")
Back to Journals » Journal of Pain Research » Volume 18
Attention Deficits in Migraine: Mismatch Negativity and P3a in an Event-Related Potential Study
Authors Nie P , Wang T, Wu Q, Chen W, Shen F, Huang L, Dong X
Received 15 November 2024
Accepted for publication 28 February 2025
Published 10 March 2025 Volume 2025:18 Pages 1161—1171
DOI https://doi.org/10.2147/JPR.S506708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Rune Häckert Christensen
Ping Nie,1,* Teng Wang,1,* Qian Wu,1 Weikai Chen,1,2 Feifei Shen,1 Lin Huang,1 Xin Dong1,3
1Department of Neurology, the First Affiliated Hospital of Nanjing Medical University, Nanjing, 210029, People’s Republic of China; 2Department of Neurology, The Third Hospital of Xiamen, Xiamen, 361000, People’s Republic of China; 3Department of Neurosurgery, Chongqing Hospital of Jiangsu Province Hospital, Chongqing, 401420, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Dong; Lin Huang, Department of Neurology, the First Affiliated Hospital of Nanjing Medical University, No.300 Guangzhou Road, Nanjing, 210029, People’s Republic of China, Email [email protected]; [email protected]
Purpose: Attention performance in chronic migraine remains unclear. The present study aimed to explore the pre-attentive detection and attention orienting ability in individuals with chronic migraine (CM) measured by mismatch negativity (MMN) and P3a components and assess their associations with migraine characteristics.
Methods: This cross-sectional observational study recruited 25 individuals with episodic migraine (EM), 25 individuals with CM and 25 healthy controls (HC) matched for age, sex, and educational level. The MMN and P3a components were measured using event-related potential (ERPs) tools with auditory oddball paradigms and migraine characteristics were collected.
Results: Individuals with CM exhibited a longer MMN latency (p = 0.010) and a lower P3a amplitude than HC (p = 0.004) and EM (p = 0.002). Correlation analysis showed that P3a amplitude was negatively correlated with headache attack frequency and the Migraine Disability Assessment Scale (MIDAS), Hamilton Anxiety Scale (HAMA), and Hamilton Depression Scale (HAMD) scores.
Conclusion: Individuals with CM showed deficits in pre-attentive detection and attention orientation. Moreover, attention-oriented dysfunction is associated with headache attack frequency, headache-related disability, anxiety and depression.
Keywords: migraine, event-related potentials, ERPs, attention, mismatch negativity, MMN, P3a
Introduction
Migraine is a common neurovascular disorder characterized by recurrent attacks of moderate-to- severe headaches accompanied by nausea, vomiting, photophobia and phonophobia.1–3 Migraine is the second most disabling disorder, affecting 9–35% of the adult population worldwide. Approximately 3% of individuals with episodic migraine (EM) progress to chronic migraine (CM) each year.4 Individuals with CM experience headache for more than 15 days per month for at least 3 months, with features of migraine headache lasting at least 8 days.5 CM has a substantial impact on daily activities and quality of life, causes considerable individual and societal costs, and is associated with multiple comorbidities.6–8
The cerebral cortex, brainstem, and trigeminovascular system are central to migraine pathogenesis. Cortical spreading depression (CSD) may underlie the pathophysiology of migraine aura, characterized by a wave of neuronal depolarization followed by inhibition9,10. The trigeminovascular system plays a key role in the pathophysiology of migraine,11 where activation of the trigeminal nerve leads to the release of vasoactive peptides, leading to neuroinflammation and central sensitization causing pain and vasodilation. The brainstem, particularly the periaqueductal gray (PAG), modulates descending pain inhibition, and dysfunction in this system contributes to the chronic pain processing in migraines.12 Additionally, cortical excitability in migraineurs has been extensively studied, showing altered habituation patterns during the interictal phase.13–16 Unlike healthy controls, individuals with migraines often show increased or unchanged responses to repetitive stimuli, indicating a disruption in habituation. These disturbances may contribute to the heightened sensory sensitivity and sensory overload experienced during migraine attacks, emphasizing the importance of cortical excitability in migraine pathophysiology.
Among the non-painful symptoms closely related to migraines, cognitive dysfunction has been reported in individuals with migraines, especially in the domains of attention, executive functioning and memory.8,17,18 Factors associated with CM, such as anxiety, depression, and sleep disturbances, may contribute to the development of cognitive disabilities. Attention is one of the most important domains of cognitive processing, ensuring the correct allocation of processing resources to relevant stimuli.19,20 Individuals with migraine often report impaired subjective attention, such as difficulty concentrating, thinking, and losing concepts of things.17,21,22 Although several studies have shown interictal attention impairment in migraine,23,24 limited information is available regarding attention deficits in individuals with CM. Hence, it is necessary to further explore attention performance in CM and to identify the underlying brain function involved in these neuropsychological impairments.
Event-related potentials (ERPs) are specific potential changes in electroencephalography (EEG), reflecting the neural activity in response to particular stimuli or events.25 ERPs are one of the most widely used tools to study neural activity during cognitive processing due to their high temporal resolution, objectivity and non-invasiveness.26 ERPs can reflect neurophysiological changes in the cerebral regions and have been used as markers of cognitive function in various neurological disorders.27 Recent studies provide evidence that migraineurs exhibit alterations in auditory attention, as reflected in ERP patterns.28 Some studies report exacerbated attention orienting responses in migraineurs during the interictal state, suggesting increased cortical excitability and dysfunction in sensory processing.29 Conversely, other studies have identified impairments in visual spatial attention, target processing, and orienting responses, indicating deficits in visual attention mechanisms in individuals with migraine.30 Mismatch negativity (MMN) and P3a are potential biomarkers that are closely related to attention.31 MMN is usually observed in auditory cortex, reflects automatic pre-attentive processing of novelty detection and is associated with auditory memory and attention shifting. MMN is an early negative ERP component elicited when deviant stimuli occur in a sequence of repetitive standard auditory stimuli.32,33 The MMN is followed by a positive P3a component, which is distributed fronto-centrally, representing automatic orienting or shifting of attention to novel stimulation.34 The amplitude and latency of P3a are influenced by individual attention, working memory, and cognitive load, etc. The amplitude of P3a usually increases as the “novelty” of the stimulus increases, while the latency may be prolonged by the allocation of attention or cognitive load.27,35 Findings regarding MMN and P3a changes in individuals with migraine have been inconsistent. Previous ERP studies have reported increased MMN and P3a amplitudes following a recurring pattern of oddball stimuli, suggesting a lack of sensory habituation in individuals with migraine.36–38 The disturbance of habituation plays a pivotal role in the pathophysiology of migraine which leads to a general vulnerability of sensory overload, which aligns with the symptom of enhanced sensitivity to light and sound in individuals with migraine.16,39 Nevertheless, a previous study assessed MMN in individuals with EM and did not observe any differences between individuals with migraine and controls.40 These inconsistencies may be due to differences in the stimulation and recording parameters used for ERPs. Additionally, a reduced P3a amplitude was reported in individuals with migraine during the interictal state41 while there was also evidence that individuals with migraine exhibited a larger P3a, indicating exacerbated attention orienting to auditory stimulation in individuals with migraine.42 The inconsistencies may be due to the diverse clinical characteristics of the patient cohorts, such as headache frequency and duration of migraine history. These previous studies primarily recruited individuals with EM, implicating attention abnormalities in individuals with migraine. However, changes in MMN and P3a components in individuals with CM remain unexplored.
Therefore, the present study aimed to explore pre-attentive information processing and attention orienting ability in individuals with migraine, especially those with CM, by measuring the MMN and P3a components using ERP tools with the dual-stimulus oddball paradigm. In addition, we assessed the correlations between these ERP components and the clinical characteristics of individuals with migraine. We hypothesize that individuals with CM will exhibit MMN and P3a abnormalities, such as reduced amplitude and/or prolonged latency, and that these changes will be significantly correlated with the clinical features of individuals with migraine.
Methods
Study Design
This cross-sectional observational study was approved by the First Affiliated Hospital of Nanjing Medical University Ethics Committee (approval No.2024-SR-288) and performed in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from all individuals.
Participants
We recruited 25 healthy controls (HC) and 50 individuals diagnosed with EM (n = 25) and CM (n = 25) from the Department of Neurology of the First Affiliated Hospital of Nanjing Medical University. Individuals with migraine were diagnosed by an experienced neurologist according to the criteria of the International Classification of Headache Disorders (ICHD-III). All the individuals had normal or corrected-to-normal vision and hearing. Individuals who did not receive daily prophylactic therapy and were drug-free for at least 48 hours. Individuals with a history of analgesic drug abuse, other headache types, or other neurological, psychiatric, or systemic disorders were also excluded. Healthy controls were voluntarily recruited from the clinical staff and the community, and they had no personal or family history of migraine.
Clinical data, including the duration of migraine history, presence or absence of aura, headache days per month, duration of headache attack and pain intensity using the visual analogue scale (VAS,0–10), were obtained via the headache diary and structural headache questionnaire. The Migraine Disability Assessment Scale (MIDAS) was used to assess the impact of migraine on the daily life, study, and work of individuals. In addition, all participants were required to complete the Hamilton Anxiety Scale (HAMA) and Hamilton Depression Scale (HAMD) in a psychological clinic to evaluate anxiety and depression.
ERP Recording and Analysis
In this study, each participant underwent ERP recording. For individuals with EM and CM, the recordings were conducted during the interictal period, defined as the absence of migraine attacks 48 h before and after the ERP recordings. Specifically, background or interval headaches during this period were allowed in individuals with CM.43 The experiment was conducted in a room with attenuated sound and light levels. Participants sat in a comfortable chair, placed 50 cm in front of a computer screen, and fixed their eyes at the center of the screen. Auditory oddball paradigms were used in this ERP study. MMN and P3a were collected and processed following the standard protocols.44–46 Participants were asked to relax and watch a silent cartoon film to help keep them engaged and relaxed. Two distinct auditory stimuli were successively presented using headphones. The stimuli consisted of standard (80 dB, 1000 hz, 50 ms duration, p = 0.8) and deviant stimuli (80 dB, 1200 hz, 100 ms duration, p = 0.2), with the stimulus interval varying randomly between 2 and 3 seconds. The task lasted about 10 minutes (Figure 1).
 |
Figure 1 Auditory oddball paradigms. Two distinct auditory stimuli were successively presented using headphones. The stimuli consisted of standard (80 dB, 1000 hz, 50 ms duration, p = 0.8) and deviant stimuli (80 dB, 1200 hz, 100 ms duration, p = 0.2), with the stimulation interval (SI) varying randomly between 2 and 3 seconds. The task lasted about 10 minutes. |
Electroencephalography (EEG) was continuously recorded from 32 Ag/AgCl electrodes placed on the scalp according to the international 10/20 standard using a BrainAmp MR ERP system. All the electrodes were referenced to the linked electrodes placed on the earlobes. Horizontal and vertical electrooculograms were simultaneously recorded with electrodes placed above and below the midpoint of the left eye and 10mm from the outer canthus of each eye to remove eye movement artifacts. The electrode impedance was maintained below 5 kΩ throughout the recording, with a low-pass filter set at 100 hz and a sample rate of 1000Hz.
The EEG was segmented into epochs from 100 ms pre-stimulus to 600 ms post-stimulus, using EEGLAB. In the offline analysis, the EEG was band-pass filtered between 0.01 and 30 hz. A −100 to 0 ms pre-stimulus baseline was used for all ERP wave-form corrections and measurements. EEG signals with amplitudes greater than ±100 μV were excluded from analysis.
MMN and P3a were obtained from the midline electrode sites Fz and Cz. The mismatch negativity (MMN) waveform was extracted by subtracting the ERP waveforms induced by the deviant auditory stimulus from those induced by the standard auditory stimulus and peaks around 100–250ms after the stimulus. The same procedures were used to identify P3a, which was defined as the maximum positive wave within a time window of 250–350ms.
Statistical Analysis
All statistical analyses were performed on IBM SPSS 26.0 for Windows. All data are expressed as the mean ± standard deviation. The Mann–Whitney U-test was used to evaluate continuous clinical parameters between the EM and CM groups. To compare the demographic and clinical variables among the CM, EM, and control groups, a Chi-square test was used for categorical variables, and the Kruskal–Wallis test was used for continuous clinical parameters. MMN and P3a data were analyzed using Generalized Estimating Equations (GEE).47–49 The model included group, electrode site, and their interaction as the primary independent variables, while the presence or absence of aura and the presence or absence of background or interictal headaches were included as covariates for adjustment. A task-related covariance matrix was selected as the structure for the independent variables. To avoid alpha inflation, post-hoc pairwise analyses were performed using the Bonferroni correction only when GEE indicated significant results. Spearman correlation analysis was used to assess the correlations between ERP components and the clinical characteristics of migraines. Statistical significance was set at p < 0.05.
Results
Participants
A total of 75 participants were included in this study, with an overall average age of 45.07 ± 1.61 years. The average ages of the participants in the healthy control group, EM group, and CM group were 45.52 ± 3.46, 42.96 ± 1.94, and 46.72 ± 2.80 years, respectively. There were no significant differences in age, sex, or educational level among the three groups. All sociodemographic data and the questionnaires used can be found in the Table 1. Compared to individuals with EM, individuals with CM had a longer duration of migraine history (p = 0.044), higher headache frequency (p < 0.001), longer duration of headache attack (p = 0.003), and more severe disability, as assessed using the MIDAS (p < 0.001). No significant difference was found in headache severity between the EM group and CM group (p = 0.092). Individuals with EM had more severe anxiety symptoms than the HC (p = 0.007). Individuals with CM showed more severe anxiety and depressive symptoms than individuals with EM (p = 0.014 and p = 0.006, respectively) and HC (p < 0.001) (Table 1).
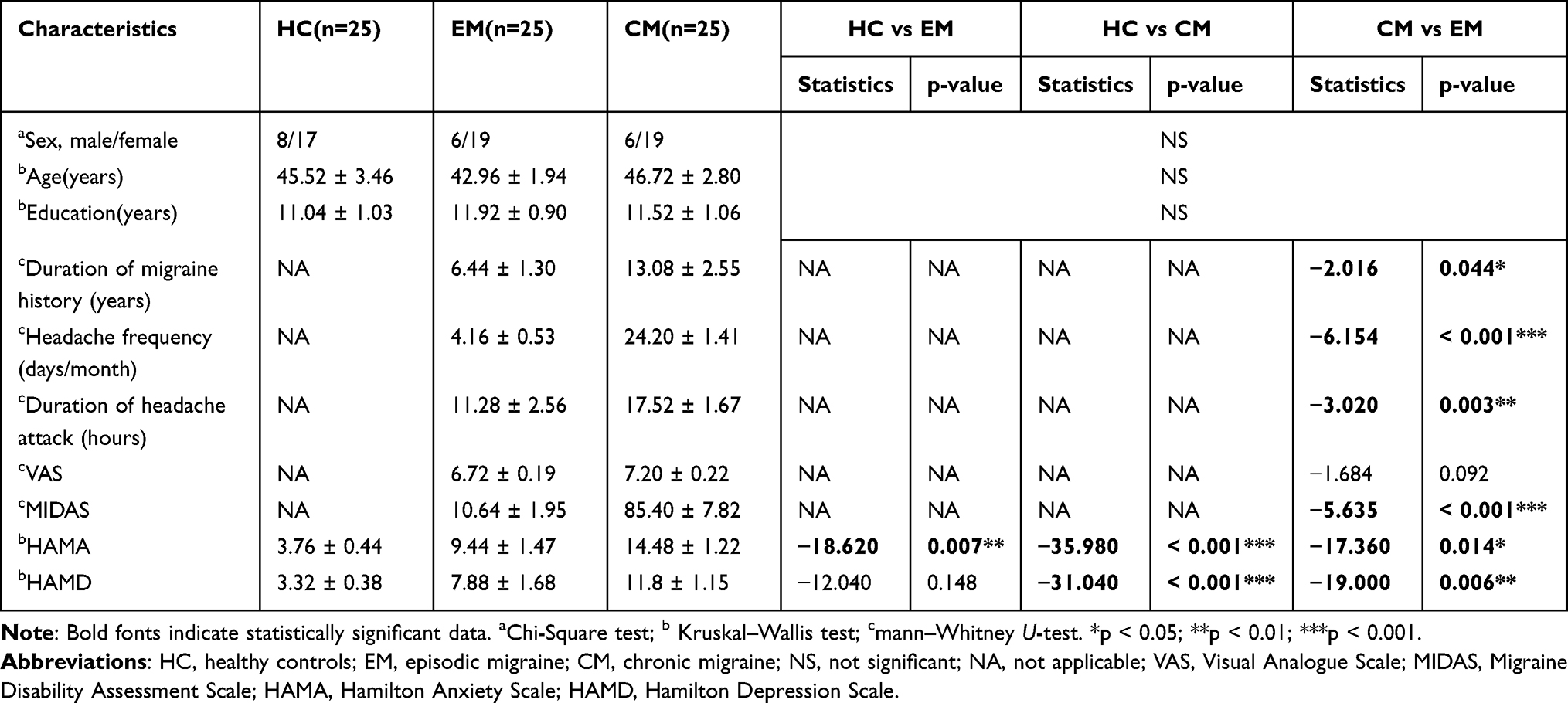 |
Table 1 Clinical and Demographic Characteristics of HC and Individuals With CM and EM |
MMN
For MMN amplitude, after adjusting for aura status and headache presence, GEE analysis revealed a significant main effect of electrode (Wald χ² = 18.237, df = 1, p < 0.001), with higher amplitudes observed at Cz compared to Fz (β = 2.380, 95% CI: [1.288, 3.473], p < 0.001). However, neither the main effect of group (Wald χ² = 4.719, df = 2, p = 0.094) nor the group × electrode interaction (Wald χ² = 2.235, df = 2, p = 0.327) reached statistical significance. Covariates of aura and background or interval headaches did not significantly contribute to the model (Wald χ² = 2.531, df = 1, p = 0.112; Wald χ² = 2.412, df = 1, p = 0.120). Nevertheless, MMN latency showed a significant main effect of group (Wald χ² = 8.672, df = 2, p = 0.013), whereas neither the electrode main effect (Wald χ² = 0.542, df = 1, p = 0.462) nor the group× electrode interaction effect (Wald χ² = 2.188, df = 2, p = 0.335) was statistically significant. Post-hoc pairwise analyses using Bonferroni correction showed that the CM exhibited a longer MMN latency than the HC (β = 21.05, 95% CI: [3.890, 38.220], p = 0.010), with no statistically significant difference between the other groups. Similarly, covariates of aura and background or interval headaches did not significantly contribute to the model (Wald χ² = 0.255, df = 1, p = 0.613; Wald χ² = 1.233, df = 1, p = 0.267). (Figure 2 and Table 2).
 |
Table 2 Amplitudes and Latencies of MMN and P3a in HC and Individuals With CM and EM |
 |
Figure 2 Grand average waveforms of MMN and P3a in HC and individuals with CM and EM (A) at electrode site Fz and (B) at electrode site Cz. Abbreviations: CM, chronic migraine; MMN, mismatch negativity; EM, episodic migraine; HC, healthy control. |
P3a
For P3a amplitude, GEE showed a significant main effect of group (Wald χ² = 13.108, df = 2, p = 0.001) and a significant main effect of electrode (Wald χ² = 39.235, df = 1, p < 0.001), but no significant group× electrode interaction (Wald χ² = 3.240, df = 2, p = 0.198) was found. Covariates of aura and background or interval headaches did not significantly contribute to the model (Wald χ² = 0.000, df = 1, p = 0.983; Wald χ² = 0.411, df = 1, p = 0.522). Post-hoc multiple comparisons using Bonferroni correction showed that the CM exhibited a lower P3a amplitude than the HC (β = −4.967, 95% CI: [−9.125, −0.809], p = 0.004) and EM (β = −4.757, 95% CI: [−8.148, −1.366], p = 0.002) groups, with no statistically significant difference between the HC and EM groups. P3a latency showed a significant main effect of the electrode (Wald χ² = 5.027, df = 1, p = 0.025). However, neither a significant main effect of group (Wald χ² = 1.694, df = 2, p = 0.429) nor a significant group× electrode interaction (Wald χ² = 1.195, df = 2, p = 0.550) was found. Similarly, covariates of aura and background or interval headaches did not significantly contribute to the model (Wald χ² = 0.291, df = 1, p = 0.589; Wald χ² = 1.151, df = 1, p = 0.698). This suggests that no significant difference was found in P3a latency among the three groups (Figure 2 and Table 2).
Correlation Analysis Between ERP Components and Migraine Characteristics
No correlation was found between MMN latency and clinical characteristics of individuals with migraine. The P3a amplitude at the Fz electrode negatively correlated with the frequency of headache attacks (r = −0.458, p = 0.001), MIDAS score (r = −0.461, p = 0.001), HAMA (r = −0.351, p = 0.014) and HAMD (r = −0.386, p = 0.006). Similarly, the P3a amplitude at the Cz electrode negatively correlated with the frequency of headache attacks (r = −0.472, p = 0.001), MIDAS score (r = −0.355, p = 0.012), HAMA (r = −0.363, p = 0.01) and HAMD (r = −0.374, p = 0.008) (Table 3).
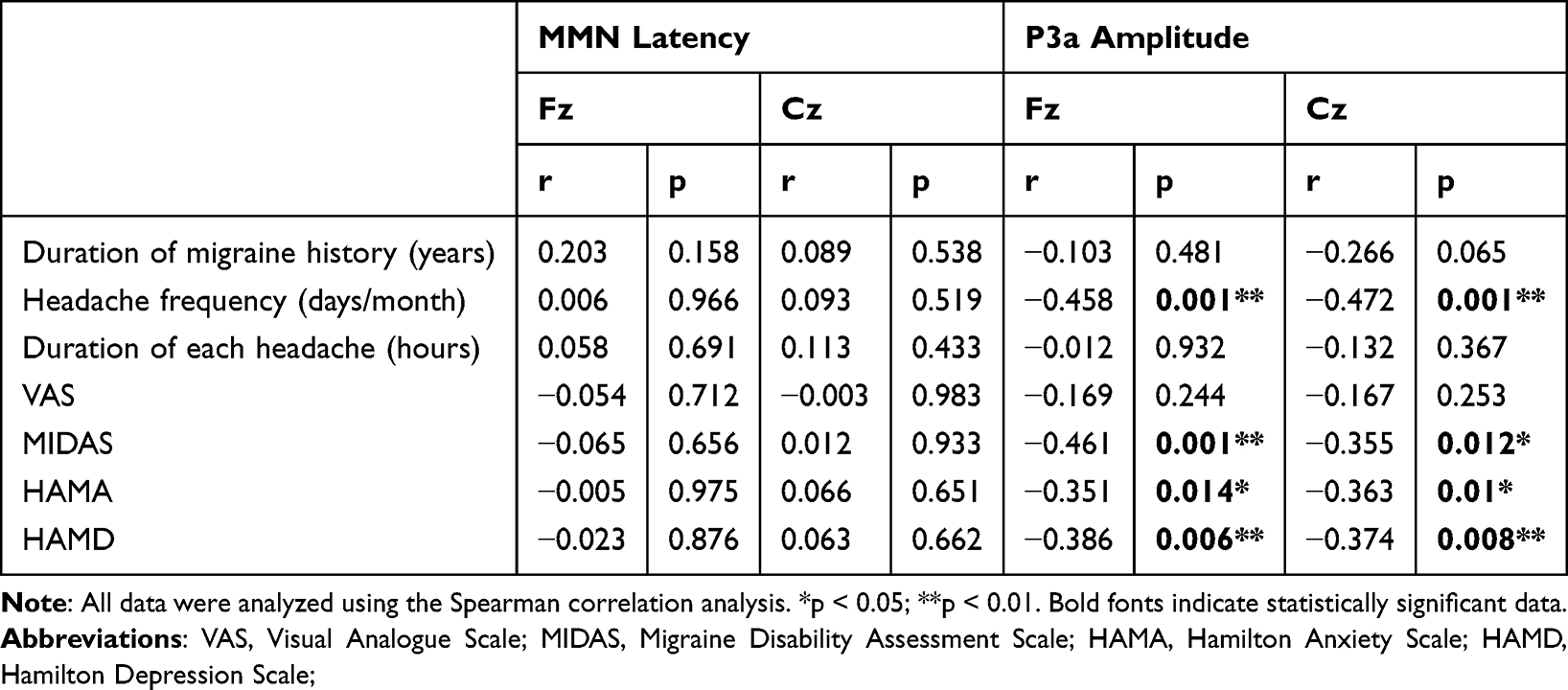 |
Table 3 Correlation Analysis Between ERP Components and Clinical Characteristics of Migraine |
Discussion
In this study, we first investigated MMN and P3a changes in individuals with CM using ERP tools in the auditory oddball paradigm. Our results suggest that individuals with CM exhibit longer MMN latency and lower P3a amplitude, representing an abnormal pre-attentive process of novelty detection and attention orienting in CM. Our study provides comprehensive insights into the attention performance in individuals with CM from the perspective of neural activity and highlights the importance of addressing cognitive dysfunction in CM in clinical practice. Additionally, we observed that P3a amplitude was negatively associated with headache frequency, headache-related disabilities, anxiety, and depression.
The MMN component originates from the bilateral auditory cortex and is an automatic response of the brain to relevant events without the active participation of the individuals.33 This reflects automatic processing of the brain in response to deviant stimuli. MMN is currently the only technical method to objectively evaluate auditory recognition and sensory memory, with no active consciousness involved.50 The prolonged MMN latency in individuals with CM in this study objectively reflected a deficit in the pre-attentive novelty detection process. A previous study showed no difference in MMN amplitudes between episodic individuals with migraines and controls,40 which is consistent with our results. It has been shown that changes in frontal grey matter structure correlate with changes in MMN.51 Individuals with migraine showed frontal grey matter alterations as a consequence of repeated migraine attacks.52 This may explain the abnormal MMN latency observed in individuals with CM.
P3a involves an early attention process in the fronto-central areas.27 P3a reflects the automatic allocation of attention.34 Our study showed that individuals with CM had a lower P3a amplitude, which reflects a dysfunction in the involuntary attentional switch. Nevertheless, no significant differences in the latency or amplitude of P3a were observed between individuals with EM and healthy individuals. An fMRI study reported that attention-specific networks can be modulated by pain.47 Hence, early attention processes and top-down control of attention processing remain preserved in individuals with EM.53 Chronic recurrent migraine attacks might have caused a constant abnormality in brain networks, resulting in attention deficits.54,55 Thus, a reduced P3a amplitude may be a clinical marker of migraine progression. Consistently, a previous study also reported reduced P3a wave amplitudes in individuals with migraine.41 Furthermore, reduced P3a amplitude indicated dysfunction in the frontal lobe. The frontal cortex plays a crucial role in pain perception and modulation, and previous studies have reported frontal dysfunction in individuals with migraine with decreased gray matter density in the frontal lobe.56,57 Therefore, frontal dysfunction indicated by a reduced P3a amplitude might produce abnormal pain perception and modulation, leading to migraine progression. It is crucial to recognize and address cognitive impairments in CM to improve the individuals’ quality of life. MMN and P3a may serve as valuable biomarkers for assessing attentional deficits in CM in both clinical and research settings. These biomarkers may help track the progression of attention impairments and assess the efficacy of interventions aimed at improving attention performance in individuals with CM.
However, previous studies have yielded conflict results.38,42 Previous ERP studies have reported increased MMN and P3a amplitudes in migraine sufferers, particularly when exposed to recurring oddball stimuli. These findings suggest a heightened cortical excitability and a lack of sensory habituation in individuals with migraine. The inability to habituate to repeated stimuli may lead to sensory overload, which is consistent with symptoms like heightened sensitivity to light and sound in individuals with migraine.58 However, our results, focusing on individuals with CM, deviate from this pattern. We found prolonged MMN latency and reduced P3a amplitude in individuals with CM, which suggests slower pre-attentive processing and impaired attention orienting, in contrast to the heightened responses typically observed in episodic migraine (EM). These inconsistencies may arise from several factors. First, differences in the stimulation paradigm used for ERPs could contribute to the variation in findings. Secondly, headache frequency and migraine history may also explain these discrepancies. Recurrent headaches in Individuals with CM could result in attentional impairments, reflected in reduced P3a amplitude and delayed MMN latency, as observed in our study. In contrast, individuals with migraine with less frequent and shorter headache episodes, may retain greater cortical responsiveness. The results of our study suggest that individuals with CM experience impairments in sensory processing, particularly in auditory information processing. Chronic pain is associated with cortical reorganization, which alters brain networks involved in sensory processing and attention.45,46
To clarify the correlation between migraine characteristics and MMN and P3a components, we performed Spearman correlation analysis. We found that the amplitude of P3a was significantly negatively correlated with headache frequency, MIDAS, HAMA, and HAMD scores in individuals with migraine. These findings indicate that early diagnosis and targeted interventions, such as strategies to reduce headache frequency and manage comorbidities like anxiety and depression, may help mitigate attention deficits and prevent further cognitive deterioration. Grey matter alteration in the frontal lobe is associated with the frequency of migraine attacks,52 which may contribute to the negative correlation between P3a amplitude and headache attack frequency. In addition, psychiatric comorbidities are risk factors for the development of migraine from episodic to chronic.59 To some extent, this is in line with our finding that individuals with CM have severe symptoms of anxiety and depression. Several studies have shown that anxiety and depression can negatively affect attention.60–62 We speculated that anxiety and depressive symptoms would have an effect on the dopamine system,63 and dopamine deficiency and excess can lead to a reduction in P3a amplitude.64
Nevertheless, our study had some limitations. First, the sample size was small, thus limiting further subgroup analysis based on sex, age, and education. Second, ERP analysis was performed during the interictal period; therefore, it was not possible to recognize attentional performance in individuals during migraine attacks. Moreover, our clinical data collection was based on a questionnaire and headache diary, thus some retrospective questions such as headache history, may have memory bias. In addition, as a cross-sectional study, we did not examine the progress of involuntary attention deficits in individuals with migraine over time. Further studies with larger sample sizes are needed to evaluate changes in involuntary attention with disease progression. Due to data limitations, we did not perform principal component analysis (PCA) and source reconstruction analysis (sLORETA) on the ERP data to further understand the underlying neural mechanisms and neural origins of the ERPs analysed. This is the direction of our future research.
Conclusions
In summary, we observed prolonged MMN latency and reduced P3a amplitudes in individuals with CM. In addition, we found a negative association between P3a amplitude and the frequency of headache attacks, MIDAS, HAMA, and HAMD scores. These findings suggest that chronic individuals with migraines exhibit deficits in pre-attentive detection and attentional orientation. Moreover, attention-orienting dysfunction is associated with the frequency of headache attacks, headache-related disabilities, anxiety, and depression. Thus, early diagnosis and intervention for migraine may be crucial to prevent deterioration of attention performance. Furthermore, these results may inform clinical interventions aimed at improving sensory processing and attentional control in individuals with migraine, particularly those with CM.
Data Sharing Statement
The data and codes supporting this study’s findings are available on request from the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Young Scholars Fostering Fund of the First Affiliated Hospital of Nanjing Medical University (PY2021006).
Disclosure
None of the authors have potential conflicts of interest to be disclosed in this work.
References
1. Thomsen AV, Ashina H, Al-Khazali HM, et al. Clinical features of migraine with aura: a REFORM study. J Headache Pain. 2024;25(1):22. doi:10.1186/s10194-024-01718-1
2. Pj G, Pr H, MO M, H J, S C, A S. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017;97(2). doi:10.1152/physrev.00034.2015
3. Goadsby PJ, Holland PR. An update: pathophysiology of migraine. Neurol Clin. 2019;37(4):651–671. doi:10.1016/j.ncl.2019.07.008
4. Lipton RB, Fanning KM, Buse DC, et al. Identifying natural subgroups of migraine based on comorbidity and concomitant condition profiles: results of the chronic migraine epidemiology and outcomes (CaMEO) study. Headache. 2018;58(7):933–947. doi:10.1111/head.13342
5. Headache classification committee of the international headache society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
6. Ashina M, Katsarava Z, Do TP, et al. Migraine: epidemiology and systems of care. Lancet. 2021;397(10283):1485–1495. doi:10.1016/S0140-6736(20)32160-7
7. Hovaguimian A, Roth J. Management of chronic migraine. BMJ. 2022;379:e067670. doi:10.1136/bmj-2021-067670
8. Gu L, Wang Y, Shu H. Association between migraine and cognitive impairment. J Headache Pain. 2022;23(1):88. doi:10.1186/s10194-022-01462-4
9. Charles AC, Baca SM. Cortical spreading depression and migraine. Nat Rev Neurol. 2013;9(11):637–644. doi:10.1038/nrneurol.2013.192
10. Eikermann-Haerter K, Ayata C. Cortical spreading depression and migraine. Curr Neurol Neurosci Rep. 2010;10(3):167–173. doi:10.1007/s11910-010-0099-1
11. Ashina M, Hansen JM, Do TP, Melo-Carrillo A, Burstein R, Moskowitz MA. Migraine and the trigeminovascular system-40 years and counting. Lancet Neurol. 2019;18(8):795–804. doi:10.1016/S1474-4422(19)30185-1
12. Aguggia M, Saracco MG, Cavallini M, Bussone G, Cortelli P. Sensitization and pain. Neurol Sci. 2013;34(Suppl 1):S37–40. doi:10.1007/s10072-013-1382-0
13. Stankewitz A, May A. Cortical excitability and migraine. Cephalalgia. 2007;27(12):1454–1456. doi:10.1111/j.1468-2982.2007.01503.x
14. Coppola G, Pierelli F, Schoenen J. Is the cerebral cortex hyperexcitable or hyperresponsive in migraine? Cephalalgia. 2007;27(12):1427–1439. doi:10.1111/j.1468-2982.2007.01500.x
15. Aurora SK, Wilkinson F. The brain is hyperexcitable in migraine. Cephalalgia. 2007;27(12):1442–1453. doi:10.1111/j.1468-2982.2007.01502.x
16. Stankewitz A, May A. The phenomenon of changes in cortical excitability in migraine is not migraine-specific--a unifying thesis. Pain. 2009;145(1–2):14–17. doi:10.1016/j.pain.2009.03.010
17. Latysheva N, Filatova E, Osipova D, Danilov AB. Cognitive impairment in chronic migraine: a cross-sectional study in a clinic-based sample. Arq Neuro-Psiquiat. 2020;78(3):133–138. doi:10.1590/0004-282X20190159
18. Vuralli D, Ayata C, Bolay H. Cognitive dysfunction and migraine. J Headache Pain. 2018;19(1):109. doi:10.1186/s10194-018-0933-4
19. Grossberg S. Attention: multiple types, brain resonances, psychological functions, and conscious states. J Integr Neurosci. 2021;20(1):197–232. doi:10.31083/j.jin.2021.01.406
20. Coull JT. Neural correlates of attention and arousal: insights from electrophysiology, functional neuroimaging and psychopharmacology. Prog Neurobiol. 1998;55(4):343–361. doi:10.1016/S0301-0082(98)00011-2
21. Raggi A, Ferri R. Information processing in migraine: a review of studies on P300. Appl Psychophysiol Biofeedback. 2020;45(3):131–144. doi:10.1007/s10484-020-09469-w
22. Gil-Gouveia R, Oliveira AG, Martins IP. Subjective cognitive symptoms during a migraine attack: a prospective study of a clinic-based sample. Pain Physician. 2016;19(1):E137–150. doi:10.36076/ppj/2016.19.E137
23. Pellegrino Baena C, Goulart AC, Santos ID, Suemoto CK, Lotufo PA, Bensenor IJ. Migraine and cognitive function: baseline findings from the Brazilian longitudinal study of adult health: ELSA-Brasil. Cephalalgia. 2018;38(9):1525–1534. doi:10.1177/0333102417737784
24. Chen C, Dong X, Gu P, et al. Attention impairment during the interictal state in migraineurs without aura: a cross-sectional study. J Pain Res. 2021;Volume 14:3073–3083. doi:10.2147/JPR.S312181
25. Hajcak G, Klawohn J, Meyer A. The utility of event-related potentials in clinical psychology. Annu Rev Clin Psychol. 2019;15:71–95. doi:10.1146/annurev-clinpsy-050718-095457
26. MacNamara A, Joyner K, Klawohn J. Event-related potential studies of emotion regulation: a review of recent progress and future directions. Int J Psychophysiol. 2022;176:73–88. doi:10.1016/j.ijpsycho.2022.03.008
27. Polich J. Updating P300: an integrative theory of P3a and P3b. Clin Neurophysiol. 2007;118(10):2128–2148. doi:10.1016/j.clinph.2007.04.019
28. Masson R, Lévêque Y, Demarquay G, et al. Auditory attention alterations in migraine: a behavioral and MEG/EEG study. Clin Neurophysiol. 2020;131(8):1933–1946. doi:10.1016/j.clinph.2020.05.024
29. Jj S, Ta P, Pl W, Kr B, Allen-Winters S, Andrasik F. Auditory event-related potentials in the interictal phase of migraine indicate alterations in automatic attention. Appl Psychophysiol Biofeedback. 2017;42(4). doi:10.1007/s10484-017-9378-9
30. Guo Y, Tian Q, Xu S, et al. The impact of attack frequency and duration on neurocognitive processing in migraine sufferers: evidence from event-related potentials using a modified oddball paradigm. BMC Neurol. 2019;19(1):73. doi:10.1186/s12883-019-1305-7
31. Justo-Guillén E, Ricardo-Garcell J, Rodríguez-Camacho M, Rodríguez-Agudelo Y, Lelo de Larrea-Mancera ES, Solís-Vivanco R. Auditory mismatch detection, distraction, and attentional reorientation (MMN-P3a-RON) in neurological and psychiatric disorders: a review. Int J Psychophysiol. 2019;146:85–100. doi:10.1016/j.ijpsycho.2019.09.010
32. Näätänen R, Paavilainen P, Rinne T, Alho K. The mismatch negativity (MMN) in basic research of central auditory processing: a review. Clin Neurophysiol. 2007;118(12):2544–2590. doi:10.1016/j.clinph.2007.04.026
33. Csépe V. On the origin and development of the mismatch negativity. Ear Hearing. 1995;16(1):91–104. doi:10.1097/00003446-199502000-00007
34. Volpe U, Mucci A, Bucci P, Merlotti E, Galderisi S, Maj M. The cortical generators of P3a and P3b: a LORETA study. Brain Res Bull. 2007;73(4–6):220–230. doi:10.1016/j.brainresbull.2007.03.003
35. Hruby T, Marsalek P. Event-related potentials--the P3 wave. Acta Neurobiol Exp. 2003;63(1):55–63. doi:10.55782/ane-2003-1455
36. Valeriani M, Galli F, Tarantino S, et al. Correlation between abnormal brain excitability and emotional symptomatology in paediatric migraine. Cephalalgia. 2009;29(2):204–213. doi:10.1111/j.1468-2982.2008.01708.x
37. de Tommaso M, Guido M, Libro G, et al. Interictal lack of habituation of mismatch negativity in migraine. Cephalalgia. 2004;24(8):663–668. doi:10.1111/j.1468-2982.2004.00731.x
38. Wang W, Schoenen J. Interictal potentiation of passive “oddball” auditory event-related potentials in migraine. Cephalalgia. 1998;18(5):261–265. discussion 241. doi:10.1046/j.1468-2982.1998.1805261.x
39. Coppola G, Pierelli F, Schoenen J. Habituation and migraine. Neurobiol Learn Mem. 2009;92(2):249–259. doi:10.1016/j.nlm.2008.07.006
40. Morlet D, Demarquay G, Brudon F, Fischer C, Caclin A. Attention orienting dysfunction with preserved automatic auditory change detection in migraine. Clin Neurophysiol. 2014;125(3):500–511. doi:10.1016/j.clinph.2013.05.032
41. Koo YS, Ko D, Lee GT, et al. Reduced frontal P3a amplitude in migraine patients during the pain-free period. J Clin Neurol. 2013;9(1):43–50. doi:10.3988/jcn.2013.9.1.43
42. Demarquay G, Caclin A, Brudon F, Fischer C, Morlet D. Exacerbated attention orienting to auditory stimulation in migraine patients. Clin Neurophysiol. 2011;122(9):1755–1763. doi:10.1016/j.clinph.2011.02.013
43. Hsiao FJ, Chen WT, Wang YF, et al. Identification of patients with chronic migraine by using sensory-evoked oscillations from the electroencephalogram classifier. Cephalalgia. 2023;43(5):3331024231176074. doi:10.1177/03331024231176074
44. Duncan CC, Barry RJ, Connolly JF, et al. Event-related potentials in clinical research: guidelines for eliciting, recording, and quantifying mismatch negativity, P300, and N400. Clin Neurophysiol. 2009;120(11):1883–1908. doi:10.1016/j.clinph.2009.07.045
45. Light GA, Williams LE, Minow F, et al. Electroencephalography (EEG) and event-related potentials (ERPs) with human participants. Curr Protoc Neurosci. 2010;Chapter 6:Unit6.25.1–24. doi:10.1002/0471142301.ns0625s52
46. Mh H, Yl C, Ss G. Mismatch negativity and P3a in drug-naive adults with attention-deficit hyperactivity disorder. Psychol Med. 2021;52(15). doi:10.1017/S0033291720005516
47. Houlihan ME, McGrath PJ, Connolly JF, et al. Assessing the effect of pain on demands for attentional resources using ERPs. Int J Psychophysiol. 2004;51(2):181–187. doi:10.1016/j.ijpsycho.2003.08.001
48. de Melo MB, Daldegan-Bueno D, Menezes Oliveira MG, de Souza AL. Beyond ANOVA and MANOVA for repeated measures: advantages of generalized estimated equations and generalized linear mixed models and its use in neuroscience research. Eur J Neurosci. 2022;56(12):6089–6098. doi:10.1111/ejn.15858
49. Ma Y, Mazumdar M, Memtsoudis SG. Beyond repeated-measures analysis of variance: advanced statistical methods for the analysis of longitudinal data in anesthesia research. Region Anesth Pain M. 2012;37(1):99–105. doi:10.1097/AAP.0b013e31823ebc74
50. Fishman YI. The mechanisms and meaning of the mismatch negativity. Brain Topogr. 2014;27(4):500–526. doi:10.1007/s10548-013-0337-3
51. Rasser PE, Schall U, Todd J, et al. Gray matter deficits, mismatch negativity, and outcomes in schizophrenia. Schizophrenia Bull. 2011;37(1):131–140. doi:10.1093/schbul/sbp060
52. Zhang X, Zhou J, Guo M, et al. A systematic review and meta-analysis of voxel-based morphometric studies of migraine. J Neurol. 2023;270(1):152–170. doi:10.1007/s00415-022-11363-w
53. Matusz PJ, Turoman N, Tivadar RI, Retsa C, Murray MM. Brain and cognitive mechanisms of top-down attentional control in a multisensory world: benefits of electrical neuroimaging. J Cognit Neurosci. 2019;31(3):412–430. doi:10.1162/jocn_a_01360
54. Krimmel SR, DeSouza DD, Keaser ML, et al. Three dimensions of association link migraine symptoms and functional connectivity. J Neurosci. 2022;42(31):6156–6166. doi:10.1523/JNEUROSCI.1796-21.2022
55. Coppola G, Di Renzo A, Petolicchio B, et al. Aberrant interactions of cortical networks in chronic migraine: a resting-state fMRI study. Neurology. 2019;92(22):e2550–e2558. doi:10.1212/WNL.0000000000007577
56. Rocca MA, Ceccarelli A, Falini A, et al. Brain gray matter changes in migraine patients with T2-visible lesions: a 3-T MRI study. Upd Int Car. 2006;37(7):1765–1770. doi:10.1161/01.STR.0000226589.00599.4d
57. Camarda C, Monastero R, Pipia C, Recca D, Camarda R. Interictal executive dysfunction in migraineurs without aura: relationship with duration and intensity of attacks. Cephalalgia. 2007;27(10):1094–1100. doi:10.1111/j.1468-2982.2007.01394.x
58. Coppola G, Di Lorenzo C, Schoenen J, Pierelli F. Habituation and sensitization in primary headaches. J Headache Pain. 2013;14(1):65. doi:10.1186/1129-2377-14-65
59. Torres-Ferrús M, Ursitti F, Alpuente A, et al. From transformation to chronification of migraine: pathophysiological and clinical aspects. J Headache Pain. 2020;21(1):42. doi:10.1186/s10194-020-01111-8
60. Chandler DA, Roach A, Ellison A, Husid Burton E, Jelsone-Swain L. Symptoms of depression together with trait anxiety increase the ability to predict alpha power change between attention and resting states. Int J Psychophysiol. 2022;182:57–69. doi:10.1016/j.ijpsycho.2022.09.010
61. Bar-Haim Y, Lamy D, Pergamin L, Bakermans-Kranenburg MJ, van IJzendoorn MH. Threat-related attentional bias in anxious and nonanxious individuals: a meta-analytic study. Psychol Bull. 2007;133(1):1–24. doi:10.1037/0033-2909.133.1.1
62. Bachmann HP, Japee S, Merriam EP, Liu TT. Emotion and anxiety interact to bias spatial attention. Emot. 2024;24(4):1109–1124. doi:10.1037/emo0001322
63. Zarrindast MR, Khakpai F. The modulatory role of dopamine in anxiety-like behavior. Arch Iran Med. 2015;18(9):591–603.
64. Apitz T, Bunzeck N. Dopamine controls the neural dynamics of memory signals and retrieval accuracy. Neuropsychopharmacol. 2013;38(12):2409–2417. doi:10.1038/npp.2013.141
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.