")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Association of Diaphragmatic Mobility and Thickening Fraction with Postoperative Pulmonary Complications in Patients Undergoing Thoracic Surgery and Their Application in Prediction
Authors Aisiaiti A, Ajiaikebaier A, Maimaitiming A, Geng Q, He B, Sun J, Zhang B
Received 5 February 2025
Accepted for publication 14 April 2025
Published 23 April 2025 Volume 2025:21 Pages 501—509
DOI https://doi.org/10.2147/TCRM.S519646
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Abudushalamu Aisiaiti,* Aiwuzaili Ajiaikebaier,* Aini Maimaitiming, Qiang Geng, Bichen He, Jinhui Sun, Bing Zhang
Center for Anesthesia and Perioperative Medicine, Xinjiang Medical University Affiliated Tumor Hospital, Urumqi, 830011, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bing Zhang, Center for Anesthesia and Perioperative Medicine, Xinjiang Medical University Affiliated Tumor Hospital, No. 789, Suzhou East Road, Urumqi, 830011, People’s Republic of China, Tel +86-9917819021, Email [email protected]
Purpose: To investigate the association of diaphragmatic mobility and thickening fraction with postoperative pulmonary complications (PPCs) in patients undergoing thoracic surgery and evaluate their values in predicting PPCs.
Patients and Methods: One hundred and nine consecutive patients undergoing thoracic surgery were prospectively enrolled. All patients underwent ultrasound measurements to obtain diaphragmatic mobility and thickening fraction. PPCs were systematically monitored and recorded from postoperative day 1 to 7. The binary logistic regression model was used to perform multivariate analysis, and the receiver operating characteristic (ROC) curve was used to evaluate predictive values.
Results: PPCs occurred in 46 patients (42.2%). Multivariate analysis identified age, smoking, surgical sites, and mean diaphragmatic mobility and thickening fraction of operated side and nonoperated side as independent risk factors for PPCs. ROC curves revealed that the AUC of mean diaphragmatic mobility and thickening fraction for predicting PPCs in patients undergoing thoracic surgery was 0.722 [standard error (SE): 0.050, 95% confidence interval (CI): 0.623~0.821, P< 0.001] and 0.757 (SE: 0.050, 95% CI: 0.659~0.855, P< 0.001), respectively. The predictive model integrating age, smoking and surgical sites yielded an AUC of 0.810 (SE: 0.041, 95% CI: 0.728~0.891, P< 0.001), while the predictive model integrating age, smoking, surgical sites and mean diaphragmatic mobility or thickening fraction yielded an AUC of 0.849 (SE: 0.037, 95% CI: 0.777~0.922, P< 0.001) and 0.881 (SE: 0.033, 95% CI: 0.815~0.946, P< 0.001), respectively.
Conclusion: Both diaphragmatic mobility and thickening fraction showed independent associations with PPCs following thoracic surgery, demonstrating moderate predictive values. The predictive models integrating age, smoking, surgical sites and diaphragmatic mobility or thickening fraction yielded high predictive values, suggesting significant clinical utility for risk stratification. Diaphragmatic mobility and thickening fraction offer a bedside, noninvasive, and cost-effective alternative for perioperative PPC prediction, particularly in resource-limited settings.
Keywords: postoperative pulmonary complications, thoracic surgery, diaphragmatic mobility, diaphragmatic thickening fraction, prediction
Introduction
Postoperative pulmonary complications (PPCs), defined as respiratory adverse events occurring after anesthesia and surgery, exhibit highly variable incidence rates (6–80%) across different surgical populations.1–5 PPCs are the major cause of increased morbidity and mortality in chest and abdominal surgery patients, and therefore several scoring systems have been developed to predict their development, including the Assess Respiratory Risk in Surgical Patients in Catalonia score (ARISCAT score),5 the Score for Prediction of Postoperative Respiratory Complications (SPORC),6 and the Local Assessment of Ventilatory Management During General Anesthesia for Surgery (LAS VEGAS) risk score.7 However, these scoring systems are limited in clinical use due to diverse perioperative factors and variability across a wide range of surgical settings. Furthermore, recent studies show the ARISCAT score underestimates PPC risk in thoracic surgery (area under curve (AUC) 0.65 versus 0.72 for diaphragmatic ultrasound),8 as it omits real-time respiratory muscle function.9
Patients with diaphragmatic dysfunction exhibit significantly higher PPC rates than those without, demonstrating a dose-dependent relationship with surgical proximity to the diaphragm – strongly implicating diaphragmatic impairment as a key PPC etiology.5 Emerging evidence supports diaphragmatic functional assessment as a valuable predictor of PPCs across diverse procedures including thoracic surgery, major abdominal surgery, radical resection of esophageal cancer and Robot-Assisted Laparoscopic Prostatectomy.2,3,10,11 Diaphragmatic mobility and thickening fraction are particularly valuable because they directly quantify diaphragmatic contractility and reserve, offering real-time, noninvasive insights into respiratory muscle function that are not captured by conventional pulmonary tests. In this study, we investigated the association of diaphragmatic mobility and thickening fraction with PPCs in patients undergoing thoracic surgery, and evaluated their values in predicting PPCs, and established predictive models integrating independent risk factors and diaphragmatic mobility or thickening fraction. The aim is to provide a more accurate method for the prediction of PPCs in patients undergoing thoracic surgery.
Patients and Methods
Patients
This was a prospective, observational cohort study, which enrolled 109 consecutive patients undergoing thoracic surgery in Xinjiang Medical University Affiliated Tumor Hospital between January 2021 and June 2021. The patients were divided into the case group who occurred PPCs within 1–7 days after surgery and the control group who did not occur PPCs. This study was approved by the Ethical Committee of Xinjiang Medical University Affiliated Tumor Hospital (No.: K-2021058) and conducted strictly according to the guidelines of the Declaration of Helsinki. All patients provided written informed consent prior to the study commencement.
Inclusion and Exclusion Criteria
This study enrolled patients scheduled for elective thoracic surgery. The exclusion criteria included ① pre-existing neuromuscular or respiratory disorders, ② unavailable or suboptimal diaphragm ultrasound imaging, ③ patients incapable of cooperation due to cognitive dysfunction, psychiatric history, etc, and ④ patient or guardian refusal to participate.
Anesthesia and Postoperative Analgesia
Standard anesthesia protocols for thoracic surgery were followed for induction and maintenance. Tracheal tube selection was individualized based on patient characteristics, surgical requirements, and airway assessment, with fiberoptic bronchoscopy confirming proper positioning. Intraoperative lung-protective ventilation strategies were systematically implemented.
An intravenous analgesic pump was used for postoperative analgesia with sufentanil of 2 μg/h and butorphanol tartrate of 0.1 mg/h. When the Visual Analogue Scale (VAS) score of a patient in the resting state was ≥3, an additional intravenous injection of parecoxib sodium 40 mg or verbiprofen 50 mg was given.
Ultrasound Measurements
All patients underwent ultrasound measurements in the resting state in a semi-recumbent position on the day before surgery. The measurements of diaphragmatic mobility and thickening fraction were performed by the same operator, ie a trained sonographer. To reduce measurement bias, all measurements were repeated three times and averaged, with operators blinded to the clinical outcomes. Diaphragmatic mobility was assessed using a low-frequency convex ultrasound probe. The liver was regarded as the echographic window for the right hemidiaphragm, while the spleen as the echographic window for the left hemidiaphragm. The probe was fixed on the chest wall and was medially, cephalad, and dorsally directed to make the ultrasound beam to reach the posterior part of the hemidiaphragmatic dome. The excursion amplitude in the vertical axis of the hemidiaphragmatic dome was then observed in the motion mode (M-mode) to assess the diaphragmatic mobility.12 Diaphragmatic thickness was measured using a high-frequency linear ultrasound probe. The probe was placed perpendicular to the chest wall at the level between the seventh and ninth intercostal space to locate the diaphragm along the midaxillary line. Thickness was measured at the end of expiration (DTEE) and the end of inspiration (DTEI), and diaphragmatic thickening fraction (DTf) was computed as follows: DTf=(DTEI-DTEE)/ DTEE. The mean of operated side and nonoperated side was used as the final study indicator.12,13
Postoperative Pulmonary Complications
PPCs were followed up and recorded between the first to the seventh day after surgery by the attending physicians who were blinded to the ultrasound results. PPCs were comprised of acute respiratory failure, hypoxemia, atelectasis, suspected pulmonary infection, pleural effusion, and use of non-invasive mechanical ventilation exceeding the first postoperative day.
Statistical Analysis
SPSS version 26.0 (SPSS Inc., USA) was used to perform statistical analysis. Student’s t-test was used to perform intergroup comparisons of the quantitative data with a normal distribution, and Mann–Whitney U-test was used to perform intergroup comparisons of the quantitative data with a skewed distribution. Chi-square test was used to perform intergroup comparisons of the qualitative data. Variables with a P-value <0.10 in the univariate analysis were included in the binary logistic regression model for multivariate analysis. Backward selection was employed to refine the model and identify independent risk factors. The receiver operating characteristic (ROC) curve was used to evaluate predictive values, and Z test was used to perform the comparison of the area under curve (AUC). The optimal cutoff value was derived by maximizing Youden’s index (J), ie, J=Sensitivity+Specificity-1. A P value of <0.05 was considered significant.
Results
General Information
The average age of the whole cohort was 56.91±9.65 years, including 66 males (60.6%) and 43 females (39.4%). The surgical sites included the esophagus (36, 33.0%), lung (57, 52.3%), and mediastinum (16, 14.7%). Seventy patients were ranked in II according to American Society of Anesthesiologists (ASA) physical status classification system, and the remaining 36 patients were ranked in III–IV. Between the first to the seventh day after surgery, 46 patients (42.2%) occurred PPCs.
Univariate Analysis
Univariate analysis was conducted between the case group and control group, and the results (Table 1) demonstrated that the following variables were significantly different, including age, smoking, surgical sites, New York Heart Association (NYHA) functional classification, albumin, arterial oxygen saturation (SaO2), preoperative maximal voluntary ventilation (MVV), preoperative forced expiratory volume in the first second (FEV1), and mean diaphragmatic mobility and DTf of operated side and nonoperated side. However, ASA physical status classification had a P value of <0.10.
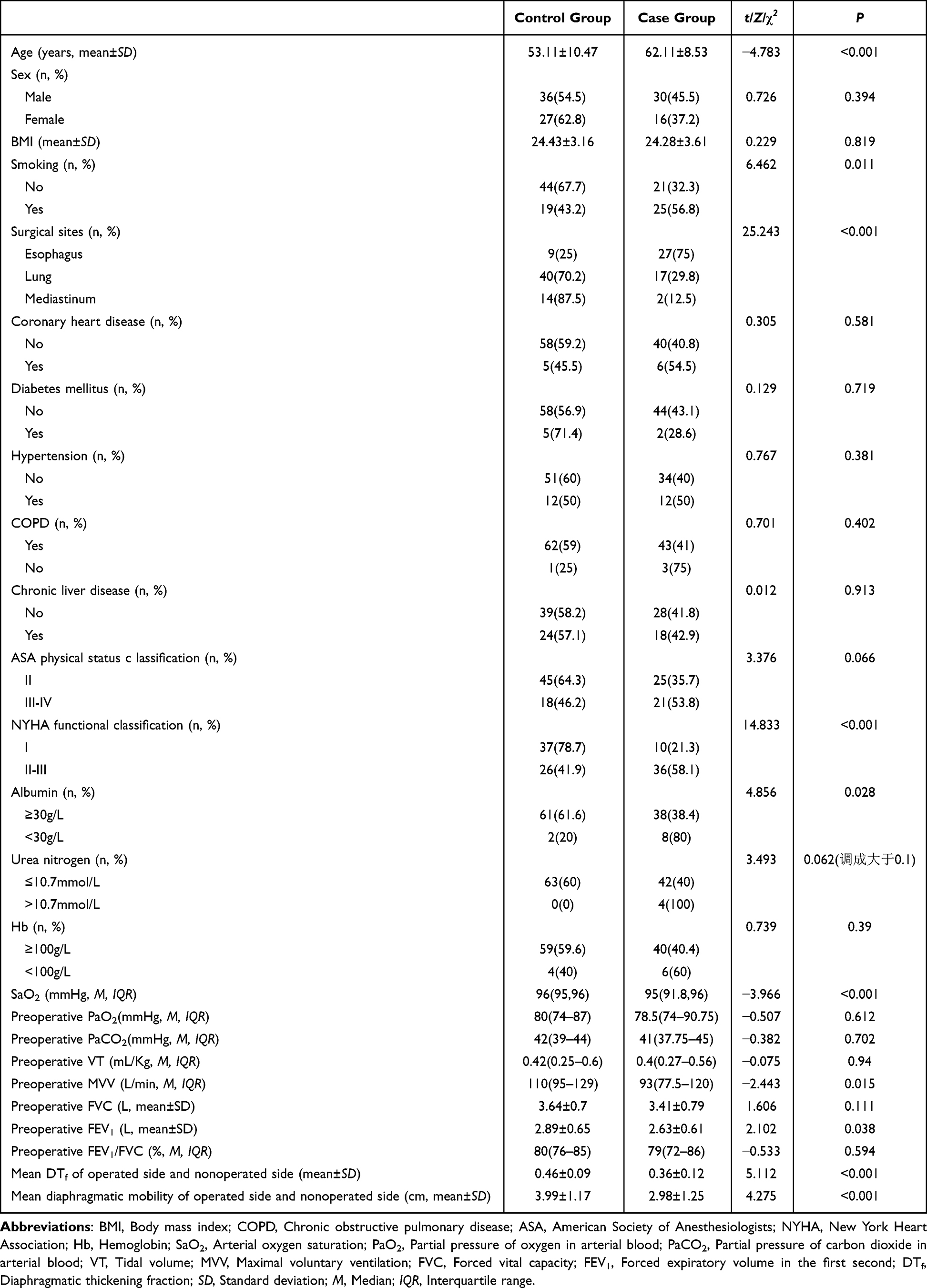 |
Table 1 Results of Univariate Analysis Between Case Group and Control Group |
Multivariate Analysis
Multivariate analysis was conducted for the variables with P<0.10 in univariate analysis, including age, smoking, surgical sites, NYHA functional classification, albumin, SpO2, preoperative MVV, preoperative FEV1, mean diaphragmatic mobility and DTf, and ASA physical status classification. As demonstrated in Table 2, the independent risk factors of PPCs in patients undergoing thoracic surgery included age, smoking, surgical sites, and mean diaphragmatic mobility and DTf of operated side and nonoperated side.
 |
Table 2 Results of Multivariate Analysis Results Between Case Group and Control Group |
Predictive Values
ROC curves (Figure 1) demonstrated that the AUC of mean diaphragmatic mobility and DTf for predicting PPCs in patients undergoing thoracic surgery was 0.722 [standard error (SE): 0.050, 95% confidence interval (CI): 0.623~0.821, P<0.001] and 0.757 (SE: 0.050, 95% CI: 0.659~0.855, P<0.001), respectively. The optimal cutoff values of diaphragmatic mobility and DTf were 3.26 cm and 0.39, respectively. As shown in Figure 2, the predictive model integrating age, smoking and surgical sites yielded an AUC of 0.810 (SE: 0.041, 95% CI: 0.728~0.891, P<0.001), while the predictive model integrating age, smoking, surgical sites and mean diaphragmatic mobility or DTf yielded an AUC of 0.849 (SE: 0.037, 95% CI: 0.777~0.922, P<0.001) and 0.881 (SE: 0.033, 95% CI: 0.815~0.946, P<0.001), respectively.
 |
Figure 1 ROC curves of mean diaphragmatic mobility and DTf for predicting PPCs in patients undergoing thoracic surgery. |
 |
Figure 2 ROC curves of predictive models integrating age, smoking, surgical sites and mean diaphragmatic mobility or DTf for predicting PPCs in patients undergoing thoracic surgery. |
Discussion
The diaphragm is the primary respiratory muscle, contributing more than 60% of thoracic volume changes during respiration.14 Among patients with diaphragmatic dysfunction, weakened cough ability results in worse pulmonary compliance and sputum retention, which may be correlated with respiratory infection and pneumonia.15–17 In addition, the impairment of pulmonary physiology causes reduced tidal volume and postoperative oxygenation index, possibly leading to postoperative hypoxemia.18–20 At the same time, patients with diaphragmatic dysfunction have respiratory mechanics and chest wall impairment due to lower inspiratory and transdiaphragmatic pressures.16,18 Respiratory mechanics and chest wall impairment combined with low tidal volume may contribute to the development of postoperative atelectasis.18,19 The above mechanisms may involve in the occurrence of PPCs.
The reference methods for assessing diaphragmatic function include transdiaphragmatic pressure assessment and phrenic nerve stimulation.21,22 However, the both methods are invasive and require considerable expertise. Furthermore, they are often unavailable at the bedside. Recently, point-of-care ultrasound has emerged as a noninvasive method for the assessment of diaphragmatic function.23,24 Studies showed that it is a superior tool in the diagnosis of diaphragmatic dysfunction among postoperative patients compared with magnetic resonance imaging and computed tomography due to its ability to provide dynamic observations and convenience.14,25 Moreover, its accuracy has been verified by the gold standard for assessing diaphragmatic function, ie transdiaphragmatic pressure assessment.13
Diaphragmatic mobility and thickening fraction have been proved to be important indicators of diaphragmatic function and correlate with PPCs in various settings.26–28 Kim et al reported that diaphragmatic inspiratory amplitude assessed by M-mode sonography demonstrated a significant association with vital capacity measured by spirometry throughout the postoperative period in patients undergoing open liver lobectomy and concluded that diaphragmatic inspiratory amplitude was a practical indicator of diaphragmatic dysfunction having ability to predict pulmonary dysfunction.26 Nørskov et al found significant reductions in diaphragmatic excursion on the surgical side of the thorax in patients undergoing thoracic surgery and indicated that a postoperative reduction in posterior diaphragmatic excursion of more than 50% was correlated with PPCs.10 Banerjee et al analyzed the association of diaphragmatic mobility and thickening with severity of interstitial lung disease, concluding that diaphragmatic excursion velocity during deep breathing had a weak to moderate association with pulmonary function parameters and might be used as an alternative marker in interstitial lung disease patients incapable of conducting pulmonary function tests.29 Spiliopoulos et al investigated the application of diaphragmatic thickening indicators in evaluating respiratory decompensation in amyotrophic lateral sclerosis. Their results demonstrated that all diaphragmatic thickening indicators were significantly associated with forced vital capacity, and diaphragmatic thickening fraction had higher AUC in predicting diaphragmatic dysfunction and the necessity for initiating of noninvasive ventilation.30
In our study, the incidence of PPCs was 41.3%, which was similar to that of other studies.31 Patients with PPCs had lower mean mobility and thickening fraction compared with those of patients without PPCs. Multivariate analysis showed that lower mean mobility and thickening fraction were independently associated with the occurrence of PPCs. ROC curves demonstrated that the AUC of mean mobility and thickening fraction in predicting PPCs was 0.722 and 0.757, respectively, having moderate predictive values. Moreover, the AUC of the prediction model integrating age, smoking, surgical type and mean mobility or thickening fraction was up to 0.881 and 0.849, respectively. The findings of this study highlight the practical utility of diaphragmatic ultrasound in perioperative risk stratification, particularly in resource-limited settings. Unlike traditional PPC prediction tools (eg, ARISCAT score) that rely on complex variables or laboratory tests, diaphragmatic mobility and thickening fraction offer a bedside, noninvasive, and cost-effective alternative. In low-resource hospitals where access to advanced pulmonary function tests or invasive diaphragmatic assessments (eg, phrenic nerve stimulation) is limited, ultrasound measurements can be rapidly performed using portable devices with minimal training.
Most previous studies used only one of mobility or thickening fraction to evaluate diaphragmatic function.6,7,10 Our study used the both indicators simultaneously. The results showed that the thickening fraction had a slightly higher AUC compared with the mobility (P>0.05), regardless of whether it was used alone or integrated into the prediction model. However, we found that the measurement of thickening fraction was more time-consuming and difficult compared with mobility in clinical practice. The reason for this is that most patients’ diaphragmatic thickness was between 3 and 7 mm, which makes the measurement of diaphragmatic thickness delicate and time-consuming. In addition, the measurement of diaphragmatic thickness requires high proficiency for operators and good coordination for patients. In contrast, the measurement of mobility is more simple and easier for patients to accept. Therefore, diaphragmatic mobility might be more applicable in clinical practice.
The main limitations of this study include two aspects. First, the relatively small sample size may limit the statistical power and generalizability of the findings. Second, potential confounders were not fully accounted for, including preoperative factors (eg, history of chronic lung disease), intraoperative variables (eg, surgical duration, anesthesia technique), and postoperative management (eg, mechanical ventilation use, early rehabilitation protocols). Future studies with larger cohorts and comprehensive covariate adjustments are needed to validate these results.
Conclusion
Both diaphragmatic mobility and thickening fraction independently predicted PPCs after thoracic surgery, exhibiting moderate predictive values. The predictive models integrating age, smoking, surgical sites and diaphragmatic mobility or thickening fraction yielded high predictive values, suggesting significant clinical utility for risk stratification. Diaphragmatic mobility and thickening fraction offer a bedside, noninvasive, and cost-effective alternative for perioperative PPC prediction, particularly in resource-limited settings.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors do not have any conflict of interest for this work.
References
1. Miskovic A, Lumb AB. Postoperative pulmonary complications. Br J Anaesth. 2017;118(3):317–334. doi:10.1093/bja/aex002
2. Fu X, Wang Z, Wang L, et al. Increased diaphragm echodensity correlates with postoperative pulmonary complications in patients after major abdominal surgery: a prospective observational study. BMC Pulm Med. 2022;22(1):400. doi:10.1186/s12890-022-02194-6
3. Liu F, Wen Q, Yang Y, et al. Diaphragmatic dysfunction is associated with postoperative pulmonary complications in the aged patients underwent radical resection of esophageal cancer: a prospective observational study. J Thorac Dis. 2024;16(6):3623–3635. doi:10.21037/jtd-24-197
4. Katsura M, Kuriyama A, Takeshima T, et al. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. 2015;2015(10):CD010356. doi:10.1002/14651858.CD010356.pub2
5. Canet J, Gallart L, Gomar C, et al; ARISCAT Group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010;113(6):1338–1350. doi:10.1097/ALN.0b013e3181fc6e0a
6. Brueckmann B, Villa-Uribe JL, Bateman BT, et al. Development and validation of a score for prediction of postoperative respiratory complications. Anesthesiology. 2013;118(6):1276–1285. doi:10.1097/ALN.0b013e318293065c
7. Neto AS, da Costa LGV, Hemmes SNT, et al; LAS VEGAS. The Las Vegas risk score for prediction of postoperative pulmonary complications: an observational study. Eur J Anaesthesiol. 2018;35(9):691–701. doi:10.1097/EJA.0000000000000845
8. Lee HJ, Park SY, Kim YT, et al. Diaphragmatic ultrasound versus ARISCAT score for predicting pulmonary complications after lung resection: a multicenter validation study. Chest. 2023;164(4):789–798. doi:10.1016/j.chest.2023.02.032
9. Zhang Y, Li X, Wang L, et al. Limitations of ARISCAT score in predicting postoperative pulmonary complications after thoracic surgery: a prospective observational study. Ann Thorac Surg. 2023;115(1):223–230. doi:10.1016/j.athoracsur.2022.08.045
10. Nørskov J, Skaarup SH, Bendixen M, et al. Diaphragmatic dysfunction is associated with postoperative pulmonary complications and phrenic nerve paresis in patients undergoing thoracic surgery. J Anesth. 2024;38(3):386–397. doi:10.1007/s00540-024-03325-5
11. Yu J, Lee Y, Park J-Y, et al. Diaphragm thickening fraction as a prognostic imaging marker for postoperative pulmonary complications in robot-assisted laparoscopic prostatectomy requiring the trendelenburg position and pneumoperitoneum. Dis Markers. 2021;2021:9931690. doi:10.1155/2021/9931690
12. Matamis D, Soilemezi E, Tsagourias M, et al. Sonographic evaluation of the diaphragm in critically ill patients. technique and clinical applications. Intensive Care Med. 2013;39(5):801–810. doi:10.1007/s00134-013-2823-1
13. Goligher EC, Laghi F, Detsky ME, et al. Measuring diaphragm thickness with ultrasound in mechanically ventilated patients: feasibility, reproducibility and validity. Intensive Care Med. 2015;41(4):734. doi:10.1007/s00134-015-3724-2
14. Scarlata S, Mancini D, Laudisio A, et al. Reproducibility and clinical correlates of supine diaphragmatic motion measured by M-mode ultrasonography in healthy volunteers. Respiration. 2018;96(3):259–266. doi:10.1159/000489229
15. Laghi F, Tobin MJ. Disorders of the respiratory muscles. Am J Respir Crit Care Med. 2003;168(1):10–48. doi:10.1164/rccm.2206020
16. Norisue Y, Santanda T, Homma Y, et al. Ultrasonographic assessment of passive cephalic excursion of diaphragm during cough expiration predicts cough peak flow in healthy adults. Respir Care. 2019;64(11):1371–1376. doi:10.4187/respcare.06780
17. Takeda S, Nakahara K, Fujii Y, et al. Effects of diaphragmatic plication on respiratory mechanics in dogs with unilateral and bilateral phrenic nerve paralyses. Chest. 1995;107(3):798–804. doi:10.1378/chest.107.3.798
18. Spadaro S, Grasso S, Dres M, et al. Point of care ultrasound to identify diaphragmatic dysfunction after thoracic surgery. Anesthesiology. 2019;131(2):266–278. doi:10.1097/ALN.0000000000002774
19. Jung KJ, Park JY, Hwang DW, et al. Ultrasonographic diaphragmatic motion analysis and its correlation with pulmonary function in hemiplegic stroke patients. Ann Rehabil Med. 2014;38(1):29–37. doi:10.5535/arm.2014.38.1.29
20. Moury PH, Cuisinier A, Durand M, et al. Diaphragm thickening in cardiac surgery: a perioperative prospective ultrasound study. Ann Intensive Care. 2019;9(1):50. doi:10.1186/s13613-019-0521-z
21. Dres M, Goligher EC, Heunks LMA, et al. Critical illness-associated diaphragm weakness. Intensive Care Med. 2017;43(10):1441–1452. doi:10.1007/s00134-017-4928-4
22. Dubé BP, Dres M, Mayaux J, et al. Ultrasound evaluation of diaphragm function in mechanically ventilated patients: comparison to phrenic stimulation and prognostic implications. Thorax. 2017;72(9):811–818. doi:10.1136/thoraxjnl-2016-209459
23. Zambon M, Greco M, Bocchino S, et al. Assessment of diaphragmatic dysfunction in the critically ill patient with ultrasound: a systematic review. Intensive Care Med. 2017;43(1):29–38. doi:10.1007/s00134-016-4524-z
24. Spadaro S, Grasso S, Mauri T, et al. Can diaphragmatic ultrasonography performed during the T-tube trial predict weaning failure? The role of diaphragmatic rapid shallow breathing index. Crit Care. 2016;20(1):305. doi:10.1186/s13054-016-1479-y
25. Laghi FA, Saad M, Shaikh H. Ultrasound and non-ultrasound imaging techniques in the assessment of diaphragmatic dysfunction. BMC Pulm Med. 2021;21(1):85. doi:10.1186/s12890-021-01441-6
26. Kim SH, Na S, Choi JS, et al. An evaluation of diaphragmatic movement by M-mode sonography as a predictor of pulmonary dysfunction after upper abdominal surgery. Anesth Analg. 2010;110(5):1349–1354. doi:10.1213/ANE.0b013e3181d5e4d8
27. Oh YJ, Lee JR, Choi YS, et al. Randomized controlled comparison of combined general and epidural anesthesia versus general anesthesia on diaphragmatic function after laparoscopic prostatectomy. Min Anestesiol. 2013;79(12):1371–1380.
28. Lerolle N, Guérot E, Dimassi S, et al. Ultrasonographic diagnostic criterion for severe diaphragmatic dysfunction after cardiac surgery. Chest. 2009;135(2):401–407. doi:10.1378/chest.08-1531
29. Banerjee S, Sanjan G, Sharma P, et al. Correlation of diaphragmatic mobility and thickening assessed by lung ultrasound with severity of interstitial lung disease. Lung India. 2024;41(5):345–352. doi:10.4103/lungindia.lungindia_139_24
30. Spiliopoulos KC, Lykouras D, Veltsista D, et al. The utility of diaphragm ultrasound thickening indices for assessing respiratory decompensation in amyotrophic lateral sclerosis. Muscle Nerve. 2023;68(6):850–856. doi:10.1002/mus.27980
31. Young CC, Harris EM, Vacchiano C, et al. Lung-protective ventilation for the surgical patient: international expert panel-based consensus recommendations. Br J Anaesth. 2019;123(6):898–913. doi:10.1016/j.bja.2019.08.017
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.