")
Back to Journals » Infection and Drug Resistance » Volume 17
Case Report: Pan-Drug Resistant Pseudomonas aeruginosa from a Child with an Infected Burn Wound at the University Teaching Hospital of Kigali, Rwanda
Authors Ndikubwimana I , Gahamanyi N , Bwanakweli T, Uwayo HD, Habimana G, Rogo T
Received 21 August 2024
Accepted for publication 22 October 2024
Published 25 October 2024 Volume 2024:17 Pages 4637—4642
DOI https://doi.org/10.2147/IDR.S486519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Innocent Ndikubwimana,1 Noel Gahamanyi,2,3 Thaddée Bwanakweli,2 Henri Desire Uwayo,2 Gaspard Habimana,4 Tanya Rogo5
1Pediatric Department, College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda; 2National Reference Laboratory, Rwanda Biomedical Centre, Kigali, Rwanda; 3Biology Department, College of Science and Technology, University of Rwanda, Kigali, Rwanda; 4Pediatric Department, Kigali University Teaching Hospital, Kigali, Rwanda; 5Pediatric Infectious Diseases, Brown University Alpert Medical School, Providence, RI, USA
Correspondence: Innocent Ndikubwimana, Email [email protected]
Background: Pseudomonas aeruginosa is a significant cause of morbidity and mortality in intensive care units, and is prevalent in nosocomial infections and cystic fibrosis. The increasing rates of antimicrobial resistance (AMR) complicate the treatment of P. aeruginosa infections, especially because of the multidrug resistance (MDR), extensively drug-resistant (XDR), and pan-drug resistant (PDR) strains.
Case Presentation: We report the case of a 4-year-old male with severe burns covering 45% of his body surface who developed nosocomial PDR P. aeruginosa infection at the University Teaching Hospital of Kigali (CHUK) in Rwanda. A wound culture yielded a PDR P. aeruginosa isolate that was resistant to all the tested antimicrobials, with intermediate resistance to colistin. However, the patient improved with a combination of ceftazidime and amikacin following cessation of fever and successful skin grafting. The patient was discharged on day 95.
Conclusion: P. aeruginosa is a common hospital-acquired pathogen that is particularly challenging to treat, owing to its antimicrobial resistance profile and biofilm production. Antibiotic-resistant strains are a significant public health threat, especially in pediatric burn units. This case underscores the critical need to strengthen infection prevention and control measures together with robust antimicrobial stewardship programs. Molecular characterization of this PDR strain will yield further details regarding its virulence and genotyping.
Keywords: Pseudomonas aeruginosa, burn wound, antimicrobial resistance, CHUK, Rwanda
Introduction
Pseudomonas aeruginosa is among the major etiologies of morbidity and mortality in intensive care units,1 and is known to predominate among nosocomial infections and cystic fibrosis cases.2 Pseudomonas aeruginosa has the ability to survive under minimal nutritional requirements and can tolerate different disinfectant conditions, allowing it to persist on surfaces and facilitate hospital-acquired infections.3 Additionally, P. aeruginosa has been associated with infections of the respiratory tract, skin, soft tissue, urinary tract, surgical sites, and the bloodstream.4
Pseudomonas aeruginosa possesses an arsenal of virulence factors contributing to its adaptation to different environments and enable it to cause diseases.5 These virulence factors empower P. aeruginosa to invade and colonize host cells and lead to clinical symptoms. This is done through interruption of host tissue integration, suppression of and escape from host immune response, and depletion of nutrients from the host.5 Pseudomonas aeruginosa virulence factors are classified into surface structures (type IV pili and flagella, outer membrane components such as lipopolysaccharide, and five secretion systems (T1SS, T2SS, T3SS, T5SS, and T6SS), secreted factors (T1SS and T2SS), and bacterial cell-to-cell interaction (quorum sensing and biofilm).6 The Lipopolysaccharide (LPS) is the first important surface structure which significantly decreases the membrane permeability.7 The out-membrane proteins (OMPs) are involved in nutrient exchange, adhesion, and antibiotic resistance.5 The formation of biofilms which associated with the flagellum, pili, and adhesions contribute to the drug resistance.5
Over the past few decades, there has been a considerable increase in antimicrobial resistance (AMR),5 known as the ability of microorganisms to nullify the effects of antimicrobials and render them ineffective.8,9 This is complicated by the limited number of alternative antimicrobials effective against drug-resistant bacteria.10 The treatment of P. aeruginosa infections is challenging because of their resistance to commonly used antimicrobials.8,11 Multidrug resistance (MDR) is defined as resistance to at least three antibiotic classes, whereas extensive drug resistance (XDR) in P. aeruginosa is defined as non-susceptibility to at least one agent in all but two or fewer antimicrobial categories.12 Pan-drug resistance (PDR) is defined as non-susceptibility to at least six antimicrobial categories (piperacillin-tazobactam, third- and fourth-generation cephalosporins, carbapenems, aminoglycosides, and fluoroquinolones).10 P. aeruginosa has developed resistance to aminoglycosides, quinolones, and beta-lactams through intrinsic, acquired, and adaptive mechanisms.1 Carbapenem-resistant P. aeruginosa (CRPA) is a global public health threat among the three critical priority pathogens designated by the World Health Organization (WHO) as requiring new antimicrobials and control measures.4,10,11
Pseudomonas aeruginosa is an opportunistic pathogen that can cause serious infections in both postoperative and burn wounds.12,13 Infection of burn wounds with P. aeruginosa is challenging because it can lead to septicemia, loss of skin grafts, prolonged hospital stay, increased hospital costs, and mortality.14 Advanced burn wounds infected with P. aeruginosa can also exhibit excessive slough, erythema, green color, and a specific smell.15 Data on P. aeruginosa infections among pediatric patients are scarce.15 This report describes a case of pan-drug-resistant P. aeruginosa isolated from a child’s burn wound at the University Teaching Hospital of Kigali (CHUK) in Rwanda.
Case Presentation
A 4-year- old male patient presented to the CHUK Emergency Department with a thermal burn from hot water on the face, whole trunk, and back, including both the upper and lower arms and buttocks. The burn wound was mixed with superficial and partial thicknesses, and covered approximately 45% of the body surface area. He was admitted to CHUK in December 2023 and received intravenous ceftriaxone and cloxacillin for 10 days starting on the day of admission, according to the doctor’s clinical judgement based on the preceding days spent by the patient at a district hospital. Blood samples were drawn on days 5 and 38 of hospitalization for bacterial culture, which yielded coagulase-negative Staphylococcus (CoNS) and gram-positive bacilli on Gram staining. Meropenem and vancomycin were administered for 21 days but the fever persisted. Ciprofloxacin was then started [received for 6 days], followed by clindamycin [received for 7 days] and piperacillin-tazobactam [received for 7 days]. A wound swab was then taken on day 51 and sent to the Microbiology Laboratory where gram-negative bacilli were found. Ceftazidime was initiated empirically while awaiting identification and antibiograms. Bacterial cultures were performed on MacConkey and blood agar. The presumptive isolate was biochemically identified using the API 20NE galleries (Biomérieux, France). The Kirby-Bauer disk diffusion method was used for the antibiogram, and interpretation was performed according to the Clinical Laboratory Standard Institute (CLSI) guidelines.16,17 From the wound grew Klebsiella spp. and P. aeruginosa. Klebsiella spp. were resistant to ampicillin, cefotaxime, ciprofloxacin, and ceftriaxone. Pseudomonas aeruginosa was found to be resistant to ciprofloxacin and imipenem (Table 1). Another negative blood culture result was obtained on day 54. In addition to the persistent fever, the burn wound appeared greenish in color. A second wound swab was collected on day 53 and sent to the National Reference Laboratory (NRL) as discs for two antibiotics (ceftazidime and amikacin) were not available at CHUK. Bacterial cultures on MacConkey and blood agar were performed at the NRL. The presumptive isolate was identified using the VITEK2. The same platform (VITEK 2) was used for antimicrobial susceptibility testing (AST). The culture grew P. aeruginosa which was resistant to all tested antibiotics, including commonly used anti-Pseudomonas drugs. This isolate showed intermediate resistance to colistin. The antibiogram was then manually repeated using the Kirby-Bauer disk diffusion method to test all the available antibiotics, including ceftazidime and amikacin, which were not tested at CHUK. The isolate was resistant to all the tested drugs (piperacillin-tazobactam, amikacin, amoxicillin-clavulanic acid, azithromycin, cefazolin, cefepime, cefotaxime, ceftazidime, ciprofloxacin, gentamicin, imipenem, levofloxacin, meropenem, ofloxacin, piperacillin, and tobramycin) (Table 1).
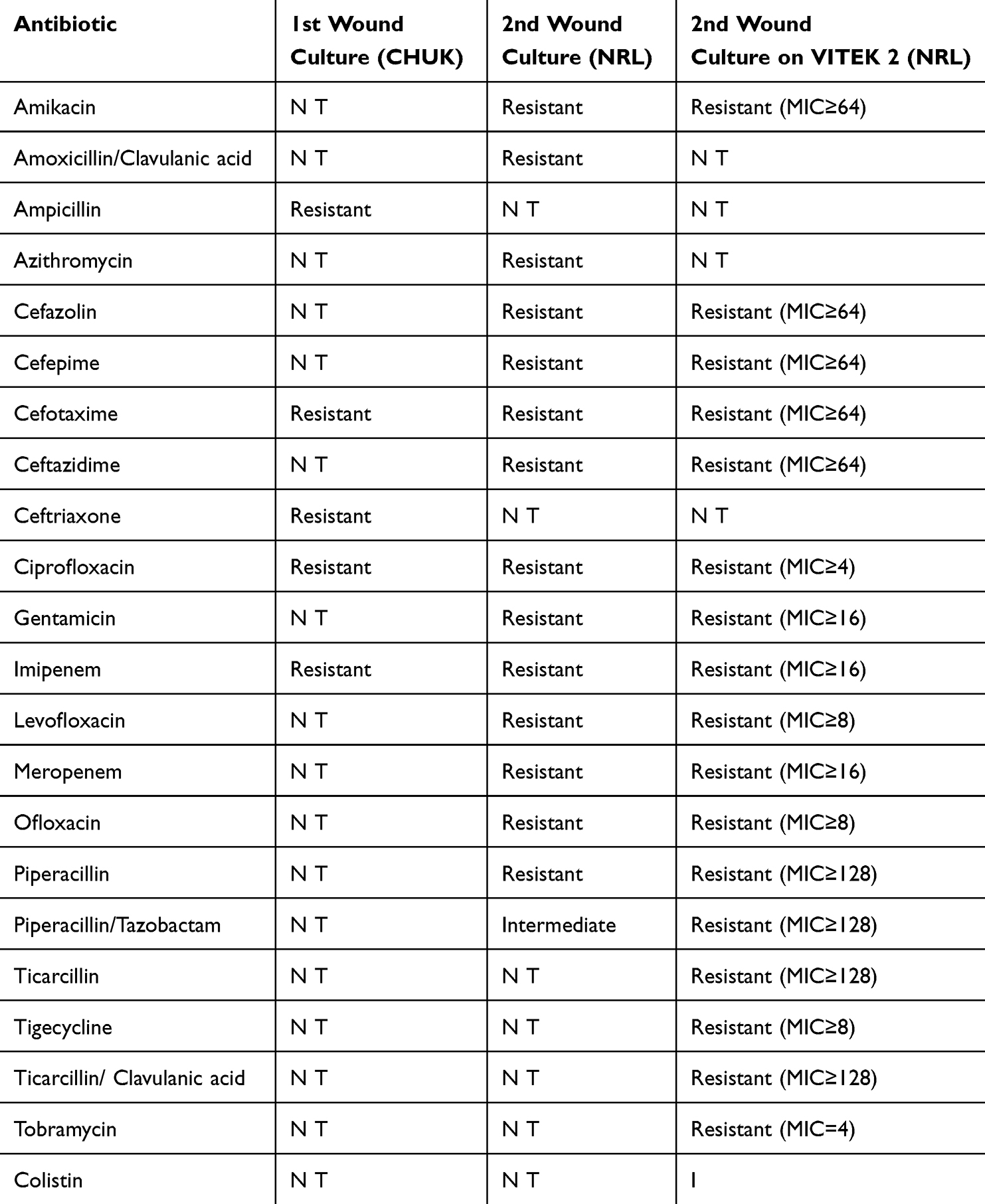 |
Table 1 Antimicrobial Susceptibility Profiles of P. aeruginosa from a Burn Wound in a 4-Year-Old Boy |
Debridement of the torso, right arm, and face was performed on day 69 of hospitalization followed by facial skin grafting. The patient’s condition improved with intravenous ceftazidime and amikacin. This combination was selected based on the literature.14,15,18 The fever resolved and the skin graft was successful. The patient was discharged on day 95.
Discussion and Conclusion
Pseudomonas aeruginosa is a common cause of hospital-acquired infections, and its treatment is complicated by MDR profiles12,16 and biofilm production.19 Worldwide, MDR and CRPA strains are known to pose public health threats, especially among children hospitalized in intensive care units.20 Patients in critical conditions, such as burns and immunocompetent status, have high rates of P. aeruginosa colonization.2,15
The routine use of antibiotics for prophylaxis among patients with burns has no effect on the risk of infection complications and does not reduce the duration of the therapy.21,22 However, perioperative prophylaxis should be reserved for skin grafting and in patients with progressive symptoms of burn complications and/or concomitant infections.23 The patient was empirically treated with antibiotics on admission, considering that he was referred from a district hospital where he had previously been hospitalized, which could have led to the development of an AMR pathogen.
The isolate (P. aeruginosa) from this case report can be classified as pan-drug-resistant because it was found to be resistant to all tested antibiotics (intermediate only to piperacillin-tazobactam). A previous case of P. aeruginosa PDR has been reported in Taiwan.24 This isolate exhibited intermediate resistance to colistin. A colistin-only sensitive case of P. aeruginosa has been previously reported in Spain.25 PDR cases are of concern due to their increased incidence, limited treatment options, and increased mortality rates.26 The World Health Organization (WHO) classified CRPA among the three critical priority pathogens requiring new antimicrobials and control measures.4,10,11 β-lactamase inhibitors, such as ceftolozane-tazobactam, ceftazidime-avibactam,27 polymyxins, fosfomycin, and doripenem, have shown efficacy against P. aeruginosa.26 However, only polymyxins are available in Rwanda, limiting the number of alternative drugs available for such cases. PDR P. aeruginosa has been reported to be sensitive to colistin, but the latter is known to be toxic, and its use should be reserved for severe cases.19,28
Despite the in vitro resistance shown by P. aeruginosa, the patient improved after combination therapy with ceftazidime and amikacin. It is important to note that obtaining a PDR isolate from clinical samples does not always yield unfavorable outcomes. Previous studies have reported that the combination of ceftazidime and amikacin is effective in treating MDR P. aeruginosa.1,14 Occasionally, even severe infections can be self-limiting when no antimicrobial agents are used.29 Additionally, the synergistic effects of both drugs may have contributed to patient improvement. Lastly, the in vivo response is sometimes different from the in vitro response owing to the complexity of the immune system.
The development of new antibiotics can take up to 15 years and is expensive. Other treatment options, including vaccines, antibodies, bacteriocins, anti-quorum sensing, and bacteriophages, should be considered to reduce the morbidity and mortality associated with PDR P. aeruginosa.30 Different studies have used cocktails of bacteriophages to treat XDR and PDR P. aeruginosa.31
The isolate described in this case report is a nosocomial infection that developed after the patient was admitted to the hospital.32 Nosocomial infections are associated with prolonged hospitalization, disability, and economic burdens.33 It is necessary to strengthen infection prevention and control (IPC) committees in resource-limited healthcare settings. This can be achieved by increasing the number of IPC staff, improving surveillance systems, and sharing infection rates among practicing surgeons.34 Clinicians should be judicious in their empirical use of antibiotics to avoid or reduce AMR development. Additional research is needed on the treatment of PDR infections in pediatric patients. The Global Action Plan on Antimicrobial Resistance (GAP-AMR) recommends IPC by improving water, sanitation, and hygiene (WASH) as one of its five objectives.35 Antimicrobial stewardship (AMS) programs should be strengthened to ensure the optimal use of antimicrobials and monitor AMR pathogens in clinical settings. We recommend whole-genome sequencing of this strain to confirm its genotype, antimicrobial resistance, and virulence genes.
Abbreviations
AMR, Antimicrobial Resistance; AMS, Antimicrobial Stewardship; CHUK, Centre Hospitalier Universitaire de Kigali; CLSI, Clinical laboratory standards Institute; CRPA, Carbapenem-resistant P. aeruginosa; GAP-AMR, Global Action Plan on antimicrobial resistance; IPC, Infection Prevention and Control; LPS, Lipopolysaccharides; MDR, Multidrug Resistance; MICs, Minimal Inhibitory Concentrations; NRL, National Reference Laboratory; NT, Not tested; OMPs, Out-membrane proteins; PDR, Pan-drug Resistance.
Data Sharing Statement
Data and materials are fully available in the manuscript text and in the table.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the University Teaching Hospital of Kigali. The University Teaching Hospital of Kigali as institution approved to publish the case details. Ref. EC/CHUK/CR/001/2024). Informed consent was obtained from patients’ caregivers.
Consent for Publication
Informed consent was obtained from the patient’s caregiver for the publication of this case report.
Acknowledgments
We thank the patients for their informed consent to publish this case report. We also recognized the contribution of the laboratory staff to microbiology-related studies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This case report was not funded.
Disclosure
The authors declare that they have no competing interests, nor do they have an associated interest that represents a conflict of interest for this submitted work.
References
1. Pang Z, Raudonis R, Glick BR, Lin TJ, Cheng Z. Antibiotic resistance in Pseudomonas aeruginosa: mechanisms and alternative therapeutic strategies. Biotechnol Adv. 2019;37:177–192. doi:10.1016/j.biotechadv.2018.11.013
2. Jurado-Martín I, Sainz-Mejías M, McClean S. Pseudomonas aeruginosa: an audacious pathogen with an adaptable arsenal of virulence factors. Int J Mol Sci. 2021;22:3128. doi:10.3390/ijms22063128
3. Awanye AM, Ibezim CN, Stanley CN, Onah H, Okonko IO, Egbe NE. Multidrug-Resistant and Extremely Drug-Resistant Pseudomonas aeruginosa in Clinical Samples From a Tertiary Healthcare Facility in Nigeria. Turk J Pharm Sci. 2022;19(4):447–454. doi:10.4274/tjps.galenos.2021.66066
4. Pungcharoenkijkul S, Traipattanakul J, Thunyaharn S, Santimaleeworagun W. Antimicrobials as single and combination therapy for colistin-resistant pseudomonas aeruginosa at a university hospital in Thailand. Antibiotics. 2020;9(8):1–11. doi:10.3390/antibiotics9080475
5. Liao C, Huang X, Wang Q, Yao D, Lu W. Virulence Factors of Pseudomonas Aeruginosa and Antivirulence Strategies to Combat Its Drug Resistance. Front Cell Infect Microbiol. 2022;12:926758. doi:10.3389/fcimb.2022.926758
6. Strateva T, Mitov I. Contribution of an arsenal of virulence factors to pathogenesis of Pseudomonas aeruginosa infections. Annals of Microbiology. 2011;61(4):717–732. doi:10.1007/s13213-011-0273-y
7. Huszczynski SM, Lam JS, Khursigara CM. The Role of Pseudomonas aeruginosa Lipopolysaccharide in Bacterial Pathogenesis and Physiology. Pathogens. 2019;9(1):6. doi:10.3390/pathogens9010006
8. Al-Orphaly M, et al. Epidemiology of Multidrug-Resistant Pseudomonas aeruginosa in the Middle East and North Africa Region. mSphere. 2021;6(3):10–128. doi:10.1128/msphere.00202-21
9. Gahamanyi N, Umuhoza T, Saeed SI, Mayigane LN, Hakizimana JN. A Review of the Important Weapons against Antimicrobial Resistance in Sub-Saharan Africa. Appl Biosci. 2023;2(2):136–156. doi:10.3390/applbiosci2020011
10. Magiorakos AP, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
11. Lister PD, Wolter DJ, Hanson ND. Antibacterial-resistant Pseudomonas aeruginosa: clinical impact and complex regulation of chromosomally encoded resistance mechanisms. Clin Microbiol Rev. 2009;22:582–610. doi:10.1128/CMR.00040-09
12. Michael Buhl SP, Willmann M. Prevalence and risk factors associated with colonization and infection of extensively drug-resistant Pseudomonas aeruginosa: a systematic review. Expert Rev Anti Infect Ther. 2015;13(9):1159–1170. doi:10.1586/14787210.2015.1064310
13. Tacconelli E, et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis. 2018;18(3):318–327. doi:10.1016/S1473-3099(17)30753-3
14. Bezares BR, Sáenz Y, Torres C, Chairat S, Yahia HB, Ben Slama K. High prevalence of imipenem-resistant and metallo-beta-lactamase-producing Pseudomonas aeruginosa in the Burns Hospital in Tunisia: detection of a novel class 1 integron. J Chemother. 2019;31(3):120–126. doi:10.1080/1120009X.2019.1582168
15. Coetzee E, Rode H, Kahn D. Pseudomonas aeruginosa burn wound infection in a dedicated paediatric burns unit. South Afr J Surg. 2013;51(2):50–53. doi:10.7196/SAJS.1134
16. Estahbanati HK, Kashani PP, Ghanaatpisheh F. Frequency of Pseudomonas aeruginosa serotypes in burn wound infections and their resistance to antibiotics. Burns. 2002;28(4):340–348. doi:10.1016/S0305-4179(02)00024-4
17. Ladhani HA, Yowler CJ, Claridge JA. Burn Wound Colonization, Infection, and Sepsis. Surg Infect. 2021;22(1):44–48. doi:10.1089/sur.2020.346
18. WHO. News release, WHO publishes list of bacteria for which new antibiotics are urgently needed. Available from: https://www.who.int/news/item/27-02-2017-who-publishes-list-of-bacteria-for-which-new-antibiotics-are-urgently-needed.
19. Chegini Z, Khoshbayan A, Taati Moghadam M, Farahani I, Jazireian P, Shariati A. Bacteriophage therapy against Pseudomonas aeruginosa biofilms: a review. Annals of Clinical Microbiology and Antimicrobials. 2020;19(1). doi:10.1186/s12941-020-00389-5
20. Logan LK, et al. Multidrug- and carbapenem-resistant Pseudomonas aeruginosa in Children, United States, 1999–2012. J Pediatric Infect Dis Soc. 2017;6(4):352–359. doi:10.1093/jpids/piw064
21. Rai S, Dash D, Agarwal N. Introducing the new face of CLSI M100 in 2023: an explanatory review. Indian Journal of Medical Microbiology. 2023;46:100432. doi:10.1016/j.ijmmb.2023.100432
22. Weinstein MP, Lewis JS. The clinical and laboratory standards institute subcommittee on Antimicrobial susceptibility testing: background, organization, functions, and processes. J Clin Microbiol. 2020;58(3). doi:10.1128/JCM.01864-19
23. Noskiewicz J, Juszczak P, Rzanny-Owczarzak M, Mańkowski P. Antibiotic therapy and infection complications in paediatric burn injuries. Postepy Hig Med Dosw. 2019;73:332–337. doi:10.5604/01.3001.0013.2019
24. Wang CY, et al. Pandrug-resistant Pseudomonas aeruginosa among hospitalised patients: clinical features, risk-factors and outcomes. Clin Microbiol Infect. 2006;12(1):63–68. doi:10.1111/j.1469-0691.2005.01305.x
25. Viedma E, et al. Nosocomial spread of colistin-only-sensitive sequence type 235 Pseudomonas aeruginosa isolates producing the extended-spectrum β-lactamases GES-1 and GES-5 in Spain. Antimicrob Agents Chemother. 2009;53(11):4930–4933. doi:10.1128/AAC.00900-09
26. Mendes Pedro D, et al. Extensively drug-resistant Pseudomonas aeruginosa: clinical features and treatment with ceftazidime/avibactam and ceftolozane/tazobactam in a tertiary care university hospital center in Portugal – a cross-sectional and retrospective observational study. Front Microbiol. 2024;15:1347521. doi:10.3389/fmicb.2024.1347521
27. Ozma MA, et al. Antibiotic therapy for pan-drug-resistant infections. EDIMES Edizioni Medico Scientifiche. 2022;30:525. doi:10.53854/liim-3004-6
28. Csenkey A, et al. Systemic antibiotic prophylaxis does not affect infectious complications in pediatric burn injury: a meta-analysis. PLoS One. 2019;14(9):e0223063. doi:10.1371/journal.pone.0223063
29. Falagas ME, Bliziotis IA, Kasiakou SK, Samonis G, Athanassopoulou P, Michalopoulos A. Outcome of infections due to pandrug-resistant (PDR) Gram-negative bacteria. BMC Infect Dis. 2005;5(1). doi:10.1186/1471-2334-5-24
30. Horcajada JP, et al. Epidemiology and treatment of multidrug-resistant and extensively drug-resistant Pseudomonas aeruginosa infections. Clin Microbiol Rev. 2019;32(4):1. doi:10.1128/CMR.00031-19
31. Souli M, Galani I, Giamarellou H. Emergence of extensively drug-resistant and pandrug-resistant Gram-negative bacilli in Europe. Eurosurveillance. 2008;13(47). doi:10.2807/ese.13.47.19045-en
32. Hensley BJ, Monson JRT. Hospital-acquired infections. Surgery. 2015;33(11):528–533. doi:10.1016/j.mpsur.2015.08.008
33. Khan HA, Baig FK, Mehboob R. Nosocomial infections: epidemiology, prevention, control and surveillance. Asian Pac J Trop Biomed. 2017;7(5):478–482. doi:10.1016/j.apjtb.2017.01.019
34. Taplitz RA, Ritter ML, Torriani FJ. 6 - Infection Prevention and Control, and Antimicrobial Stewardship. In: Cohen J, Powderly WG, Opal SM, editors. Infectious Diseases.
35. Sano D, et al. Updated research agenda for water, sanitation and antimicrobial resistance. J Water Health. 2020;18(6):858–866. doi:10.2166/wh.2020.033
36. Reynolds D, Kollef M. The Epidemiology and Pathogenesis and Treatment of Pseudomonas aeruginosa Infections: an Update. Drugs. 2021;81:2117–2131. doi:10.1007/s40265-021-01635-6
37. Garzone P, Lyon J, Yu VL. Third-Generation and Investigational Cephalosporins: i. Structure-Activity Relationships and Pharmacokinetic Review. Drug Intell Clin Pharm. 1983;17(7–8):507–515. doi:10.1177/106002808301700703
38. Wood SJ, Kuzel TM, Shafikhani SH. Pseudomonas aeruginosa: infections, Animal Modeling, and Therapeutics. Cells. 2023;12:199. doi:10.3390/cells12010199
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.