")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 17
Association Between Nonalcoholic Fatty Liver Disease and the Risk of Cardiovascular Disease in the Middle-Age and Elderly Population of Northern China: A Cross-Sectional Study
Authors Zhang X, Wang L, Wang G , Li J, Mu Y , Wang S , Li X
Received 19 June 2024
Accepted for publication 13 August 2024
Published 21 August 2024 Volume 2024:17 Pages 3079—3085
DOI https://doi.org/10.2147/DMSO.S474912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Konstantinos Tziomalos
Xuebing Zhang,1 Lianjie Wang,1 Ge Wang,1 Jiayue Li,1 Yiming Mu,2 Shidong Wang,1 Xiaoran Li1
1Department of Endocrinology, Dongzhimen Hospital Beijing University of Chinese Medicine, Beijing 100700, People’s Republic of China; 2Department of Endocrinology, First Medical Centre of Chinese PLA General Hospital, Beijing 100853, People’s Republic of China
Correspondence: Shidong Wang; Xiaoran Li, Email [email protected]; [email protected]
Background: Nonalcoholic fatty liver disease (NAFLD) has become a major global health burden, which increases the risk of extra-hepatic complications such as type 2 diabetes mellitus (T2DM), dyslipidemia, metabolic syndrome (MetS), and cardiovascular disease (CVD). However, NAFLD remains underappreciated and underdiagnosed. Our study aimed to explore the prevalence of NAFLD and the association between NAFLD and CVD events among adults aged 40 and older in Northern China.
Methods: This study was conducted in the Shijingshan district of Beijing, China from November 2011 to August 2012. A total of 18891 subjects were recruited in the study. The information including demographical information, lifestyle, previous history of diabetes, hypertension, dyslipidemia, CVD, and liver disease were gathered. Data on physical examination, blood lipid profile, fasting blood glucose, and 2-hour blood glucose were recorded. Determination of MetS was according to T2DM guideline of Chinese Diabetes Society (2020 edition). The association between CVD and NAFLD was evaluated by multivariate logistic regression.
Results: The prevalence of NAFLD was 15.2%. After adjustment for age, smoking status, alcohol intake, WC, hypertension, dyslipidemia and hyperglycemia, the odds ratios (ORs) of CVD in men were 1.622 (95%CI: 1.345– 1.957) and 1.990 (95%CI: 1.709– 2.316) in women with NAFLD, compared with the subjects without NAFLD.
Conclusions: NAFLD is independently associated with increased risk of CVD development.
Keywords: nonalcoholic fatty liver disease, metabolic syndrome, cardiovascular disease, middle-aged and elderly, Chinese
Introduction
Up to 2021, nonalcoholic fatty liver disease (NAFLD) has become a major global health burden, affecting 32.4% of adult population worldwide.1 According to Chinese surveillance data in 2018, the prevalence of NAFLD was 29.2% in China.2 NAFLD is characterized by the accumulation of more than 5% fat in liver, which is the most common chronic liver disease and encompasses a large spectrum of diseases from simple liver steatosis to cirrhosis.3 Increasing evidence suggests that NAFLD is not only a progressive liver disease, but also a multisystem disorder as it increases the risk of extra-hepatic complications such as type 2 diabetes mellitus (T2DM), dyslipidemia metabolic syndrome (MetS), and cardiovascular disease (CVD).4–6 NAFLD is strongly associated with characteristics of MetS and is considered as a liver manifestation of MetS.7 In addition, it has been confirmed that CVD is the leading cause of death among the subjects with NAFLD.8 NAFLD and CVD share similar risk factors such as T2DM, dyslipidemia and obesity.9 However, NAFLD is not a bystander during the development of CVD and it has been found to be a vital risk factor independent of other traditional risk factors for CVD.10 Some meta-analyses have been conducted to conform the strong association between NAFLD and CVD.11–14 Multiple pathophysiological mechanisms Linking NAFLD with CVD co-exist in both diseases, such as insulin resistance, systemic low-grade inflammation, endothelial dysfunction, increased oxidative stress and an atherogenic lipoprotein profile, which may elucidate the relationship between NAFLD and CVD.15 Several Chinese studies have shown that NAFLD remained as an independent risk factor for CVD even after adjusting for demographic and metabolic factors.16–18 However, NAFLD as a very important CVD risk factor remains underappreciated and underdiagnosed. In this regard, increasing awareness of adverse cardiovascular outcomes of NAFLD among Cardiologists may help to decrease the huge burden of metabolic-associated diseases. Our recently published study shown that waist-height-ratio (WHtR) and waist-hip-ratio (WHR) were the most powerful anthropometric indices for predicting T2DM in middle-aged and elderly Chinese men and women respectively,19 which could better reflect the accumulation of abdominal fat. The above two parameters had some advantages, such as non-invasive, simple, convenient and economical. However, WHtR and WHR couldn’t distinguish between visceral fat and subcutaneous fat. NAFLD, defined as excess adipose tissue deposition in the liver, represents visceral fat accumulation. Visceral adiposity correlates more closely to metabolic disorders. Therefore, we conducted this survey in order to explore the prevalence of NAFLD and the association between NAFLD and CVD events among adults aged 40 and older on a large scale in Northern China.
Methods
Study Population
This study was a cross-sectional survey and used a cluster sampling method, which was conducted in the Shijingshan district of Beijing, China from November 2011 to August 2012. The detailed procedures and exclusion standards were described in the previous publication.20 At last, a total of 19,274 residents aged 40 and older from three urban communities in the Shijingshan district signed the informed consent before the investigation. We excluded the subjects with incomplete demographic information, no availability of fasting blood glucose or 2-hour blood glucose (n = 129). In addition, the participants with excessive alcohol intake (>80 g/d; n = 36), a history of virus hepatitis, liver carcinoma, liver cirrhosis, autoimmune liver disease, hyperthyroidism, hypothyroidism or schistosomiasis were also excluded (n=218). Finally, a total of 18891 subjects were recruited in the study. Our study was approved by the Chinese PLA General Hospital Ethics Committee (NO.EC2012-046).
Clinical Data and Biochemical Indicators
We collected clinical data including demographical information, lifestyle, previous history of diabetes, hypertension and dyslipidemia according to a standard questionnaire through face-to-face interviews by unified trained physicians in advance. Methods of physical examination, tests of biochemical indicators, and performance of 75 g OGTT or standard meal test were already described in detail in a previous publication.19
Metabolic syndrome (MetS) was defined as the presence of at least three of the following metabolic abnormalities: WC≥90cm and ≥85cm in Chinese men and women, respectively; fasting blood glucose ≥6.1 mmol/L or 2-hour blood glucose ≥7.8 mmol/L or already taking antidiabetic agents; systolic blood pressure ≥130mmHg and/or diastolic blood pressure ≥85mmHg or taking antihypertensive medicine; fasting TG level ≥1.7 mmo1/L; fasting HDL-C level <1.04 mmol/L.21 Determination of CVD, fatty liver disease was based on the participants’ self-report. CVD encompassed coronary heart disease (CHD) and stroke. Smoking was defined as smoking one or more cigarettes daily for at least a half year. Regular drinking was defined as at least once a week for a half year.
Statistical Analysis
Statistical analysis was performed on SPSS software version 16.0 (SPSS Inc., USA). Variables were presented as means ± standard deviation (SD), median (interquartile ranges), or n (%). Means of continuous variables were compared using t test. The percentage difference between groups was compared using χ2 test. Multivariate Logistic regression was used to evaluate the association between CVD and NAFLD. The 2-tailed test was used, and P <0.05 was regarded as statistically significant.
Results
A total of 6,605 men (NAFLD 1,102; non-NAFLD 5503) and 12,286 (NAFLD 1769; nod-NAFLD 10,517) women were included in this study. The prevalence of NAFLD was 15.2% in the total population, 16.7% in men and 14.4% in women. The prevalence of NAFLD was higher in men than that in women (p<0.001). The prevalence of metabolic syndrome was 52.9% among the subjects with NAFLD and 29.4% among those without NAFLD (p<0.001).The prevalence of CVD was 18.4% in the NAFLD population and 9.7% in the non-NAFLD population (p<0.001).The average values of BMI, WC, WHR, WHtR, SBP, DBP and serum T-CHO, TG, HDL-C, LDL-C, FPG, PG2h, HbA1c levels were significantly higher in the subjects with NAFLD than those without NAFLD. On the contrary, serum HDL-C level was significantly lower among NAFLD participants than those without NAFLD (Tables 1 and 2).
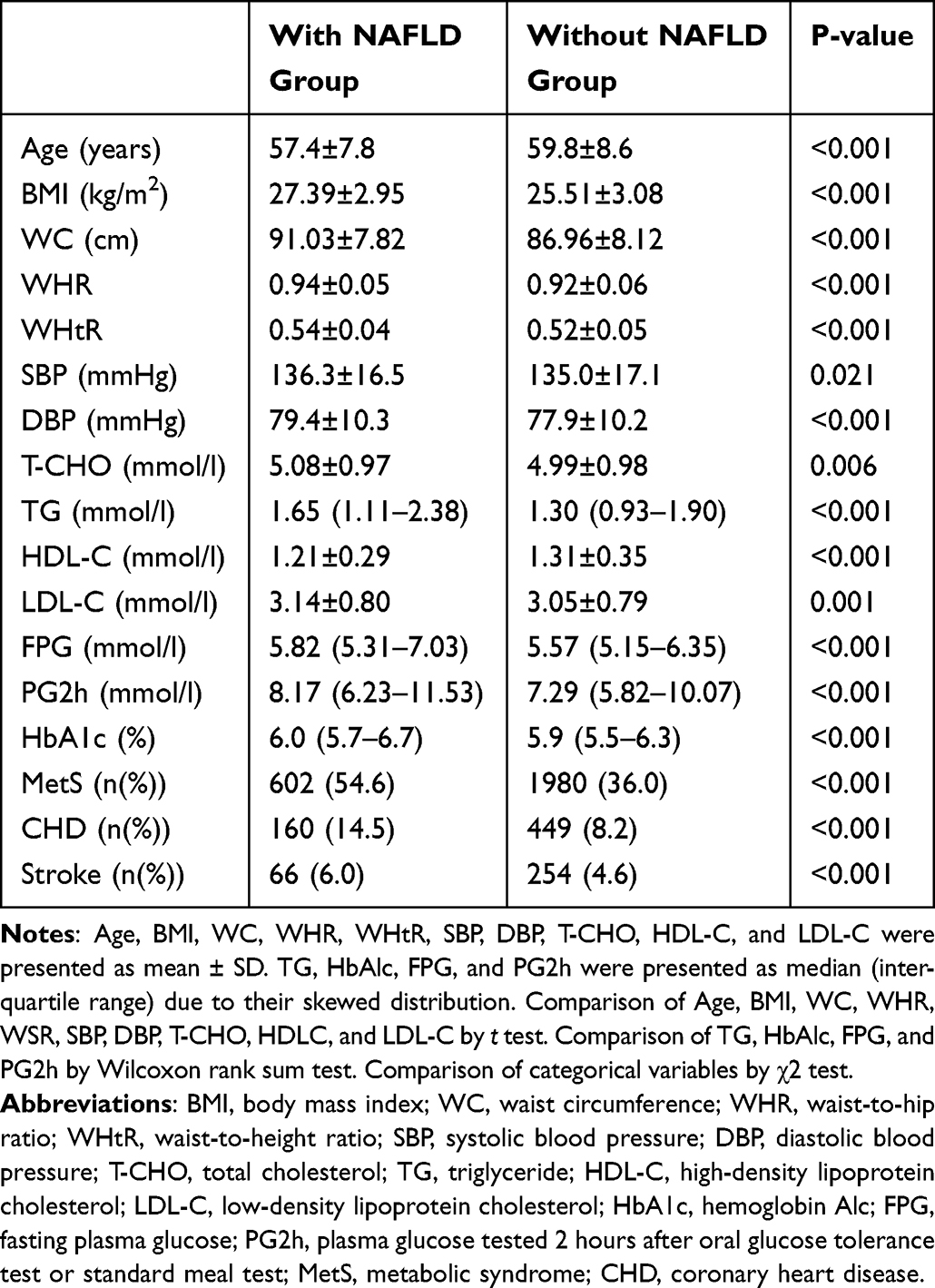 |
Table 1 Baseline Characteristics of Subjects with or Without NAFLD Among Men |
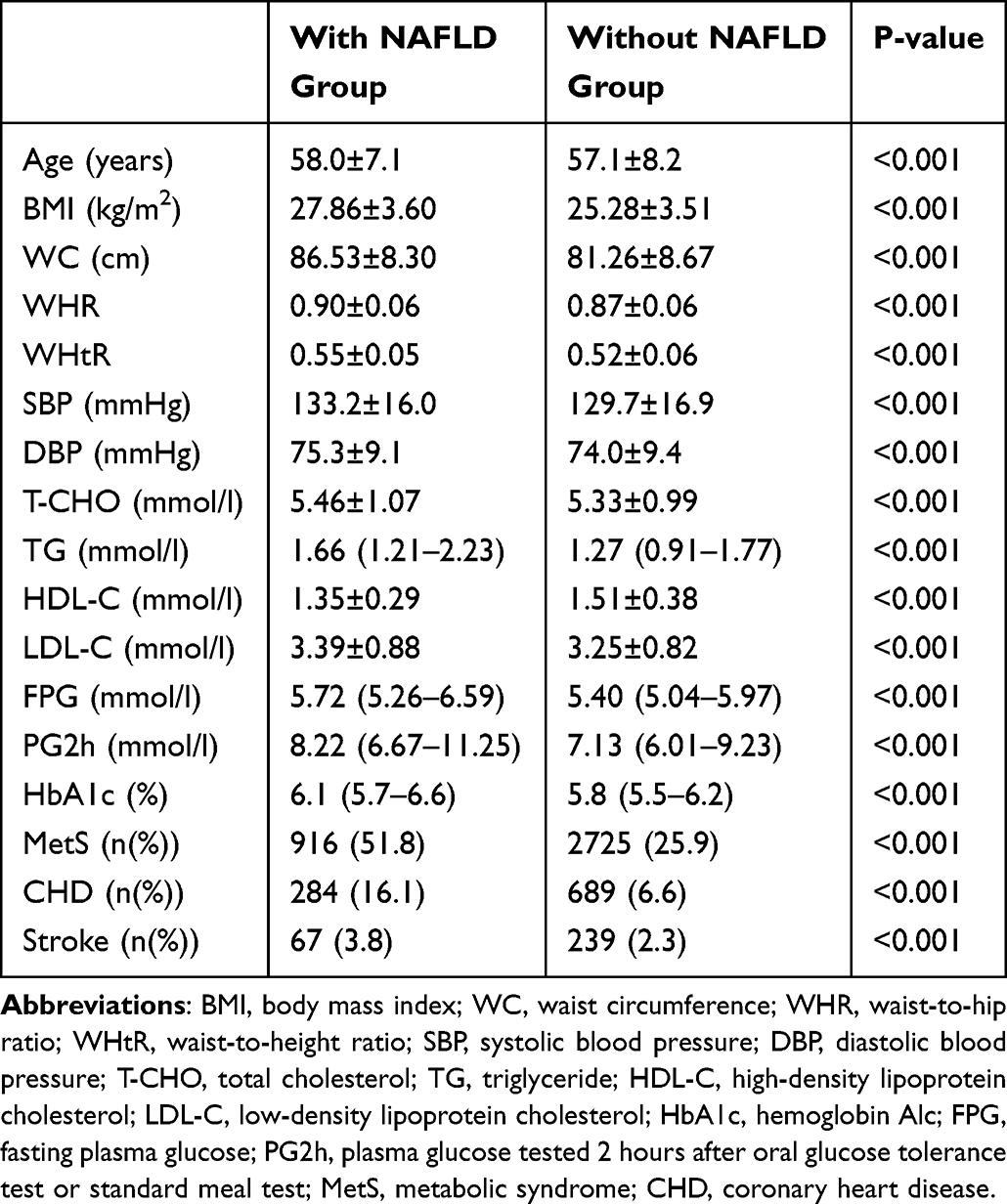 |
Table 2 Baseline Characteristics of Subjects with or Without NAFLD Among Women |
Multivariate Logistic Regression Between NAFLD and CVD
We assayed the correlation between NAFLD and CVD separately in men and women. After adjustment for age, smoking status, alcohol intake, WC, hypertension, dyslipidemia and hyperglycemia, the odds ratios (ORs) of CVD in men were 1.622 (95%CI: 1.345–1.957) and 1.990 (95%CI: 1.709–2.316) in women with NAFLD, compared with the subjects without NAFLD (Tables 3 and 4). The OR value of CVD was 1.841 (95%CI: 1.636–2.070) in the whole population. Among women, the OR value of CVD was 1.990 (95%CI: 1.709–2.317) after further adjustment for menstruation status in the NAFLD group compared with non-NAFLD group.
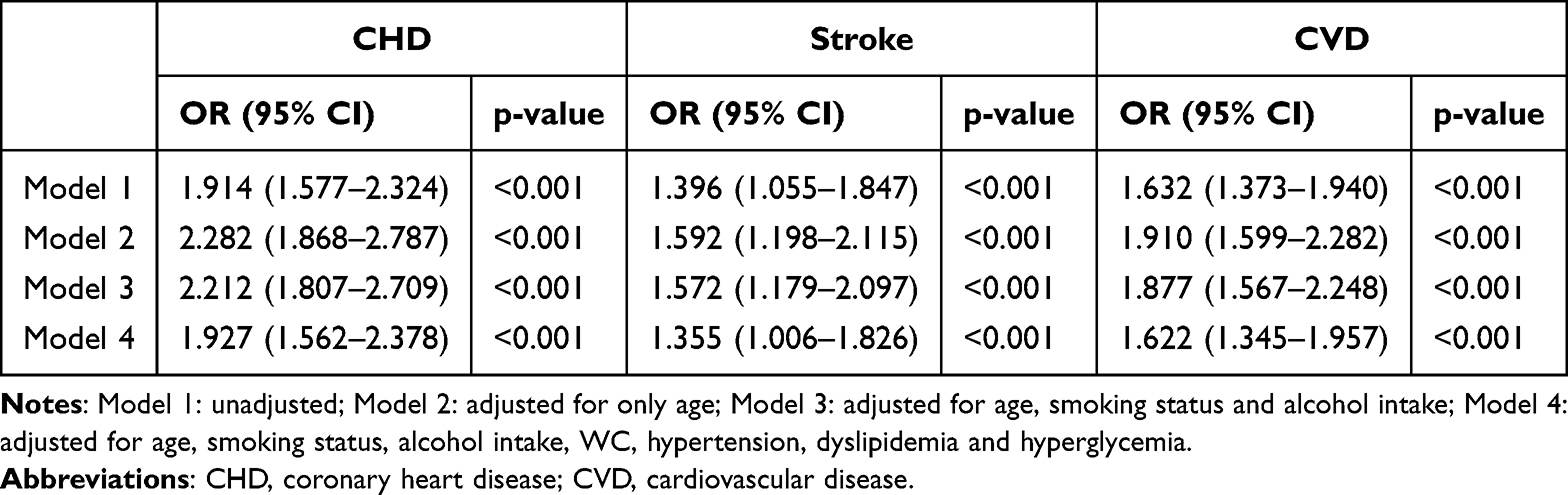 |
Table 3 Multiple Logistic Regression for CVD in Men |
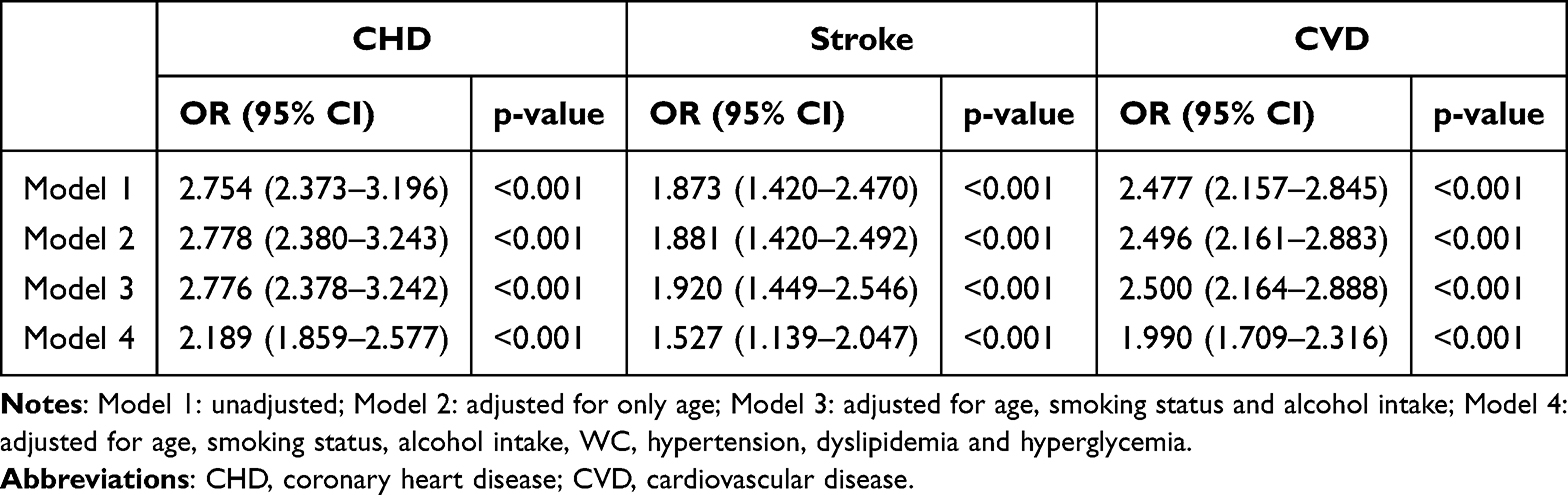 |
Table 4 Multiple Logistic Regression for CVD in Women |
Discussion
In our study, the prevalence of NAFLD was 15.2% (men 16.7% and women 14.4%), which was significantly lower than the present 29.2%. One main reason may be that our study was conducted from 2011to 2012 and at that time NAFLD indeed was underappreciated and underdiagnosed. On the other hand, it may be because of a rapid increasing of prevalence of NAFLD in the past decades due to the heavy burden of obesity and T2DM which were closely correlated with NAFLD.22,23
We found that prevalence of metabolic syndrome was 52.9% in the participants with NAFLD and 29.4% among those without NAFLD (p<0.001). The ORs of CVD among subjects with NAFLD were 1.622 (95%CI: 1.345–1.957) and 1.990 (95%CI: 1.709–2.316) respectively in men and women, compared with those without NAFLD. The results were similar with a previous study conducted among Shanghai adults.24 NAFLD is defined by excess fat deposition in the liver and may be used to reflect visceral fat accumulation. The previous research has shown that visceral adiposity is a better predictor of metabolic abnormalities than subcutaneous fat.25 The insulin resistance (IR) plays an important role in the link between NAFLD and components of MetS, which is tightly associated with visceral adipose tissue mass.26 As a result, the individuals with NAFLD tend to cluster metabolic abnormalities including T2DM, obesity, atherogenic dyslipidemia, which have been established as cardiometabolic risk factors. Therefore, it is not surprising that NAFLD increases the risk of CVD development. In addition, due to the co-existence of NAFLD and MetS in general, the 2020 International Panel of Experts recommended that NAFLD should be renamed as metabolic-associated fatty liver disease (MAFLD), which emphasized the vital role of metabolic dysregulation in disease pathogenesis.27,28 In addition, recently, a multisociety Delphi consensus statement suggested that NAFLD was replaced with metabolic dysfunction-associated steatotic liver disease (MASLD).29
Our study demonstrated that NAFLD remained as a risk factor for CVD after adjustment for other traditional risk factors such as age, smoking, obesity, hyperglycemia, dyslipidemia, high blood pressure. Several previous meta-analyses have shown that NAFLD independently associated with an increased risk of CVD.14,30–32 Accordingly, this suggested that NAFLD maybe contributed actively to the pathogenesis of atherosclerosis except for as a maker for CVD, resulting in an increased risk of incident CVD finally.
It is well known that postmenopausal women are at high risk of developing CVD because of aging and absence of estrogen protection. Postmenopausal women had a greater intra-abdominal fat area and a stronger IR compared with premenopausal women.33 In our study, menstruation-status as a variable was put in the logistic-regression analyses. We found that NAFLD increased the risk of CVD regardless of whether or not menopause among women. It suggested that NAFLD appeared to weaken the protective effects of estrogen and increased the risk of incident CVD among premenopausal women.
The strength of this study lied in the large sample size containing a great quantity of confounders. Our survey had several limitations. First, this was a cross-sectional investigation which could not explore causality. Secondly, we relied on self-report to identify NAFLD and CVD events.
In conclusion, NAFLD is independently associated with increased risk of CVD development. Therefore, in the individuals complicated with NAFLD, it is necessary to early screen and access the CVD risk.
Ethical Approval and Informed Consent
This study complies with the Declaration of Helsinki and was approved by the First Medical Centre of Chinese PLA General Hospital Ethics Committee.
Acknowledgments
This study was supported by grants from the National Key New Drug Creation and Manufacturing Program of the Ministry of Science and Technology (2011ZX09307001-08). We would like to thank all authors for their contributions.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Riazi K, Azhari H, Charette JH, et al. The prevalence and incidence of NAFLD worldwide: a systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(9):851–861. doi:10.1016/S2468-1253(22)00165-0
2. Zhou F, Zhou J, Wang W, et al. Unexpected Rapid Increase in the Burden of NAFLD in China From 2008 to 2018: a Systematic Review and Meta-Analysis. Hepatology. 2019;70:1119–1133. doi:10.1002/hep.30702
3. Maurice J, Manousou P. Non-alcoholic fatty liver disease. Clin Med Lond. 2018;18(3):245–250. doi:10.7861/clinmedicine.18-3-245
4. Targher G, Tilg H, Byrne CD. Non-alcoholic fatty liver disease: a multisystem disease requiring a multidisciplinary and holistic approach. Lancet Gastroenterol Hepatol. 2021;6(7):578–588. doi:10.1016/S2468-1253(21)00020-0
5. Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62:S47–64.
6. Long MT, Zhang X, Xu H, et al. Hepatic fibrosis associates with multiple cardiometabolic disease risk factors: the Framingham Heart Study. Hepatology. 2020. doi:10.1002/hep.31608
7. Cheung O, Sanyal AJ. Recent advances in nonalcoholic fatty liver disease. Curr Opin Gastroen. 2010;26:202–208. doi:10.1097/MOG.0b013e328337b0c4
8. Anstee QM, Targher G, Day CP. Progression of NAFLD to diabetes mellitus, cardiovascular disease or cirrhosis. Nat Rev Gastroenterol Hepatol. 2013;10(6):330–344. doi:10.1038/nrgastro.2013.41
9. Chiriac S, Stanciu C, Girleanu I, et al. Nonalcoholic Fatty Liver Disease and Cardiovascular Diseases: the Heart of the Matter. Can J Gastroenterol Hepatol. 2021;2021:6696857. doi:10.1155/2021/6696857
10. Liang Y, Chen H, Liu Y, et al. Association of MAFLD With Diabetes, Chronic Kidney Disease, and Cardiovascular Disease: a 4.6-Year Cohort Study in China. J Clin Endocrinol Metab. 107(1):88–97. doi:10.1210/clinem/dgab641
11. Targher G, Byrne CD, Lonardo A, Zoppini G, Barbui C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: a meta-analysis. J Hepatol. 2016;65(3):589–600. doi:10.1016/j.jhep.2016.05.013
12. Mahfood Haddad T, Hamdeh S, Kanmanthareddy A, Alla VM. Nonalcoholic fatty liver disease and the risk of clinical cardiovascular events: a systematic review and meta-analysis. Diabetes Metab Syndr. 2017;11 Suppl 1:S209–S216. doi:10.1016/j.dsx.2016.12.033
13. Wu S, Wu F, Ding Y, Hou J, Bi J, Zhang Z. Association of non-alcoholic fatty liver disease with major adverse cardiovascular events: a systematic review and meta-analysis. Sci Rep. 2016;6:33386. doi:10.1038/srep33386
14. Tang ASP, Chan KE, Quek J, et al. Non-alcoholic fatty liver disease increases risk of carotid atherosclerosis and ischemic stroke: an updated meta-analysis with 135,602 individuals. Clin Mol Hepatol. 2022;28(3):483–496. doi:10.3350/cmh.2021.0406
15. Stahl EP, Dhindsa DS, Lee SK, Sandesara PB, Chalasani NP, Sperling LS. Nonalcoholic Fatty Liver Disease and the Heart: JACC State-of-The-Art Review. J Am Coll Cardiol. 2019;73:948–963. doi:10.1016/j.jacc.2018.11.050
16. Wu R, Hou F, Wang X, et al. Nonalcoholic Fatty Liver Disease and Coronary Artery Calcification in a Northern Chinese Population: a Cross Sectional Study. Sci Rep. 2017;7:9933. doi:10.1038/s41598-017-09851-5
17. Wong VW, Wong GL, Yip GW, et al. Coronary artery disease and cardiovascular outcomes in patients with non-alcoholic fatty liver disease. Gut. 2011;60:1721–1727. doi:10.1136/gut.2011.242016
18. Sun L, Lü SZ. Association between non-alcoholic fatty liver disease and coronary artery disease severity. Chin Med J. 2011;124:867–872.
19. Zhang X, Yan W, Wang B, Wang L, Mu Y, Wang S. Association Between Some Different Obesity Anthropometric Indices and Type 2 Diabetes Mellitus in Middle-Aged and Elderly Chinese Men and Women in Beijing, China: a Cross-Sectional Study. Diabetes Metab Syndr Obes. 15:1799–1807. doi:10.2147/DMSO.S359657
20. Zhang X, Mu Y, Yan W, Ba J, Li H. Prevalence of stroke and metabolic disorders in the middle-aged and elderly Chinese with type 2 diabetes. Chin Med J. 2014;127:3537–3542. doi:10.3760/cma.j.issn.0366-6999.20141018
21. Chinese Diabetes Society. Guideline for the prevention and treatment of type 2 diabetes mellitus in China (2020 edition). Chin J Diabetes Mellitus. 2021;13(4):315–409.
22. Chen K, Shen Z, Gu W, et al. Meinian Investigator Group. Prevalence of obesity and associated complications in China: a cross-sectional, real-world study in 15.8 million adults. Diabetes Obes Metab. 2023;25(11):3390–3399. doi:10.1111/dom.15238
23. Li Y, Teng D, Shi X, et al. Prevalence of diabetes recorded in mainland China using 2018 diagnostic criteria from the American Diabetes Association: national cross sectional study. BMJ. 2020;369(997). doi:10.1136/bmj.m997
24. Fan JG, Zhu J, Li XJ, et al. Fatty liver and the metabolic syndrome among Shanghai adults. J Gastroenterol Hepatol. 2005;20(12):1825–1832. doi:10.1111/j.1440-1746.2005.04058.x
25. Tchernof A, Despres JP. Pathophysiology of human visceral obesity: an update. Physiol Rev. 2013;93:359–404. doi:10.1152/physrev.00033.2011
26. Rinaldi L, Pafundi PC, Galiero R, et al. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrat Rev Antioxi. 2021;10:270.
27. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73:202–209. doi:10.1016/j.jhep.2020.03.039
28. Zhang XL, Fan JG, Wei L, Shi JP, Zheng MH. Promoting the term MAFLD: china in action. Lancet Gastroenterol Hepatol. 2022;7:598. doi:10.1016/S2468-1253(22)00127-3
29. Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542–1556. doi:10.1016/j.jhep.2023.06.003
30. Toh JZK, Pan XH, Tay PWL, et al. A Meta-Analysis on the Global Prevalence, Risk factors and Screening of Coronary Heart Disease in Nonalcoholic Fatty Liver Disease. Clin Gastroenterol Hepatol. 2022;20(11):2462–2473.e10. doi:10.1016/j.cgh.2021.09.021
31. Arslan U, Yenerçağ M. Relationship between non-alcoholic fatty liver disease and coronary heart disease. World J Clin Cases. 8(20):4688–4699. doi:10.12998/wjcc.v8.i20.4688
32. Caussy C, Aubin A, Loomba R. The Relationship Between Type 2 Diabetes, NAFLD, and Cardiovascular Risk. Curr Diab Rep. 21(5):15. doi:10.1007/s11892-021-01383-7
33. Toth MJ, Tchernof A, Sites CK, et al. Effect of menopausal status on body composition and abdominal fat distribution. Int J Obes Relat Metab Disord. 2000;24(2):226–231. doi:10.1038/sj.ijo.0801118
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.