")
Back to Journals » Infection and Drug Resistance » Volume 18
Application of Targeted Next-Generation Sequencing in Bronchoalveolar Lavage Fluid for the Detection of Pathogens in Pulmonary Infections
Authors Dai X, Xu K, Tong Y, Li J, Dai L, Shi J, Xie H, Chen X
Received 6 October 2024
Accepted for publication 16 January 2025
Published 27 January 2025 Volume 2025:18 Pages 511—522
DOI https://doi.org/10.2147/IDR.S499265
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Xianning Dai,1 Kai Xu,1 Yu Tong,1 Jing Li,2 Liya Dai,1 Jianyou Shi,1 Haibin Xie,3 Xi Chen3
1Department of Clinical Laboratory, Wenzhou People’s Hospital, Wenzhou Maternal and Child Health Care Hospital, Zhejiang, People’s Republic of China; 2Department of PCCM, Wenzhou People’s Hospital, Wenzhou Maternal and Child Health Care Hospital, Zhejiang, People’s Republic of China; 3Department of Immunization Planning, Prevention and Health Care, Centers for Disease Control of Luchen, Zhejiang, People’s Republic of China
Correspondence: Xi Chen, Department of Immunization Planning, Prevention and health care,Centers for Disease Control of Luchen, No. 3320 Guojing Road, Wenzhou, Zhejiang, 325005, People’s Republic of China, Tel +86 577 56760657, Fax +86 577 56760654, Email [email protected]
Objective: This study aims to evaluate the utility of targeted next-generation sequencing (tNGS) in bronchoalveolar lavage fluid (BALF) for hospitalized patients with pulmonary infections.
Methods: A cohort of 358 patients who received diagnosis and treatment for respiratory infections in the department of Respiratory Medicine at Wenzhou People’s hospital from January 2023 to April 2024 were selected for this study. The BALF of the patients was analyzed using tNGS, and the diagnostic efficacy of tNGS was subsequently compared with that of conventional testing methods (CTs) for pathogen detection.
Results: Through the analysis of tNGS from the cohort, the pathogen detection rate in BALF using tNGS was significantly higher than that of CTs (90.22% VS 57.26%, P=0.001). Among them, Tropheryma Whipplei (6.15%), Bordetella pertussis (2.51%), Non-tuberculous mycobacteria (1.96%), Mycobacteria tuberculosis (1.40%), Chlamydia pneumoniae (1.96%), Chlamydia psittaci (0.56%), Legionella pneumophila (0.28%) were detected using tNGS alone, and the CTs results of these microorganisms were all negative. Among the various types of mixed infections observed, concurrent presence of bacteria and viruses was the most common, accounting for 37.15%. The detection rates of tNGS and CTs have statistical significance (66.87% VS 35.12%, P=0.001). Furthermore, a total of 61 cases of antimicrobial resistance genes were detected, including 34 cases of 23S rRNA A2063G, 6 cases of KPC, 5 cases of OXA, 2 cases of CTX-M, 3 cases of IMP, 1 case of NDM and 13 cases of mecA. Using the clinical diagnosis as references, the positive coincidence rate of the tNGS was significantly higher compared to that of the CTs (P=0.012).
Conclusion: Compared to CTs, the application of tNGS enables the identification of a greater diversity of organisms and exhibits superior accuracy, effectively identifying pathogens that are undetectable by CTs, especially fastidious and atypical organisms. Consequently, it holds immense potential in pathogen diagnosis and offers valuable clinical guidance for patients with pulmonary infections.
Keywords: bronchoalveolar lavage fluid, targeted next-generation sequencing, pneumonia, pathogen, culture, antimicrobial resistant
Background
Infectious diseases remain a significant threat to human health and life globally. Presently, the global incidence of infectious diseases is on the rise, with pathogens exhibiting increasingly diverse and complex patterns. Epidemiological investigations and research findings indicate that pulmonary infection is one of the most prevalent infectious diseases in clinical practice, exhibiting higher incidence and mortality rates among elderly individuals and those with compromised immune function.1,2 Furthermore, for adult community-acquired pneumonia (CAP), approximately 62% of patients still lack a clearly identified pathogenic bacterium, which is also one of the major causes of death from infectious diseases.3 Therefore, rapid identification of the causative pathogens is crucial for the effective treatment and prognosis of patients with pulmonary infections.
However, in China, nearly half of patients with pulmonary infections lack a definitive etiological diagnosis.4 Conventional testing methods (CTs) for pulmonary pathogens primarily employ three detection methods: etiology-based approaches, molecular biology-based techniques, and immunology-based strategies. While these methods possess distinct advantages, they often exhibit limitations when applied to complex infectious diseases, such as cumbersome procedures, prolonged processing times, narrow detection ranges, and low sensitivity.5,6 Furthermore, patients with negative results from traditional pathogen detection often receive empirical antibiotic treatment that may not cover true pathogens, thereby worsening infections. The widespread use of antibiotics can promote resistance while facilitating the accumulation/transmission of multi-drug-resistant (MDR) pathogens. CTs for pathogen detection are no longer sufficient to meet current needs for rapid and accurate diagnosis. Therefore, establishing new methods for rapid and accurate pathogen detection is crucial for the timely implementation of rational prevention and treatment strategies against infectious diseases.
In recent years, with the advancement of biological research from macro to micro domains, pathogen detection methods have also evolved from histological levels to molecular scales. There has been an increasing number of reports on the application of next-generation sequencing (NGS).7–9 Compared to CTs, NGS offers advantages in pathogen screening from various specimen types, including sputum, blood, pleural fluid, abdominal fluid, bronchoalveolar lavage fluid (BALF), and lung tissue specimens.10 The applications of NGS in pathogen detection encompass targeted next-generation sequencing (tNGS) and metagenomic next-generation sequencing (mNGS). mNGS has the capability to detect all potential pathogen sequences in a sample; however, it is susceptible to interference from human host genes, resulting in reduced sensitivity for pathogen detection. Additionally, mNGS lacks the ability to simultaneously consider both DNA and RNA processes of pathogens, and its high testing cost limits its clinical application.11 Compared to mNGS, tNGS combines ultra-multiplex PCR amplification with high-throughput sequencing technology to accurately detect various known pathogens and antimicrobial resistance genes (ARGs) in test samples. It enables precise broad-spectrum pathogen detection within an average time frame of only 12–14 hours. Moreover, tNGS offers a significantly lower testing cost (approximately 1/5 to 1/6 that of mNGS), making it a valuable method for diagnosing lower respiratory tract infections (LRTIs).
More and more studies focus on mNGS applied to BALF analysis, while fewer studies utilize tNGS techniques. This study aims to evaluate the pathogen detection rate and distribution as well as the concordance between tNGS and traditional testing by comparing them. It intends to provide evidence for early clinical diagnosis of pathogens and precision treatment based on an understanding the application value of targeted sequencing technology in detecting pulmonary infection pathogens from BALF.
Materials and Methods
General Information
The study cohort comprised 358 patients with pulmonary infectious diseases who were diagnosed and treated in the Department of Pulmonary and Critical Care Medicine (PCCM) at Wenzhou People’s Hospital between January 2024 and April 2024, including 189 males and 169 females, with an average age of 51.37 ± 16.52 years. The clinical data of the enrolled patients, including age, gender, clinical symptoms, routine laboratory test results such as white blood cell count (WBC), C-reactive protein (CRP), procalcitonin (PCT), and traditional culture results were collected and analyzed. Additionally, tNGS screening was performed on the collected BALF. The pathogens commonly screened are listed in Table 1. Based on the comprehensive evaluation of medical history, clinical symptoms, pulmonary signs, laboratory tests, and chest CT results, a total of 231 patients with underlying pulmonary conditions were accurately diagnosed, including 141 cases of community-acquired pneumonia (CAP), 26 cases of bronchiectasis,18 cases of chronic obstructive pulmonary disease (COPD), 16 cases of chronic bronchitis, 9 cases of pulmonary tuberculosis (TB), and 21 cases of concomitant multiple underlying pulmonary diseases. The diagnostic criteria for pulmonary infection encompass the presence of new or worsening focal or diffuse infiltrative lesions on chest CT, in conjunction with at least one of the following four pneumonia-related clinical manifestations: (I) recent onset of cough, sputum production, or exacerbation of pre-existing respiratory symptoms, accompanied by or without purulent sputum, chest pain, dyspnea and hemoptysis;(II) fever with a temperature ≥38.0°C; (III) signs indicative of lung consolidation and/or auscultatory findings revealing moist rales; (IV) peripheral blood leukocyte count >10×109/L or <4×109/L. Exclusion criteria: (I) Severe heart disease (cardiac insufficiency, acute myocardial infarction), or accompanied by coagulation disease, anemia, etc. (II) Patients exhibit low to lerance towards electronic bronchoscopy examination. The study was conducted in accordance with the principles of the Declaration of Helsinki, and approval was obtained from the Medical Ethics Committee of our hospital. Written informed consent was obtained from all participants or their legal guardians.
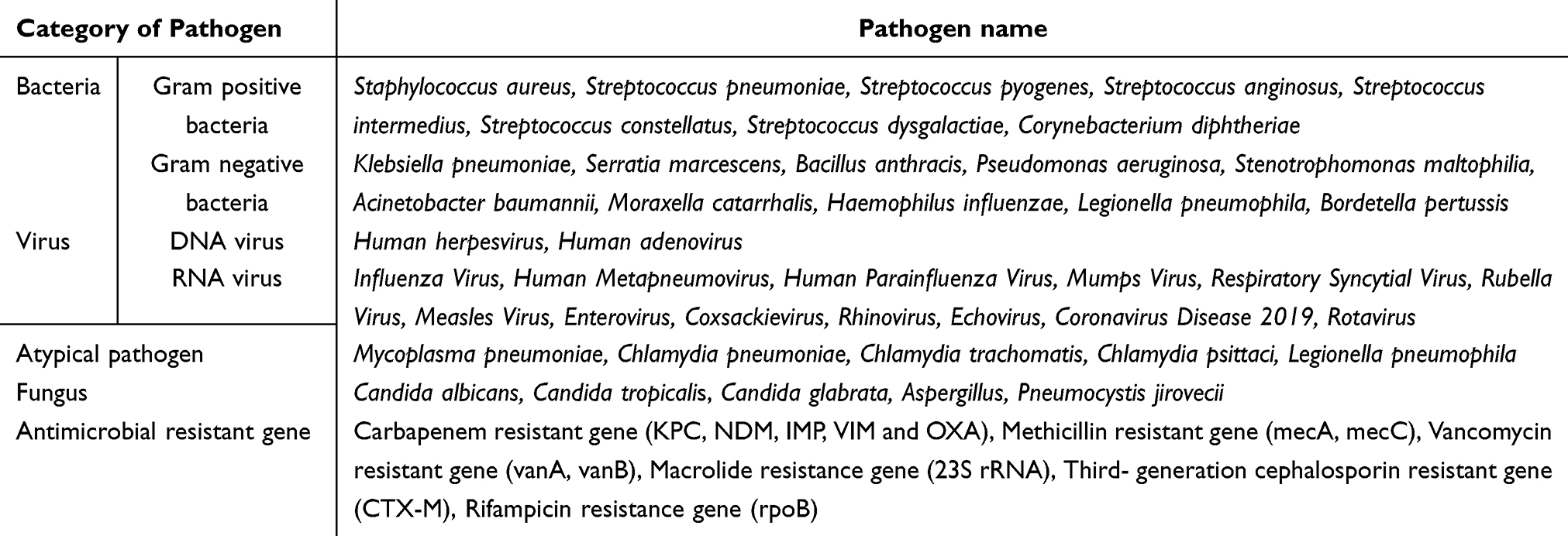 |
Table 1 Respiratory Pathogen Names and Classification |
The present study was granted approval by the Medical Ethics Committee of our hospital, with informed consent obtained from both participants or their families.
Sample Processing and DNA Extraction
All patients underwent bronchoscopy, and BALF samples were collected from the specific lesion site identified through pulmonary CT imaging. After transferring 800 μL of BALF to a Lysing Matrix E tube containing glass microbeads, the cell wall was disrupted using a biological sample homogenizer (ShenKe Bio-technology, Co., Ltd., Huzhou, China), followed by centrifugation of the sample at 12,000 rpm for five minutes (Thermo Fisher Scientific, United States). At least 500 μL of the supernatant was transferred into the High Pure DNA/RNA Kit (GensKey Bio-Technology Co., Ltd., Tianjin, China) in conjunction with the GeneRotex-96 automated nucleotide extraction and purification system (TianLong Biotechnology Co., Ltd., Suzhou, China) for DNA/RNA extraction, strictly adhering to the manufacturer’s protocol. The extracted DNA/RNA was stored at −20 °C until library preparation.
Library Preparation and Sequencing
The DNA library was constructed using the DNA Library Prep Kit (GensKey Bio- Technology Co., Ltd., Tianjin, China), which involved two rounds of PCR amplification. After enriching the target pathogen sequences, PCR products were amplified again using primers that contained sequencing adapters and distinct barcodes. The Qubit 4.0 fluorescence spectrophotometer (Thermo Fisher Scientific, United States) was used to monitor the quality and quantity of the library. The Quality-approved library was cyclized to form a single-stranded ring structure and then rolled into create a DNA nanosphere, which was loaded onto a sequencing microarray. tNGS sequencing was performed on MGISEQ-2000 platform using a universal sequencing reagent kit (GensKey Bio- Technology Co., Ltd., Tianjin, China).
Data Analysis
The raw sequencing data undergo initial identification to eliminate low-quality data, followed by comparison of the resulting high-quality data using the data management and analysis system (Genseq-BSI). The pathogen sequences are aligned with the Self-Built clinical pathogen database to obtain species information and corresponding microbial sequences from the samples. Finally, prior to issuing the final test report, doctors comprehensively analyze tNGS results, considering factors such as clinical symptoms, conventional tests, and laboratory test results. The microbiological data presented in this study were extracted from the final clinical report.
Statistical Analysis
The data analysis was performed using SPSS19.0 statistical software. Quantitative data were presented as mean±standard deviation, categorical data were presented as counts with percentages [n(%)], and statistical comparisons were performed using the chi-square test. A significance level of P < 0.05 was considered statistically significant.
Results
General Information
The basic characteristics for all patients were listed in Table S1 including 231 patients in the underlying pulmonary disease (UPD) group and 127 in the non-underlying pulmonary disease (NUPD) group. The predominant clinical symptoms observed in all patients included fever (23.18%), cough (89.66%), hemoptysis (3.35%), and chest tightness (23.18%). The age of patients in the UPD group was significantly higher than that in the NUPD group (P=0.008). Furthermore, the number of patients with cough and phlegm in the UPD group was significantly higher than that in the NUPD group (P=0.000). While the comparison of remaining clinical data between the two groups was presented in Table 2, revealing no statistically significant difference (P > 0.05).
 |
Table 2 The Basic Characteristics of 358 Patients With Pulmonary Infections |
Overall Pathogen Detection Results of tNGS
Pathogen Positivity Rate
Through the analysis of tNGS data from the cohort, a high pathogen detection rate of 90.22% (323/358) was found. The pathogens detected in 323 tNGS-positive patients were classified into four categories: bacteria, fungi, viruses and atypical pathogens (Mycoplasma / Chlamydia), including 36 pathogens were detected (16 bacteria species, 5 fungi, 12 viruses, and 3 atypical pathogens). The three most frequently detected bacteria were Haemophilus influenzae (H. influenzae) at 29.33%, Streptococcus pneumoniae (S. pneumoniae) at 22.35%, and Staphylococcus aureus (S. aureus) at 10.34%. Among fungi, Candida albicans (C. albicans) accounted for 7.82%, Pneumocystis jirovecii (P. jirovecii) for 6.70%, and Aspergillus species for 7.54% (including 18 cases of Aspergillus fumigatus, two cases of Aspergillus flavus, and one case of Aspergillus niger), which exhibited the highest detection rates. In terms of viruses, Human herpesvirus 4 (HHV-4) accounted for 13.69%, Human herpesvirus 7 (HHV-7) for 12.85%, and Influenza virus B (IVB) for 11.17%. Mycoplasma pneumoniae (M. pneumoniae), accounting for 13.97%, was the predominant atypical pathogen (Figure 1).
 |
Figure 1 Detection rate of respiratory pathogens in tNGS screening. |
Types of Pathogen Infection
Moreover, an analysis of pathogen infection types using tNGS revealed that 33.13% (107/323) of patients presented with single infections, with bacterial infection accounting for the highest proportion at 16.10% (52/323). While the remaining 66.87% (216/323) of patients exhibited mixed infections (Table 3). Among the various types of mixed infections observed, concurrent presence of bacteria and viruses was the most common, accounting for 37.15% (120/323). Notably, as shown in Figure 2, the combination of H. influenzae and S. pneumoniae exhibited the highest detection rate at 12.50% (27/216), followed by the combination of H. influenzae and HHV-4, accounting for 11.11% (24/216), and the combination of H. influenzae and Human adenovirus (HAdv), accounting for 8.33% (18/216).
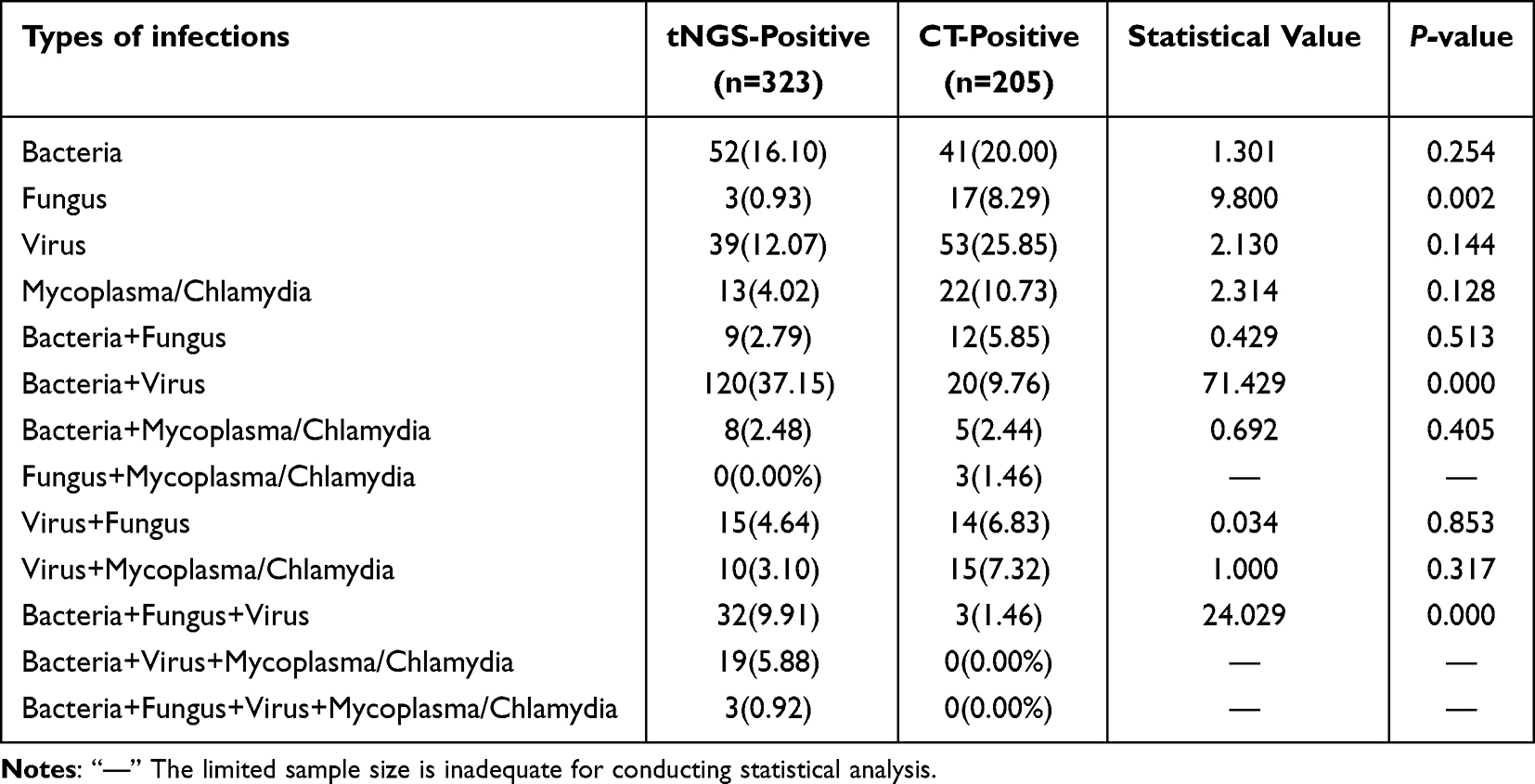 |
Table 3 Comparison of Detection Results Between tNGS and CTs |
 |
Figure 2 Detection frequency of mixed infections with respiratory pathogens. The size and intensity of the dots increase in accordance with the higher frequency of mixed infections. |
Identification of Antimicrobial Resistance Genes
As shown in Table S2, a total of 61 cases of antimicrobial resistance genes (ARGs) were detected, including macrolide-resistant genes at 55.74% (34 cases of 23S rRNA A2063G), carbapenem-resistant genes at 24.59% (6 cases of KPC, 5 cases of OXA, 3 cases of IMP, and 1 case of NDM), methicillin-resistant genes at 21.31% (13 cases of mecA), and third-generation cephalosporin-resistant genes at 3.28% (2 cases of CTX-M).
Among these, the prevalence of ARGs was observed to be 68.00% (34/50) in M. pneumoniae, 54.55% (12/22) in Klebsiella pneumoniae (K. pneumoniae), 77.78% (7/9) in Acinetobacter baumannii (A. baumannii), 57.14% (4/7) in Escherichia coli (E. coli), 14.29% (2/14) in Stenotrophomonas maltophilia (S. maltophilia), 15.38% (4/26) in Pseudomonas aeruginosa (P. aeruginosa), and 35.14% (13/37) in S. aureus.
Comparison of Detection Results Between tNGS and CTs
Comparison of Detection Rates
As shown in Table 3. The pathogen detection rate of CTs was 57.26% (205/358), whereas tNGS demonstrated a significantly higher pathogen detection rate in BALF at 90.22% (323/358), with statistical significance observed (P=0.001). The two methods (tNGS vs CTs) produced comparable outcomes in terms of the number of identified bacteria (14 vs 8), fungi (7 vs 4), viruses (12 vs 5), and other pathogen types (3 vs 1). Furthermore, a comparison between the two methods revealed significant differences in detection rates for bacteria (75.23% vs 39.51%, P=0.000), viruses (73.68% vs 51.22%, P=0.000), but not for fungi (19.20% vs 22.44%,P=0.368) or other types of pathogens (16.41% vs 21.95%,P =0.110). Among the double positive samples, 34 out of 187 patients’results were completely matched, 132 were partially matched, and 21 were completely mismatched. There were 5 (2.44%,5/205) samples that tested only positive for CTs, and 136 (42.11%,136/323) samples that tested only positive for tNGS (Figure 3A). Additionally, CTs revealed mixed infections in 35.12% (72/205) of patients, while the proportion of patients with mixed infections detected by tNGS methods was significantly higher at 66.87% (P=0.001).
 |
Figure 3 The comparison between targeted next-generation sequencing (tNGS) and conventional testing methods (CTs) for the diagnosis of pulmonary infection in pathogen detection. (A) The number of patients diagnosed using both tNGS and CTs, neither and only tNGS or CTs. (B) The concordance rates of patients with complete detection, partial detection, and no pathogen detection using tNGS and CTs were determined based on clinical diagnosis. |
Comparison of Diagnostic Performances
The performances of tNGS and CTs for pathogen identification were evaluated with clinical diagnosis as a reference. In the study, the positive coincidence rate of the tNGS method was 88.55% (317/358), whereas that of the CTs was 57.26% (205/358). Thus, the tNGS method exhibited a significantly higher positive coincidence rate compared to CTs (P=0.012). The tNGS method partially identified pathogens in 32 out of the total 358 cases, while no pathogens were detected in 41 cases. In contrast, the CTs partially identified pathogens in 154 cases and failed to identify any pathogens in the remaining 153 cases (Figure 3B). Additionally, Tropheryma whipplei (T. whipplei) accounted for 6.15%, Bordetella pertussis (B. pertussis) for 2.51%, non-tuberculous mycobacteria (NTM) for 1.96%, Chlamydia pneumoniae (C. pneumoniae) for 1.96%, Mycobacterium tuberculosis (MTB) for 1.40%, Chlamydia psittaci (C. psittaci) for 0.56%, and Legionella pneumophila (L. pneumophila) for 0.28%. These pathogens were exclusively identified by tNGS, whereas CT testing yielded negative results for these microorganisms.
Discussion
In the study, the overall detection rate of pathogens using tNGS screening was 90.22% in 358 BALF specimens, which is generally comparable to the report by Wu et al, with a rate of 90.30% in mNGS screening.12 However, it significantly surpasses several conventional test methods, including the isolation and culture method (39.30%),13 Multiplex qRT-PCR method (61.29%),14 PCR-Capillary electrophoresis (54.67%),15 and Immunofluorescence assay (36.70%).16 The results demonstrated that tNGS offers distinct advantages over CTs, including a comprehensive range of clinically prevalent pathogen profiles and exceptional testing accuracy. Moreover, 36 organisms were detected using tNGS in 358 BALF specimens, among which the top three pathogens were H.influenzae, S.pneumoniae, and M. pneumoniae, which are similar to the common pathogens found in the guidelines for community-acquired pneumonia (CAP) in Chinese populations.17 These findings suggest that bacterial infections remain the primary causative agent of LRTIs. However, recent research data from Chinese CAP indicated a shift in the pathogenic characteristics of CAP, with a notable surge in the detection rate of viral pneumonia. Currently, viral pneumonia accounts for approximately 27.5% to 39.2% of CAP cases in China.18–20 In our study, the detection of virus using tNGS mainly occurred in the form of mixed infection with bacteria and viruses. And the most prevalent viruses associated with LRTIs included HHV-4, HHV-7, IVB, HAdv, and HMPV. The ratio of virus detection by tNGS significantly surpasses that of CTs (73.68% vs 51.22%, P=0.000), which is consistent with the findings reported by Huang et al.21 The limited efficacy of traditional methods in virus detection primarily arises from challenges associated with virus cultivation and insufficient throughput of PCR testing. In contrast to bacterial pneumonia, the current availability of effective antiviral drugs is limited, necessitating a primary focus on symptom management in treatment. Moreover, in terms of pathogen detection, tNGS has demonstrated its capability to identify rare pathogens such as P.jiroveci, T.Whipplei, C.psittaci, and L.pneumophila, which often remain undetected due to the inherent limitations imposed by culture conditions and techniques in routine microbial testing.
With the advancement of pathogen detection methods, there is an increasing focus on mixed infections of multiple pathogens in the respiratory tract.22 The prevailing notion posits that such co-infections may contribute to disease exacerbation, thereby leading to an unfavorable prognosis for patients. However, due to the lack of specific clinical features for such infections, it is challenging to differentiate between single and mixed infections based solely on clinical characteristics, demographics or imaging. In a retrospective study, the diagnostic roles of NGS and conventional testing in mixed lung infections were compared, and the results showed that NGS outperformed conventional testing in terms of speed and sensitivity.23 In our study, 66.87% of patients exhibited mixed infections. The combination of H. influenzae and S. pneumoniae exhibited the highest detection rate at 12.50%, followed by the combination of H. influenzae and HHV-4, accounting for 11.11%, and the combination of H. influenzae and Adv, accounting for 8.33%. It revealed that H. influenzae is one of the main pathogens causing CAP in elderly individuals, often appearing in the form of mixed infections. Divergent perspectives exist in reports regarding the impact of mixed infections on disease progression or treatment duration. While some studies have demonstrated an association between co-infection of influenza virus with bacteria such as H. influenzae or S. pneumoniae, and increased disease severity or mortality risk, others have suggested that the presence of specific normal bacterial flora in respiratory epithelial cells hinders consistent conclusions regarding the severity of respiratory diseases and length of hospitalization caused by mixed infections involving bacteria.24 Therefore, this study’s model of mixed infection should be considered alongside clinical symptoms, laboratory tests, and other factors.
The conventional drug susceptibility test necessitates operation following a positive culture result, leading to delayed results and suboptimal timeliness. In contrast, tNGS can simultaneously identify pathogenic microorganisms and ARGs, thereby predicting drug resistance more efficiently. In the study, the main clinical drug-resistant bacteria include A. baumannii, M. pneumoniae, E. coli, K. pneumoniae, S. aureus, P. aeruginosa, and S. maltophilia. It shows that extensively drug-resistant Gram-negative bacilli (XDR-GNB), especially carbapenem-resistant organisms (CRO), as common multi-drug resistant (MDR) bacteria in hospitals, should receive more attention. Among them, the phenomenon of carbapenem-resistant Enterobacterales (CRE), carbapenem-resistant A. baumannii (CRAB), and carbapenem-resistant P. aeruginosa (CRPA) is particularly serious. Enterobacterales bacteria, including species such as Proteus, Klebsiella, Escherichia, and Enterobacter, are the most prevalent in hospital-acquired infections.25 Notably, the misuse and overuse of antibiotics have led to a significant rise in the detection rate of carbapenem-resistant K.pneumoniae (CRKP), which has now emerged as the predominant strain among CRE. A survey conducted in the United States revealed an average incidence rate of carbapenem-resistant Enterobacteriaceae (CRE) of 2.94 per 10,000 patient admissions between 2012 and 2013, with 42% of these CRE isolates identified as carbapenemase-producing K. pneumoniae.26,27 In China, surveillance data from 2021 indicated that, after 17 consecutive years of monitoring, the resistance rates of K. pneumoniae to imipenem and meropenem increased from 3.0% and 2.9% to 25% and 26.3%, respectively,25 Similarly CRAB and CRPA present a substantial threat to hospitalized patients due to the limited availability of effective therapeutic options. Therefore, Rapid and accurate differentiation among various carbapenemase classes is crucial for initiating early and effective therapy. M. pneumoniae is a significant cause of CAP globally, especially among children. Macrolides are the first-line treatment for M. pneumoniae CAP (MPP), but their overuse has resulted in resistance in many regions. M. pneumoniae can develop macrolide resistance via point mutations in the 23S rRNA gene, reducing the antibiotic’s affinity for the ribosome. The most common mutation is A2063G, followed by A2064G. In this study, the carriage rate of the 23S rRNA A2063G gene mutation in M. pneumoniae was 68.00%, which was much higher than that in other countries,28 such as France (8.3–9.8%),United States (8.2%), Germany (3%-3.6%), Denmark (0.9%-2.9%). The evidence indicates that the inappropriate and excessive use of macrolides for treating MPP significantly increases the risk of resistance development in China. Methicillin-resistant S. aureus (MRSA) is mediated by the mecA and mecC genes, which encode penicillin-binding protein 2a (PBP2a) and PBP2c enzymes, respectively. In this study, only the MRSA carrying mecA (mecA-MRSA) was detected, with a prevalence of 35.14%. Despite the low prevalence of human mecC-MRSA infections, the transmission between hosts shows a significant potential for spread. Reservoirs exist in wildlife, livestock, and pets, and zoonotic transmission could increase human clinical cases.29
Furthermore, the present study utilized a comprehensive clinical diagnosis as the reference standard, and the positive concordance rate of tNGS was significantly superior to that of CTs (P =0.012). The majority of bacteria were missed by CTs. Despite being considered the gold standard, the culture method exhibits a very low positivity rate in LRTIs.30,31 Compared to CTs, the application of tNGS enables the identification of a greater diversity of organisms and exhibits superior accuracy and effectively identifies pathogens that are undetectable by CTs, especially fastidious and atypical organisms. tNGS not only enables pathogen diagnosis but also facilitates the investigation of infectious disease epidemiology and identification of resistance genes, thereby mitigating the risk of empirical treatment failure.
However, tNGS also has limitations. Firstly, although tNGS demonstrates a favorable pathogen detection effect, the absence of standardized interpretation for tNGS reports currently poses a challenge.32 Moreover, due to variations in doctors’ personal experience and knowledge levels, there may be discrepancies in result interpretation. Therefore, clinical analysis should consider the patient’s condition and other relevant clinical data. Secondly, tNGS cannot yet fully detect drug resistance, and the degree of association between reported drug resistance genotypes and phenotypes exhibits a certain gap necessitating confirmation through drug sensitivity testing. A study on bacterial infections in the lower respiratory tract revealed that mNGS detected a total of 183 drug-resistant genes in 41 patient respiratory samples. Out of these, only 24 genes exhibited consistency with the resistant phenotype, whereas 16 genes did not correspond to the observed phenotype.33 Lastly, It is difficult to distinguish between commensal bacteria and pathogenic bacteria using tNGS. Therefore, clinicians should take into account the distinctive characteristics of the microbiota, including its sequencing numbers, exposure history or medical background in specific environments, clinical symptoms, and examinations to arrive at comprehensive assessments. For example, if a specific pathogen demonstrates a substantial advantage in terms of relative sequence numbers compared to other pathogens, it is likely to be the causative agent. Conversely, when the relative abundance is low (referring to the proportion of sequences from a particular microorganism out of the total detected sequences) and the patient does not exhibit any associated clinical symptoms, there is a high probability that colonization by commensal bacteria has been identified. Respiratory tract colonizing pathogens such as S.aureus, S.maltophilia, P.aeruginosa, A.baumannii,Candida or certain viruses can transition from colonization to pathogenicity in cases of immunodeficiency or respiratory barrier dysfunction.
Therefore, tNGS technology still requires continuous refinement to enhance its diagnostic efficiency in LRTIs and achieve better alignment with the clinical application requirements.
Conclusion
In conclusion, the application of tNGS in BALF demonstrates a higher detection rate of pathogenic microorganisms, thereby enhancing the accuracy of pathogenic diagnosis in infected patients. tNGS surpasses traditional microbial culture methods in terms of speed, comprehensiveness, and accuracy. Consequently, tNGS holds significant clinical value for infection diagnosis by facilitating targeted antibiotic usage, reducing drug resistance occurrence, and shortening disease duration. However, tNGS still cannot entirely supplant conventional diagnostic methods, rather, it can serve as a supplementary and indispensable testing approach in specific clinical scenarios. By integrating comprehensive analysis, the prompt and precise diagnosis of infectious diseases can genuinely be achieved, thereby benefiting a greater number of medical professionals and patients.
Data Sharing Statement
All data generated or analysed during this study are available in the supplementary information files accompanying this published article.
Ethics Approval and Consent to Participate
The study protocol was reviewed and approved by the Research Ethics Committee of Wenzhou People’s Hospital and adhered to the ethical standards for medical research involving human subjects (Ethics approval No. KY-2024-218). Written informed consent was obtained from the parents of all participants prior to enrollment.
Consent for Publication
Not applicable.
Acknowledgments
The authors sincerely thank all subjects for participating and cooperating with them.
Funding
The research was funded by the Science and Technology Planning Project of Wenzhou (Y2023797,Y20240766). The Health Talent Program of Wenzhou People’s Hospital (No.RC-LCYJX202415).
Disclosure
Conflicts of interest are not declared by the authors.
References
1. Langelier C, Kalantar KL, Moazed F, et al. Integrating host response and unbiased microbe detection for lower respiratory tract infection diagnosis in critically ill adults. Proc Natl Acad Sci USA. 2018;115(52):E12353–E12362. doi:10.1073/pnas.1809700115
2. Azoulay E, Russell L, Van de Louw A, et al. Diagnosis of severe respiratory infections in immunocompromised patients. Intensive Care Med. 2020;46(2):298–314. doi:10.1007/s00134-019-05906-5
3. Womack J, Kropa J. Community-acquired pneumonia in adults: rapid evidence review. Am Family Phys. 2022;105(6):625–630.
4. Zhu YG, Tang XD, Lu YT, Zhang J, Qu JM. Contemporary situation of community-acquired pneumonia in china: a systematic review. J Translational Intern Med. 2018;6(1):26–31. doi:10.2478/jtim-2018-0006
5. Jain S, Self WH, Wunderink RG, et al. Community-acquired pneumonia requiring hospitalization among U.S. adults. New Engl J Med. 2015;373(5):415–427. doi:10.1056/NEJMoa1500245
6. Pendleton KM, Erb-Downward JR, Bao Y, et al. Rapid pathogen identification in bacterial pneumonia using real-time metagenomics. Am J Respir Crit Care Med. 2017;196(12):1610–1612. doi:10.1164/rccm.201703-0537LE
7. Gaston DC, Miller HB, Fissel JA, et al. Evaluation of metagenomic and targeted next-generation sequencing workflows for detection of respiratory pathogens from bronchoalveolar lavage fluid specimens. J Clin Microbiol. 2022;60(7):e0052622. doi:10.1128/jcm.00526-22
8. Li S, Tong J, Liu Y, Shen W, Hu P. Targeted next generation sequencing is comparable with metagenomic next generation sequencing in adults with pneumonia for pathogenic microorganism detection. J Infect. 2022;85(5):e127–e129. doi:10.1016/j.jinf.2022.08.022
9. Fu ZF, Zhang HC, Zhang Y, et al. Evaluations of clinical utilization of metagenomic next-generation sequencing in adults with fever of unknown origin. Front Cell Infect Microbiol. 2021;11:745156. doi:10.3389/fcimb.2021.745156
10. Miao Q, Ma Y, Wang Q, et al. Microbiological diagnostic performance of metagenomic next-generation sequencing when applied to clinical practice. Clin Infect Dis. 2018;67(suppl_2):S231–S240. doi:10.1093/cid/ciy693
11. Zheng Y, Qiu X, Wang T, Zhang J. The diagnostic value of metagenomic next-generation sequencing in lower respiratory tract infection. Front Cell Infect Microbiol. 2021;11:694756. doi:10.3389/fcimb.2021.694756
12. Wu X, Li Y, Zhang M, et al. Etiology of severe community-acquired pneumonia in adults based on metagenomic next-generation sequencing: a prospective multicenter study. Infect Dis Ther. 2020;9(4):1003–1015. doi:10.1007/s40121-020-00353-y
13. Hao J, Li W, Wang Y, Zhao J, Chen Y. Clinical utility of metagenomic next-generation sequencing in pathogen detection for lower respiratory tract infections and impact on clinical outcomes in southernmost China. Front Cell Infect Microbiol. 2023;13:1271952. doi:10.3389/fcimb.2023.1271952
14. Huang S, Chen J, Wang J, et al. Application of MRT-qPCR for pathogen detection of lower respiratory tract infection. Am J Transl Res. 2022;14(5):3311–3318.
15. Li X, Chen B, Zhang S, et al. Rapid detection of respiratory pathogens for community-acquired pneumonia by capillary electrophoresis-based multiplex PCR. SLAS Technology. 2019;24(1):105–116. doi:10.1177/2472630318787452
16. Zhu Q, Zhou J, Li F, et al. Nasopharyngeal aspirates in children with severe community-acquired pneumonia collected within 3 days before bronchoscopy can partially reflect the pathogens in bronchoalveolar lavage fluids. BMC Infect Dis. 2022;22(1):814. doi:10.1186/s12879-022-07749-w
17. Sun Y, Li H, Pei Z, et al. Incidence of community-acquired pneumonia in urban China: a national population-based study. Vaccine. 2020;38(52):8362–8370. doi:10.1016/j.vaccine.2020.11.004
18. Yin L, Zhang Y, Zheng Y, et al. Early detection of aspergillus species in lower respiratory tract is associated with higher mortality in viral community-acquired pneumonia: a multicenter prospective cohort study in China. Lung. 2023;201(4):387–396. doi:10.1007/s00408-023-00638-2
19. Shang L, Xu J, Cao B. Viral pneumonia in China: from surveillance to response. Lancet Public Health. 2020;5(12):e633–e634. doi:10.1016/S2468-2667(20)30264-4
20. Zhou F, Wang Y, Liu Y, et al. Disease severity and clinical outcomes of community-acquired pneumonia caused by non-influenza respiratory viruses in adults: a multicentre prospective registry study from the CAP-China Network. Europ resp J. 2019;54(2):1802406. doi:10.1183/13993003.02406-2018
21. Huang J, Jiang E, Yang D, et al. Metagenomic next-generation sequencing versus traditional pathogen detection in the diagnosis of peripheral pulmonary infectious lesions. Infect Drug Resist. 2020;13:567–576. doi:10.2147/IDR.S235182
22. Day MJ, Carey S, Clercx C, et al. Aetiology of canine infectious respiratory disease complex and prevalence of its pathogens in Europe. J Comparative Pathol. 2020;176:86–108. doi:10.1016/j.jcpa.2020.02.005
23. Zhang D, Chen S, Wang Y, et al. The evaluation of next-generation sequencing assisted pathogenic detection in immunocompromised hosts with pulmonary infection: a retrospective study. Clin Resp J. 2022;16(12):793–801. doi:10.1111/crj.13542
24. Arranz-Herrero J, Presa J, Rius-Rocabert S, et al. Determinants of poor clinical outcome in patients with influenza pneumonia: a systematic review and meta-analysis. Int J Infect Dis. 2023;131:173–179. doi:10.1016/j.ijid.2023.04.003
25. Ma J, Song X, M L, et al. Global spread of carbapenem-resistant Enterobacteriaceae: epidemiological features, resistance mechanisms, detection and therapy. Microbiol Res. 2023;266:127249. doi:10.1016/j.micres.2022.127249
26. Ambretti S, Bassetti M, Clerici P, et al. Screening for carriage of carbapenem-resistant Enterobacteriaceae in settings of high endemicity: a position paper from an Italian working group on CRE infections. Antimicrob Resist Infect Control. 2019;8(1):136. doi:10.1186/s13756-019-0591-6
27. Abbas R, Chakkour M, Zein El Dine H, et al. General overview of Klebsiella pneumonia: epidemiology and the role of siderophores in its pathogenicity. Biology. 2024;13(2):78. doi:10.3390/biology13020078
28. Cao B, Qu JX, Yin YD, Eldere JV. Overview of antimicrobial options for Mycoplasma pneumoniae pneumonia: focus on macrolide resistance. Clin Resp J. 2017;11(4):419–429. doi:10.1111/crj.12379
29. Lozano C, Fernández-Fernández R, Ruiz-Ripa L, Gómez P, Zarazaga M, Torres C. Human mecC-Carrying MRSA: clinical Implications and Risk Factors. Microorganisms. 2020;8(10):1615. doi:10.3390/microorganisms8101615
30. Feldman C, Shaddock E. Epidemiology of lower respiratory tract infections in adults. Expert Rev Resp Med. 2019;13(1):63–77. doi:10.1080/17476348.2019.1555040
31. Gao Q, Li L, Su T, et al. A single-center, retrospective study of hospitalized patients with lower respiratory tract infections: clinical assessment of metagenomic next-generation sequencing and identification of risk factors in patients. Respir Res. 2024;25(1):250. doi:10.1186/s12931-024-02887-y
32. Chen Q, Yi J, Liu Y, et al. Clinical diagnostic value of targeted next-generation sequencing for infectious diseases (Review). Mol Med Rep. 2024;30(3):153. doi:10.3892/mmr.2024.13277
33. Charalampous T, Kay GL, Richardson H, et al. Nanopore metagenomics enables rapid clinical diagnosis of bacterial lower respiratory infection. Nature Biotechnol. 2019;37(7):783–792. doi:10.1038/s41587-019-0156-5
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Diagnosis of Non-Tuberculous Mycobacterial Pulmonary Disease by Metagenomic Next-Generation Sequencing on Bronchoalveolar Lavage Fluid
Zhang X, Chen H, Lin Y, Yang M, Zhao H, Hu J, Han D
Infection and Drug Resistance 2023, 16:4137-4145
Published Date: 26 June 2023