")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Biomarkers of Suicidal Ideation in Depression: Insights From VMHC Analysis and Machine Learning
Authors Wang X, Liu F, Hu X, Zhang Q, Guan X, Wu J, Long X, Lu Z
Received 31 October 2024
Accepted for publication 17 February 2025
Published 13 April 2025 Volume 2025:21 Pages 855—865
DOI https://doi.org/10.2147/NDT.S500301
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Rakesh Kumar
Xinlin Wang,1,* Fei Liu,1,* Xinyi Hu,1 Qiong Zhang,1 Xiaofeng Guan,1 Jiaxin Wu,1 Xiangyun Long,2 Zheng Lu1
1Department of Psychiatry, Tongji Hospital, School of Medicine, Tongji University, Shanghai, 200092, People’s Republic of China; 2Department of Psychiatry, the Affiliated Brain Hospital, Guangzhou Medical University, Guangzhou, 510370, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zheng Lu, Department of Psychiatry, Tongji Hospital, School of Medicine, Tongji University, 389 Xincun Road, Shanghai, 200092, People’s Republic of China, Email [email protected] Xiangyun Long, Department of Psychiatry, the Affiliated Brain Hospital, Guangzhou Medical University, Guangzhou, 510370, People’s Republic of China, Email [email protected]
Background: Suicidal ideation (SI) is a major cause of death in patients with major depressive disorder (MDD). Although current clinical tools can assess suicide risk, objective neurobiological markers based on research remain lacking. Clinical evidence suggests that resting-state functional magnetic resonance imaging (rs-fMRI) studies utilizing voxel-mirrored homotopic connectivity (VMHC) analysis can uncover the neural mechanisms underlying mental disorders. This study explores differences in interhemispheric connectivity between MDD patients with and without SI, aiming to identify imaging biomarkers for suicide risk.
Methods: This study included 48 SI patients and 44 non-SI patients. VMHC values were calculated to assess interhemispheric functional connectivity. Brain regions with significant differences between the groups were identified. A support vector machine (SVM) model was applied to evaluate the utility of VMHC values in distinguishing SI patients from non-SI patients with MDD.
Results: Patients with suicidal ideation exhibited significantly increased VMHC values in the superior frontal gyrus, putamen, inferior temporal gyrus, and cerebellum compared to those without suicidal ideation. The SVM model achieved an accuracy of 77.2%, sensitivity of 83.3%, specificity of 70.5%, and an area under the curve (AUC) of 0.81. When combining VMHC values from multiple brain regions, classification accuracy improved to 86.8%.
Conclusion: MDD patients with SI exhibit abnormal interhemispheric connectivity, with VMHC abnormalities in specific brain regions serving as potential biomarkers for suicide risk. The integration of machine learning and neuroimaging highlights the clinical relevance of VMHC as a tool for early detection and targeted intervention in suicide prevention.
Keywords: suicidal ideation, major depressive disorder, support vector machine, fMRI, voxel-mirrored homotopic connectivity, biomarkers, neuroimaging
Introduction
Major depressive disorder (MDD) represents a critical global public health issue, with a high disability rate and an increasing prevalence.In recent years, the global suicide rate has continued to rise, posing a significant challenge in the field of public health. According to data from the World Health Organization (WHO), approximately 800,000 people die by suicide each year, making it the second leading cause of death among individuals aged 15 to 29. It is estimated that approximately 27% of individuals will experience MDD or related symptoms at some point in their lives.1,2 Suicide, the most severe outcome of depression, poses a significantly elevated risk for individuals with MDD, imposing a profound burden on patients, their families, and society at large. However, the underlying mechanisms of MDDSI pathogenesis remain poorly understood. Additionally, suicidal ideation (SI) is not merely a symptom of depression but is thought to be driven by specific neurobiological processes. Investigating the neural mechanisms of SI is therefore crucial for early identification and intervention efforts.3 The process of suicide is generally divided into three stages: the generation of SI, the development of a suicide attempt (SA), and the execution of suicidal behavior.4 SI is a key predictor of future suicidal behavior and has been identified as a significant risk factor for suicide attempts and death by suicide.5,6 Consequently, SI can be considered the initial step in the progression towards suicide. Understanding the brain changes associated with SI in MDD patients is essential for elucidating the development of SI, which may facilitate early interventions and reduce suicide rates. Despite this, the precise neural mechanisms involved in suicide pathogenesis remain largely unknown.7,8 Moreover, it can overcome the subjectivity and inaccuracy of traditional psychological assessments by providing objective neurobiological data, enabling the identification of high-risk individuals who may not openly express or may conceal suicidal ideation. This not only facilitates early intervention and personalized treatment but also advances the understanding of the neural mechanisms underlying suicide.
In recent years, resting-state functional magnetic resonance imaging (rs-fMRI) has emerged as an effective tool for investigating the neural mechanisms underlying mental disorders by detecting neuronal activity that reflects the brain’s functional dynamics.9 Although increasing evidence suggests a relationship between disrupted neural connectivity and the cognitive and emotional dysfunctions associated with MDD, there remains no consensus on the specific brain regions linked to suicidal ideation (SI) in patients with depression.10 Taylor et al reported that, compared to patients with depression without SI, those with SI exhibited reduced cortical thickness in the insula, caudal middle frontal gyrus, superior parietal gyrus, and temporal gyrus.11 Similarly, Sun et al found significant differences in the fractional amplitude of low-frequency fluctuations (fALFF) in the bilateral cerebellum (CB), superior frontal gyrus (SFG), and left parahippocampal gyrus (PHG), as well as in the gray matter volume (GMV) of the left superior temporal gyrus (STG) between MDD patients with SI (R-MDD-SI) and those without SI (R-MDD-NSI).12 Additionally, other studies have revealed abnormal gray matter volumes in patients with SI, particularly in the lingual gyrus.13 At the cortical level, SI patients show reduced functional connectivity among the right anterior cingulate cortex (ACC), medial orbitofrontal cortex (OFC), and right middle temporal gyrus, while dynamic functional connectivity between the left posterior cingulate cortex (PCC) and left inferior frontal gyrus is increased, reflecting more frequent switching between these regions.13,14 Moreover, Chen et al found that SI was associated with decreased resting-state regional homogeneity (ReHo) in the right insula and right frontal lobe, alongside increased ReHo in the left middle temporal gyrus and right middle frontal gyrus.15 There is growing evidence that structural and functional changes in the frontal, temporal, and parietal lobes are linked to SI.16 These interconnected brain regions are involved in emotional processing, regulation, and self-referential thinking, but their functions become disrupted in MDD. The most common finding across studies on SI in MDD is the presence of abnormalities in brain regions within the default mode network (DMN). Therefore, we focused on exploring the abnormalities in the DMN in MDD patients with SI. Specifically, we aimed to differentiate between MDD patients with SI (MDDSI) and those without SI (MDDNSI) based on these abnormal brain regions.
Voxel-mirrored homotopic connectivity (VMHC) is a novel rs-fMRI parameter commonly used to assess the degree of functional connectivity between the bilateral cerebral hemispheres. It has been extensively applied to investigate abnormal homotopic connectivity in various psychiatric disorders.17–19 This parameter quantifies the functional connectivity between each voxel in one hemisphere and its mirrored counterpart in the opposite hemisphere during resting state, reflecting the synergistic interaction between the two hemispheres.20 This synergy plays a critical role in coordinating cognitive, emotional, and behavioral functions, and impairments in these areas can contribute to suicidal tendencies.21,22 In patients with depressive disorders, the potential of VMHC has also been validated. For instance, Guo found that MDD patients exhibited significantly reduced VMHC levels in core regions of the default mode network (DMN), such as the anterior cingulate cortex (ACC) and posterior cingulate cortex (PCC).23 These regions are closely associated with rumination, a common symptom in MDD. Such abnormalities may lead to difficulties in processing emotional stimuli and self-referential thinking, thereby increasing the risk of suicidal ideation (SI). Traditional local indicators, such as ALFF or ReHo, often fail to capture this global dysfunction. Notably, VMHC excels in revealing abnormalities in cross-hemispheric collaboration within the DMN. Abnormalities in the DMN have been repeatedly identified as a core feature of SI in MDD. By integrating VMHC analysis, researchers can gain deeper insights into the specific role of the DMN in the development of SI, providing new clues for potential clinical interventions. These findings lay a foundation for the development of objective clinical tools, facilitating the early identification of high-risk individuals and the implementation of interventions, ultimately reducing the risk of suicide.Furthermore, VMHC is likely to be sensitive to MDD-related lesions, as alterations in any region of one hemisphere can impact the VMHC of corresponding areas.Most previous studies12,24–26 have focused on regions of interest (ROI), such as ROI-ROI, ROI-voxel, or network-based functional connectivity in MDDSI patients, while few have investigated changes in VMHC among MDDSI patients. Currently, no studies have combined VMHC features with machine learning methods, such as Support Vector Machine (SVM), to differentiate between MDDSI and MDDNSI patients. However, SVM demonstrates exceptional performance in handling small sample sizes and high-dimensional datasets, making it particularly suitable for neuroimaging studies of psychiatric disorders with limited sample sizes. Integrating VMHC with SVM could support the development of objective clinical tools, facilitating early intervention and reducing the risk of suicide.
Materials and Methods
Participants
A total of 48 right-handed MDDSI patients (20 males and 28 females), aged 18–65 years, along with 44 age-, gender-, and education-matched MDDNSI patients were included in this study. The study protocol was thoroughly explained to all participants, and informed consent was obtained prior to their participation. This study was approved by the Ethics Committee of Tongji Hospital in Shanghai, China, and complies with the Declaration of Helsinki.
The inclusion criteria were as follows: (1) patients were diagnosed with MDD based on the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5); (2) imaging findings and symptom information were available; (3) patients were assessed using the Beck Scale for Suicidal Ideation (BSI), which contains 19 items;27 (4) the Hamilton Depression Rating Scale (HAMD-17) score was≥17.28 The exclusion criteria were as follows: (1) patients had other mental disorders such as schizophrenia, bipolar disorder, or neurodevelopmental disorders; (2) patients had current or previous drug dependence or abuse (alcohol, cocaine, or other substances); (3) patients had a history of neurological diseases, physical illnesses, or severe traumatic brain injury; (4) patients had contraindications to MRI.
Assessment
SI was assessed based on the Beck Scale for Suicide Ideation (BSI) with 19 items. This study primarily used item 4 (“Have you ever had thoughts of actively ending your own life?”) and item 5 (“Do you wish death would come naturally without you taking any action?”) to categorize patients. Patients with scores greater than 0 were assigned to the MDDSI group (Major Depressive Disorder with Suicidal Ideation), while the remaining patients were assigned to the MDDNSI group (Major Depressive Disorder without Suicidal Ideation).
HAMD-17 (17-item Hamilton Depression Rating Scale): This scale was used to assess the severity of depressive symptoms, including low mood, sleep disturbances, and somatic symptoms. A total score of HAMD-17 ≥17 was used as an inclusion criterion to ensure that patients met the threshold for moderate to severe depressive symptoms.Both the BSI and HAMD-17 have been validated in multiple studies for their high reliability and validity. They have demonstrated high sensitivity and specificity in assessing suicidal ideation and are strongly correlated with the results of other psychological measurement tools.29 HAMD-17 has also shown excellent reliability and validity in evaluating the severity of depression, with outstanding consistency in predicting depression severity and clinical diagnoses.30 These studies indicate that both scales are reliable assessment tools in their respective fields. The high internal consistency and extensively validated cross-cultural applicability of these scales provide a solid foundation for replicating research.
Imaging Data Acquisition
Imaging was performed using a Siemens Magnetom Verio 3.0T MRI scanner at Tongji Hospital, Shanghai, China. Foam padding was applied to minimize head movement. A standard magnetic coil was used for radio frequency transmission and reception of nuclear magnetic resonance signals. Subjects were instructed to close their eyes but remain awake during the scan. Spin echo planar imaging (EPI) was employed parallel to the anterior-posterior commissure plane. The scanning parameters were as follows: repetition time (TR) = 2530 ms, echo time (TE) = 3 ms, image matrix = 64 × 64, flip angle (FA) = 90°, field of view (FOV) = 384×384 mm², 30 consecutive slices with a thickness of 3.6 mm and spacing of 4.5 mm, and a total scanning time of 8 minutes (240 volumes). High-resolution structural images were acquired using a fast gradient echo T1-weighted sequence: TR = 2530 ms, TE = 3 ms, FOV = 256×256 mm², matrix = 256 × 256, slice thickness = 1 mm with no gap, inversion time (TI) = 1100 ms, and FA = 7°.
Image Preprocessing
The Data Processing Assistant for Resting-State fMRI (DPARSF5.4, http://rfmri.org/DPARSF) was used to preprocess the functional images.31 The first 10 time points were discarded to ensure stable signal conditions, utilizing Statistical Parametric Mapping software (SPM12, http://www.fil.ion.ucl.ac.uk/spm). Subsequently, slice timing and head motion corrections were applied. DARTEL registration was employed to normalize the participants’ images to the MNI standard space. The fMRI data were then spatially smoothed using a Gaussian kernel with a full width at half maximum (FWHM) of 4 mm. The Friston 24-parameter model was used to regress out nuisance covariates, including head motion, and to correct for linear drift. Band-pass filtering (0.01–0.1 hz) was applied to reduce low-frequency drift and high-frequency noise.
VMHC Calculation
VMHC analysis was performed using DPARSF 6.2 software. First, the time series of each voxel in one hemisphere were extracted for each subject. Then, the Pearson correlation coefficient between the time series in one hemisphere and those in the symmetrical hemisphere was calculated. Subsequently, the correlation coefficients were transformed into Z-values using Fisher’s Z-transformation, and a whole-brain VMHC map was generated for each participant. Brain regions showing significant differences between MDDSI and MDDNSI patients were selected as regions of interest (ROIs). The average VMHC of these ROIs was extracted for all participants to determine whether these regions exhibit specific VMHC abnormalities in MDDSI patients compared to MDDNSI patients.
Statistical Analysis
Clinical and neuroimaging data were compared between MDDSI and MDDNSI patients. SPSS 25.0 software (Chicago, IL) was used for statistical analysis of clinical data, while DPARSF software on the MatLab 2022b platform was employed for neuroimaging data analysis. Continuous data with a normal distribution and homogeneity of variance were compared using independent sample t-tests, and categorical data were compared using Chi-square tests. Continuous data are expressed as the mean and standard deviation, while qualitative data are reported as the median and quartiles. If a significant difference was observed between the two groups, gender, age, and education level were used as covariates for RS-fMRI data analysis. Multiple comparisons were corrected using Gaussian Random Field (GRF) correction. A statistically significant difference was defined as p < 0.001 at the voxel level and p < 0.05 at the cluster level. The VMHC values of abnormal brain regions were extracted for further correlation analysis and classification.
The support vector machine (SVM) is a powerful supervised learning algorithm, known for its strong performance in handling small sample sizes, high-dimensional feature spaces, and nonlinear problems.32 Using SVM, the VMHC values of brain regions were treated as potential neuroimaging markers, and the accuracy of differential classification was validated, enhancing our understanding of the neural mechanisms underlying SI in MDD. This method was employed to assess whether the extracted VMHC values could distinguish MDDSI patients from MDDNSI patients. The PRoNTo toolbox for SVM was used to achieve optimal accuracy, sensitivity, and specificity by applying the “Leave-One-Out” method. We utilized a binary SVM with a linear kernel to classify the VMHC features of the MDDSI and MDDNSI groups and optimized the regularization parameter C through grid search. The area under the receiver operating characteristic curve (AUC) was calculated to represent the predictive performance of the SVM model.
Results
Demographic Information and Standardized Tests
As shown in Table 1, there were no statistically significant differences in gender, age, education level, duration of illness, onset rate, HAMD-17, and HAMA between the SI group and the NSI group (all P > 0.05).
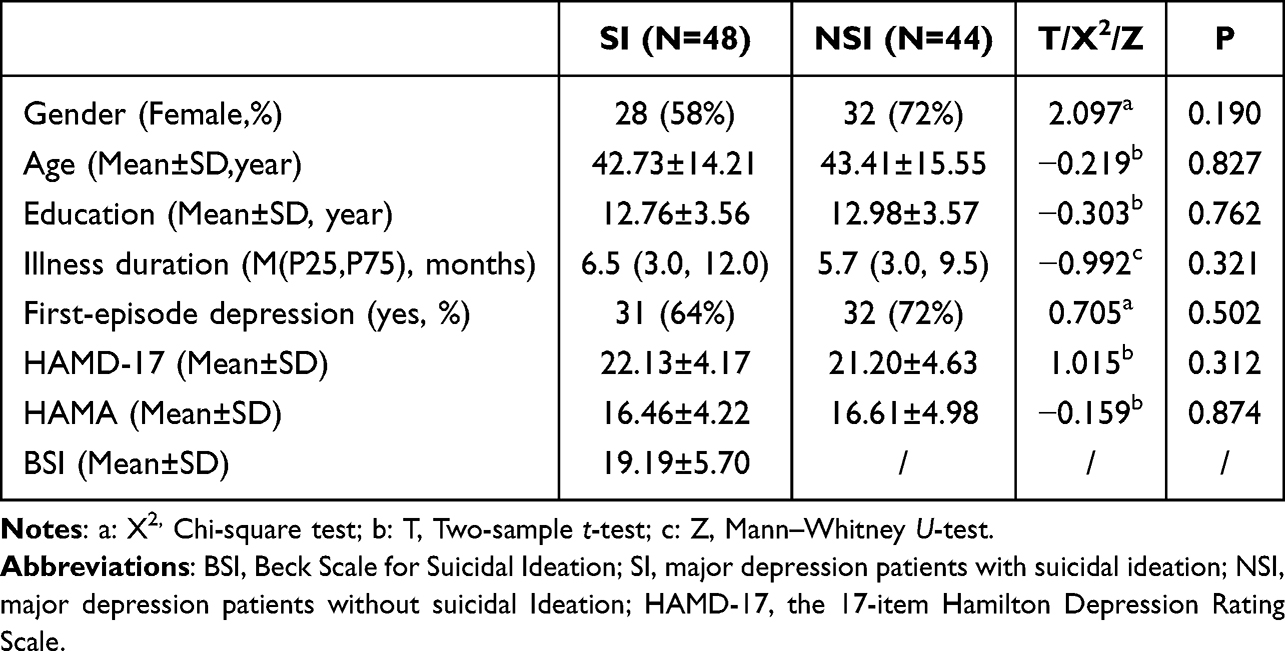 |
Table 1 Demographic and Clinical Characteristics of the SI and NSI Groups (Statistical Values Included) |
Group Comparisons in VMHC Maps
The VMHC values of bilateral superior frontal gyrus, putamen, inferior temporal gyrus, and cerebellum in the MDDSI patients were markedly higher than in the MDDNSI group (Table 2 and Figure 1) (GRF correction; voxel level, p<0.001, cluster level, p<0.05; cluster size, >64).
 |
Table 2 Significant VMHC Differences Across Groups |
 |
Figure 1 VMHC differences between MDDSI and MDDNSI patients, highlighting regions with significant interhemispheric connectivity alterations. |
Correlations Analyses
Figure 2 shows the correlation analysis between VMHC and clinical features. DPABI software of MatLab2022b platform was used to extract VMHC values of different brain regions of all the subjects. Results showed the VMHC values of bilateral inferior temporal gyrus were positively related to BSI, and the VMHC values of bilateral putamen were positively related to BSI.
 |
Figure 2 Correlation analysis between VMHC values and BSI scores, indicating the relationship between altered connectivity and suicidal ideation severity. |
SVM Results
The SVM was utilized to model VMHC values to evaluate whether these metrics could effectively distinguish between patients with MDDSI and MDDNSI. The analysis revealed that the inferior temporal gyrus demonstrated optimal classification performance, achieving an accuracy of 81.6%, sensitivity of 70.5%, specificity of 83.3%, and an AUC of 0.81 (Table 3 and Figure 3). When differentiating between MDDSI and MDDNSI patients, the superior frontal gyrus was identified as the second most effective Region of Interest (ROI), with an accuracy of 74.1%, sensitivity of 68.2%, specificity of 72.9%, and an AUC of 0.74 (Table 3). Upon integrating the abnormal VMHC values across these four brain regions, the overall model significantly improved its predictive accuracy for classifying MDDSI versus MDDNSI patients, with an accuracy of 86.8%, sensitivity of 82.9%, and specificity of 80.4%, achieving an AUC of 0.84.
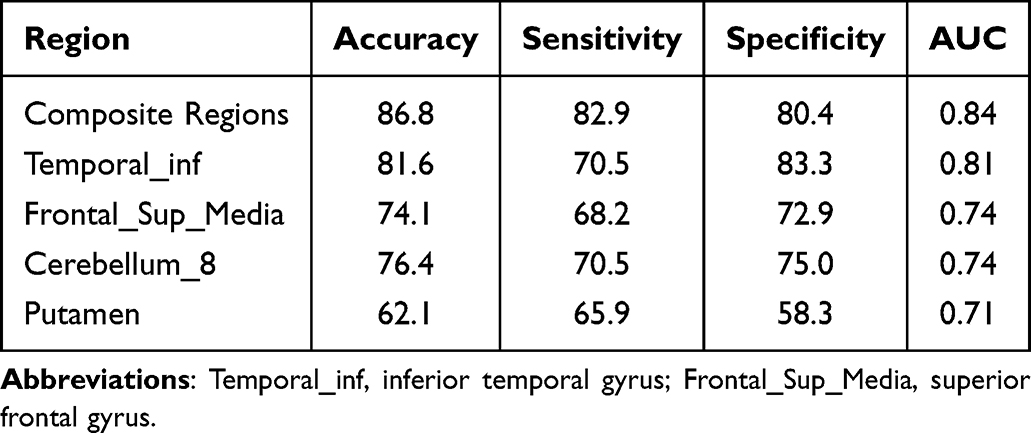 |
Table 3 SVM Classification Results, Showing Accuracy, Sensitivity, Specificity, and AUC Values for Each ROI |
 |
Figure 3 SVM model performance for distinguishing between MDDSI and MDDNSI patients based on VMHC values, with a focus on the inferior temporal gyrus. |
Discussion
In this study, VMHC was utilized to compare brain activity between MDDSI and MDDNSI patients. The results indicated that, relative to the MDDNSI group, the MDDSI group exhibited significantly increased VMHC in the bilateral superior frontal gyrus, putamen, inferior temporal gyrus, and cerebellum, reflecting enhanced synchrony and compensatory information exchange. Furthermore, the VMHC values in the bilateral inferior temporal gyrus and putamen were positively correlated with BSI scores in MDDSI patients. According to the SVM analysis, the VMHC values in the inferior temporal gyrus and superior frontal gyrus demonstrated the highest AUC, sensitivity, specificity, and accuracy. When integrating multiple abnormal brain regions, the classification accuracy increased to 86.8%.
The frontal lobe, located at the front of the brain, is one of its most crucial regions. It is closely associated with advanced cognitive functions such as emotional regulation, thinking, attention, problem-solving, motivation, and behavioral planning. The superior frontal gyrus and inferior temporal gyrus are key components of the default mode network, which is involved in various neural functions. The default mode network plays an important role in emotional processing, self-regulation, activity, and recalling experiences.32,33 Li et al found that MDD patients exhibited increased GMV in the right frontal gyrus after electroconvulsive therapy (ECT).34 Pearson correlation analysis revealed that baseline BSI scores were negatively correlated with the GMV of the left superior frontal gyrus.35 It has been reported that right frontal gyrus activity decreases in depressed patients who attempted suicide after being exposed to angry facial expressions. Similarly, adult male subjects with suicide attempts showed reduced activity in the right frontal gyrus in response to strong angry and neutral facial expressions, compared to healthy subjects and depressed individuals without suicide attempts.36 This suggests that individuals with suicide attempts may be more sensitive to opposing opinions, more prone to act on negative emotions, and less attentive to mild positive stimuli. Such sensitivity reflects a heightened response to failure signals, a characteristic of the cognitive model of suicide.In addition, Kim et al, using network-based statistics (NBS), reported a functional connectivity (FC) network that could distinguish MDD patients with SI from those without SI, with some areas overlapping with the left frontal gyrus.37 Kuang et al found that baseline BSI scores in patients with SI were negatively correlated with ALFF values in the left inferior temporal gyrus, and that ALFF values in this region decreased after ECT.38 Li et al found that the dynamic parameters of the left inferior temporal gyrus were reduced (indicating less temporal variability) in MDD patients with SI compared to those without SI. This temporal variability could predict SI severity (r = 0.43, p = 0.03).39 Zhang et al observed delayed responses in the right putamen and left inferior temporal gyrus in SI patients, compared to a control group.40 In SI patients, the left inferior temporal gyrus showed reduced activity, indicating the importance of homologous connectivity between these brain regions in the pathogenesis of depression.
Joana et al found a significant association between SI and the functional connectivity network, which includes connections among the superior frontal gyrus, cerebellum, and the temporal-occipital region. This suggests that the cerebellum may be involved in the functional connectivity network related to SI.41 Studies have confirmed that the cerebellum plays an important role in higher-level cognitive processes and is involved in emotion regulation in diseases such as depression and bipolar disorder (BD). Research has also shown that cerebellar volume is reduced in BD patients who have attempted suicide. Shaffer et al reported that the cerebellum is part of the neural circuits associated with suicidal behavior in patients with depression and bipolar disorder.42–44 Zhang et al found that both the left posterior lobe of the cerebellum in suicide patients and the right cerebellum in suicide attempt (SA) patients exhibited delayed responses. Additionally, suicide attempt victims showed reduced activity in the right cerebellum when exposed to neutral faces, compared to exposure to mild, happy, and neutral faces.45 Furthermore, cerebellar volume was reduced in patients with highly lethal suicide attempts compared to non-suicidal patients.46
The putamen, a part of the striatum, is typically associated with visual responses, motor-related activities, and reward responses.47 Several studies have explored the relationship between the putamen and suicide. In adolescent suicide research, a lack of serotonin release is considered a biomarker of suicidal behavior. Serotonin is released from the raphe nucleus in the brainstem to the dorsal striatum, which is composed of the caudate nucleus and putamen. In SI patients, serotonin levels in the putamen are significantly reduced.48,49 In a PET study conducted on adults with depression and at least one suicide attempt, the serotonin binding potential, measured by serotonin transporter (SERT) activity, was significantly reduced in the midbrain/pons and putamen compared to healthy controls.50 In another fMRI study on adolescents, an increase in SI was found to be associated with decreased putamen activity during social exclusion tasks.51 Studies have also reported reduced activity in the right putamen of SI patients.40 During cognitive and emotional tasks, putamen activity decreases, suggesting that the putamen may help explain the relationship between cognition, emotion, and suicide. Reduced connectivity in the putamen has been observed during motor tasks. In cases of suicide attempts (SA) with high impulsivity, putamen volume was found to be reduced.52,53 Based on these findings, putamen dysfunction may be associated with a higher risk of SI and may contribute to suicide attempts by increasing impulsivity. This study deepens the understanding of the neural mechanisms underlying suicidal ideation (SI) by revealing the close association between SI and functional abnormalities in the putamen, cerebellum, superior frontal gyrus, and inferior temporal gyrus. Functional abnormalities in the putamen, which plays a key role in reward processing and impulse control, may impair an individual’s ability to regulate negative emotions, increasing tendencies toward behavioral dysregulation and emotional sensitivity. The cerebellum, as a critical node in higher-order cognitive and emotional regulation, may exacerbate persistent responses to negative emotions, particularly under stress. Altered functionality in the superior frontal gyrus may contribute to cognitive-emotional dysregulation associated with SI by enhancing negative rumination and pessimistic predictions. Meanwhile, dysfunction in the inferior temporal gyrus may affect the processing and interpretation of emotional stimuli, further intensifying feelings of isolation and social withdrawal.
Currently, the assessment of SI in MDD is primarily based on clinical scales. Although existing clinical tools can assess suicide risk, research on objective neurobiological markers remains relatively limited. Machine learning methods based on brain imaging provide a more objective measurement approach, with the potential to significantly improve the accuracy of SI assessment in MDD patients. ROC analysis was performed to evaluate the effectiveness of SVM classification. In the present study, the SVM model achieved an accuracy of 86.8%, a sensitivity of 82.9%, a specificity of 80.4%, and an AUC of 0.84 in predicting SI in MDD. Therefore, abnormal VMHC values in these brain regions may serve as potential biomarkers for distinguishing MDDSI patients from MDDNSI patients.This study highlights the association between changes in VMHC values in the superior frontal gyrus, inferior temporal gyrus, putamen, and cerebellum and suicidal ideation (SI) in patients with depression, further deepening the understanding of its neural mechanisms. Functional impairments in these brain regions may contribute to the development of SI by affecting emotional regulation, cognitive biases, and impulse control. However, the study has certain limitations.
First, the small sample size and cross-sectional design may affect the stability of the results and weaken the ability to infer causality. Additionally, the duration of suicidal ideation (SI) was not included as a variable in the analysis, which may limit a comprehensive understanding of the neuroimaging characteristics of SI. Second, economic factors were not systematically collected or analyzed, and only right-handed individuals were included in the study. These factors may limit the generalizability of the findings and the ability to account for potential socioeconomic and neurobiological variations. Third, since this study focused primarily on Chinese patients, the findings may have certain limitations when applied to other populations.
Future research should aim to collect multicenter data, include a broader population, and adopt longitudinal designs with extended follow-up periods to validate these findings and explore the potential moderating effects of related variables. Furthermore, it is essential to test whether these findings are applicable to different racial and cultural contexts, enhancing the cross-cultural applicability of the results and promoting the global clinical application of these neuroimaging biomarkers.In the future, integrating multimodal imaging techniques such as T1, DTI, and fMRI could provide a more comprehensive understanding of the neural imaging mechanisms associated with VMHC abnormalities. These VMHC biomarkers hold promise for combination with psychological assessment tools to enable risk stratification, early diagnosis, and personalized interventions for high-risk patients. However, clinical application still faces challenges, including high equipment and analysis costs, technical complexity, lack of standardized diagnostic thresholds, difficulties in data interpretation, and concerns over patient privacy and ethical considerations. Addressing these issues will require technological advancements and interdisciplinary collaboration to promote the broader clinical use of VMHC biomarkers.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cai H, Jin Y, Liu S. et al. Prevalence of suicidal ideation and planning in patients with major depressive disorder: a meta-analysis of observation studies[J]. J Affect Disord. 2021;293:148–158. doi:10.1016/j.jad.2021.05.115
2. Lorenzo-Luaces L. Heterogeneity in the prognosis of major depression: from the common cold to a highly debilitating and recurrent illness[J]. Epidemiol Psychiatr Sci. 2015;24(6):466–472. doi:10.1017/S2045796015000542
3. Fried EI, Nesse RM. Depression sum-scores don’t add up: why analyzing specific depression symptoms is essential[J]. BMC Med. 2015;13(1):72. doi:10.1186/s12916-015-0325-4
4. Meyer RE, Salzman C, Youngstrom EA, et al. Suicidality and risk of suicide--definition, drug safety concerns, and a necessary target for drug development: a consensus statement[J]. J Clin Psychiatry. 2010;71(8):e1–e21. doi:10.4088/JCP.10cs06070blu
5. Werbeloff N, Markou M, Hayes JF, et al. Individual and area-level risk factors for suicidal ideation and attempt in people with severe depression[J]. J Affect Disord. 2016;205:387–392. doi:10.1016/j.jad.2016.08.015
6. Stange JP, Kleiman EM, Sylvia LG, et al. Specific mood symptoms confer risk for subsequent suicidal ideation in bipolar disorder with and without suicide attempt history: multi-wave data from step-bd[J]. Depress Anxiety. 2016;33(6):464–472. doi:10.1002/da.22464
7. Angst J, Angst F, Stassen HH. Suicide risk in patients with major depressive disorder[J]. J Clin Psychiatry. 1999;60(Suppl 2):57–62. discussion 75-6, 113-6.
8. Vuorilehto M, Valtonen HM, Melartin T, et al. Method of assessment determines prevalence of suicidal ideation among patients with depression[J]. Eur Psychiatry. 2014;29(6):338–344. doi:10.1016/j.eurpsy.2013.08.005
9. Keilholz S, Caballero-Gaudes C, Bandettini P, et al. Time-resolved resting-state functional magnetic resonance imaging analysis: current status, challenges, and new directions[J]. Brain Connect. 2017;7(8):465–481. doi:10.1089/brain.2017.0543
10. Jacobs RH, Barba A, Gowins JR, et al. Decoupling of the amygdala to other salience network regions in adolescent-onset recurrent major depressive disorder[J]. Psychol Med. 2016;46(5):1055–1067. doi:10.1017/S0033291715002615
11. Taylor WD, Boyd B, Mcquoid DR, et al. Widespread white matter but focal gray matter alterations in depressed individuals with thoughts of death[J]. Prog Neuropsychopharmacol Biol Psychiatry. 2015;62:22–28. doi:10.1016/j.pnpbp.2015.05.001
12. Sun F, Yan J, Pang J, et al. Distinct effects of first-episode and recurrent major depressive disorder on brain changes related to suicidal ideation: evidence from the REST-meta-MDD Project[J]. J Affect Disord. 2024;351:472–480. doi:10.1016/j.jad.2024.01.213
13. Wagner G, Li M, Sacchet MD, et al. Functional network alterations differently associated with suicidal ideas and acts in depressed patients: an indirect support to the transition model[J]. Transl Psychiatry. 2021;11(1):100. doi:10.1038/s41398-021-01232-x
14. Du L, Zeng J, Liu H, et al. Fronto-limbic disconnection in depressed patients with suicidal ideation: a resting-state functional connectivity study[J]. J Affect Disord. 2017;215:213–217. doi:10.1016/j.jad.2017.02.027
15. Chen VC, Chou YS, Tsai YH, et al. Resting-state functional connectivity and brain network abnormalities in depressive patients with suicidal ideation[J]. Brain Topogr. 2021;34(2):234–244. doi:10.1007/s10548-020-00817-x
16. Li BJ, Friston K, Mody M, et al. A brain network model for depression: from symptom understanding to disease intervention[J]. CNS Neurosci Ther. 2018;24(11):1004–1019. doi:10.1111/cns.12998
17. Hoptman MJ, Zuo XN, D’angelo D, et al. Decreased interhemispheric coordination in schizophrenia: a resting state fMRI study[J]. Schizophr Res. 2012;141(1):1–7. doi:10.1016/j.schres.2012.07.027
18. Anderson JS, Druzgal TJ, Froehlich A, et al. Decreased interhemispheric functional connectivity in autism[J]. Cereb Cortex. 2011;21(5):1134–1146. doi:10.1093/cercor/bhq190
19. Deng K, Yue JH, Xu J, et al. Impaired robust interhemispheric function integration of depressive brain from REST-meta-MDD database in China[J]. Bipolar Disord. 2022;24(4):400–411. doi:10.1111/bdi.13139
20. Chen Q, Bi Y, Yan W, et al. Abnormal voxel-mirrored homotopic connectivity in first-episode major depressive disorder using fMRI: a machine learning approach[J]. Front Psychiatry. 2023;14:1241670. doi:10.3389/fpsyt.2023.1241670
21. Guo W, Liu F, Dai Y, et al. Decreased interhemispheric resting-state functional connectivity in first-episode, drug-naive major depressive disorder[J]. Prog Neuropsychopharmacol Biol Psychiatry. 2013;41:24–29. doi:10.1016/j.pnpbp.2012.11.003
22. Wang Y, Zhong S, Jia Y, et al. Reduced interhemispheric resting-state functional connectivity in unmedicated bipolar II disorder. Acta Psychiatr Scand. 2015;132(5):400–407. doi:10.1111/acps.12429
23. Guo W, Liu F, Zhang J, et al. Dissociation of regional activity in the default mode network in first-episode, drug-naive major depressive disorder at rest. J Affect Disord. 2013;151(3):1097–1101. doi:10.1016/j.jad.2013.09.003
24. Yang J, Palaniyappan L, Xi C, et al. Aberrant integrity of the cortico-limbic-striatal circuit in major depressive disorder with suicidal ideation[J]. J Psychiatr Res. 2022;148:277–285. doi:10.1016/j.jpsychires.2022.02.003
25. Li W, Wang C, Lan X, et al. Resting-state functional connectivity of the amygdala in major depressive disorder with suicidal ideation[J]. J Psychiatr Res. 2022;153:189–196. doi:10.1016/j.jpsychires.2022.07.001
26. He M, Ping L, Chu Z, et al. Identifying changes of brain regional homogeneity and cingulo-opercular network connectivity in first-episode, drug-naïve depressive patients with suicidal ideation[J]. Front Neurosci. 2022;16:856366. doi:10.3389/fnins.2022.856366
27. Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the scale for suicide ideation[J]. J Consult Clin Psychol. 1979;47(2):343–352. doi:10.1037/0022-006X.47.2.343
28. Hamilton M. The assessment of anxiety states by rating[J]. Br J Med Psychol. 1959;32(1):50–55. doi:10.1111/j.2044-8341.1959.tb00467.x
29. Ozcelik HS, Ozdel K, Bulut SD, Orsel S. The reliability and validity of the Turkish version of the Beck Scale for Suicide Ideation (Turkish BSSI). Klinik Psikofarmakoloji Bülteni / Bulletin of Clinical Psychopharmacology. 2015;25(2):141–150. doi:10.5455/bcp.20141214105009
30. Ma S, Yang J, Yang B, et al. The patient health questionnaire-9 vs. the Hamilton rating scale for depression in assessing major depressive disorder. Front Psychiatry. 2021;12:747139. doi:10.3389/fpsyt.2021.747139
31. Yan CG, Wang XD, Zuo XN, et al. DPABI: data Processing & Analysis for (Resting-State) Brain Imaging[J]. Neuroinformatics. 2016;14(3):339–351. doi:10.1007/s12021-016-9299-4
32. Buckner RL, Dinicola LM. The brain’s default network: updated anatomy, physiology and evolving insights[J]. Nat Rev Neurosci. 2019;20(10):593–608. doi:10.1038/s41583-019-0212-7
33. Axelrod V, Rees G, Bar M. The default network and the combination of cognitive processes that mediate self-generated thought[J]. Nat Hum Behav. 2017;1(12):896–910. doi:10.1038/s41562-017-0244-9
34. Li X, Chen X, Yu R, et al. Changes in gray matter volume following electroconvulsive therapy in adolescent depression with suicidal ideation: a longitudinal structural magnetic resonance imaging study[J]. Front Psychiatry. 2022;13:944520. doi:10.3389/fpsyt.2022.944520
35. Jollant F, Lawrence NS, Giampietro V, et al. Orbitofrontal cortex response to angry faces in men with histories of suicide attempts[J]. Am J Psychiatry. 2008;165(6):740–748. doi:10.1176/appi.ajp.2008.07081239
36. Pan LA, Phillips ML. Toward identification of neural markers of suicide risk in adolescents[J]. Neuropsychopharmacology. 2014;39(1):236–237. doi:10.1038/npp.2013.233
37. Kim K, Kim SW, Myung W, et al. Reduced orbitofrontal-thalamic functional connectivity related to suicidal ideation in patients with major depressive disorder[J]. Sci Rep. 2017;7(1):15772. doi:10.1038/s41598-017-15926-0
38. Li X, Chen X, Zhou Y, et al. Altered regional homogeneity and amplitude of low-frequency fluctuations induced by electroconvulsive therapy for adolescents with depression and suicidal ideation[J]. Brain Sci. 2022;12(9):1121. doi:10.3390/brainsci12091121
39. Li J, Duan X, Cui Q, et al. More than just statics: temporal dynamics of intrinsic brain activity predicts the suicidal ideation in depressed patients[J]. Psychol Med. 2019;49(5):852–860. doi:10.1017/S0033291718001502
40. Chen CF, Chen WN, Zhang B. Functional alterations of the suicidal brain: a coordinate-based meta-analysis of functional imaging studies[J]. Brain Imaging Behav. 2022;16(1):291–304. doi:10.1007/s11682-021-00503-x
41. Reis JV, Vieira R, Portugal-Nunes C, et al. Suicidal ideation is associated with reduced functional connectivity and white matter integrity in drug-naïve patients with major depression[J]. Front Psychiatry. 2022;13:838111. doi:10.3389/fpsyt.2022.838111
42. Schmahmann JD. The role of the cerebellum in cognition and emotion: personal reflections since 1982 on the dysmetria of thought hypothesis, and its historical evolution from theory to therapy[J]. Neuropsychol Rev. 2010;20(3):236–260. doi:10.1007/s11065-010-9142-x
43. Stoodley CJ, Schmahmann JD. Evidence for topographic organization in the cerebellum of motor control versus cognitive and affective processing[J]. Cortex. 2010;46(7):831–844. doi:10.1016/j.cortex.2009.11.008
44. Johnson SL, Carver CS, Tharp JA. Suicidality in bipolar disorder: the role of emotion-triggered impulsivity[J]. Suicide Life Threat Behav. 2017;47(2):177–192. doi:10.1111/sltb.12274
45. Jollant F, Perreira F, Fiori LM, et al. Neural and molecular correlates of psychological pain during major depression, and its link with suicidal ideas[J]. Prog Neuropsychopharmacol Biol Psychiatry. 2020;100:109909. doi:10.1016/j.pnpbp.2020.109909
46. Hwang JP, Lee TW, Tsai SJ, et al. Cortical and subcortical abnormalities in late-onset depression with history of suicide attempts investigated with MRI and voxel-based morphometry[J]. J Geriatr Psychiatry Neurol. 2010;23(3):171–184. doi:10.1177/0891988710363713
47. Vicente AF, Bermudez MA, Romero Mdel C, et al. Putamen neurons process both sensory and motor information during a complex task[J]. Brain Res. 2012;1466:70–81. doi:10.1016/j.brainres.2012.05.037
48. Mathur BN, Lovinger DM. Serotonergic Action on Dorsal Striatal Function[J]. Vol. 18 Suppl 1. Parkinsonism Relat Disord; 2012:S129–31.
49. Hörtnagl H, Pifl C, Hörtnagl E, et al. Distinct gradients of various neurotransmitter markers in caudate nucleus and putamen of the human brain[J]. J Neurochem. 2020;152(6):650–662. doi:10.1111/jnc.14897
50. Nye JA, Purselle D, Plisson C, et al. Decreased brainstem and putamen SERT binding potential in depressed suicide attempters using [11C]-zient PET imaging[J]. Depress Anxiety. 2013;30(10):902–907. doi:10.1002/da.22049
51. Harms MB, Casement MD, Teoh JY, et al. Adolescent suicide attempts and ideation are linked to brain function during peer interactions[J]. Psychiatry Res Neuroimaging. 2019;289:1–9. doi:10.1016/j.pscychresns.2019.05.001
52. Marchand WR, Lee JN, Garn C, et al. Striatal and cortical midline activation and connectivity associated with suicidal ideation and depression in bipolar II disorder[J]. J Affect Disord. 2011;133(3):638–645. doi:10.1016/j.jad.2011.04.039
53. Dombrovski AY, Siegle GJ, Szanto K, et al. The temptation of suicide: striatal gray matter, discounting of delayed rewards, and suicide attempts in late-life depression[J]. Psychol Med. 2012;42(6):1203–1215. doi:10.1017/S0033291711002133
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.