")
Back to Journals » Risk Management and Healthcare Policy » Volume 18
Assessment of Diagnostic Knowledge and the Management of Bell’s Palsy Among Primary HealthCare Physicians in Saudi Arabia
Authors Al Jaber MY , Al Shammari A, Al Subaie FT, Alhowaish Z , Al Harbi MM, AlNaaim SA
Received 30 December 2024
Accepted for publication 8 April 2025
Published 2 May 2025 Volume 2025:18 Pages 1493—1502
DOI https://doi.org/10.2147/RMHP.S514912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Jongwha Chang
Mothana Yousif Al Jaber,1,* Ahmad Al Shammari,1,* Faisal Talal Al Subaie,1,* Zakaria Alhowaish,1,* Mahmoud Mohammed Al Harbi,1,* Saud A AlNaaim2,*
1College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia; 2Department of Neuroscience, College of Medicine, King Faisal University, Al-Ahsa, Saudi Arabia
*These authors contributed equally to this work
Correspondence: Mothana Yousif Al Jaber, College of Medicine, King Faisal University, Alhasa, Saudi Arabia, P.O. Box 400, Al-Ahsa, 31982, Saudi Arabia, Email [email protected]
Purpose: Bell’s palsy is a common cause of acute peripheral facial nerve paralysis. Its symptoms can mimic other severe conditions, posing diagnostic challenges for primary care physicians (PCPs). This study aimed to assess the diagnostic knowledge and management preparedness of PCPs in Saudi Arabia regarding Bell’s palsy. Particular emphasis was placed on identifying critical knowledge gaps that may affect clinical decision-making, especially in corticosteroid dosing and standardized diagnostic approaches.
Patients and Methods: A cross-sectional observational study was conducted in Al-Ahsa, Saudi Arabia. A total of 204 physicians participated in the study. Non-probability convenience sampling was used to recruit participants, which included general practitioners and family medicine physicians with at least 1 year of clinical experience. Structured surveys were distributed both online and in person to collect data on demographic information, knowledge of Bell’s palsy, diagnostic confidence, treatment approaches, and perceived barriers. Data analysis was performed using descriptive statistics and binary logistic regression in SPSS version 26.
Results: The mean knowledge score was 11.06 (standard deviation = 3.01), with significant gaps in areas such as the House–Brackmann grading system (57.8% correct) and the recurrence of Bell’s palsy (54.4% correct). Although most respondents correctly identified the cranial nerve (94.1%) and treatment timeline (65.7%), their knowledge of corticosteroid dosage was suboptimal (56.4%). Family medicine physicians had higher knowledge levels than general practitioners (p = 0.004). Moreover, 52.5% reported no diagnostic barriers, whereas 47.5% mentioned issues such as unclear diagnostic criteria (17.2%) and limited tools (8.3%). Among those interested in additional education, 94.1% preferred online training.
Conclusion: Although PCPs showed a strong understanding of Bell’s palsy, significant gaps were identified in advanced diagnostic and management areas. Addressing these deficiencies, particularly in corticosteroid dosing and structured diagnostic frameworks, is essential to enhancing clinical preparedness. These findings underscore the need for targeted educational interventions, including online training and standardized diagnostic protocols, to bridge knowledge gaps, improve diagnostic accuracy, and optimize patient management strategies.
Keywords: Bell’s palsy, peripheral facial nerve paralysis, public health, cross-sectional
Introduction
Bell’s palsy is a prevalent form of acute peripheral facial nerve paralysis of unknown etiology, responsible for 60–70% of all instances of unilateral facial paralysis globally.1 It is typically characterized by the abrupt onset of facial muscle weakness or paralysis on one side, often accompanied by pain around the ear or changes in taste sensation.1,2 While Bell’s palsy is usually self-limiting, early and accurate diagnosis is crucial for initiating appropriate treatment, such as corticosteroids, to enhance recovery and minimize potential complications.1,3
Primary care physicians (PCPs) are pivotal in the initial evaluation and management of Bell’s palsy as they are usually the first point of contact for patients presenting with facial paralysis. However, misdiagnosis or delayed diagnosis may occur as the symptoms of Bell’s palsy may resemble those of other severe conditions, such as cerebrovascular accidents, Ramsay Hunt syndrome, or tumors.2 Unlike Bell’s palsy, conditions such as ischemic or hemorrhagic strokes require urgent intervention, making it crucial for PCPs to quickly and accurately differentiate between them. Additionally, Ramsay Hunt syndrome, caused by varicella-zoster virus reactivation, presents with vesicular eruptions, which may not always be apparent in the early stages, further complicating diagnosis.2
PCPs must have a thorough understanding of the condition and be able to confidently distinguish it from other possible causes of facial paralysis. General practitioners (GPs) typically encounter an acute case of Bell’s palsy approximately once every 2 years.4 Due to this rarity, they are unlikely to develop sufficient expertise to manage cases where acute medical treatment is ineffective. Moreover, studies suggest that PCPs often face similar challenges with other neurological conditions, such as multiple sclerosis and myasthenia gravis, where the overlap of symptoms with more common disorders contributes to diagnostic uncertainty.5 Furthermore, timely referral to a facial reanimation service is critical because reconstructive options decrease monthly.5
The growing demand for primary healthcare services in Saudi Arabia underscores the importance of providing PCPs with the requisite knowledge and diagnostic confidence to effectively manage conditions such as Bell’s palsy.6 A study in the Qurayyat region of Saudi Arabia showed that Bell’s palsy was approximately 25.7 per 100,000 per year.7
The lack of research in the knowledge means that gaps in PCPs’ ability to distinguish Bell’s palsy from other neurological conditions remain unquantified, potentially leading to variability in patient management and outcomes. This significant gap underscores the need for research to identify areas for improvement and guide targeted educational initiatives. Our study aimed to assess the knowledge and diagnostic confidence of PCPs in managing Bell’s palsy in Saudi Arabia and to highlight potential areas for professional development, and ultimately provide a reference for improving the management of Bell’s palsy in Saudi Arabia.
Materials and Methods
Study Design and Population
This cross-sectional observational study was conducted to assess the diagnostic knowledge and preparedness of PCPs in Al-Ahsa, Saudi Arabia for managing Bell’s palsy. The study included physicians working in primary healthcare centers (PHCCs) and general hospitals across the Al-Hofuf, Al-Mubarraz, and Al-Omran sectors. The total population comprised 455 physicians distributed across 71 PHCCs and 11 general hospitals, although only 67 PHCCs and 5 general hospitals were included in the study. Data were collected using a combination of online and in-person questionnaires for comprehensive coverage. Participants were recruited using a non-probability convenience sampling technique. This study was conducted according to the STROBE guidelines.8
Eligibility Criteria
Participants were required to meet specific eligibility criteria for inclusion in the study. Physicians had to be between the ages of 25 and 60 years, with at least 1 year of clinical experience in managing Bell’s palsy cases. Eligible participants included General Practitioners (GPs) and family medicine physicians actively practicing in either Primary Healthcare Centers (PHCCs) or general hospitals within the targeted sectors in Al-Ahsa. Physicians were excluded from the study if they had less than one year of clinical experience, were specialists (eg, neurologists or otolaryngologists), or were not actively practicing. Additionally, participants who provided incomplete responses were excluded to ensure the data accurately reflected the knowledge and preparedness of primary care physicians in managing Bell’s palsy.
Data Collection Tools and Procedure
The data collection process used a structured survey instrument designed to capture relevant information in both online and in-person formats. The survey comprised the following four key sections:
- Demographic and Professional Background: Capturing participants’ age, sex, years of experience, and workplace details.
- Knowledge of Bell’s Palsy: Assessing understanding of the condition, its causes, symptoms, and diagnostic criteria.
- Diagnostic Confidence and Treatment Approaches: Exploring self-reported confidence in diagnosing and managing Bell’s palsy.
- Barriers to Effective Management and Training Needs: Identifying obstacles and areas for professional development.
The survey was distributed over a 1-month period, from November 19 to December 19, 2024, using convenience sampling across the included healthcare facilities.
Questionnaire Validation
The knowledge section was adapted from previous studies.9–11 Specifically, key questions were selected and modified to align with the study objectives, ensuring relevance to the target population. Any necessary linguistic and contextual adjustments were made to enhance clarity and applicability. Then, the survey instrument was meticulously developed by the principal investigator, a neurologist, in collaboration with the research team. To ensure content validity, the questionnaire was reviewed by two external neurology experts, whose feedback and recommendations were included in the final version. The instrument was subjected to a pilot study involving 30 physicians to refine the instrument further. Reliability was confirmed using a Pearson correlation coefficient of 0.82 and Cronbach’s alpha value of 0.75, demonstrating strong internal consistency.
Minimum Sample Size Estimation
Sample size was calculated using the Raosoft® software program,12 based on a 95% confidence level, 5% margin of error, and 50% assumed population proportion. From a total population of 455 physicians working in Al-Ahsa, the required sample size was 209.
Data Analysis
Data analysis was conducted using IBM SPSS Statistics software version 26. In the knowledge assessment, participants received 1 point for each correct response and 0 points for incorrect answers. The total knowledge score was calculated by summing the scores for all questions, with a possible score range of 0–15 points.
The frequencies and corresponding percentages for each question were determined. Additionally, the mean and standard deviation values were computed for each question to provide a detailed descriptive analysis. Binary logistic regression analysis was used to evaluate the impact of various variables on knowledge scores. Accordingly, age was categorized into two groups: >42 years and ≤42 years. Similarly, years of experience were divided into two categories: <18 years and ≥18 years. To analyze the relationship between years of experience and the knowledge score, the knowledge score was transformed into a three-tier model: A) Poor (0–5 points), B) Average (6–10 points) and C) Excellent (11–15 points). This transformation was applied in the correlation graph to clearly present the distribution and trends in knowledge levels among the different experience groups.
To minimize the risk of missing data, all survey questions were designed as mandatory fields, ensuring complete responses from participants. Additionally, a total of 12 responses were excluded from the final analysis as they did not meet the inclusion criteria, specifically for not being Primary Healthcare Physicians. Given the absence of missing data, no imputation techniques were required.
Ethical Considerations
Ethical approval was obtained from the King Faisal University Research Ethics Committee (KFU-REC-2024-DEC-ETHICS2916). Participation in the study was entirely voluntary, and informed consent was obtained from all respondents before their involvement. Confidentiality and anonymity were rigorously maintained throughout the research process to protect participants’ identities and ensure compliance with ethical standards.
Results
Demographics
A total of 216 participants completed the questionnaire; however, 12 were excluded, including 7 interns and 5 doctors from other specialties, leaving 204 (94.4%) valid responses. This yielded a valid response rate of 97.61% based on a targeted sample size of 209 participants.
Among the 204 healthcare professionals included in this study, the majority were male (68.1%), while females comprised the remaining 31.9% of the cohort. Regarding medical specialties, 61.8% were general practitioners, whereas 38.2% were family medicine specialists. Most participants were affiliated with hospitals (53.4%), followed by PHCCs (45.6%); only 1.0% reported non-hospital affiliations. The mean age of the participants was 42.38 years (SD = 11.23), and the mean duration of medical practice was 18.38 years (SD = 11.39). Additionally, the survey evaluated whether the participants had encountered patients with Bell’s palsy in their clinical practice. A total of 61.1% reported having encountered patients with Bell’s palsy, while 38.9%, had not (Table 1).
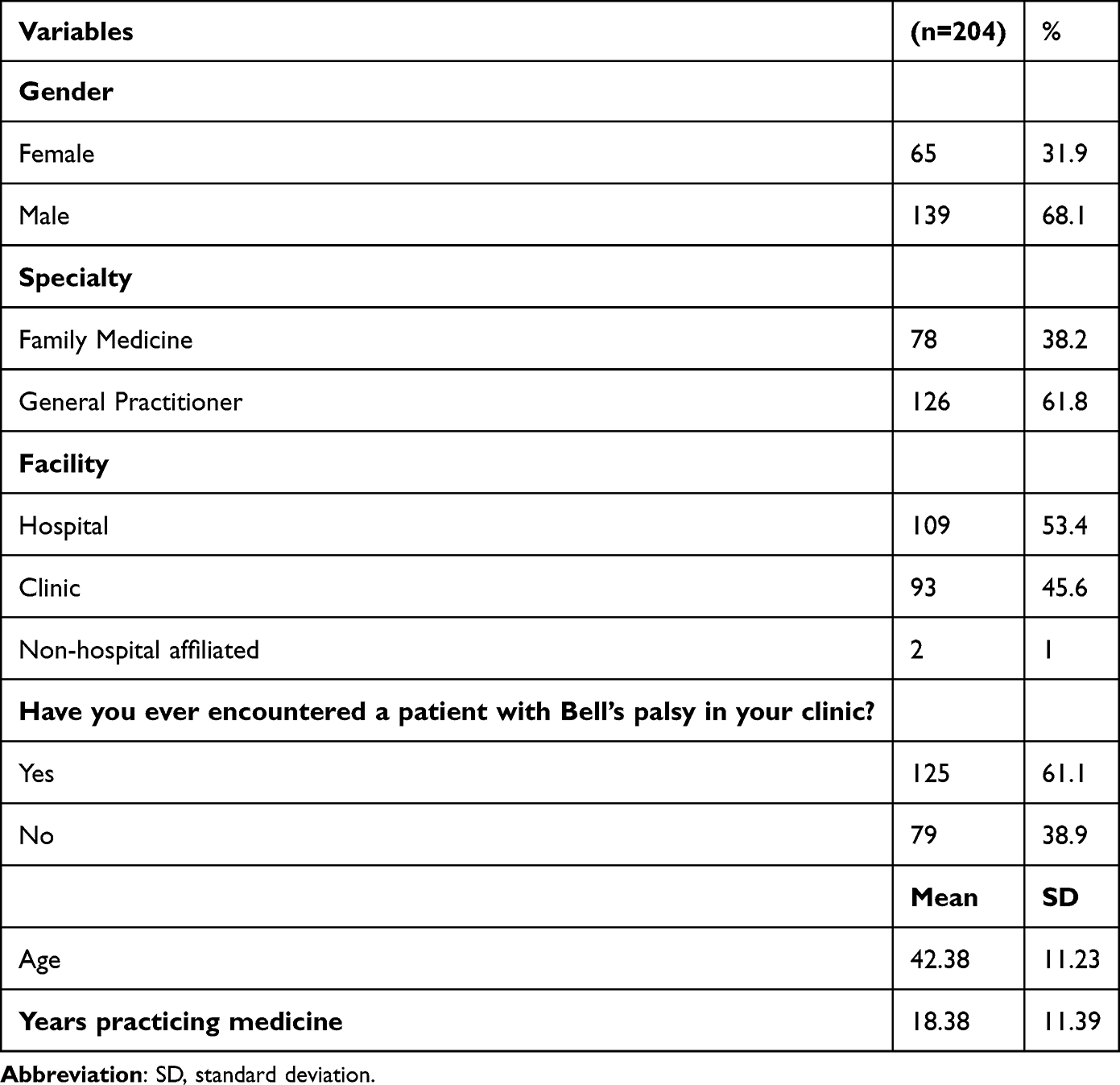 |
Table 1 Characteristics of the Included Participants |
Knowledge Assessment
The knowledge assessment revealed varying levels of understanding of Bell’s palsy among the participants. Most participants demonstrated a strong grasp of core concepts, with the majority correctly identifying the affected cranial nerve (94.1%, mean = 0.94, SD = 0.24) and recognizing that Bell’s palsy is a peripheral facial palsy (83.3%, mean = 0.83, SD = 0.37). Similarly, a high percentage correctly associated viral infections as potential triggers (92.6%, mean = 0.93, SD = 0.26) and identified early ocular complications (89.2%, mean = 0.89, SD = 0.31). However, knowledge was weaker in certain areas, such as whether Bell’s palsy could affect both sides of the face (44.1%, mean = 0.44, SD = 0.49), the optimal antiviral medication (62.7%, mean = 0.63, SD = 0.48), familiarity with the House–Brackmann Grading System (57.8%, mean = 0.58, SD = 0.49), and the understanding that Bell’s palsy could recur in the same patient (54.4%, mean = 0.54, SD = 0.49).
Furthermore, participants showed a moderate understanding of treatment timelines (65.7%, mean = 0.66, SD = 0.47) and the duration of Bell’s palsy (66.2%, mean = 0.66, SD = 0.47). They displayed better knowledge of the next steps for non-improvement within two to three weeks (85.8%, mean = 0.86, SD = 0.35), appropriate diagnostic tests (78.4%, mean = 0.78, SD = 0.41), and awareness of potential complications (77.9%, mean = 0.78, SD = 0.41). Overall, the total mean knowledge score was 11.06 (SD = 3.01), reflecting a generally good level of knowledge, but with identifiable gaps (Table 2).
 |
Table 2 Knowledge Questions with the Frequency of Correct and Incorrect Answers |
Knowledge About Corticosteroids
Among the 149 (70%) participants who responded to questions about corticosteroid use in patients with Bell’s palsy, the overall mean knowledge score was 1.8 (SD = 1.28), indicating the need for improvement in this area. Regarding the most recommended type of corticosteroid, prednisolone was correctly identified by the majority (68.5%, mean = 0.58, SD = 0.49), followed by dexamethasone (26.8%), while hydrocortisone (3.4%) and “I don’t know” responses (2%) were less frequent.
For the recommended dosage, 56.4% correctly selected 60–80 mg/d (mean = 0.67, SD = 0.39). However, misconceptions were noted, with 26.2% selecting 20 mg/d and 12.8% selecting 30–40 mg/d. A small proportion (4.6%) of respondents were unsure.
Knowledge of the recommended duration of corticosteroid therapy was high, with 70.5% correctly identifying 5–7 days (mean, 0.70; SD, 0.45). Misunderstandings were observed among 18.8%, who incorrectly selected 2–3 weeks, while smaller groups selected either 1–3 days (3.4%), “More than a month” (3.4%), or “I don’t know” (4%) (Table 3).
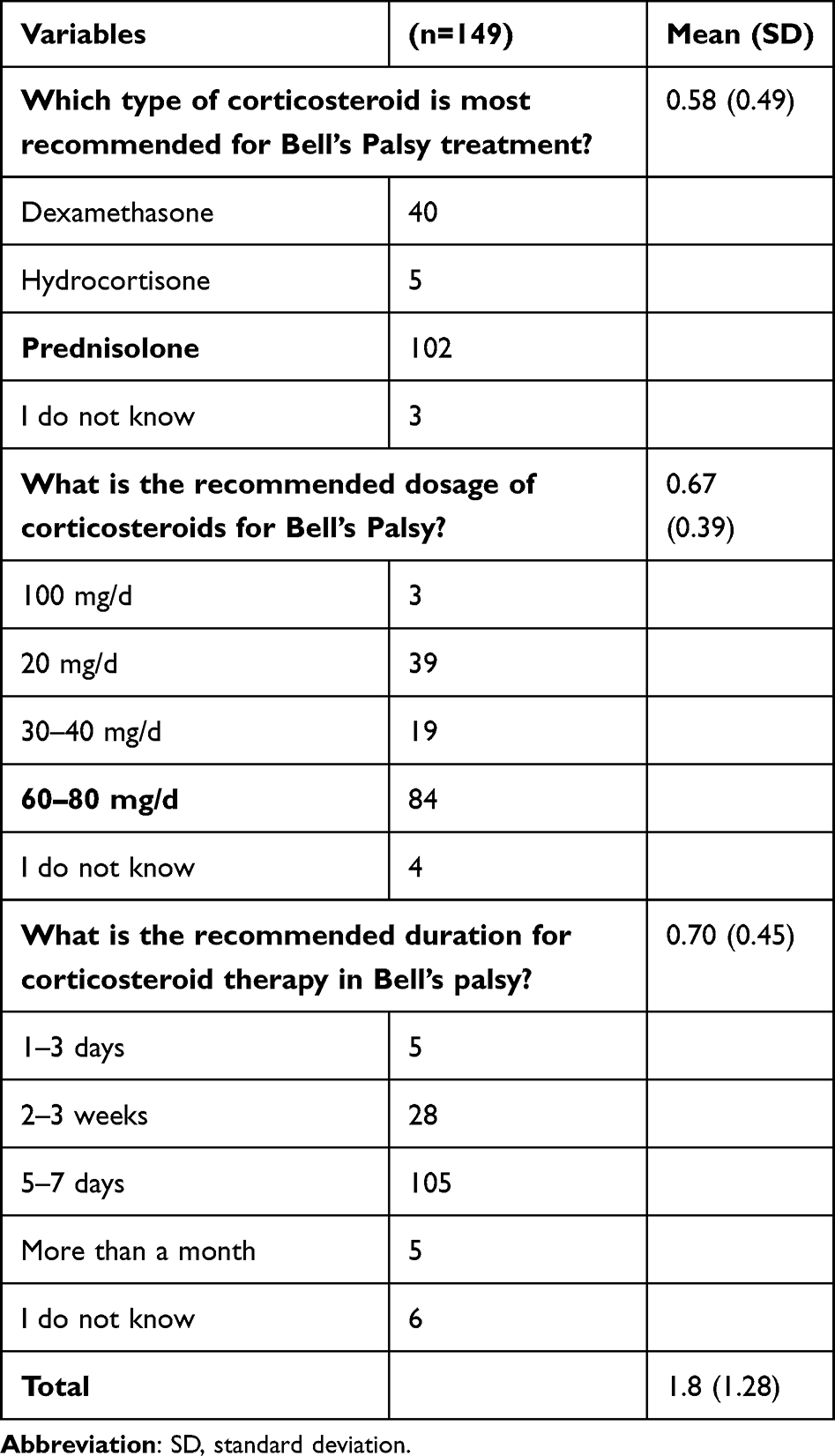 |
Table 3 Multiple Choice Knowledge Questions with the Mean Number of Correct Answers |
Barriers and Future Directions
Among the 204 (96%) participants, over half (52.5%) reported facing no barriers to diagnosing Bell’s palsy. However, the remaining 47.5% identified various challenges, the most common being a lack of clear diagnostic criteria (17.2%) combined with difficulty in distinguishing Bell’s palsy from other conditions (4.4%) or limited diagnostic tools (8.3%). Time constraints were cited less frequently, with only 2% identifying it as a standalone issue and 1.5% reporting it in combination with other factors. Notably, a small minority (0.5%) faced multiple barriers, including all four factors (lack of criteria, limited tools, time constraints, and diagnostic challenges).
Regarding interest in additional training, 61.3% expressed a willingness to enhance their knowledge of Bell’s palsy, with online sessions being overwhelmingly preferred (94.1%) over on-site training sessions (5.9%). These findings suggest the need for targeted educational interventions, particularly in an accessible online format, to address the identified diagnostic challenges and improve confidence in managing Bell’s palsy (Table 4).
 |
Table 4 Barriers and Future Perspectives |
Factors That Affecting the Knowledge Score
Logistic regression analysis revealed that being a GP was significantly associated with lower knowledge levels about Bell’s palsy (p = 0.004), with GPs having 14.5% lower odds of having higher knowledge than other specialties (OR = 0.855, 95% confidence interval [CI]: 0.769–0.951). In contrast, gender, working in a hospital facility, having encountered a patient with Bell’s palsy, being over 42 years old, and having over 18 years of practice were not significantly associated with knowledge (p > 0.05). Although the odds ratios for these variables ranged from 1.014 to 1.091, they indicated minimal and non-significant effects on knowledge (Table 5).
 |
Table 5 Regression Analysis of the Association Between Knowledge Score and Multiple Factors |
We also transferred the knowledge score to the three-point scoring system (Excellent, Average, and Poor) to detect any possible correlation between knowledge and years of experience. However, there was no significant difference in correlation (Figure S1).
Discussion
Our cross-sectional study provides valuable insights into the diagnostic knowledge and preparedness of PCPs in managing Bell’s palsy in Al-Ahsa, Saudi Arabia. The high response rate of 97.61% underscores the significant interest of healthcare professionals in enhancing their understanding of this condition, which aligns with the increasing global prevalence of peripheral facial nerve disorders.1,2
The results revealed that participants had substantial knowledge of fundamental aspects of Bell’s palsy, such as its idiopathic origin (85.4%) and association with viral triggers (92.6%); however, there are notable gaps in their understanding of advanced diagnostic tools and treatment protocols. These findings are consistent with those of previous studies showing that while physicians are proficient in identifying common symptoms, they may miss details such as grading scales and evidence-based interventions.2,3
A key finding was the limited familiarity with the House–Brackmann grading system, with only 57.8% of respondents recognizing its clinical utility. This aligns with previous research highlighting that the absence of standardized diagnostic tools in primary care impedes accurate severity assessments and effective treatment planning.4 Similarly, knowledge of corticosteroid therapy, known as the cornerstone of Bell’s palsy management, was incomplete. Only 56.4% of participants identified the correct dosage of 60–80 mg/day, and 70.5% understood the optimal treatment duration of 7–10 days, underscoring the need for enhanced training.5,12,13
Diagnostic barriers remain a major challenge, with 17.2% of participants having trouble distinguishing Bell’s palsy from other conditions such as Ramsay Hunt syndrome, cerebrovascular accidents, and tumors. This aligns with global data showing that diagnostic ambiguity often leads to delayed or inappropriate treatment, further underscoring the need for comprehensive education.14,15
Our analysis also highlighted an association between specialty and diagnostic confidence, with family medicine physicians demonstrating superior knowledge than GPs. This finding is supported by research showing that specialized training enhances diagnostic accuracy and preparedness for managing complex neurological conditions.16,17 Additionally, 38.4% of the participants identified the absence of formalized continuing medical education for Bell’s palsy as a barrier to professional development, consistent with findings in similar healthcare systems.18
Interestingly, while 61.1% of the respondents reported encountering cases of Bell’s palsy during their clinical practice, only 44.3% had received formal training in its management. This discrepancy indicates a reliance on experiential learning rather than structured education, a trend observed in other studies of neurological disorders in primary care.19,20 Furthermore, a strong preference for online training formats (94.1%) suggests the opportunity to leverage digital platforms to deliver targeted and accessible education.21
While our analysis revealed no association between the age and sex with the knowledge score among primary healthcare physicians. A study by Altowayan et al, 2023 conducted among the general population in Al-Qassim Region, showed that age and sex were significantly associated with the knowledge score.22
The participants showed a good understanding of the ocular complications associated with Bell’s palsy, such as lagophthalmos and exposure keratitis, with 88.3% correctly identifying these risks. This is consistent with previous studies emphasizing the importance of eye care to prevent vision loss in managing Bell’s palsy.23 However, only 52.7% were aware of referral pathways for facial reanimation services, which are critical for patients with persistent or severe symptoms.24,25 Physical therapists in Saudi Arabia demonstrate moderate knowledge and positive attitudes toward BP rehabilitation.2 This underscores the potential for interdisciplinary collaboration between PCPs and physical therapists to enhance the rehabilitation and management of Bell’s palsy in the region.
The strong preference for online training (94.1%) highlights a promising avenue for educational interventions aimed at improving physicians’ confidence in diagnosing and managing Bell’s palsy. To maximize effectiveness, future training programs should be designed with interactive components, such as case-based learning, expert-led discussions, and self-assessment modules.
Our analysis highlights the need for targeted interventions to address gaps in knowledge, particularly regarding grading systems, corticosteroid use, and advanced management strategies. Establishing regional guidelines and integrating Bell’s palsy-focused modules into ongoing medical education programs could significantly enhance diagnostic confidence and patient outcomes.
Interdisciplinary collaboration, particularly with specialists such as neurologists or otolaryngologists, could play a pivotal role in enhancing PCPs’ diagnostic confidence and management of Bell’s palsy. By fostering a multidisciplinary approach, PCPs could benefit from expert guidance on complex cases, ultimately improving the accuracy of diagnosis and treatment decisions. Future research could explore how structured collaboration and regular consultations with specialists may enhance PCPs’ knowledge, reduce diagnostic uncertainty, and improve patient outcomes.
This study has several limitations. First, its cross-sectional design captures data at a single point in time, which limits the ability to observe changes in PCPs’ knowledge or practices over time. Second, the regional focus on Al-Ahsa restricts the generalizability of the findings to other regions or healthcare systems with different resources, training standards, or patient demographics. Third, the study relied on self-reported data, which may introduce response bias. Fourth, non-probability convenience sampling may introduce selection bias. Fifth, the one-month data collection period, which may introduce bias related to physician availability. However, recruitment efforts were structured to include physicians from various shifts and practice settings to enhance representativeness. Sixth, our study was specific to diagnostic knowledge, future studies should study a more comprehensive level of knowledge. Future research should consider longitudinal designs, broader geographic coverage, and objective assessments to provide a more comprehensive understanding of PCPs’ preparedness to manage Bell’s palsy.
Conclusion
This study provides valuable insights into the strengths and limitations of PCPs’ knowledge and preparedness to manage Bell’s palsy in Al-Ahsa, Saudi Arabia. Although participants demonstrated commendable expertise in certain areas, significant gaps were identified in grading systems, corticosteroid use, and understanding recurrence patterns. These findings underscore the need for targeted educational initiatives, such as online training modules, and the integration of Bell’s palsy-focused content into primary care curricula. To effectively design and implement these online training modules, it is crucial that they are interactive, evidence-based, and tailored to address the specific knowledge gaps identified in this study. Such modules could include video demonstrations of clinical scenarios, quizzes to reinforce learning, and resources for ongoing self-assessment.
Furthermore, future research should explore the impact of such training interventions on diagnostic accuracy, particularly through longitudinal studies that assess knowledge retention and changes in clinical practice over time.
To improve patient outcomes, we recommend establishing clear diagnostic protocols, enhancing access to training resources, and placing greater emphasis on early intervention strategies. Specific examples of early intervention strategies include the timely use of corticosteroid therapy within 72 hours of symptom onset, eye care interventions such as lubrication and protection against corneal exposure, and prompt referral for facial reanimation services in cases of persistent symptoms. Additionally, these strategies could be better integrated into primary care settings by ensuring that they are included in clinical guidelines and reinforced through training programs and regular case discussions. Collaboration between academic institutions and healthcare organizations is crucial for promoting evidence-based practices and equipping PCPs with the necessary skills for effective management. Also, continuous professional development or workshops to reinforce knowledge and improve patient outcomes are needed.
Abbreviations
PCPs, Primary Care Physicians; GPs, General Practitioners; PHCCs, Primary Healthcare Centers.
Funding
This work was supported by the Deanship of Scientific Research, Vice Presidency for Graduate Studies and Scientific Research, King Faisal University, Saudi Arabia (Grant No: KFU243009).
Disclosure
The authors report no conflicts of interest in this work.
References
1. van Veen MM, ten Hoope BWT, Bruins TE, Stewart RE, Werker PMN, Dijkstra PU. Therapists’ perceptions and attitudes in facial palsy rehabilitation therapy: a mixed methods study. Physiother Theory Pract. 2022;38(12):2062–2072. doi:10.1080/09593985.2021.1920074
2. Albishi A, Al-Ageel H, AlAbdulwahab S. Knowledge and attitude towards bell’s palsy rehabilitation among physical therapists in Saudi Arabia: a cross-sectional study. Risk Manag Healthc Policy. 2024;17:2401–2413. doi:10.2147/RMHP.S481457
3. Peitersen E. Bell’s Palsy: the spontaneous course of 2500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol. 2002;122(7):4–30. doi:10.1080/000164802760370736
4. Glass GE, Tzafetta K. Bell’s palsy: a summary of current evidence and referral algorithm. Fam Pract. 2014;31(6):631–642. doi:10.1093/fampra/cmu058
5. Baugh RF, Basura GJ, Ishii LE, et al. Clinical practice guideline: Bell’s palsy. Otolaryngol Head Neck Surg. 2013;149(S3):S1–27.
6. Tiemstra JD, Khatkhate N. Bell’s palsy: diagnosis and management. Am Fam Physician. 2007;76(7):997–1002.
7. Alanazi F, Kashoo FZ, Alduhishy A, Aldaihan M, Ahmad F, Alanazi A. Incidence rate, risk factors, and management of Bell’s palsy in the Qurayyat region of Saudi Arabia. PeerJ. 2022;10:e14076.
8. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. STROBE initiative. the strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344–349. doi:10.1016/j.jclinepi.2007.11.008
9. Sullivan FM, Swan IRC, Donnan PT, et al. Early treatment with prednisolone or acyclovir in bell’s palsy. N Engl J Med. 2007;357(16):1598–1607. doi:10.1056/NEJMoa072006
10. Gronseth GS, Paduga R. Evidence-based guideline update: steroids and antivirals for Bell palsy. Neurology. 2012;79(22):2209–2213. doi:10.1212/WNL.0b013e318275978c
11. Adour KK. Diagnosis and management of facial paralysis. N Engl J Med. 1982;307(6):348–351. doi:10.1056/NEJM198208053070605
12. Raosoft. Raosoft Sample Size Calculator [Computer Program]. Seattle, WA: Raosoft, Inc; 2004.
13. Bleicher JN, Hamiel S, Gengler JS, Antimarino J. A survey of facial paralysis: etiology and incidence. Ear Nose Throat J. 1996;75(6):355–358. doi:10.1177/014556139607500608
14. Quant EC, Jeste SS, Muni RH, Cape AV, Bhussar MK, Peleg AY. The benefits of steroids versus steroids plus antivirals for treatment of Bell’s palsy: a meta-analysis. BMJ. 2009;339(sep07 1):b3354–b3354. doi:10.1136/bmj.b3354
15. Kim C, Lelli GJ. Current considerations in the management of facial nerve palsy. Curr Opin Ophthalmol. 2013;24(5):478–483. doi:10.1097/ICU.0b013e3283634869
16. House JW, Brackmann DE. Facial nerve grading system. Otolaryngol Head Neck Surg. 1985;93(2):146–147. doi:10.1177/019459988509300202
17. Valls-Solé J. Facial nerve palsy and hemifacial spasm. Handbook Clin Neurol. 2013;115:367–380. doi:10.1016/B978-0-444-52902-2.00020-5
18. May M, Schaitkin BM. The Facial Nerve. New York: Thieme Medical Publishers; 2000:256–270.
19. Kim J, Lee HY, Kim MN, Loehrl T, Poetker DM. Prognosis and recovery in Bell’s palsy: a prospective study. Am J Otolaryngol. 2012;33(5):473–479. doi:10.1016/j.amjoto.2011.08.009
20. Peitersen E. The natural history of Bell’s palsy. Am J Otol. 1982;4(2):107–111.
21. Gagyor I, Madhok VB, Daly F, Sullivan F. Antiviral treatment for Bell’s palsy (idiopathic facial paralysis). Cochrane Database Syst Rev. 2019;2019(9):1.
22. Altowayan RM, Alruwaysan SA, Alraddadi S, et al. Knowledge and awareness regarding Bell’s Palsy in the Al-Qassim Region, Saudi Arabia. Cureus. 2023;15(12):e51327. doi:10.7759/cureus.51327
23. Murakami S, Mizobuchi M, Nakashiro Y, Doi T, Hato N, Yanagihara N. Bell Palsy and Herpes Simplex Virus: identification of viral DNA in endoneurial fluid and muscle. Ann Intern Med. 1996;124(1_Part_1):27. doi:10.7326/0003-4819-124-1_Part_1-199601010-00005
24. Bayoumy AB, de Ru JA. Cochrane systematic review antiviral treatment for bell’s palsy: an opposing opinion! SN Compr Clin Med. 2020;2(7):928–932. doi:10.1007/s42399-020-00339-4
25. Novak CB. Rehabilitation Strategies for Facial Nerve Injuries. Semin Plast Surg. 2004;18(1):47–51. doi:10.1055/s-2004-823123
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.