")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Ascorbic Acid and Esketamine for Mental Disorders in Women with Miscarriage: A Randomized Controlled Double-Blind Trial Protocol
Authors Ke Z, Zhang Y , Cai B, Luo J, Ma Y, Chen Q, Deng L
Received 8 January 2025
Accepted for publication 28 March 2025
Published 11 April 2025 Volume 2025:21 Pages 815—825
DOI https://doi.org/10.2147/NDT.S516355
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Zhaojuan Ke,1 Ying Zhang,1 Binyang Cai,1 Jie Luo,1 Yao Ma,2 Qibin Chen,1 Linya Deng1
1Department of Anesthesiology, The First Affiliated Hospital of Chongqing Medical University, Chongqing, 400016, People’s Republic of China; 2Department of Geriatrics and National Clinical Research Center for Geriatrics, West China Hospital, Sichuan University, Chengdu, Sichuan Province, 610041, People’s Republic of China
Correspondence: Jie Luo, Department of Anesthesiology, The First Affiliated Hospital of Chongqing Medical University, No. 1 Youyi Road, Yuzhong District, Chongqing, 400016, People’s Republic of China, Tel +86-023-89011069, Email [email protected]
Purpose: Pregnancy leads to vulnerabilities and susceptibilities to mental disorders. Miscarriage, as an adverse pregnancy outcome, and following curettage for treatment, add the risks of further psychiatric disorders, including depression, anxiety, insomnia, etc., and current approaches to prevention are unsatisfactory. Ketamine and its S-enantiomer esketamine can prevent postpartum depression, and esketamine even treats depressive symptoms after miscarriage curettage, but their side effects bring limitations. Ascorbic acid (AA, Vitamin C) can modulate mood and enhance ketamine’s antidepressant efficacy synergistically, reducing its dosages and adverse effects potentially. The purpose of this study is to clarify the beneficial modification of AA on esketamine for preventing depression and other mental disorders in patients with miscarriage after painless curettage, as well as the interaction between AA and esketamine.
Patients and Methods: This study is a 2× 2 factorial, double-blinded, randomized, controlled trial that will recruit women with miscarriage undergoing painless curettage. A total of 424 participants will be recruited and randomly 1:1:1:1 allocated to the following four groups (106 in each): Group A0K0 (normal saline and normal saline), Group A0K1 (normal saline and esketamine), Group A1K0 (AA and normal saline), and Group A1K1 (AA and esketamine). The primary outcome is the incidence of depression on postoperative day 7, assessed with the Edinburgh Postnatal Depression Scale (EPDS). The secondary outcomes include the EPDS score, assessments of anxiety, sleep, and pain, adverse events, perianesthetic data and patient satisfaction.
Discussion: This study provides the clinical trial-based evidence of the effects of AA alone or in combination/interacting with the emerging rapid-acting antidepressant esketamine on depression and other mental disorders in patients with miscarriage undergoing painless curettage. Our data are expected to suggest AA’s potential application for optimizing strategies of promoting post-miscarriage mental health, and its possible adjunctive improvement of (es)ketamine’s usage as antidepressants. One major limitation is that this study is a single-center study, and the results might be biased due to regional factors.
Keywords: ketamine, vitamin C, depression, anxiety, sleep disorders, pain
Introduction
Pregnancy and childbirth are periods of a woman’s life when physical and mental health fluctuates significantly, and she has severe vulnerabilities and susceptibility to psychiatric disorders. Miscarriage is generally defined as the loss of a pregnancy before viability, and an estimated 23 million miscarriages occur globally every year, translating to 44 pregnancy losses each minute.1 As a kind of adverse pregnancy without positive encouragement from childbirth, miscarriage causes both physical and psychological consequences with greater psychological frustration, being strongly associated with anxiety, depression, post-traumatic stress, and suicide, which even exist 9 months after a pregnancy loss.1,2 Moreover, those who undergo curettage as a necessary treatment will experience a heavier burden of mental illness from both trauma and bereavement, including depression, anxiety, sleep disorders, and postoperative pain as overlapping comorbidities, with greater impact on their long-term prognosis, but often underestimated.3,4 Ranking in the top priorities for research in miscarriage, attention has been paid to the screening and control of high-risk factors and searching for better treatment strategies, meanwhile, the development of prophylaxis benefits the patients by preventing chronic prolongation of early adverse symptoms.5 However, the current prevention methods are unsatisfactory and have yet to be explored, opening space for new options.
Painless curettage under general anesthesia can eliminate the fear and pain during the procedure, improve the comfort, and reduce the neuropsychiatric impairment aggravated by the procedure. As conventional anesthetics and analgesics, ketamine and its S-enantiomer esketamine (S-ketamine), when used as elements in general anesthesia or with subanesthetic doses as additional medications, have been found to alleviate postoperative depression, anxiety, sleep disturbance, and pain in patients undergoing a variety of surgeries.6–9 Evidence has supported the use of ketamine or esketamine with additional subanesthetic doses for postpartum depression (PPD), pain and overall mental impairment in women undergoing cesarean delivery or labor analgesia.10–12 As the anesthetic components or with additional subanesthetic doses, ketamine or esketamine can additionally treat postoperative depressive symptoms and pain severity or prophylactically improve postoperative mood in patients undergoing painless curettage for miscarriage.13,14 As compared with ketamine, esketamine has a higher affinity for glutamate N-methyl-D-aspartate receptor (NMDAR), being two times more potent, but has side effects and potential risks as well, including psychiatric and cardiovascular adverse effects especially, which has also become the concern limiting its clinical application.7,14,15 Ketamine and its isomers are new rapid antidepressants, which have been regarded as the most important advance in the treatment of depression in the past half century, and the exploration and development of related clinical applications can be recognized as research priorities.16,17
Ascorbic acid (AA, ie vitamin C) is a water-soluble vitamin that has been shown to be negatively associated with depression.18 AA deficiency is widely associated with stress-related disorders such as depression and anxiety, and AA supplementation can produce antidepressant effects and improve mood.19 Preclinical studies have shown that administration of AA produces antidepressant-like and anxiolytic-like effects similar to ketamine in mice.20–22 Intraoperative intravenous AA administration can relief postoperative pain, reduce morphine consumption, and promote functional recovery.23 Although AA has not been able to treat depression independently so far, it may be used as an adjunct to antidepressant treatment. Clinical evidence indicates that AA-adjuvant fluoxetine therapy reduces depressive symptoms in children with major depressive disorder significantly.24 The combination of AA and sub-effective dose ketamine can reverse the depressive-like behavior induced by chronic unpredictable stress completely in mice.25 Furthermore, the synergistic effects of AA on ketamine are also shown in a study on ketamine for anesthesia in rabbits, indicating that AA shortens the time to onset of ketamine anesthesia, prolongs the duration of anesthesia, and reduces heart rate significantly.26
Mechanisms that underlie the synergistic effects of AA and esketamine remain obscure. Deficits of neuroplasticity is a major cause of depression, and women during pregnancy and childbirth are more vulnerable and susceptible to depression because of the particularly highly activated neuroplasticity, the abnormalities of which are the target for the therapeutic effects of antidepressants such as (es)ketamine as well.27–30 (Es)ketamine, as a NMDAR antagonist, enhances glutamate release from the presynaptic membrane, and glutamate’s activation of α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid receptor (AMPAR) initiates a series of intracellular signal transduction cascades, ultimately leading to changes in structural and functional neuroplasticity.31,32 Similar to ketamine, AA elevates synaptic protein levels and dendritic remodeling, reversing deficits of hippocampus synaptic plasticity caused by depression modeling factors.22,33 Neuroplasticity may be an important overlapping target for the synergistic effects of ascorbic acid and (es)ketamine.
Therefore, in view of the positive effects of AA on depression, anxiety, postoperative pain, etc., as well as its synergistic effects on the efficacy of ketamine and the corresponding reduction of adverse effects, it can be assumed that the use of AA alone or in combination with ketamine may be an alternative for the neuropsychiatric health of patients with miscarriage undergoing curettage. The purpose of this study is to explore the efficacy and safety of AA or its combination with esketamine, as well as their possible interactions, in these patients for prevention of psychiatric disorders.
Materials and Methods
Study Design
Ethical approval of this study was received from the Institutional Review Board of the First Affiliated Hospital of Chongqing Medical University (ethics approval number: 2024–239-01) and registered in the Chinese Clinical Trial Registry (number: ChiCTR2400094712). This study is designed according to the Standard Protocol Items: Recommendations for Interventional Trials (SPIRIT), and it is a prospective factorial-designed randomized controlled and blinded trial. This study is aimed to investigate the effects of AA, esketamine, and their combination in patients with miscarriage undergoing painless curettage, and the interaction between AA and esketamine. The participants are randomly divided into four groups, Group A0K0, Group A0K1, Group A1K0, and Group A1K1, according to the 2×2 factorial design at each level of the two factors (AA and esketamine). The authors adhere to the Declaration of Helsinki for the clinical trial. Flowchart of the study process can be found in Figure 1.
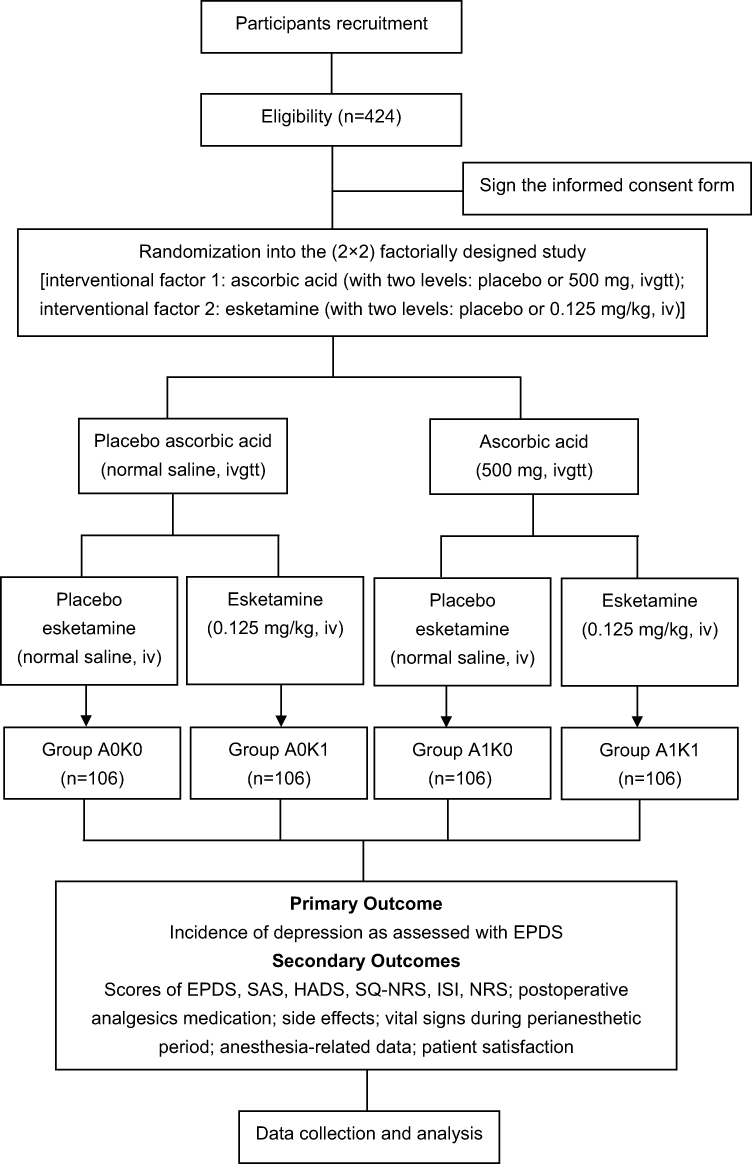 |
Figure 1 Study design and flow chart. Abbreviations: AA, ascorbic acid; EPDS, Edinburgh Postnatal Depression Scale; HADS, Hospital Anxiety and Depression Scale; ISI, Insomnia Severity Index; NRS, Numeric Rating Scale; SAS, Self-Rating Anxiety Scale; SQ-NRS, Sleep Quality Numerical Rating Scale. |
Participant and Recruitment
After signing on the informed consent form, the eligible participants are enrolled in the trial and can withdraw at any time.
Inclusion criteria: (1) females with the ages between 18 and 45 years, American Society of Anesthesiologists classification 1 to 2, body mass index being 18.5–30 kg/m2; (2) patients with miscarriage who are scheduled for elective painless curettage under intravenous general anesthesia; (3) the patient understands, agrees and signs the informed consent.
Exclusion Criteria: (1) those with American Society of Anesthesiologists classification ≥ 3; (2) complicated with serious diseases, such as uncontrolled hypertension, uncontrolled diabetes, severe dysfunctions of heart, liver, kidney, or lung or any contraindications to (es)ketamine or AA; (3) allergy to AA or (es)ketamine; (4) history of any mental illness; (5) history of antipsychotic medication; (6) neurological dysfunction; (7) epilepsy; (8) history of (es)ketamine abuse or dependence; (9) previous trials of (es)ketamine were ineffective or had serious adverse effects; (10) drug or alcohol dependence; (11) acute genital inflammation, such as vaginitis, pelvic inflammatory diseases; (12) failure of medical induction of abortion; (13) suffering from diseases or conditions that affect the completion or efficacy evaluation, such as cognitive impairment, illiteracy, mental disability, etc.; (14) participated in other clinical trials within the past 6 months.
Dropout Criteria: (1) violation of legitimacy of the trial; (2) patients with serious complications during trial intervention, procedure, or anesthesia; (3) patients or their families who request to withdraw from the trial for various reasons.
Randomization, Allocation Concealment and Blinding
A total of 424 participants will be included, and randomly divided into four groups in equal proportions (106 in each group). With a serial number randomly generated by the computer, each participant is assigned to a specific group, and information of allocation is concealed in opaque sealed envelopes. These groups include intervention with normal saline and normal saline (Group A0K0), normal saline and esketamine (Group A0K1), AA and normal saline (Group A1K0), and AA and esketamine (Group A1K1). The interventions for each group are prepared by specific personnel who does not participate in the further process of the trial. A second investigator conducts the implementation of the interventions with the information from the envelopes, and other investigators collect and manage the data. Both AA and esketamine can be prepared into colorless transparent liquids, which can be modified to the appearance of normal saline as their controls. Therefore, both patients and observers can be double-blinded.
Intervention
AA (0.5 g/2 mL, Shandong Xinhua Pharmaceutical Co., Ltd, Zibo, Shandong, China) is used with a dose of 500 mg, combined with 100 mL normal saline, and slowly dripped intravenously (ivgtt) before induction of general anesthesia. Esketamine (50 mg/2 mL, Hengrui Pharmaceutical Co., Ltd, Lianyungang, Jiangsu, China) is used with a dose of 0.125 mg/kg, and slowly injected intravenously (iv) after anesthetic induction. The control of AA is 100 mL normal saline, and the control of esketamine is a slow intravenous bolus of normal saline with the same appearance. According to the study design, the participants in different groups receive the following interventions: (1) Group A0K0, normal saline (100 mL, ivgtt) and normal saline (the same appearance as esketamine, iv); (2) Group A0K1, normal saline (100 mL, ivgtt) and esketamine (0.125 mg/kg, iv); (3) Group A1K0, AA 500 mg combined with normal saline (100 mL, ivgtt) and normal saline (the same appearance as esketamine, iv); (4) Group A1K1, AA 500 mg combined with normal saline (100 mL, ivgtt) and esketamine (0.125 mg/kg, iv).
Outcomes
Outcomes are measured preoperatively, after the recovery from anesthesia, and from the 1st to the 42nd day after the procedures using a series of self-report scales or questionnaires, and objective indicators by other independent investigators, and the classification and timing for assessment of each outcome are shown in Table 1 and Figure 2. In order to reduce the bias of detection, the evaluations of a different scale are conducted by the same corresponding investigator who has been trained.
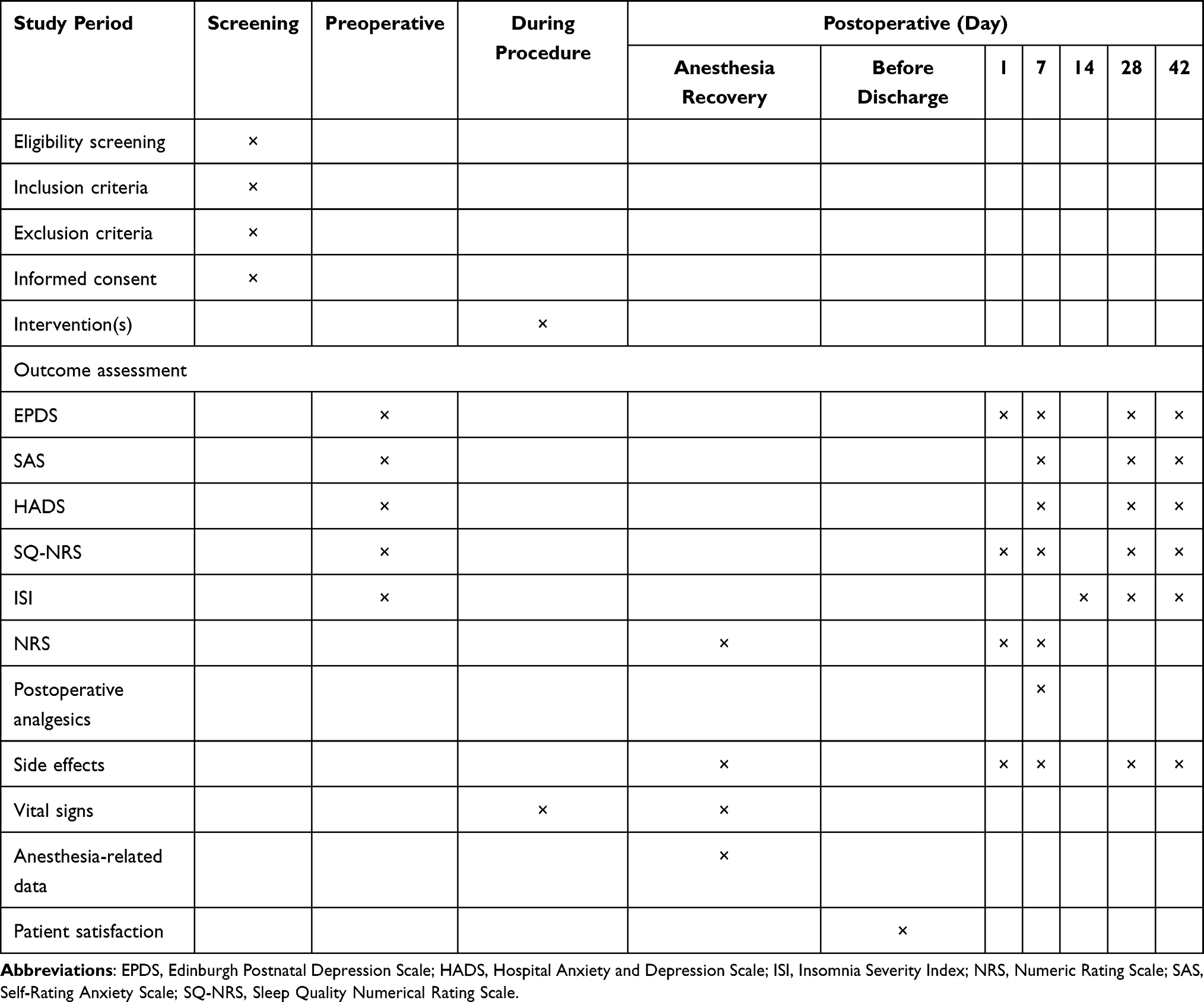 |
Table 1 Overview of Time Points in This Trial |
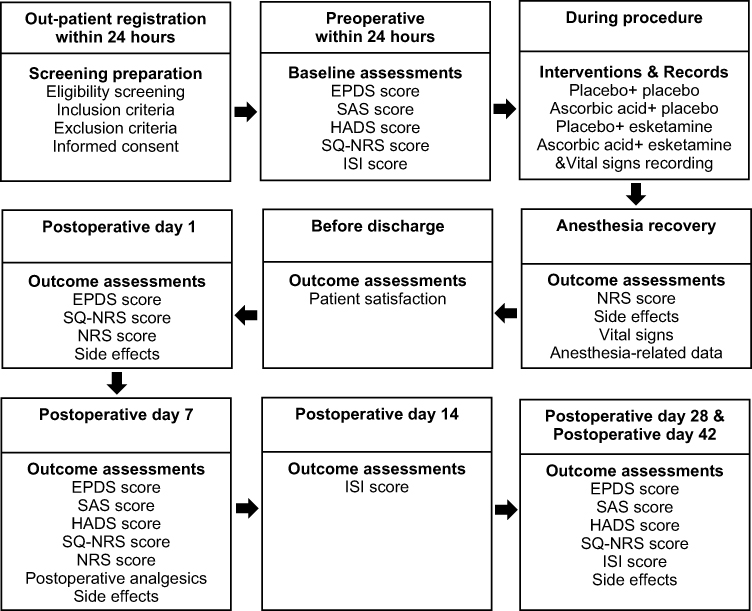 |
Figure 2 Overview of the timeline in this study. Abbreviations: EPDS, Edinburgh Postnatal Depression Scale; HADS, Hospital Anxiety and Depression Scale; ISI, Insomnia Severity Index; NRS, Numeric Rating Scale; SAS, Self-Rating Anxiety Scale; SQ-NRS, Sleep Quality Numerical Rating Scale. |
Primary Outcome
The primary outcome measure is the incidence of depression as assessed with the Edinburgh Postpartum Depression Scale (EPDS) score on the 7th day after procedures. Positive screening for depression is defined as a score of 10 or more in the EPDS, and the incidence of depression is calculated as a percentage (%) of the number of patients with EPDS score of 10 or more in the total participants.34 The EPDS is a self-report inventory and widely used screening tool for perinatal depression among pregnant and postpartum women with satisfactory sensitivity and specificity, which consists of 10 questions on how the participant has felt during the past seven days, with each item being scored from 0 to 3 and a total score being from 0 to 30, and higher scores indicate higher depressive levels.35,36
Secondary Outcomes
Secondary outcomes are as follows: the EPDS scale score to assess the severity of depressive symptoms (measured preoperatively, 1, 7, 28 and 42 days postoperatively); the Self-Rating Anxiety Scale (SAS) score to assess the anxiety status (measured preoperatively, 7, 28 and 42 days postoperatively); the Hospital Anxiety and Depression Scale (HADS) score to assess the depressive and anxiety status (measured preoperatively, 7, 28 and 42 days postoperatively); the Sleep Quality Numerical Rating Scale (SQ-NRS) score to assess the sleep quality (measured preoperatively, 1, 7, 28 and 42 days postoperatively); the Insomnia Severity Index (ISI) score to assess the condition of insomnia (measured preoperatively, 14, 28 and 42 days postoperatively); the Numeric Rating Scale (NRS) to assess the postoperative pain (measured after recovery from anesthesia, 1 and 7 days postoperatively); the medication of postoperative analgesics (measured on postoperative day 7); the side effects of esketamine, including hallucinations, headache, dizziness, nightmares, diplopia, blurred vision, nausea, vomiting, dramatic fluctuations in blood pressure and/or heart rate (increase of over 20% from the baseline), etc. (measured during anesthesia, 1, 7, 28, and 42 days postoperatively); the vital signs during perianesthetic period, including body temperature, respiration, heart rate, oxygen saturation, blood pressure, etc.; anesthesia-related data, including anesthesia duration, dosages of anesthetics (recorded at the end of recovery from anesthesia); and patient satisfaction (before discharge).
The SAS is commonly used for assessing anxiety, which includes psychological and somatic symptoms evaluation in a total of 20 items assessed with point scale ranging from 1 to 4. The index score is obtained from the raw score (from 20 to 80) multiplied by 1.25, converted to a decimal, and multiplied by 100. The cut-off score is the original score of 36 or the index score of 45 or more.37,38 The HADS consists of a total of 14 items, half of which are for depression and the rest for anxiety. HADS has good psychometric properties and has been used for evaluating depression and anxiety in women with miscarriage.2,39 The SQ-NRS uses numbers 0–10 to assess the subjective sleep quality (0 = best sleep and 10 = worst sleep): good sleep quality (0–3); moderate sleep quality (4–6); poor sleep quality (7–10), indicating that the individual is significantly dissatisfied with their sleep and may require further evaluation or intervention.40,41 The ISI is a 7-item scale for assessing the severity of insomnia symptoms, as well as the day mental anguish and dysfunction, with each item of 0–4 points and the total score of 0–28 points, and the higher the score, the more severe the insomnia.42,43 NRS uses numbers 0–10 to indicate the level of pain: no (0), mild (1–3), moderate (4–6), and severe (7–10); and it is one of the most commonly used measures for pain with good responsiveness and detectability.44,45 Patient satisfaction is evaluated with a questionnaire before discharge.
Safety Outcomes and Monitoring
Observations of adverse events of AA and/or esketamine are focused on. Participants are asked to inform the study staff about any adverse events (AEs), which are defined as any new unintended adverse medical event in the participants following the intervention(s). AEs are self-reported by the participants, assessed by a physician, and recorded in the medical record report. In the case of severe AEs, the study will be suspended to break the blind, required treatment will be administered to ensure the patients’ safety, and the events will be reported to the Institutional Review Board.
Sample Size Estimation
The primary outcome is the incidence of depression on postoperative day 7. The Power Analysis and Sample Size software (PASS, version 2021; NCSS Statistical Software, Kaysville, UT, USA) is used. The incidence of depression in the control group (Group A0K0) was 21.6% with Group A0K1 and Group A1K0 having similar incidences and there was 18.5% lower in Group A1K1. Assuming a test level of α = 0.05 (two-sided), a power of (1-β) = 0.9 and the allocation ratio of 1:1:1:1, the sample size of each group required is 95. Considering a dropout rate of 10%, the total sample size is 424 participants finally.
Statistical Analysis
Data will be acquired and analyzed in accordance with the intention-to-treat (ITT) principle. The statisticians performing data analysis are blinded to study grouping and interventions. SPSS for Windows (version 26, IBM Corp., USA) will be used. Data will be presented according to their statistical characteristics and distributions. After conducting a normality test on the data, continuous variables will be expressed as mean and standard deviation (with a normal distribution) or median (interquartile range, with an abnormal distribution) and analyzed with analysis of variance or nonparametric tests. Categorical variables will be expressed as counts and percentages and analyzed with the chi-square test or Fisher’s exact test. Statistical significance is set at a P value of less than 0.05 with a two-tailed test.
Dissemination
Results of the study can be shared by publishing in academic journals.
Discussion
Being more susceptible to depression and some other adverse mental states, women are even more vulnerable when experience pregnancy, miscarriage and curettage, and are at high risks of suffering from psychiatric disorders, comorbidities, and recurrence in the rest of their lives. Timely suppression in the early vulnerable period has the significance of preventing long-term recurrence. Recently, ketamine and its isomers have come to the fore as novel rapid antidepressants, exert good effects on the prevention of PPD, anxiety, and pain in parturients, and alleviate postoperative depressive symptoms and pain in women with miscarriage after curettage up to 42 days after procedure.10–14 However, the side effects associated with (es)ketamine reduce the tolerability and adherence of patients significantly. Development of the efficacy and/or safety of ketamine and its isomers are also being explored, including the modification of its own structure and synergistic improvement with external combinations with other drugs or therapies.
AA is a potential adjuvant agent, which has shown superior effects in previous preclinical studies with a synergistic effect on the efficacy of ketamine and possibly indirect reduction of side effects as well.25,26 AA is a neuromodulator, provides support and structure to neurons, and participates in many essential processes in the central nervous system.46 The antidepressant mechanism of AA includes improvement of neurogenesis and synaptic plasticity, antioxidant effects, regulations of monoaminergic, glutamatergic, and γ-aminobutyric acid (GABA) neurotransmitter systems, activating the mammalian target of rapamycin pathway and downstream synaptic proteins, regulation of NO-sGC-cGMP signaling pathway, etc.19,20,22,47–49 However, to the best of our knowledge, there has been no direct evidence of the effects of AA alone or combined ketamine from clinical trials. The results of this study may be the first to provide related randomized controlled trial-based clinical evidence in women with miscarriage undergoing curettage.
This study is a prospective factorial design clinical trial with measures including randomized group, control group, and blind design to guarantee the reliability of results. In this study, curettage is the treatment required for the condition of these participants, and general anesthesia and procedures of the curettage are implemented according to clinical routines. In this trial, a group of experienced senior surgeons and anesthesiologists are selected to ensure the comparability of factors during the procedures between groups and sufficient safety.
Being one of the interventions in this trial, esketamine has been approved for treating depression in nasal spray form since 2019.50 Subsequently, evidence has supported the effectiveness of its intravenous dosage form for prevention of PPD and associated psychosomatic dysfunctions.10,11 Based on the synergy of effect of AA and ketamine, the dose of esketamine selected is a subeffective dose for preventing PPD referring to previous studies. Esketamine is injected intravenously slowly after the administration of general anesthetics and analgesics. Reasonable and safe dosages, routes and methods of medication of esketamine can be guaranteed. Regarding the other intervention, AA in this study is used based on previous studies and reference from the manufacturer’s instructions, and its dose is selected and optimized for better efficacies within the safe range.23,24
We adopt a comprehensive evaluation in the measurements of outcomes. Considering the subjectivity of the self-rating scales, the three main neuropsychiatric outcomes are each assessed with two scales to indicate the overlapping main measures more accurately and the relevant states more comprehensively. Symptoms of depression are assessed with the EPDS and HADS, those of anxiety are assessed with the SAS and HADS, and sleep quality is assessed with ISI and SQ-NRS. The scales are the commonly used scales currently available for relevant assessments. With in-depth communication and detailed guidance to the participants to obtain their active cooperation, the credibility of the results can be ensured by minimizing the interference of confounding factors on the data. During the interventions and procedures, anesthesia-related data and the participants’ perianesthesia vital signs are recorded objectively.
The safety of this study is fully considered as well. The procedures and general anesthesia in curettage are current medical routines. The dose of esketamine is significantly lower than its conventional anesthetic dose with the risk of severe side effects being relatively low. AA is a well-known common vitamin. In this study, the dosage and route of AA administration were within the scope of the manufacturer’s instructions, and the enrollment of participants excludes those with high-risk factors for complications, hence the risk of adverse effects of AA is generally very low. Nevertheless, we still make detailed records and analyses of any possible adverse effect. If it occurs, the participants will be treated in time, and the study will be suspended to break the blindness, so as to ensure their safety.
In addition, AA has the advantages of being widely known, safe and convenient, inexpensive and easy to obtain with good public acceptance and patient medication compliance as well. AA may be considered as a putative candidate for assisting or even partially replacing esketamine to participate in rapid antidepressant treatment with better socioeconomic value.
This study also has some limitations. First, it is a single-center study, with the differences in countries, regions, or races with distinct economic and cultural backgrounds, the mental and psychological states of the subjects selected in this study might be regional, and the results might be biased. Second, mental status scales are assessed mainly subjectively, but we will try to reduce the associated interferences as possible. Third, dropouts may occur at longer-term follow-up later in this study, but we will try to enhance their cooperation through better communication.
Conclusion
In conclusion, by investigating the effects of AA for neuropsychiatric health after curettage for miscarriage in women, either alone or when combined with esketamine, if it is found that group A1K0 (vs A0K0) and/or group A1K1 (vs A0K1) have significant advantages in the assessments of EPDS, SAS, HADS, SQ-NRS, ISI, NRS, and/or side effects, etc., and/or AA interacts with the efficacies of esketamine, clinical evidence can be expected to be provided for supporting AA’s use in pharmacotherapy for optimizing related prevention and treatment strategies. Meanwhile, the possible superior efficacy and safety of AA combination over esketamine may also help to provide insights for modifying new rapid antidepressant therapies.
Abbreviations
AA, ascorbic acid; AE, adverse event; AMPAR, α-amino-3-hydroxy-5-methyl-4-isoxazole-propionic acid receptor; EPDS, Edinburgh Postnatal Depression Scale; GABA, γ-aminobutyric acid; HADS, Hospital Anxiety and Depression Scale; ISI, Insomnia Severity Index; NMDAR, N-methyl-D-aspartate receptor; NRS, Numeric Rating Scale; PPD, postpartum depression; SAS, Self-Rating Anxiety Scale; SQ-NRS, Sleep Quality Numerical Rating Scale.
Acknowledgments
This work was supported by the Natural Science Foundation of Chongqing, China (Grant No. CSTB2024NSCQ-MSX1252) and Chongqing Medical Scientific Research Project (Joint Project of Chongqing Health Commission and Science and Technology Bureau), China (Grant No. 2025MSXM116).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Quenby S, Gallos ID, Dhillon-Smith RK, et al. Miscarriage matters: the epidemiological, physical, psychological, and economic costs of early pregnancy loss. Lancet. 2021;397(10285):1658–1667. doi:10.1016/S0140-6736(21)00682-6
2. Farren J, Jalmbrant M, Falconieri N, et al. Posttraumatic stress, anxiety and depression following miscarriage and ectopic pregnancy: a multicenter, prospective, cohort study. Am J Obstet Gynecol. 2020;222(4):367.e361–367.e22.
3. Jacob L, Gerhard C, Kostev K, Kalder M. Association between induced abortion, spontaneous abortion, and infertility respectively and the risk of psychiatric disorders in 57,770 women followed in gynecological practices in Germany. J Affect Disord. 2019;251:107–113. doi:10.1016/j.jad.2019.03.060
4. Herbert D, Young K, Pietrusińska M, MacBeth A. The mental health impact of perinatal loss: a systematic review and meta-analysis. J Affect Disord. 2022;297:118–129. doi:10.1016/j.jad.2021.10.026
5. Prior M, Bagness C, Brewin J, et al. Priorities for research in miscarriage: a priority setting partnership between people affected by miscarriage and professionals following the James Lind Alliance methodology. BMJ Open. 2017;7(8):e016571. doi:10.1136/bmjopen-2017-016571
6. Yip E, Fleck D. The use of prophylactic ketamine to mitigate postoperative depressive symptoms: a systematic review. J Perianesth Nurs. 2024;S1089–9472(24)00210–7. doi:10.1016/j.jopan.2024.05.026
7. Guo J, Qiu D, Gu HW, et al. Efficacy and safety of perioperative application of ketamine on postoperative depression: a meta-analysis of randomized controlled studies. Mol Psychiatry. 2023;28(6):2266–2276. doi:10.1038/s41380-023-01945-z
8. Qiu D, Wang XM, Yang JJ, et al. Effect of intraoperative esketamine infusion on postoperative sleep disturbance after gynecological laparoscopy: a randomized clinical trial. JAMA Network Open. 2022;5(12):e2244514. doi:10.1001/jamanetworkopen.2022.44514
9. Zhou D, Liu F, Jiang F, Ye X, Gong X, Zhang M. Sub-anesthesia dose of S-ketamine reduces postoperative pain and anxiety in patients receiving breast and thyroid surgery: a randomized, controlled trial. Pain Physician. 2023;26(3):257–264. doi:10.36076/ppj.2023.26.257
10. Li S, Zhou W, Li P, Lin R. Effects of ketamine and esketamine on preventing postpartum depression after cesarean delivery: a meta-analysis. J Affect Disord. 2024;351:720–728. doi:10.1016/j.jad.2024.01.202
11. Wang S, Deng CM, Zeng Y, et al. Efficacy of a single low dose of esketamine after childbirth for mothers with symptoms of prenatal depression: randomised clinical trial. BMJ. 2024;385:e078218. doi:10.1136/bmj-2023-078218
12. Wang W, Ling B, Zhao H, et al. Effect of esketamine on postpartum depression after labor analgesia and potential mechanisms: a randomized, double-blinded controlled trial. BMC Anesthesiol. 2024;24(1):4. doi:10.1186/s12871-023-02377-6
13. Jiang M, Li Q, Mao M, et al. Evaluation of clinical effects of esketamine on depression in patients with missed miscarriage: a randomized, controlled, double-blind trial. J Affect Disord. 2023;329:525–530. doi:10.1016/j.jad.2023.02.127
14. Mostafa RH, Khamis AM, Saleh AN, et al. Acute effects of ketamine infusion on postoperative mood scores in patients undergoing dilation and curettage: a randomized double-Blind controlled study. Anesthesiol Res Pract. 2021;2021:6674658. doi:10.1155/2021/6674658
15. Short B, Fong J, Galvez V, Shelker W, Loo CK. Side-effects associated with ketamine use in depression: a systematic review. Lancet Psychiatry. 2018;5(1):65–78. doi:10.1016/S2215-0366(17)30272-9
16. Marwaha S, Palmer E, Suppes T, Cons E, Young AH, Upthegrove R. Novel and emerging treatments for major depression. Lancet. 2023;401(10371):141–153. doi:10.1016/S0140-6736(22)02080-3
17. Singh I, Morgan C, Curran V, Nutt D, Schlag A, McShane R. Ketamine treatment for depression: opportunities for clinical innovation and ethical foresight. Lancet Psychiatry. 2017;4(5):419–426. doi:10.1016/S2215-0366(17)30102-5
18. Zhao D, Long X, Wang J. Association of dietary vitamin C intake with depression in adults: a cross-sectional study of NHANES from 2005 to 2020. J Affect Disord. 2024;358:113–120. doi:10.1016/j.jad.2024.05.032
19. Moritz B, Schmitz AE, Rodrigues ALS, Dafre AL, Cunha MP. The role of vitamin C in stress-related disorders. J Nutr Biochem. 2020;85:108459. doi:10.1016/j.jnutbio.2020.108459
20. Moretti M, Budni J, Freitas AE, Rosa PB, Rodrigues AL. Antidepressant-like effect of ascorbic acid is associated with the modulation of mammalian target of rapamycin pathway. J Psychiatr Res. 2014;48(1):16–24. doi:10.1016/j.jpsychires.2013.10.014
21. Fraga DB, Olescowicz G, Moretti M, et al. Anxiolytic effects of ascorbic acid and ketamine in mice. J Psychiatr Res. 2018;100:16–23. doi:10.1016/j.jpsychires.2018.02.006
22. Fraga DB, Camargo A, Olescowicz G, et al. A single administration of ascorbic acid rapidly reverses depressive-like behavior and hippocampal synaptic dysfunction induced by corticosterone in mice. Chem Biol Interact. 2021;342:109476. doi:10.1016/j.cbi.2021.109476
23. Han G, Gan Y, Wang Q, Sun S, Kang P. Effect of perioperative single dose intravenous vitamin C on pain after total Hip arthroplasty. J Orthop Surg Res. 2024;19(1):712. doi:10.1186/s13018-024-05193-x
24. Amr M, El-Mogy A, Shams T, Vieira K, Lakhan SE. Efficacy of vitamin C as an adjunct to fluoxetine therapy in pediatric major depressive disorder: a randomized, double-blind, placebo-controlled pilot study. Nutr J. 2013;12:31. doi:10.1186/1475-2891-12-31
25. Moretti M, Werle I, da Rosa PB, et al. A single coadministration of subeffective doses of ascorbic acid and ketamine reverses the depressive-like behavior induced by chronic unpredictable stress in mice. Pharmacol Biochem Behav. 2019;187:172800. doi:10.1016/j.pbb.2019.172800
26. Elsa A, Ubandawaki S. Ketamine anaesthesia following premedication of rabbits with vitamin C. J Vet Sci. 2005;6(3):239–241.
27. Paternina-Die M, Martínez-García M, Martín de Blas D, et al. Women’s neuroplasticity during gestation, childbirth and postpartum. Nat Neurosci. 2024;27(2):319–327.
28. Brown KA, Gould TD. Targeting metaplasticity mechanisms to promote sustained antidepressant actions. mol Psychiatry. 2024;29(4):1114–1127.
29. Kim JW, Suzuki K, Kavalali ET, Monteggia LM. Bridging rapid and sustained antidepressant effects of ketamine. Trends mol Med. 2023;29(5):364–375. doi:10.1016/j.molmed.2023.02.003
30. Ren Z, Wang M, Aldhabi M, et al. Low-dose S-ketamine exerts antidepressant-like effects via enhanced hippocampal synaptic plasticity in postpartum depression rats. Neurobiol Stress. 2022;16:100422. doi:10.1016/j.ynstr.2021.100422
31. Krystal JH, Kaye AP, Jefferson S, et al. Ketamine and the neurobiology of depression: toward next-generation rapid-acting antidepressant treatments. Proc Natl Acad Sci U S A. 2023;120(49):e2305772120. doi:10.1073/pnas.2305772120
32. Khan Z, Hameed M, Khan FA. Current role of perioperative intravenous ketamine: a narrative review. Anesthesiol Perioperative Sci. 2023;1(4):36. doi:10.1007/s44254-023-00035-1
33. Fraga DB, Costa AP, Olescowicz G, et al. Ascorbic acid presents rapid behavioral and hippocampal synaptic plasticity effects. Prog Neuropsychopharmacol Biol Psychiatr. 2020;96:109757. doi:10.1016/j.pnpbp.2019.109757
34. Luo SC, Duan KM, Fang C, et al. Correlations between SIRT genetic polymorphisms and postpartum depressive symptoms in Chinese parturients who had undergone cesarean section. Neuropsychiatr Dis Treat. 2020;16:3225–3238. doi:10.2147/NDT.S278248
35. Levis B, Negeri Z, Sun Y, Benedetti A, Thombs BD. Accuracy of the Edinburgh postnatal depression scale (EPDS) for screening to detect major depression among pregnant and postpartum women: systematic review and meta-analysis of individual participant data. BMJ. 2020;371:m4022. doi:10.1136/bmj.m4022
36. Cao Y, Fu L, Zhang X, Xia L, Zhou R. The relationship between perioperative use of esketamine and postpartum depression risk: a systematic review and meta-analysis of randomized controlled trials. Neuropsychiatr Dis Treat. 2024;20:1041–1048. doi:10.2147/NDT.S451930
37. Dunstan DA, Scott N. Norms for Zung’s Self-rating Anxiety Scale. BMC Psychiatry. 2020;20(1):90. doi:10.1186/s12888-019-2427-6
38. Dunstan DA, Scott N, Todd AK. Screening for anxiety and depression: reassessing the utility of the Zung scales. BMC Psychiatry. 2017;17(1):329. doi:10.1186/s12888-017-1489-6
39. Thapar AK, Thapar A. Psychological sequelae of miscarriage: a controlled study using the general health questionnaire and the Hospital Anxiety and Depression Scale. Br J Gen Pract. 1992;42(356):94–96.
40. Zhang Y, Cui F, Ma JH, Wang DX. Mini-dose esketamine-dexmedetomidine combination to supplement analgesia for patients after scoliosis correction surgery: a double-blind randomised trial. Br J Anaesth. 2023;131(2):385–396. doi:10.1016/j.bja.2023.05.001
41. Martin S, Chandran A, Zografos L, Zlateva G. Evaluation of the impact of fibromyalgia on patients’ sleep and the content validity of two sleep scales. Health Qual Life Outcomes. 2009;7:64. doi:10.1186/1477-7525-7-64
42. Morin CM, Buysse DJ. Management of insomnia. N Engl J Med. 2024;391(3):247–258. doi:10.1056/NEJMcp2305655
43. Kyle SD, Siriwardena AN, Espie CA, et al. Clinical and cost-effectiveness of nurse-delivered sleep restriction therapy for insomnia in primary care (HABIT): a pragmatic, superiority, open-label, randomised controlled trial. Lancet. 2023;402(10406):975–987. doi:10.1016/S0140-6736(23)00683-9
44. Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. 2011;152(10):2399–2404. doi:10.1016/j.pain.2011.07.005
45. He S, Renne A, Argandykov D, Convissar D, Lee J. Comparison of an Emoji-Based visual analog scale with a numeric rating scale for pain assessment. JAMA. 2022;328(2):208–209. doi:10.1001/jama.2022.7489
46. Moretti M, Fraga DB, Rodrigues ALS. Ascorbic acid to manage psychiatric disorders. CNS Drugs. 2017;31(7):571–583. doi:10.1007/s40263-017-0446-8
47. Moretti M, Rodrigues ALS. Functional role of ascorbic acid in the central nervous system: a focus on neurogenic and synaptogenic processes. Nutr Neurosci. 2022;25(11):2431–2441. doi:10.1080/1028415X.2021.1956848
48. Maratha S, Sharma V, Walia V. Antidepressant like effect of ascorbic acid in mice: possible involvement of NO-sGC-cGMP signaling. Neurochem Res. 2022;47(4):967–978. doi:10.1007/s11064-021-03496-7
49. Rosa PB, Neis VB, Ribeiro CM, Moretti M, Rodrigues AL. Antidepressant-like effects of ascorbic acid and ketamine involve modulation of GABAA and GABAB receptors. Pharmacol Rep. 2016;68(5):996–1001. doi:10.1016/j.pharep.2016.05.010
50. Kim J, Farchione T, Potter A, Chen Q, Temple R. Esketamine for treatment-resistant depression - First FDA-approved antidepressant in a new class. N Engl J Med. 2019;381(1):1–4. doi:10.1056/NEJMp1903305
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.