")
Back to Journals » Nature and Science of Sleep » Volume 17
Association of Weight Change Across Adulthood with Obstructive Sleep Apnea: The Multi-Ethnic Study of Atherosclerosis
Authors Du J, Zhao W, Liu Y, Li S, Zhang Z, Zhou Y, Sun W, Ai H, Nie S, Gong W
Received 7 February 2025
Accepted for publication 28 May 2025
Published 6 June 2025 Volume 2025:17 Pages 1191—1204
DOI https://doi.org/10.2147/NSS.S520901
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sarah L Appleton
Jiaqi Du,1 Wenlong Zhao,1 Yixiang Liu,1 Siyi Li,1 Zekun Zhang,1 Yun Zhou,1 Wenrui Sun,1 Hui Ai,1 Shaoping Nie,1 Wei Gong2
1Center for Coronary Artery Disease, Division of Cardiology, Beijing Anzhen Hospital, Capital Medical University, National Clinical Research Center for Cardiovascular Diseases, Beijing Institute of Heart, Lung, and Blood Vessel Diseases, Beijing, People’s Republic of China; 2Department of Cardiology, Beijing Hospital, National Center of Gerontology, Institute of Geriatric Medicine, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China
Correspondence: Wei Gong, Department of Cardiology, Beijing Hospital, No. 1 Dahua Road, Dongdan, Dongcheng District, Beijing, 100730, People’s Republic of China, Email [email protected] Shaoping Nie, Center for Coronary Artery Disease, Division of Cardiology, Beijing Anzhen Hospital, Capital Medical University, No. 2 Anzhen Road, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Purpose: The association between weight change across adulthood and obstructive sleep apnea (OSA) is unclear. This study aimed to evaluate the effect of weight change across adulthood on OSA and subsequent mortality.
Methods: This study included 2019 participants of the Multi-Ethnic Study of Atherosclerosis (MESA). Weight at ages 20 and 40 was recalled at Exam 1, and height and weight were measured in Exam 5 and used to calculate current body mass index (BMI). Home-based polysomnography was conducted for each enrolled participants in the MESA Sleep Study immediately following Exam 5. The relationship between changes in BMI across adulthood and the risk of OSA was investigated using logistic regression and restricted cubic splines. In addition, the association between BMI change and all-cause mortality was examined using Cox regression.
Results: Of 2019 participants (median age: 67 years; 930 [46.1%] men), 970 (48.0%) had OSA. Compared to the non-OSA group, participants in the OSA group were older, more often male, and had greater weight changes across adulthood. Logistic regression showed that increased BMI across adulthood was an independent risk factor for OSA. Further studies showed that both mild (0– 10%) and significant (> 10%) increases in BMI between the ages of 20 and 40 were associated with a higher risk of OSA, and this finding remained after adjustment for current BMI. Subgroup analyses showed consistent results for participants with current BMI < 30 or ≥ 30. In addition, weight gain from age 20 to 40 was also associated with an increased mortality risk after OSA diagnosis.
Conclusion: Weight gain in early adulthood was associated with a higher risk of OSA and subsequent mortality, regardless of weight status in later life. Therefore, maintaining a normal body weight in early adulthood should be actively promoted to prevent OSA and improve prognosis.
Keywords: weight change, early adulthood, obstructive sleep apnea, prognosis
Introduction
Obesity has become a global public health problem. Epidemiological studies have shown that global obesity rates increased from 3% in men and 6% in women to 11% and 15%, respectively, between 1975 and 2016.1 The World Obesity Atlas showed that about 2.2 billion adults and 430 million children were overweight/obese globally in 2020, and it is projected to reach 3.3 billion and 770 million respectively by 2035. Therefore, weight control, especially early weight control, is of great public health importance.
Obesity is the most important risk factor for obstructive sleep apnea (OSA), and about 50–60% of obese individuals have comorbid OSA.2,3 Back in 2003, Tishler et al found that body mass index (BMI) was a risk factor for sleep-disordered breathing and that its effect decreased with age.4 Obesity can increase the risk of OSA through several pathophysiological mechanisms. First, obesity leads to fat accumulation in the neck, thereby increasing the risk of upper airway collapse.5 Additionally, abnormal visceral fat deposition can raise intra-abdominal pressure, which in turn affects diaphragmatic movement.6 Obese individuals are also more prone to ventilatory control imbalances, leading to a reduction in functional residual lung capacity, further heightening the risk of OSA.7 Genetic factors also play a significant role in the development of obesity and OSA, with related genes potentially influencing energy metabolism, appetite regulation, and adipocyte differentiation.8 However, previous studies have only discussed the association between body weight at a single measurement and the risk of OSA, ignoring the effect of dynamic changes in body weight at different stages on OSA. A recent study showed that individuals who went from normal weight to obese between early and middle adulthood had a higher risk of all-cause and cardiovascular death. In contrast, in middle to late adulthood, weight loss was independently associated with mortality.9 However, no relevant studies have reported the effect of weight changes in adulthood on OSA.
The Multi-Ethnic Study of Atherosclerosis (MESA) is a multicenter prospective study designed to investigate the characteristics and predictors of subclinical atherosclerosis.10 The ethnic diversity, validated home-based polysomnography (PSG), and long-term follow-up of the MESA make it an excellent choice for studying the risk factor and prognosis of OSA. Using data from its primary and ancillary studies, we explored the effect of weight change at different stages of adulthood on OSA and subsequent mortality. This study aims to improve the early screening and diagnosis of OSA and further emphasize the importance of early weight control, which has certain public health significance.
Methods
Study Design and Population
The MESA is a multicenter prospective study designed to investigate the characteristics and prognosis of subclinical cardiovascular disease and the risk factors for its progression to clinically overt cardiovascular disease. Between July 2000 and August 2002, the study enrolled 6814 community-dwelling participants without evidence of cardiovascular disease from six field centers in the United States. The study was approved by the Institutional Review Board, written informed consent was obtained from all participants, and detailed methodology has been previously published.10–12 This post-hoc analysis of MESA was approved by the Institutional Review Board of Beijing Anzhen Hospital, Capital Medical University (No. KS2024028), with a waiver of informed consent granted for the retrospective use of de-identified data.
Enrolled participants received a total of 5 exams at 2-year intervals. After completing Exam 5 (2010–2013), 4077 participants were invited to participate in the MESA Sleep Study (2010–2012), of whom 1816 were excluded due to ineligibility or inability to participate. The MESA Sleep Study consisted of a home-based PSG, sleep questionnaire and diary, and actigraphy for the following 7 days. Of the 2261 participants in the MESA Sleep Study, 2057 had successful PSG data. In addition, 13 participants with central sleep apnea and 25 participants with missing data were excluded, and 2019 participants were included in the final analysis (Figure 1).
 |
Figure 1 Participant inclusion flowchart. Abbreviations: Mesa, the Multi-Ethnic Study of Atherosclerosis; PSG, polysomnography. |
PSG and OSA Definition
Home-based PSG was performed using the Somte System (Compumedics, Australia), which recorded electroencephalogram, airflow, finger pulse oximetry, leg movement, and other data. In this study, apnea was defined as a complete reduction in airflow amplitude for ≥ 10s. Hypopnea was defined as a > 30% reduction in airflow amplitude for ≥ 10s accompanied by a 4% oxygen desaturation. Apnea-hypopnea index (AHI) was defined as the number of apneas and hypopneas per hour of total recording time. According to guidelines of the Adult Obstructive Sleep Apnea Task Force of the American Academy of Sleep Medicine,13 ≥ 15 obstructive respiratory events per hour in the absence of sleep-related symptoms is sufficient for the diagnosis of OSA. Several studies have also found that OSA diagnosed using an AHI ≥15/h as a cut-off value was strongly associated with future cardiovascular events.14,15 Therefore, for this analysis, participants were divided into an OSA group (AHI ≥15/h) and a non-OSA group (AHI <15/h).
Assessment of BMI and Covariates
Figure 2 provides information on data items and chronology of the data collection. BMI was calculated by dividing weight (kg) by the square of height (m2). The height and weight of all participants were measured at Exam 5, from which the current BMI was calculated. In addition, weight at ages 20 and 40 was recalled at Exam 1 (median age 58 years), while height at Exam 1 was used as a proxy to calculate BMI at ages 20 and 40. We also calculated the change in BMI for two-time intervals: ΔBMI from age 20 to 40, and ΔBMI from age 40 to current.
 |
Figure 2 Flow diagram of data collection timeline and information gathered. Abbreviations: BMI, body mass index; OSA, obstructive sleep apnea; Mesa, the Multi-Ethnic Study of Atherosclerosis; PSG, polysomnography. |
Demographic characteristics, medical history, and family history were collected at Exam 5. Both smoking and drinking status were divided into three categories: never, previous, and current use. Hypertension was defined as seated systolic blood pressure ≥140 mmHg and/or diastolic blood pressure ≥90 mmHg. Diabetes was defined as fasting glucose level ≥7 mmol/L and/or use of any oral hypoglycemic agents or insulin.
Outcome and Follow-up
From 2000 to 2015, the MESA study followed participants by telephone, surface mail, or electronic mail. The follow-up endpoint was the occurrence of the outcome event or the end of 2015. We analyzed follow-up data after the MESA Sleep Study, with an average follow-up of 4.0 years. The outcome for this analysis was all-cause mortality, as most of the other outcomes had occurred before the MESA Sleep Study.
Statistical Analysis
Normally distributed variables were described as mean and standard deviation, and comparisons between groups were made using the independent samples t-test. Variables with skewed distributions were described as medians (quartile 1, quartile 3), and comparisons were made using the Mann–Whitney U-test. Categorical variables were shown as numbers (percentages) and were compared by χ2 test. Pearson’s correlation coefficients were calculated between BMI and its change in adulthood and AHI. Multivariate logistic regression was used to assess the association of BMI and its changes in adulthood with OSA, while restricted cubic splines (RCS) were used to explore possible non-linear correlations. In addition, logistic regression was used to explore the association between BMI change patterns and absolute weight gain with OSA. Cox regression was used to assess the association between BMI and its change with all-cause mortality in both OSA and non-OSA patients, and RCS were used to describe the dose-response relationship. In the multivariate regression analysis, Model 1 was adjusted for current age, sex, and race; Model 2 was adjusted for Model 1 plus education, income, smoking status, hypertension, and diabetes; Model 3 was adjusted for Model 2 plus BMI before change; and Model 4 was further adjusted for current BMI. To demonstrate the robustness of the results, the stratified analyses of associations between BMI change pattern and OSA by current age, sex, and current BMI were performed. Furthermore, the sensitivity analysis also took into account the participants who self-reported a previous diagnosis of OSA and different diagnostic criteria for OSA. A P value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS 26.0 (IBM Corp., NY, USA) and R software 4.3.2 (R Foundation, Vienna, Austria).
Results
Clinical Characteristics and BMI Changes of OSA and Non-OSA Groups
A total of 2019 participants were included in the final analysis, with a median age of 67 years. Table 1 demonstrates the clinical characteristics of participants in the OSA and non-OSA groups. In terms of demographic characteristics, participants in the OSA group were older, more likely to be male, Hispanic, or Chinese, less educated, and current drinkers. Regarding medical history, a higher proportion of participants in the OSA group had comorbid hypertension and diabetes. For PSG data, patients in the OSA group had significantly higher AHI and percentage of time spent at SaO2 below 90% (T90), while the average and minimum oxygen saturation during sleep were lower than in non-OSA patients. For anthropometric indicators, participants in the OSA group had greater weight and BMI at all three time points in adulthood. For all participants, the changes in BMI from age 20 to 40 and age 40 to current were 2.8 (1.4, 5.0) and 2.8 (0.7, 5.5) kg/m2, respectively. In particular, participants in the OSA group had a greater increase in BMI than participants in the non-OSA group in adulthood, which led to an increasing weight gap between the two groups (Figure 3A). There was no statistically significant difference between the two groups in the remaining characteristics. The results of the correlation analysis showed a linear correlation between the 20’s, 40’s and current BMI, with correlation coefficients ranging from 0.401 to 0.667 (Supplementary Table 1).
 |
Table 1 Clinical Characteristics for Participants Stratified by OSA Status |
 |
Figure 3 Changes in body weight across adulthood. (A) BMI at age 20, 40 and current age in OSA and non-OSA groups; (B) Proportion of BMI increase patterns across adulthood; (C) Proportion of weight gain patterns across adulthood. Abbreviations: BMI, body mass index; OSA, obstructive sleep apnea. |
The Relationship Between BMI and Its Changes in Adulthood and OSA
Of the 2019 participants enrolled, 970 (48.0%) were diagnosed with OSA. Logistic regression showed that greater BMI and its increase in adulthood (20’s, 40’s and current) were the risk factors for OSA, which still held true after adjusting for confounders such as age, sex, and race (Table 2). Meanwhile, the RCS curves showed a progressive increase in the risk of OSA with increasing BMI and its changes in adulthood. Among them, there was a non-linear correlation between the change in BMI from age 20 to 40 and the risk of OSA (Figure 4).
 |
Table 2 Odds Ratios (95% Confidence Intervals) for OSA Associated with BMI and Its Changes During Adulthood (Treated as a Continuous Variable) |
 |
Figure 4 Restricted cubic splines of BMI and its changes across adulthood with OSA. (A) BMI at age 20; (B) BMI at age 40; (C) Current BMI; (D) ΔBMI from age 20 to 40; (E) ΔBMI from age 40 to current. Abbreviations: BMI, body mass index. Notes: Model was adjusted for current age, sex, race, education, income, smoking status, hypertension, and diabetes. |
To further investigate the relationship between BMI change pattern in adulthood and OSA, participants were divided into 3 groups: decreased/no increase in BMI, mild increase in BMI (0–10%), and significant increase in BMI (>10%). Between the ages of 20 and 40, only 10.8% of the participants had a decreased/no increase in BMI; the proportions of mild and significant increases in BMI were 29.8% and 59.4%, respectively, higher than after the age of 40 (Figure 3B). Logistic regression showed that increased BMI during this period was associated with a higher risk of OSA. Surprisingly, this result held after adjustment for current BMI. From age 40 to current, the increase in BMI also increased the risk of OSA, but the OR was consistently smaller than that from age 20 to 40 (Table 3). The results of the correlation analyses showed a weak positive correlation between BMI and its change with AHI at all stages of adulthood (Supplementary Table 1).
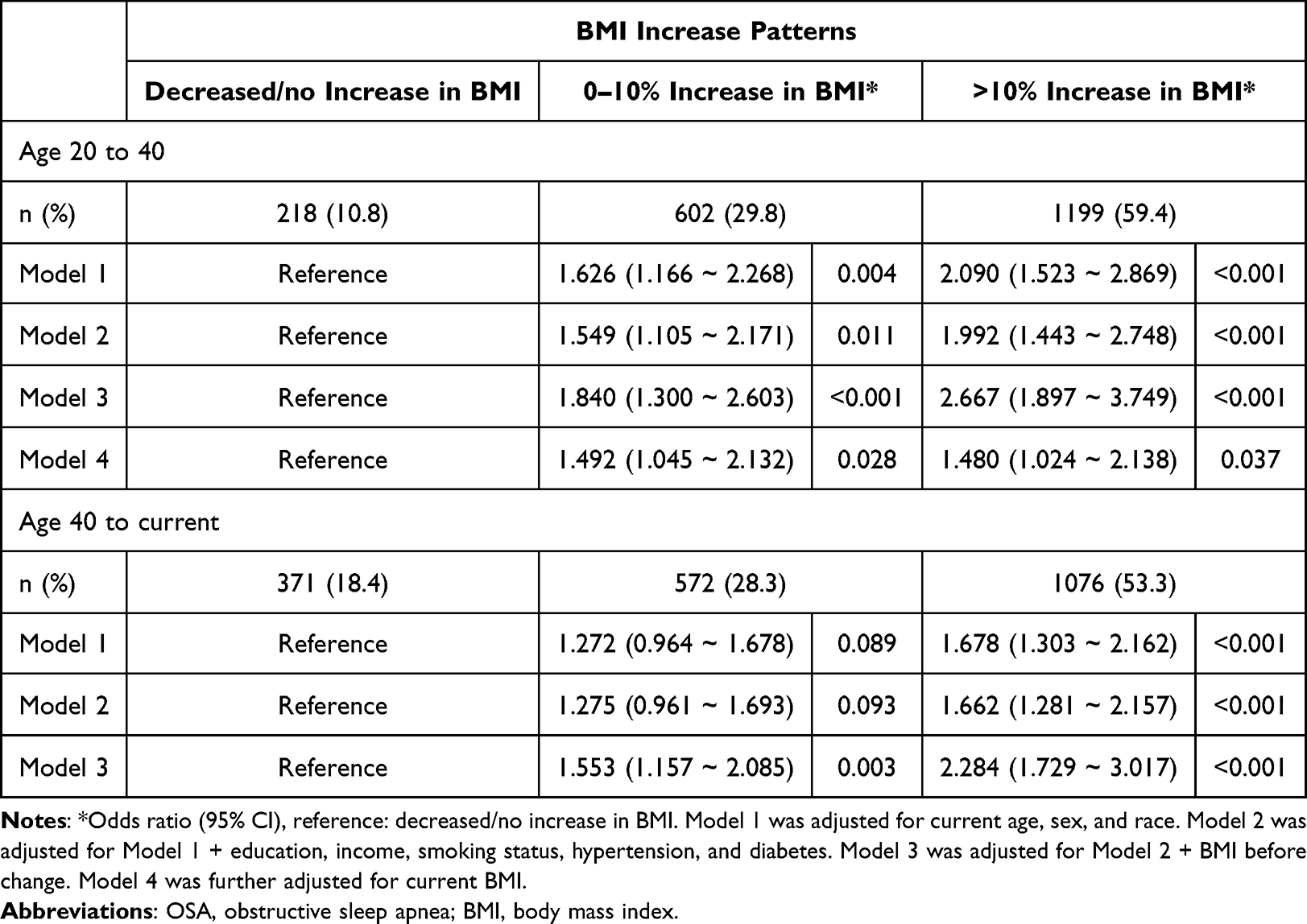 |
Table 3 Odds Ratios (95% Confidence Intervals) for OSA Associated with BMI Increase Patterns During Adulthood (Treated as Categorical Variables) |
The relationship between absolute weight gain and the risk of OSA was also investigated. Between the ages of 20 and 40, the proportion of weight loss/no weight gain was only 10.8%. In contrast, the proportions of participants who gained 0–10 kg and >10 kg reached 50.9% and 38.3%, respectively, higher than after the age of 40 (Figure 3C). The risk of OSA was 1.934 and 3.134 times higher in participants with a weight gain of 0–10 kg and >10 kg, compared with those with weight loss/no weight gain. After adjusting for current BMI, the effect of weight gain on OSA remained significant. From age 40 to current, weight gain also increased the risk of OSA, but its effect appeared to be less than it is during the age 20 to 40 (Table 4). In addition, there were significant differences in PSG data such as AHI and T90 for patients with different BMI increase patterns and weight gain patterns, as shown in Supplementary Tables 2–3.
 |
Table 4 Odds Ratios (95% Confidence Intervals) for OSA Associated with Weight Gain Patterns During Adulthood (Treated as Categorical Variables) |
Association of BMI and Its Changes with All-Cause Mortality
Participants were followed for an average of 4.0 years after the MESA-Sleep study. A total of 87 (4.3%) all-cause deaths occurred during follow-up, including 51 (5.3%) in the OSA group and 36 (3.4%) in the non-OSA group (P = 0.044). For participants in the OSA group, BMI at age 40 years and change from age 20 to 40 were independent risk factors for all-cause mortality. After adjusting for current BMI, increasing BMI between the ages of 20 and 40 was still associated with a higher risk of death. In contrast, change in BMI from age 40 to current was a somewhat protective factor for all-cause mortality (Table 5). The RCS curves showed a consistent conclusion that weight gain from age 20 to 40 and weight loss after age 40 increased the risk of all-cause mortality (Figure 5). For participants without OSA, the relationship between weight change and all-cause mortality was similar to that of OSA patients, as shown in Table 5 and Supplementary Figure 1. The main findings of this study are visually summarized in the Graphical Summary, which highlights the key relationships between BMI changes and OSA risk and mortality.
 |
Table 5 Hazard Ratios (95% Confidence Intervals) for Mortality Associated with BMI and Its Changes During Adulthood (Treated as Continuous Variables) |
 |
Figure 5 Restricted cubic splines of BMI and its changes with mortality in patients with OSA. (A) BMI at age 20; (B) BMI at age 40; (C) Current BMI; (D) ΔBMI from age 20 to 40; (E) ΔBMI from age 40 to current. Abbreviations: BMI, body mass index. Notes: Model was adjusted for current age, sex, race, education, income, smoking status, hypertension, and diabetes. |
Sensitivity Analysis
To make the results more reliable, sensitivity analyses were performed by stratifying by age, sex and current BMI. For ΔBMI from age 20 to 40, the effect on OSA was consistent across age, sex, and current BMI subgroups (Supplementary Tables 4–6). The relationship between the BMI increase pattern in early adulthood and OSA was consistent across age and sex subgroups, and this relationship varied between current BMI subgroups, but all were statistically significant (Supplementary Tables 7–9). The relationship between weight gain pattern and OSA was similar to the BMI increase pattern, as shown in Supplementary Tables 10–12. Furthermore, we excluded 93 participants who self-reported a previously diagnosed sleep apnea in Exam 4 (median age 63 years), and the main results were consistent with the overall population, as shown in Supplementary Tables 13–15. When using an AHI ≥5/h as the diagnostic threshold of OSA, the main results remained unchanged, as shown in Supplementary Tables 16.
Discussion
In post-hoc analyses of this large prospective cohort study, we found independent associations between changes in BMI at different stages of adulthood and the risk of OSA. Regardless of weight status in later life, weight gain in early adulthood significantly increased the risk of OSA. Furthermore, increasing BMI in early adulthood also increased the risk of all-cause mortality, both in patients with and without OSA. The results of this study highlight the importance of weight control in early adulthood in preventing OSA and improving the prognosis, and suggest that early screening for OSA in high-risk groups, such as obese individuals, is essential.
Weight changes vary at different stages of adulthood. Weight gain is more rapid in early adulthood, when overweight and obesity tend to accumulate. In contrast, body weight tends to stabilize or even decrease in middle to late adulthood.16,17 In this study, we found that the proportion of mild and significant increases in BMI reached 29.8% and 59.4% between the ages of 20 and 40, which is higher than after the age of 40. In addition, previous studies have shown that once a person becomes obese, it is difficult to lose weight and keep it off over time.18,19 In this study, 957 (47.4%) participants were overweight/obese at the age of 40, of whom only 6.7% became normal weight in late adulthood (median age 67 years). These results suggested that preventing weight gain in early adulthood may be more meaningful and feasible than losing weight later in life.
There is a strong link between obesity and OSA. Epidemiological studies have shown that about half of patients with OSA are obese.20 And in severely obese individuals, the prevalence of OSA can be as high as 40–90%.21 Obesity increases the risk of OSA by affecting upper airway anatomy, lung volume, and stability of respiratory control, while OSA can cause reduced physical activity, increased appetite, and insulin resistance, leading to further weight gain.22,23 Our study showed consistent results: BMI and its increase were consistently greater in OSA patients than in non-OSA patients. And BMI at different stages in adulthood (20’s, 40’s, and current (median age 67 years)) was positively associated with the risk of OSA, suggesting that weight control throughout adulthood has implications for the prevention of OSA.
As early as 1999, a retrospective study found that patients with OSA were more likely to have experienced weight gain in the year prior to diagnosis.24 Based on a longitudinal cohort of the Sleep Heart Health Study, Newman et al found an association between changes in body weight and changes in the respiratory disturbance index;25 however, the study focused only on the relationship over a 5-year interval, leaving the long-term association throughout adulthood unclear. Our study found that the change in BMI from age 20 to 40 and from age 40 to current was an independent risk factor for OSA, suggesting that not only BMI itself but also its dynamic changes deserve our attention. To further explore the effects of BMI changes at different stages of adulthood on OSA, we defined three patterns of BMI increase (see Methods for details). The results showed that both mild and significant increases in BMI from age 20 to 40 were significantly associated with OSA, regardless of current BMI. After the age of 40, the association between BMI increase and OSA remains, but appears to weaken with age. We also examined the association of absolute weight gain with OSA and found results consistent with the BMI increase pattern. This finding suggests that weight control in early adulthood is critical for the prevention of OSA. Possible reasons are as follows: Redistribution of bodily fat away from the extremities towards the trunk usually occurs during adolescence and early adulthood, and this process is more rapid in males.26 Besides, early obesity may be accompanied by a longer-term accumulation of metabolic disorders such as diabetes and hypertension, jointly leading to the occurrence of OSA.27 The “metabolic memory” effect may explain the legacy effect induced by weight gain in early adulthood, which can increase the risk of OSA independently of late-life weight via insulin resistance, low-grade inflammation, and other pathways.28
The association between weight in adulthood and prognosis has been discussed in several previous studies.29,30 A prospective study in the United States found that overweight and obese participants in early adulthood (age 21) had a 19% and 64% higher mortality rate, respectively, than normal-weight individuals.31 Another study of more than 120,000 participants without cardiovascular disease found that being overweight or obese in mid-adulthood (average age 51.4 years) significantly increased the risk of cardiometabolic multimorbidity over the next 10 years.32 Similar results were found in our study: BMI at age 20 and 40 was an independent risk factor for all-cause mortality. In addition, due to the high variability of body weight in adulthood, many studies have also explored the association between BMI changes and prognosis during this period. A prospective cohort study found that both weight gain from early to middle adulthood and weight loss from middle to late adulthood were associated with an increased mortality risk, suggesting that weight changes at different times may have different prognostic implications.9 In this study, we found that increased BMI from 20 to 40 years of age was an independent risk factor of all-cause mortality, regardless of current BMI. In contrast, weight loss rather than weight gain from middle to late adulthood was significantly associated with mortality risk. Combining the effects of weight change in adulthood on OSA and prognosis, it is reasonable to assume that early adulthood is a critical period for weight control.
There is no sufficient evidence that treatments such as continuous positive airway pressure can improve the cardiovascular prognosis of patients with OSA, and existing randomized controlled trials such as the SAVE and RICCADSA trials have all produced negative results.33–35 Therefore, we should pay more attention to the prevention of OSA. The results of this study suggest that maintaining a normal body weight in adulthood, especially in early adulthood, should be actively encouraged to reduce the risk of OSA. At the same time, for individuals who experience significant weight gain in adulthood, particularly in early adulthood (eg, BMI increase >10% or weight gain >10 kg), early OSA screening should be actively conducted to minimize the potential health impact. Developing OSA screening tools and algorithms based on individual weight history for high-risk populations is highly meaningful and will be one of our next steps. To our knowledge, this study is the first to assess the relationship between weight change in adulthood and the risk of OSA. Given the current pandemic trends of obesity and OSA, more relevant studies are needed in the future to provide sufficient evidence to support prevention, screening, and prognostic improvement.
This study also has some limitations: firstly, we used self-reported body weight at 20 and 40 years of age, which may be different from actual values. However, some studies have demonstrated the validity and reliability of self-reported body measurements by comparing them with prospectively measured body measurements. Second, the screening for OSA in this study was done later, which means that the age of diagnosis of OSA may be later than the age of onset. However, we excluded participants with self-reported previous diagnoses of sleep apnea in sensitivity analysis, and the results remained robust. Third, the outcome for this analysis was all-cause mortality only, as most of the other outcomes occurred before the MESA Sleep Study and could not be analyzed.
Conclusion
This study found that weight gain in early adulthood was associated with a higher risk of OSA and subsequent mortality, regardless of weight status in later life. This suggests that accumulation of excess weight during this critical period may increase the risk of OSA by altering upper airway anatomy, increasing fat distribution, and impairing respiratory control. Therefore, it is crucial to actively promote healthy weight maintenance in young adults, incorporating early screening, lifestyle counseling, and targeted interventions. These proactive strategies could play a key role in preventing OSA and improving long-term health conditions.
Abbreviations
OSA, obstructive sleep apnea; BMI, body mass index; MESA, the Multi-Ethnic Study of Atherosclerosis; PSG, polysomnography; AHI, apnea-hypopnea index; RCS, restricted cubic splines; T90, time spent at SaO2 below 90%.
Data Sharing Statement
Data for this study were derived from the MESA, available at the National Heart, Lung, and Blood Institute BioLINCC data repository. Researchers can apply for access to this database by visiting https://biolincc.nhlbi.nih.gov/home.
IRB Approval
This study conformed to the recommendations in the Declaration of Helsinki. The Institutional Review Board of Beijing Anzhen Hospital, Capital Medical University granted ethical approval (No. KS2024028) for this post-hoc analysis and waived the requirement for informed consent, as the study involved retrospective analysis of de-identified data.
Acknowledgments
The authors are indebted to the investigators at MESA and to the patients who participated and made this study possible. The MESA Sleep Study was funded by NIH-NHLBI Association of Sleep Disorders with Cardiovascular Health Across Ethnic Groups (RO1 hL098433). MESA is supported by NHLBI funded contracts HHSN268201500003I, N01-HC-95159, N01-HC-95160, N01-HC-95161, N01-HC-95162, N01-HC-95163, N01-HC-95164, N01-HC-95165, N01-HC-95166, N01-HC-95167, N01-HC-95168 and N01-HC-95169 from the National Heart, Lung, and Blood Institute, and by cooperative agreements UL1-TR-000040, UL1-TR-001079, and UL1-TR-001420 funded by NCATS. The National Sleep Research Resource was supported by the National Heart, Lung, and Blood Institute (R24 hL114473, 75N92019R002).
Author Contributions
J.D. -conceptualization, data curation, writing - original draft; W.Z. -data curation, writing - original draft; Y.L. -methodology, writing - original draft; S.L. – investigation, writing - review and editing; Z.Z. -visualization, validation, writing - original draft; Y.Z. -visualization, validation, writing - original draft; W.S. -data curation, investigation, writing - original draft; H.A. –methodology, supervision, writing - review and editing; S.N. -methodology, supervision, funding acquisition, writing - review and editing; W.G. -conceptualization, methodology, funding acquisition, project administration, writing - review and editing. All authors have given final approval of the version to be published, agreed on the journal to which the article has been submitted, and agreed to be accountable for all aspects of the work.
Funding
The study was supported by Noncommunicable Chronic Diseases-National Science and Technology Major Project (2024ZD0529100); National Natural Science Foundation of China [grant numbers 82370338, 82270258]; National High Level Hospital Clinical Research Funding (BJ-2024-226); Beijing Physician Scientist Training Program [BJPSTP-2024-07]; CS Optimizing Antithrombotic Research Fund [BJUHFCSOARF201901-08]; Beijing Natural Science Foundation [24JL001].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Abarca-Gómez L, Abdeen ZA, Hamid Z, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. 2017;390(10113):2627–2642. doi:10.1016/s0140-6736(17)32129-3
2. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct Target Ther. 2023;8(1):218. doi:10.1038/s41392-023-01496-3
3. Drager LF, Togeiro SM, Polotsky VY, Lorenzi-Filho G. Obstructive sleep apnea: a cardiometabolic risk in obesity and the metabolic syndrome. J Am Coll Cardiol. 2013;62(7):569–576. doi:10.1016/j.jacc.2013.05.045
4. Tishler PV, Larkin EK, Schluchter MD, Redline S. Incidence of sleep-disordered breathing in an urban adult population: the relative importance of risk factors in the development of sleep-disordered breathing. JAMA. 2003;289(17):2230–2237. doi:10.1001/jama.289.17.2230
5. Romero-Corral A, Caples SM, Lopez-Jimenez F, Somers VK. Interactions between obesity and obstructive sleep apnea: implications for treatment. Chest. 2010;137(3):711–719. doi:10.1378/chest.09-0360
6. Messineo L, Bakker JP, Cronin J, Yee J, White DP. Obstructive sleep apnea and obesity: a review of epidemiology, pathophysiology and the effect of weight-loss treatments. Sleep Med Rev. 2024;78:101996. doi:10.1016/j.smrv.2024.101996
7. Abourjeili J, Salameh E, Noureddine M, Bou Khalil P, Eid AA. Obstructive sleep apnea: beyond the dogma of obesity! Respir Med. 2024;222:107512. doi:10.1016/j.rmed.2023.107512
8. Goodarzi MO. Genetics of obesity: what genetic association studies have taught us about the biology of obesity and its complications. Lancet Diabetes Endocrinol. 2018;6(3):223–236. doi:10.1016/s2213-8587(17)30200-0
9. Chen C, Ye Y, Zhang Y, Pan XF, Pan A. Weight change across adulthood in relation to all cause and cause specific mortality: prospective cohort study. BMJ. 2019;367(l5584). doi:10.1136/bmj.l5584
10. Bild DE, Bluemke DA, Burke GL, et al. Multi-ethnic study of atherosclerosis: objectives and design. Am J Epidemiol. 2002;156(9):871–881. doi:10.1093/aje/kwf113
11. Chen X, Wang R, Zee P, et al. Racial/ethnic differences in sleep disturbances: the multi-ethnic study of atherosclerosis (Mesa). Sleep. 2015;38(6):877–888. doi:10.5665/sleep.4732
12. Zhang GQ, Cui L, Mueller R, et al. The national sleep research resource: towards a sleep data commons. J Am Med Inform Assoc. 2018;25(10):1351–1358. doi:10.1093/jamia/ocy064
13. Epstein LJ, Kristo D, Strollo PJ Jr, et al. Clinical guideline for the evaluation, management and long-term care of obstructive sleep apnea in adults. J Clin Sleep Med. 2009;5(3):263–276.
14. Lee CH, Sethi R, Li R, et al. Obstructive sleep apnea and cardiovascular events after percutaneous coronary intervention. Circulation. 2016;133(21):2008–2017. doi:10.1161/circulationaha.115.019392
15. Sánchez-de-la-Torre M, Sánchez-de-la-Torre A, Bertran S, et al. Effect of obstructive sleep apnoea and its treatment with continuous positive airway pressure on the prevalence of cardiovascular events in patients with acute coronary syndrome (ISAACC study): a randomised controlled trial. Lancet Respir Med. 2020;8(4):359–367. doi:10.1016/s2213-2600(19)30271-1
16. Zhou M, Zhu NB, Yu CQ, et al. Analysis on adulthood weight change in adults in China. Zhonghua Liu Xing Bing Xue Za Zhi. 2019;40(5):510–514. doi:10.3760/cma.j.issn.0254-6450.2019.05.004
17. Sheehan TJ, DuBrava S, DeChello LM, Fang Z. Rates of weight change for black and white Americans over a twenty year period. Int J Obes Relat Metab Disord. 2003;27(4):498–504. doi:10.1038/sj.ijo.0802263
18. Fontana L, Hu FB. Optimal body weight for health and longevity: bridging basic, clinical, and population research. Aging Cell. 2014;13(3):391–400. doi:10.1111/acel.12207
19. van Baak MA, Mariman ECM. Obesity-induced and weight-loss-induced physiological factors affecting weight regain. Nat Rev Endocrinol. 2023;19(11):655–670. doi:10.1038/s41574-023-00887-4
20. Kuvat N, Tanriverdi H, Armutcu F. The relationship between obstructive sleep apnea syndrome and obesity: a new perspective on the pathogenesis in terms of organ crosstalk. Clin Respir J. 2020;14(7):595–604. doi:10.1111/crj.13175
21. Schwartz AR, Patil SP, Laffan AM, Polotsky V, Schneider H, Smith PL. Obesity and obstructive sleep apnea: pathogenic mechanisms and therapeutic approaches. Proc Am Thorac Soc. 2008;5(2):185–192. doi:10.1513/pats.200708-137MG
22. Kurnool S, McCowen KC, Bernstein NA, Malhotra A. Sleep apnea, obesity, and diabetes - an intertwined trio. Curr Diab Rep. 2023;23(7):165–171. doi:10.1007/s11892-023-01510-6
23. Muscogiuri G, Barrea L, Annunziata G, et al. Obesity and sleep disturbance: the chicken or the egg? Crit Rev Food Sci Nutr. 2019;59(13):2158–2165. doi:10.1080/10408398.2018.1506979
24. Phillips BG, Hisel TM, Kato M, et al. Recent weight gain in patients with newly diagnosed obstructive sleep apnea. J Hypertens. 1999;17(9):1297–1300. doi:10.1097/00004872-199917090-00009
25. Newman AB, Foster G, Givelber R, Nieto FJ, Redline S, Young T. Progression and regression of sleep-disordered breathing with changes in weight: the sleep heart health study. Arch Intern Med. 2005;165(20):2408–2413. doi:10.1001/archinte.165.20.2408
26. Mueller WH. The changes with age of the anatomical distribution of fat. Soc Sci Med. 1982;16(2):191–196. doi:10.1016/0277-9536(82)90022-3
27. Ryder JR, Xu P, Inge TH, et al. Thirty-year risk of cardiovascular disease events in adolescents with severe obesity. Obesity. 2020;28(3):616–623. doi:10.1002/oby.22725
28. Yang T, Qi F, Guo F, et al. An update on chronic complications of diabetes mellitus: from molecular mechanisms to therapeutic strategies with a focus on metabolic memory. Mol Med. 2024;30(1):71. doi:10.1186/s10020-024-00824-9
29. Bmimc G, Di Angelantonio E, N BS, et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 2016;388(10046):776–786. doi:10.1016/s0140-6736(16)30175-1
30. Bhaskaran K, Dos-Santos-Silva I, Leon DA, Douglas IJ, Smeeth L. Association of BMI with overall and cause-specific mortality: a population-based cohort study of 3·6 million adults in the UK. Lancet Diabetes Endocrinol. 2018;6(12):944–953. doi:10.1016/s2213-8587(18)30288-2
31. Hirko KA, Kantor ED, Cohen SS, Blot WJ, Stampfer MJ, Signorello LB. Body mass index in young adulthood, obesity trajectory, and premature mortality. Am J Epidemiol. 2015;182(5):441–450. doi:10.1093/aje/kwv084
32. Kivimäki M, Kuosma E, Ferrie JE, et al. Overweight, obesity, and risk of cardiometabolic multimorbidity: pooled analysis of individual-level data for 120 813 adults from 16 cohort studies from the USA and Europe. Lancet Public Health. 2017;2(6):e277–e285. doi:10.1016/s2468-2667(17)30074-9
33. McEvoy RD, Antic NA, Heeley E, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea. N Engl J Med. 2016;375(10):919–931. doi:10.1056/NEJMoa1606599
34. Peker Y, Glantz H, Eulenburg C, Wegscheider K, Herlitz J, Thunström E. Effect of positive airway pressure on cardiovascular outcomes in coronary artery disease patients with nonsleepy obstructive sleep apnea. The RICCADSA randomized controlled trial. Am J Respir Crit Care Med. 2016;194(5):613–620. doi:10.1164/rccm.201601-0088OC
35. Guo R, Guo Q, Hao W, Fan J, Nie S, Wang X. Continuous positive airway pressure therapy and long-term outcomes in patients with coronary artery disease and obstructive sleep apnea: a meta-analysis of randomized trials. CVIA. 2024;9(1). doi:10.15212/cvia.2023.0086
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Value of the Systemic Inflammatory Response Index in Patients with Acute Coronary Syndrome and Obstructive Sleep Apnea
He Q, Zhou Y, Tong X, Zhen L, Shi S, Gong W, Nie S
Journal of Inflammation Research 2025, 18:7515-7527
Published Date: 9 June 2025