")
Back to Journals » Cancer Management and Research » Volume 17
Assessment of Knowledge Gaps in Cervical Cancer Screening and HPV Vaccination Among Chinese Women: A Comprehensive Population-Based Study
Authors Huang X, Ruan G , Sun P
Received 14 October 2024
Accepted for publication 14 January 2025
Published 11 February 2025 Volume 2025:17 Pages 267—279
DOI https://doi.org/10.2147/CMAR.S500946
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Xinxin Huang,1 Guanyu Ruan,2 Pengming Sun2
1The Ministry of Health, Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China; 2Laboratory of Gynecologic Oncology, Fujian Clinical Research Center for Gynecologic Oncology, Fujian Matermity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics, Fujian Medical University, Fuzhou, Fujian Province, People’s Republic of China
Correspondence: Guanyu Ruan; Pengming Sun, Email [email protected]; [email protected]
Background: While studies on cervical cancer screening (CCS) and human papillomavirus (HPV) vaccine uptake exist in China, few have examined both within populations participating in CCS programs.
Methods: This cross-sectional, population-based survey included 37,797 women aged 18– 64 years attending gynecological outpatient clinics. Participants completed a questionnaire assessing CCS awareness and participation. Additionally, HPV vaccine knowledge was investigated in a sub-sample of 17,010 women aged < 45 years.
Results: The mean age of participants was 45.06 years (SD: 8.52). The mean CCS knowledge score was 63.13%, with 52.53% reporting prior CCS uptake. Factors associated with lower CCS knowledge included low monthly household income, lack of rural cooperative medical insurance, low literacy, not having received CCS within the past 3 years, unmarried status, and childbirth history. A strong positive correlation was observed between CCS knowledge and adherence to CCS recommendations (Spearman correlation coefficient: 0.708, p < 0.01). Awareness of the HPV vaccine was reported by 48.33% of participants, with HPV vaccine knowledge positively correlated with CCS awareness (Spearman correlation coefficient: 0.629, p < 0.01). CCS knowledge partially mediated the relationship between HPV vaccine knowledge and willingness to vaccinate, with a mediating effect size of 21.16%.
Conclusion: Integrated health education efforts targeting CCS and HPV vaccine awareness are essential. Empowering women to understand the significance of HPV vaccination and regular CCS participation can enhance cervical cancer prevention strategies.
Keywords: knowledge, cervical cancer, HPV vaccine, screening, mediating effect
Introduction
Cervical cancer (CC) is the second most common cancer and the second leading cause of cancer-related deaths among women of reproductive age globally in 2020, with 604,127 new cases and 341,831 deaths.1 China accounts for nearly one-fifth of the global burden of CC.2 In China, the age-standardized incidence and mortality rates of CC are 10.42 per 100,000 people and 2.84 per 100,000 people, respectively.3
CC can be prevented through vaccination and screening with appropriate follow-up and treatment.4 To accelerate the elimination of CC, in 2020, the World Health Organization released a global strategy that sets out 90–70-90 milestones for the world to achieve by 2030: that is, 90% of girls will be vaccinated against HPV by the age of 15 years, 70% of women aged 35–45 years will receive high-quality screening, and 90% of diagnosed patients will be treated.5 Nineteen hundred forty-four countries, including China, have committed themselves to this program, which aims to eradicate this cancer.
Cervical cancer screening (CCS) programs that contribute to the reduction of incidence and mortality rates play an important role in the prevention of this disease.6 CCS is an effective secondary prevention measure and a long-term management strategy to control cervical precancer and cancer. For a woman who has CCS just once in her life after 35 years of age, her risk of dying from CC decreases by 70%. If she is screened every 5 years, her risk of dying CC decreases by more than 85%.7 CCS strategies differ between countries.6 In 2009, China initiated the National Cervical Cancer Screening Program (NCCSP), providing free CCS for women aged 35 to 64 years with government financial support. The coverage of screening is essential for reducing the incidence of CC.8 Developed countries with comprehensive cancer screening programs have experienced sustained decreases in cancer incidence and mortality, while many developing countries continue to experience increases in cancer incidence and mortality.9 There are many sociocultural and clinical factors and barriers affecting CCS and its effectiveness.10 The Guidelines for CC Prevention and Control11 mention that one of the barriers to the control of CC is a lack of knowledge of CC and its prevention. Many studies from different countries have confirmed that a lack of knowledge about CC is a significant barrier to attending a CCS program.12 A recent report showed that 130 million women between the ages of 30 and 49 years in China have never received CCS,13 and understanding the knowledge of the population can help optimize CCS strategies.
Up to 99% of CC cases are associated with high-risk HPV.14 The HPV vaccine can reduce the incidence of CC by approximately 70%. It also prevents other diseases, such as anal cancer, genital warts, and oropharyngeal cancer.15 HPV vaccination is a key measure for preventing CC. Vaccines that protect against HPV are recommended by the World Health Organization (WHO). They are approved for use in many countries. China approved the bivalent vaccine (2-valent HPV) in 2016, the quadrivalent vaccine (4-valent HPV) in 2017, and the nine-valent vaccine (9-valent HPV) in 2018. In 2023, the Chinese government issued the Circular on the Issuance of the Action Plan for Accelerating the Elimination of Cervical Cancer (2023–2030), proposing to improve the comprehensive prevention and treatment mechanism for CC and to promote HPV vaccination services for girls of school age. Overall promotion and key breakthroughs have actively promoted the incorporation of HPV vaccination into local policies for the benefit of people in places where it is possible to do so; in Fujian Province, where this study was carried out, the government initiated a work program to provide free HPV vaccination for school-age girls, and the vaccination rate for school-age girls has reached more than 90%.
Several studies have been conducted in China to characterize HPV vaccination behavior. Most of these have focused on female college students and parents of girls in junior and senior high school, or specifically on health care workers. Some studies have also examined women’s attitudes to CCS screening. For example, in China’s first study of CCS awareness and factors influencing it in rural areas of different socio-economic regions in 2013, women with more than 60% of the total score were defined as having high awareness, while the opposite was true for low awareness.16 However, there are few studies of HPV perceptions specifically among women under 45 years of age, and few studies analyzing perceptions of CCS and HPV vaccine. Acceptance of HPV vaccination and CCS has been reported to be associated with understanding and perceptions of CC.17 Therefore, understanding the knowledge and acceptance of women in the audience is essential for developing national screening and vaccination programs. Because the current age for HPV vaccination is under 45 years, and the age for CCS funded by the Chinese government is under 65 years, we recruited adult women aged 18–64 years to participate in this survey. We hypothesized that women’s perceptions of CCS would influence their knowledge of the HPV vaccine and play a role in the relationship between HPV vaccine knowledge and vaccination.
This survey was conducted to assess the knowledge of CCSs, awareness of the HPV vaccine, current status of participation, and influencing factors among residents of Fujian Province, China. The results of this study can provide a scientific basis for the effective promotion of women’s CCS policies and the popularisation of HPV vaccination.
Methods
Study Design and Participants
A cross-sectional population-based survey was conducted between October and November 2023 in Fujian Province in southeastern China. The subjects of this study were women between the ages of 18 and 64 years who were recruited from gynecological clinics, physical examination centers, or cervical cancer screening sites. In China, the government provides free CCS for some women between the ages of 35 and 64. All counties and districts in Fujian Province carry out free CCS, so all counties and districts conduct study recruitment. Women were invited to participate in the study if they attended gynecological clinics at CCS sites and medical examination centers. After giving informed consent, participants completed an electronic cross-sectional survey in the clinic.
Study Instrument
Data collection for this study was carried out using the Chinese online survey application “Questionnaire Star” (https://www.wjx.cn/). Respondents were asked to complete an electronic questionnaire by scanning a QR code or clicking on a link generated by QuestionStar. China’s National Health Commission (NHC) updated and issued the Cervical Cancer Screening Work Program in 2022, which contains 10 core pieces of knowledge on health education for CC prevention and treatment that are certified by an expert group (Table 1).
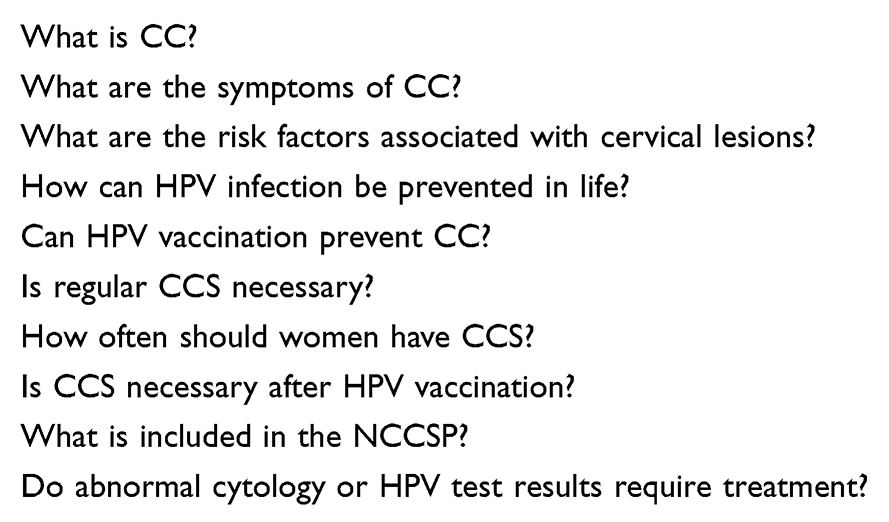 |
Table 1 Ten Core Knowledge of Health Education on Cervical Cancer Control Promulgated by NHC |
The questionnaire was designed by epidemiologists and gynecologists and was based on the National Health Commission of China’s core knowledge of health education for cervical cancer prevention and control, with additional items on knowledge of the HPV vaccine and willingness to be vaccinated. The questionnaire underwent two rounds of Delphi expert correspondence. To ensure validity and efficacy, the questionnaire was first piloted with 200 women aged 18–64, and the content and language were adapted based on their feedback.
Different studies in medicine have different definitions of high awareness. Some scholars think that more than 75% of the total score is considered as high awareness,18 and some scholars think that more than 70%19 or 50%20 of the total score is defined as high awareness. To compare public acceptance and knowledge of CCS projects in China after more than ten years of government financial support, this study was consistent with the way it was defined in China in 2013,16 where ratings above 60% of the total score were defined as high levels of knowledge.
Survey Items
The questionnaire consisted of four parts: the first part was a short introduction to the purpose of the study and need-to-know information was used to determine whether participants agreed to participate in the study. The second section collected the demographic characteristics of the participants. In the third section, knowledge about CCS and the level of recommendation. In the fourth section, women under 45 years of age were asked about their knowledge of the HPV vaccine, vaccination status, and reasons for not wanting to receive the HPV vaccine. Correct answers were scored and incorrect answers were not scored. 10 questions were asked on knowledge of CCS and 10 questions were asked on knowledge of the HPV vaccine, each scoring 10 points. The title was taken from the Cervical Cancer Screening Work Programme updated and published by the NHC of China. Higher scores indicate greater awareness. The questionnaire has been tested for reliability and validity. Higher scores indicate higher levels of awareness.
Study Variables
The dependent variables in this study were respondents’ awareness of the CCS and HPV vaccine and their vaccination intentions. The independent variables include age, marital status, fertility status, type of medical insurance, level of education received, per capita monthly household income, and occupation.
Statistical Analyses
Statistical analyses were performed using SPSS 26.0. Continuous variables are expressed as the means ± standard deviations (SDs) or as medians [interquartile ranges], and Student’s t-tests or Wilcoxon rank-sum tests were performed depending on the normality of the distributions of the variables, as appropriate. The categorical variables were expressed as n (%), and the chi-square test or Fisher’s exact probability test was performed for comparison. For the multivariate models, multiple linear regression was used for the model with a continuous dependent variable, and logistic regression was used for the models with a dichotomous dependent variable. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated by multivariable analysis using backward logistic regression analysis. We used the Wald statistic, in which the variables with p≥0.15 were eliminated from the model one by one. Correlations were calculated using Pearson’s or Spearman correlation coefficients. The level of significance was 0.05 for all analyses.
Results
Participant Characteristics
As the system was logically set up so that only participants who completed all the questions could submit the questionnaire, all the questionnaires recorded were valid. A total of 37,797 valid questionnaires were collected. The average age was 45.06±8.52 years. Table 2 summarizes the socioeconomic and demographic characteristics of the study participants. Most participants (28,599, 75.66%) were aged 36 to 55, and the largest proportion were first married (33,986, 89.92%). The proportion of people with an education level of junior high school and below was the largest (24382, 64.51%). Women with a per capita monthly income of RMB 3000–5000 make up the largest proportion, at 41.34%, followed by those with a per capita monthly income of less than RMB 3,000, at 37.32%.
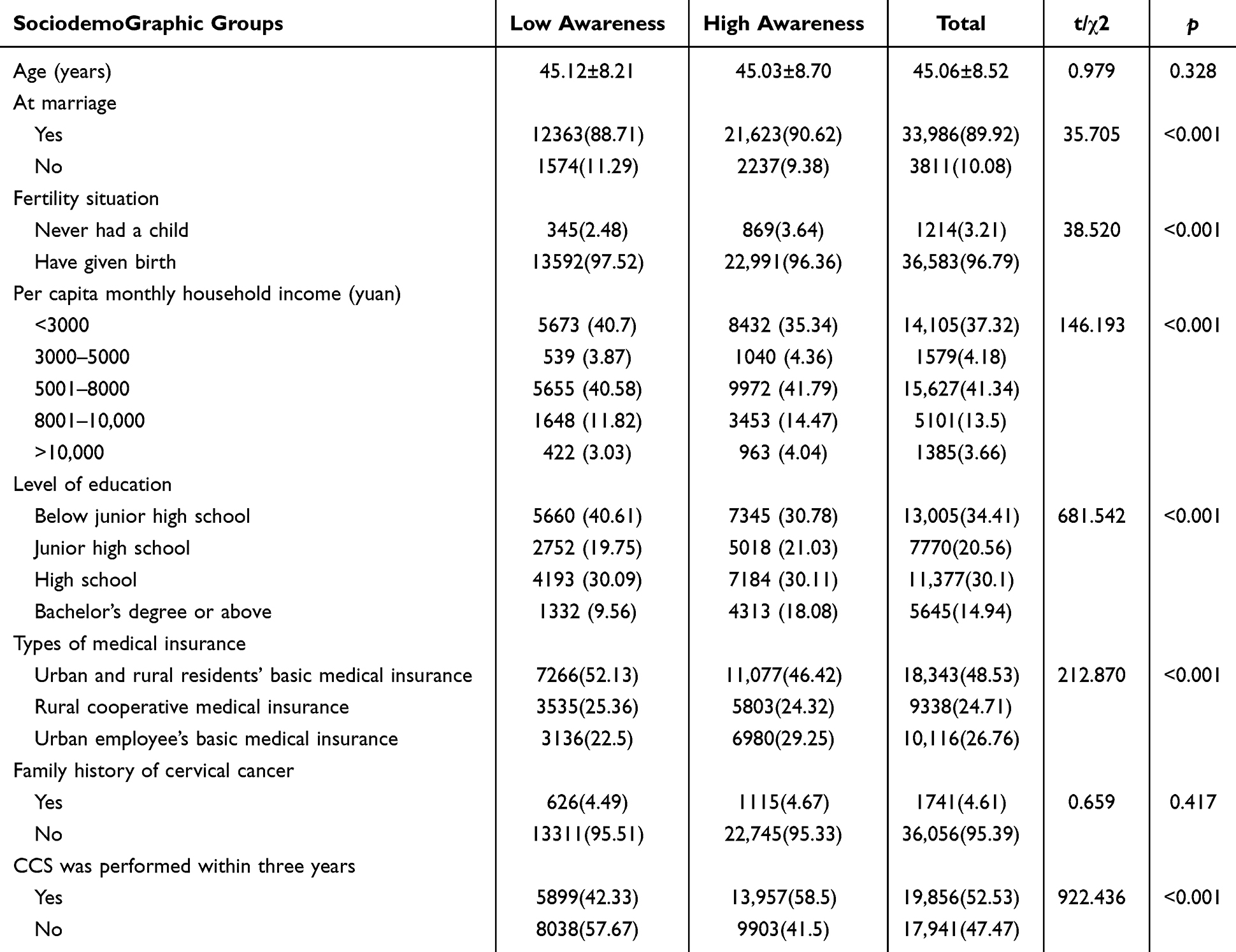 |
Table 2 Demographic and Socioeconomic Characteristics of the Study Participants (N = 37,797) |
CCS Total Knowledge Level
Most participants had heard of CCS (34,709, 91.83%). The Cronbach’s alpha coefficient of the knowledge questionnaire was 0.758. Correlation coefficients between the total score and other items ranged from 0.413 to 0.698 (p<0.01). The test-retest reliability was 0.903.
The average score of the respondents was 6.38±2.58, and the awareness rate was 63.13%.
There was no significant difference in age or family history of CC between the high-awareness group and the low-awareness group. Statistically significant differences were found between the high-awareness group and the low-awareness group in terms of marital status, fertility status, per capita monthly household income, level of education, type of medical insurance, and CCS performed within three years. As shown in Table 2.
A binary logistic regression equation was fitted with high knowledge as the dependent variable (1=high knowledge, 0=low knowledge) and factors significant in the univariate analysis as the independent variables, and it was found that low per capita monthly household income, rural and urban health insurance, low literacy level, no CCS within three years, not being married, and having a child were the risk factors for low knowledge of CCS, as shown in Table 3 and Figure 1. As per capita monthly household income decreases, literacy decreases, and the risk of low awareness increases.
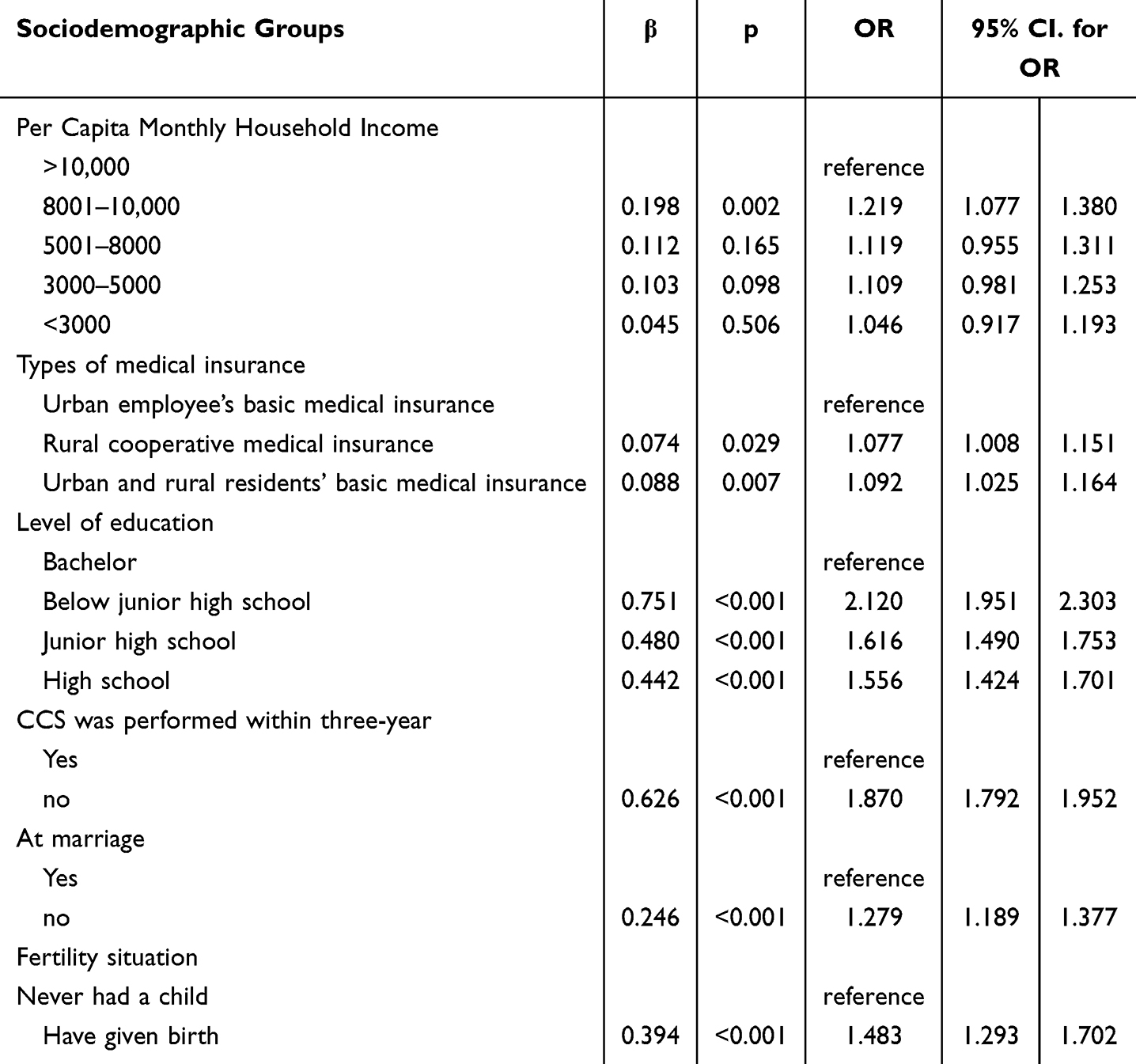 |
Table 3 Multivariable Logistic Regression of Low CCS Awareness Rate (N = 37,797) |
 |
Figure 1 Forest plot showing the low awareness of CCS. |
Recommending CCS
Of the survey respondents, 19,856 (52.53%) had received a CCS within three years. We separately investigated the extent to which women recommended CCSs to their surrounding relatives, friends, and colleagues. A ten-point scale of 0–10 was used. Larger scores indicated greater recommendation. The quadratic spacing for the total degree of recommendation score was [9(5,10)]. The Spearman correlation coefficient between the degree of recommendation and the knowledge score was 0.708 (p<0.01).
HPV Vaccination Survey
HPV Vaccine Awareness
The recommended age for HPV vaccination is younger than 45 years. In this study, 17,010 surveyed women under 45 years of age were surveyed about HPV vaccine awareness and vaccination. The Cronbach’s alpha coefficient was 0.736. Correlation coefficients between the total score and other items ranged from 0.490 to 0.767 (p<0.01). The test-retest reliability was 0.927. The mean score for knowledge of the HPV vaccine was 5.50 (SD ±1.27), and the high awareness rate was 48.33%. The Spearman correlation coefficient between the total CCS knowledge level and the HPV vaccine awareness score was 0.629 (p<0.01).
Using the HPV vaccine awareness score as the dependent variable and the potentially relevant factors as independent variables, a one-way analysis of variance was conducted, followed by a multifactor linear regression of meaningful variables using a stepwise method, and it was found that there was a linear relationship between age, CC prevention knowledge and HPV vaccine awareness score (F= 26537.766, p<0.001). The regression coefficient of age was 0.011, and that of CC prevention knowledge was 0.703. As shown in Table 4.
 |
Table 4 Analysis of Awareness of the HPV Vaccine (N = 17,010) |
HPV Vaccination Status
We surveyed women about their willingness to receive the HPV vaccine using a 0–10 ten-point scale. Larger scores indicate a greater willingness to be vaccinated. The median willingness to HPV vaccination was 7 (interquartile range, 3–10). Women’s CCS knowledge showed a partial mediating effect in the relationship between HPV vaccine knowledge and willingness to receive HPV vaccine, the mediating effect size was 21.16%.
A total of 5,364 (31.54%) women had been vaccinated with the HPV vaccine, including full vaccination and partial dose vaccination. Those who had been vaccinated had higher scores on HPV vaccine perceptions than those who had not been vaccinated (p<0.01), as shown in Figure 2.
 |
Figure 2 HPV vaccine awareness scores in the HPV vaccine and HPV unvaccinated groups. |
A survey of 387 women under 45 years of age who explicitly indicated that they were not willing to receive the HPV vaccine was conducted to investigate the reasons for the vaccine, and six common reasons were investigated in the form of multiple-choice questions. Multiple response analysis revealed that all the items were selected 607 times, of which 161 chose “the vaccine was too expensive” (26.52%), 126 chose “I am unlikely to be infected” (20.76%), 116 people were “worried about the side effects of the vaccine” (19.11%), 108 people felt that “it may not be effective” (17.79%), 68 because “the appointment and vaccination process takes too long” (11.20%), and 28 because “they are already infected with HPV” (4.61%), as shown in Figure 3.
 |
Figure 3 Distribution of reasons for refusal of the HPV vaccine. |
Discussion
This study explored Chinese women’s knowledge of CCS and HPV vaccines. The data from this study showed that among the women surveyed, 63.13% had a high knowledge of CCS. Low per capita monthly household income, no employee health insurance, low literacy, not having received CCS within 3 years, not being married, and having given birth were risk factors for low CCS knowledge. The recommended CCS and CC knowledge scores were highly positively correlated. The level of CCS awareness and HPV vaccination status were positively correlated. There was a linear relationship between age, CC prevention knowledge, and HPV vaccine awareness score. Women’s CCS knowledge showed a partial mediating effect in the relationship between HPV vaccine knowledge and willingness to receive HPV vaccine, the mediating effect size was 21.16%.
China’s first survey of rural women in different economic regions in 2013 found an overall awareness of CCS of only 19.5%,16 comparable to the findings of a study conducted in Nigeria at the time.21 In recent years, Fujian Province in China, where this study was conducted, has used government funding to provide free CCS to women while regularly promoting knowledge about CC prevention and treatment to the community through coloring pages, notice boards, short videos, official websites, and public telephone numbers. The survey examined the public’s knowledge of core health education on CC prevention and control and revealed that the knowledge rate was 63.13%, which was significantly greater than that in 2013. This suggests that continued investment in health education can help to raise public awareness.
Our data suggest that low per-capita household income, rural health insurance, urban health insurance, low literacy, not having received CCS within 3 years, not being married, and having given birth are associated with low knowledge of CCS. In China, a 2022 survey collected through a large e-commerce platform22 showed that women with a university degree or higher, a higher monthly household income, and living in an urban area tended to have a greater level of CCS knowledge, These characteristics were consistent with this research.
Data from the 2013 study also suggest that regional economic status also affects awareness.16 The 2022 survey22 and the present study did not analyze regional economic status but instead used a more precise monthly per capita household income, reducing bias. Both studies found that risk increased with decreasing monthly per capita income, providing more favorable evidence for the relationship between individual economic status and CC knowledge. Women with higher incomes were more likely to receive screening services. This may be because they are more knowledgeable about medical issues or because they have greater access to healthcare services.
Our results suggest that not having received CCS within 3 years is a risk factor for low knowledge of CCS. The reason for this is hypothesized to be related to the fact that the current healthcare facilities that offer CCSs tend to promote it at the time of registering women’s information, such as distributing paper materials on the spot, showing a short video, and having a dedicated person to talk about it. As a result, women receiving CCSs have a relatively good awareness rate.
Contrary to previous studies, we found that compared with urban workers’ basic medical insurance, in addition to rural cooperative medical insurance, urban and rural residents’ basic medical insurance is also a factor for low awareness of CCS. The government-funded NCCSP gives priority to rural women and poor urban women. In addition to free screening, women can also undergo CCS through employee medical check-ups and self-funded medical check-ups. However, for a considerable period in the past, unemployed women and housewives were not eligible for staff medical examinations and may have been unwilling to attend at their own expense, which objectively resulted in the worst knowledge.
Being unmarried and having children were also risk factors for lack of CCS knowledge. Currently, most of the CC health information available to people comes from gynecological outpatient clinics, and unmarried people have fewer chances to visit gynecological outpatient clinics. In the same way, women who have given birth and do not have any gynecological symptoms rarely take the initiative to go to the gynecological clinic for medical check-ups due to traditional attitudes. As a result, they have limited access to appropriate knowledge.
The present study revealed that 52.53% of all participating respondents had received a CCS. Under China’s NCCSP, every woman aged 35–64 years should receive free CCS every five years. By 2030, the actual number of people screened for CC should be at least 70% of the target population. This survey was conducted using a cross-sectional convenience sample, and therefore, a somewhat biased CCS rate may have been obtained. 2022 A survey in China based on a collection of large e-commerce platforms showed that the proportion of those who had received a CCS was 60%, which was slightly greater than that in this survey.22 The number of new cases of CC and associated mortality can be significantly reduced through organized, high-quality CCS.16 However, even if the country has a viable CCS program, the lack of knowledge and negative health-seeking behavior of the population can lead to the underutilization of such services.23 Consistent with the findings of the 2022 survey,22 we calculated the correlation coefficient to show that the degree of CCS recommendation and the CCS awareness score were highly positively correlated. CC is largely preventable with appropriate screening and follow-up, as precancerous lesions can be detected before they become invasive. A study in the United States showed24 that 60% of 367 women aged 21 years and older diagnosed with invasive CC had not been screened for CC. A lack of knowledge about CC is one factor that prevents women from being screened.25
HPV vaccines have reduced the incidence of CC in most developed countries.26 The difference between our study and previous studies is that we looked at both CCS and HPV vaccine awareness among women in an age group that receives the HPV vaccine. Among the women under 45 years of age surveyed in this study, the HPV vaccination rate was only 31.54%, and knowledge of the vaccine was significantly greater among vaccinated women than among unvaccinated women. HPV vaccine awareness increased with increasing age and knowledge of CCSs. Despite the low rate of HPV vaccination, we found that women’s median willingness to be vaccinated against HPV was as high as 7. A survey in western China a few years ago came to the same conclusion, with women’s willingness to be vaccinated against HPV being much greater than their knowledge of HPV.27 Therefore, future health interventions should move from willingness to practice. The China 2022 HPV vaccination willingness survey of female students in colleges and universities in Henan Province28 revealed that 92.8% indicated that they were willing to be vaccinated or advised that their friends and relatives be vaccinated. The willingness to receive HPV vaccination found in this survey was lower than that of college students, which is considered to be related to the included population; college students have relatively more ability and channels to access new media information and are more receptive.
Vaccine hesitancy, as defined by the WHO Strategic Advisory Group of Experts (SAGE), refers to delays in accepting or refusing vaccination despite the availability of vaccination services. Recent literature reports that ignorance about HPV infection, cervical cancer, and preventive measures is the main reason for low vaccination rates.29 Having identified the reasons for the hesitancy in HPV vaccination, the future government will be able to plan and implement effective programs to increase the uptake. We analyzed the reasons for not wanting to receive the HPV vaccine, of which the greatest reason was the price, followed by “I am unlikely to be infected”, “I am worried about the side effects of the vaccine”, “The vaccine may not be effective”, “The booking and vaccination process is too lengthy”, and “I am already infected with HPA”. A study of US college students reported that a brief educational intervention increased HPV knowledge assessment scores from 45% to 79%.30 A cross-sectional study of family doctor-contracted services (FDCSs) and CCS behaviors in Shenzhen, China, in 2020 showed that women who participated in FDCSs had higher levels of HPV-related knowledge than noncontracted women and had higher levels of past screening participation and willingness to be screened in the future, revealing the positive impact of FDCSs in guiding CC prevention.31 Evidence from the UK has shown that primary health care plays a key role in the prevention of CC, as healthcare providers discuss cancer risk with patients and promote risk reduction strategies.32 A community-based randomized controlled trial in Tanzania33 in 2020 showed that delegating the task of CCSs from healthcare professionals to community health workers and providing health education, counseling, and navigational assistance to women in the community, women in the intervention group had increased knowledge, awareness, intention to screen, and beliefs about their health during a 6-month follow-up period. Healthcare resource allocation varies from country to country, and studies with participants from different cultural backgrounds may affect the extrapolation of results. Since the gradual introduction of FDCSs in China in 2009, family doctors have played the role of gatekeepers in the primary healthcare system. The fact that CCS knowledge partially mediates HPV vaccine awareness and vaccine intention is a novel finding of our data. Therefore, it is recommended that HPV vaccine campaigns and CC control campaigns be held in parallel in the future.
From a public health perspective, several practices could be pursued. First, improve the professional skills of staff in medical institutions and vaccination centers. In China, HPV vaccination counseling is mainly provided by gynecologists and pediatricians, while vaccination is usually administered in community health centers. An effective way to overcome community reluctance is to equip healthcare workers with a thorough knowledge of the HPV vaccine so that they can fully understand the benefits and risks of vaccination and confidently recommend it to the public.30 China 2020’s first survey of healthcare workers in Shanghai, Guangzhou, and Shenzhen found better knowledge of HPV and the vaccine.34 A previous study found 78% of women wanted more information from their doctor about HPV.35 Recommendations from healthcare providers are the most important and consistent factor influencing community decision-making. In the future, it will be necessary first to provide uniform training for health workers throughout the country to improve their acceptance of CCS and HPV vaccines and then to standardize the content of health education provided by health workers to the community and improve their counseling skills. Where appropriate, health workers, in conjunction with community workers, will visit women’s homes to promote health education, conduct peer education, share typical cases, and encourage women to communicate regularly with them about health promotion activities, thus continuously expanding the scope of health education. Secondly, a targeted approach to publicity for different groups of people. For young women, personalized health education can be provided through new media, such as official media, WeChat, short videos, microfilms, etc., but should not be neglected for middle-aged and old-aged women in rural and urban families. In-depth and easy-to-understand health education content should be developed based on traditional media, and the publicity venues should be expanded from gynecological outpatient clinics and medical examination centers to health centers in rural areas, and the number of health education practitioners should be expanded from medical personnel to community workers. Third, the number of vaccination sites should be increased, the number of vaccines in stock at nearby sites should be announced regularly, and the vaccination process should be optimized to reduce barriers to HPV vaccination. Fourth, it is recommended that the government implement some preferential policies. In addition to continuing to provide free vaccination for school-age girls, partial free vaccination could be provided for low-income populations, which would help increase HPV vaccination coverage in these populations. Some Chinese cities have included HPV vaccination in their residents’ health insurance. Hospitals and government departments in other cities should consider gradually incorporating HPV vaccination into the health care system, which would help raise awareness and increase vaccination rates.
Advantage
This study has several strengths. First, it is one of the few surveys to report both CC prevention and HPV vaccine knowledge in a population covering free government cervical cancer screening, which contributes to the existing literature. Second, the sample size of the survey is large, and according to the composition of the population in the counties and districts, stratified cluster sampling was used, covering all counties and districts in Fujian Province, China, so it is representative of the population in China. Third, we set up a unified guideline through the “Questionnaire Star” platform, so the homogeneity is better; moreover, we set up a logical check of the questions and stipulated that the same mobile phone number can only submit the questionnaire once. This ensures the quality of the questionnaire.
Limitations
We acknowledge the limitations of this study. This study used a cross-sectional design. As such, inferring causal relationships between inferred variables may be limited. This study used convenience sampling, and therefore, the results may not be representative of the population studied. Recall bias may be present because the data were self-reported by the respondents. However, despite these limitations, the results of this study provide a basis for further updating the content and methods of health education, popularising primary prevention, and conducting intervention studies in the future.
Conclusion
We concluded that women’s knowledge of CCS was significantly greater than it was 10 years ago and that their awareness of the HPV vaccine was lower than that of CCS. There was a positive correlation between the level of CCS awareness and HPV vaccination status. In the future, there is a need to synchronize HPV vaccine campaigns with CC campaigns, develop more targeted health education programs, standardize the training of primary care providers on the content and skills of health education, to expand the delivery of health education from health care providers to community workers and to improve women’s access to and availability of services in health facilities. Shortly, this study will demonstrate other intervening factors that can contribute to the HPV vaccination program and the spread of CCS in China.
Abbreviations
CC, Cervical cancer; CCS, Cervical cancer screening; HPV, human papillomavirus; NCCSP, National Cervical Cancer Screening Program; NHC, National Health Commission.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Ethical Considerations
This study design and the content of the questionnaires were approved by the Human Subjects Ethics Committee of Fujian Maternity and Child Health Hospital College of Clinical Medicine for Obstetrics & Gynecology and Pediatrics. All participants provided written informed consent, which was documented in the records. Personal codes were assigned to all patients, and no personal information (personal identifiers) was obtained by the investigators at any time before, during, or after the study. All information about the study and participants’ rights was provided in the information letter provided to participants. The study was conducted following the principles of the Declaration of Helsinki.
Consent to Participate
All Participants Provided Consent for Participation.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Agency for Research on Cancer. Global cancer observatory: cancer today. Lyon, France: international agency for research on cancer. 2020. Available from: https://gco.iarc.fr/today/data/factsheets/cancers/23-Cervix-uteri-fact-sheet.pdf.
2. Arbyn M, Weiderpass E, Bruni L, et al. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020;8(2):e191–203. doi:10.1016/S2214-109X(19)30482-6
3. Duan R, Qiao Y, Clifford G, et al. Cancer burden attributable to human papillomavirus infection by sex, cancer site, age, and geographical area in China. Cancer Med. 2020;9(1):374–384. doi:10.1002/cam4.2697
4. Bouvard V, Wentzensen N, Mackie A. The IARC perspective on cervical cancer screening. N Engl J Med. 2021;385(20):1908–1918. doi:10.1056/NEJMsr2030640
5. World Health Organization. Global strategy to accelerate the elimination of cervical cancer. Available from: https://www.who.int/publications/i/item/9789240014107.
6. Chan CK, Aimagambetova G, Ukybassova T, et al. Human papillomavirus infection and cervical cancer: epidemiology, screening, and vaccination-review of current perspectives. J Oncol. 2019;2019:3257939. doi:10.1155/2019/3257939
7. Bedell SL, Goldstein LS, Goldstein AR, et al. Cervical cancer screening: past, present, and future. Sex Med Rev. 2020;8(1):28–37. doi:10.1016/j.sxmr.2019.09.005
8. Zhang X, Chen W, Zhu X, et al. Multiple center research on relationship between screening quality and detection of cervical cancer - six provinces, china, June-December 2021. China CDC Wkly. 2023;5(14):301–305. doi:10.46234/ccdcw2023.038
9. Musa J, Achenbach CJ, O’Dwyer LC, et al. Effect of cervical cancer education and provider recommendation for screening on screening rates: a systematic review and meta-analysis. PLoS One. 2017;12(9):e0183924. doi:10.1371/journal.pone.0183924
10. Devarapalli P, Labani S, Nagarjuna N, et al. Barriers affecting uptake of CCS in low and middle-income countries: a systematic review. Indian J Cancer. 2018;55(4):318–326. doi:10.4103/ijc.IJC_253_18
11. WHO. Comprehensive Cervical Cancer Control a Guide to Essential Practice. Geneva: WHO press; 2006.
12. Yanikkerem E, Goker A, Piro N, et al. Knowledge about cervical cancer, pap test, and barriers towards cervical screening of women in Turkey. J Cancer Educ. 2013;28(2):375–383. doi:10.1007/s13187-012-0409-1
13. Zhang M, Bao H, Wang L, et al. Analysis of cervical cancer screening and related factors in China. Natl Med J China. 2021;101(24):1869–1874.
14. Human papillomavirus (HPV) and cervical cancer[EB/OL]. (11 Nov 2020).
15. Markowitz LE, Naleway AL, Lewis RM, et al. Declines in HPV vaccine type prevalence in women screened for cervical cancer in the United States: evidence of direct and herd effects of vaccination. Vaccine. 2019;37(29):3918–3924. doi:10.1016/j.vaccine.2019.04.099
16. Di J, Shannon R, Jiuling W. Knowledge of cervical cancer screening among women across different socio-economic regions of China. PLoS One. 2015;10(12):e0144819. doi:10.1371/journal.pone.0144819
17. Bhatla N, Singhal S. Primary HPV Screening for Cervical Cancer. Best Pract Res Clin Obstet Gynaecol. 2020;65:98–108. doi:10.1016/j.bpobgyn.2020.02.008
18. Umbreen G, Rehman A, Avais M, et al. Knowledge, attitude, practice and barriers associated with influenza vaccination among health care professionals working at tertiary care hospitals in Lahore, Pakistan: a multicenter analytical cross-sectional study. Vaccines. 2023;11(1):136. doi:10.3390/vaccines11010136
19. Salman M, Mustafa ZU, Rao AZ, et al. Serious inadequacies in high alert medication-related knowledge among Pakistani nurses: findings of a large, multicenter, cross-sectional survey. Front Pharmacol. 2020;11:1026. doi:10.3389/fphar.2020.01026
20. Bari MS, Hossain MJ, Ahmmed F, et al. Perception, and willingness towards immunization among Bangladeshi population during COVID-19 vaccine rolling period. Vaccines. 2021;9(12):1449. doi:10.3390/vaccines9121449
21. Nwankwo K, Aniebue U, Aguwa E, Anarado AN, Agunwah E. Knowledge attitudes and practices of cervical cancer screening among urban and rural Nigerian women: a call for education and mass screening. European J Cancer Care. 2011;20(3):362–367. doi:10.1111/j.1365-2354.2009.01175.x
22. Zhang B, Wang S, Yang XK. Willingness, uptake and barriers of cervical cancer screening services among Chinese adult females: a national cross-sectional survey based on a large e-commerce platform. BMC Women's Health. 2023;23(1):435. doi:10.1186/s12905-023-02554-2
23. Ndikom CM, Ofi BA. Awareness, perception and factors affecting utilization of cervical cancer screening services among women in Ibadan, Nigeria: a qualitative study. Reprod Health. 2012;9(1):11. doi:10.1186/1742-4755-9-11
24. Benard Vicki B, Jackson JE, Greek A. A population study of screening history and diagnostic outcomes of women with invasive cervical cancer. Cancer Med. 2021;10(12):4127–4137. doi:10.1002/cam4.3951
25. Issa T, Babi A, Azizan A. Factors associated with cervical cancer screening behavior of women attending gynecological clinics in Kazakhstan: a cross-sectional study. Women's Health. 2021; 17(9):1–9. doi:10.1177/17455065211004135
26. Irino S, Ose H, Takata N, Kamoshida S, Ohsaki H. Barriers to undergoing cervical cancer screening among health sciences university students in Japan: a cross-sectional study. Nurs Health Sci. 2023;25(3):466–473. doi:10.1111/nhs.13043
27. He J, He L. Knowledge of HPV and acceptability of HPV vaccine among women in western China: a cross-sectional survey. BMC Women's Health. 2018;18(1):130. doi:10.1186/s12905-018-0619-8
28. Fengzhi Z, Manman L, Li X, et al. Knowledge of cervical cancer prevention and treatment, and willingness to receive HPV vaccination among college students in China. BMC Public Health. 2022;22(1):2269. doi:10.1186/s12889-022-14718-0
29. Prisha P, Tan KS, Lee CP. Malaysian women’s viewpoint on HPV screening and vaccination: a study on barriers. Vaccines. 2023;11(1):139. doi:10.3390/vaccines11010139
30. Lambert EC. College students’ knowledge of human papillomavirus and effectiveness of a brief educational intervention. J AM BOARD FAM PRACT. 2001;14(3):178–183.
31. Wei L, Weikang H, Chaofan M. Associations between the signing status of family doctor contract services and cervical cancer screening behaviors: a cross-sectional study in Shenzhen. China BMC Public Health. 2023;23(1):573. doi:10.1186/s12889-023-15462-9
32. Funston G, O’Flynn H, Ryan N, et al. Recognizing gynecological cancer in primary care: risk factors, red flags, and referrals. Adv Ther. 2018;35(4):577–589. doi:10.1007/s12325-018-0683-3
33. Mboineki JF, Wang P, Dhakal K, et al. The Effect of Peer-Led Navigation Approach as a Form of Task Shifting in Promoting Cervical Cancer Screening Knowledge, Intention, and Practices Among Urban Women in Tanzania: a Randomized Controlled Trial. CANCER CONTROL. 2022;29:10732748221089480. doi:10.1177/10732748221089480
34. Li J, Kang J, Mao Y, et al. Investigating HPV- and HPV Vaccine-Related Knowledge, Perceptions, and Information Sources among Health Care Providers in Three Big Cities in China. Vaccines. 2020;8(3).
35. Montgomery MP, Dune T, Shetty PK, et al. Knowledge and acceptability of human papillomavirus vaccination and cervical cancer screening among women in Karnataka, India. J CANCER EDUC. 2015;30(1):130–137. doi:10.1007/s13187-014-0745-4
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.