")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Association Between Lactate-to-Albumin Ratio and 28-Day All-Cause Mortality in Critical Care Patients with COPD: Can Both Arterial and Peripheral Venous Lactate Serve as Predictors?
Authors Zhao K, Zhou L, Ni Y, Tao J, Yu Z, Li X, Wang L
Received 29 October 2024
Accepted for publication 4 May 2025
Published 11 May 2025 Volume 2025:20 Pages 1419—1434
DOI https://doi.org/10.2147/COPD.S503625
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Kelan Zhao,1,* Linshui Zhou,1,* Yeling Ni,1 Jieying Tao,1 Ziyu Yu,1 Xiaojuan Li,2 Lu Wang1
1Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China; 2Department of Scientific Research, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiaojuan Li, Department of Scientific Research, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China, Email [email protected] Lu Wang, Department of Pulmonary and Critical Care Medicine, The First Affiliated Hospital of Zhejiang Chinese Medical University (Zhejiang Provincial Hospital of Chinese Medicine), Hangzhou, Zhejiang, People’s Republic of China, Email [email protected]
Background: Lactate-to-albumin ratio (LAR) has been reported as a useful predictor for multiple critical illnesses. However, the association between LAR and mortality in patients with chronic obstructive pulmonary disease (COPD) remains unclear. This study aims to clarify the correlation between LAR and 28-day all-cause mortality in patients with COPD and to investigate whether LAR calculated using arterial lactate (AL) or peripheral venous lactate (PVL) can serve as predictive indicators.
Methods: A total of 1428 patients from the Medical Information Mart for Intensive Care (MIMIC) IV database (version 2.2) and 2467 patients from the eICU Collaborative Research Database (eICU-CRD, version 2.0) were included in this study. Propensity score matching (PSM) method was conducted to control confounders. Cox proportional hazards model, Kaplan–Meier survival method, subgroup analysis and receiver operating characteristic (ROC) analysis were performed to assess the predictive ability of LAR. To verify our hypothesis, data from the two databases were analyzed individually.
Results: After adjusting for covariates, LAR calculated using either AL (MIMIC IV, HR = 1.254, 95% CI, 1.013– 1.552, P = 0.038) or PVL (eICU-CRD, HR = 1.442, 95% CI, 1.272– 1.634, P < 0.001) was independently associated with 28-day all-cause mortality in COPD patients. Kaplan–Meier analysis showed that patients with higher LAR value had significantly higher all-cause mortality (all P < 0.05). This association was consistent across subgroup analyses. In addition, the ROC analysis suggested that LAR calculated using PVL may have better predictive performance compared to using AL.
Conclusion: LAR calculated using both AL and PVL can independently predict the 28-day all-cause mortality after ICU admission in patients with COPD and higher level of LAR is related to higher mortality risk.
Keywords: chronic obstructive pulmonary disease, lactate-to-albumin ratio, all-cause mortality, 28-day, prognosis factors, cohort
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent respiratory disease characterized by persistent airflow limitation, typically progressive and associated with an enhanced chronic inflammatory response of the lung tissues to harmful particles or gases.1 Caused by exposure to inhaled noxious particles, notably tobacco smoke and pollutants,2 COPD has increasingly been regarded as a major cause of death worldwide with an estimated prevalence of more than 10% of the population aged 30–79 years in 2019 and 3.197 million deaths worldwide.3–5 Moreover, one study has demonstrated that patients with comorbid COPD have a higher 28-day mortality rate (13.90%) in intensive care unit (ICU) compared to those without COPD (8.07%).6 Thus, finding a useful indicator for prognostic evaluation is in urgent need.
Lactate was erroneously assumed to be a waste product of energy metabolism deleterious effects until 1980s.7 As a product of anaerobic metabolism, lactate itself can be used as an important indicator of tissue hypoperfusion as well as cellular hypoxia. With advances in research, however, evidence suggests that lactate plays important roles in many physiological and pathological processes, ranging from energy regulation, immune response, memory formation, wound healing to tumor progression.8 As a signalling molecule in inflamed tissues,9 lactate has been demonstrated to be associated with prognosis and mortality of varieties of diseases.10–12 Albumin, a traditional indicator for assessing malnutrition status and liver disease, has been confirmed to be a negative acute-phase protein in inflammatory response with the ability of binding a variety of inflammatory mediators and modulating oxidative stress.13,14 In addition, previous studies have reported that low levels of serum albumin are related to the mortality in COPD patients.15,16 Thus, lactate-to-albumin ratio (LAR) as a predictor of COPD patients’ prognosis, which investigate the ratio of inverse variations induced by distinct mechanisms, incorporates factors such as inflammation, tissue hypoperfusion and malnutrition status, may reduce potential biases in using a single predictor.
Several studies have shown that LAR is associated with mortality of critically ill patients, such as sepsis,17 acute pancreatitis,18 acute myocardial infarction,19 acute respiratory failure20 and so on. Previously, most of the relevant studies selected arterial blood lactate or did not mention the lactate sources, and one latest study21 focused on the relationship between LAR (with lactate from artery) and acute exacerbation of chronic obstructive pulmonary disease (AECOPD). While venous blood collection is safer and more convenient than arterial blood collection, this retrospective study aimed to investigate whether lactate-to-albumin ratio calculated using lactate from both sources is independent predictor of 28-day mortality in COPD patients. Therefore, we extracted data from the Medical Information Mart for Intensive Care IV (MIMIC-IV, version 2.2) containing arterial lactate (AL) and the eICU Collaborative Research Database (eICU-CRD, version 2.0) containing peripheral venous lactate (PVL) for analysis.
Methods
Data Sources
All data in this study were extracted from the Medical Information Mart for Intensive Care IV (MIMIC-IV, version 2.2) database and the eICU Collaborative Research Database (eICU-CRD, version 2.0).22,23 The MIMIC-IV database is a large online database, comprising data from patients admitted to the Beth Israel Deaconess Medical Center (BIDMC) from 2008 to 2019. The eICU-CRD database is a multi-center intensive care unit (ICU) database which contains over 200,000 admissions selected by eICU Programs across the United States between 2014 and 2015. The included patients’ health information was de-identified for protecting patients’ privacy. Therefore, informed consent was waived for this study. All data in this study were extracted by the first author (Kelan Zhao), who has completed the Collaborative Institutional Training Initiative (CITI) course and passed the online training (ID: 11773736).
Study Population
We extracted patients with COPD according to the International Classification of Diseases, Ninth Revision (ICD-9) and ICD-10 codes (code = 49120, 49121, 49122, 496, J44, J440, J441 and J449). Patients who were younger than 18 years old or spent less than 24 hours in ICU were excluded from this analysis. In cases of repeated ICU admissions, only the first admission for each patient was selected. After excluding participants with missing LAR data, comorbid severe liver diseases or admitted to hospital for liver diseases as main diagnosis, the final sample for analysis consisted of 3895 participants (1428 from MIMIC IV and 2467 from eICU-CRD) (Figure S1).
Data Extraction
PostgreSQL tool (version 15.3) was used to extract data from MIMIC-IV and eICU-CRD databases. The LAR was defined as lactate/albumin count and was chosen as the main study variable in this study. For AL from MIMIC-IV database, PVL from eICU-CRD database and serum albumin, only the initial examination results after admission were selected. We extracted the first record of demographic information [age, gender, ethnicity, body mass index (BMI)], vital signs [heart rate (HR), mean blood pressure (MBP), respiratory rate (RR), pulse oximetry-derived oxygen saturation (SpO2)], laboratory data [alanine aminotransferase (ALT), aspartate aminotransferase (AST), anion gap, bicarbonate, calcium, chloride, sodium, white blood cell (WBC), red blood cell (RBC), hemoglobin, platelet, hematocrit, creatinine, glucose, blood urea nitrogen (BUN)], comorbidity diseases (liver disease, congestive heart failure, diabetes, malignant cancer, myocardial infarction, renal disease), scoring systems [sequential organ failure assessment (SOFA), Oxford acute severity of illness score (OASIS) from MIMIC IV and acute physiology and chronic health evaluation IV score (APACHE IV) from eICU], as well as data on mechanical ventilation (MV) use after patients’ ICU admissions. The primary outcome was defined as 28-day all-cause mortality after ICU admission among COPD patients.
Management of Missing Data and Outliers
Variables with more than 15% values missing were excluded to reduce bias. For variables with less than 5% missing values, the missing data were imputed using the mean value. For variables with missing data proportions between 5% and 15%, multiple imputation methods were used to impute the missing values. In this study, covariates with abnormal values (above 99% or below 1%) were replaced with 99% or 1% of the point values using the “winsor2” command in STATA software (version 17.0).
Statistical Analysis
Continuous variables were assessed by the Kolmogorov–Smirnov test. Variables that followed a normal distribution were compared with the independent sample t-test and were reported as mean ± standard deviation. Skewed distributions were analyzed by the Kruskal–Wallis test and presented as median and interquartile range (IQR). Categorical variables were expressed as numbers (percentages) and were analyzed by the chi-square test. In addition, we determined the cut-off value of LAR using X-tile software (version 3.6.1) and used this value to divide the patients into high-LAR and low-LAR groups.
To reduce the bias and maintain the baseline balance between the low- and high-LAR groups, propensity score matching (PSM) was employed. We used a logistic regression model to calculate the propensity score and all the variables listed in Tables 1 or 2 were controlled in this model. The PSM was performed by 1:1 nearest-neighbor matching without replacement and a caliper width of 0.02.
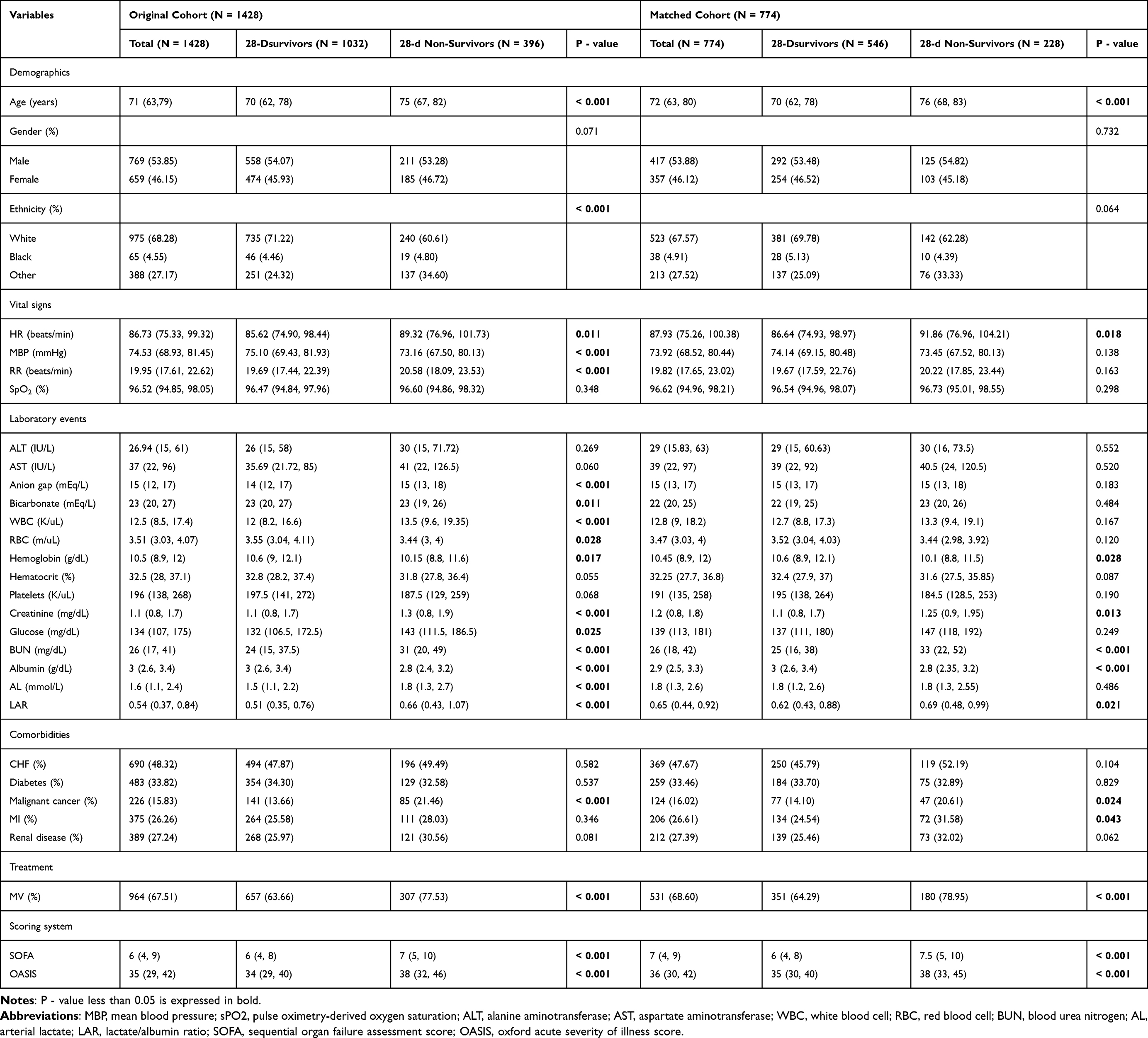 |
Table 1 Baseline Characteristics Between Survivors and Non-Survivors (MIMIC IV Database) |
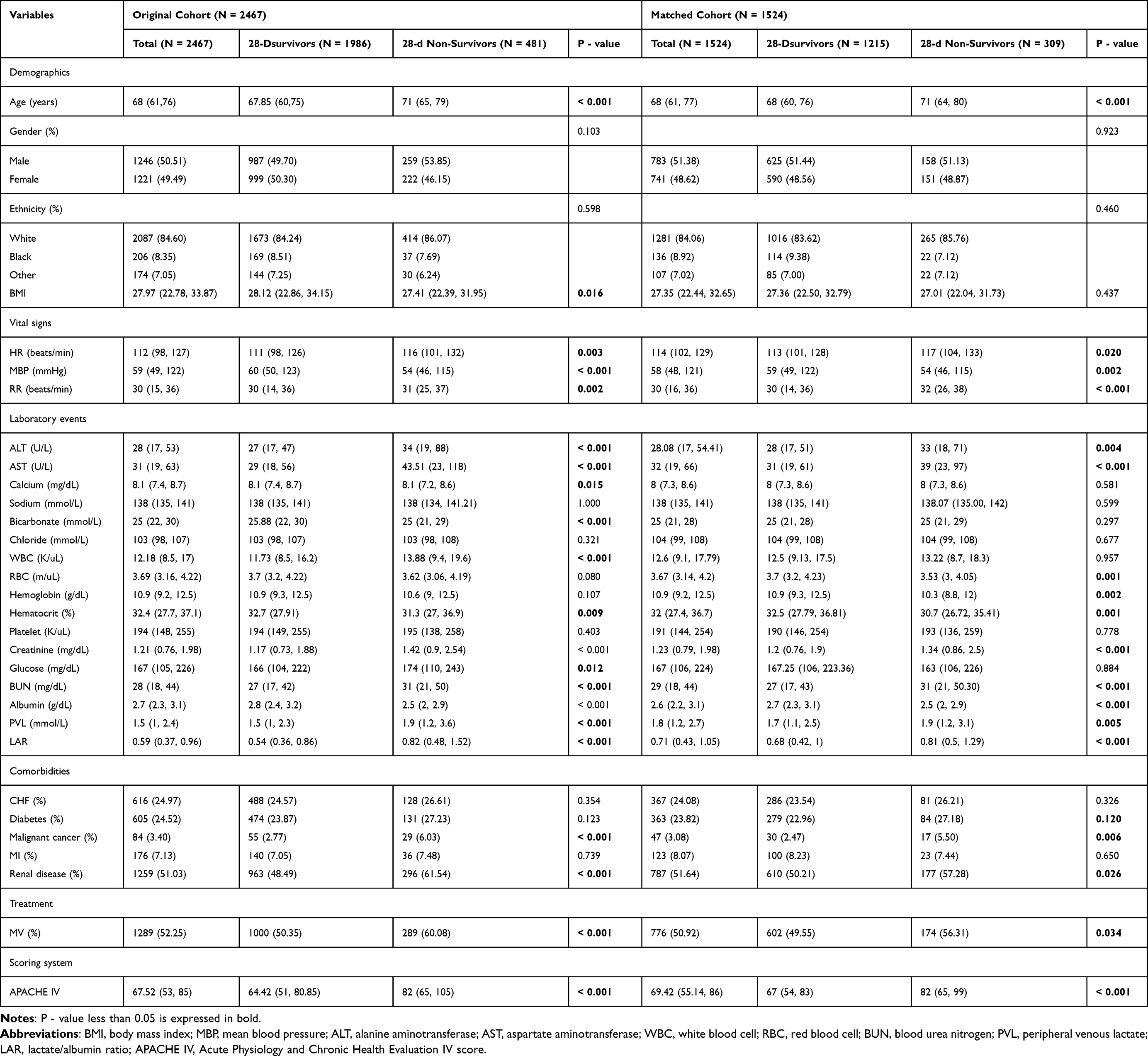 |
Table 2 Baseline Characteristics Between Survivors and Non-Survivors (eICU-CRD Database) |
Multivariate Cox regression models were performed in both original cohort and matched cohort to evaluate the relationship between LAR and 28-day mortality in COPD patients and the hazard ratio (HR) and 95% confidence interval (CI) were used. Kaplan–Meier curves and Log rank tests were performed in both original and matched cohort to describe the association between LAR and patients’ survival status. To guarantee the robustness of the findings, subgroup analysis with interaction effects was performed. The receiver operating characteristic (ROC) curve was used to compare the LAR calculated using AL and the LAR calculated using PVL for the 28-day mortality prediction. Further ROC analysis was conducted on subgroups subsequently.
To demonstrate that both LAR (using AL and PVL) can predict the mortality in COPD patients, analysis of two databases were performed individually.
All tests are double-sided in this study, and statistical significance was established as P < 0.05. SPSS software (version 22.0), STATA software (version 17.0), GraphPad Prism software (version 10.0), R software (version 2.15.3) and X-tile software (version 3.6.1) were used to do statistical analysis and produce figures.
Results
Baseline Characteristics
In this study, 1428 patients from MIMIC IV database and 2467 patients from eICU-CRD database were considered eligible for analysis according to the inclusion and exclusion criteria (Figure S1). The cut-off value of LAR was set at 0.65 in MIMIC IV database and 0.71 in eICU-CRD database according to the X-tile software (Figure 1). Consequently, participants were divided into high-LAR and low-LAR groups. After PSM (Figure 2), 774 patients from MIMIC IV database and 1524 patients from eICU-CRD database were selected. Baseline characteristics of the survival and non-survival groups were listed in Table 1 and Table 2.
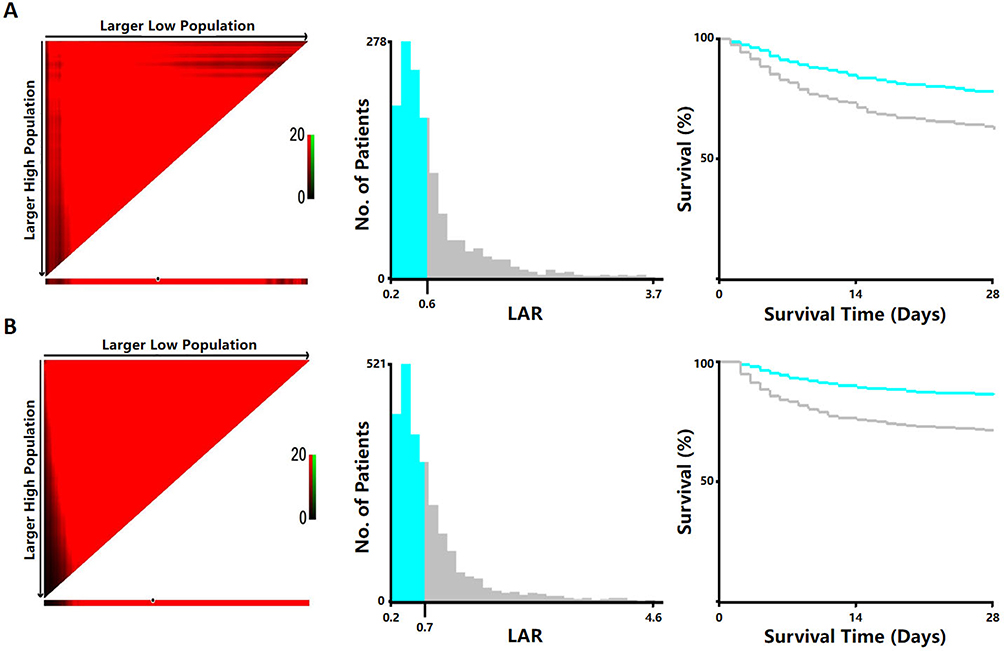 |
Figure 1 (A) Cut-off value of LAR for 28-day mortality in patients with COPD calculated using X-tile in MIMIC. (B) Cut-off value of LAR for 28-day mortality in patients with COPD calculated using X-tile in eICU. Abbreviation: LAR, lactate/albumin ratio. |
 |
Figure 2 (A) Standardized mean differences (SMD) between the original and matched cohorts in MIMIC. (B) Standardized mean differences (SMD) between the original and matched cohorts in eICU. Abbreviations: SOFA, sequential organ failure assessment; OASIS, Oxford acute severity of illness score; WBC, white blood cell; AST, aspartate aminotransferase; ALT, alanine aminotransferase; MV, mechanical ventilation; BUN, blood urea nitrogen; SpO2, pulse oximetry-derived oxygen saturation; MBP, mean blood pressure; RBC, red blood cell; APACHE IV, acute physiology and chronic health evaluation IV score; BMI, body mass index; PSM, propensity score matching. |
In MIMIC IV database, patients have a median age of 71 (range 29–91) and 53.85% of them were male, 68.28% of them were white. The 28-day all-cause mortality after ICU admission was 27.73%. The non-survivors had higher age, heart rate, respiratory rate, anion gap, WBC, creatinine, glucose, BUN, AL, LAR and lower mean blood pressure, bicarbonate, RBC, hemoglobin, albumin compared with the survivors (all P < 0.05). Compared to the survivors, non-survivors also exhibited higher incidence of comorbidities of malignant cancer, higher use of mechanical ventilation and higher severity scores including SOFA and OASIS (all P < 0.05). In eICU-CRD database, participants’ median age was 68 (range 24–89) and 50.51% of them were male, 84.60% of them were white. The 28-day mortality was 19.50%. The non-survivors had higher age, heart rate, respiratory rate, ALT, AST, WBC, creatinine, glucose, BUN, lactate, LAR, Apache IV score and had lower BMI, mean blood pressure, calcium, bicarbonate, hematocrit, albumin compared to the survivors (all P < 0.05). The non-survivors were more likely to suffer malignant cancer and renal disease and require mechanical ventilation (all P < 0.05).
LAR (Calculated Using AL) Was an Independent Prognostic Factor of 28-Day Mortality
Multivariate Cox models were used to estimate the correlation between LAR (calculated using AL) and outcomes of 28-day all-cause mortality in patients with COPD (Table 3). In the unadjusted Cox model, the LAR calculated using AL (before PSM: HR = 1.855, 95% CI, 1.523–2.259, P < 0.001; after PSM: HR = 1.337, 95% CI, 1.029–1.736, P = 0.030) was associated with 28-day mortality in patients with COPD. In Model 1, after adjusting for age, gender, ethnicity and vital signs, the LAR calculated using AL (before PSM: HR = 1.699, 95% CI, 1.391–2.075, P < 0.001; after PSM: HR = 1.357, 95% CI, 1.044–1.764, P = 0.023) remain significantly relating to the 28-day mortality. In Model 2, ALT, AST, anion gap, bicarbonate, WBC, RBC, hemoglobin, hematocrit, creatinine, glucose, BUN, MV and scoring systems were additionally adjusted on Model 1, showing that LAR calculated using either AL (before PSM: HR = 1.361, 95% CI, 1.092–1.697, P = 0.006; after PSM: HR = 1.358, 95% CI, 1.042–1.769, P = 0.024) is still significantly related to the 28-day mortality. In Model 3, comorbidities including congestive heart failure, diabetes, malignant cancer, myocardial infarction and renal disease were adjusted upon Model 2. According to this, LAR was still identified as an independent predictor of the 28-day mortality when calculated using AL (before PSM: HR = 1.354, 95% CI, 1.085–1.691, P = 0.007; after PSM: HR = 1.391, 95% CI, 1.066–1.815, P = 0.015).
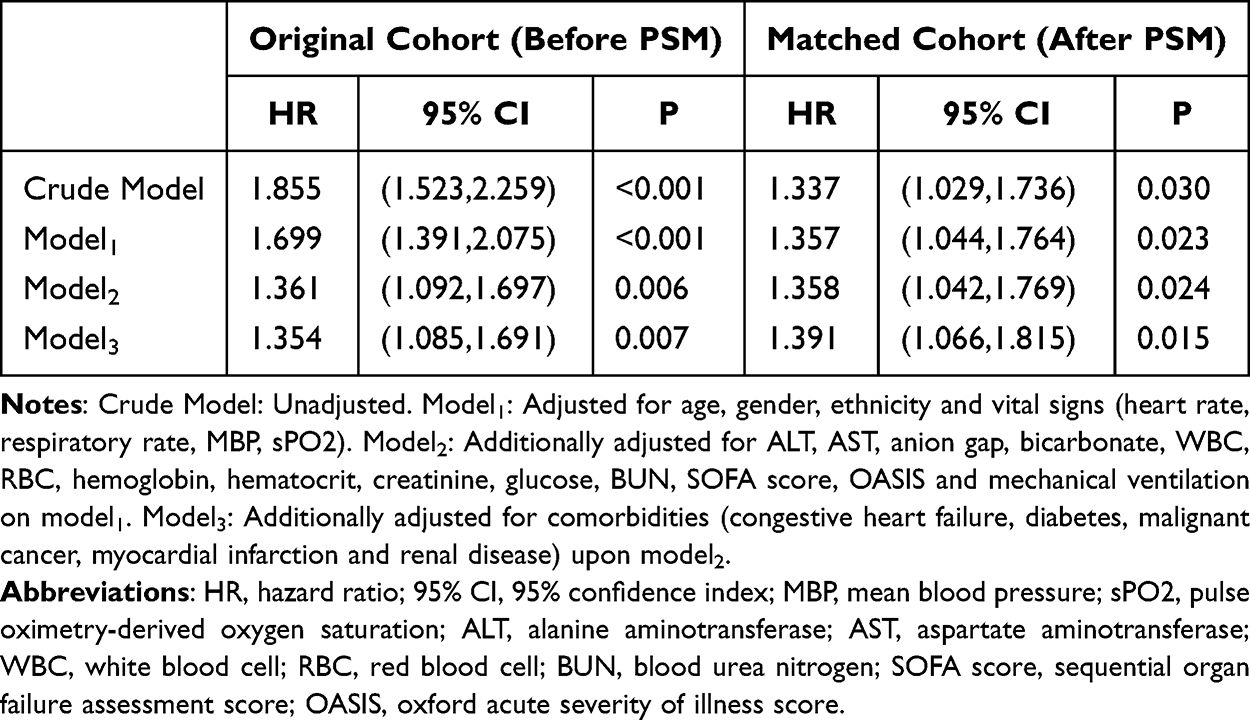 |
Table 3 Cox Regression Analysis of the Associations Between LAR (Calculated Using Arterial Lactate) and 28-Day Mortality (MIMIC IV) |
LAR (Calculated Using PVL) Was an Independent Prognostic Factor of 28-Day Mortality
Multivariate Cox models were performed to estimate the relationship between LAR (calculated using PVL) and outcomes of 28-day all-cause mortality in patients with COPD (Table 4). In the unadjusted Cox model, the LAR calculated using PVL (before PSM: HR = 2.383, 95% CI, 1.989–2.857, P < 0.001; after PSM: HR = 1.524, 95% CI, 1.215–1.913, P < 0.001) was associated with 28-day mortality of patients with COPD. In Model 1, after adjusting for age, gender, ethnicity and vital signs, the LAR (before PSM: HR = 2.280, 95% CI, 1.898–2.739, P < 0.001; after PSM: HR = 1.525, 95% CI, 1.215–1.914, P < 0.001) remain significantly relating to the 28-day mortality. In Model 2, ALT, AST, bicarbonate, WBC, RBC, hemoglobin, hematocrit, creatinine, glucose, BUN, MV and scoring system were additionally adjusted on Model 1, showing that the LAR calculated using PVL (before PSM: HR = 1.739, 95% CI, 1.429–2.117, P < 0.001; after PSM: HR = 1.579, 95% CI, 1.257–1.985, P < 0.001) is still significantly related to the 28-day mortality. In Model 3, comorbidities were adjusted upon Model 2. According to this, the LAR was still identified as an independent predictor of the 28-day mortality (before PSM: HR = 1.749, 95% CI, 1.436–2.130, P < 0.001; after PSM: HR = 1.576, 95% CI, 1.254–1.980, P < 0.001).
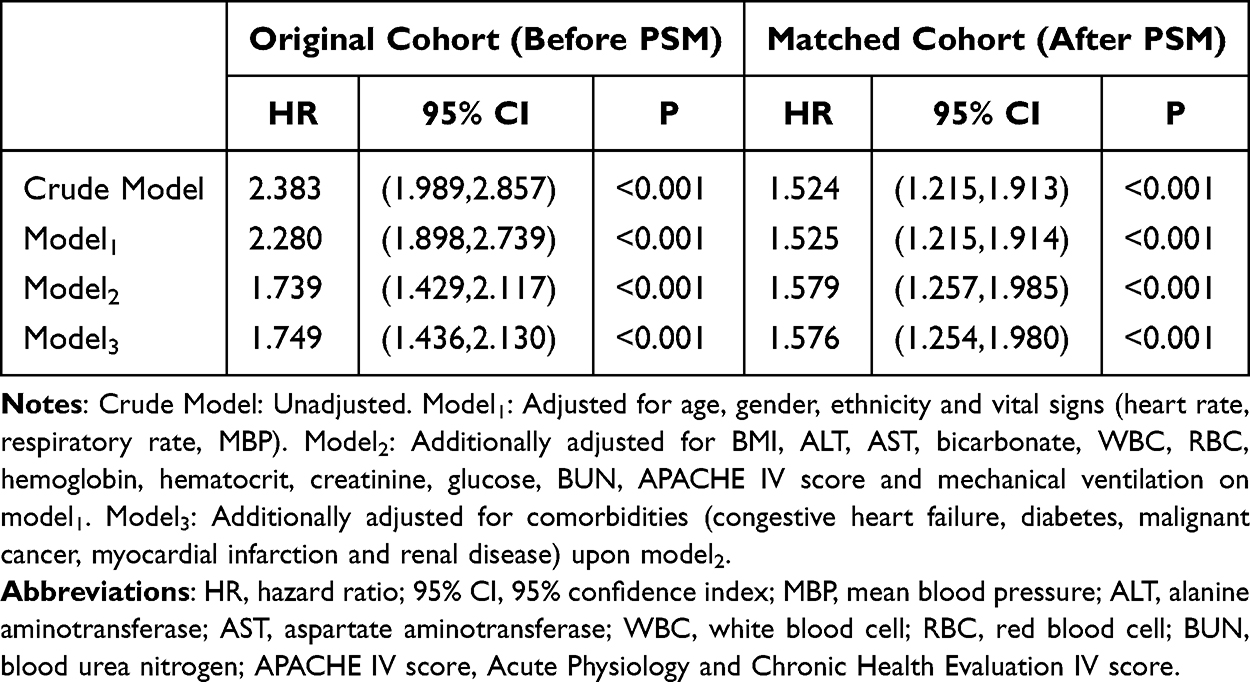 |
Table 4 Cox Regression Analysis of the Associations Between LAR (Calculated Using Peripheral Venous Lactate) and 28-Day Mortality (eICU-CRD) |
Survival Analysis
Kaplan–Meier survival method and Log rank test were deployed to compare the prognosis between high-LAR and low-LAR groups. Regardless of whether AL or PVL is used to calculate the LAR value, analyses showed that in the original cohorts, patients in the high LAR group had a significantly higher 28-day all-cause mortality than the low LAR group (P < 0.001, Figure 3A and B). Moreover, the survival curves of matched cohorts were consistent with the original cohorts (P < 0.05, Figure 3C and D).
 |
Figure 3 (A) Kaplan Meier curve of high and low LAR (calculated using arterial lactate) groups (MIMIC, before PSM, log-rank P < 0.001). (B) Kaplan Meier curve of high and low LAR (calculated using arterial lactate) groups (MIMIC, after PSM, log-rank P = 0.028). (C) Kaplan Meier curve of high and low LAR (calculated using peripheral venous lactate) groups (eICU, before PSM, log-rank P < 0.001). (D) Kaplan Meier curve of high and low LAR (calculated using peripheral venous lactate) groups (eICU, after PSM, log-rank P < 0.001). |
Subgroup Analysis
Subgroup analysis with interaction effects was carried out to indicate whether the correlation between LAR and 28-day all-cause mortality in patients with COPD was stable age, gender, ethnicity, common diseases and the use of mechanical ventilation were analyzed in Figures 4 and 5. The results showed no significant interaction with each subgroup (P for interaction: 0.289–0.884, LAR calculated using AL, MIMIC; 0.051–0.997, LAR calculated using PVL, eICU), evidencing that LAR is an independent prognostic factor.
 |
Figure 4 Forest plot for the subgroup analysis of the association between 28-d mortality and LAR (calculated using arterial lactate) using the MIMIC IV database. Abbreviations: HR, hazard ratio; 95% CI, 95% confidence index. |
 |
Figure 5 Forest plot for the subgroup analysis of the association between 28-d mortality and LAR (calculated using peripheral venous lactate) using the eICU-CRD database. Abbreviations: HR, hazard ratio; 95% CI, 95% confidence index. |
ROC Analysis
The ROC curve was constructed to evaluate the predictive ability of LAR, calculated separately using AL and PVL, for 28-day mortality after ICU admission in COPD patients (Figure S2). The area under curve (AUC) of the LAR calculated using PVL (AUC = 0.654, 95% CI, 0.625–0.683, P < 0.001) was larger than that of the LAR calculated using AL (AUC = 0.615, 95% CI, 0.583–0.647, P < 0.001). Subsequently, ROC analysis was performed in subgroups (Table S1), and the results suggested that LAR calculated using PVL may have better and more robust predictive performance for the 28-day mortality. Specifically, the subgroup of patients with combined diabetes (AUC = 0.698, 95% CI, 0.643–0.753, P < 0.001) or malignant cancer (AUC = 0.710, 95% CI, 0.589–0.831, P = 0.002) showed higher AUC values, indicating that LAR (calculated using PVL) might have greater predictive value in these two subgroups.
Discussion
As the third major cause of mortality worldwide, COPD has placed a substantial economic burden on societies globally.24 Thus, finding new prognostic indicators for prognostic evaluation is urgently needed. A previous study has reported that LAR is associated with 28-day mortality after ICU admission in patients with AECOPD.21 However, whether LAR calculated using either AL or PVL is an independent prognostic factor for the prognosis of patients with COPD remains unclear.
To our knowledge, this is the first study focusing on the relationship between LAR (using lactate from different sources) and the prognosis of COPD patients. The results of this study suggested that after balancing the baseline by PSM and adjusting the confounding factors using multiple COX regression analysis, LAR calculated using both AL and PVL are independent predictors of 28-day all-cause mortality in ICU patients with COPD. Kaplan–Meier curves showed that patients in high LAR group have a remarkably higher risk of 28-day mortality than those in low LAR group. In addition, subgroup analyses indicated that the relationships between LAR and 28-day mortality in different subgroups were all stable The results of the ROC analysis suggested that LAR, calculated using PVL, may have better and more robust predictive performance, especially in subgroups of patient with combined diabetes and malignant cancer.
Although the mechanism of predicting 28-day mortality in COPD patients by LAR is unclear, there are several possible explanations. Firstly, patients with COPD are more likely to suffer from hypoxemia and hypercapnia result from airflow limitation and gas exchange abnormalities.1 As a marker of anaerobic metabolism,25 the serum lactate level may increase consequently. Secondly, we infer that lung lactate is a major source of elevated systemic lactate levels in COPD patients, since pathological conditions enhance lung lactate release, and this release is linked to the severity of lung injury, as demonstrated in previous research.26 Additionally, this study suggested that lactate levels may be increased not only by the acceleration of anaerobic metabolism but also by cytokine effects on lung cells and elevated energy metabolism in both inflammatory and parenchymal cells within the lung. During inflammation, lactate can also trigger intracellular signals and promote chronic inflammatory processes.9 Thirdly, albumin is used to be considered as a negative acute-phase protein in inflammatory response.13 Thus, low serum albumin levels may reflect the increased persistent inflammation during acute exacerbation of COPD or the deterioration of clinical status.27 Fourthly, different COPD phenotypes have been found to be associated with nutritional status, including cachexia, frailty and obesity. In this context, serum albumin, as a marker of nutritional status, may be valuable for evaluating the condition of COPD patients.28 Moreover, previous studies suggested that serum albumin is good to be used to evaluate the severity of disease.29 In conclusion, the two indicators are influenced by a complex array of factors. For instance, patients with sepsis, liver dysfunction or diabetic ketoacidosis may exhibit abnormalities in lactate metabolism; the use of certain medications, such as β2 -agonists and metformin, can also lead to alterations in lactate levels.10,30 Similarly, comorbid liver diseases also can alter albumin levels.13 Therefore, after excluding patients with severe liver disease in our study, using the ratio between blood lactate and serum albumin provides a more reliable approach for predicting the prognosis of COPD patients. However, the exact mechanism still needs to be clarified in the future.
Previous studies have demonstrated that, although PVL and AL levels are not in perfect agreement, the PVL levels are highly predictive of AL levels.31,32 With a generally higher level than AL, PVL has been proved to be a predictor for assessing initial severity of sepsis and is even more reliable than AL.33 Additionally, pH and HCO3− values from arterial and venous blood show good agreement, making venous blood gas analysis a useful tool for the initial assessment of COPD exacerbation.34 The results of this study has also demonstrated that LAR calculated using PVL has a better predictive ability for 28-day mortality COPD patients, particularly in patients with comorbid diabetes or malignant cancer. Thus, since arterial blood gas sampling is invasive, painful, and risky, venous blood gas analysis seems to be a good alternative.
There are some limitations to our study. Firstly, our study is based on two clinical centers, and we did analysis individually for there is only one source lactate data from each database. As a result, the comparison of the predictive ability of LAR, calculated using AL and PVL, is limited. Secondly, despite excluding patients with severe liver diseases and performing PSM to minimize the differences, there are still some unmeasured confounders affecting this study, such as PaO2 and PaCO2 (because of more than 15% missing values). Thirdly, the population data collection period for the database used in this study spans from 2008 to 2019. With the evolution of medical knowledge and the enhancement of clinical protocols, we cannot assure whether potential differences in clinical management may introduce bias to the study. To avoid those limitations of retrospective study, future research should focus on developing multivariable prediction models that incorporate LAR along with other clinical and laboratory parameters to enhance predictive accuracy.
Conclusion
In conclusion, the present study indicated that LAR calculated using both AL and PVL are independent predictors of 28-day mortality in COPD patients, and a higher LAR value (>0.65 using lactate from artery, >0.71 using lactate from peripheral vein) was associated with a higher mortality risk. Our findings suggest that LAR calculated using PVL demonstrates superior predictive ability for the mortality compared with LAR calculated using AL. Nevertheless, further prospective studies are needed to confirm the predictive value of LAR (calculated using AL and PVL) and support its use in clinical practice.
Data Sharing Statement
The original datasets presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding authors.
Ethics Statement
This study was approved by the institutional review boards of the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center. As all data used in this study were anonymized, the Ethics Committee of the First Affiliated Hospital of Zhejiang Chinese Medical University provided ethics approval of this work (2024-KL-416-01).
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We are grateful to the MIMIV-IV and eICU-CRD participants and staff. We appreciate all the reviewers who participated in the review.
Author Contributions
All authors made significant contributions to the work reported, including conception, study design, execution, data acquisition, analysis, and interpretation. They participated in drafting, revising, or critically reviewing the manuscript. All authors approved the final version for publication, agreed on the journal for submission, and take responsibility for all aspects of the work.
Funding
The study was funded by the Student Scientific Research Fund Project of Zhejiang Chinese Medical University in 2024 (Project No. 06) and the Zhejiang Province Traditional Chinese Medicine Science and Technology Plan Project (Project No. 2023ZR020).
Disclosure
Miss Kelan Zhao reports grants from the Student Scientific Research Fund Project of Zhejiang Chinese Medical University in 2024, during the conduct of the study. Dr Lu Wang reports grants from the Zhejiang Province Traditional Chinese Medicine Science and Technology Plan Project, during the conduct of the study. The authors declare that they have no conflicts of interest.
References
1. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
2. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
3. Mei F, Dalmartello M, Bonifazi M, et al. Chronic obstructive pulmonary disease (COPD) mortality trends worldwide: an update to 2019. Respirology. 2022;27(11):941–950. doi:10.1111/resp.14328
4. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
5. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi:10.1371/journal.pmed.0030442
6. Huang W, Xie R, Hong Y, Chen Q. Association between comorbid chronic obstructive pulmonary disease and prognosis of patients admitted to the intensive care unit for non-COPD reasons: a retrospective cohort study. Int J Chron Obstruct Pulmon Dis. 2020;15:279–287. doi:10.2147/COPD.S244020
7. Ferguson BS, Rogatzki MJ, Goodwin ML, Kane DA, Rightmire Z, Gladden LB. Lactate metabolism: historical context, prior misinterpretations, and current understanding. Eur J Appl Physiol. 2018;118(4):691–728. doi:10.1007/s00421-017-3795-6
8. Certo M, Tsai CH, Pucino V, Ho PC, Mauro C. Lactate modulation of immune responses in inflammatory versus tumour microenvironments. Nat Rev Immunol. 2021;21(3):151–161. doi:10.1038/s41577-020-0406-2
9. Li X, Yang Y, Zhang B, et al. Lactate metabolism in human health and disease. Signal Transduct Target Ther. 2022;7(1):305. doi:10.1038/s41392-022-01151-3
10. MacDonald MI, Polkinghorne KR, MacDonald CJ, et al. Elevated blood lactate in COPD exacerbations associates with adverse clinical outcomes and signals excessive treatment with β2 -agonists. Respirology. 2023;28(9):860–868. doi:10.1111/resp.14534
11. Vincent JL, Quintairos E, Silva A, Couto LJ, Taccone FS. The value of blood lactate kinetics in critically ill patients: a systematic review. Crit Care. 2016;20(1):257. doi:10.1186/s13054-016-1403-5
12. Haas SA, Lange T, Saugel B, et al. Severe hyperlactatemia, lactate clearance and mortality in unselected critically ill patients. Intensive Care Med. 2016;42(2):202–210. doi:10.1007/s00134-015-4127-0
13. Ward ES, Gelinas D, Dreesen E, et al. Clinical significance of serum albumin and implications of fcrn inhibitor treatment in igg-mediated autoimmune disorders. Front Immunol. 2022;13:892534. doi:10.3389/fimmu.2022.892534
14. Artigas A, Wernerman J, Arroyo V, Vincent JL, Levy M. Role of albumin in diseases associated with severe systemic inflammation: pathophysiologic and clinical evidence in sepsis and in decompensated cirrhosis. J Crit Care. 2016;33:62–70. doi:10.1016/j.jcrc.2015.12.019
15. Pellicori P, McConnachie A, Carlin C, Wales A, Cleland JGF. Predicting mortality after hospitalisation for COPD using electronic health records. Pharmacol Res. 2022;179:106199. doi:10.1016/j.phrs.2022.106199
16. Connars AF, Dawson NV, Thomas C, et al. Outcomes following acute exacerbation of severe chronic obstructive lung disease. The SUPPORT investigators (study to understand prognoses and preferences for outcomes and risks of treatments). Am J Respir Crit Care Med. 1996;154(4 Pt 1):959–967. doi:10.1164/ajrccm.154.4.8887592
17. Shadvar K, Nader-Djalal N, Vahed N, et al. Comparison of lactate/albumin ratio to lactate and lactate clearance for predicting outcomes in patients with septic shock admitted to intensive care unit: an observational study. Sci Rep. 2022;12(1):13047. doi:10.1038/s41598-022-14764-z
18. Liu Q, Zheng HL, Wu MM, et al. Association between lactate-to-albumin ratio and 28-days all-cause mortality in patients with acute pancreatitis: a retrospective analysis of the MIMIC-IV database. Front Immunol. 2022;13:1076121. doi:10.3389/fimmu.2022.1076121
19. Chen Y, Lai W, Yang K, Wu B, Xie D, Peng C. Association between lactate/albumin ratio and prognosis in patients with acute myocardial infarction. Eur J Clin Invest. 2024;54(1):e14094. doi:10.1111/eci.14094
20. Lu Y, Guo H, Chen X, Zhang Q. Association between lactate/albumin ratio and all-cause mortality in patients with acute respiratory failure: a retrospective analysis. PLoS One. 2021;16(8):e0255744. doi:10.1371/journal.pone.0255744
21. Xie J, Liu H, He Q, Li C. Relationship between lactate-to-albumin ratio and 28-day mortality in patients with exacerbation of chronic obstructive pulmonary disease admitted to the intensive care unit. Eur J Med Res. 2024;29(1):258. doi:10.1186/s40001-024-01867-8
22. Johnson AEW, Bulgarelli L, Shen L, et al. MIMIC-IV, a freely accessible electronic health record dataset. Sci Data. 2023;10(1):1. doi:10.1038/s41597-022-01899-x
23. Pollard TJ, Johnson AEW, Raffa JD, Celi LA, Mark RG, Badawi O. The eICU collaborative research database, a freely available multi-center database for critical care research. Sci Data. 2018;5(1):180178. doi:10.1038/sdata.2018.178
24. Chen S, Kuhn M, Prettner K, et al. The global economic burden of chronic obstructive pulmonary disease for 204 countries and territories in 2020-50: a health-augmented macroeconomic modelling study. Lancet Glob Health. 2023;11(8):e1183–e1193. doi:10.1016/S2214-109X(23)00217-6
25. Janotka M, Ostadal P. Biochemical markers for clinical monitoring of tissue perfusion. mol Cell Biochem. 2021;476(3):1313–1326. doi:10.1007/s11010-020-04019-8
26. Iscra F, Gullo A, Biolo G. Bench-to-bedside review: lactate and the lung. Crit Care. 2002;6(4):327–329. doi:10.1186/cc1519
27. Gunen H, Hacievliyagil SS, Kosar F, et al. Factors affecting survival of hospitalised patients with COPD. Eur Respir J. 2005;26(2):234–241. doi:10.1183/09031936.05.00024804
28. Beijers RJHCG, Steiner MC, Schols AMWJ. The role of diet and nutrition in the management of COPD. Eur Respir Rev. 2023;32(168):230003. doi:10.1183/16000617.0003-2023
29. Bretschera C, Boesiger F, Kaegi-Braun N, et al. Admission serum albumin concentrations and response to nutritional therapy in hospitalised patients at malnutrition risk: secondary analysis of a randomised clinical trial. EClinicalMedicine. 2022;45:101301. doi:10.1016/j.eclinm.2022.101301
30. Andersen LW, Mackenhauer J, Roberts JC, Berg KM, Cocchi MN, Donnino MW. Etiology and therapeutic approach to elevated lactate levels. Mayo Clin Proc. 2013;88(10):1127–1140. doi:10.1016/j.mayocp.2013.06.012
31. Oi Y, Mori K, Yamagata H, et al. Peripheral venous lactate levels substitute arterial lactate levels in the emergency department. Int J Emerg Med. 2022;15(1):7. doi:10.1186/s12245-022-00410-y
32. Van Tienhoven AJ, Van Beers CAJ, Siegert CEH. Agreement between arterial and peripheral venous lactate levels in the ED: a systematic review. Am J Emerg Med. 2019;37(4):746–750. doi:10.1016/j.ajem.2019.01.034
33. Contenti J, Corraze H, Lemoël F, Levraut J. Effectiveness of arterial, venous, and capillary blood lactate as a sepsis triage tool in ED patients. Am J Emerg Med. 2015;33(2):167–172. doi:10.1016/j.ajem.2014.11.003
34. McKeever TM, Hearson G, Housley G, et al. Using venous blood gas analysis in the assessment of COPD exacerbations: a prospective cohort study. Thorax. 2016;71(3):210–215. doi:10.1136/thoraxjnl-2015-207573
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Prognostic Performance of Lung Diffusing Capacity in Preserved Ratio Impaired Spirometry: An Observational Cohort Study
Ogata H, Sha K, Kotetsu Y, Enokizu-Ogawa A, Katahira K, Ishimatsu A, Taguchi K, Moriwaki A, Yoshida M
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2791-2799
Published Date: 28 October 2022
Association Between Blood Urea Nitrogen to Serum Albumin Ratio and Mortality in Critically Ill Patients With Chronic Obstructive Pulmonary Disease: A Retrospective Study
Li J, Peng J, Cheng C, Zhang J, Li L
International Journal of Chronic Obstructive Pulmonary Disease 2025, 20:349-360
Published Date: 17 February 2025