount could be extended to 12 weeks depending on the patient’s condition. Compared with the previous single prescription, which could only be prescribed for 7 days, the average amount of medicine that can now be prescribed per prescription has considerably increased, which leads to an increase in the average prescription amount.
The DDDs of progestogen single preparations increased by 162.88% in five years, whereas the increase in the amount of drug consumed was only 80.88%. The “Documents on Guaranteed Supply and Stable Pricing of Drugs in Short Supply in the Xinjiang Production and Construction Corps, Chongqing, Henan, Guangxi Zhuang Autonomous Region, Hainan, Yunnan, Qinghai, Ningxia and Xinjiang” was issued in May 2021.46 Nine provinces in China have included short supplies of drugs (such as progesterone injections) in two-year centralized procurements, thus resulting in price reductions.
The DDCs of the top 10 sex hormone drugs in terms of the amount of drug that is consumed can vary widely, which indicates that different drugs impose different financial burdens on patients. China’s tertiary public hospitals have now implemented zero-profit sales and abolished drug addition. B/A was shown to be calculated at 1 for the estradiol/estradiol dydrogesterone, which is the most frequently prescribed combination. Tibolone, which ranks first among people aged 51–60, will have a B/A = 1 after 2021, thus indicating that the sales amount and DDDs of the two drugs are in good agreement and that the drug costs are reasonable. The B/A and DDC corroborate each other (to a certain extent). A smaller B/A, the higher the drug price and the higher the DDC. The B/A ranking values of estradiol and drospirenone, and oral progesterone are less than 1, which causes a considerable burden on patients. Therefore, doctors should consider not only the safety and effectiveness of drugs but also the costs of drugs and the burden on patients when choosing drugs.
Limitations
This study only focuses on the trends and patterns of MHT in patients with MPS. Non-hormonal drugs and non-drug treatments are not included. The compliance of menopausal women with sex hormone therapy and the possible causes and factors of discontinuation are not analysed.
Conclusion
This study shows that the average age of menopausal syndrome patients in China from 2019 to 2023 is 48.22±5.94 years old. The prescription frequency of estradiol/estradiol dydrogesterone is highest among people aged 35–50, while tibolone ranks first among people aged 51–60. The estrogen and progestogen compound preparation is the most commonly used form of clinical treatment for MPS. The top-ranked agents, estradiol/estradiol dydrogesterone, tibolone, dydrogesterone, and estradiol, demonstrate well-established efficacy, favorable safety profiles, and rational clinical application. The consultation rate is higher in economically developed areas of China, among people with more mental work, and among patients with medical insurance. The recent abolition of the drug price markup policy by the state, along with the implementation of centralized drug procurement in certain regions, has alleviated financial burdens on patients to some extent. However, both the consultation rate for MPS and the treatment rate for MHT remain suboptimal. This study aims to address these gaps by providing valuable insights into the current utilization of MHT and MPS management in China. The findings offer a foundation for government and medical institutions to optimize future policy development and clinical practice optimization, ultimately improving the management of menopausal syndrome patients receiving sex hormone therapy.
Ethics Approval and Informed Consent
This study protocol was approved by the Ethics Committee of the Obstetrics and Gynecology Hospital of Fudan University (approval number: 2023–01).
The research data originated from the “Hospital Prescription Analysis Cooperation Project” of the Hospital Pharmacy Committee of the Chinese Pharmaceutical Association. This research only analysed on prescriptions, and the prescriptions were all anonymous. Therefore, informed consent was exempted in the Ethics Committee of the Obstetrics and Gynecology Hospital of Fudan University (approval number: 2023–01) because this study was based on routinely collected data. Annexed is the exempted informed consent form for ethical approval.
Consent for Publication
All authors approved the final manuscript and the submission to this journal.
Acknowledgments
We gratefully acknowledge the experts who generously shared their insights and expertise.
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Menopause Subgroup. Chinese Society of Obstetrics and Gynecology, Chinese Medical Association, The 2023 Chinese menopause symptom management and sex hormone drugs guidelines. Zhonghua Fu Chan Ke Za Zhi. 2023;58(1):4–21. doi:10.3760/cma.j.cn112141-20221118-00706
2. Kong F, Wang J, Zhang C, et al. Assessment of sexual activity and menopausal symptoms in middle-aged Chinese women using the Menopause Rating Scale. Climacteric. 2019;22(4):370–376. doi:10.1080/13697137.2018.1547702
3. Crandall CJ, Mehta JM, Manson JE. Management of Menopausal Symptoms: a Review. JAMA. 2023;329(5):405–420. doi:10.1001/jama.2022.24140
4. Lobo RA, Gompel A. Management of menopause: a view towards prevention. Lancet Diabetes Endocrinol. 2022;10(6):457–470. doi:10.1016/S2213-8587(21)00269-2
5. Peinado-Molina RA, Hernández-Martínez A, Martínez-Vázquez S, et al. Pelvic floor dysfunction: prevalence and associated factors. BMC Public Health. 2023;23(1):2005. doi:10.1186/s12889-023-16901-3
6. Bai R, Liu Y, Zhang L, et al. Projections of future life expectancy in China up to 2035: a modelling study. Lancet Public Health. 2023;8(12):e915–e922. doi:10.1016/S2468-2667(22)00338-3
7. Gatenby C, Simpson P. Menopause: physiology, definitions, and symptoms. Best Pract Res Clin Endocrinol Metab. 2024;38(1):101855. doi:10.1016/j.beem.2023.101855
8. Faubion SS, Crandall CJ, Davis L, et al. “The 2022 hormone Therapy Position Statement of The North American Menopause Society” Advisory Panel. The 2022 hormone therapy position statement of The North American Menopause Society. Menopause. 2022;29(7):767–794. doi:10.1097/GME.0000000000002028
9. Voedisch AJ, Dunsmoor-Su R, Kasirsky J. Menopause: a Global Perspective and Clinical Guide for Practice. Clin Obstet Gynecol. 2021;64(3):528–554. doi:10.1097/GRF.0000000000000639
10. You Y, Yu Q, Yu Q, et al. Exploring menopausal symptoms, attitudes, and behaviors among menopausal women in China: an online research perspective. Menopause. 2024;31(11):1006–1013. doi:10.1097/GME.0000000000002428
11. Lin L, Yu Q, Yu Q, et al. Attitude and knowledge for menopause management among health professionals in mainland China. Climacteric. 2020;23(6):614–621. doi:10.1080/13697137.2020.1775809
12. Yang L, Zheng RM, Wang SX, et al. The status of menopause outpatient clinics in maternal and children health institutions and general hospitals in 11 provinces of China. Zhonghua Yu Fang Yi Xue Za Zhi. 2020;54(5):529–533. doi:10.3760/cma.j.cn112150-20190716-00570
13. Wang L, Li F, Yu XW. Investigation and analysis of characteristics of menopause-related symptoms and menopausal hormone therapy cognition status. J Xi’an Jiaotong Univ. 2024;45:629–636.
14. Xiao GZ, Yang L, et al. Research on the Application of Interrupted Time-series Analysis in the Effect Evaluation of the Payment Reform of Basic Medical Insurance. Chin J Health Stat. 2024;41(03):360–364. doi:10.11783/j.issn.1002-3674.2024.03.007
15. Morabia A, Costanza MC. Recent reversal of trends in hormone therapy use in a European population. Menopause. 2006;13(1):111–115. doi:10.1097/01.gme.0000172595.68648.16
16. Santoro N, Neal-Perry G, Peters BA, et al. The Menopause Transition: signs, Symptoms, and Management Options. J Clin Endocrinol Metab. 2021;106(1):1–15. doi:10.1210/clinem/dgaa764
17. Lu J, Xie L, Zheng X, et al. Prevalence of menopausal symptoms and attitudes towards menopausal hormone therapy in women aged 40–60 years: a cross-sectional study. BMC Women's Health. 2023;23(1):472. doi:10.1186/s12905-023-02621-8
18. Zhang Y, Xiong X, Lin Y, et al. Knowledge and attitudes of premenopausal women in southern China toward menopause and menopausal hormone therapy. Climacteric. 2025;28(2):191–199. doi:10.1080/13697137.2025.2455168
19. Dong ZY, Sheng GJ, et al. Estimating Production and Demand Functions of Hospitals: An Evaluation of China’s Hospital Rating System. China Econ Q. 2025;25(01):86–102. doi:10.13821/j.cnki.ceq.2025.01.06
20. Harlow SD, Gass M, Hall JE, STRAW 10 Collaborative Group. Executive summary of the Stages of Reproductive Aging Workshop + 10: addressing the unfinished agenda of staging reproductive aging. Menopause. 2012;19(4):387–395. doi:10.1097/gme.0b013e31824d8f40
21. WHO Collaborating Centre for Drug Statistics Methodology. ATC/DDD Index 2024. Available from: http://www.whocc.no/. Accessed 2024.
22. Wang ZH. A Survey of Anxiety and Depression in Menopausal Women During the COVID Outbreak Closed-Off management. Hebei Medical University; 2023.
23. Davis SR, Baber RJ. Treating menopause-MHT and beyond. Nat Rev Endocrinol. 2022;18(8):490–502. doi:10.1038/s41574-022-00685-4
24. Duralde ER, Sobel TH, Manson JE. Management of perimenopausal and menopausal symptoms. BMJ. 2023;8:e072612. doi:10.1136/bmj-2022-072612
25. Rahman R, Panay N. Diagnosis and management of premature ovarian insufficiency. Best Pract Res Clin Endocrinol Metab. 2021;35(6):101600. doi:10.1016/j.beem.2021.101600
26. Sharami SH, Eslami-Kenarsari H, Farzadi S, et al. The association of sociodemographic factors and history of chronic diseases on menopausal symptoms: a cross-sectional study. Health Sci Rep. 2024;7(5):e2103. doi:10.1002/hsr2.2103
27. Chen W, Chen J, Tang H, et al. Advances in diagnosis and treatment of perimenopausal syndrome. Open Life Sci. 2023;18(1):20220754. doi:10.1515/biol-2022-0754
28. Cho L, Kaunitz AM, Faubion SS, et al. Rethinking Sex Hormone Drugs: for Whom, What, When, and How Long? Circulation. ACC CVD in Women Committee. 2023;147:597–610.
29. Judd HL, The Writing Group for the PEPI Trial. Effects of hormone replacement therapy on endometrial histology in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA. 1996;275(5):370–375. doi:10.1001/jama.1996.03530290040035
30. Liu JH, Pinkerton JV. Prescription Therapies. In: Crandall CJ, editor. Menopause Practice: A Clinician’s Guide.
31. Yu Q, Ren M, Tatarchuk T, et al. Ultra-low-dose estradiol and dydrogesterone for treatment of vasomotor symptoms in Europe and China. Climacteric. 2024;27(5):1–7. doi:10.1080/13697137.2024.2380364
32. Del Río JP, Barreto GE, Hidalgo-Lanussa O, et al. Tibolone as Hormonal Therapy and Neuroprotective Agent. Trends Endocrinol Metab. 2020;31(10):742–759. doi:10.1016/j.tem.2020.04.007
33. Liu X, Zhu Z, Wang X. Analysis of medication treatment for women with osteoporosis: a real-world retrospective study from Chinese tertiary grade A hospital. Bone Rep. 2024;21:101778. doi:10.1016/j.bonr.2024.101778
34. Casiano Evans EA, Hobson DTG, Rahn DD, et al. Nonestrogen Therapies for Treatment of Genitourinary Syndrome of Menopause: a Systematic Review. Obstet Gynecol. 2023;142(3):555–570. doi:10.1097/AOG.0000000000005288
35. Munro MG, Critchley HO, Broder MS, et al. FIGO Working Group on Menstrual Disorders, FIGO classification system (PALM-COEIN) for causes of abnormal uterine bleeding in nongravid women of reproductive age. Int J Gynaecol Obstet. 2011;113(1):3–13. doi:10.1016/j.ijgo.2010.11.011
36. Wang L, Zhang W, Xia H-X, et al. Dydrogesterone treatment for menstrual-cycle regularization in abnormal uterine bleeding - ovulation dysfunction patients. World J Clin Cases. 2020;8(15):3259–3266. doi:10.12998/wjcc.v8.i15.3259
37. Gompel A, Plu-Bureau G. Progesterone, progestins and the breast in menopause treatment. Climacteric. 2018;21(4):326–332. doi:10.1080/13697137.2018.1476483
38. Van Lieshout LAM, Bekkers RLM, Verwijmeren K, et al. Ovarian cancer risk after salpingectomy for ectopic pregnancy or hydrosalpinx: results of the OCASE nationwide population-based database study. Hum Reprod. 2021;36(1):211–218. doi:10.1093/humrep/deaa264
39. Hinds L, Price J. Menopause, hormone replacement and gynaecological cancers. Menopause Int. 2010;16(2):89–93. doi:10.1258/mi.2010.010018
40. Tang R, Yu Q, Ruan X, et al. Changes in menopausal symptoms comparing oral estradiol versus transdermal estradiol. Climacteric. 2024;27(2):171–177. doi:10.1080/13697137.2023.2273530
41. Chang WC, Wang JH, Ding DC. Conjugated equine estrogen used in postmenopausal women associated with a higher risk of stroke than estradiol. Sci Rep. 2021;11(1):10801. doi:10.1038/s41598-021-90357-6
42. Diedrich CM, Roovers JWR, Verri FM, et al. Effects of topical estrogen therapy on the vaginal microcirculation in women with vulvovaginal atrophy. Neurourol Urodyn. 2019;38(5):1298–1304. doi:10.1002/nau.23977
43. Al Wattar BH, Talaulikar V. Non-oestrogen-based and complementary therapies for menopause. Best Pract Res Clin Endocrinol Metab. 2024;38(1):101819. doi:10.1016/j.beem.2023.101819
44. Rani P, Zehra D, Mansoor M, et al. FDA approved fezolinetant (Veozah): a critical evaluation of its efficacy and safety for menopausal vasomotor symptoms, calling for prospective research. Arch Women's Ment Health. 2024;27(6):943–946. doi:10.1007/s00737-024-01456-y
45. Vitale SG, Angioni S, Succu AG, et al. Efficacy and Safety of Non-Ablative Dual Wavelength Diode Laser Therapy for Genitourinary Syndrome of Menopause: a Single-Center Prospective Study. Adv Ther. 2024;41(12):4617–4627. doi:10.1007/s12325-024-03004-7
46. Henan Provincial Medical Security Administration. Documents on Guaranteed Supply and Stable Pricing of Drugs in Short Supply in the Xinjiang Production and Construction Corps, Chongqing, Henan, Guangxi Zhuang Autonomous Region, Hainan, Yunnan, Qinghai, Ningxia, and Xinjiang 2021. Available from: http://ylbzj.cq.gov.cn/zwgk_535/gstz/202105/t20210521_9314932.html.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.