")
Back to Journals » Journal of Pain Research » Volume 18
Assessing the Benefit of a Digital Pain Alert System in a Community Hospital
Authors Grosman-Rimon L , Jorgoni L, Casey J, Tory S, Kumbhare D , Solanki J, Collins BE, Wegier P
Received 5 July 2024
Accepted for publication 22 November 2024
Published 25 January 2025 Volume 2025:18 Pages 429—439
DOI https://doi.org/10.2147/JPR.S477670
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Liza Grosman-Rimon,1 Linda Jorgoni,1 Jane Casey,2 Susan Tory,1 Dinesh Kumbhare,3 Jhanvi Solanki,1 Barbara E Collins,1 Pete Wegier1,4
1Humber River Health, Research Institute, Toronto, Canada; 2Tampa General Hospital, Tampa, FL, USA; 3Department of Medicine, Division of Physical Medicine and Rehabilitation, University Health Network, Toronto, Canada; 4University of Toronto, Institute of Health Policy, Management and Evaluation University of Toronto, Toronto, Canada
Correspondence: Liza Grosman-Rimon, Humber River Health, 235 Wilson Ave, North York, Toronto, ON, M3M 0B2, Canada, Tel +1416-242-82109, Email [email protected]
Introduction: In the last decade, clinical alert systems were developed for clinical use, including patient deterioration and other urgent clinical situations. However, investigations focusing on digital pain alert systems to assess and manage pain on time in in-hospital patients are scarce. The objective of the study was to assess the implementation of digital pain alerts in the various departments of a community hospital.
Methods: Administrative data from the year 2020 to 2023 were collected. Only data from cases when pain alert was activated were included. Data included pain alert activation frequency, pain alert response duration (time from pain alert activation to alert stop when medication was administered), the department from which the pain alert was activated.
Results: There was a steady significant decrease in the mean pain alert response duration over time from 2020 to 2023. The department with the shortest pain alert response duration was the Department of Surgery, and Cardiology (252.76 ± 4.712). The longest time delay was in the ICU (463.27± 2.73 min) and at the Mental Health Department (440.59± 5.46 min) (p < 0.01). The pain alert response duration gradually decreased from 2020 to 2023, with decreases from the first year in all of the units/departments, except for the ICU. NPS scores at the start of the alert to 30 minutes after alert stop decreased significantly.
Conclusion: Management of pain improved over time across the hospital, and in most of the departments, suggesting that with experience, digital pain alert systems have the potential to improve pain management by providing timely pain intervention.
Keywords: digital pain alert, community hospital, pain management, command centre
Introduction
Pain is one of the chief complaints of hospital patients.1 Moreover, the prevalence of acute pain and acute-on-chronic pain is high in patients treated in the hospital.2–9 Inappropriate pain management of patients has negative consequences including increased length of stay and associated costs as well as decreased patient satisfaction and quality of life.6 Perioperative pain is also a major risk factor that can lead to the development of chronic pain, increased complications, increased morbidity and increased mortality.10–13 Across many hospital settings, pain is often under-assessed and therefore under-treated.2,6,14–16
In the last decade, clinical alert systems have developed for clinical use, including patient deterioration,17–19 sepsis detection,20–24 and other urgent clinical situations25. These automated digital alerting systems have leveraged predictive algorithms and machine learning to provide early warnings to clinical staff that action may need to be taken.20–23 Nevertheless, in-hospital alert systems for pain are not commonly used. Tools have developed to detect and assess pain via medical devices and wearable sensors.26–29 However, investigations focusing on digital pain alert systems to assess and manage pain on time in in-hospital patients are scarce. A digital pain alert system was implemented in Humber River Health (HRH) to decrease the time delay from pain alert activation to pain medication administration. This pain alert system was implemented as part of the command center—a centralized management system—supported by information technology and real-time data to assess and manage pain. The objective of the study was to assess the implementation of digital pain alerts in the various departments of a community hospital.
Methods
Study Design
A descriptive, retrospective study was conducted at Humber River Health (HRH), in Toronto, Ontario, Canada. HRH is a fully digital hospital and one of Canada’s largest community hospitals, based in the northwest Greater Toronto Area. As a digital hospital, HRH utilizes the most advanced digital healthcare technologies, which are integrated within many types of medical devices, communication tools, and other information systems. The study was approved by the Veritas Institutional Review Board (IRB) Inc., an independent ethics review board (IRB Number: 2024–3316-16,805-1). This retrospective study, using administrative data, was performed in accordance with ethical guidelines. Informed consent was waived by Veritas IRB Inc ethics review board since administrative data was used (https://www.veritasirb.com/index.html).
Command Centre’s and Risk of Harm Screen
The command centre at HRH supports the monitoring and coordination of many aspects of patient care and hospital operations (GE HealthCare Technologies, Inc. Chicago, Illinois, USA). At HRH, the command centre integrates with the hospital electronic medical record (EMR) (Meditech, Medical Information Technology, Inc. MA, USA) to present the latest information entered by the clinicians managing patient care, providing clinical information within 30 seconds to 2 minutes after entry. The Command Centre application is deployed as a web application delivering quality performance.
The infrastructure design of the Command centres support proactive operations management and best practices by team colocation (clinical decision team members are located in the same room with a global view), real-time data collection, predictive analytics, and clear protocols.30 The command centres were shown to improve the integration of multiple services into the day-to-day operation, communication and coordination, as well as the employment of prediction and an early warning system.31 It acts as a centralized hub where hospital staff from multiple clinical departments and support services are co-located with a set of 33 screens – LCD video screens displaying a wall of analytics (decision support applications within the Command Centre Software Platform). These display screens show analytic insights from a series of analytics in an easy-to-read format, enabling staff to quickly respond to and act on vital information. Large screens are located in both the inpatient units and command centre. The visual display of real-time data on these large screens provides clinicians with concurrent information, which is paired with defined protocols, and workflows, to support decision making.32 The data is continuously monitored 24-hours a day, seven days a week by Command Centre staff, including the Clinical Expeditor, a senior nurse that monitors the quality and safety-related alerts. The Risk of Harm screen displays alerts including pain, pressure injuries, falls, and delirium. The screen increases the visibility of key harm risks in real-time and alerts when risks are high or when mitigating actions are not taken, enabling prompt responses that reduce the likelihood of adverse events.
The Command Centre utilizes a software package deployed via a web-based application, designed to provide real-time insights into patient care and hospital workflow, in order to allow faster intervention and reduced risks. The Risk of Harm application alert occurs when the nurse documents patient’s pain on the electronic medical record and subsequent medication administration does not align with hospital protocols (in the case of pain alert, there is time delay from pain alert activation to pain medication administration). Frontline nurses hold primary responsibility for following hospital protocols, while unit-based charge nurses provide immediate oversight when the Command Centre application signals a deviation. If the issue persists, the Clinical Expeditor in the Command Centre intervenes to ensure compliance, either via direct mobile communication or in-person follow-up.
Clinical staff members were trained on all aspects of the alerts. Training includes 3 phases: familiarization in phase one, an education day in phase two, and reinforcement and validation in phase three (Table 1).
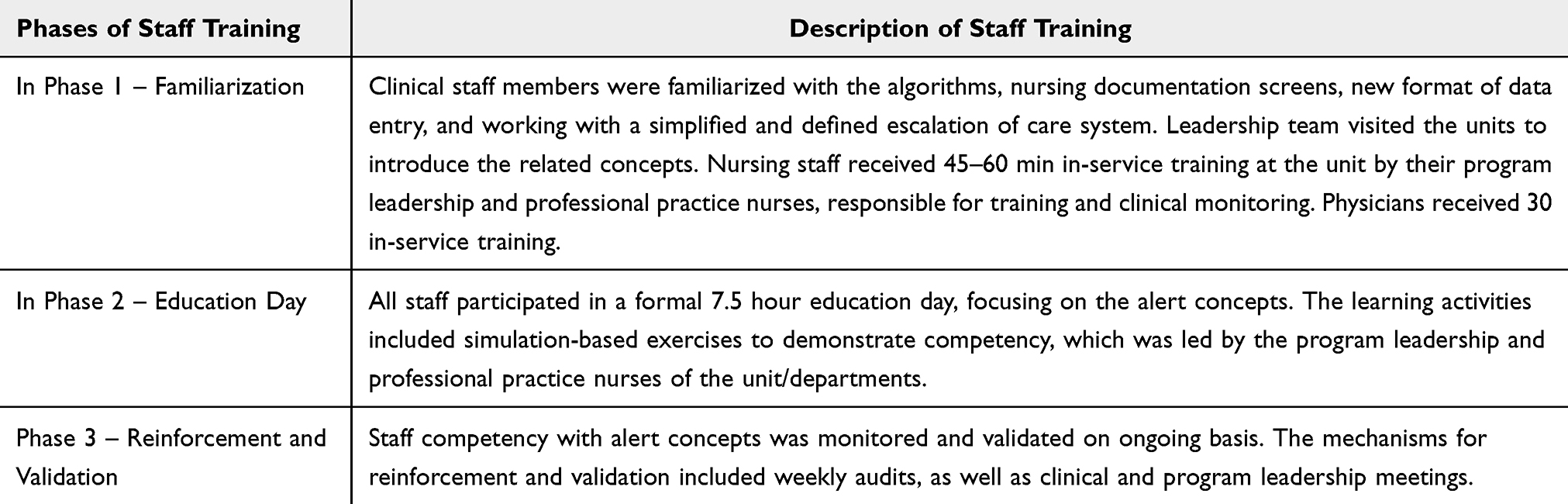 |
Table 1 Phases and Description of Staff Training |
Pain Alert System
A pain alert algorithm was implemented as part of the command centre operation. The pain alert was launched on Dec 18th 2019. The numeric pain scale (NPS) was used to assess pain, 11-point NPS ranges from 0 – representing no pain, to 10 – representing extreme pain. The bedside nurse inputted the NPS score after asking the patients to rate their pain on the NPS. Alerts are activated: (1) when the pain score is NPS ≥ 6 (pain exceeds the set threshold), and (2) when patient’s “pain goal is not met” (For example, if the patient set a goal of 3 on the NPS after a clinical procedure, and the pain score is 4, the alert is activated). For cases when the “pain goal is not met” patients can set the goal to any number on the NPS. The NPS scores were recorded when alert started and 30 minutes after the alert stopped. The alert stops when pain medications are administered or the “pain goal was met”. If no action has been taken within 1 hour of an alert being activated, the unit nurse lead follows up with the bedside nurse. If no action has been taken 2 hours after an alert is activated (“red alert”), a clinical expeditor in the Command Centre follows up with the bedside nurse. The clinical expeditor provides a summary of all red alerts from the previous 24 hours to clinical staff at morning bed meetings.
Data Collection
Administrative data from the year 2020 to 2023 were collected. Data included pain alert activation frequency, pain alert response duration (time from pain alert activation to alert stopping when medication was administered), and the department from which the pain alert was activated. Only data from cases when pain alert was activated were included. Data were collected from the Intensive Care Unit (ICU), the Surgery Departments, the Mental Health Department, Cardiology, Nephrology, Mental Health Department, Paediatrics Unit, Mother-Neonatal Units, and the Medicine Department. Data from patients unable to indicate their pain levels, including patients who are unconscious, somnolent, intubated, as well as neonates/infants were excluded.
Statistical Analysis
The IBM SPSS statistics software (IBM SPSS Statistics for Windows, Version 23.0. Armonk, NY: IBM Corp) was used for analysis. Descriptive statistics were performed, and the data were presented as mean±standard error (SE) or percentages as appropriate. One-way analysis of variance (ANOVA) was performed with Scheffe as a post Hoc test to assess the differences in the pain alert response duration in different units/departments and different years. Repeated measure ANOVA was performed to assess the differences between NPS scores when alert started and 30 minutes after the alert stopped from 2020 to 2023. The correlations between pain alert response duration and pain score difference (time from pain score at activation to score at alert stop) was assessed using the Spearman correlation coefficient. A p-value of <0.05 was considered significant.
Results
The total number of pain alerts activated between 2020 and 2023 was 33690, with 14701 in 2020, 8927 in 2021, 6974 in 2022, and 3088 in 2023 (Table 2).
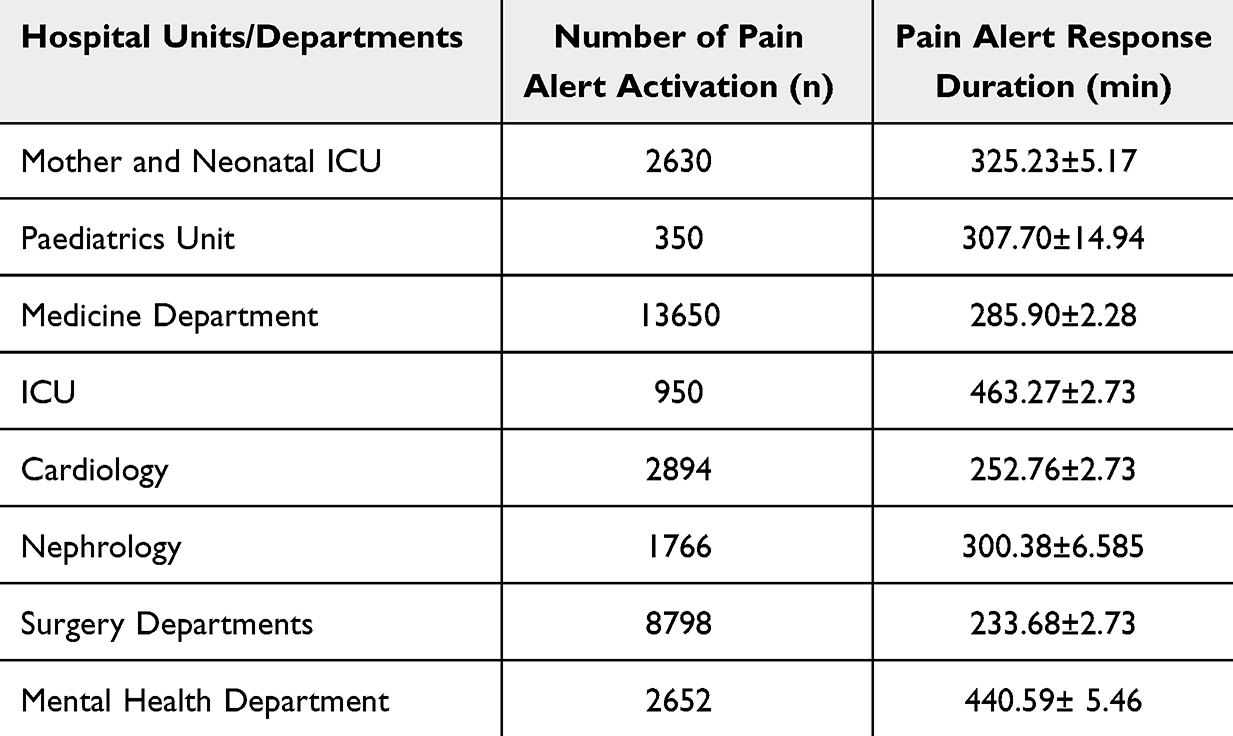 |
Table 2 The Time Delay From Alert Starts to Drop at Different Departments |
Pain Alert Response Duration
The mean pain alert response duration from 2020 to 2023 was 290.65±1.480 min. There was a steady and significant decrease in the mean pain alert response duration, with 352.54±2.35 min in 2020, 287.40±2.85 min in 2021, 219.27± 2.798 min in 2022, 166.64±3.52 min in 2023 (p<0.001), (Figure 1). From 2020 to 2023, the department with the shortest pain alert response duration was the Department of Surgery (233.68 ± 2.735), and the department of Cardiology (252.76 ± 4.712) (p < 0.01) (Figure 2). The longest pain alert response duration was in the ICU (463.27±2.73 min) and the Department of Mental Health (440.59± 5.46 min) (p < 0.01). The pain alert response duration gradually decreased from 2020 to 2023, with decreases from the first year in all of the units/departments, except for the ICU (Figure 3). Table 3 presents mean pain alert response duration for each department from 2020 to 2023.
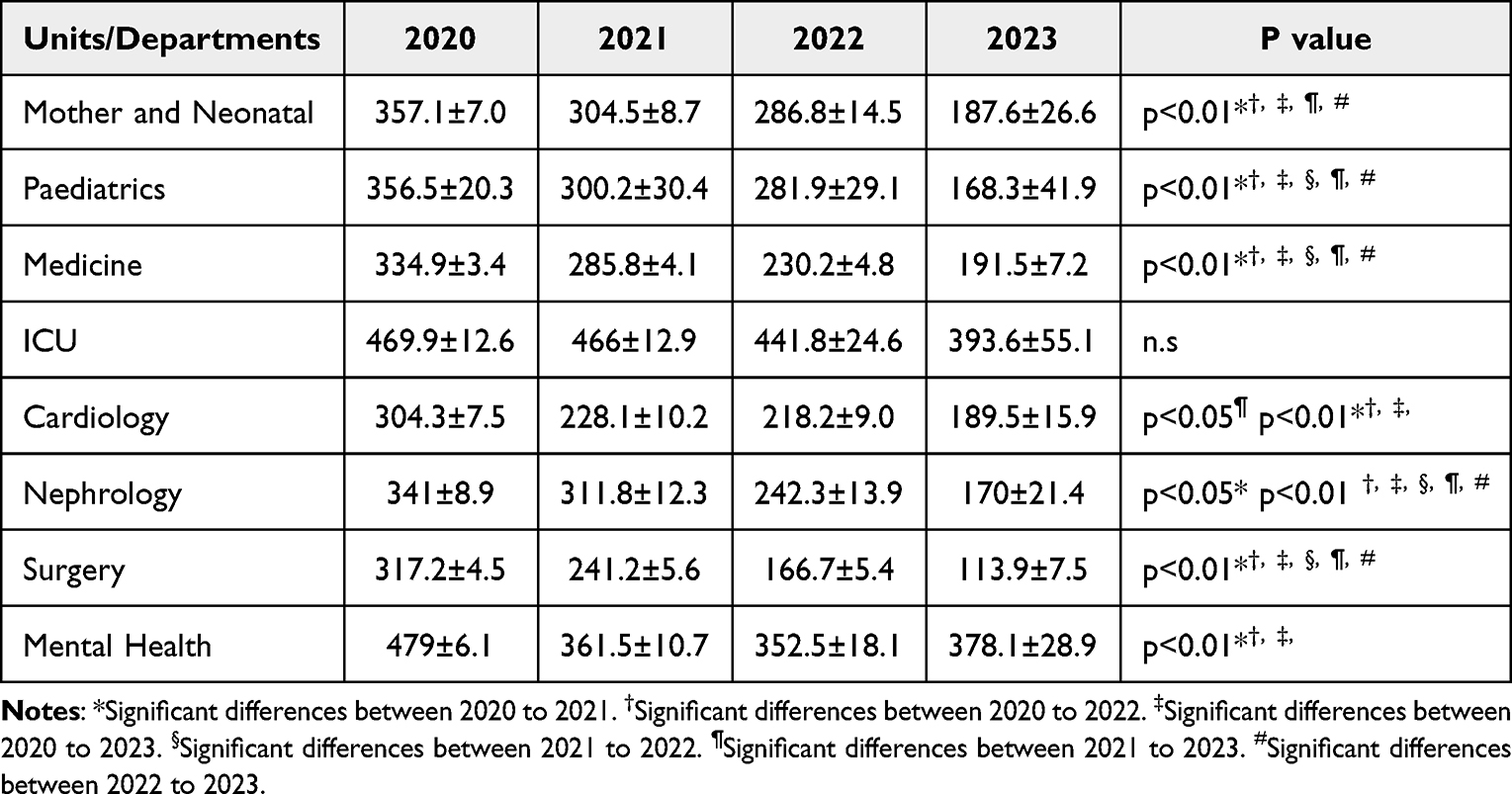 |
Table 3 Mean Pain Alert Response Duration for Different Unit/Department From 2020 to 2023 |
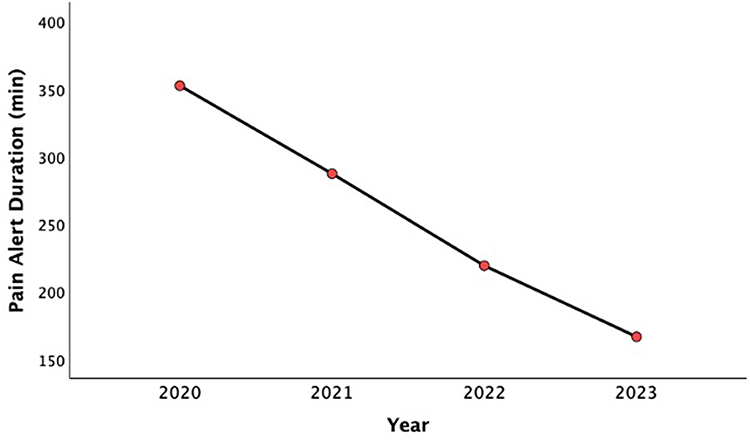 |
Figure 1 Mean pain alert response duration from 2020 to 2023. |
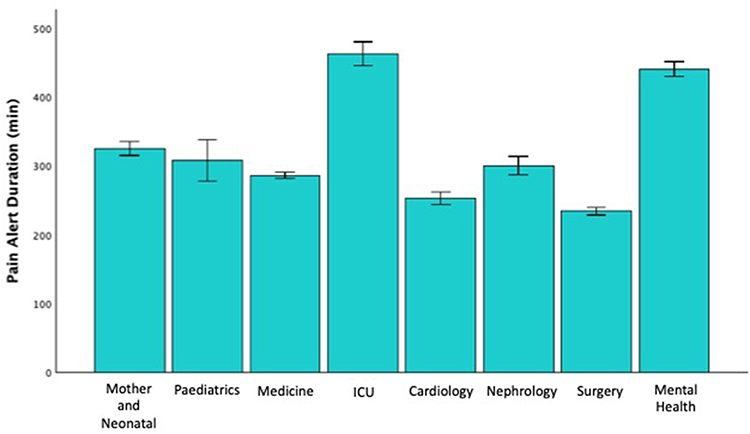 |
Figure 2 Pain alert response duration in different units/departments from 2020 to 2023. |
 |
Figure 3 Pain alert response duration from 2020 to 2023 in different units/departments. |
In a subgroup analysis, 50.6% of the cases were “pain exceeding the threshold”, and for 49.4% cases the “pain goal not met”. In the subgroup of cases with pain exceeding the threshold, the mean pain alert response duration was 131.8±2.7, while in the subgroup of cases with the “pain goal not met”, the mean duration was 447.0±2.1. In all units/departments, cases with pain exceeding the threshold subgroup, the mean pain alert response duration was shorter than the subgroup of cases with “pain goal not met”, with Mother-Neonatal Units 139.6±7.0 vs429.5±12.4 (p<0.01), Paediatrics 138.9±13.6 vs 543.3±69.8 (p<0.01), Medicine 149.0±1.8 vs 464.5±6.6, ICU 199.1±23.4 vs 502.7±22.0 p<0.01), Cardiology 141.8±4.1 vs 438.8±13.5 p<0.01), Nephrology 135.2± 5.2 vs 521.7±22.2, and Surgery 112.3±2.0 vs 512.8±13.4. In the Mental Health Department, an alert based on “pain goal not met” was not implemented (Figure 4).
 |
Figure 4 Pain alert response duration in the subgroups of cases with “pain exceeding the threshold” and cases with “pain goal not met” in different units/departments. |
NPS Scores at Alert Start and Stop
The mean NPS score at the start of the alert to 30 minutes after the alert stopped decreased significantly (3.9±0.02 vs 2.8±0.01, p<0.001).
In the subgroup of cases with pain exceeding the threshold, the mean NPS score from the years 2020 to 2023 significantly decreased from the alert start to 30 minutes after alert the stop (6.5±0.01 to 4.7±0.02, p<0.001). In the subgroup of cases with pain exceeding the threshold, NPS scores significantly decreased for alert start to alert stop in each year from 2020 to 2023 (Figure 5a, Table 4).
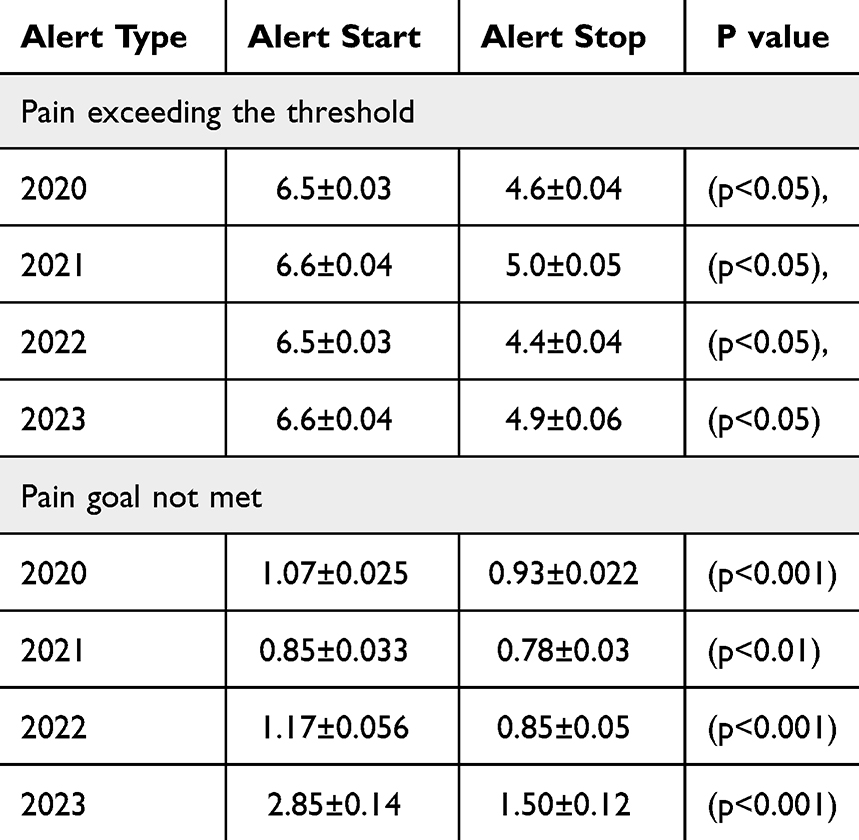 |
Table 4 Differences in NSP Scores at Alert Start to Alert Stop From 2020 to 2023 |
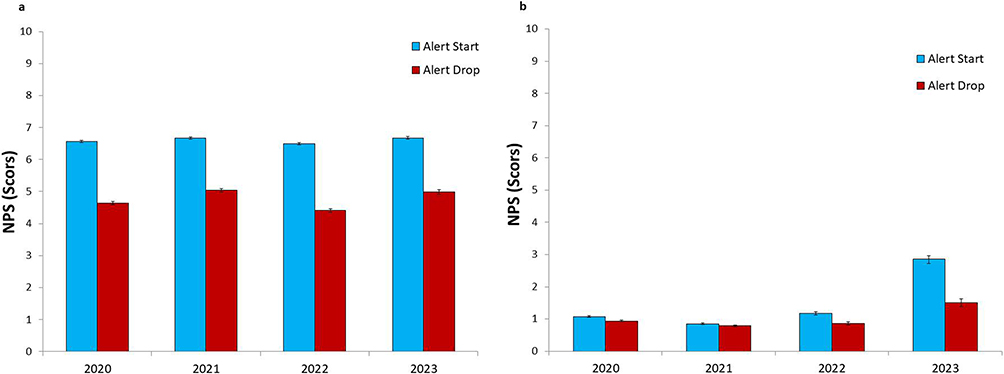 |
Figure 5 (a) NPS scores at pain alert start and after alert stop for subgroup of cases with “pain exceeding the threshold”. (b) NPS scores at pain alert start and after alert stop for subgroup of cases with “pain goal not met”. |
In the subgroup of cases with “pain goal not met”, the mean NPS score from the years 2020 to 2023 decreased from alert start to 30 minutes after alert stop (1.04±0.01 vs 0.89±0.01) (p<0.001). In the subgroup of cases with pain exceeding the threshold, NPS score significantly decreased for alert start to alert stop in each year from 2020 to 2023 (Figure 5b).
There was a significant moderate correlation between pain alert response duration and pain score difference (r=0.45, p<0.001).
Medications that were administered after pain alert activation included Acetaminophen, Acetaminophen/Codeine/Caffeine, Celecoxib, Codeine, Diclofenac, Diclofenac/Misoprostol, Fentanyl, Gabapentin, Hydromorphone, Ibuprofen, Indomethacin, Ketamine, Ketorolac, Meloxicam, Meperidine, Methadone, Morphine, Morphine HCL, Naproxen, Oxycodone, Oxycodone/Acetaminophen and Pregabalin.
Discussion
The major finding of the study was the steady and significant decrease in pain alert response duration as the years progressed, suggesting that there was an improvement with experience over time in addressing pain. There were differences between units/departments. Different factors may account for the variability in pain alert response-time in different units/departments, including differences in implementation strategies of the pain alert system, staff training, procedures, patient volume and flow, and clinical practices. Furthermore, despite the improvement in most units/departments, these factors may also be responsible for the delay in pain alert response time.
It is possible that in some departments pain management was a priority, while other departments have the opportunity to further address pain indicators.
During the design of the pain alert system, a pain level of “6” was chosen as a healthcare quality indicator based on patient feedback, a level requiring intervention. Many patients are complex cases requiring multimodal analgesia – the use of more than one pharmacological class of analgesic medication. While pain alerts below “6” are expected to be managed on the in-patient units at the bedside, the command centre’s alert system is a monitoring tool providing a centralized safety net, and triggering a dialogue for intervention or change in treatment plan when the score is 6 and above.
Alerts are activated in two cases: when pain exceeds the set threshold (NPS ≥ 6), and when the patient’s “pain goal is not met”. In this study, only cases when the pain alert was activated were included. We presume that in cases when the alert was not activated, treatment of pain was timely. For cases where the pain alert was activated, the delay in pain management could be due to a shortage of staff, a large volume of patients, suboptimal workflow, staff turnover (new staff are not fully trained). This delay could be investigated in future studies to optimize the management of pain.
In addition, the pain alert response duration was much shorter in the subgroup of cases with pain exceeding the threshold compared to the subgroup of cases with “pain goal not met”. Moreover, in the subgroup of cases with “pain goal not met”, the alert started at low pain levels when alert started, while in the subgroup of cases with pain exceeding the threshold, the pain levels were much higher when alert started. Patients set their pain goal at every staff shift and it is possible that the clinical staff deemed that the pain levels require more urgent response in the subgroup of patients with pain exceeding the threshold, while in the subgroup of patients with “pain goal not met” the pain level goal was set to low levels, which may consider by the clinical staff not necessitating urgent response and immediate intervention. In both cases, further improvement in time responses is warranted to achieve optimal management of pain.
Another interesting finding is that the number of pain alerts activated between 2020 and 2023 decreased. It is possible that with the implementation of the pain alert system, staff awareness of pain management improved. Nevertheless, even though the number of pain alerts activation decreased over the years, in the cases when the pain alert was activated, management of pain can be further improved by ideally shortening the time of alert activation to pain medication administration by even a few minutes.
In our hospital, the digital pain alert system was implemented to decrease the time from pain alert activation to pain medication administration. The aim was to decrease the time delay from pain alert identification and activation to pain medication administration, in order to address pain early within a hospital setting. In the last few decades, most research has focused on pain detection and assessments using technological innovation, but the majority of studies did not assess tools to address pain after the assessment. Sensors and algorithms have developed to detect and assess pain using medical devices and wearable sensors.26 A systematic review presented several wearable electronic devices such as wristbands, smartwatches, and belts for assessment of chronic pain intensity, reflecting physiologic or biometric parameters, including psychomotor and sleep patterns, space and time mobility, heart rate variability, and skeletal muscle electrical activity.27 Wearable electronic devices can reliably reflect physiologic or biometric parameters correlated with pain. A previous investigation showed that a smartphone-based system developed for real-time pain measurement using a wrist-worn electrodermal activity sensor was able to accurately detect pain28 Similarly in a recent study, algorithms were developed for the detection of pain in real-time, using a physiological dataset associated with acute pain induction in healthy adults. Study participants were exposed to acute pain while being monitored using electrocardiography for the measurements of a series of respiratory and heart rate variability features.29 These technological alert system algorithms have the potential to automatically detect pain in both a controlled environment and the real world. However, in these studies, pain was not addressed and managed.
In addition, currently medical devices and wearable sensors that monitor physiological parameters to assess pain are not part of the pain alert systems. Future studies should incorporate medical devices and wearable sensors within pain alert systems, and assess the effectiveness of pain management and the effect on pain levels. Incorporating medical devices and wearable sensors that detect pain levels using physiological parameters within the pain alert system in the future can benefit patients especially those who are unconscious, somnolent, and intubated.
In recent years, clinical alert systems have been developed for many clinical settings, including hospitals, for the management of urgent and high-risk situations that require expeditious interventions. These include the identification of deteriorating patients,17–19 sepsis20–24 and other severe events.25 These automated digital alerting systems have been used to provide early warning, increase staff awareness, and improve patient management.20–23 Since inappropriate management of pain has severe negative consequences to the health outcomes10–13 and quality of life of patients,6 it is important to address pain early and provide timely intervention.
In this study, we observed a significant decrease in the pain scores from the pain alert start to 30 minutes after the pain alert stopped. Nevertheless, the average pain levels remain moderate. Future studies should investigate additional strategies to improve pain management, including improving organizational culture, staff education and training.
The major limitation of the study is that it is a single centre and observational study. Furthermore, although our findings suggest that the implementation of a digital pain alert system improves pain management; it is possible that the improvement in pain alert response duration is due to improvement in medical care over time. This study was a descriptive study that did not follow up with patients and assess patient-reported outcomes. In addition, in most units/departments the pain alert response duration gradually decreased over time. However, we cannot generalize the findings to all clinical settings. Further research is warranted to assess the effect of digital pain alert in different clinical settings and medical institutions. Longitudinal studies should assess additional variables such as patients’ satisfaction. Reassessments of pain scores were completed 30 minutes after administration of pain medication, which was part of our hospital clinical protocol. In many hospital settings, pain is reassessed between 30 and 60 minutes after medication administration. In this study, we did not assess pain based on the medication’s onset of action, peak effectiveness, and the duration of the medication that produces the effect. Future studies may thoroughly investigate the effects of the alert system on pain levels based on the specific medication and their effects.
The lag between the time the nurse enters the pain and the administration of analgesia is often attributed to obtaining an order and dispensing the medication. In more complex cases requiring multimodal analgesia, the nurse may consult with other members of the clinical team. In addition, there are many reasons for the delay in response time, including factors that may be related to the shortage of staff, heavy workload, suboptimal protocols and workflow, and/or misuse of resources. These factors were beyond the scope of the current study. The Command Centre has the potential to mitigate some of these factors to some extent; nevertheless, these factors can affect the management of pain and should be addressed in future.
The Effects of the Pain Alert Operation on These Factors Should Also Be Assessed in Future Studies
Future studies should assess new technologies in conjunction with a digital pain alert system, such as sensors and algorithms that can detect and assess pain in real-time using medical devices and wearable sensors, which can improve much further pain management. In our study, patients who were unconscious, somnolent, intubated, as well as neonates/infants were excluded since they were unable to indicate their pain levels. New technology and algorithms for the detection of pain using physiological parameters may be useful in these patient populations.
The pain alert system’s role is limited to providing alarms and promptly recognizing warning signs from patients’ pain levels. It is important to note that although the system alerts for the need to address pain, medication administration to the patient was based on the judgment of the clinical staff.
Conclusion
Pain alert systems are not widely used in the clinical setting, especially in hospitals, where many patients suffer from pain.2–9 In this study, we temporally assessed a digital pain alerting system in different departments across a community hospital. We observed a decrease in both the mean pain alert response duration in most of the departments, and the total number of pain alerts activated over the years. Despite that, the management of pain can be further improved, especially in cases where the “pain goal was not met”.
It is important to emphasize that the digital pain alert system, which has the potential to improve pain management, can be implemented along with strategies for improved organizational culture, staff education and training. More research is needed to confirm the findings and determine whether other digital pain alert systems affect the response time for pain alerts and other patient outcomes.
Disclosure
The authors LGR, LJ, JC, ST, DK, JS, BEC, and PW have no competing interests to disclose.
References
1. Lin RJ, Reid MC, Liu LL, Chused AE, Evans AT. The barriers to high-quality inpatient pain management: a qualitative study. Am J Hospice Palliative Care. 2015;32(6):594–599. doi:10.1177/1049909114530491
2. Gianni W, Madaio RA, Di Cioccio L, et al. Prevalence of pain in elderly hospitalized patients. Arch Gerontol Geriatrics. 2010;51(3):273–276. doi:10.1016/j.archger.2009.11.016
3. Melotti RM, Samolsky-Dekel BG, Ricchi E, et al. Pain prevalence and predictors among inpatients in a major Italian teaching hospital. A baseline survey towards a pain free hospital. European J Pain. 2005;9(5):485–495. doi:10.1016/j.ejpain.2004.09.010
4. Strohbuecker B, Mayer H, Evers GC, Sabatowski R. Pain prevalence in hospitalized patients in a German university teaching hospital. J Pain Sympt Manage. 2005;29(5):498–506. doi:10.1016/j.jpainsymman.2004.08.012
5. Fortner BV, Demarco G, Irving G, et al. Description and predictors of direct and indirect costs of pain reported by cancer patients. J Pain Sympt Manage. 2003;25(1):9–18. doi:10.1016/S0885-3924(02)00597-3
6. Whelan CT, Jin L, Meltzer D. Pain and satisfaction with pain control in hospitalized medical patients: no such thing as low risk. Arch Intern Med. 2004;164(2):175–180. doi:10.1001/archinte.164.2.175
7. Bjørnnes AK, Rustøen T, Lie I, Watt-Watson J, Leegaard M. Pain characteristics and analgesic intake before and following cardiac surgery. European J Cardiovasc Nursing. 2016;15(1):47–54. doi:10.1177/1474515114550441
8. Gohari J, Grosman-Rimon L, Arazi M, et al. Clinical factors and pre-surgical depression scores predict pain intensity in cardiac surgery patients. BMC Anesthesiol. 2022;22(1):204. doi:10.1186/s12871-022-01740-3
9. Sinderovsky A, Grosman-Rimon L, Atrash M, et al. The effects of preoperative pain education on pain severity in cardiac surgery patients: a pilot randomized control trial. Pain Manag Nursing. 2023;24(4):e18–e25. doi:10.1016/j.pmn.2023.02.003
10. Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet. 2006;367(9522):1618–1625. doi:10.1016/S0140-6736(06)68700-X
11. Katz J, Seltzer Z. Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurotherapeutics. 2009;9(5):723–744. doi:10.1586/ern.09.20
12. Rodgers A, Walker N, Schug S, et al. Reduction of postoperative mortality and morbidity with epidural or spinal anaesthesia: results from overview of randomised trials. BMJ. 2000;321(7275):1493. doi:10.1136/bmj.321.7275.1493
13. Wu CL, Raja SN. Treatment of acute postoperative pain. Lancet. 2011;377(9784):2215–2225. doi:10.1016/S0140-6736(11)60245-6
14. Cascinu S, Giordani P, Agostinelli R, et al. Pain and its treatment in hospitalized patients with metastatic cancer. Supportive Care Cancer. 2003;11(9):587–592. doi:10.1007/s00520-003-0491-3
15. Marks RM, Sachar EJ. Undertreatment of medical inpatients with narcotic analgesics. Ann Intern Med. 1973;78(2):173–181. doi:10.7326/0003-4819-78-2-173
16. Conway Morris A, Howie N. Pain in medical inpatients: an under-recognised problem? J Royal College Phys Edinburgh. 2009;39(4):292–295. doi:10.4997/JRCPE.2009.401
17. Tarassenko L, Hann A, Young D. Integrated monitoring and analysis for early warning of patient deterioration. Br J Anaesth. 2006;97(1):64–68. doi:10.1093/bja/ael113
18. Bailey TC, Chen Y, Mao Y, et al. A trial of a real-time alert for clinical deterioration in patients hospitalized on general medical wards. J Hospital Med. 2013;8(5):236–242. doi:10.1002/jhm.2009
19. Escobar GJ, Liu VX, Schuler A, Lawson B, Greene JD, Kipnis P. Automated identification of adults at risk for in-hospital clinical deterioration. N Engl J Med. 2020;383(20):1951–1960. doi:10.1056/NEJMsa2001090
20. Zhang Z, Chen L, Xu P, et al. Effectiveness of automated alerting system compared to usual care for the management of sepsis. NPJ Digital Med. 2022;5(1):101. doi:10.1038/s41746-022-00650-5
21. Joshi M, Ashrafian H, Arora S, Khan S, Cooke G, Darzi A. Digital alerting and outcomes in patients with sepsis: systematic review and meta-analysis. J Med Internet Res. 2019;21(12):e15166. doi:10.2196/15166
22. Sawyer AM, Deal EN, Labelle AJ, et al. Implementation of a real-time computerized sepsis alert in nonintensive care unit patients. Crit Care Med. 2011;39(3):469–473. doi:10.1097/CCM.0b013e318205df85
23. Umscheid CA, Betesh J, VanZandbergen C, et al. Development, implementation, and impact of an automated early warning and response system for sepsis. J Hospital Med. 2015;10(1):26–31. doi:10.1002/jhm.2259
24. Grosman-Rimon L, Rivlin L, Spataro R, et al. Trend of mortality and length of stay in the emergency department following implementation of a centralized sepsis alert system. Digital Health. 2024;10:20552076241250255. doi:10.1177/20552076241250255
25. Cook DA, Enders F, Caraballo PJ, Nishimura RA, Lloyd FJ. An automated clinical alert system for newly-diagnosed atrial fibrillation. PLoS One. 2015;10(4):e0122153. doi:10.1371/journal.pone.0122153
26. Chen J, Abbod M, Shieh JS. Pain and stress detection using wearable sensors and devices-a review. Sensors. 2021;21(4):1030.
27. Avila FR, McLeod CJ, Huayllani MT, et al. Wearable electronic devices for chronic pain intensity assessment: a systematic review. Pain Pract. 2021;21(8):955–965. doi:10.1111/papr.13047
28. Kong Y, Posada-Quintero HF, Chon KH. Real-time high-level acute pain detection using a smartphone and a wrist-worn electrodermal activity sensor. Sensors. 2021;21(12):3956. doi:10.3390/s21123956
29. Winslow BD, Kwasinski R, Whirlow K, Mills E, Hullfish J, Carroll M. Automatic detection of pain using machine learning. Front Pain Res. 2022;3:1044518. doi:10.3389/fpain.2022.1044518
30. Kane EM, Scheulen JJ, Püttgen A, et al. Use of systems engineering to design a hospital command center. Jt Comm J Qual Patient Saf. 2019;45(5):370–379. doi:10.1016/j.jcjq.2018.11.006
31. Grosman-Rimon L, Li DHY, Collins BE, Wegier P. Can we improve healthcare with centralized management systems, supported by information technology, predictive analytics, and real-time data?: a review. Medicine. 2023;102(45):e35769. doi:10.1097/MD.0000000000035769
32. Collins BE. Use of high-reliability principles in the evolution of a hospital command centre. Healthcare Quarterly. 2021;23(4):46–52. doi:10.12927/hcq.2020.26393
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.