")
Back to Journals » Infection and Drug Resistance » Volume 18
Are Glucocorticoids Truly Effective in Improving the Clinical Prognosis of HSV-1 Encephalitis?
Authors Xie S, Sun W, Lai Z, Liu X
Received 3 December 2024
Accepted for publication 20 February 2025
Published 5 March 2025 Volume 2025:18 Pages 1287—1296
DOI https://doi.org/10.2147/IDR.S501628
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sandip Patil
Shuhua Xie, Wei Sun, Zhaohui Lai, Xianghong Liu
Department of Neurology, Ganzhou People’s Hospital, Jiangxi, 341000, People’s Republic of China
Correspondence: Xianghong Liu, Email [email protected]
Background: Survivors of herpes simplex encephalitis (HSE) commonly experience significant neurological sequelae, imposing a substantial burden on both society and families. The efficacy of glucocorticoids in treating patients with HSE remains controversial. This study aims to evaluate the effectiveness of glucocorticoids in patients with HSE and analyze the clinical characteristics of this patient population.
Methods: This retrospective study evaluated the clinical characteristics, auxiliary examinations, and patient prognosis of HSE patients diagnosed with mNGS, and analyzed the prognosis of patients in both Glucocorticoid and Non-glucocorticoid groups. Assess the prognosis based on the improvement of GOS score and MMSE score at 1 and 3 months after discharge.
Results: A retrospective analysis was conducted in 29 hSE patients who met the criteria for GOS score improvement 3 months after discharge. The hormone group was better than the non-hormone group (2 (0– 2) scores VS 1 (1– 2) scores). There was no significant difference between the two groups in GOS score 1 month after discharge. However, no statistical difference was found in improving patient outcomes between the two groups.
Conclusion: Despite the hormone group not obtaining the anticipated positive outcomes, potentially due to the relatively limited sample size in this study, previous case series reports have indicated that glucocorticoids, when used as an adjunct to acyclovir therapy, may enhance patient outcomes. Consequently, further extensive clinical studies involving multiple centers and larger sample sizes are warranted to investigate this matter further.
Keywords: herpes simplex encephalitis, herpes simplex virus, glucocorticoid, atypical clinical manifestations, clinical prognosis
Corrigendum for this paper has been published.
Introduction
Infection with herpes simplex virus type 1 (HSV-1) has the potential to lead to life-threatening herpes simplex encephalitis.1 In recent years, advancements in diagnostic techniques such as Polymerase Chain Reaction(PCR), metagenomic Next Generation Sequencing (mNGS), and imaging, as well as the widespread clinical use of acyclovir, have contributed to a decreased mortality rate among HSE patients, dropping from 70% to 20%. Nonetheless, 70% of surviving patients continue to experience permanent neurological symptoms.2,3 Consequently, there is a pressing demand for the exploration of more efficacious treatment strategies in order to achieve improved clinical outcomes.
Brain damage resulting from HSE is well known to be caused by viral replication and an excessive inflammatory response, offering potential targets for the exploration of novel therapeutic approaches. Recent studies have assessed the long-term prognosis of HSE patients following antiviral treatment with acyclovir. Findings indicate a 15% mortality rate after 180 days from symptom onset. Among the surviving population, 14% experience full recovery, 23% have mild sequelae, 28% exhibit moderate neurological dysfunction, and 20% suffer from severe neurological sequelae.4 These neurological disabilities impose a substantial economic burden on society, necessitating the urgent improvement of treatment plans to reduce the occurrence of long-term HSE sequelae. Some researchers postulate that sustained low-level virus replication in the brain may contribute to neurological dysfunction in HSE patients. However, high-dose acyclovir (15mg/kg every 8 hours for 14 or 21 days) does not enhance the prognosis of adult patients.5 Another randomized, placebo-controlled clinical trial evaluated the efficacy of valacyclovir in HSE treatment. Results indicate that oral administration of valacyclovir for an additional 3 months (3 times a day, 2g each time) does not provide additional benefits compared to standard acyclovir treatment. The evaluation, based on Mini-mental State Examination (MMSE) and Mattis Dementia Rating Scale 12 months after onset, suggests that current active antiviral therapy falls short of achieving optimal therapeutic effects for HSE patients.6
Glucocorticoids, commonly used as broad-spectrum anti-inflammatory drugs, exert their anti-inflammatory effects through both genomic and non-genomic mechanisms.7 The genomic mechanism involves the interaction between glucocorticoid receptors and transcription factors, such as AP-1 and NF-κB, leading to the inhibition of pro-inflammatory genes. Non-genomic mechanisms involve the regulation of signal transduction pathways by glucocorticoid receptors and various kinases.8 However, glucocorticoids can also exhibit pro-inflammatory effects in the presence of injury or pathogens. In a study, rats with depleted glucocorticoid levels due to adrenalectomy, pituitary resection, or drug blockade were inoculated with HSV-1 into their brain ventricles one day later. Results revealed comparable viral titers in the brains of rats with depleted circulating glucocorticoids compared to the control group. Additionally, the synthesis of IL-1β and prostaglandin E2 was reduced.9 These inflammatory factors are associated with decreased fever, physical activity, and aggressive behavior, suggesting the involvement of autoimmune responses in the progression of HSE in patients.
Currently, guidelines recommend the use of glucocorticoids in the treatment of HSE only for specific conditions such as cerebral edema, intracranial hypertension, and cerebral herniation. While animal studies, case reports, and small case series have suggested the potential benefits of adjunctive glucocorticoid therapy in HSE, the lack of clinical trial validation hinders its widespread application in patients.2 The efficacy of glucocorticoids has been demonstrated in large-scale clinical trials for other central nervous system infections, such as bacterial and tuberculous meningitis.10 Several case series reports suggest that the use of glucocorticoids as adjunctive therapy with acyclovir may confer additional benefits.2 However, the German trial of acyclovir and glucocorticoids for the treatment of herpes simplex virus encephalitis (GACHE trial) was terminated prematurely due to slow recruitment of participants, and no statistical differences were observed in the main endpoint events of the study.11 Therefore, this study aims to evaluate the therapeutic impact of glucocorticoids in patients with HSV and explore the clinical characteristics of these cases.
Materials and Methods
Research Subjects
We retrospectively collected clinical data from patients diagnosed with HSE who were hospitalized in the neurology department of our institution between January 2018 and June 2023. This study received approval from the Ethics Committee of our institution and was conducted in accordance with the principles outlined in the 1964 helsinki Declaration.
Patients were selected based on the following inclusion criteria: (1) detection of HSV-1 virus infection through cerebrospinal fluid mNGS (2) fulfillment of diagnostic criteria for herpes simplex virus encephalitis; (3) adherence to the standard protocol for antiviral treatment and follow-up for 1–3 months after discharge; (4) receipt of written informed consent from either the patient or their family members. Exclusion criteria were as follows: (1) presence of central nervous system tumors; (2) encephalitis combined with multiple pathogen infections; (3) autoimmune encephalitis; (4) incomplete clinical data and non-standard case records; (5) previous history of puncture injury.
Data Collection
The recorded baseline characteristics, such as demographic information, time from symptom onset to hospital admission, infection risk factors, and presenting symptoms, contribute to a comprehensive understanding of the studied infection. The patient underwent antiviral treatment, cranial imaging, and laboratory tests to further evaluate their condition.
Clinical Outcomes
As per the Glasgow Outcome Scale (GOS), patient prognosis is categorized into five groups: death, vegetative state, severe sequelae necessitating daily assistance, moderate sequelae necessitating independent living, no sequelae, or mild sequelae. Assessment of outcomes occurs at discharge and during follow-up at 1 and 3 months post-discharge. A GOS score of < 4 indicates a poor prognosis. The MMSE yields a total score of 30 points, with a rating of 27–30 points being deemed normal and a score below 27 indicating cognitive impairment. Dementia classification criteria vary based on the subjects’ educational levels: ≤ 17 points for illiteracy, ≤ 20 points for primary school education, ≤ 22 points for secondary school education, and ≤ 23 points for university education. Mild dementia is defined as MMSE scores ≥ 21 points, moderate dementia as MMSE scores of 10–20 points, and severe dementia as MMSE scores of ≤ 9 points.
Statistical Analysis
Data analysis was performed using SPSS 22.0 software, with the chi-square test employed to assess differences between two groups for count data. Results were presented as n (%), representing the number and percentage within each group. For normally distributed measurement data, T-test was utilized and outcomes were reported as mean±SD, indicating the mean and standard deviation. In the case of non-normal distribution, non-parametric tests were used and results were expressed as M (IQR), denoting the median and interquartile range (25th to 75th percentile).
Results
Clinical Characteristics of the Patient
Through rigorous adherence to inclusion and exclusion criteria, we enrolled 29 patients, all of whom received a diagnosis of herpes simplex virus type 1 encephalitis utilizing mNGS technology. Table 1 outlines the demographic characteristics of these patients, including 20 males and 9 females, with an average age of (45.83 ± 17.41) years. Notably, 2 patients (6.9%) had comorbid type 2 diabetes. The mean duration from symptom onset to hospital admission for treatment was 5 (3–7.5) days. Upon admission, 23 patients (79.3%) presented with a body temperature exceeding 38.0°C. Regarding symptoms, 16 cases (55.2%) experienced headaches, 12 cases (41.4%) reported nausea and vomiting, and 4 cases (13.8%) manifested abnormal motor sensations. Additionally, 21 cases (72.4%) demonstrated advanced cortical dysfunction, characterized by personality changes, decreased memory, and abnormal mental behavior. The average interval from symptom onset to completion of imaging examination for each patient was 7 (4–11) days, with variation in lesion distribution across different brain regions. Cerebrospinal fluid (CSF) analysis revealed an average of 90 CSF cells (predominantly lymphocytes) in all patients. All patients underwent mNGS testing, yielding an average sequence number of 17206 (729–47,722). The average length of hospital stay for all patients was 18 (11–22) days. The table below presents the Glasgow Coma Scale (GCS), GOS, and MMSE scores at admission, discharge, and one month post-discharge.
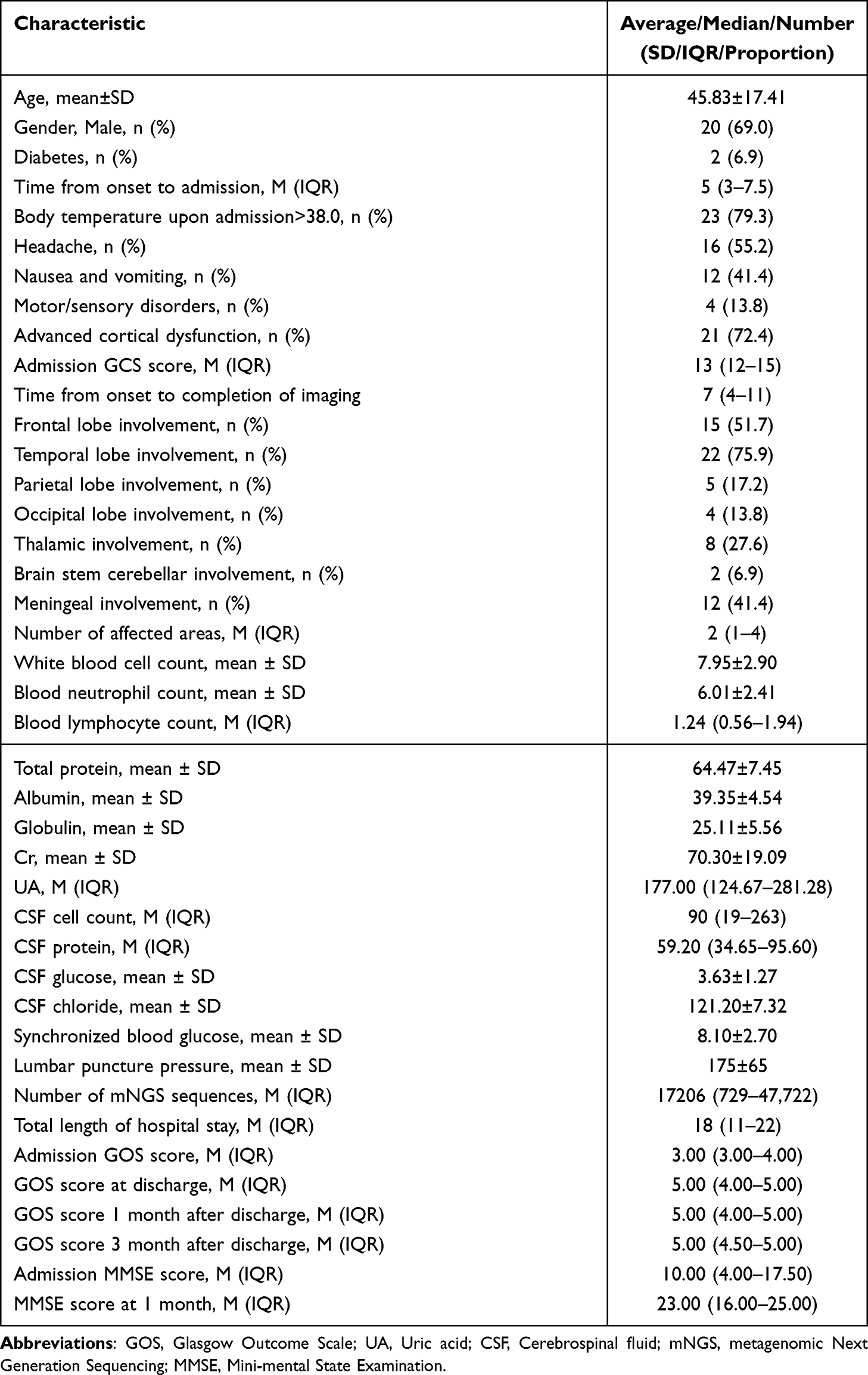 |
Table 1 Clinical Characteristics of 29 Patients with HSE |
Univariate Analysis of Hormone Use and Nonuse Groups
We conducted a meticulous analysis of the data from these 29 patients, 15 of whom received Glucocorticoid therapy. A comparative assessment of the two groups revealed that a single time point GOS score of 5, denoting a normal state, may not adequately reflect a patient’s recovery. As such, we utilized the admission score as a baseline and assessed efficacy by examining changes in GOS and MMSE scores post-treatment. Our findings demonstrated superior improvement in GOS scores three months post-discharge in the glucocorticoid group compared to the non-glucocorticoid group (2 (0–2) points vs 1 (1–2) points, P=0.780) (Table 2). And the improvement in GOS score after 3 months is better than that after 1 month (Figures 1 and 2). However, there was minimal disparity in GOS scores at one month post-discharge between the two groups. Regrettably, statistical analysis did not reveal a significant difference in patient prognosis improvement between the glucocorticoid and non-glucocorticoid groups.
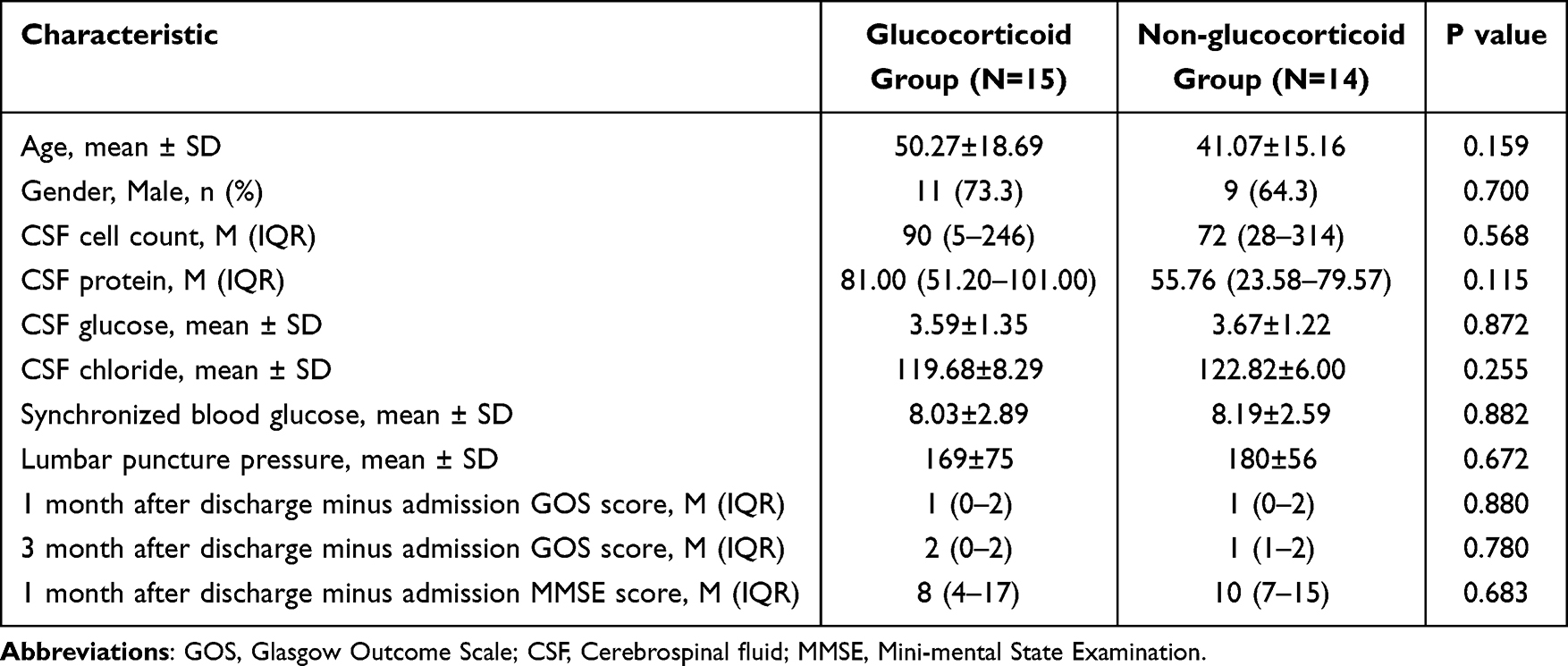 |
Table 2 Comparison of the Prognosis and CSF Characteristics Between the Glucocorticoid Group and Non-Glucocorticoid Group |
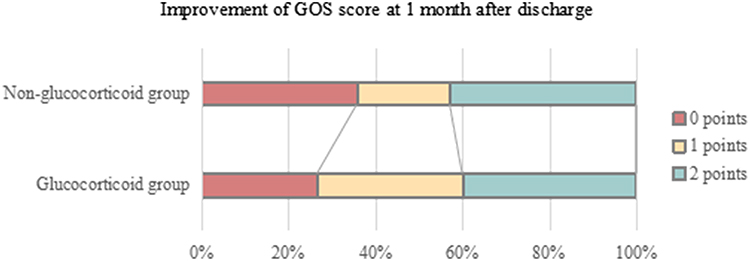 |
Figure 1 Improvement of GOS score at 1 month after discharge. |
 |
Figure 2 Improvement of GOS score at 3 month after discharge. |
Univariate Analysis of Good Prognosis Group and Poor Prognosis Group
We classified patients into two groups based on their GOS score after one month of discharge, with scores less than 5 indicating a poor prognosis group and a score of 5 indicating a good prognosis group. Out of the total sample, 11 patients (37.9%) were in the poor prognosis group, while 18 patients (62.1%) were in the good prognosis group. The average age of the good prognosis group was lower than that of the poor prognosis group (42.50 ± 17.35 years vs 51.27 ± 16.87 years, P=0.193). The hospital admission time was significantly earlier in the good prognosis group compared to the poor prognosis group (5 cases (2–6) vs 7 cases (5–13), P=0.028). The proportion of patients with advanced cortical dysfunction was significantly higher in the poor prognosis group (11 cases, 100.0%) compared to the good prognosis group (10 cases, 55.6%). Similarly, the proportion of patients with temporal lobe involvement was significantly higher in the poor prognosis group (11 cases, 100.0%) compared to the good prognosis group (11 cases, 61.1%). Additionally, the number of viral sequences was significantly lower in the good prognosis group (6612, 550–53208) compared to the poor prognosis group (23732, 12,907–7306) (Table 3).
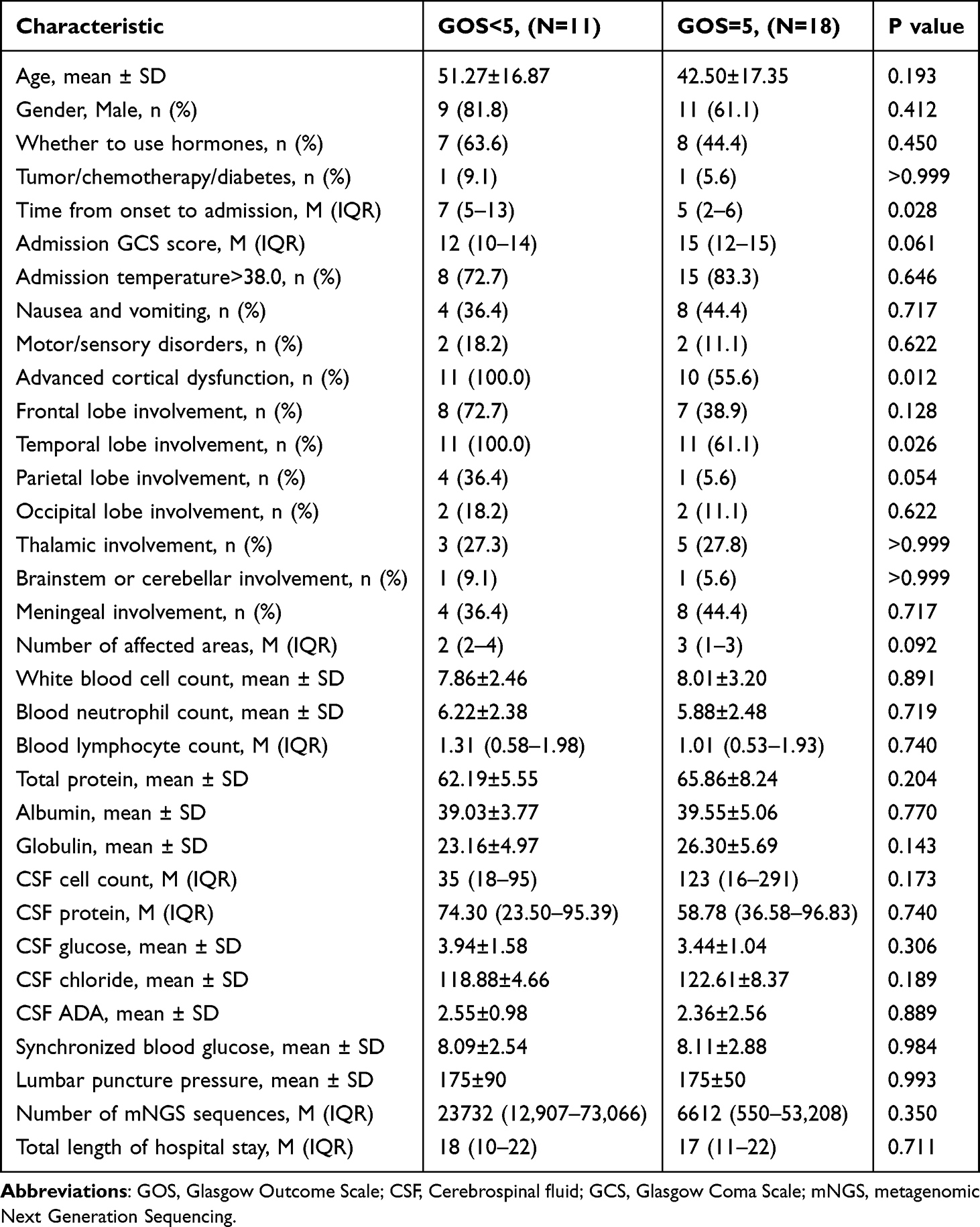 |
Table 3 Compare the Clinical Characteristics of Patients with Good and Poor Prognosis Groups |
Multivariate Analysis of Grouping Based on 1-month GOS Scores
We categorized the patients into two groups based on their GOS scores one month after discharge. We then conducted a binary logistic regression analysis on potential predictors and confounding factors (variables with p<0.1 in univariate analysis) between the group with a good prognosis and the group with a poor prognosis. The specific factors assessed included the time from onset to admission, symptoms of advanced cortical dysfunction, GCS score, involvement of the temporal lobe, involvement of the parietal lobe, and the number of affected areas. However, the multivariate regression analysis did not identify any independent prognostic factors (Table 4).
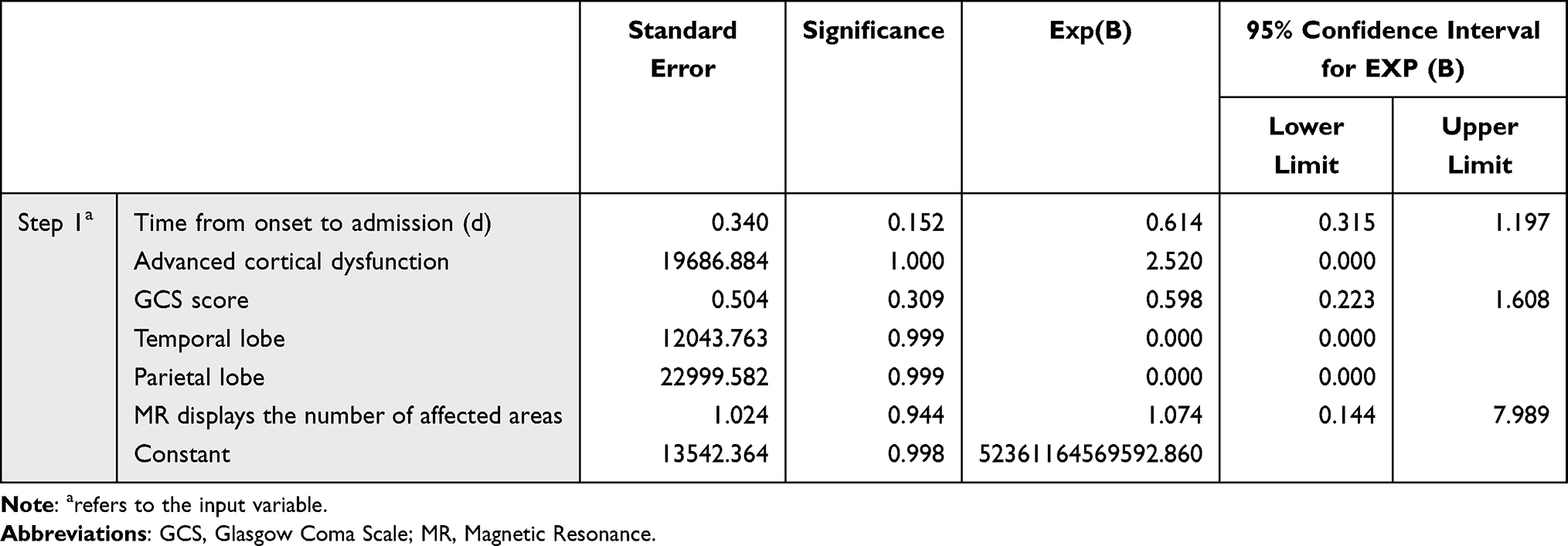 |
Table 4 Logistic Regression Analysis of Potential Predictive Factors for Two Groups of Patients with Different Prognosis |
Discussion
HSE is responsible for 50–75% of cases of viral encephalitis, with an annual incidence rate of approximately 2–4 cases per million individuals.12 In adults and children, more than 90% of HSE cases are caused by HSV-1 infection, whereas encephalitis caused by HSV-2 typically occurs in newborns or immunocompromised patients.13 Around 30% of HSE cases result from primary HSV-1 infection, while the remaining cases are attributed to virus reactivation or reinfection.14 Unlike arboviruses and enteroviruses, the incidence of HSE remains constant throughout the year and is not influenced by geographical location. The disease exhibits a bimodal age distribution, with a small peak occurring in children (aged 6 months to 3 years) and a larger peak in adult patients (over 50 years old).15 In our study, the average age of onset was 45.83±17.41 years, with males accounting for 69.0% of cases. Although there is no significant difference in the incidence rate of HSE between individuals with normal immune function and those with impaired immune function, the latter group experiences higher incidence rates and mortality.16 Among our patients, only two had diabetes, and no other immune deficiency diseases were identified.
The typical clinical manifestations of HSE encompass various symptoms and signs. These include headache, vomiting, alterations in consciousness, mental symptoms, memory loss, cognitive decline, aphasia, mild hemiplegia, hemiblindness, ataxia, hyperactivity (such as tremors, myoclonus, and dance-like movements), and others. Approximately one-third of patients experience partial or systemic seizures.17,18 In some cases, the onset of HSE is subacute or chronic, and patients may initially seek psychiatric treatment due to abnormal mental behavior, which can lead to misdiagnosis and impact treatment and prognosis. In our study, non-specific HSE symptoms such as fever, headache, nausea, and vomiting were commonly observed in all patients. Conversely, characteristic clinical symptoms of HSE, such as personality changes, abnormal behavior, and other impairments in higher-level cortical function, were frequently present. However, motor sensory disorders and disturbances in consciousness were relatively rare, indicating a correlation with the affected brain regions and the extent of tissue damage.
The immune response elicited during HSE serves to initially restrict viral replication and subsequently needs to be controlled to prevent excessive inflammation and damage to vulnerable organs like the brain. Therefore, the host immune response is considered a delicate balance, functioning as a double-edged sword. Immunomodulatory drugs should be administered at critical stages of HSE to attenuate delayed and excessive inflammation in the central nervous system, thereby reducing the risk of neurological complications. This immune regulation strategy should be combined with antiviral therapy to suppress viral replication and inflammatory response.2,19 The role of glucocorticoids, commonly used as broad-spectrum anti-inflammatory drugs in HSV treatment, remains controversial. Multiple studies have demonstrated that glucocorticoids can enhance both inflammation and immunity, but their effects appear to be dose-dependent. Lim’s study revealed that low levels of glucocorticoids can promote the production of nitric oxide and the mRNA expression of enzymes necessary for the synthesis of pro-inflammatory cytokines, chemokines, and mediators. Conversely, high concentrations of glucocorticoids strongly inhibit macrophage function, thereby suppressing the transcription of inflammatory genes.20
Our dataset comprised 15 patients who received steroid treatment and 14 patients who did not. By evaluating the prognosis based on the improvement of GOS scores and MMSE scores during the first and third months after discharge in both groups, as well as performing univariate analysis of cerebrospinal fluid and other indicators, we observed that the hormone group exhibited better improvement in GOS scores compared to the non-hormone group at the three-month mark after discharge. This finding aligns with the majority of previous studies, which indicate that short-term outcomes following viral meningitis are often unfavorable but show improvement during long-term follow-up.21 However, the two datasets did not demonstrate significant statistical differences (Table 2), possibly due to the limited number of cases included in our study.
The GOS score at one month post-discharge was categorized into two groups: good prognosis and poor prognosis. Univariate analysis revealed that a shorter duration from symptom onset to admission was associated with a better prognosis for patients. Therefore, it is recommended to initiate antiviral treatment promptly for patients suspected of having herpes simplex virus encephalitis based on clinical manifestations and initial cerebrospinal fluid examination.1,22 Furthermore, the combination of advanced cortical dysfunction and involvement of the temporal lobe indicates a poorer prognosis, possibly due to the retrograde entry of HSV into the skull through cranial nerves, with the frontal and temporal lobes being the initial sites of infection. Routine and biochemical indicators of cerebrospinal fluid did not show significant differences between the two groups. However, the number of virus detection sequences (Reads) was significantly lower in the good prognosis group compared to the poor prognosis group. The number of detected sequences reflects the pathogen’s load, nucleic acid extraction amount, and the proportion of human source sequences in the sample. This suggests that the group with a poor prognosis had a higher viral load, although the difference between the two groups did not reach statistical significance.
Limitations
The study’s sample size is relatively small and may not be representative of the entire population, limiting the generalizability of the results. Future research will utilize larger sample sizes to validate findings and offer more precise and comprehensive results. Additionally, the GOS score, employed to assess prognosis and recovery, was designed for evaluating recovery after brain injury and may not fully capture subtle neurocognitive impairments in patients with central nervous system infections, potentially leading to an exaggerated effect. Overall, larger and more comprehensive studies are needed to enhance understanding of the clinical symptoms, imaging features, and hormone therapy effects in HSE patients.
Conclusion
In summary, this retrospective study examined the potential impact of hormones in patients with HSE, analyzed the clinical and imaging features of 29 hSV patients, and compared the clinical indicators between patients with favorable and unfavorable prognoses. Although the hormone group did not yield the expected positive results, extensive prior case series reports suggest that incorporating glucocorticoids as adjunctive medication with acyclovir treatment may enhance benefits. This warrants further multicenter, large-scale clinical trials to validate our hypothesis.
Research Ethics Committee (REC)/Institutional Review Board (IRB)
Clinical Research Ethics Subcommittee of Ganzhou People’s Hospital “This paper has been uploaded to Research Square as a preprint: https://www.researchsquare.com/article/rs-3998490/v1”.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Acknowledgments
An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR.
The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Science and Technology Plan Project of Jiangxi Provincial Health Commission, Fund No.: SKJP220210011.
Disclosure
The authors declare no conflicts of interest.
References
1. Bradshaw MJ, Venkatesan A. Herpes simplex virus-1 encephalitis in adults: pathophysiology, diagnosis, and management. Neurotherapeutics. 2016;13:493–508. doi:10.1007/s13311-016-0433-7
2. Piret J, Boivin G. Immunomodulatory strategies in herpes simplex virus encephalitis. Clin Microbiol Rev. 2020;33. doi:10.1128/CMR.00105-19
3. Armangue T, Spatola M, Vlagea A, et al. Spanish herpes simplex encephalitis study, frequency, symptoms, risk factors, and outcomes of autoimmune encephalitis after herpes simplex encephalitis: a prospective observational study and retrospective analysis. Lancet Neurol. 2018;17:760–772. doi:10.1016/S1474-4422(18)30244-8
4. Jouan Y, Grammatico-Guillon L, Espitalier F, et al. Long-term outcome of severe herpes simplex encephalitis: a population-based observational study. Crit Care. 2015;19(1):345. doi:10.1186/s13054-015-1046-y
5. Stahl JP, Mailles A, De Broucker T, et al. Herpes simplex encephalitis and management of acyclovir in encephalitis patients in France. Epidemiol Infect. 2012;140:372–381. doi:10.1017/S0950268811000483
6. J.w. G Jr, Skoldenberg B, Hart J, et al. National institute of, and G. Infectious diseases collaborative antiviral study, herpes simplex encephalitis: lack of clinical benefit of long-term valacyclovir therapy. Clin Infect Dis. 2015;61:683–691. doi:10.1093/cid/civ369
7. Cruz-Topete D, Cidlowski JA. One hormone, two actions: anti- and pro-inflammatory effects of glucocorticoids. Neuroimmunomodulation. 2015;22:20–32. doi:10.1159/000362724
8. Cain DW, Cidlowski JA. Immune regulation by glucocorticoids. Nat Rev Immunol. 2017;17:233–247. doi:10.1038/nri.2017.1
9. Ben-Hur T, Cialic R, Itzik A, et al. A novel permissive role for glucocorticoids in induction of febrile and behavioral signs of experimental herpes simplex virus encephalitis. Neuroscience. 2001;108(1):119–127. doi:10.1016/S0306-4522(01)00404-3
10. de Gans J, van de Beek D. European dexamethasone in adulthood bacterial meningitis study, dexamethasone in adults with bacterial meningitis. N Engl J Med. 2002;347:1549–1556. doi:10.1056/NEJMoa021334
11. Martinez-Torres F, Menon S, Pritsch M, et al. Protocol for German trial of acyclovir and corticosteroids in herpes-simplex-virus-encephalitis (GACHE): a multicenter, multinational, randomized, double-blind, placebo-controlled German, Austrian and Dutch trial [ISRCTN45122933]. BMC Neurol. 2008;8:40. doi:10.1186/1471-2377-8-40
12. Jorgensen LK, Dalgaard LS, Ostergaard LJ, et al. Incidence and mortality of herpes simplex encephalitis in Denmark: a nationwide registry-based cohort study. J Infect. 2017;74(1):42–49. doi:10.1016/j.jinf.2016.09.004
13. Aurelius E, Johansson B, Skoldenberg B, Forsgren M. Encephalitis in immunocompetent patients due to herpes simplex virus type 1 or 2 as determined by type-specific polymerase chain reaction and antibody assays of cerebrospinal fluid. J Med Virol. 1993;39:179–186. doi:10.1002/jmv.1890390302
14. Vora NM, Holman RC, Mehal JM, et al. Burden of encephalitis-associated hospitalizations in the United States, 1998-2010. Neurology. 2014;82:443–451. doi:10.1212/WNL.0000000000000086
15. Hjalmarsson A, Blomqvist P, Skoldenberg B. Herpes simplex encephalitis in Sweden, 1990-2001: incidence, morbidity, and mortality. Clin Infect Dis. 2007;45:875–880. doi:10.1086/521262
16. Tan IL, McArthur JC, Venkatesan A, Nath A. Atypical manifestations and poor outcome of herpes simplex encephalitis in the immunocompromised. Neurology. 2012;79:2125–2132. doi:10.1212/WNL.0b013e3182752ceb
17. Hansen AE, Vestergaard HT, Dessau RB, et al. Long-term survival, morbidity, social functioning and risk of disability in patients with a herpes simplex virus type 1 or type 2 central nervous system infection, Denmark, 2000-2016. Clin Epidemiol. 2020;12:745–755. doi:10.2147/CLEP.S256838
18. Gnann JW Jr, Whitley RJ. Herpes Simplex Encephalitis: an Update. Curr Infect Dis Rep. 2017;19:13. doi:10.1007/s11908-017-0568-7
19. Piret J, Boivin G. Innate immune response during herpes simplex virus encephalitis and development of immunomodulatory strategies. Rev Med Virol. 2015;25:300–319. doi:10.1002/rmv.1848
20. Lim HY, Muller N, Herold MJ, et al. Glucocorticoids exert opposing effects on macrophage function dependent on their concentration. Immunology. 2007;122:47–53. doi:10.1111/j.1365-2567.2007.02611.x
21. Petersen PT, Bodilsen J, Jepsen MPG, et al. Danish study group of infections of the, clinical features and prognostic factors in adults with viral meningitis. Brain. 2023;146:3816–3825. doi:10.1093/brain/awad089
22. Tunkel AR, Glaser CA, Bloch KC, et al. Infectious diseases society of, the management of encephalitis: clinical practice guidelines by the infectious diseases society of America. Clin Infect Dis. 2008;47:303–327. doi:10.1086/589747
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.