")
Back to Journals » Infection and Drug Resistance » Volume 18
Assessment Framework for Infection Prevention and Control Competence in Trained Nurses in Regional Medical Communities: Development and Implementation
Authors Min QF, Gong XW, Qi ZP, Yang JS
Received 2 December 2024
Accepted for publication 21 April 2025
Published 14 May 2025 Volume 2025:18 Pages 2537—2546
DOI https://doi.org/10.2147/IDR.S508535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Qi-Fen Min, Xiao-Wen Gong, Zhi-Ping Qi, Jian-Shui Yang
Department of Infection Management, Changzhou Cancer Hospital, Changzhou, Jiangsu Province, 213032, People’s Republic of China
Correspondence: Jian-Shui Yang, Department of Infection Management, Changzhou Cancer Hospital, No. 68 of Red River Road, Xinqiao District, Changzhou, Jiangsu Province, 213032, People’s Republic of China, Tel +8618861452356, Fax +860519-69807240, Email [email protected]
Objective: To develop an assessment Framework for improving the competence of professional nurses in infection prevention and control within a regional medical community, and to evaluate the effectiveness of this system.
Methods: Analytic Hierarchy Process (AHP) was used to determine the weights of each index. An evaluation index system was established with 3 primary indexes, 9 secondary indexes, and 28 tertiary indexes, based on expert input and guidelines. The assessment framework for infection prevention competence was then implemented in 20 professional nurses from the regional medical community, who received standardized training from January 2018 to December 2023.
Results: The cumulative weights assigned to the primary indexes were 0.463, 0.317, and 0.220. For the secondary indexes, weights ranged from 0.025 to 0.293, and for the tertiary indexes, weights ranged from 0.003 to 0.100. After standardized training, the total competence score in infection prevention and control of nurses significantly increased from 79.50 to 89.75 (P < 0.001). The number of nurses with a bachelor degree increased from 7 to 20 (P < 0.001), and those with intermediate or higher professional titles rose from 7 to 20 (P = 0.010). The number of nurses holding provincial and municipal IPC certificates also significantly increased.
Conclusion: The study successfully developed a scientifically robust evaluation system for the competence in infection prevention and control among professional nurses. Standardized training significantly enhanced nurses’ capabilities, highlighting the importance of tailored training programs and continuous improvement of evaluation systems to meet evolving requirements.
Keywords: competency of infection prevention and control, evaluation system, hierarchical analysis, homogenized training, professional nurses in medical communities
Introduction
Hospital infection management is a critical component of healthcare quality and patient safety, particularly in primary healthcare institutions. However, China faces several challenges in the status and competence evaluation of hospital infection management personnel. Hospital infection management personnel in primary healthcare institutions are predominantly nurses, resulting in a uniform professional structure that lacks experts in clinical medicine, public health, and microbiology.1 This structure often leads to limited capacity and expertise for comprehensive hospital infection management. For example, a study in Zhejiang province found that many primary healthcare institutions lacked basic training materials and knowledge regarding sterile item procurement and waste management.1 Additionally, resource constraints in primary healthcare institutions affect their ability to implement effective infection control measures, including the absence of dedicated hospital infection management organizations and standardized practices for sterilization and waste management.2
To address these challenges, structured evaluation systems have been proposed. The World Health Organization (WHO) ‘s Infection Prevention and Control Assessment Framework (IPCAF) includes eight core components, such as Infection Prevention and Control (IPC) education and training, nosocomial infection surveillance, and implementation of multimodal strategies.2 This framework helps identify strengths and weaknesses in IPC resources and practices. Hierarchical analysis is also used to simplify complex issues by breaking them down into multiple tiers and computing cumulative weights based on the relative significance of indicators.3 This method helps prioritize key areas like hand hygiene compliance and sterilization practices. However, due to the lack of theoretical foundation, practical capacity and financial resources, IPCAF is not fully applicable to primary health care institutions4–6. The WHO has set forth new requirements for professional nurses in hospital infection prevention and control, encompassing aspects such as scientific research and management.7 Therefore, it is necessary to develop a scientific and comprehensive evaluation framework to guide the infection prevention and control training and practice of nurses in community hospitals.
Analytic Hierarchy Process (AHP), developed by Saaty, is a powerful multicriteria decision-making tool that has been used in numerous applications in various fields of economics, politics and engineering.8 The analysis has several advantages in establishing evaluation systems, including strong systematicity, clear logic, integration of qualitative and quantitative analysis, scientific weight allocation, intuitive comparison of multiple alternatives, and strong capacity for dynamic adjustment. These features make it particularly suitable for fields such as hospital infection management and medical quality evaluation, where it can provide scientific and effective solutions for complex decision-making problems.9,10 This judgment and decision-making way on intricate issues could be applied in the development of the evaluation system for the competence in infection prevention and control.
Therefore, we aimed to develop an assessment framework for improving the competence of professional nurses in infection prevention and control within a regional medical community, and to evaluate the effectiveness of this system in the actual clinical work environment.
Materials and Methods
Participants
Based on the AHP method, 8 experts in the field of infection prevention and control helped to establish the evaluation framework system of this study by independent evaluation of WHO system indicators. From January 2018 to December 2023, 20 IPC nurses in the community hospital were included in the study and trained according to this evaluation framework system. We compared the improvement in infection prevention and control indicators of participants before and after training.
The Establishment and Content of the Evaluation Framework System
With input from 8 authorized experts in the municipal hospital infection quality control center, each with credentials issued by the provincial training course and over six years of experience in infection prevention and control management, a set of well-structured and comprehensive index guidelines were developed for supporting professional nurses in infection prevention and control. These guidelines were developed based on the WHO’s IPC evaluation system and Guidelines for Training Professionals in Hospital Infection Management (WS/T525-2016).11 The evaluation index system for infection prevention and control competence among nursing staff was established and the formulated rules encompassed 3 primary indexes, 9 secondary indexes, and 28 tertiary indexes (Table 1).12 Key components of this framework included establishing a quality control organization for hospital infection management, delineating clear roles and responsibilities, enhancing the training and supervision system, and creating a collaborative network for open information exchange, communication channels, resource sharing, and talent exchange.
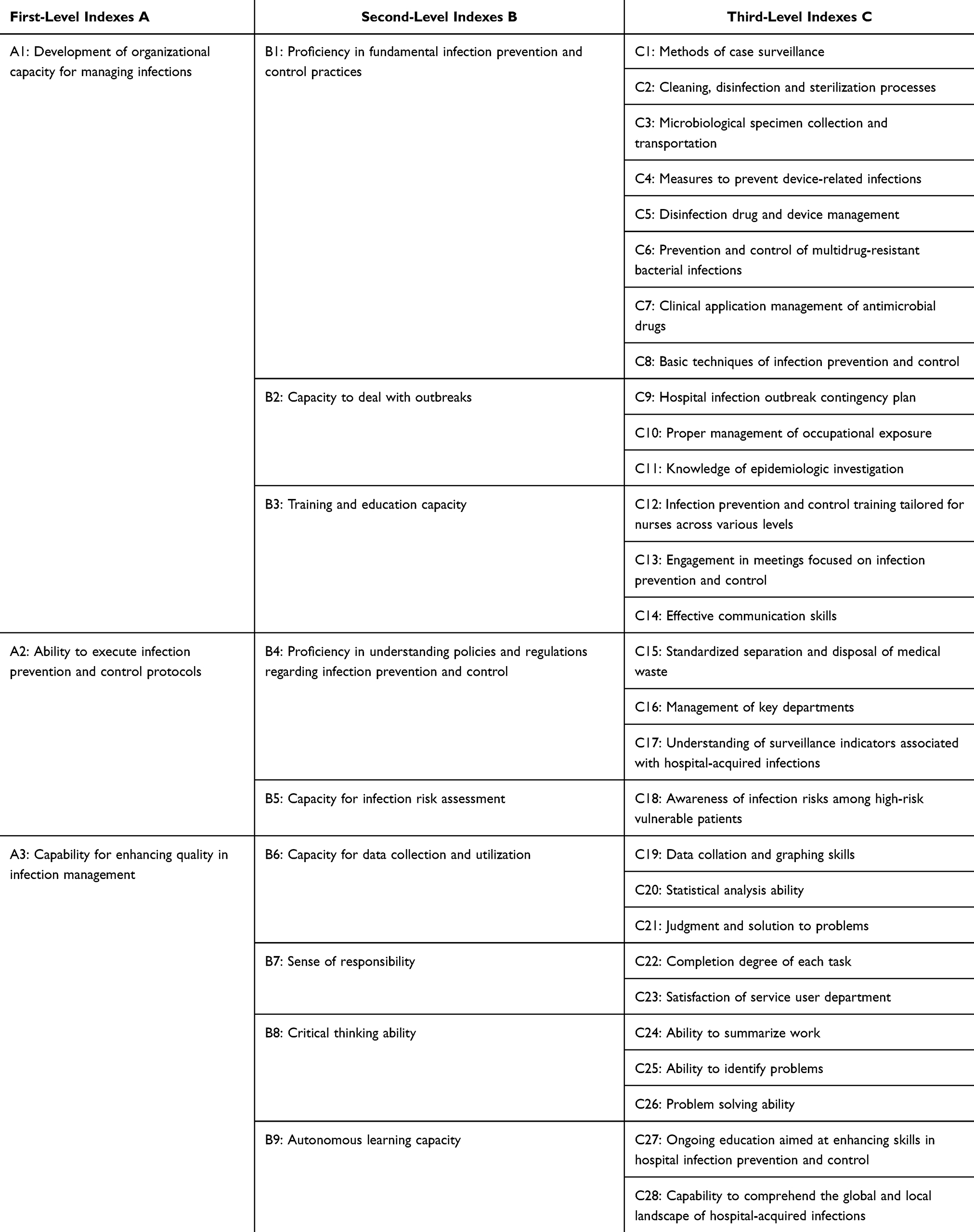 |
Table 1 Assessment Framework with Three-Tiered Indexes for Professional Nurses in Hospital Infection Prevention and Control |
Determination of the Weights of Evaluation Indexes
For each index tier, we aggregated the average scores given by the eight experts in infection prevention and control to assess their relative importance. Hierarchical analysis was utilized to determine the weights assigned to each evaluation index. In this context, “aij” represented the assigned importance value of the ith index relative to the jth index, while “aji” denoted the assigned importance value of the jth index relative to the ith index. The value “aii” indicated the comparison of the ith index with itself. The method of assigning relative importance is outlined in detail in Table 2. According to mathematical principles, “aii = 1” and “aij * aji = 1.” By utilizing the mean scores allotted by the experts to determine relative importance, a judgment matrix was constructed and subjected to consistency testing to compute the weight of each index.
 |
Table 2 Relative Importance Assignment Scale |
Training Method and Data Collection
20 IPC nurses in community hospitals received unified training. The training covers organizational capacity for managing infections, Ability to execute infection prevention and control protocols and capability for enhancing quality in infection Three aspects of management to ensure that all participants receive the same training and assessment. Data of participants before and after the training were obtained through interviews and questionnaires.
Statistical Analysis
We utilized Excel 2010 to aggregate and organize the data, while statistical analysis was conducted using SPSS 23.0 software. Quantitative data were presented as mean ± standard deviation, and intergroup comparisons were performed using the t-test. Count data were expressed as the number of cases and percentages, with intergroup comparisons conducted using Fisher’s exact probability method. A significance level of P ≤ 0.05 was deemed statistically significant. Weight calculations were performed using the weighting method in hierarchical analysis, with a consistent ratio (C.R). < 0.10 indicating that the judgment matrix successfully passed the consistency test.
Results
Display of AHP Index
A judgment matrix was formed for the three primary-level indexes, yielding a C.R. of 0.001. The cumulative weights assigned to ‘Development of organizational capacity for managing infections’, ‘Ability to execute infection prevention and control protocols’, ‘Capability for enhancing quality in infetion management’ were 0.463, 0.317, and 0.220, respectively (Table 3).
 |
Table 3 Assigning Weights to the Primary-Level Indexes for Professional Nurses Involved in Hospital Infection Prevention and Control |
Three judgment matrices were established for the nine second-level indexes, resulting in C.R. of 0.016, 0, and 0.012, respectively. The cumulative weights assigned to ‘Proficiency in fundamental infection prevention and control practices’, ‘Capacity to deal with outbreaks’, ‘Training and education capacity’, ‘Proficiency in understanding policies and regulations regarding infection prevention and control’, ‘Capacity for infection risk assessment’, ‘Capacity for data collection and utilization’, ‘Sense of responsibility’, ‘Critical thinking ability’, ‘Autonomous learning capacity’ were 0.293, 0.108, 0.062, 0.212, 0.105, 0.106, 0.054, 0.035, and 0.025, respectively (Table 4). Nine judgment matrices were formulated for the 28 third-level indexes. The cumulative weights assigned to these indexes were as follows: 0.076, 0.029, 0.026, 0.041, 0.015, 0.049, 0.036, 0.021, 0.070, 0.025, 0.013, 0.037, 0.017, 0.008, 0.080, 0.032, and 0.100, respectively, and 0.105, 0.041, 0.018, 0.047, 0.043, 0.011, 0.003, 0.020, 0.012, 0.019, and 0.006, respectively. The C.R. for these judgment matrices was 0.097, 0.002, 0.003, 0.027, 0, 0.009, 0, 0.012, and 0, respectively (Table 5).
 |
Table 4 Allocating Weights to the Secondary-Level Indexes for Professional Nurses Engaged in Hospital Infection Prevention and Control |
 |
Table 5 Allocating Weights to the Tertiary-Level Indexes for Professional Nurses Involved in Hospital Infection Prevention and Control |
Training Effectiveness
Following homogenized training, there was a significant increase in the total score of professional nurses in infection prevention and control, rising from 79.50 to 89.75 (P < 0.001). Moreover, the number of nurses holding a bachelor’s degree surged from 7 to 20 (P < 0.001). Additionally, the number of nurses with intermediate or higher professional titles climbed from 7 to 20 (P = 0.010), including 8 with deputy senior titles and 5 with senior titles. The number of nurses who acquired the provincial certificate for professionals in infection prevention and control rose from 3 to 15 (P < 0.001), while those who obtained municipal-level or higher certificates increased from 5 to 20 (P < 0.001). Furthermore, there was a more than two-fold rise in the number of nurses publishing papers on infection prevention and control (P = 0.041). Additionally, all 20 nurses had successfully completed further studies (P < 0.001) (Table 6).
 |
Table 6 Professional Nurses Engaged in Hospital Infection Prevention and Control Within Our Region from 2018 to 2023 |
Discussion
IPC programs are essential for reducing healthcare-associated infections (HAIs) and antimicrobial resistance (AMR), promoting patient and healthcare worker safety, and strengthening healthcare systems.13 The World Health Organization (WHO) has developed a comprehensive IPC evaluation system based on eight core components, which provide a structured framework for assessing and improving IPC practices at both national and facility levels. This study referred to the WHO’s guidelines on core components of IPC programs emphasizing the importance of structured training and the implementation of standardized evaluation tools to improve IPC capacity. The evaluation system of our study is based on evidence-based guidelines and expert consensus, ensuring that the evaluation criteria are grounded in the latest scientific knowledge, which is both scientific and comprehensive. The system’s comprehensive nature is evident in its coverage of multiple dimensions of IPC, from program implementation and guideline development to education, surveillance, and infrastructure. This multi-faceted approach ensures that all critical aspects of IPC are assessed and addressed. Compared with WHO’s IPC evaluation system, the evaluation system of this study also took ‘Critical thinking ability’ and ‘Autonomous learning capacity’ into account. Critical thinking and self-learning abilities are essential for healthcare professionals as they enable effective problem-solving, continuous professional development, and adaptation to evolving healthcare challenges. These skills empower professionals to critically assess clinical situations, challenge assumptions, and make informed decisions, ultimately enhancing patient care.14 Moreover, self-learning fosters a proactive approach to knowledge acquisition, allowing healthcare workers to stay updated with the latest medical advancements and best practices. This is particularly crucial in a rapidly changing healthcare landscape where lifelong learning is necessary to maintain competence and address complex patient needs.15 The use of AHP aligns with WHO’s recommendations for developing scientifically valid and reliable evaluation systems.7 AHP provides a structured and scientific approach to competence evaluation, addressing the challenges of limited expertise and resource constraints in primary healthcare institutions.16 This method is particularly innovative in the context of China, where the application of AHP in hospital infection management is still in its early stages.17 However, its potential for improving decision-making and resource allocation is evident18. This study innovatively integrates AHP with standardized training programs, providing a novel approach to enhancing IPC competence in primary healthcare settings.
The scientificity of AHP lies in its ability to convert qualitative factors into quantitative weights through pairwise comparisons and consistency tests.16 This method reduces subjectivity and enhances the reliability of decision-making. In this study, C.R. for all judgment matrices was below 0.10, indicating that the evaluation system passed the consistency test. This ensures that the weights assigned to each index are scientifically grounded and reliable. Compared with WHO evaluation system, this evaluation has stronger practicability. In addition, the new system has passed the expert consultation and consistency test, which ensures the scientific and reliable scoring indicators. The new system more accurately reflects the capabilities and needs of primary IPC nurses.
The study demonstrates the practical application of AHP in enhancing the capacity of hospital infection management nurses. A practical case study in Shanghai19 demonstrated the effectiveness of AHP in evaluating IPC competence. The study found that many primary healthcare institutions lacked basic training materials and knowledge regarding sterile item procurement and waste management. By implementing an AHP-based evaluation system, the study identified key areas for improvement and provided targeted training to enhance IPC capacity. This case highlights the applicability of AHP in addressing real-world challenges in hospital infection management. Similar tools have been developed based on the WHO’s core competencies and have shown good evidence of validity and reliability.20,21 Such tools can be applied in countries of all income classifications, making it possible to design educational initiatives and enhance core competencies globally.
However, despite its strengths, AHP also has several limitations when applied to IPC evaluation systems. While AHP provides a structured approach to developing IPC evaluation systems, its limitations in handling subjectivity, complexity, interdependencies, and dynamic environments must be considered. Combining AHP with other methodologies, such as fuzzy logic or Delphi techniques, can help mitigate some of these limitations and enhance the robustness of IPC evaluation systems. AHP relies heavily on pairwise comparisons made by experts to determine the relative importance of criteria and sub-criteria. This process introduces subjectivity, as different experts may have varying opinions and experiences.22 This can lead to inconsistencies in the evaluation results, especially when multiple experts are involved.23 IPC environments are dynamic, with evolving threats and changing guidelines. AHP, however, is based on static pairwise comparisons and may not easily adapt to rapid changes. This can limit its effectiveness in continuously improving IPC practices. AHP assumes independence among criteria, which may not always be the case in IPC settings. For example, hand hygiene compliance may be interdependent with staff training and availability of supplies. Ignoring these interdependencies can lead to an incomplete evaluation of IPC practices.24 AHP focuses primarily on quantitative metrics derived from pairwise comparisons, potentially overlooking qualitative aspects of IPC. For instance, the quality of staff training or the effectiveness of communication channels may be difficult to quantify but are crucial for IPC success. AHP uses a C.R. to validate the pairwise comparisons. However, achieving a low C.R. (typically <0.1) can be challenging, especially when dealing with a large number of criteria. This may lead to questions about the reliability of the evaluation system.
Conclusion
This study provides valuable insights into the application of AHP in evaluating the competence of hospital infection management nurses. The results demonstrate significant improvements in nurse competence and highlight the effectiveness of AHP in addressing complex decision-making problems in healthcare. Future research should focus on further refining the evaluation system and exploring its application in other healthcare settings. Policymakers should prioritize resource allocation and targeted interventions to enhance IPC capacity in primary healthcare institutions.
Data Sharing Statement
The datasets generated and/or analysed during the current study are not publicly available but are available from the corresponding author (Jian-Shui Yang) on reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the declaration of Helsinki. This study protocols were approved by Changzhou Cancer Hospital committee. Informed consent was obtained from all participants.
Consent for Publication
Consent for publication was obtained from all participants whose data are included in this manuscript.
Funding
This study was supported by a grant from the 2023 Changzhou “Longcheng Medical Star” Health Youth Science and Technology Talent Support Project (Changzhou Medical Association, lcyx2023010), 2023 Changzhou Health and Health Young Talent Training Project (Changzhou Health Commission, CZQM2023021), the Applied Basic research Program of Changzhou Technology Division (CJ20241024).
Disclosure
None of the authors have any financial disclosure or conflict of interest.
References
1. Ali A, Amer S, Maha S, et al. The contribution of multidisciplinary teams to infection control in hospital settings: analyzing the roles of laboratory technologists, pharmacists, nurses, and psychologists in reducing hospital-acquired infections. Inter J Innov Res Engine Multidisciplin Phys Sci. 2020;4(8):2349–7300.
2. Kuhar D, Carrico R, Cox K, et al. Infection control in healthcare personnel: infrastructure and routine practices for occupational infection prevention and control services. 2019.
3. Huang C, Feng Z, Shen H, et al. Development of nurse manager’s core competence evaluation indicator system about hospital infection prevention and control. Chin Nurs Manage. 2022;22(12):1820–1825.
4. Zhao J, Qin B, Yan R, et al. Status and trend of the main healthcare-associated infection indicators in tertiary public hospitals in China (2018-2020). Chin J Hospital Inf Manage. 2022;21(06):524–31.
5. Amavasi B, Zimmerman PA. Infection prevention and control continuous education and training in pre-registration nursing programmes. Nurse Educ Today. 2024;133:106051. doi:10.1016/j.nedt.2023.106051
6. Shi Q, Hu B, Gao X, et al. Review of research on competency of nosocomial infection control personnel in China. Shanghai J Prev Med. 2024;36(05):511–515.
7. EUCIC. The EUCIC infection prevention and control certificate European training programme [EB/OL]. 2023.
8. Leal JE. AHP-express: a simplified version of the analytical hierarchy process method. MethodsX. 7:100748. doi:10.1016/j.mex.2019.11.021
9. He M, Lu H, Shen N, et al. Consensus on quality indicators for pediatric oncology nursing care in Mainland China: a Delphi method and analytic hierarchy process. J Pediatr Hematol Oncol Nurs. 2022;39(5):326–334.
10. Vimonkittipong U, Tochaiwat K, Sirithanyarat S, et al. Modified analytic hierarchy process site selection model for dental clinics in high-rent commercial buildings. J Int Soc Prev Community Dent. 2022;12(4):411–417. doi:10.4103/jispcd.JISPCD_89_22
11. Wu AH, Huang X, Li LY. Training guidelines for hospital infection management professionals (WS/T525-2016). Chin J Infect Control. 2018;16(01):94–97.
12. Mu J, Mao YP, Zhang L, et al. Construction of evaluation index system for hospital infection prevention and control ability of nursing staff based on Delphi method. Chin J Inf Control. 2022;21(12):1229–1235.
13. Leong M, Picton R, Wratten M, et al. Baseline evaluation of the world health organization (WHO) infection prevention and control (IPC) core components in Pacific Island Countries and Territories (PICTs). Antimicrob Resist Infect Control. 2024;13(1):108. doi:10.1186/s13756-024-01447-9
14. Heydari S, Beigzadeh A. Medical students’ perspectives of reflection for their professional development. BMC Med Educ. 2024;24(1):1399.
15. Hart EJ, de Heer-Koster MH, van der Harst M, et al. Key tips to shift student perspectives through transformative learning in medical education. BMC Med Educ. 2025;25(1):202. doi:10.1186/s12909-025-06754-2
16. Shshank C, Sangeeta P, Anuj K, et al. An overview of multi-criteria decision analysis and the applications of AHP and TOPSIS methods. Inter J Mathemat Engin Manage Sci. 2024;3(9):581–615.
17. Felix A, Abraão L, Carneiro M, et al. Cultivating excellence: development and validation of a bilingual competency self-assessment tool for infection prevention and control practitioners. Am J Infect Control. 2025;53(5):S0196–6553(24)00930–1. doi:10.1016/j.ajic.2024.12.020
18. Zhao Y, Wang T, Zhang C, et al. Research on the application of AHP-FAST-FBS in the design of home entrance disinfection devices in the post-pandemic era. Sci Rep. 2024;14(1):20550.
19. Yi Q, Liu Z, Liu X, et al. The development strategies of amateur table tennis matches in China based on the SWOT-AHP model: a case study in Shanghai. Sci Rep. 2024; 14(1):12060.
20. Multistate point-prevalence survey of health care-associated infections. N Engl J Med. 2022;386(24):2348. doi:10.1056/NEJMx210023
21. Mahdi Mousavi S, Jahadi Naeini M. Application of the analytical hierarchy process (AHP) in occupational health and safety [Internet]. Bus Manage Eco IntechOpen. 2025;147.
22. Akköse M, Polat Y. Multi-criteria decision analysis for supporting the selection of subclinical mastitis screening tests to use in large- and small-scale dairy farms in Türkiye. Trop Anim Health Prod. 2023;56(1):6. doi:10.1007/s11250-023-03844-5
23. Attari MYN, Moslemi Beirami AA, Ala A, et al. Resolving the practical factors in the healthcare system management by considering a combine approach of AHP and ANP methods. Eval Program Plann. 2023;100:102339. doi:10.1016/j.evalprogplan.2023.102339
24. Rishabh R, Das K. Selection of a suitable healthcare Supplier using AHP and TOPSIS methods hybridized in metaheuristic environment. SN Comput. 2025;6(2):164. doi:10.1007/s42979-025-03710-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.