")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Causal Relationship and Potential Common Pathogenic Mechanisms Between Alopecia Areata and Related Cancer
Received 18 September 2024
Accepted for publication 11 December 2024
Published 17 December 2024 Volume 2024:17 Pages 2911—2921
DOI https://doi.org/10.2147/CCID.S496720
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Zexin Zhu,1 Xiaoxue Wang2
1Department of Surgical Oncology, the Comprehensive Breast Care Center, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China; 2Department of Dermatology, The Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China
Correspondence: Xiaoxue Wang, Department of Dermatology, the Second Affiliated Hospital of Xi’an Jiaotong University, Xi’an, People’s Republic of China, Email [email protected]
Objective: Alopecia areata (AA) is an autoimmune skin disease. Observational studies have reported an association between AA and cancer. However, the causal relationship between AA and cancer has not been reported. We employed a two-sample Mendelian randomization (MR) study to assess the causality between AA and 17 subtypes of cancers.
Methods: We employed a two-sample Mendelian randomization (MR) study to assess the causality between AA and 17 subtypes of cancers. AA and cancers’ association genome-wide association study (GWAS) data were collected. The inverse variance weighted (IVW) method was utilized as the principal method in our Mendelian randomization (MR) study, with additional use of the MR-Egger, weighted median, simple mode, and weighted mode methods. After that, we explored the underlying biological mechanisms by Bioinformatic Analysis.
Results: According to our MR analysis, AA has a causal relationship with hepatic bile duct cancer (HBDC, (odds ratio [OR] = 0.944, 95% confidence interval [CI] = 0.896– 0.994, P-value = 0.030) and colorectal cancer (CRC, OR = 0.981, 95% CI = 0.963– 0.999, P-value = 0.046). AA could decrease the risk of HBDC and CRC. No causal link between AA and other subtypes of cancers was observed. No heterogeneity or pleiotropy was observed. Furthermore, disease-related genes were obtained, Gene Ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analysis results showed that the set of genes associated with immunity-inflammatory signaling pathway.
Conclusion: This study provided new evidence of the relationship between AA with HBDC and CRC. AA may play a protective role in both HBDC and CRC progression. This could provide newer avenues for research in search of treatment for HBDC and CRC.
Keywords: alopecia areata, cancer, causal relationship, colorectal cancer, hepatic bile duct cancer, Mendelian randomization
Introduction
Alopecia areata (AA) is an autoimmune skin disorder where patients suffering from AA were characterized by hair loss in focal regions, such as the complete scalp, including eyelashes and eyebrows, or even any hair-bearing surface.1–3 The clinical presentation of AA can range from small patches of hair loss to widespread involvement of the scalp or the entire body.1,3 Statistically, AA has affected nearly 2% of the general population, regardless of ethnic groups, genders, and age-based groups.1,4 While the exact pathogenesis of AA remains unclear, it is believed that the collapse of the immune privilege of the hair follicle caused by immunological mechanism plays a fundamental role in AA progression.2 Genetic factors and environment factors (including immunology, oxidative stress, microbiome, and allergy) contribute to the pathogenesis of AA.2,5,6 Traditional treatment options for AA mainly refer to the usage of corticosteroids (intralesional, topical or systemic), immunosuppressants such as methotrexate are supplementary treatments for recalcitrant and extensive AA.7 Besides, Janus kinase (JAK) inhibitors, Tumor necrosis factor-α (TNF-α) inhibitors (such as adalimumab and etanercept) were considered as new treatment strategies for AA.8–10 It is important to note that while treatments for AA are of limited efficacy or are associated with potential side effects, many patients experience unpredictable cycles of hair loss and regrowth, with some cases being persistent and extensive.1,2
Studies also reported that AA is associated with various other disorders. For instance, AA greatly impacts the quality of life for patients, lead to the development of psychological disorders such as anxiety and depression.11 Atopic diathesis including asthma, atopic dermatitis, allergic rhinitis and allergic conjunctivitis were more prevalent in patients with AA compared with matched control subjects.12 A systematic review indicated that patients with AA were more likely to suffer from thyroid diseases, psychiatric diseases, vitamin D deficiency, ophthalmic abnormalities.13
Mendelian randomization (MR) utilizes one or more genetic variants as instrumental variables (IVs) based on genome-wide association studies (GWAS). MR studies can infer the causal effects of exposure on an outcome. Recently, MR analysis also reported the causal relationship between AA and other diseases. For instance, MR analysis showed that AA was associated with an increased risk of myocardial infarction (MI).14 Similarly, AA could causally increase the risk of major depression disorder (MDD) and anxiety.15 However, to our knowledge, no study has yet investigated the causal effect of AA on the risk of cancer using Mendelian randomization. Our investigation aimed to explore the AA variants as instrumental variables for cancer risk utilizing two-sample MR, screen the gene sets and characteristic crosstalk genes of AA and related cancer.
Materials and Methods
Study Design
According to the MR framework (Figure 1), three key assumptions are included: (1) Relevance Assumption: Single nucleotide polymorphisms (SNPs) that are substantially linked to exposures (AA) are used as Instrumental variables (IVs). (2) Independence Assumption: These SNPs (IVs) should not show any correlation with the relevant confounding factor. (3) Exclusivity Assumption: These SNPs (IVs) should affect outcomes (different subtypes of cancers) only through its effect on exposure.16–19
 |
Figure 1 Flowchart schematic diagram followed by the MR analysis’ principal of this study. |
Data Sources
We utilized summary data associated with AA and 17 subtypes of cancers from MRC Integrative Epidemiology Unit Open GWAS database (https://gwas.mrcieu.ac.uk). Accession numbers finn-b-L12_ALOPECAREATA for AA, 289 cases and 211,139 controls, information of different subtypes of cancers were detailed in Table 1, summary data were accessed from IEU Open GWAS project database (https://gwas.mrcieu.ac.uk). Our study was conducted by secondary analysis of data from other studies, all participants or their family members have provided informed written consent in the original studies.
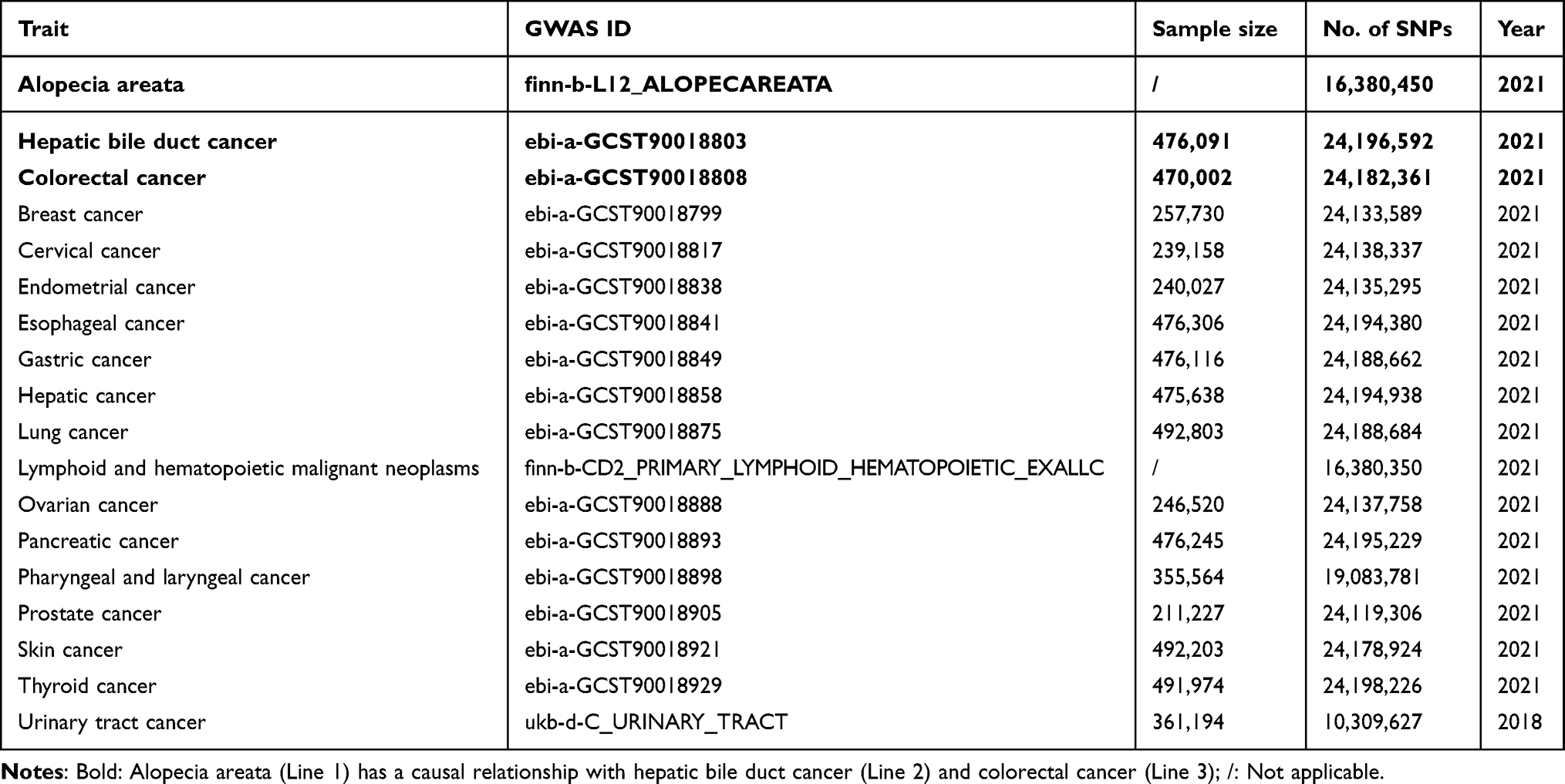 |
Table 1 Information of GWAS Summary Data Source Included in the Study |
Instrumental Variables (IVs) Selection
Related IVs for MR analysis followed particular principles: SNPs should be associated with exposures at the locus-wide significance level: P-value <5e-06. In addition, linkage disequilibrium (LD) coefficient r2 should be less than 0.001, not closely related (clumping window more than 10,000 kb) to ensure exposure instrument independence. We used the F statistic to measure the strength of the IVs, the values of F-statistics were more than 10.16–19
MR Analysis
Causal associations between AA and cancers were determined utilizing MR analysis. In the exposure-outcome analysis, we employed MR with more than two SNPs serving as IVs. Our MR analysis using each of the five methods: inverse variance-weighted (IVW) was performed as the primary statistical analysis method in our MR analysis for evaluating causal effects, besides, weighted median, and MR-Egger, simple mode, weighted mode were utilized.16–19
The heterogeneity of the chosen SNPs was evaluated using Cochrane’s Q test, a P-value of more than 0.05 suggested the lack of heterogeneity. The random effects model was used once significant heterogeneity has been identified. We evaluated the possible bias from horizontal pleiotropy using the weighted median and MR-Egger regression in order to gauge the robustness of the IVW method. The MR-PRESSO (MR-Pleiotropy RESidual Sum and Outlier) test was used to appraise outliers that might have been influenced by horizontal pleiotropy. The causal-effect estimates for individual variants were displayed using Scatter plot. Thereafter, we performed a “leave-one-out” analysis to examine the stability of the results in the context of a single SNP’s influence and presented the findings in a forest plot.16–19
All statistical analysis were conducted in R software (Version 4.3.2) using the TwoSampleMR package (Version 0.5.8). The statistical significance level is P-value <0.05. Pooled ORs (odds ratio) with 95% confidence interval (CI) were calculated.
Acquisition the Related Genes
Disease-related genes were obtained from The GeneCards database (https://www.genecards.org/), using the key word “alopecia areata” and causal related cancers. Intersection of the disease genes were used to obtain the crosstalk genes.
Enrichment Analysis of Crosstalk Genes
The R software packages “org.Hs.eg.db” and “clusterProfiler” were used to enrich the obtained crosstalk genes of AA and related cancers in the Gene Ontology (GO) categories of molecular function (MF), biological process (BP), and cellular component (CC). Thereafter, Kyoto Encyclopedia of Genes and Genomes (KEGG) enrichment analysis were performed on the obtained crosstalk genes in AA and related cancers. Adjust P-value <0.05 was used as a filtering condition.
Results
Instrumental Variables
According to the quality control principle as mentioned, 12 SNPs related with AA were adopted as Instrumental variables (IVs). The SNPs included in the exposure data are detailed in Supplementary Table S1.
MR Analysis
We conducted the two-sample MR analysis between AA and 17 subtypes of cancers. The IVW MR analysis demonstrated that AA has a causal relationship with hepatic bile duct cancer (HBDC, OR = 0.944, 95% CI = 0.896–0.994, P-value = 0.030, Table 2) and colorectal cancer (CRC, OR = 0.981, 95% CI = 0.963–0.999, P-value = 0.046, Table 3), respectively. Interestingly, AA play protective roles in both HBDC and CRC. No causal association between AA and other cancers was observed (Figure 2). Using the MR-Egger, the relationship between AA and HBDC, CRC was visualized, respectively (Figure 3a and b).
 |
Table 2 Causal Relationship Between AA and HBDC |
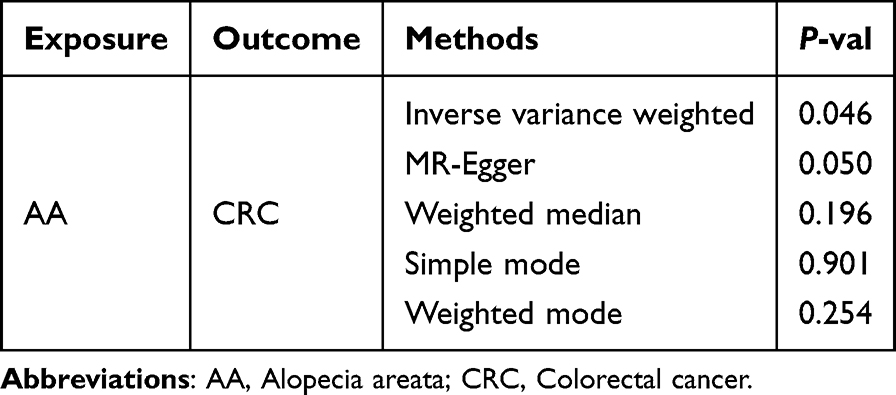 |
Table 3 Causal Relationship Between AA and CRC |
 |
Figure 2 Forest plot of Mendelian randomization analysis for Alopecia areata on 17 subtypes of cancers risk. OR, odds ratio; CI, confidence interval; * P-value <0.05. |
 |
Figure 3 Scatter plots showing significant causal effects. (a) Alopecia areata on Hepatic bile duct cancer; (b) Alopecia areata on Colorectal cancer. |
Sensitivity Analysis
According to the analysis of Cochran’s Q test, our IVW-MR analysis results demonstrated no evidence of heterogeneity among the reported results. Furthermore, the MR-Egger regression analysis results provided evidence that there exists no significant horizontal pleiotropy in our MR analysis, and MR-PRESSO analysis indicated that no outliers were identified (Table 4). The symmetric funnel plot (Figure 4) indicated no evidence of horizontal pleiotropy. We also conducted leave-one-out method to identify and delete abnormal instrumental variables (Figure 5). The results showed the robustness of our results. These results suggest that the MR analysis results were relatively stable.
 |
Table 4 Sensitivity Analysis of Our MR |
 |
Figure 4 Funnel plot of our Mendelian randomization study. (a) Alopecia areata on Hepatic bile duct cancer; (b) Alopecia areata on Colorectal cancer. |
 |
Figure 5 Results of “Leave-one-out” sensitivity analysis in our Mendelian randomization study. (a) Alopecia areata on Hepatic bile duct cancer; (b) Alopecia areata on Colorectal cancer. |
Reversed MR
We also conducted the reversed MR. We identified 11 SNPs from HBDC, 76 SNPs from CRC (detailed in supplementary Tables S2 and S3). No significant results were detected when AA was conducted as the outcome (Tables 5 and 6). These results indicated that HBDC or CRC has no causal impact on AA.
 |
Table 5 Reverse Causality Between HBDC and AA |
 |
Table 6 Reverse Causality Between CRC and AA |
Crosstalk Genes and Enrichment Analysis
A total of 613 AA disease genes, 4892 hBDC disease genes, 12,806 CRC disease genes were obtained from the GeneCard, respectively. As shown in Figure 6a, considering the intersection of these diseases, 287 intersecting genes were obtained (Table S4 for details).
 |
Figure 6 Disease genes and enrichment analysis. (a) intersecting genes between AA and causal related cancers; (b) biological process (BP); (c) cellular component (CC); (d) molecular function (MF); (e) Kyoto Encyclopedia of Genes and Genomes (KEGG) Enrichment analysis. AA= Alopecia areata. HBDC= Hepatic bile duct cancer. CRC= Colorectal cancer. |
GO enrichment results showed that the set of genes associated with inflammatory response, immune response, positive regulation of interleukin-6, interleukin-8, interleukin-10, interleukin-12 production, positive regulation of T cell proliferation, positive regulation of inflammatory response, the set of genes related to immune inflammation were significantly enriched among the crosstalk genes of AA, HBDC and CRC, as shown in Figure 6b-d. The KEGG enrichment results showed that Cytokine–cytokine receptor interaction, Th17 cell differentiation, Toll-like receptor signaling pathway, Janus kinase (JAK) signal transducer and activator of transcription (JAK-STAT) pathway signaling pathway, Intestinal immune network for IgA production, Tumor necrosis factor (TNF) signaling pathway were significantly enriched among the crosstalk genes of AA and causal related cancers, as shown in Figure 6e, Table S5 for details.
Discussion
We conducted a bidirectional MR analysis to investigate the causal relationship between AA and 17 subtypes of cancers. Our results showed that AA has a causal effect on HBDC and CRC, in contrast, HBDC or CRC has no causal impact on AA. Furthermore, these results provided evidence for a protective effect of AA on HBDC and CRC risk. To the best of our knowledge, this MR analysis is the first to investigate the causal relationship between AA and cancers.
HBDC (intrahepatic Cholangiocarcinoma, iCCA) accounts for 2% of all malignancies.20 Anatomically, HBDC arises from the epithelium of the bile ducts (BD) and can involve any part of the biliary tract.20,21 HBDC is the second most common cause of primary liver cancer, after hepatocellular carcinoma (HCC).22 Surgical resection is still the possible curative therapy for HBDC, while the anatomical location influences the surgical techniques employed.22 Radiotherapy in selected cases, and systemic chemotherapy also play a significant role in both curative and palliative cohort.22,23 Generally, the prognosis of HBDC is poor, accordingly, one-year survival for HBDC was 25% and 5-year survival was 5% in Europe.23
Colorectal cancer (CRC) accounts for about 10% of all diagnosed cancers and cancer-related deaths worldwide each year.24,25 It is the second most common cancer in women and the third most common in men. Women have a lower incidence and mortality rate compared to men, with rates approximately 25% lower.25 The incidence of CRC worldwide is predicted to increase to 2.5 million new cases in 2035.25,26 Risk factors such as obesity, lack of physical exercise, and smoking contribute to the increased risk of developing CRC. Treatments for CRC include endoscopic resection (for some early cancers) and surgical local excision, radiotherapy and systemic therapy, such as chemotherapy, targeted therapy, and immunotherapy.25,27
MR analysis has reported several factors associated with HBDC or CRC. Ulcerative colitis (UC) patients could increase the incidences of HBDC,28 in addition, specific gut microbiota and metabolites have causal relationship with HBDC.29 Living habits were also demonstrated to have causal impact on liver cancer: sleep duration has a negative correlation with HBDC, in contrast, there was a positive correlation found between insomnia and nap during the day with HBDC.30 Likewise, MR analysis also indicated alcohol consumption, higher body mass index (BMI), low 25-hydroxyvitamin D could increase the risk of CRC.31–33
Observational studies have reported the relationship between AA and cancers.34,35 Accordingly, AA decreased the risk of nonmelanoma skin cancer and melanoma.34 Additionally, liver cancer, uterine, and cervix cancer were also significantly lower in patients with AA. In contrast, AA patients were more likely to suffer from lymphoma, breast cancer, kidney, and urinary bladder cancer.35 However, our MR study did not find the causal relationship between AA and skin cancer, breast cancer, cervix cancer, lymphoma or urinary bladder cancer. Interestingly, a recent systematic review and meta-analysis conducted by Sophia Ly et al investigated the comorbid conditions associated with AA. The findings indicated that AA may serve as a protective factor against specific types of cancer, as individuals with AA demonstrated reduced odds of developing colorectal cancer (odds ratio [OR] 0.61, 95% confidence interval [CI] 0.42–0.89) and hepatocellular carcinoma (OR 0.37, 95% CI 0.25–0.56) in comparison to healthy control subjects. These outcomes provide additional corroboration for our findings.36
To our known, no studies reported the relationship between AA and HBDC or CRC, our MR analysis uncovered new evidence suggesting the potential link between AA and these two cancers. Immune-related factors may be potential explanations for the protective role of AA in cancer progression. As mentioned, the pathophysiology of AA is not fully understood, while breaking down of the immune privilege of the hair follicles followed by autoimmune attack was believed to be the leading cause of AA.35,37 On the other hand, upregulation of NKG2D ligands (NKG2DLs) compared with the infiltration of cytotoxic subset of CD8+NKG2D+ T cells in AA patient is the major pathogenesis of AA.35,38 NKG2D and its ligand are known for their protective role in tumor immune surveillance, combined with the immune defense against tumors effect achieved by NK cells.39 In our Enrichment Analysis, we also find immune-related inflammation was significantly enriched among the crosstalk genes of AA, HBDC and CRC. It should also be noted that, we also find that Th17 cell differentiation, Toll-like receptor signaling pathway, JAK-STAT signaling pathway, Intestinal immune network for IgA production, TNF signaling pathway were significantly enriched among the crosstalk genes, these pathways were related to immunity-inflammation procedure, regulating autoimmunity and cancer.40–42 Meanwhile, the mechanism of how AA decreased the risk of HBDC and CRC remains uncertain.
There are several limitations to our study. First, due to the original GWAS statistics, we were unable to divide the cohorts or perform subgroup analyses. Second, our analysis only included individuals of the European population. Although using a single European population to investigate causal relationships can minimize population stratification bias, it is important to interpret these findings with caution regarding their applicability to other populations. Further research is required on the mechanism of how AA decreased HBDC and CRC risk.
Conclusion
In conclusion, our MR study has provided the first-ever evidence that AA has a causal impact on HBDC and CRC, AA decreased the risk of both HBDC and CRC. Besides, our results do not support a causal association between AA and other subtypes of cancers. Further studies focusing on AA may provide newer avenues for research in search of treatment targeted therapy in the treatment of HBDC and CRC.
Abbreviations
AA, Alopecia Areata; HBDC, Hepatic bile duct cancer; CRC, Colorectal cancer; MR, Mendelian randomization; IVW, Inverse-variance weighted; SNP, Single nucleotide polymorphism; IVs, Instrumental variables; GWAS, Genome-wide association study; LD, Linkage disequilibrium; WM, Weighted median; OR, Odds ratio; CI, Confidence interval; JAK-STAT, Janus kinase (JAK) signal transducer and activator of transcription; UC, Ulcerative colitis; BMI, body mass index.
Data Sharing Statement
No original data were generated in the present study. The datasets mentioned in this article are publicly available. Details see Supplementary Tables.
Ethics Statement
This study is exempt from ethical review as per Article 32 of the Measures for Ethical Review of Life Science and Medical Research Involving Human Beings (National Science and Technology Ethics Committee, China). The exemption is based on the use of non-harmful, non-sensitive data from open, legal databases.
Acknowledgments
We acknowledge GWAS database for providing their platforms and contributors for uploading their meaningful datasets.
Funding
This work has been funded by the Natural Science Foundation of Shaanxi Province (S2023-JC-QN-0537), the Youth Fund of the Second Affiliated Hospital of Xi’an Jiaotong University (YJ(QN) 202318).
Disclosure
The authors declare that they have no competing interests.
References
1. Pratt CH, King LE, Messenger AG, Christiano AM, Sundberg JP. Alopecia areata. Nature Reviews Disease Primers. 2017;3(1). doi:10.1038/nrdp.2017.11
2. Zhou C, Li X, Wang C, Zhang J. Alopecia areata: an update on etiopathogenesis, diagnosis, and management. Clinical Reviews in Allergy & Immunology. 2021;61(3):403–423. doi:10.1007/s12016-021-08883-0
3. Sterkens A, Lambert J, Bervoets A. Alopecia areata: a review on diagnosis, immunological etiopathogenesis and treatment options. Clin Exp Med. 2021;21(2):215–230. doi:10.1007/s10238-020-00673-w
4. Lee HH, Gwillim E, Patel KR, et al. Epidemiology of alopecia areata, ophiasis, totalis, and universalis: a systematic review and meta-analysis. J Am Acad Dermatol. 2020;82(3):675–682. doi:10.1016/j.jaad.2019.08.032
5. Simakou T, Butcher JP, Reid S, Henriquez FL. Alopecia areata: a Multifactorial Autoimmune Condition. J Autoimmun. 2019;98(98):74–85. doi:10.1016/j.jaut.2018.12.001
6. Rajabi F, Drake LA, Senna MM, Rezaei N. Alopecia areata: a review of disease pathogenesis. Br J Dermatol. 2018;179(5):1033–1048. doi:10.1111/bjd.16808
7. Phan K, Ramachandran V, Sebaratnam DF. Methotrexate for alopecia areata: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(1):120–127.e2. doi:10.1016/j.jaad.2018.06.064
8. Xing L, Dai Z, Jabbari A, et al. Alopecia areata is driven by cytotoxic T lymphocytes and is reversed by JAK inhibition. Nature Med. 2014;20(9):1043–1049. doi:10.1038/nm.3645
9. Strober BE, Siu K, Alexis AF, et al. Etanercept does not effectively treat moderate to severe alopecia areata: an open-label study. J Am Acad Dermatol. 2005;52(6):1082–1084. doi:10.1016/j.jaad.2005.03.039
10. Bolduc C, Bissonnette R. Safety and efficacy of adalimumab for the treatment of severe alopecia areata: case series of three patients. J Cutaneous Med Surg. 2012;16(4):257–260. doi:10.1177/120347541201600407
11. Toussi A, Barton VR, Le ST, Agbai ON, Kiuru M. Psychosocial and psychiatric comorbidities and health-related quality of life in alopecia areata: a systematic review. J Am Acad Dermatol. 2021;85(1):162–175. doi:10.1016/j.jaad.2020.06.047
12. Kridin K, Renert‐Yuval Y, Guttman‐Yassky E, Cohen AD. Alopecia areata is associated with atopic diathesis: results from a population-based study of 51,561 patients. J Aller Clin Immunol Pract. 2020;8(4):1323–1328.e1. doi:10.1016/j.jaip.2020.01.052
13. Lee S, Lee H, Lee CH, Lee WS. Comorbidities in alopecia areata: a systematic review and meta-analysis. J Am Acad Dermatol. 2019;80(2):466–477.e16. doi:10.1016/j.jaad.2018.07.013
14. O’Hagan R, Caldas SA, Correa da Rosa JM, Guttman‐Yassky E, Ungar B. Alopecia areata is associated with increased genetic risk of myocardial infarction: a Mendelian randomization study. J Eur Acad Dermatol Venereol. 2023;37(11):e1341–e1343. doi:10.1111/jdv.19318
15. Yu N, Guo Y. Association between alopecia areata, anxiety, and depression: insights from a bidirectional two-sample Mendelian randomization study. J Affective Disord. 2024;350:328–331. doi:10.1016/j.jad.2024.01.152
16. Bowden J, Del Greco MF, Minelli C, Davey Smith G, Sheehan N, Thompson J. A framework for the investigation of pleiotropy in two-sample summary data Mendelian randomization. Stat Med. 2017;36(11):1783–1802. doi:10.1002/sim.7221
17. Boef AGC, Dekkers OM, le Cessie S. Mendelian randomization studies: a review of the approaches used and the quality of reporting. Int J Epidemiol. 2015;44(2):496–511. doi:10.1093/ije/dyv071
18. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through Egger regression. Int J Epidemiol. 2015;44(2):512–525. doi:10.1093/ije/dyv080
19. Wang X, Zhu Z. Role of Ubiquitin-conjugating enzyme E2 (UBE2) in two immune-mediated inflammatory skin diseases: a Mendelian randomization analysis. Archives of Dermatological Res. 2024;316(6). doi:10.1007/s00403-024-02976-4
20. Khan AS, Dageforde LA. Cholangiocarcinoma. Surg Clin North Am. 2019;99(2):315–335. doi:10.1016/j.suc.2018.12.004
21. Welzel TM, Graubard BI, El–Serag HB, et al. Risk factors for intrahepatic and extrahepatic cholangiocarcinoma in the United States: a population-based case-control study. Clin Gastroenterol Hepatol. 2007;5(10):1221–1228. doi:10.1016/j.cgh.2007.05.020
22. Vithayathil M, Khan SA. Current epidemiology of cholangiocarcinoma in Western countries. J Hepatol. 2022;77(6):1690–1698. doi:10.1016/j.jhep.2022.07.022
23. Squadroni M, Tondulli L, Gatta G, Mosconi S, Beretta G, Labianca R. Cholangiocarcinoma. Crit rev oncol/hematol. 2017;116:11–31. doi:10.1016/j.critrevonc.2016.11.012
24. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. Ca a Cancer J Clinicians. 2018;68(6):394–424. doi:10.3322/caac.21492
25. Dekker E, Tanis PJ, Vleugels JLA, Kasi PM, Wallace MB. Colorectal Cancer. Lancet. 2019;394(10207):1467–1480. doi:10.1016/s0140-6736(19)32319-0
26. Arnold M, Sierra MS, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global patterns and trends in colorectal cancer incidence and mortality. Gut. 2016;66(4):683–691. doi:10.1136/gutjnl-2015-310912
27. Ferlitsch M, Moss A, Hassan C, et al. Colorectal polypectomy and endoscopic mucosal resection (EMR): European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy. 2017;49(03):270–297. doi:10.1055/s-0043-102569
28. Huang J, Li X, Hong J, et al. Inflammatory bowel disease increases the risk of hepatobiliary pancreatic cancer: a two‐sample Mendelian randomization analysis of European and East Asian populations. Cancer Med. 2023;12(12):13599–13609. doi:10.1002/cam4.6057
29. Xu Jia L, Ge Gao M, Xian Chen X, Ming Rong Y, Li Huang L, Jin Sheng H. Genetically predicted causal effects of gut microbiota and gut metabolites on digestive tract cancer: a two-sample Mendelian randomization analysis. World J Oncol. 2023;14(6):558–569. doi:10.14740/wjon1737
30. Yang X, Wang J, Wang H. Association between sleep traits and primary liver cancer: a Mendelian randomization analysis. Eur. J. Clin. Invest. 2023;53(8). doi:10.1111/eci.14002
31. Li Y, Ye D, Zhou W, Liu B, Mao Y, Sun X. Alcohol consumption and colorectal cancer risk: a Mendelian randomization study. Front Genetics. 2022;23(13):967229. doi:10.3389/fgene.2022.967229
32. Suzuki S, Goto A, Nakatochi M, et al. Body mass index and colorectal cancer risk: a Mendelian randomization study. Cancer Sci. 2021;112(4):1579–1588. doi:10.1111/cas.14824
33. Lawler TP, Warren Andersen S. Serum 25-Hydroxyvitamin D and cancer risk: a systematic review of Mendelian randomization studies. Nutrients. 2023;15(2):422. doi:10.3390/nu15020422
34. Mostaghimi A, Qureshi S, Joyce C, Guo Y, Huang KP. Reduced incidence of skin cancer in patients with alopecia areata: a retrospective cohort study. Cancer Epidemiol. 2016;41:129–131. doi:10.1016/j.canep.2016.02.009
35. Chen CC, Chang YT, Liu HN, Chen YJ. Cancer risk in patients with alopecia areata: a nationwide population-based matched cohort study. Cancer Med. 2018;7(5):2153–2159. doi:10.1002/cam4.1448
36. Ly S, Manjaly P, Kamal K, et al. Comorbid conditions associated with alopecia areata: a systematic review and meta-analysis. Am J Clin Dermatol. 2023;24(6):875–893. doi:10.1007/s40257-023-00805-4
37. Petukhova L, Duvic M, Hordinsky M, et al. Genome-wide association study in alopecia areata implicates both innate and adaptive immunity. Nature. 2010;466(7302):113–117. doi:10.1038/nature09114
38. Ito T, Ito N, Saatoff M, et al. Maintenance of hair follicle immune privilege is linked to prevention of NK cell attack. J Invest Dermatol. 2008;128(5):1196–1206. doi:10.1038/sj.jid.5701183
39. López-Soto A, Huergo-Zapico L, Acebes-Huerta A, Villa-Alvarez M, Gonzalez S. NKG2D signaling in cancer immunosurveillance. Int J Cancer. 2014;136(8):1741–1750. doi:10.1002/ijc.28775
40. Biswas S, Mandal G, Payne KK, et al. IgA transcytosis and antigen recognition govern ovarian cancer immunity. Nature. 2021;591(7850):464–470. doi:10.1038/s41586-020-03144-0
41. Knochelmann HM, Dwyer CJ, Bailey SR, et al. When worlds collide: th17 and Treg cells in cancer and autoimmunity. Cell. Mol. Immunol. 2018;15(5):458–469. doi:10.1038/s41423-018-0004-4
42. Zhao H, Wu L, Yan G, et al. Inflammation and tumor progression: signaling pathways and targeted intervention. Signal Transduct Targeted Ther. 2021;6(1). doi:10.1038/s41392-021-00658-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Genetically Predicted Serum Albumin and Risk of Colorectal Cancer: A Bidirectional Mendelian Randomization Study
Lv L, Sun X, Liu B, Song J, Wu DJH, Gao Y, Li A, Hu X, Mao Y, Ye D
Clinical Epidemiology 2022, 14:771-778
Published Date: 21 June 2022
The Causal Relationship Between Gastroesophageal Reflux Disease and Chronic Obstructive Pulmonary Disease: A Bidirectional Two-Sample Mendelian Randomization Study
Liu B, Chen M, You J, Zheng S, Huang M
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:87-95
Published Date: 10 January 2024
Exploring a Potential Causal Link Between Dietary Intake and Chronic Obstructive Pulmonary Disease: A Two-Sample Mendelian Randomization Study
Zhang C, Yu L, Xiong T, Zhang Y, Liu J, Zhang J, He P, Xi Y, Jiang Y
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:297-308
Published Date: 26 January 2024
Genomics-Microbiome Based Assessment of Bidirectional Causality Between Gut Microbiota and Psoriasis
Gao Q, Liu JH, Ma WY, Cheng ZL, Hao PS, Luo NN
Clinical, Cosmetic and Investigational Dermatology 2024, 17:435-445
Published Date: 13 February 2024
The Impact of the COVID-19 Pandemic on Incidence and Short-Term Survival for Common Solid Tumours in the United Kingdom: A Cohort Analysis
Barclay NL, Burkard T, Burn E, Delmestri A, Miquel Dominguez A, Golozar A, Guarner-Argente C, Avilés-Jurado FX, Man WY, Roselló Serrano À, Rosen AW, Tan EH, Tietzova I, Prieto Alhambra D, Newby D
Clinical Epidemiology 2024, 16:417-429
Published Date: 11 June 2024