")
Back to Journals » Infection and Drug Resistance » Volume 18
Azithromycin in the Management of Upper Respiratory Tract Infections (URTIs): Indian Real-Life Experience
Authors Dominic M, Srivastava R, Shah K, Naik SM, Rout K, Ray B, Patil D , Rana D , Swami OC
Received 24 July 2024
Accepted for publication 19 December 2024
Published 27 January 2025 Volume 2025:18 Pages 523—531
DOI https://doi.org/10.2147/IDR.S488479
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Azithromycin in Upper Respiratory Tract Infections – Video abstract [488479]
Views: 400
Mathew Dominic,1 Rakesh Srivastava,2 Kshitij Shah,3 Sudhir M Naik,4 Khageswar Rout,5 Bidhan Ray,6 Dinesh Patil,7 Darshan Rana,7 Onkar C Swami7
1Medical Trust Hospital, Ernakulam, 682016, Kerala, India; 2Raj ENT Centre and Voice Clinic, Lucknow, 226010, Uttar Pradesh, India; 3Criticare Asia Hospital, Mumbai, 400028, Maharashtra, India; 4The Oxford Medical College and Research Hospital, Bangalore, 562107, Karnataka, India; 5LASER ENT Clinic, Bhubaneswar, 751021, Orissa, India; 6IIMSAR & Dr. BC Roy Hospital, Haldia, 721631, West Bengal, India; 7Alembic Pharmaceuticals Limited, Mumbai, Maharashtra, 400099, India
Correspondence: Onkar C Swami, Alembic Pharmaceuticals Limited, Mumbai, 400099, Maharashtra, India, Tel +91 9372423101, Email [email protected]
Objective: Upper Respiratory Tract Infections (URTIs) pose a significant public health challenge worldwide. Azithromycin has been approved for its management due to broad-spectrum antibacterial properties and favorable pharmacokinetics. This study aims to evaluate the effectiveness and safety of Azithromycin in treatment of URTIs in a real-world setting.
Methods: This multicenter, retrospective, observational study was conducted across 184 Ear, Nose, and Throat (ENT) clinics in India. Medical records of adults (≥ 18 years) who received Azithromycin 500 mg for 5 days to treat URTIs and provided consent were retrieved. Sore throat, fever, and interference with daily activities were assessed alongside clinical signs (pharyngeal erythema, tonsillar erythema, and exudates/plugs on tonsils). Clinical global impression of change was evaluated using a 7-point rating scale. Statistical analyses included paired t-tests for mean score changes and the McNemar–Bowker test to evaluate symptom improvement from baseline to day 5.
Results: Data from 884 patients were analyzed. With 5 days of Azithromycin therapy, significant reduction in proportion of patients reporting URTI symptoms and signs was noted. Proportion of patients reporting sore throat was reduced from 95.8% to 10.4%; work absenteeism dropped from 47.9% to 1%; and fever subsided in 97.4% of patients. Clinical signs also improved notably, with moderate-to-severe pharyngeal erythema (90.9% of patients at baseline to 13.6% at day 5), tonsillar erythema (84% of patients at baseline to 9.6%), and tonsillar exudates (58.3% patients at baseline to 4.4%). Also, 97.2% of patients showed considerable improvement in their Clinical Global Impression score with Azithromycin. Adverse events were reported by 2.37% of patients.
Conclusion: Azithromycin demonstrates a significant improvement in clinical manifestations of URTIs, with a low incidence of adverse events.
Keywords: Azithromycin, Upper Respiratory Tract Infections (URTIs), URTIs, sore throat, pharyngeal erythema, tonsillar erythema, India
Introduction
Upper respiratory tract infections (URTIs) are a common clinical presentation in the outpatient department (OPD) in India.1 About 87% of respiratory infections are attributed to URTIs.2 Amongst bacterial pathogens, Streptococcus pyogenes, or Group A Streptococcus (GAS), causes a spectrum of diseases ranging from mild to severe pharyngitis.3 Other bacteria implicated in causing pharyngitis include Group B & C streptococci, Chlamydia pneumoniae, Mycoplasma pneumoniae, Haemophilus influenzae, Neisseria meningitidis, Neisseria gonorrhoeae, Arcanobacterium haemolyticum, Fusobacterium necrophorum, and Corynebacterium diphtheriae. Pharyngitis may accompany tonsillitis, tonsillar exudates, peritonsillar abscess, retropharyngeal abscess, and epiglottitis.4,5
In URTIs, clinicians prescribe antibiotics only if there are signs and symptoms of bacterial infections. Guidelines recommend macrolides and penicillins for the treatment of Group A Streptococcus-mediated URTIs. Azithromycin, an azalide macrolide antibiotic, has been approved to manage upper and lower respiratory tract infections in more than 100 countries.6 Azithromycin has a spectrum of activity that encompasses the pathogens implicated in causing upper and lower respiratory tract infections. The structural difference of azithromycin compared to other macrolides confers distinct pharmacokinetic and pharmacodynamic advantages, which make it the preferred macrolide antibiotic for the treatment of URTIs.7,8
Antimicrobial resistance (AMR) has emerged as a chronic public health problem globally, with the forecast of annual 10 million deaths by 2050. The prominent causes contributing to this problem are the misuse of antibiotics, inadequate duration of treatment,9,10 and injudicious use in industrial and animal husbandry sectors.11 The long duration of antibiotic treatment not only affects patient compliance but also increases overall cost and contributes to the emergence of AMR. Therefore, a shorter duration of antibiotic treatment is preferred to ensure better patient compliance and reduce the chances of developing AMR. Short-term courses of antibiotics may be an appropriate treatment for infections in a real-life scenario.12,13
There is limited Indian data assessing the effectiveness and safety of Azithromycin in managing URTIs such as tonsillitis and pharyngitis. The present study evaluates the effectiveness and safety of Azithromycin in treating URTIs in a real-life scenario.
Material and Methods
Study Design & Duration
This was a multicenter, retrospective, observational, real-world evidence study across 184 Ear, Nose, and Throat (ENT) Centres in India conducted over a period of 12 weeks.
Patient Characteristics
Medical records of adult patients (over 18 years old) who had provided consent for the future use of their medical record data for research were retrieved. The analysis focused on patients with URTIs who received Azithromycin 500 mg for 5 days, following local prescribing guidelines, and adhered to the treatment regimen.
Data Retrieval Method
Data was retrieved from the medical records of the patients, which matched the above inclusion criteria. The physicians retrieved anonymized data at the source in specially designed case record forms (CRF). Three important symptoms, viz., sore throat or difficulty in swallowing, fever, and interference with daily activities, along with three important signs, viz., pharyngeal erythema, tonsillar erythema, and exudates/plugs on tonsils, were of interest. These symptoms and signs were scored based on a three-point scale of 0−214 as mentioned in Table 1.
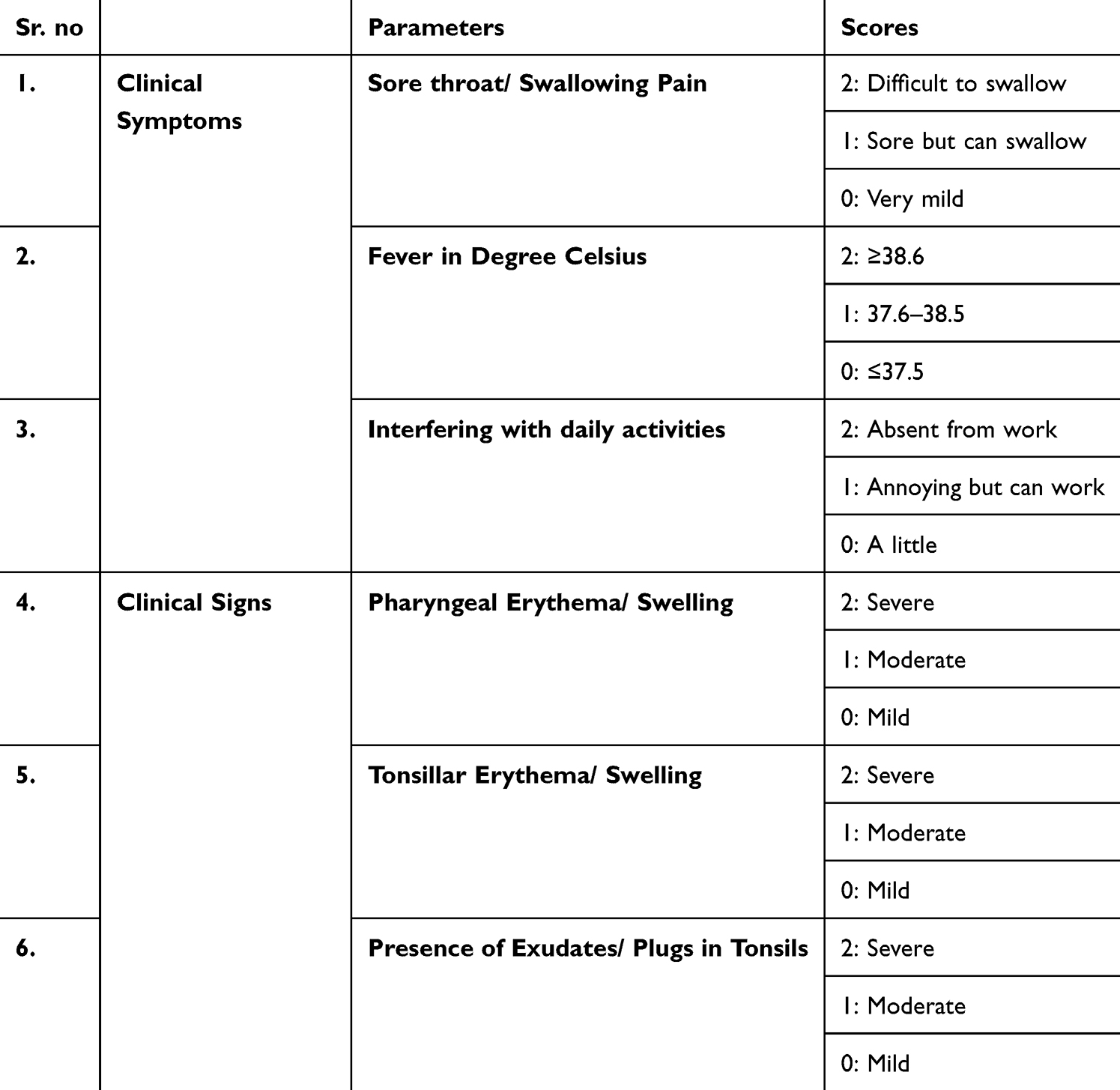 |
Table 1 Clinical Scoring System for Acute Pharyngo-Tonsillitis |
Safety information in terms of reported adverse events was also recorded. The physician’s clinical opinion of the effectiveness of azithromycin was recorded in CRF, which was an improvement in the clinical scoring system for the six parameters described earlier.
Assessment
A score for each symptom and sign was calculated, and a cumulative score for all six parameters were assessed. Improvement was noted after 5 days of azithromycin treatment. On day 5, the clinical global impression for change was analyzed using a 7-point rating scale.15,16
Outcome Measures and Statistical Analysis
Data was managed using Microsoft Excel. Categorical variables were presented as frequencies and percentages, while quantitative data was summarized using mean ± standard deviation (SD). The study evaluated the treatment’s effectiveness by applying a paired t-test to assess changes in mean scores from baseline to Day 5 for the discussed clinical parameters of URTIs. The Mc Nemar-Bowker test was used to evaluate the proportion of patients showing improvement in symptom scores from baseline to Day 5. A significance level of p < 0.05 (95% confidence interval) was used to determine statistical significance.
Sample Size
Convenience sampling was used as a practical method to obtain the patient’s data meeting inclusion criteria by utilizing the medical records available from the 184 ENT Centres across India within the stipulated time.
Ethical Consideration
The Indira IVF hospital institutional Ethics Committee approved this study. The study was registered with the Clinical Trial Registry of India (CTRI) with a registration number of CTRI/2024/04/066497.
Results
Baseline Characteristics
Last 06 months’ databases of 184 ENT Centres across India was evaluated to include the data of 884 patients who satisfied the inclusion criteria for assessment. The demographic parameters are mentioned in Table 2.
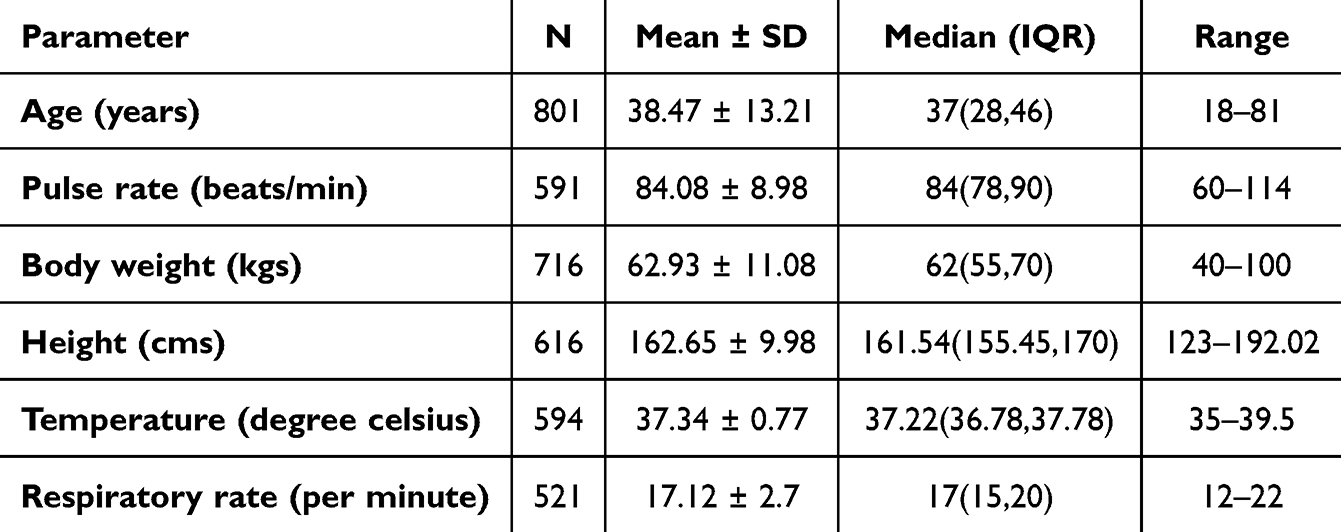 |
Table 2 Demographics and Baseline Parameters |
Effectiveness Outcomes
On Day 5, significant improvement in clinical scores across all six parameters was observed, affirming Azithromycin’s effectiveness in improving overall clinical outcomes in URTIs (Table 3).
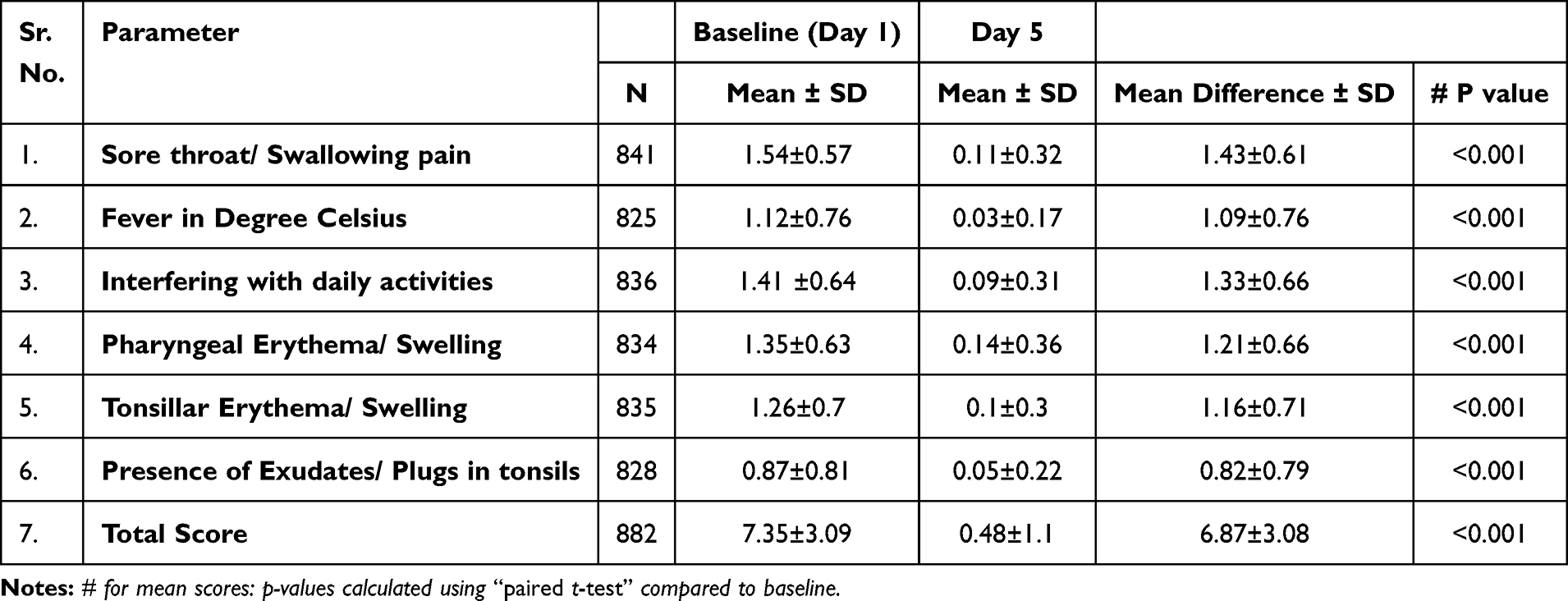 |
Table 3 Effectiveness Outcomes- Changes in Mean Clinical Score |
With Azithromycin 500 mg for 5 days’ therapy, significant reduction in proportion of patients reporting URTI symptoms and signs was noted. Proportion of patients reporting sore throat, with or without difficulty in swallowing, was reduced from 95.8% to 10.4% by day 5. Fever resolved in 97.4% of patients by day 5, and work absenteeism decreased dramatically from 47.9% patients reporting the same at baseline to only 1% patients by day 5. Also, 90.9% of patients had moderate to severe pharyngeal erythema at baseline which were reduced to 13.6% patients by day 5, and 84% patients with moderate to severe tonsillar erythema were reduced to only 9.6% patients. Only 4.4% of patients had moderate-to-severe tonsillar exudates by day 5, a notable decrease from 58.3% patients at baseline, demonstrating substantial clinical improvement for all parameters (Table 4).
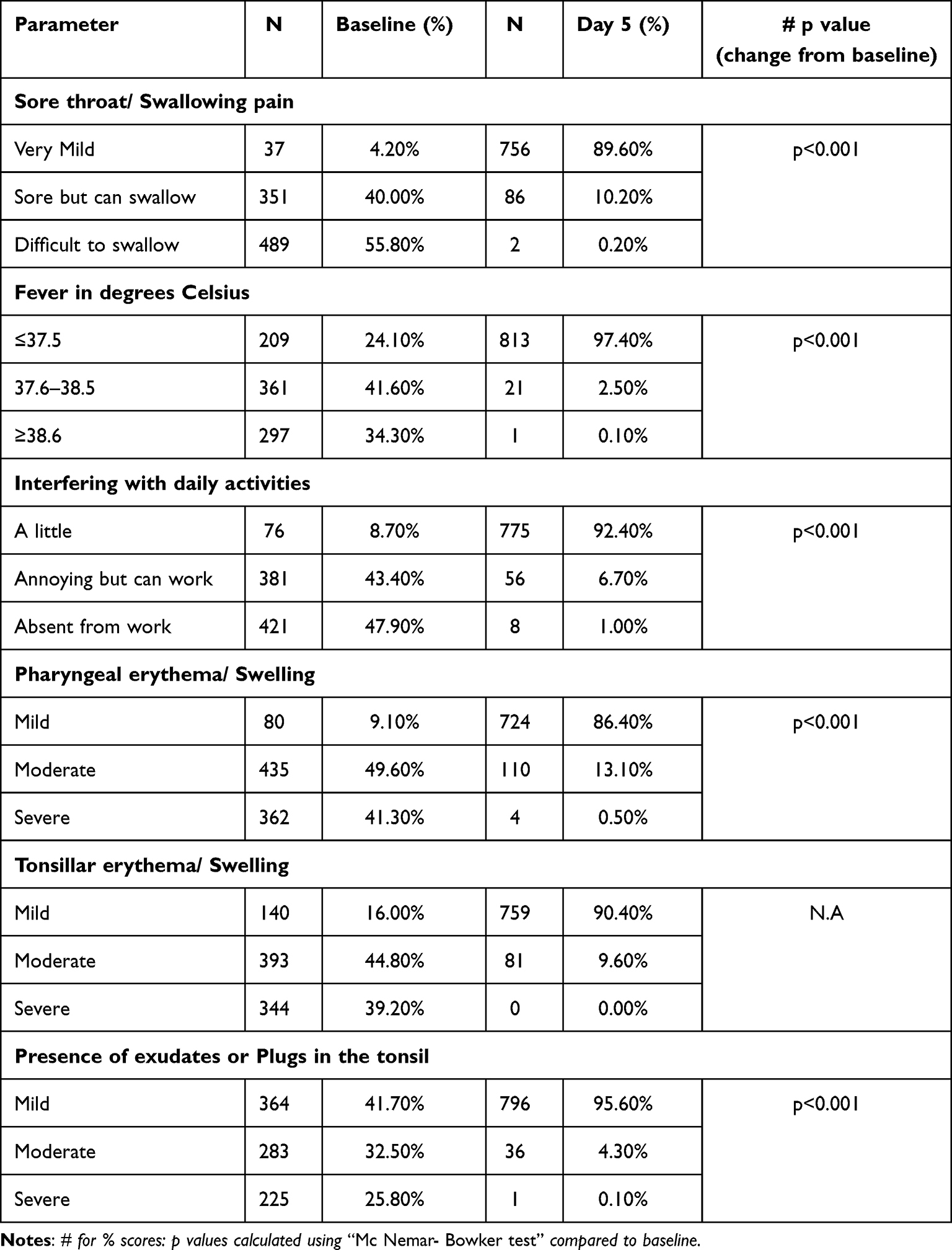 |
Table 4 Effectiveness Outcomes – Proportion of Patients Showing Improvement in Symptom Score |
As per investigators’ rating, 97.2% of patients reported much to very much improvement in Clinical Global Impression score with azithromycin 500 mg once daily for five days in treatment of URTIs (Table 5).
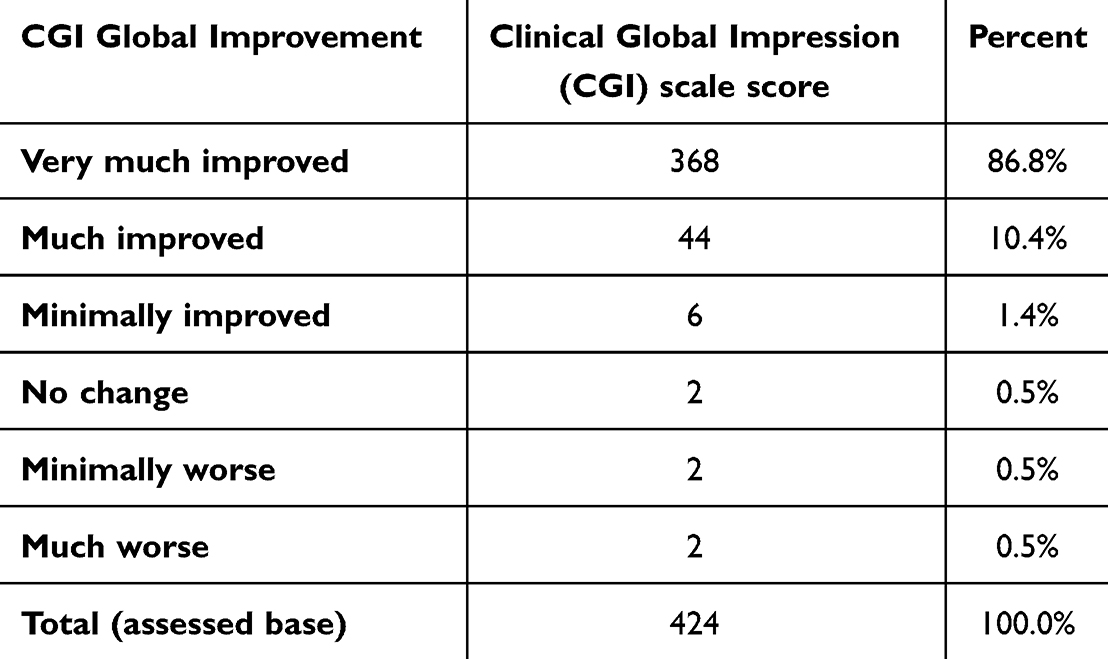 |
Table 5 Clinical Global Impression (CGI) Score at Day 5 |
Safety Assessment
Of 884 patients, 21 (2.37%) reported adverse events. Of these, 18 patients (85.7%) had gastrointestinal adverse effects, which included nausea, loose stools, and gastritis, classified as mild severity, and 3 patients (14.3%) had nonspecific adverse events.
Discussion
Acute URTIs are frequently encountered two to five times annually,17 indicating a significant disease burden. This contributes to 40% of workplace absenteeism and approximately 10% of visits to outpatient clinics and emergency departments.18,19 Current challenges in managing URTI include the changing sensitivity pattern of the bacterial pathogens responsible for URTI. Rising resistance rates to commonly used antibiotics have been documented across India.20–23
Azithromycin has been the most prescribed antibiotic globally for managing URTIs.24 Azithromycin is structurally different from other macrolides. The nitrogen atom in position 9 of the lactone cycle provides a second site of protonation and stabilizes azithromycin in the acidic gastric environment. Additionally, it leads to better absorption and improved gastrointestinal tolerability.25 Another benefit of azithromycin’s unique structure is its prolonged serum and tissue half-lives, which facilitate once-a-day administration. Azithromycin has an expanded spectrum of activity against respiratory pathogens such as H. influenzae, M. catarrhalis, and Streptococcus pneumoniae and against atypical pathogens, such as Legionella pneumophila, Chlamydia pneumoniae, and Mycoplasma pneumoniae.26 The improved activity of Azithromycin against gram-negative isolates such as H. influenzae and M. catarrhalis is also attributed to its structural difference compared to other macrolides.27
Azithromycin is extensively and rapidly distributed from serum into the intracellular compartments and finally into the tissues, from where it is subsequently eliminated slowly. It has a long elimination half-life (84–87 h).28,29 This leads to a good post-antibiotic effect.30 Macrophages and polymorphonuclear leucocytes concentrate azithromycin at levels greater than those found in tissues.31 Even after a single 500 mg dose of azithromycin, tissue concentrations exceed serum concentrations 100-fold.30 The presence of high azithromycin concentrations in tonsillar tissue is responsible for the efficacy of a once-daily regimen over five days in treating tonsillopharyngitis.31,32 Azithromycin has a spectrum of activity that encompasses the pathogens implicated in causing upper and lower respiratory tract infections.32 Azithromycin has anti-inflammatory and immunomodulatory properties by modulating phospholipids and transcription factors AP-1, NF-kappaB, and other inflammatory cytokines. Azithromycin can also modulate the activity of macrophages which contribute to the defense mechanisms of the body.33 Clinical cure rates of up to 99% after treatment with azithromycin have been reported in patients with group A beta-hemolytic streptococcal pharyngitis/tonsillitis in adults and adolescents.34 A recently published systematic review reported that Azithromycin demonstrated superior efficacy with fewer adverse effects, was cost-effective, and improved the quality of life in individuals with upper respiratory tract infections.35
The findings from this study present compelling clinical implications for the management of tonsillopharyngitis. With Azithromycin 5 days’ treatment, there was a remarkable reduction in symptom severity across key indicators such as sore throat and fever. This rapid alleviation of symptoms not only signifies treatment effectiveness but enhances patient comfort as well. Furthermore, the substantial decrease in interference with daily activities score by 93.6% signifies the practical impact of treatment, allowing patients to resume work faster. Moreover, the significant reductions in pharyngeal and tonsillar erythema scores by 89.7% and 92.1%, respectively, highlight the efficacy of the therapeutic approach in reducing inflammation. The shift from moderate to mild severity in both erythema types by day 5 suggests robust control of the inflammatory process. Additionally, the marked improvement in tonsillar exudates by 94.2% signifies effective management of the infectious component of tonsillopharyngitis. These clinical outcomes not only support the preferred treatment regimen but also emphasize the importance of timely intervention in achieving rapid symptom resolution and optimizing patient outcomes. These results were reflected in the high Clinical Global Impression (CGI) scores rated by the physicians on day 5.
The rapid resolution of symptoms such as sore throat with or without difficulty in swallowing and fever observed in the current study indicates good clinical response of patients to azithromycin in treating URTIs. Reduction in work absenteeism due to morbidity related to URTI after treatment with azithromycin reiterates the effectiveness and utility of azithromycin in the management of tonsillopharyngitis. A significant reduction in the severity of symptoms and erythema scores at day 5 as compared to baseline underscores the choice of azithromycin in the management of tonsillopharyngitis. The low incidence of adverse drug reactions with azithromycin, once-a-day dosing, and short duration of therapy improved patient adherence to treatment.
Strengths and Limitations
The study’s strength lies in its comprehensive evaluation of azithromycin treatment for URTIs, supported by a large sample size and a multicenter design. Incorporating a clinical scoring system further enhances the study’s robustness by providing objective measures to assess treatment effectiveness across diverse patient populations and settings. These methodological strengths underscore the study’s capacity to generate reliable and generalizable findings regarding the effectiveness of azithromycin in managing URTI. The retrospective nature of the study with biases like missing data, lack of control drug, and the inability to analyze concomitant medications affecting the overall course of treatment are a few limitations of the present study.
Conclusion
In India, URTIs impose a substantial burden. This multicenter real-world study underscores the pivotal role of five-day azithromycin therapy in managing acute URTIs. The treatment significantly improves key clinical manifestations of URTIs, viz., sore throat, fever, interference with daily activities, pharyngeal erythema, tonsillar erythema, and exudates, with a low incidence of adverse events. The study reports significant improvement in physician-rated clinical global impression scores in 97% of patients, emphasizing both the effectiveness and safety of azithromycin in treating URTIs.
Data Sharing Statement
Analyzed data are available and presented as tables. Individual de-identified participant data cannot be made available. This data will be available on request if really required after contacting the corresponding author.
Ethics and Consent Statements
The study was approved by Indira IVF Hospital Institutional Ethics Committee – Mumbai and registered with the Clinical Trial Registry of India (CTRI/2024/04/066497). The study was conducted in accordance with the norms of good clinical practice (GCP). Data of patients who had provided consent to use their data for future research was retrieved. Data anonymization process was carried out when collecting patients’ information.
Acknowledgments
Authors thank Ms. Vaishali Dalvi, Ms. Mihira Chavan for supporting data management, and Mr. N. Shrikant for supporting statistical analysis.
Funding
The research work and publication costs were funded by Alembic Pharmaceuticals Limited, India.
Disclosure
Dr. Dinesh Patil, Dr. Darshan Rana, and Dr. Onkar C. Swami are full-time employees of Alembic Pharmaceuticals Limited, India which actively markets Azithromycin. Other authors have no conflicts of interest to declare for this work.
References
1. Parmar DM, Jadav SP, Shah BK. Can azithromycin be substituted for amoxycillin in upper respiratory tract infections? An observation based on a drug utilization at some primary health centers. Indian J Pharmacol. 2007;39(1):55. doi:10.4103/0253-7613.30766
2. Jain N, Lodha R, Kabra SK. Upper respiratory tract infections. Indian J Pediatr. 2001;68(12):1135–1138. doi:10.1007/BF02722930
3. Shrestha S, Malla B, Haramoto E. Group A Streptococcus pyogenes in wastewater: applicability of wastewater-based epidemiology for monitoring the prevalence of GAS pharyngitis during the late COVID-19 pandemic phase. Sci Total Environ. 928:172447. doi:10.1016/j.scitotenv.2024.172447
4. Gottlieb M, Long B, Koyfman A. Clinical Mimics: an Emergency Medicine-Focused Review of Streptococcal Pharyngitis Mimics. J Emerg Med. 2018;54(5):619–629. doi:10.1016/j.jemermed.2018.01.031
5. Brennan-Krohn T, Ozonoff A, Sandora TJ. Adherence to guidelines for testing and treatment of children with pharyngitis: a retrospective study. BMC Pediatr. 2018;18(1):43. doi:10.1186/s12887-018-0988-z
6. Bisno AL, Gerber MA, Gwaltney JM, Kaplan EL, Schwartz RH. Infectious Diseases Society of America. Practice guidelines for the diagnosis and management of group A streptococcal pharyngitis. Infectious Diseases Society of America. Clin Infect Dis off Publ Infect Dis Soc Am. 2002;35(2):113–125. doi:10.1086/340949
7. Milstone AP. Use of azithromycin in the treatment of acute exacerbations of COPD. Int J Chron Obstruct Pulmon Dis. 2008;3(4):515–520. doi:10.2147/COPD.S1189
8. Ioannidis JP, Contopoulos-Ioannidis DG, Chew P, Lau J. Meta-analysis of randomized controlled trials on the comparative efficacy and safety of azithromycin against other antibiotics for upper respiratory tract infections. In: Database of Abstracts of Reviews of Effects (DARE): Quality-assessed Reviews [Internet] [Internet]. Centre for Reviews and Dissemination (UK); 2001
9. Endashaw Hareru H, Sisay D, Kassaw C, Kassa R. Antibiotics non-adherence and its associated factors among households in southern Ethiopia. SAGE Open Med. 2022;10:20503121221090472. doi:10.1177/20503121221090472
10. O’Neill J. Antimicrobial Resistance: tackling a crisis for the health and wealth of nations. [Internet]. HM Government. Wellcome Trust; 2014 20. Available from: https://amr-review.org/sites/default/files/AMR%20Review%20Paper%20-%20Tackling%20a%20crisis%20for%20the%20health%20and%20wealth%20of%20nations_1.pdf.
11. Samreen AI, Malak HA, Abulreesh HH, Abulreesh HH. Environmental antimicrobial resistance and its drivers: a potential threat to public health. J Glob Antimicrob Resist. 2021;27:101–111. doi:10.1016/j.jgar.2021.08.001
12. Falagas ME, Karageorgopoulos DE, Grammatikos AP, Matthaiou DK. Effectiveness and safety of short vs. long duration of antibiotic therapy for acute bacterial sinusitis: a meta-analysis of randomized trials. Br J Clin Pharmacol. 2009;67(2):161–171. doi:10.1111/j.1365-2125.2008.03306.x
13. Spellberg B, Rice LB. Duration of Antibiotic Therapy: shorter Is Better. Ann Intern Med. 2019;171(3):210–211. doi:10.7326/M19-1509
14. Suzumoto M, Hotomi M, Billal DS, Fujihara K, Harabuchi Y, Yamanaka N. A scoring system for management of acute pharyngo-tonsillitis in adults. Auris Nasus Larynx. 2009;36(3):314–320. doi:10.1016/j.anl.2008.07.001
15. Guy W. “Clinical Global Impressions”. ECDEU Assessment Manual for Psychopharmacology—Revised. Department of Health, Education, and Welfare; Public Health Service, Alcohol; Drug Abuse, and Mental Health Administration Rockville, MD: U.S; National Institute of Mental Health; Psychopharmacology Research Branch; Division of Extramural Research Programs, 218–222; 1976: https://search.worldcat.org/title/ECDEU-assessment-manual-for-psychopharmacology/oclc/2344751.
16. Busner J, Targum SD. The Clinical Global Impressions Scale. Psychiatry Edgmont. 2007;4(7):28–37.
17. Johnston S, Holgate S. Epidemiology of Viral Respiratory Infections. In: Viral and Other Infections of the Human Respiratory Tract. London: Chapman & Hall; 1996:1–38.
18. Fendrick AM, Monto AS, Nightengale B, Sarnes M. The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch Intern Med. 2003;163(4):487–494. doi:10.1001/archinte.163.4.487
19. Kirkpatrick GL. The common cold. Prim Care. 1996;23(4):657–675. doi:10.1016/S0095-4543(05)70355-9
20. Fazaludeen Koya S, Ganesh S, Selvaraj S, et al. Antibiotic consumption in India: geographical variations and temporal changes between 2011 and 2019. JAC-Antimicrob Resist. 2022;4(5):dlac112. doi:10.1093/jacamr/dlac112
21. Laxminarayan R, Chaudhury RR. Antibiotic Resistance in India: drivers and Opportunities for Action. PLoS Med. 2016;13(3):e1001974. doi:10.1371/journal.pmed.1001974
22. Taneja N, Sharma M. Antimicrobial resistance in the environment: the Indian scenario. Indian J Med Res. 2019;149(2):119–128. doi:10.4103/ijmr.IJMR_331_18
23. Gandra S, Joshi J, Trett A, Lamkang AS, Laxminarayan R. Scoping Report on Antimicrobial Resistance in India. Center for Disease Dynamics, Economics & Policy.; 2017
24. Alvear G, Santibáñez L, Sepúlveda R, Ramírez V, Martínez B. Prescription of antibiotics in acute respiratory infections non-pneumonia in a private outpatient practice. Rev Médica Chile. 2022;150(8):1000–1009. doi:10.4067/S0034-98872022000801000
25. Lima L, Antonio Pinto J, Nunes H, et al. Efficacy of azithromycin versus other antibiotics in the treatment of patients with upper respiratory tract infections. Clin Microbiol Infect Dis. 2021;6(1):1–4. doi:10.15761/CMID.1000183
26. Dunn CJ, Barradell LBA. A review of its pharmacological properties and use as 3-day therapy in respiratory tract infections. Drugs. 1996;51(3):483–505. doi:10.2165/00003495-199651030-00013
27. Pechère JC. Effect of the molecular structure of azithromycin on pharmacokinetics and the antimicrobial activity. Pathol Biol (Paris). 1995;43(6):483–487.
28. Chang WK, Chen CH, Chen YA, et al. Unique Pharmacokinetic Parameters with Prolonged Elimination Half-life of Oral Azithromycin and Analysis of Pharmacokinetic Phenotype in Young Taiwanese Population. Int J Pharmacol. 2018;14(7):981–991. doi:10.3923/ijp.2018.981.991
29. Kong FYS, Rupasinghe TW, Simpson JA, et al. Pharmacokinetics of a single 1g dose of azithromycin in rectal tissue in men. PLoS One. 2017;12(3):e0174372. doi:10.1371/journal.pone.0174372
30. Lalak NJ, Morris DL. Azithromycin clinical pharmacokinetics. Clin Pharmacokinet. 1993;25(5):370–374. doi:10.2165/00003088-199325050-00003
31. Lode H. The pharmacokinetics of azithromycin and their clinical significance. Eur J Clin Microbiol Infect Dis off Publ Eur Soc Clin Microbiol. 1991;10(10):807–812. doi:10.1007/BF01975832
32. Firth A, Prathapan PA. The First Broad-spectrum Therapeutic. Eur J Med Chem. 2020;207(1):112739. doi:10.1016/j.ejmech.2020.112739
33. Patel PH, Hashmi MF. Macrolides. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024: http://www.ncbi.nlm.nih.gov/books/NBK551495/.
34. Jorgensen DM. Single-dose extended-release oral azithromycin vs. 3-day azithromycin for the treatment of group A beta-haemolytic streptococcal pharyngitis/tonsillitis in adults and adolescents: a double-blind, double-dummy study. Clin Microbiol Infect off Publ Eur Soc Clin Microbiol Infect Dis. 2009;(12):1103–1110.
35. Swami O, Bharathi MB, Dutt S, et al. The Efficacy, Safety, and Economic Outcomes of Using Azithromycin in Respiratory Tract Infections: a Systematic Literature Review. Medical Research Archives. 12(9).
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.