")
Back to Journals » Journal of Pain Research » Volume 18
Auricular Acupuncture for Perioperative Pain Management: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Authors Zhou Y, Bao Q, Yang C, Li S, Yin Z, Xiong J , Sun M, Yang J , Liu F, Liang F
Received 27 August 2024
Accepted for publication 13 January 2025
Published 25 January 2025 Volume 2025:18 Pages 441—454
DOI https://doi.org/10.2147/JPR.S488525
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jinlei Li
Yan Zhou,1,* Qiongnan Bao,1,* Chen Yang,1,* Shuhao Li,1,* Zihan Yin,1 Jian Xiong,1 Mingsheng Sun,1 Jiao Yang,2 Fang Liu,3 Fanrong Liang1
1Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, People’s Republic of China; 2Rehabilitation Medicine Center, West China Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Department of Integrated Chinese and Western Medicine, Sichuan Cancer Hospital, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Fanrong Liang, Acupuncture and Tuina School, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, 610075, People’s Republic of China, Email [email protected] Fang Liu, Department of Integrated Chinese and Western Medicine, Sichuan Cancer Hospital, Chengdu, Sichuan, 610041, People’s Republic of China, Email [email protected]
Purpose: We conducted a more comprehensive systematic review and meta-analysis to evaluate the effectiveness of auricular acupuncture (AA) in perioperative pain management.
Methods: Randomized controlled trials (RCTs) findings were retrieved from the Embase, Cochrane Central Register of Controlled Trials, PubMed, Web of Science, Chinese Biomedical Literature Database, Wanfang, VIP, and China National Knowledge Infrastructure databases from their inception to March 2024 using the search terms “pain”, “auriculotherapy”, and “randomized controlled trial”. The experimental group was treated with AA alone or in combination with analgesic drugs, whereas the control group was treated with sham auricular acupuncture, placebo, conventional treatment, or no treatment. The primary outcome was the perioperative pain score. The secondary outcomes were analgesic requirements, anxiety score, and adverse events (AEs). RevMan version 5.4 was used for data analysis.
Results: The analysis included a total of 21 RCTs with 1527 participants. AA was superior to the control group for reducing pain intensity (mean difference [MD]= − 0.44; 95% confidence interval [CI]: − 0.72 to − 0.17) and analgesic requirement (standardized mean difference [SMD]= − 0.88, 95% CI: − 1.29 to − 0.46). Perioperative anxiety improvement did not differ significantly between the AA and control groups (MD= − 5.45, 95% CI: − 32.99 to 22.09). Subgroup analysis showed that AA exerted a significant analgesic effect as a preoperative intervention and in orthopedic surgery. The results of the sensitivity analysis demonstrated the stability of the results of the meta-analysis. AA-related AEs were mainly nausea, vomiting, and drowsiness. None of the patients in the experimental group dropped out of the trial due to AA-related AEs.
Conclusion: Current evidence suggests that AA may be a promising treatment option for improving perioperative pain with few AEs. However, owing to the low quality of the current evidence, large-sample, high-quality RCTs are needed to prove this conclusion.
Keywords: ear acupuncture, analgesic requirements, anxiety score, adverse events
Introduction
Pain is an unpleasant sensation and emotional experience associated with actual or potential tissue damage.1 Despite advancements in the understanding of pain mechanisms and the emergence of methods for acute pain management, insufficient treatment of postoperative pain remains a significant concern.2 The incidence of postoperative pain is 75%, with 80% of patients reporting severe pain during their hospital stay.3 Moreover, approximately 70% of patients report moderate or severe pain during the perioperative period.4 Perioperative pain affects postoperative recovery, prolongs hospital stay, increases the risks of respiratory and cardiovascular complications,5 and is closely associated with postoperative delirium.6 Additionally, pain seriously affects patients’ quality of life and imposes a significant financial burden on the health system.7
Opioids remain the mainstream treatment option for perioperative pain; however, their clinical use is limited by adverse effects, including respiratory depression, pruritus, and gastrointestinal reactions.8 Although non-steroidal anti-inflammatory drugs can provide non-addictive analgesia, they have a ceiling effect and can lead to reduced hemostatic function, poor bone healing, renal dysfunction, and gastrointestinal toxicities.8 Thus, complementary and alternative medicines (CAMs), such as acupuncture and manual therapies, have become increasingly popular in the United States because of their safety and cost-effectiveness.7
Auricular acupuncture (AA), a type of CAM, differs from traditional Chinese medicine (TCM) in that it is based on a map of acupoints superimposed on the auricle. Points on the auricle are stimulated to regulate the corresponding body parts or organs.9 The connection between auricle, zangfu, and meridians forms the foundation for managing perioperative pain. AA not only regulates sympathetic and parasympathetic nerves through the thalamic pathway; It also stimulates non-specific immunity and mobilizes the activity of various immune factors through humoral regulation.10 Compared with analgesics, AA has the advantages of non-addictive and non-toxic side effects. It is easier to perform than other forms of acupuncture. Clinical studies have demonstrated the benefit of AA for perioperative pain from total knee arthroplasty,11 gastric cancer surgery,12 hemorrhoids,13 and first-trimester abortion.14,15 A 2008 systematic review (SR) of AA for postoperative pain reported the results as “promising, but not convincing”.16 Recent SRs on auriculotherapy for pain management have focused on acute and postoperative pain.7,9,10 Although the results favor auriculotherapy, these studies involved non-acupuncture modalities applied to auricular acupoints, such as acupressure or transcutaneous electrical nerve stimulation, and did not conduct subgroup analyses of different intervention timing, thus limiting our understanding of AA efficacy. In conclusion, there is no consensus on the efficacy of AA for perioperative pain. Additional randomized controlled trials (RCTs) have been conducted in recent years to validate AA for perioperative pain and should be included in updated systematic reviews to identify the latest evidence of AA in the treatment of perioperative pain.
In this research context, we conducted a more comprehensive literature search with pain intensity as the main outcome of the SR and performed a meta-analysis of the efficacy of AA as an independent treatment modality for perioperative pain. We also reported analgesic requirements, perioperative anxiety, and adverse events (AEs) to provide additional evidence for clinical decision-making.
Materials and Methods
This review follows the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA).17 The protocol has been previously registered on PROSEPERO (ID: CRD42024529778).
Search Strategy
We searched the following eight electronic databases from their inception to March 2024: Embase, Cochrane Central Register of Controlled Trials, PubMed, Web of Science, China Biomedical Literature Database, Wanfang Database, VIP Database, and China National Knowledge Infrastructure. Only studies written in Chinese or English language were included. The search strategy involved a combination of Medical Subject Heading terms and free words, which were adjusted according to different databases, and included “pain”, “perioperative pain”, “postoperative pain”, “auriculotherapy”, “ear acupuncture”, “auricular acupuncture”, “electroauricular acupuncture”, and “randomized controlled trial”. The search strategies are shown in Supplementary Enclosure. We also manually searched the relevant references of published reviews to identify other eligible studies.
Inclusion Criteria
(1) Study types: This review included only RCTs evaluating the efficacy of AA for perioperative pain. (2) Participants: The participants were adults with perioperative pain but no serious complications, with no restrictions on operation type or participant sex, race, or degree of pain. (3) Interventions: The experimental group received AA or electroauricular acupuncture (EAA), alone or in combination with analgesic drugs for pain treatment. Studies combining AA with body acupuncture or other CAM (including herbal medicine, massage, and exercise) and studies comparing AA with EAA were excluded (Because our study was not to evaluate the efficacy of adding an electrical stimulus to the AA). Other auricular acupoint stimulation modalities, such as auricular acupressure or transcutaneous electrical acupoint stimulation, were also excluded. (4) Control interventions: The control group received sham auricular acupuncture (SAA), placebo, analgesic drugs, or no treatment for perioperative pain. (5) Outcomes: The primary outcomes were perioperative pain scores, including the visual analog scale (VAS) and Numerical Rating Scale (NRS). The secondary outcomes were analgesic requirement, anxiety score (VAS), and AEs.
Study Selection
All retrieved literature was imported into EndNote X9. After removing duplicates, two reviewers independently performed an initial screening of the literature based on the titles and abstracts. Two reviewers then screened the full text according to the inclusion criteria and determined the eligible studies. Any disagreement was resolved by negotiation between the two reviewers. If the two reviewers disagreed, a third reviewer made a final determination.
Data Extraction
Using a predesigned data extraction form, two evaluators independently extracted the following information: basic information (first author, country, publication year, generation of randomized protocol, and blinding method), characteristics of the study participants (sample size, age, diagnostic criteria for disease, inclusion and exclusion criteria, etc), intervention and control measures, outcome indicators (definition of indicators, measurement time points, etc), and AEs. Disagreements were resolved by a third reviewer.
Assessment of the Risk of Bias (ROB)
The ROB in each included trial was assessed by two reviewers using the Cochrane Collaboration criteria.18 The evaluation covered the following seven areas: randomization, allocation concealment, researcher and participant blindness, outcome evaluator blindness, incomplete outcome data integrity, selective reporting, and other biases. Each area was evaluated as low risk, concern, or high risk. Differences in assessments were resolved through discussions among all researchers.
Data Synthesis and Statistical Analysis
All data were imported into RevMan version 5.4 for analysis. Continuous variables were analyzed using mean differences (MDs) or standardized mean differences (SMDs) with 95% confidence intervals (CIs). P <0.05 indicated statistical significance. A random-effects model was applied to analyze the data (I2 >50% or P ≤0.1). The meta-analysis of pain intensity used VAS and NRS results. Owing to the connection between pain assessment scales,19 the VAS results were converted into their corresponding scores on an 11-point NRS (0: no pain, 10: extreme pain). For studies with multiple data points (ie, measuring pain intensity at multiple time points after AT intervention), the data point with the smallest effect size was extracted for meta-analysis. Pre-planned subgroup analyses were performed to explore the sources of heterogeneity based on intervention means (The included studies were divided into a group of AA and a group of EAA according to whether the intervention was supplemented with current or not), intervention time-point (According to the intervention time-point, the included studies were divided into preoperative intervention group and postoperative intervention group), and operation type (According to the type of surgery, the included studies were divided into orthopedics surgery, gastrointestinal surgery, hemorrhoids surgery, ENT surgery, gynecologic surgery and exodontia surgery). We performed sensitivity analyses to verify the stability of the results. Publication bias was assessed using funnel plots.
Evaluation of Evidence Quality
Based on the Grading of Recommendations Assessment, Development, and Evaluation (GRADE)20 system, the quality of evidence was graded separately by two reviewers as high, moderate, low, and very low. The GRADE system considers study limitations, inconsistent results, insufficient accuracy, indirect evidence, and publication biases. Any disagreements in grading were decided by a third reviewer.
Results
Search results
A total of 5785 studies were initially retrieved from the eight databases. After removing duplicates, the titles and abstracts of 3039 studies were screened, 3011 of which were excluded for not meeting the inclusion criteria. Finally, 21 RCTs11–15,21–36 were included after reading the full texts. The screening flowchart is shown in Figure 1.
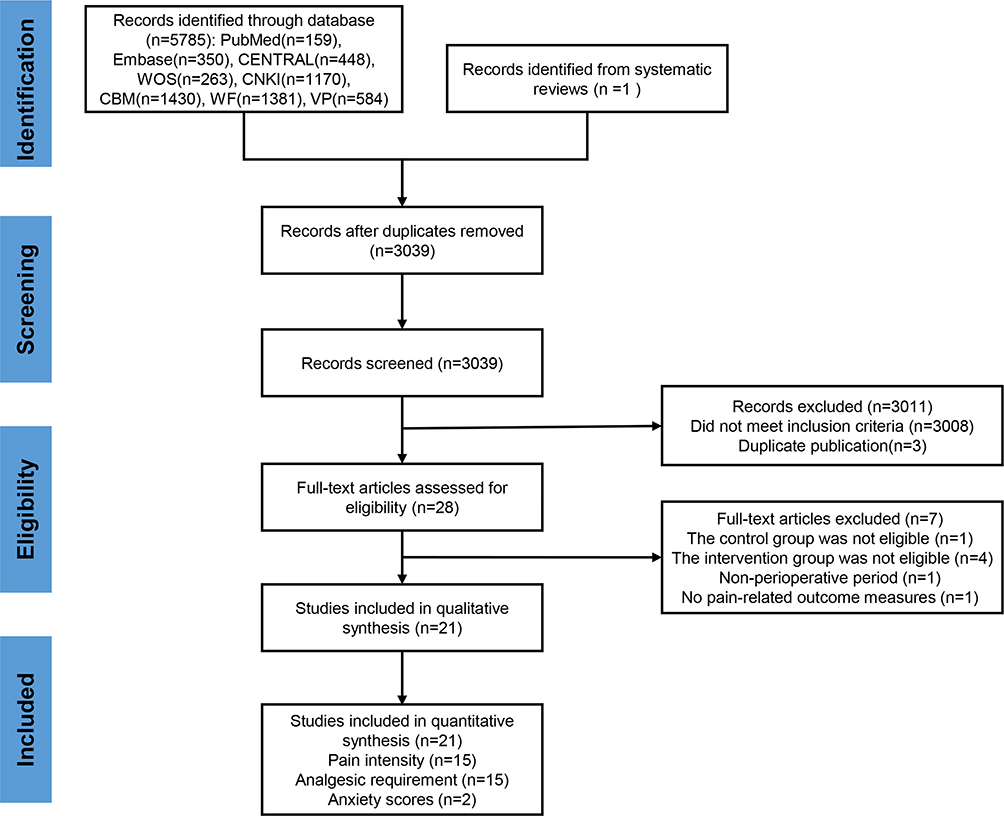 |
Figure 1 Flow diagram of the screening process. |
General Characteristics of the Included Studies
The 21 RCTs included 1527 participants. The maximum and minimum sample sizes were 120 and 10 participants, respectively. The selected studies were published between 1986 and 2023. Nine studies (43%) were from China, five (24%) from the United States, three (14%) from Germany, two (10%) from Austria, one (5%) from the Egypt, and one (5%) from the United Kingdom. Thirteen (61.9%) studies were sham-controlled and eight (38.1%) were open-label trials. Nineteen studies (90.5%) applied a two-group parallel design, 16 of which compared AA with SAA, conventional analgesics, or no intervention, while three compared EAA with conventional analgesics or SAA. Two studies (9.5%) were three-arm trials comparing AA with EAA or SAA. The characteristics of the included studies are presented in Table 1.
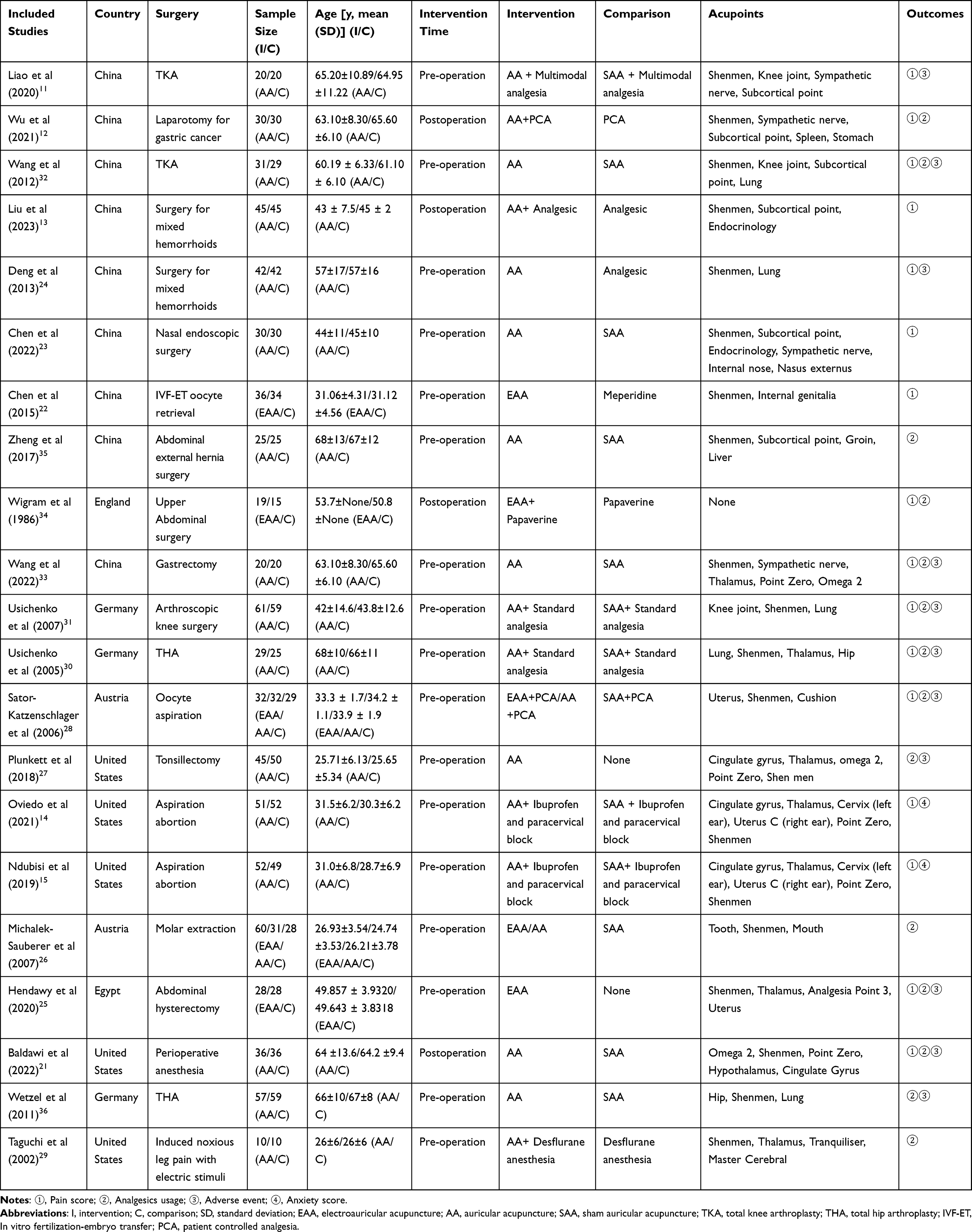 |
Table 1 Characteristics of Included Studies |
Risk of Bias
Eighteen studies11–15,21–30,32,33,35 (85.71%) were rated as low-risk because they used appropriate randomized sequence generation methods. No study was rated as high-risk in terms of random sequence generation. Eleven studies14,15,21,25,26,28,29,31,33,35,37 (52.38%) reported allocation concealment. Patient blinding was described in 13 studies14,15,21,23,26–33,37 (61.9%). Ten studies14,15,21,25,28–31,33,37 (47.62%) reported blinding of outcome assessments. All included studies11–15,21–35,37 (100%) were rated as low-risk in terms of incomplete outcome data. Two studies31,33 (9.52%) had a low ROB for selective reporting. None of the studies were rated as having a high risk of blinding of outcome assessment, selective reporting, or other biases (Figure 2).
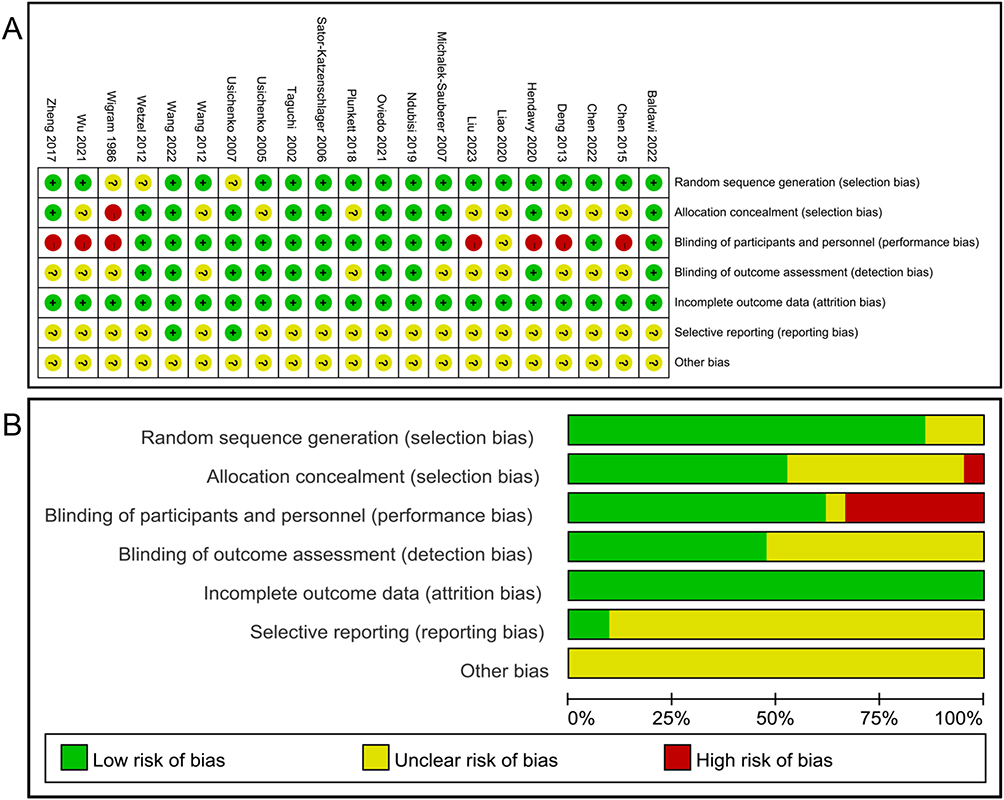 |
Figure 2 (A) Risk of bias item for included RCTs. (B) Risk of bias item presented as percentages across all included RCTs. |
Outcomes
Primary outcomes
A total of 17 RCTs11–15,21–25,28,30–34 reported pain intensity; however, two studies11,15 were not included in the meta-analysis because of incomplete data. Owing to significant heterogeneity among the 15 studies included in the meta-analysis12–14,21–25,28,30–34 (P <0.00001, I2=93%), a random-effects model was used for data analysis. The AA group demonstrated a greater improvement in perioperative pain than the control group (MD= −0.44, 95% CI: −0.72 to −0.17; P=0.002) (Figure 3).
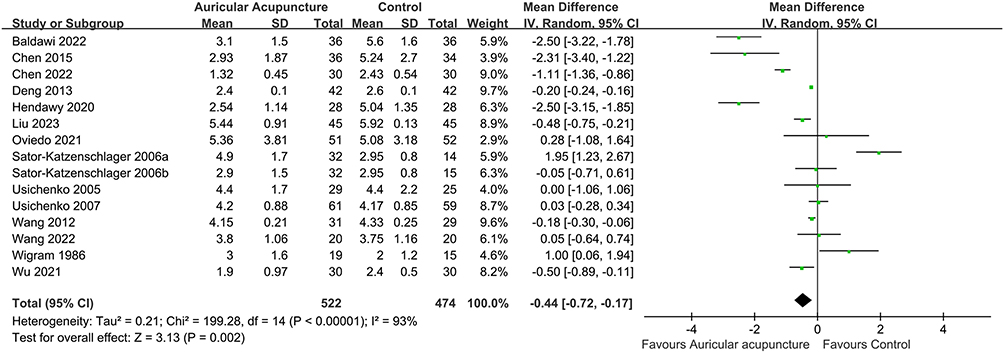 |
Figure 3 Meta-analysis of the pain intensity. Abbreviations: SD, standard deviation; CI, confidence interval. |
Secondary outcomes
Analgesic Requirement
Fifteen RCTs12,21,25–35,37 reported analgesic requirement, which was significantly lower in the AA group than that in the control group (SMD= −0.88, 95% CI: −1.29 to −0.46; P <0.0001; I2=88%) (Figure 4A). In addition, two studies11,25 reported significantly later time to first analgesic request in the AA group than that in the control group.
 |
Figure 4 Meta-analysis of the analgesic requirement (A) and anxiety scores (B). Abbreviations: SD, standard deviation; CI, confidence interval. |
Anxiety Scores
Two RCTs14,15 reported anxiety scores, and the results of the meta-analysis showed no significant difference in improving perioperative anxiety between the AA and control groups [MD=−5.45, 95% CI: −32.99 to 22.09; P=0.7; I2=84%, Figure 4B].
Adverse Events
Eleven studies reported AEs and number of patients. The perioperative AEs mainly included nausea, vomiting, and drowsiness. No serious AEs were associated with AA. Local earache after AA was reported in three studies.30,31,33 Acupuncture syncope reaction was reported in one study,24 and auricular hemorrhage after needle removal was reported in one study,30 but all were tolerated and no patients withdrew from the trial because of AA-related AEs (Supplementary Table S1).
Subgroup and Sensitivity Analyses
The results of subgroup analyses of pain intensity and analgesia requirements according to intervention modality and intervention timing showed no significant differences between EAA and control treatment, although the studies showed significant heterogeneity. Compared with the control group, AA better relieved perioperative pain and reduced the need for analgesia. Similarly, compared with the control group, postoperative AA significantly reduced the need for analgesics; however, pain intensity showed no significant improvement. Thus, preoperative AA showed advantages in the above two aspects. In addition, AA demonstrated no significant effect on pain intensity in patients undergoing gastrointestinal or gynecological surgery, but significantly affected pain relief in patients undergoing orthopedic; hemorrhoid; and ear, nose, and throat (ENT) surgeries compared with the control group. Pain relief was the most significant in patients undergoing ENT surgery. The subgroup meta-analysis of the analgesia requirement according to surgery type showed that AA significantly reduced the analgesic drug needs of patients undergoing orthopedic and ENT surgery but not those undergoing gastrointestinal, gynecological, or tooth extraction surgery. Sensitivity analyses showed that both the pain intensity and analgesic requirements were stable (Table 2).
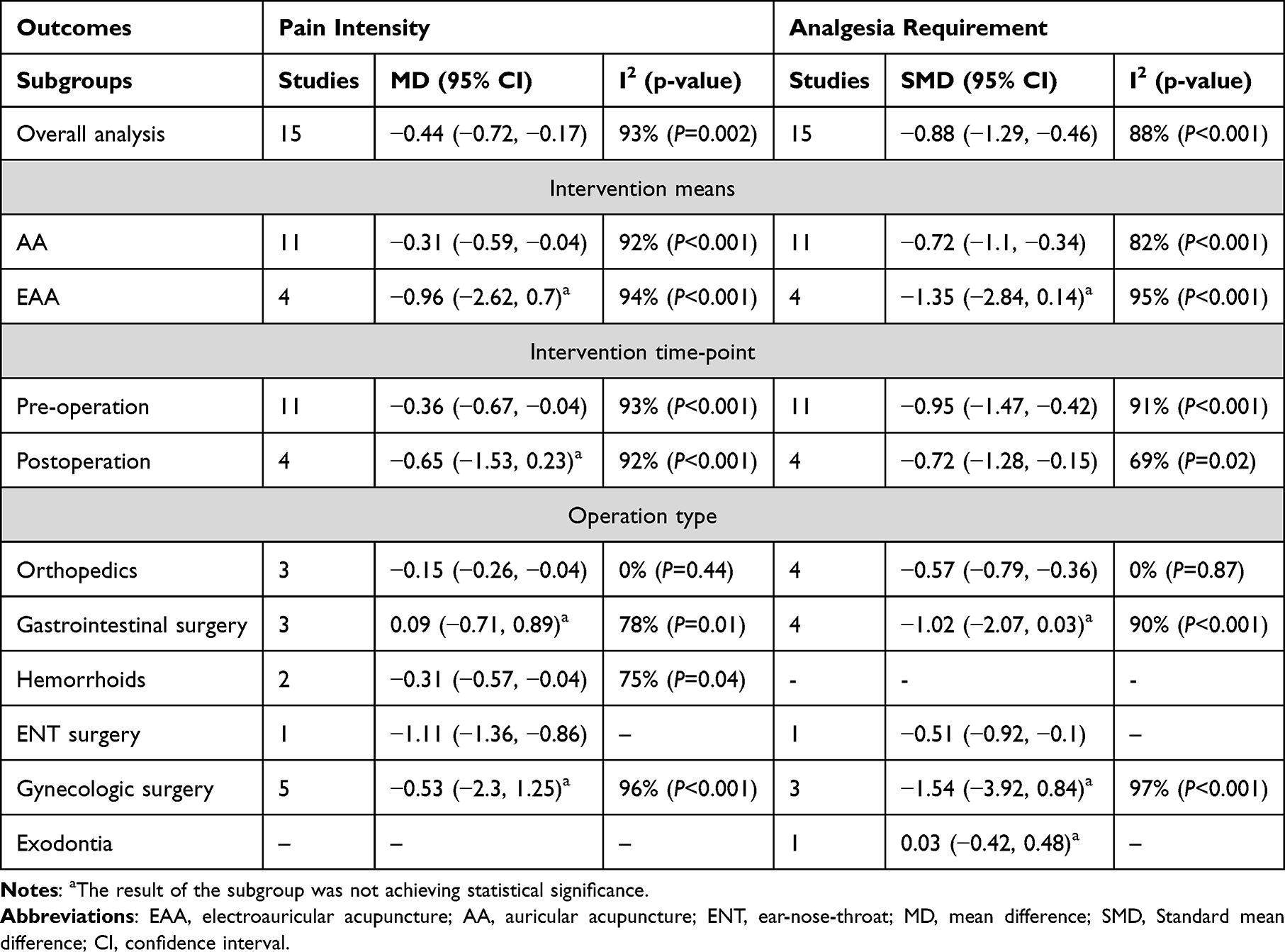 |
Table 2 Subgroup Analyses of Pain Intensity and Analgesia Requirement |
Publication Bias
We plotted funnel plots with MD as the midpoint to determine publication bias in the 15 studies on pain intensity (Figure S1). Two reviewers independently judged the symmetry of the funnel plots. Both believed that the plots were asymmetrical, indicating potential publication bias in the studies on pain intensity.
Quality of Evidence Assessment
The quality of evidence for pain intensity and analgesic requirement was rated as very low due to serious heterogeneity and significant publication bias. The quality of evidence for anxiety scores was also rated as very low due to serious imprecision, in addition to the above reasons (Supplementary Table S2).
Discussion
The results of the present meta-analysis showed that AA can relieve perioperative pain and reduce the need for analgesics but has no significant effect on perioperative anxiety. However, only two studies reported perioperative anxiety scores. The results of the subgroup analysis showed that perioperative pain relief was the most significant in the AA group for preoperative interventional and ENT surgery. In the AA group, the preoperative interventional, orthopedic, and ENT surgery groups had a lower demand for analgesic drugs. No serious AA-related AEs occurred. However, publication bias and low-quality evidence were present.
AA is a unique treatment system that differs from TCM. AA is based on Nogier’s hypothesis that the locations of acupoints on the auricle correspond to the organs and parts of an upside-down baby’s body.16 Stimulating the auricular acupoints can regulate the function of the corresponding parts of the human body. AA has been widely used for perioperative analgesia, while EAA has been applied for anesthesia in head, neck and chest surgery.38 AA could also serve as an effective supplement to routine treatment during the first trimester of uterine aspiration.15 In their 2008 review of studies on AA in the treatment of postoperative pain, Usichenko et al showed that AA was effective in alleviating postoperative pain. However, the results were not convincing owing to methodological flaws in the included studies.16 A subgroup analysis of perioperative pain in a meta-analysis of all types of pain, AA group showed a significant reduction in analgesic requirement,9 but four of the five studies included in the subgroup analysis were from the same research team, leading to the possibility that this result was weakened by investigator bias. One meta-analysis concluded that AA was at least as effective as painkillers for Immediate Pain relief.7 A recent systematic review and meta-analysis indicated that auricular acupressure may improve postoperative acute pain, but higher quality studies are needed to determine a more accurate effect size.10 Therefore, the effects of AA on perioperative pain remain unclear.
The present review evaluated the efficacy and safety of AA as a standalone modality for perioperative pain management. The results revealed significantly lower pain intensity and analgesic requirements in the AA group than those in the control group; the sensitivity analyses were stable Moreover, AA did not improve perioperative anxiety, contrary to previous findings.39 This review included only two studies in the meta-analysis of perioperative anxiety, with significant heterogeneity between the studies, leading to limited interpretation and generalization of the results. In conclusion, owing to the small number of RCTs, insufficient sample size, and large heterogeneity between studies, we found limited evidence to support the effectiveness and safety of AA in improving perioperative pain. Future studies with larger sample sizes, improved study designs, and higher-quality evidence are needed to validate our conclusions.
Only 13 of the 21 included studies used SAA as a control, and studies have found that placebo effects and expectations stimulate areas of the brain that control pain pathways and regulate mood.40 Given the effectiveness of placebo analgesia and the positive physiological effects of acupuncture at any body point to relieve pain,40,41 future RCTs with SAA as the control are recommended to verify the analgesic efficacy of AA. Regarding the choice of outcome indicators, it was taken into account that analgesic requirements are influenced by the surgical site and the economic situation of the patient.10 Therefore, analgesic requirement may not be reliable as a measure of AA effectiveness, and it is recommended that future studies use pain intensity as an outcome measure.
The results of subgroup analysis according to intervention mode revealed that EAA had no significant effect on either pain intensity or analgesic need; however, as this analysis included only four studies with significant heterogeneity, drawing conclusions about these results is difficult. There were no AA-related serious AEs in the included studies, so AA is safer and more convenient than current pain management measures. AA may be a promising treatment for perioperative pain and can be used as a complementary alternative to multimodal pain management strategies.
The results of subgroup analysis by intervention timing revealed that preoperative intervention significantly reduced perioperative pain and analgesic needs. This is consistent with previous findings showing that acupuncture has a pre-emptive analgesic effect42 lower morphine use during gynecological surgery in the lower abdomen for preoperative acupuncture than postoperative acupuncture.43 According to the preemptive analgesic theory, preoperative intervention can prevent central sensitization caused by incision and inflammation.33
The results of subgroup analyses according to the surgical category, including orthopedics, gastrointestinal surgery, hemorrhoids, ENT surgery, gynecologic surgery, and exodontia, revealed that AA may have the most significant analgesic effect on hemorrhoids, indicating that AA may be an ideal alternative therapy for postoperative pain in patients undergoing hemorrhoid surgery. However, the analgesic effects of AA during gastrointestinal and gynecological surgeries were not significant. These results are consistent with those reported by Wang et al33 and Oviedo et al.14 Different postoperative care or short intervention times may affect AA efficacy, and high-quality RCTs are needed to verify AA efficacy in such patients.
Standardizing AA interventions across different studies is a challenge. Different operation types indicate the inclusion of different study populations, and accordingly, postoperative care, acupuncture details, and treatment plans will also be different. These confounding factors will inevitably lead to the heterogeneity of research outcomes. In order to ensure the quality of research and the reproducibility of research results, it is recommended that future study should strictly follow the CONSORT (Consolidated Standards of Reporting Trials) statement44 and the Standards for Reporting Interventions in Clinical Trials of Acupuncture.45
The included studies selected different auricular acupoints, among which Shenmen was the most frequently used (20 studies), followed by the thalamus (seven studies) and subcortical points (six studies). However, these three acupoints were mostly used in combination with other auricular acupoints, and the sample size was small; therefore, we cannot conclude that a particular auricular acupoint demonstrated a unique effect on perioperative pain. The distribution of auricular acupoints (Supplementary Table S3) was generally in the overlapping regions of the auricular branches of the vagus nerve, the auricular great nerve, and the auricular temporal nerve, consistent with the current view that the auricular vagus reflex is one mechanism through which AA provides analgesia. Neurophysiologically, stimulation of auricular nerve endings by AA is transmitted through the peripheral nervous system to the central nervous system (CNS), releasing neurotransmitters that regulate endogenous pain control mechanisms. When descending neural pathways are activated, endorphins are released from the posterior horn of spinal cord (PHSC), making it difficult for the CNS to diffuse and perceive pain stimulus. Another mechanism of AA analgesia is Gate Control Theory, which transmits nonpainful stimuli through Aβ fibers rather than painful stimuli through Aδ or C fibers to neutralize painful sensations in the PHSC.46 In addition, stimulation of the auricular region induces the release of acetylcholine from the vagus nerve, which inhibits the production of proinflammatory cytokines through cholinergic antiinflammatory pathways, thereby suppressing inflammation.47,48 However, the exact mechanisms underlying AA analgesia require further investigation.
The present study aimed to elucidate the effectiveness and safety of AA for perioperative pain by performing a systematic review and meta-analysis to provide an evidence-based basis for clinical decision-making. This review complied with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. The results of the subgroup analysis revealed that preoperative AA significantly reduced perioperative pain and analgesic requirements and that the analgesic effect of AA on hemorrhoids may be the most significant. These findings may help physicians make better clinical decisions.
Although a random-effects model was used in this study, statistical heterogeneity was still substantial. Clinical heterogeneity (the difference in enrolled patients, interventions, controls, and outcomes of the included studies) may account for the differences. Subgroup analysis was performed according to intervention means, intervention time-point, and operation type. However, this heterogeneity is difficult to assess in terms of patient differences, acupuncture details (auricular point selection, acupuncture depth, acupuncture response, treatment frequency, duration, and course of treatment), as these factors are difficult to unify. In view of the above situation, this study narrowed the inclusion criteria, performed strict quality evaluation, and conducted subgroup analysis to improve the power of the conclusions.
This review has several limitations. First, as a random-effects model was used for the meta-analysis, heterogeneity of the included studies was assumed. However, the size of the estimated effect may reflect inevitable bias in acupuncture studies. Second, in the meta-analysis, significant heterogeneity was observed in all groups analyzed, except for the orthopedic subgroup. We were unable to eliminate potential confounding factors that differed in the inclusion population, acupoint prescriptions, treatment frequency, and treatment duration, which may have increased the outcome heterogeneity and reduced the quality of evidence. Third, the number of included studies was limited, the sample sizes varied greatly, and most were single-center studies, making it difficult to determine the influence of contingency factors. Fourth, because the studies in the database are constantly updated, the studies we collected may differ from the actual number included. Therefore, future reviews need to consider the timing factor. Fifth, we included only English and Chinese studies, which undoubtedly introduced language bias, so future studies need to cancel language restrictions to eliminate language bias. Moreover, the methodological shortcomings of the studies included in this review were mainly a lack of adequate allocation concealment and blinding, which may have led to an overestimation of intervention effects.49,50
Conclusion
Current evidence suggests that auricular acupuncture, as a relatively safe alternative therapy for perioperative pain, can reduce pain intensity and the analgesic needs of patients. Auricular acupuncture exerted a significant analgesic effect during preoperative interventions and hemorrhoid surgery and was ineffective in gastrointestinal and gynecological surgeries. However, owing to the low quality of the current evidence, further large-sample, high-quality randomized controlled trials are needed to demonstrate the efficacy and safety of auricular acupuncture in relieving perioperative pain. Future randomized controlled trials may consider the following points. Firstly, rigorous randomization, allocation concealment, and blinding should be designed to improve methodological quality. Secondly, combined with clinical practice and evidence-based methods, optimal auricular point selection, treatment course and treatment frequency should be determined, and a standardized perioperative pain management auricular acupuncture program should be designed.
Abbreviations
AA, auricular acupuncture; AE, adverse event; EAA, electroauricular acupuncture; ENT, ear, nose, and throat; CAM, complementary and alternative medicine; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development, and Evaluation; MD, mean difference; RCT, randomized controlled trial; ROB, risk of bias; SAA, sham auricular acupuncture; SMD, standardized mean difference; SR, systematic review; TCM, traditional Chinese medicine; VAS, visual analog scale.
Data Sharing Statement
All the data was shown in the article.
Acknowledgments
We would like to thank Editage (www.editage.cn) for English language editing.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is financially supported by the Sichuan Province Key Research and Development Project (grant number 2023YFS0328, 2021YFS0087, Grantee: FL, MSS), Joint Fund for Regional Innovation and Development of National Natural Science Foundation of China (grant number U21A20404, Grantee: FRL) and Youth Fund Project of National Natural Science Foundation of China (grant number 82305380, Grantee: JY). Four funders contributed to the study design and data collection.
Disclosure
The author(s) report no conflicts of interest in this work. The review protocol is not prepared.
References
1. Lovich-Sapola J, Smith CE, Brandt CP. Postoperative pain control. Surg Clin North Am. 2015;95:301–318. doi:10.1016/j.suc.2014.10.002
2. Dolin SJ, Cashman JN, Bland JM. Effectiveness of acute postoperative pain management: I. Evidence from published data. Br J Anaesth. 2002;89:409–423. doi:10.1093/bja/89.3.409
3. Pyati S, Gan TJ. Perioperative pain management. CNS Drugs. 2007;21:185–211. doi:10.2165/00023210-200721030-00002
4. Apfelbaum JL, Chen C, Mehta SS, et al. Postoperative pain experience: results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg. 2003;97:534–540. doi:10.1213/01.ANE.0000068822.10113.9E
5. Khan RS, Ahmed K, Blakeway E, et al. Catastrophizing: a predictive factor for postoperative pain. Am J Surg. 2011;201:122–131. doi:10.1016/j.amjsurg.2010.02.007
6. O’Gara BP, Gao L, Marcantonio ER, et al. Sleep, pain, and cognition: modifiable targets for optimal perioperative brain health. Anesthesiology. 2021;135:1132–1152. doi:10.1097/ALN.0000000000004046
7. Murakami M, Fox L, Dijkers MP. Ear acupuncture for immediate pain relief—a systematic review and meta-analysis of randomized controlled trials. Pain Med. 2017;18:551–564. doi:10.1093/pm/pnw215
8. Brown AK, Christo PJ, Wu CL. Strategies for postoperative pain management. Best Pract Res Clin Anaesthesiol. 2004;18:703–717. doi:10.1016/j.bpa.2004.05.004
9. Asher GN, Jonas DE, Coeytaux RR, et al. Auriculotherapy for pain management: a systematic review and meta-analysis of randomized controlled trials. J Altern Complement Med. 2010;16:1097–1108. doi:10.1089/acm.2009.0451
10. Zhong Q, Wang D, Bai Y-M, et al. Effectiveness of auricular acupressure for acute postoperative pain after surgery: a systematic review and meta-analysis. Chin J Integr Med. 2019;25:225–232. doi:10.1007/s11655-019-3063-1
11. Liao H, Zhan W-F, Zhu M-H, et al. Clinical observation of auricular acupuncture for pain after total knee arthroplasty. Guide Tradit Chin Med. 2020;26:64–67.
12. Wu L-H, Zhang -Y-Y, Wang X-Q, et al. Effect of auricular intradermal needling on postoperative pain of gastric cancer patients. Guide Tradit Chin Med. 2021;27:120–124.
13. Liu H-M, Sha J-T, Zhao W, et al. Clinical study of auricular acupuncture with intradermal needle in the prevention and treatment of postoperative pain of mixed hemorrhoids with “shi re xia zhu” syndrome. Hebei J Tradit Chin Med. 2023;45:98–101.
14. Oviedo JD, Marquez E, Gold MA, et al. Auricular acupressure and auricular acupuncture as an adjunct for pain management during first trimester aspiration abortion: a randomized, double-blinded, three-arm trial. Contraception. 2021;103:342–347. doi:10.1016/j.contraception.2021.02.005
15. Ndubisi C, Danvers A, Gold MA, et al. Auricular acupuncture as an adjunct for pain management during first trimester abortion: a randomized, double-blinded, three arm trial. Contraception. 2019;99:143–147. doi:10.1016/j.contraception.2018.11.016
16. Usichenko TI, Lehmann C, Ernst E. Auricular acupuncture for postoperative pain control: a systematic review of randomised clinical trials. Anaesthesia. 2008;63:1343–1348. doi:10.1111/j.1365-2044.2008.05632.x
17. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.
18. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
19. Hjermstad MJ, Fayers PM, Haugen DF, et al. Studies comparing numerical rating scales, verbal rating scales, and visual analogue scales for assessment of pain intensity in adults: a systematic literature review. J Pain Symptom Manage. 2011;41:1073–1093. doi:10.1016/j.jpainsymman.2010.08.016
20. Schünemann HJ, Oxman AD, Brozek J, et al. Grading quality of evidence and strength of recommendations for diagnostic tests and strategies. BMJ. 2008;336:1106–1110. doi:10.1136/bmj.39500.677199.AE
21. Baldawi M, McKelvey G, Patel VR, et al. Battlefield acupuncture use for perioperative anesthesia in veterans affairs surgical patients: a single-center randomized controlled trial. J Integr Complement Med. 2022;28:683–688. doi:10.1089/jicm.2021.0429
22. Chen H, Wang Y-P, Xing J-Q, et al. Application of electro-auricular acupuncture analgesia in in vitro fertilization-embryo transfer oocyte retrieval. Jiangsu Med J. 2015;41:2863–2865.
23. Chen L-L, Xiong Q, Chen P. The effect of intradermal needling on postoperative pain and sleep quality in patients with functional endoscopic sinus surgery. shang hai zhen jiu za zhi. 2022;41.
24. Deng B-L, Jiao -L-L, Zhang Y-M, et al. Effect of auricular acupuncture on perioperative analgesia of mixed hemorrhoids. Shang hai zhen jiu za zhi. 2013;32:650–652.
25. Hendawy HA, Abuelnaga ME. Postoperative analgesic efficacy of ear acupuncture in patients undergoing abdominal hysterectomy: a randomized controlled trial. BMC Anesthesiol. 2020;20. doi:10.1186/s12871-020-01187-4
26. Michalek-Sauberer A, Heinzl H, Sator-Katzenschlager SM, et al. Perioperative auricular electroacupuncture has no effect on pain and analgesic consumption after third molar tooth extraction. Anesth Analg. 2007;104:542–547. doi:10.1213/01.ane.0000253233.51490.dd
27. Plunkett A, McCoart A, Howard RS, et al. A randomized, single-blind, prospective trial of auricular ‘battlefield’ acupuncture for the reduction of postoperative tonsillectomy pain in adults. Pain Manag. 2018;8:287–295. doi:10.2217/pmt-2018-0007
28. Sator-Katzenschlager SM, Wölfler MM, Kozek-Langenecker SA, et al. Auricular electro-acupuncture as an additional perioperative analgesic method during oocyte aspiration in IVF treatment. Human Reprod. 2006;21:2114–2120. doi:10.1093/humrep/del110
29. Taguchi A, Sharma N, Ali SZ, et al. The effect of auricular acupuncture on anaesthesia with desflurane. Anaesthesia. 2002;57:1159–1163. doi:10.1046/j.1365-2044.2002.02832.x
30. Usichenko TI, Dinse M, Hermsen M, et al. Auricular acupuncture for pain relief after total Hip arthroplasty—a randomized controlled study. Pain. 2005;114:320–327. doi:10.1016/j.pain.2004.08.021
31. Usichenko TI, Kuchling S, Witstruck T, et al. Auricular acupuncture for pain relief after ambulatory knee surgery: a randomized trial. CMAJ Can Med Assoc J. 2007;176:179–183. doi:10.1503/cmaj.060875
32. Wang J-F, Bang H-X, Cai Y-H, et al. Clinical application of auricular acupuncture analgesia in the perioperative period of total knee arthroplasty. Zhong yi zheng gu za zhi. 2012;24:3–6.
33. Wang X-Q, Xiao L, Duan P-B, et al. The feasibility and efficacy of perioperative auricular acupuncture technique via intradermal needle buried for postoperative movement-evoked pain after open radical gastrectomy: a randomized controlled pilot trial. Explore. 2022;18:36–43. doi:10.1016/j.explore.2021.09.007
34. Wigram JR, Lewith GT, Machin D, et al. Electroacupuncture for postoperative pain. Physiother Pract. 1986;2:83–88. doi:10.3109/09593988609022422
35. Zheng X, Wan L, Gao F, et al. Effect of ear point embedding on plasma and effect site concentrations of propofol-remifentanil in elderly patients after target-controlled induction. Zhongguo Zhen Jiu. 2017;37:869–873. doi:10.13703/j.0255-2930.2017.08.017
36. Wetzel B, Pavlovic D, Kuse R, et al. The Effect of Auricular Acupuncture on Fentanyl Requirement During Hip Arthroplasty. The Clinical Journal of Pain. 2011;27(3): 262–267. doi:10.1097/AJP.0b013e3181fd516c
37. Collazo Chao E. The effect of auricular acupuncture on fentanyl requirement during Hip arthroplasty. A randomized controlled trial. Revista Internacional de Acupuntura. 2012;6:56–57. doi:10.1016/S1887-8369(12)70053-4
38. Cheng SB, Ding LK. Practical application of acupuncture analgesia. Nature. 1973;242:559–560. doi:10.1038/242559a0
39. Usichenko TI, Hua K, Cummings M, et al. Auricular stimulation for preoperative anxiety—a systematic review and meta-analysis of randomized controlled clinical trials. J Clin Anesth. 2022;76:110581. doi:10.1016/j.jclinane.2021.110581
40. Atlas LY, Wager TD. A meta-analysis of brain mechanisms of placebo analgesia: consistent findings and unanswered questions. Handb Exp Pharmacol. 2014;225:37–69.
41. Le Bars D, Dickenson AH, Besson JM. Diffuse noxious inhibitory controls (DNIC). I. Effects on dorsal horn convergent neurones in the rat. Pain. 1979;6:283–304. doi:10.1016/0304-3959(79)90049-6
42. Gonçalves de Freitas AT, Lemonica L, De Faveri J, et al. Preemptive analgesia with acupuncture monitored by c-Fos expression in rats. J Acupunct Meridian Stud. 2016;9:16–21. doi:10.1016/j.jams.2015.08.002
43. Sim CK, Xu PC, Pua HL, et al. Effects of electroacupuncture on intraoperative and postoperative analgesic requirement. Acupunct Med. 2002;20:56–65. doi:10.1136/aim.20.2-3.56
44. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869. doi:10.1136/bmj.c869
45. MacPherson H, Altman DG, Hammerschlag R, et al. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): extending the CONSORT statement. PLoS Med. 2010;7:e1000261. doi:10.1371/journal.pmed.1000261
46. Damien J, Colloca L, Bellei-Rodriguez C, et al. Pain modulation: from conditioned pain modulation to placebo and nocebo effects in experimental and clinical pain. Int Rev Neurobiol. 2018;139:255–296.
47. Mercante B, Ginatempo F, Manca A, et al. Anatomo-physiologic basis for auricular stimulation. Med Acupunct. 2018;30:141–150. doi:10.1089/acu.2017.1254
48. Jiang Y, Cao Z, Ma H, et al. Auricular vagus nerve stimulation exerts antiinflammatory effects and immune regulatory function in a 6-OHDA model of Parkinson’s disease. Neurochem Res. 2018;43:2155–2164. doi:10.1007/s11064-018-2639-z
49. Pildal J, Hróbjartsson A, Jørgensen KJ, et al. Impact of allocation concealment on conclusions drawn from meta-analyses of randomized trials. Int J Epidemiol. 2007;36:847–857. doi:10.1093/ije/dym087
50. Wood L, Egger M, Gluud LL, et al. Empirical evidence of bias in treatment effect estimates in controlled trials with different interventions and outcomes: meta-epidemiological study. BMJ. 2008;336:601–605. doi:10.1136/bmj.39465.451748.AD
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.