")
Back to Journals » Journal of Inflammation Research » Volume 18
Association Between Pan-Immune-Inflammation Value and Dipper/Non-Dipper Status in Newly Diagnosed Hypertensive Patients
Authors Ateş MS , Yıldırım A, Sökmen E
Received 11 February 2025
Accepted for publication 8 May 2025
Published 13 May 2025 Volume 2025:18 Pages 6217—6228
DOI https://doi.org/10.2147/JIR.S522032
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Muhammet Salih Ateş, Alp Yıldırım, Erdoğan Sökmen
Department of Cardiology, Kırsehir Ahi Evran Education and Research Hospital, Kırsehir, Turkey
Correspondence: Muhammet Salih Ateş, Ahi Evran University Faculty of Medicine, Kervansaray Mahallesi, 2019. Sokak. No: 1, Merkez, Kırşehir, 40200, Türkiye, Tel +90 555 602 98 88, Email [email protected]
Purpose: This study aimed to investigate the association between the pan-immune-inflammation value (PIV) and dipper/non-dipper status in newly diagnosed hypertensive (HT) patients. Given the role of systemic inflammation in circadian blood pressure (BP) pattern, we hypothesized that elevated PIV levels would be linked to an impaired nocturnal BP decline.
Patients and Methods: A total of 725 newly diagnosed hypertensive patients and 343 normotensive controls were prospectively included in the study. The HT patients were further classified as dipper (n=339) or non-dipper (n=386) based on 24-hour ambulatory BP monitoring (ABPM). PIV was calculated as (neutrophil count × platelet count × monocyte count) / lymphocyte count. Multivariate logistic regression analysis was performed to assess the independent association between PIV quartiles and non-dipper status. Receiver operating characteristic (ROC) curve analysis was conducted to determine the predictive value of PIV.
Results: PIV was significantly higher in non-dipper hypertensive patients compared with dipper hypertensive patients (p< 0.001). In multivariate regression models adjusted for age, sex, body mass index (BMI), smoking, diabetes mellitus, and echocardiographic parameters, the highest PIV quartile (Q4) was independently associated with non-dipper status (OR: 12.56, 95% CI: 7.31– 21.56, p< 0.001). ROC analysis demonstrated that a PIV cutoff of 326.96 predicted non-dipper status with a sensitivity of 70.5% and specificity of 65.5% (AUC: 0.725, p< 0.001).
Conclusion: Elevated PIV levels were significantly associated with non-dipper hypertension, reinforcing the contribution of systemic inflammation to circadian BP dysregulation. These findings suggest that PIV may serve as a potential biomarker for risk stratification and personalized treatment approaches in hypertensive patients.
Keywords: pan-immune-inflammation value, hypertension, circadian blood pressure pattern, non-dipper status, inflammation
Introduction
One of the world’s major health problems is hypertension (HT), which affects a worldwide population greater than 1.3 billion and is a significant contributor to heart disease and related deaths.1 Vascular dysfunction and end-organ damage are caused by a complex interaction of hemodynamic, neurohormonal, and inflammatory processes.2 Despite advancements in antihypertensive therapy, a substantial proportion of patients continue to experience disease progression and associated complications.3
Circadian regulation of blood pressure (BP) plays a critical role in cardiovascular (CV) health.4 A physiological nocturnal BP decline, known as the dipper pattern, is associated with favorable CV outcomes. In contrast, non-dipper HT, characterized by attenuated nocturnal BP reduction, has been linked to increased risks of arterial stiffness, target organ damage, and adverse CV events.5 The mechanisms underlying the dipper and non-dipper phenotypes remain incompletely understood, but accumulating evidence suggests that chronic inflammation and immune dysregulation contribute to these distinct BP patterns.
In recent years, systemic inflammatory markers derived from routine blood parameters have gained attention as potential predictors of CV risk, such as lymphocyte count, platelet count, neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR), monocyte to lymphocyte ratio (MLR).6,7 Drugescu et al and Bozduman et al reported that lymphocyte count, PLR, NLR and MLR became elevated in non-dipper HT and were also associated significantly with non-dipping circadian BP pattern.8,9 On the other hand, Sunbul et al proposed that PLR but not NLR was independently associated with non-dipping circadian BP pattern despite increase in both ratios in non-dipper HT patients.10 Conflicting results also present regarding the platelet counts in different circadian BP patterns in HT patients. Some studies reported a significantly decreased platelet counts in non-dipper HT patients, whereas some others reported no difference in platelet counts between non-dipper and dipper circadian BP pattern not only in HT patients, but also in prehypertensive and normotensive subjects.9,11 However, a composite marker called the pan-immune-inflammation value (PIV), which includes platelet, lymphocyte, monocyte and neutrophil counts, was proposed to provide a better and more comprehensive assessment of bodily inflammatory and immune status than these conventional indices like platelet counts, NLR, PLR, neutrophil and lymphocyte counts. In this regard, the superiority of PIV was demonstrated over the conventional inflammatory indices such as NLR and PLR in the prediction of prognosis, degree of stenosis and impaired coronary flow after percutaneous coronary intervention in ACS patients. Furthermore, elevated PIV was found be related to poor outcomes in a number of different disease states, including coronary artery disease, HT, and heart failure.12 However, its role in circadian BP regulation remains largely unexplored.
Given the well-established link between systemic inflammation and HT, we hypothesized that PIV may be associated with circadian changes in BP. In this regard, we aimed to perform a study to assess the association of PIV with dipper/non-dipper status in newly diagnosed hypertensive patients. By elucidating this association, we sought to provide novel insights into the inflammatory mechanisms underlying circadian BP pattern, which may have implications for risk stratification and targeted therapeutic strategies in HT management.
Methods
Study Design and Patient Recruitment
We conducted the current prospective and observational study between December 2024 and February 2025 to investigate the association between PIV and the dipper/non-dipper status in newly diagnosed patients with HT. Participants were consecutively included from the cardiology outpatient clinic of a tertiary center. The selection criteria called for (1) a diagnosis of essential HT confirmed through 24-hour ambulatory BP monitoring (ABPM), characterized by a respective mean 24-hour systolic BP (SBP) and diastolic BP (DBP) ≥ 130 mmHg/ 80 mmHg, or a respective mean daytime (06:00–22:00) SBP and DBP ≥135/85 mmHg, or a respective mean nighttime (22:00–06:00) SBP and DBP ≥120/70 mmHg in line with the relevant guidelines.13 Patients were excluded if they had (1) secondary HT, (2) prior antihypertensive medication use, (3) acute or chronic infections, (4) autoimmune or hematological disorders, (5) malignancies, (6) chronic inflammatory diseases, (7) history of acute coronary syndrome or cerebrovascular events, or (8) lacking laboratory or clinical data. Our study protocol was in compliance with the Declaration of Helsinki and was approved by the Ahi Evran University Clinical Research Ethics Committee (Decision No: 2024/20-176, Date: December 10, 2024). The study participants gave written informed consent.
Blood Pressure Measurement and Circadian Pattern Classification
All participants underwent 24-hour ABPM using a validated oscillometric ABPM device (The Mobil-O-Graph manufactured by I.E.M. GmbH, Stolberg, Germany). Measurements were taken every 30 minutes during the daytime, from 06:00 until 22:00, and every 60 minutes during the nighttime, from 22:00 until 06:00. A qualified daytime and nighttime measurement were defined as having at least 14 valid readings and at least 7 valid readings during the awake and the asleep periods, respectively. Sleep and awake periods were assessed based on the self-information of patients.14
The device was calibrated before each measurement, and the participants were instructed to maintain their usual daily activities while restricting excessive movements during the recordings. The mean 24-h, daytime, and nighttime SBP and DBP were calculated. Patients were classified as dippers if their nocturnal SBP decreased by ≥10% relative to daytime SBP and as non-dippers if their nocturnal SBP reduction was <10%.
Echocardiographic Assessment
Transthoracic echocardiography was performed using the Philips Affiniti CVx CV Ultrasound System (manufactured by Philips Medical Systems in Andover, MA, USA) by consultant cardiologists blinded to the ABPM findings. Simpson’s biplane method was utilized to calculate the left ventricular ejection fraction (LVEF). Standard echocardiographic parameters, including left atrial diameter (LAD), early mitral inflow velocity (E-wave), early diastolic mitral annular velocities (E’ septal and E’ lateral), and E/E’ ratios, were measured in accordance with American Society of Echocardiography guidelines.
Laboratory and Inflammatory Markers
Blood samples from the venous system were taken in the morning following an overnight fast of at least eight hours. Parameters from the complete blood count (CBC), such as white blood cells, neutrophils, lymphocytes, monocytes, and platelet counts, were examined using a computerized hematology analyzer (The Beckman Coulter DXH 800 analyzer manufactured by Beckman Coulter, Fullerton, CA, USA). Routine biochemical markers, including serum creatinine, fasting glucose, total cholesterol, LDL-C, HDL-C, triglycerides, and hemoglobin, were measured using standard enzymatic methods. PIV was computed as neutrophil count × platelet count × monocyte count divided by the lymphocyte count.
Statistical Analysis
Statistical analyses were conducted using SPSS (version 29.0, IBM Corp., Armonk, NY, USA). Continuous variables showing non-normal distribution required evaluation of normality using the Kolmogorov–Smirnov test; data were presented as median and interquartile range (IQR), specified as the 25th to 75th percentile. Given the non-parametric nature of the data, Kruskal–Wallis test was used to compare continuous variables among the three study groups, and ANOVA was performed as a supplementary parametric approach when necessary. The chi-square test was used to analyze categorical variables.
To evaluate the independent association between PIV and non-dipper status, multivariate logistic regression analysis was conducted. The PIV was categorized into quartiles (Q1–Q4), with Q1 serving as the reference group, and three separate models were developed to examine the association while controlling for potential confounders. Model 1 was an unadjusted crude model, assessing the direct association between PIV quartiles and dipper/non-dipper status. Model 2 was adjusted for body mass index (BMI), sex, age, diabetes mellitus, smoking status, coronary artery disease (CAD) and chronic obstructive pulmonary disease (COPD) to account for key demographic and clinical factors. Model 3 included additional adjustments such as serum creatinine, hemoglobin, total cholesterol, LDL-C, HDL-C, triglycerides, LVEF, LAD, and E/E’ ratios (septal and lateral) to ensure a comprehensive multivariable analysis incorporating metabolic and echocardiographic parameters.
Additionally, univariate and multivariate analyses were performed in an attempt to delineate the independent predictors of non-dipper status. Variables of <0.05 p value in the univariate regression model were incorporated in multivariate analysis through a backward stepwise selection method to optimize the model and exclude non-significant variables. PIV was included in the analysis as a continuous variable. Correlations between PIV and ambulatory BP parameters were assessed using Spearman correlation coefficient, given the non-parametric distribution of the data. Two-tailed p-value was accepted to be statistically significant, if it is <0.05.
Results
Study Population and Demographics
A total of 1248 patients were initially screened for recruitment to the study. Following application of the exclusion criteria, 152 patients were removed from consideration due to existing secondary HT, previous use of antihypertensive medication, acute or chronic infections, autoimmune disorders, a history of cancer, chronic inflammatory conditions, prior CV or cerebrovascular events, or missing clinical data. In addition, 28 patients were excluded due to incomplete laboratory results. Thus, the final study cohort comprised 1068 patients, which were categorized into the non-dipper hypertensive (n=386), dipper hypertensive (n=339), and control (n=343) groups (Figure 1).
 |
Figure 1 Flowchart Depicting the Patient Selection Process and Group Classification. |
Mean age (p = 0.897), BMI (p = 0.103), and gender distribution (p = 0.971) did not significantly differ among the groups. However, significant differences were observed in total cholesterol (p<0.001), LDL-C (p<0.001), HDL-C (p=0.001), and triglyceride levels (p<0.001), with higher values seen in hypertensive groups compared with the controls. The ambulatory BP parameters demonstrated significantly higher 24-h, daytime, and nighttime systolic and diastolic BPs in the hypertensive groups compared with the controls (p<0.001 for all). Additionally, white blood cell (WBC) count, neutrophil count, platelet count, monocyte count, and PIV were significantly elevated in the non-dipper group compared with the dipper hypertensive patients and the controls (p<0.001 for all) (Table 1).
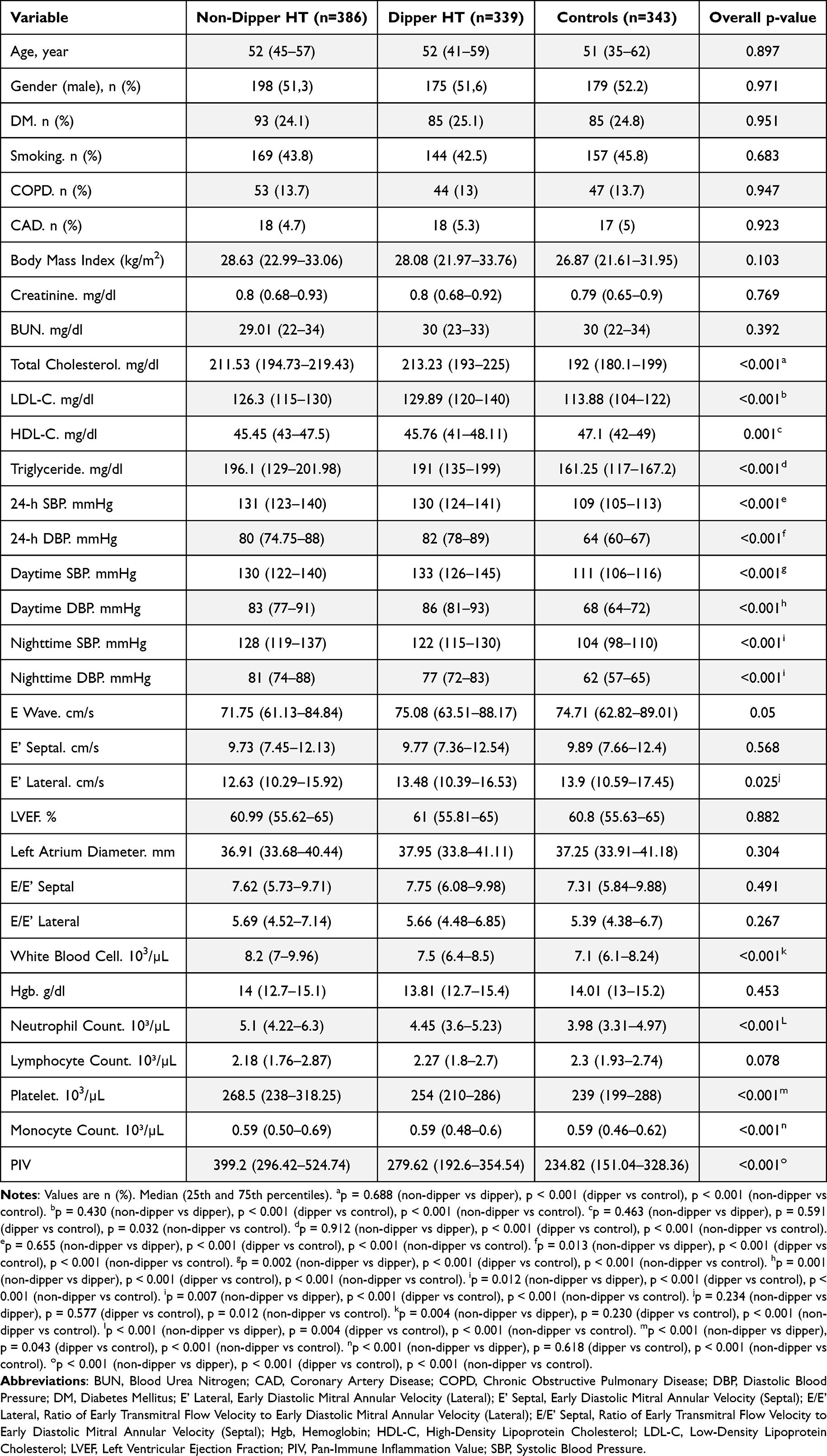 |
Table 1 Baseline Clinical, Biochemical, Echocardiographic, and Ambulatory Blood Pressure Monitoring Parameters of Patients According to Non-Dipper Hypertension, Dipper Hypertension, and Control Groups |
Correlation Between PIV and Clinical Parameters in Hypertensive Patients
Bivariate correlation analysis between the dipper and the nondipper HT patients revealed that PIV was significantly correlated with the nighttime SBP (r=0.085, p=0.022), nighttime DBP (r=0.090, p=0.015), and triglyceride levels (r=0.086, p=0.021). On the other hand, PIV was found to be negatively correlated with LDL-C (r=−0.119, p=0.001). No statistically significant correlations were observed with the other parameters (Table 2).
 |
Table 2 Bivariate Correlation Analysis According to PIV in Hypertensive Patients |
Multivariate Logistic Regression Analysis of PIV Quartiles and Nondipper Status in Hypertensive Patients
Multivariate logistic regression analyses between the dipper and the nondipper HT patients were performed to assess the association between PIV quartiles and non-dipping circadian pattern. In the unadjusted Model 1, patients in the greatest PIV quartile (Q4) had a significantly higher odds ratio (OR) for non-dipper HT (OR: 12.06, 95% CI: 7.09–20.49, p<0.001) compared with the reference Q1 group. This association remained robust in Model 2 (adjusted for BMI, sex, age, smoking, diabetes mellitus, COPD, and CAD) (OR: 12.50, 95% CI: 7.32–21.36, p<0.001) and Model 3 (fully adjusted for metabolic/echocardiographic parameters) (OR: 12.56, 95% CI: 7.31–21.56, p<0.001). A significant trend was observed across all models (p for trend <0.001), indicating a strong relationship between increasing PIV levels and non-dipper HT (Table 3).
 |
Table 3 Multivariable Logistic Regression Analysis for the Association Between Pan-Immune-Inflammation Value (PIV) Quartiles and Non-Dipper Status in Hypertensive Patients |
Univariate and Multivariate Predictors of Nondipper Status in Hypertensive Patients
In the univariate analysis between the dipper and the nondipper HT patients, nighttime SBP (OR: 1.012, 95% CI: 1.003–1.020, p=0.005), nighttime DBP (OR: 1.027, 95% CI: 1.013–1.041, p<0.001), lower E-wave velocity (OR: 0.987, 95% CI: 0.977–0.997, p=0.010), and a higher PIV (OR: 1.005, 95% CI: 1.004–1.006, p<0.001) were significantly associated with non-dipper status. In the multivariate analysis, nighttime DBP (OR: 1.025, 95% CI: 1.010–1.039, p=0.001), E-wave velocity (OR: 0.988, 95% CI: 0.977–0.999, p=0.026), and PIV (OR: 1.005, 95% CI: 1.004–1.006, p<0.001) remained independently associated with non-dipper HT (Table 4).
 |
Table 4 Univariate and Multivariate Logistic Regression Analyses for Factors Associated with Non-Dipper Status in Hypertensive Patients |
ROC Curve Analysis for PIV in Predicting Nondipper Status in Hypertensive Patients
A cut-off of 326.96 for PIV emerged as an optimal value in the ROC curve analysis to distinguish the subjects with non-dipper HT with respective sensitivity and a specificity of 70.5% and 65.5% (AUC: 0.725; p < 0.001) (Figure 2).
 |
Figure 2 ROC Analysis Depicting Sensitivity and Specificity of Pan-Immune-Inflammation Value (PIV) in the Prediction of Non-Dipper Status in Hypertensive Patients. |
Discussion
Main finding of our study was that, independently of traditional CV risk factors, PIV was significantly associated with non-dipper HT. Our findings also suggest that increased systemic inflammation, as reflected by PIV, contributes to circadian BP pattern, particularly impairing physiological nocturnal BP decline. Patients with higher PIV levels exhibited a greater tendency toward a non-dipper pattern, indicating a potential role of systemic inflammation in disrupting normal vascular homeostasis.
Significance of systemic inflammation has been underscored in the development of HT by previous studies, with many of whom demonstrating that immune system imbalances led to vascular dysfunction, increased arterial stiffness, and caused damage to vital organs.2,6,7 Inflammation-mediated HT is linked to the activation of neutrophils, monocytes, and platelets, all of which are key components of PIV. Although the relationship between inflammatory markers and circadian BP patterns has been explored in previous studies, the specific role of PIV in predicting non-dipper status has not been thoroughly investigated. Wu et al examined the relationship of PIV with long-term CV mortality in hypertensive patients and demonstrated that higher PIV levels were linked to an increase in CV risk and all-cause mortality.12 Their finding is consistent with ours, as non-dipper HT is recognized as an independent risk for adverse CV outcomes. However, Wu et al did not seek to evaluate circadian BP patterns, making our findings a valuable addition to the existing literature by establishing a direct link between systemic inflammation and nocturnal BP regulation.
Non-dipping HT has been consistently associated with a worse prognosis compared to dipping HT, primarily due to its link with increased inflammation, vascular damage, and a higher incidence of end-organ complications.5 Studies reveal that patients with a non-dipping BP pattern are at an elevated risk of CV and cerebrovascular events. This heightened risk is largely attributed to the chronic inflammatory processes observed in such patients. Elevated markers such as neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and systemic immune-inflammation index (SII) were demonstrated to independently predict non-dipping HT and its associated complications.10,15
Inflammatory pathways play a pivotal role in non-dipping HT etiopathogenesis.6,16 Neutrophils can influence the vascular environment by elevating oxidative stress levels, which may impair endothelial function. Additionally, they play a role in recruiting other immune cells to tissues by releasing chemokines and cytokines with chemoattractant properties. This immune activation supports a proinflammatory state that contributes to the onset and progression of arterial hypertension.17 Supporting these premises, a large cohort study encompassing 9383 normotensive subjects from Japanese population indicated that elevated neutrophil levels were associated with the development of a new hypertension during a follow-up period of around 40 years.18 Furthermore, greater neutrophils levels indicate acute inflammatory activation, while reduced lymphocyte counts reflect systemic immune suppression, both of which are hallmark features in these patients. Elevated neutrophil levels are typically associated with inflammatory responses, whereas reduced lymphocyte counts may indicate physiological stress and compromised overall health; therefore, NLR may serves as a marker of systemic inflammation and stress, and changes in NLR have been observed in individuals with HT.10 Beyond HT, Bozduman et al reported an additional increase in NLR both in normotensive and hypertensive non-dippers, reflecting a further escalated inflammatory status in non-dipping circadian BP pattern.9 This inflammatory burden reflected by a higher NLR may contribute to impaired nocturnal blood pressure decline by promoting endothelial dysfunction and sympathetic overactivity.19–21
Additionally, platelet activation has been found to be more pronounced in non-dipping hypertensive individuals, contributing to a pro-thrombotic state and further vascular injury. This inflammatory milieu not only accelerates vascular damage but also exacerbates left ventricular hypertrophy, endothelial dysfunction, and arterial stiffness, all of which contribute to the observed adverse clinical outcomes.3,22,23
Furthermore, non-dipping HT has been linked to significant alterations in hematological parameters. Studies by Akyüz et al and Sunbul et al have demonstrated that white blood cell count, neutrophil levels, and PLR are significantly higher in non-dipping hypertensive patients compared to their dipping counterparts.10,15 These findings underline the crucial role of inflammation in mediating the poor prognosis associated with this condition compared with the nondipper HT.
Previous studies have explored the prognostic value of PIV for such CV diseases as myocardial infarction and cardiac failure.24,25 Murat et al demonstrated that PIV was superior to other inflammatory markers in predicting mortality in ST-segment elevation acute coronary syndrome patients, highlighting its role in acute CV events.26 Similarly, Cetinkaya et al found that PIV was significantly associated with the severity of coronary artery disease in patients with non-ST-segment elevation acute coronary syndrome, further supporting its role as a marker of systemic vascular inflammation.27 In addition to its association with HT, PIV has been implicated in other CV conditions, including aortic dissection and stroke. Yu et al reported that elevated PIV levels were predictive of postoperative in-hospital deaths in acute type-A aortic dissection patients, suggesting a strong link between systemic inflammation and vascular instability.28 Similarly, Chen et al demonstrated that PIV had a J-shaped association with stroke risk in hypertensive individuals, emphasizing the complex relationship between immune activation and cerebrovascular events.29 These findings further reinforce the role of PIV as a marker of vascular inflammation and highlight its relevance in the broader context of CV disease. Although our study did not evaluate the patients’ prognosis in the long run, the observed association between PIV and non-dipper HT suggests that increased systemic inflammation might be indulged in the progression of hypertensive end-organ damage over time. These studies provide indirect evidence that immune activation contributes to vascular dysfunction, which is a key feature of HT and related complications. However, no study investigated the association between PIV and the circadian pattern of HT.
The relationship of inflammation with HT also has been examined in the context of systemic immune activation. Chronic low-grade inflammation is a hallmark of HT, with elevated inflammatory cytokines like tumor necrosis factor-alpha, C-reactive protein and interleukin-6 observed in hypertensive individuals.2,6,16,22 Immune cell infiltration of the vascular endothelium increased oxidative stress, and platelet activation are well-established mechanisms contributing to endothelial dysfunction and arterial stiffness.3 PIV, as a composite index incorporating neutrophils, monocytes, platelets, and lymphocytes, captures a more comprehensive representation of immune system activation compared to traditional inflammatory markers. Our findings suggest that increased PIV may reflect an exaggerated immune response that interferes with BP regulation, particularly during the nocturnal period. Previous studies also supported this hypothesis by documenting that the patients with increased inflammatory burden exhibit blunted dipping in the nocturnal BP, thus conferring a higher risk of CV complications.
The clinical implications of our findings are significant, as non-dipper HT has been linked to an increased myocardial infarction, stroke and heart failure risks. Current HT management strategies primarily focus on BP reduction without specific consideration of the inflammatory status. Our study suggests that PIV could prove to be valuable biomarker in the identification of high-risk hypertensive patients who might benefit from more intensified therapeutic interventions. Given the inflammatory nature of HT, we consider that future researches should focus more on whether anti-inflammatory strategies, such as IL-6 inhibitors or colchicine, could modulate this variability in BP and improve CV prognosis in non-dipper hypertensive patients. Additionally, the concept of chronotherapy, which involves timing antihypertensive medication according to circadian rhythms, may be further optimized by incorporating inflammatory markers, such as PIV, into treatment algorithms.
Despite its strengths, a number of limitations may apply to our study. The cross-sectional design of the study prevents causal inferences, so future longitudinal studies are warranted to identify whether PIV predicts progression to non-dipper HT over time. Additionally, we did not assess specific inflammatory cytokines or immune cell subpopulations, which could have provided further mechanistic insights into the relationship between inflammation and BP regulation. We also did not follow up the nondipper patients regarding the possible CV end-points in order to establish a link between PIV and the patients’ prognosis. Our study population was also limited to a single center, necessitating external validation in larger, multi-ethnic cohorts to ensure generalizability. Furthermore, all participants in our study were Caucasian and recruited from a central region of the country; thus, the potential influence of ethnic or regional differences could not be evaluated. Future research should focus on elucidating the precise molecular mechanisms linking PIV to HT and evaluating whether targeted anti-inflammatory interventions can mitigate BP fluctuations in non-dipper patients.
Our results may help incorporate new insights in the inflammatory pathways behind different HT phenotypes and emphasize the importance of immune system activation in BP regulation. The identification of PIV as a significant predictor of non-dipper HT reinforces its role as a potential biomarker for risk assessment and tailored treatment approaches in patients with HT.
Conclusion
Our study provides novel evidence that elevated PIV levels might be associated with non-dipper HT, fortifying the contribution of systemic inflammation in BP dysregulation. Therefore, our findings propose that PIV could prove a useful biomarker not only in risk stratification but for targeted intervention in hypertensive patients. The integration of inflammatory markers into HT management strategies may improve patient outcomes by identifying individuals at higher risk of adverse CV events. Future large-scale studies are warranted to explore the clinical utility of PIV in guiding personalized antihypertensive therapy and its potential as a therapeutic target in inflammation-driven HT.
Data Sharing Statement
Data are available upon request.
Author Contributions
All authors have made significant contributions to the work reported, which may include the conception, study design, execution, acquisition of data, analysis and interpretation, or all of these areas; drafting, revising, or critically reviewing the article; giving final approval of the version to be published; agreeing on the journal to which the article has been submitted; and accepting responsibility for all aspects of the work.
Funding
No funding is available.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Oparil S, Acelajado MC, Bakris GL, et al. Hypertension. Nat Rev Disease Primers. 2018;4:18014. doi:10.1038/nrdp.2018.14
2. Madhur MS, Elijovich F, Alexander MR, et al. Hypertension: do inflammation and immunity hold the key to solving this epidemic? Circ Res. 2021;128(7):908–933. doi:10.1161/CIRCRESAHA.121.318052
3. Deussen A, Kopaliani I. Targeting inflammation in hypertension. Curr Opin Nephrol Hypertens. 2023;32(2):111–117. doi:10.1097/MNH.0000000000000862
4. Sun Y, Zhang Y, Liu F, et al. The relationship between circadian rhythm of blood pressure and vascular dysfunction in essential hypertension. Clin Exp Hypertens. 2023;45(1):2229535. doi:10.1080/10641963.2023.2229535
5. Gavriilaki M, Anyfanti P, Nikolaidou B, et al. Nighttime dipping status and risk of cardiovascular events in patients with untreated hypertension: a systematic review and meta‐analysis. J Clin Hypertension. 2020;22(11):1951–1959. doi:10.1111/jch.14039
6. Xiao L, Harrison DG. Inflammation in hypertension. Can J Cardiol. 2020;36(5):635–647. doi:10.1016/j.cjca.2020.01.013
7. Jin N, Huang L, Hong J, et al. The association between systemic inflammation markers and the prevalence of hypertension. BMC Cardiovasc Disord. 2023;23(1):615. doi:10.1186/s12872-023-03661-6
8. Drugescu A, Roca M, Zota IM, et al. Relationships between easily available biomarkers and non-dipper blood pressure pattern in patients with stable coronary artery disease. Life. 2023;13(3):640. doi:10.3390/life13030640
9. Bozduman F, Yildirim E, Cicek G. Biomarkers of nondipper hypertension in prehypertensive and hypertensive patients. Biomark Med. 2019;13(5):371–378. doi:10.2217/bmm-2018-0247
10. Sunbul M, Gerin F, Durmus E, et al. Neutrophil to lymphocyte and platelet to lymphocyte ratio in patients with dipper versus non-dipper hypertension. Clin Exp Hypertens. 2014;36(4):217–221. doi:10.3109/10641963.2013.804547
11. Meric M, Yuksel S, Coksevim M, Gulel O. The effect of mean platelet volume/platelet count ratio on dipper and non-dipper blood pressure status. Medicina. 2019;55(11):742. doi:10.3390/medicina55110742
12. Wu B, Zhang C, Lin S, Zhang Y, Ding S, Song W. The relationship between the pan-immune-inflammation value and long-term prognoses in patients with hypertension: national health and nutrition examination study, 1999–2018. Front Cardiovasc Med. 2023;10:1099427. doi:10.3389/fcvm.2023.1099427
13. McEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension: developed by the task force on the management of elevated blood pressure and hypertension of the European Society of Cardiology (ESC) and endorsed by the European Society of Endocrinology (ESE) and the European Stroke Organisation (ESO). Eur Heart J. 2024;45(38):3912–4018. doi:10.1093/eurheartj/ehae178
14. Agarwal R, Tu W. Minimally sufficient numbers of measurements for validation of 24-hour blood pressure monitoring in chronic kidney disease. Kidney Int. 2018;94(6):1199–1204. doi:10.1016/j.kint.2018.08.021
15. Akyüz A, Işık F. Systemic immune-inflammation index: a novel predictor for non-dipper hypertension. Cureus. 2022;14(8). doi:10.7759/cureus.28176
16. Güntürk EE, İ G, Topuz AN, Akkaya H, Topuz M. Serum interleukin-18 levels are associated with non-dipping pattern in newly diagnosed hypertensive patients. Blood Press Monit. 2021;26(2):87–92. doi:10.1097/MBP.0000000000000487
17. Araos P, Figueroa S, Amador CA. The role of neutrophils in hypertension. Int J Mol Sci. 2020;21(22):8536. doi:10.3390/ijms21228536
18. Tatsukawa Y, Hsu WL, Yamada M, et al. White blood cell count, especially neutrophil count, as a predictor of hypertension in a Japanese population. Hypertens Res. 2008;31(7):1391–1397. doi:10.1291/hypres.31.1391
19. Sarejloo S, Dehesh M, Fathi M, et al. Meta-analysis of differences in neutrophil to lymphocyte ratio between hypertensive and non-hypertensive individuals. BMC Cardiovasc Disord. 2023;23(1):283. doi:10.1186/s12872-023-03304-w
20. Demir M. The relationship between neutrophil lymphocyte ratio and non-dipper hypertension. Clin Exp Hypertens. 2013;35(8):570–573. doi:10.3109/10641963.2013.764893
21. Liu X, Zhang Q, Wu H, et al. Blood neutrophil to lymphocyte ratio as a predictor of hypertension. Am J Hypertens. 2015;28(11):1339–1346. doi:10.1093/ajh/hpv034
22. Justina VD, Giachini FR, Sullivan JC, Webb RC. Toll-like receptors contribute to sex differences in blood pressure regulation. J Cardiovasc Pharmacol. 2020;76(3):255–266. doi:10.1097/FJC.0000000000000869
23. Nurkoç SG, Yakışan T. Mean platelet volume/platelet count ratio and dipper/non-dipper hypertensive patients. Angiology. 2024;00033197241274825. doi:10.1177/00033197241274825
24. Liu Y, Liu J, Liu L, et al. Association of systemic inflammatory response index and pan-immune-inflammation-value with long-term adverse cardiovascular events in ST-segment elevation myocardial infarction patients after primary percutaneous coronary intervention. J Infl Res. 2023;16:3437–3454. doi:10.2147/JIR.S421491
25. Murat B, Murat S, Altınbas ME, et al. Association of pan immune-inflammation value with long term outcomes of acute decompensated heart failure. Arq Bras Cardiol. 2024;121:e20230817. doi:10.36660/abc.20230817
26. Murat B, Murat S, Ozgeyik M, Bilgin M. Comparison of pan‐immune‐inflammation value with other inflammation markers of long‐term survival after ST‐segment elevation myocardial infarction. Eur J Clin Invest. 2023;53(1):e13872. doi:10.1111/eci.13872
27. Cetinkaya Z, Kelesoglu S, Tuncay A, et al. The role of pan-immune-inflammation value in determining the severity of coronary artery disease in NSTEMI patients. J Clin Med. 2024;13(5):1295. doi:10.3390/jcm13051295
28. Yu X, Chen Y, Peng Y, Chen L, Lin Y. The pan-immune inflammation value at admission predicts postoperative in-hospital mortality in patients with acute type A aortic dissection. J Infl Res. 2024;17:5223–5234. doi:10.2147/JIR.S468017
29. Chen J, Luo C, Tan D, Li Y. J-shaped associations of pan-immune-inflammation value and systemic inflammation response index with stroke among American adults with hypertension: evidence from NHANES 1999–2020. Front Neurol. 2024;15:1417863. doi:10.3389/fneur.2024.1417863
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.