")
Back to Journals » International Journal of Women's Health » Volume 16
Causal Relationship Between Endometriosis, Female Infertility, and Primary Ovarian Failure Through Bidirectional Mendelian Randomization
Received 23 July 2024
Accepted for publication 26 November 2024
Published 9 December 2024 Volume 2024:16 Pages 2143—2155
DOI https://doi.org/10.2147/IJWH.S488351
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Jiayi Guo,* Yongjun Wang,* Guansheng Chen
Department of Gynecology and Obstetrics, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiayi Guo, Department of Gynecology and Obstetrics, Beijing Jishuitan Hospital, Capital Medical University, Beijing, 100035, People’s Republic of China, Email [email protected]
Background: Endometriosis and its associated gynecological diseases such as female infertility and primary ovarian failure (POF), impose a long-term disease burden on women. This study aims to explore the causal relationships between these conditions through a two-sample bidirectional Mendelian randomization (MR) study.
Methods: We utilized large-scale GWAS data and conducted bidirectional MR analyses using methods such as Inverse Variance Weighted (IVW) and MR-Egger to assess the causal relationships between endometriosis and female infertility, POF, amenorrhoea, and oligomenorrhoea.
Results: MR analysis revealed significant causal relationships between endometriosis and female infertility (OR=1.430, 95% CI 1.306– 1.567, P< 0.01) as well as POF (OR=1.348, 95% CI 1.050– 1.731, P=0.019). Reverse MR analysis indicated causal relationships between amenorrhoea (OR=1.076, 95% CI 1.009– 1.148, P=0.026) and female infertility (OR=1.340, 95% CI 1.092– 1.645, P< 0.01) with endometriosis. Sensitivity analyses confirmed the robustness of these findings (heterogeneity: Q_pval> 0.05, pleiotropy: pval> 0.05).
Conclusion: This study suggested that managing endometriosis may help prevent conditions such as female infertility and POF, and vice versa. Future research is needed to confirm these findings in more diverse populations.
Keywords: Endometriosis, primary ovarian failure, female infertility, bidirectional Mendelian randomization, two-sample Mendelian randomization, IVW analysis, sensitivity analysis
Introduction
Endometriosis is a highly heterogeneous chronic inflammatory disease affecting approximately 10% of women of reproductive age worldwide.1 The prevalence of endometriosis is about 6–10% in Western countries, whereas in Asian countries, this proportion may be higher, with some studies reporting up to 15%.2,3 This disease commonly affects women aged 30 to 40 years but can also be found in adolescents and postmenopausal women.4 Additionally, the prevalence of endometriosis is as high as 20–50% among women undergoing infertility treatment and 30–70% among those experiencing chronic pelvic pain.5 Endometriosis significantly impacts patients’ quality of life and increases healthcare costs, leading to substantial economic and social burdens.
Endometriosis involves the implantation and growth of ectopic endometrial-like tissue, causing local chronic inflammation and fibrosis.6 Imbalanced hormone levels, low BMI, and retrograde menstruation are considered risk factors for endometriosis.7 The pathogenesis of endometriosis involves multiple complex biological processes, including cell proliferation, inflammatory response, immune evasion, and angiogenesis, and is typically associated with high estrogen levels.8
As a multi-systemic disease, the chronic inflammatory response and immune dysregulation caused by endometriosis may increase the risk of other gynecological diseases in patients with endometriosis.9 For example, chronic inflammation may promote adenomyosis and uterine fibroids, while immune system abnormalities may increase the risk of ovarian cancer.10,11 Among common gynecological diseases, polycystic ovary syndrome (PCOS) is a prevalent endocrine and metabolic disorder characterized by chronic anovulation and hyperandrogenemia.12 PCOS not only causes menstrual irregularities and infertility but also increases the risk of metabolic syndrome, type 2 diabetes, and cardiovascular diseases.13 Studies have found that metabolic disorders caused by PCOS and exposure to high estrogen levels can lead to endometrial hyperplasia, with a higher incidence of endometriosis in PCOS patients.14 However, despite the known associations between PCOS and endometriosis, the causal mechanisms linking these two conditions remain unclear. Investigating this causal relationship is critical for understanding the interplay between metabolic and reproductive health in women.
Primary ovarian failure (POF) refers to the state of ovarian insufficiency before the age of 40. POF patients face increased risks of osteoporosis and cardiovascular diseases due to early estrogen deficiency.15 Research shows that the common etiologies of POF and endometriosis may include genetic susceptibility and immune system abnormalities.16,17 Despite these known associations, there is a significant research gap in understanding whether POF may causally influence endometriosis risk, or vice versa. Exploring the potential bidirectional causal relationships between endometriosis and POF could offer new insights into the shared pathophysiological mechanisms, particularly concerning premature ovarian aging and inflammation.
Amenorrhoea and oligomenorrhoea are menstrual disorders that share overlapping pathological mechanisms with endometriosis, such as inflammation and tissue fibrosis affecting the normal function of the endometrium.18 Additionally, endometriosis is a significant cause of female infertility, potentially interfering with fertility through mechanisms such as pelvic adhesions, impaired ovarian function, and altered uterine environment.19 Female infertility severely impacts women’s quality of life and mental health, often leading to anxiety and depression.20
Despite numerous observational studies revealing potential associations between endometriosis and various gynecological diseases, the causality remains uncertain due to methodological limitations such as confounding factors and reverse causation.21 Furthermore, few studies have comprehensively explored the bidirectional causal relationships between endometriosis and specific gynecological diseases like PCOS and POF. This gap in the literature highlights the need for rigorous methods to disentangle these complex relationships and better understand how managing one condition might influence the progression of the other.
To address these issues, the Mendelian Randomization (MR) method has been introduced. MR utilizes genetic variations as instrumental variables, leveraging the random allocation of genes to control for confounding factors and reverse causation, thereby providing a more accurate assessment of causal relationships between diseases.22 Previous studies employing MR have already elucidated causal relationships between endometriosis and certain health issues. For instance, one study using MR analysis found a causal association between endometriosis and low bone density.23 Another study revealed a causal relationship between endometriosis and depression using MR.24 These findings not only demonstrate the efficacy of MR in uncovering causal relationships related to endometriosis but also lay the theoretical foundation for further research.
Compared to traditional observational studies, MR studies offer significant advantages. Firstly, genetic variations are randomly allocated at conception, and their distribution is not influenced by environmental factors or individual behaviors, helping to reduce confounding bias.25 Secondly, using genetic variations as instrumental variables effectively prevents reverse causation, allowing for a more accurate evaluation of causal relationships.26 Therefore, MR is considered a powerful tool for validating causal relationships between diseases.
This study aims to investigate the causal relationships between endometriosis and gynecological diseases through a two-sample bidirectional MR approach. The objective is to verify whether endometriosis is a causative factor for other gynecological diseases and to explore whether other gynecological diseases increase the risk of endometriosis. By conducting this research, we hope to address the current research gaps and provide new scientific evidence for the prevention and treatment of these diseases, ultimately reducing the disease burden on patients and improving their quality of life.
Materials and Methods
Study Design
This study employed a two-sample bidirectional MR design to investigate the causal relationships between endometriosis and the risks of other gynecological diseases (Figure 1). The study data were sourced from publicly available large-scale genome-wide association studies (GWAS) databases, covering more than 500,000 individuals of European ancestry. Data collection for the GWAS studies occurred between January 1998 and December 2019, and our MR analysis was performed between January 2024 and March 2024.
 |
Figure 1 Diagram of causal relationships between endometriosis and gynecological diseases. |
MR analysis is based on three key assumptions: 1) The single nucleotide polymorphisms (SNPs) are strongly associated with the exposure factors; 2) The SNPs are independent of confounding factors; 3) The SNPs affect the outcome only through the exposure factors. SNPs associated with endometriosis and other gynecological diseases were used as instrumental variables. These gynecological diseases, such as PCOS, POF, and amenorrhoea, have known genetic components that contribute to their pathogenesis, making them suitable for GWAS-based MR analysis. After screening, SNPs that met these three core assumptions were included in the MR analysis.
The two-sample bidirectional MR analysis was conducted in two steps to assess the potential bidirectional causal relationships. In the first step, endometriosis was treated as the exposure, and we analyzed its potential causal effect on gynecological diseases (female infertility, POF, and amenorrhoea), using methods such as inverse variance weighted (IVW), weighted median, and MR-Egger to strengthen the validity and robustness of the findings. In the second step, the roles were reversed, and we examined whether gynecological diseases increase the risk of developing endometriosis.27 Similar to Step 1, we used IVW, weighted median, and MR-Egger methods to explore these relationships.
Bidirectional MR analysis was chosen because it addresses the limitation of traditional one-directional approaches, which might miss important reverse causal relationships. Given the complex interplay between endometriosis and other conditions, this approach ensures that both potential pathways are considered, offering a fuller picture of the underlying biological mechanisms.
To ensure the robustness of our findings, sensitivity analyses, including Cochran’s Q test, MR-PRESSO, and leave-one-out methods, were conducted to assess heterogeneity and pleiotropy (Figure 2). This study aims to reveal the potential causal relationships between endometriosis and other gynecological diseases, providing a theoretical foundation for the prevention and treatment of these related conditions.
 |
Figure 2 Research design. |
Data Sources
The data for this study were sourced from GWAS databases, primarily the GWAS catalog (https://gwas.mrcieu.ac.uk/). Endometriosis-related data covered 77,257 samples and included a total of 16,377,306 SNPs. The gynecological diseases included in this study are PCOS, POF, amenorrhoea, oligomenorrhoea, and female infertility. Detailed sources and data are provided in Table 1. This study predominantly used data from individuals of European ancestry, which may limit the generalizability of the results to other populations. Future studies involving diverse cohorts are required to validate these findings across different ethnic groups.
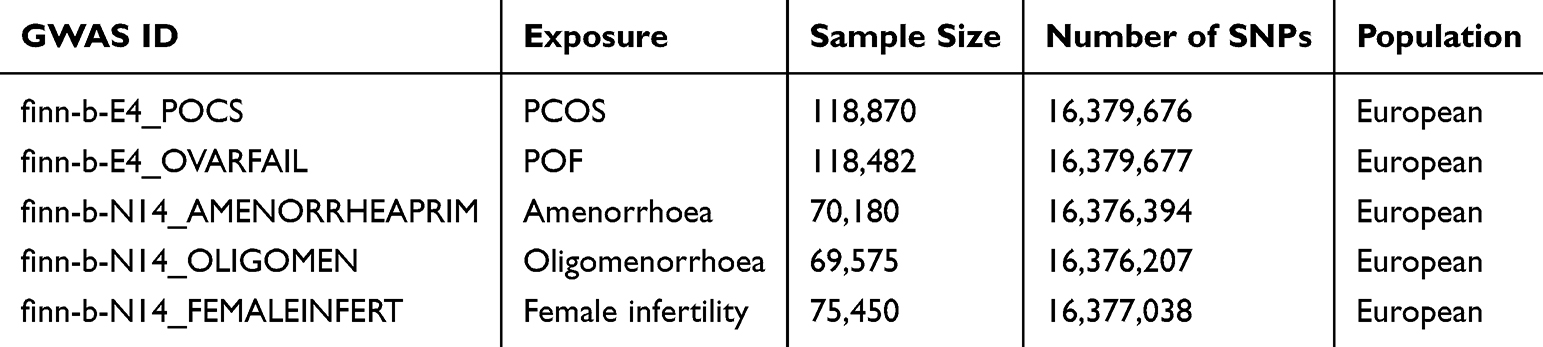 |
Table 1 Detailed Sources and Data of SNPs Related to Gynecological Diseases |
All data used in this study were sourced from publicly available databases, where prior ethical approval and informed consent were secured in the original studies. In accordance with Article 16 of the Measures for the Ethical Review of Life Sciences and Medical Research Involving Humans in China, which allows exemption from ethical review for research based on legally obtained public or anonymized data, no further ethical approval was required for this study.
Selection of Instrumental Variables
In this study, the selection of instrumental variables was conducted strictly according to the standards of MR studies. First, SNPs associated with endometriosis and gynecological diseases were selected from the GWAS database.28 To ensure that the selected SNPs had a strong and reliable association with the exposure variables, we applied a stringent p-value threshold of 5e-08. This threshold is commonly used in MR studies to minimize the inclusion of weak genetic associations. In cases where no instrumental SNPs met this strict threshold, the p-value was relaxed to 5e-6 to allow for the selection of sufficient instrumental variables while maintaining a reasonable confidence level in the genetic associations.
To ensure that the selected SNPs were independent and not in linkage disequilibrium (LD), we applied a criterion of r2 < 0.001. These ensures that the SNPs are not correlated with each other, which could otherwise introduce bias into the MR analysis. Specifically, SNPs within a 1000 kb window that exhibited an r2 value higher than this threshold were excluded from the analysis. This process helps maintain the assumption that the SNPs affect the outcome only through the exposure, reducing the risk of confounding.
Additionally, the F-statistic was calculated for each instrumental variable to assess the strength of the association between the SNPs and the exposure. An F-value greater than 10 generally was used as the threshold for strong instruments, as values below this level could indicate weak instruments, which may lead to biased and unreliable causal estimates. By ensuring that all selected SNPs met this F-statistic threshold, we minimized the risk of weak instrument bias in our MR analysis.
MR Analysis
In this study, MR analysis was conducted using the TwoSampleMR version 0.5.7 package in R to evaluate the causal effects of endometriosis on other gynecological diseases. The primary methods used include IVW, weighted median, MR-Egger, and Wald ratio, considering multiple statistical models to ensure the robustness and reliability of the study results.29 IVW was the main method used to determine the causal relationship between exposure and outcome, with other methods providing supplementary information. A causal relationship was confirmed if the beta direction of IVW, weighted median, and MR-Egger were consistent (all greater than 0 or all less than 0), and at least the p-value of IVW was less than 0.05.
IVW calculates a weighted average of the effects of multiple genetic variants based on the inverse of their variances, assuming all instrumental variables are valid and free from horizontal pleiotropy. However, IVW is sensitive to pleiotropy, which may bias the results, necessitating sensitivity analyses of the MR results.
Using these three methods together enhances the reliability and robustness of causal inference. When the results are consistent across these methods, the credibility of the causal relationship is enhanced. If the results are inconsistent, further investigation into potential pleiotropy or instrumental variable selection issues is required to ensure the accuracy and reliability of the study findings.
The Wald ratio method was applied in cases where a single SNP served as an instrumental variable, estimating causal effects by calculating the effect ratio of the exposure on the outcome divided by the effect of the exposure on the SNP. Although simple and suitable for single instrumental variables, this method cannot be applied when multiple SNPs are used and may rely heavily on the available data.
Sensitivity Analysis
To ensure the robustness and reliability of the MR analysis results, comprehensive sensitivity analyses were conducted in this study.30
First, heterogeneity was assessed using Cochran’s Q test. A Q_test result with p > 0.05 indicated no heterogeneity among the genetic instruments, suggesting that the instruments were consistent in their estimation of the causal effect. In cases of heterogeneity (p < 0.05), we employed the IVW random-effects model or weighted median method for more robust estimates. When heterogeneity was present, results from the weighted median or IVW random-effects model were used; when heterogeneity was absent, the standard IVW random-effects model was used to produce the causal estimates.
Second, the presence of pleiotropy was assessed using the MR-PRESSO test. This method was used to detect horizontal pleiotropy by identifying and excluding outliers that could bias the causal estimates. After removing outliers, the analysis was rerun to evaluate whether pleiotropy persisted. A pleiotropy test result with p > 0.05 indicated no pleiotropy. If pleiotropy remained unresolved, the results were interpreted with caution, and adjustments were made where necessary.
Third, the leave-one-out method was used to iteratively exclude each instrumental variable, calculate the meta-effect of the remaining instrumental variables, and observe the impact on the results. This allowed us to assess the influence of each SNPs on the overall findings. If excluding a specific SNP significantly changed the results, it was excluded from the analysis.
When results from MR-Egger and IVW were inconsistent, MR-Egger was given more weight, as it accounts for directional pleiotropy. A non-zero MR-Egger intercept suggested pleiotropy, and adjustments were made accordingly. In such cases, we highlighted the need for cautious interpretation.
Overall, these sensitivity analyses confirmed the robustness and reliability of the causal estimates, showing consistency across methods and indicating that pleiotropy or heterogeneity was unlikely to drive the observed causal relationships.
Results
Causal Relationship Analysis of SNPs Related to Gynecological Diseases
MR analysis was conducted with endometriosis as the exposure and gynecological diseases as the outcomes. After screening, a total of 11 SNPs associated with endometriosis were included, all of which were strongly associated with endometriosis as the exposure (F > 10). The IVW method estimated potential causal relationships between endometriosis and female infertility (OR=1.430, 95% CI 1.306–1.567, P<0.01) and POF (OR=1.348, 95% CI 1.050–1.731, P=0.019) (Figure 3). The trends detected by MR-Egger, IVW, and weighted median methods were consistent, showing that as endometriosis increases, the risks of female infertility (Figure 4) and POF (Figure 5) also increase. Clinically, these findings suggest that early diagnosis and proactive management of endometriosis could play a critical role in preserving fertility and preventing ovarian insufficiency, particularly in women who are planning to conceive or are at high risk for reproductive complications. By intervening earlier in the disease progression, healthcare providers may reduce these long-term risks.
 |
Figure 3 Forest plot of the results from two-sample Mendelian randomization (MR) analysis of endometriosis and gynecological diseases. Each row represents different outcomes or exposures, indicating the strength and direction of the associations. The red diamonds represent the OR, and the horizontal lines represent the 95% CI. The far-right column notes the number of single nucleotide polymorphisms (SNPs) used in each analysis. P < 0.05 is denoted by an asterisk (*), representing statistically significant results. |
 |
Figure 4 Visualization of two-sample Mendelian randomization (MR) analysis. (A) Scatter plot showing the effect of endometriosis on female infertility. Each point represents a single nucleotide polymorphism (SNP). The x-axis represents the effect sizes of SNPs on Hip osteoarthritis, and the y-axis represents their effect on fasting insulin levels. (B) Forest plot. Each horizontal line reflects the estimated result of a single SNP. A line entirely to the left of 0 indicates a positive correlation, while a line entirely to the right of 0 indicates a negative correlation. Results crossing 0 are considered non-significant. The red line at the bottom represents the combined results of multiple SNPs. |
 |
Figure 5 Visualization of two-sample Mendelian randomization (MR) analysis. (A) Scatter plot showing the effect of endometriosis on POF. Each point represents a single nucleotide polymorphism (SNP). The x-axis represents the effect sizes of SNPs on Hip osteoarthritis, and the y-axis represents their effect on fasting insulin levels. (B) Forest plot. Each horizontal line reflects the estimated result of a single SNP. A line entirely to the left of 0 indicates a positive correlation, while a line entirely to the right of 0 indicates a negative correlation. Results crossing 0 are considered non-significant. The red line at the bottom represents the combined results of multiple SNPs. |
No potential causal relationships were found between endometriosis and amenorrhoea (OR=1.028, 95% CI 0.806–1.31, P=0.825), oligomenorrhoea (OR=1.073, 95% CI 0.868–1.325, P=0.515), or PCOS (OR=0.979, 95% CI 0.774–1.239, P=0.863) (Figure 3). These findings further emphasize that not all gynecological conditions are directly influenced by endometriosis, and tailored clinical approaches should focus on the specific comorbidities that are at higher risk, such as infertility and POF.
In the sensitivity analysis, the results of heterogeneity testing (Q_pval > 0.05) and pleiotropy testing (pval > 0.05) were not statistically significant (Table 2), indicating that the MR analysis results did not exhibit heterogeneity or horizontal pleiotropy.
 |
Table 2 Sensitivity Analysis Results of Endometriosis on Gynecological Diseases |
Causal Relationship Analysis of SNPs Related to Endometriosis
Reverse MR analysis was conducted with gynecological diseases as the exposure and endometriosis as the outcome. For PCOS and POF, only one SNP was selected after screening; thus, the Wald ratio method was used for their analysis. The SNPs included in the reverse MR analysis were all strongly associated with the gynecological diseases as the exposure (F > 10). The IVW results were significant, indicating potential causal relationships between genetically predicted amenorrhoea (OR=1.076, 95% CI 1.009–1.148, P=0.026) and female infertility (OR=1.340, 95% CI 1.092–1.645, P<0.01) with endometriosis (Figure 6). The trends detected by MR-Egger, IVW, and weighted median methods were consistent, showing that as the risks of amenorrhoea (Figure 7) and female infertility (Figure 8) increase, the risk of endometriosis also increases. From a clinical perspective, these results imply that women presenting with amenorrhoea or infertility should be closely monitored for potential development of endometriosis. Early identification of endometriosis in these high-risk groups may facilitate timely intervention and improve reproductive outcomes.
 |
Figure 6 Forest plot of the results from two-sample Mendelian randomization (MR) analysis of gynecological diseases and endometriosis. Each row represents different outcomes or exposures, indicating the strength and direction of the associations. The red diamonds represent the OR, and the horizontal lines represent the 95% CI. The far-right column notes the number of single nucleotide polymorphisms (SNPs) used in each analysis. P < 0.05 is denoted by an asterisk (*), representing statistically significant results. |
 |
Figure 7 Visualization of two-sample Mendelian randomization (MR) analysis. (A) Scatter plot showing the effect of amenorrhoea on endometriosis. Each point represents a single nucleotide polymorphism (SNP). The x-axis represents the effect sizes of SNPs on Hip osteoarthritis, and the y-axis represents their effect on fasting insulin levels. (B) Forest plot. Each horizontal line reflects the estimated result of a single SNP. A line entirely to the left of 0 indicates a positive correlation, while a line entirely to the right of 0 indicates a negative correlation. Results crossing 0 are considered non-significant. The red line at the bottom represents the combined results of multiple SNPs. |
 |
Figure 8 Visualization of two-sample Mendelian randomization (MR) analysis. (A) Scatter plot showing the effect of female infertility on endometriosis. Each point represents a single nucleotide polymorphism (SNP). The x-axis represents the effect sizes of SNPs on Hip osteoarthritis, and the y-axis represents their effect on fasting insulin levels. (B) Forest plot. Each horizontal line reflects the estimated result of a single SNP. A line entirely to the left of 0 indicates a positive correlation, while a line entirely to the right of 0 indicates a negative correlation. Results crossing 0 are considered non-significant. The red line at the bottom represents the combined results of multiple SNPs. |
No potential causal relationships were found between oligomenorrhoea (OR=1.010, 95% CI 0.967–1.055, P=0.651), PCOS (OR=0.957, 95% CI 0.864–1.059, P=0.393), POF (OR=1.052, 95% CI 0.978–1.132, P=0.175), and endometriosis (Figure 6). These findings suggest that while some conditions like amenorrhoea and infertility are linked with endometriosis, others may not share the same causal pathways, highlighting the importance of personalized risk assessment in clinical practice.
As with the first analysis, sensitivity analysis confirmed the robustness of these results, with no evidence of heterogeneity or pleiotropy affecting the conclusions (Table 3).
 |
Table 3 Sensitivity Analysis Results of Gynecological Diseases on Endometriosis |
Discussion and Conclusion
This study explored the causal relationships between gynecological diseases and endometriosis through MR analysis. The bidirectional MR analysis found that: 1) There is a potential negative causal relationship between genetically predicted endometriosis and female infertility and POF. 2) There is a potential negative causal relationship between genetically predicted amenorrhoea, female infertility, and endometriosis. 3) The results suggest that there may be a potential bidirectional causal relationship between endometriosis and female infertility. The MR analysis in this study did not exhibit heterogeneity or horizontal pleiotropy, and no additional causal relationships were found.
The pathological mechanisms of endometriosis may involve chronic inflammation, immune system abnormalities, and oxidative stress. These factors can lead to ovarian tissue damage and follicle depletion, triggering the onset of POF.31 Specifically, chronic inflammation caused by endometriosis may increase pro-inflammatory cytokines in the local environment, directly affecting normal ovarian function and promoting premature follicle depletion.4 Additionally, immune system abnormalities, such as the activation of autoimmune responses, can also damage ovarian tissue, further increasing the risk of POF.32 Immune dysregulation, similar to that seen in endometriosis, has been linked to tumor-associated immune cells in cancers such as cervical cancer, where specific immune cell subpopulations contribute to disease progression.33 However, there are currently few studies on the association between endometriosis and POF, with previous research focusing more on the discussion of BMI and its association with endometriosis and POF.10,34 It has been found that lipid metabolism and hormonal level changes caused by the pathological mechanisms of endometriosis and POF are related to BMI,35,36 indicating a causal relationship between gynecological diseases and BMI.37 Regarding the negative causal relationship between endometriosis and POF found in this study, current research does not yet support this result.
Previous Mendelian randomization studies have investigated the link between endometriosis and other conditions, including ovarian cancer. For instance, Wang et al38 have explored the causal relationship between endometriosis and epithelial ovarian cancer. Their findings indicated a potential causal link between endometriosis and increased ovarian cancer risk, highlighting the long-term risks of untreated or severe endometriosis. In contrast, our study focused on the relationship between endometriosis and non-cancerous gynecological diseases, such as POF and female infertility. While both studies used similar methodological approaches, our research provides novel insights into the bidirectional nature of the relationship between endometriosis and infertility, which was not examined in the context of ovarian cancer. This bidirectional link suggests that managing endometriosis may not only prevent associated gynecological diseases but also improve fertility outcomes, providing a new dimension to endometriosis management.
Some studies have found that endometriosis is associated with an increased risk of ovarian cancer,8 and both ovarian cancer and POF cause changes in estrogen levels. Mechanistic studies, such as those using scRNA-seq to analyze ovarian cancer subpopulations, have provided insights into how genetic and environmental factors contribute to disease progression.39 Endometriosis is also related to changes in hormone levels. However, this study did not include ovarian cancer and BMI as instrumental variables. Future research could increase the sample size and include these variables for further investigation.
A potential negative causal relationship was also found between genetically predicted amenorrhoea and endometriosis. Chronic pelvic inflammation and tissue fibrosis caused by endometriosis may interfere with normal menstrual cycles, leading to amenorrhoea.40 Additionally, exposure to adverse hormone levels, medications, or retrograde menstruation are considered risk factors for endometriosis. Various hypotheses have been proposed regarding the pathogenesis of endometriosis, such as the retrograde menstruation hypothesis, hematogenous and lymphatic spread hypotheses.41,42 Suda et al based on the retrograde menstruation hypothesis, suggested that frequent menstrual cycles and increased menstrual flow could raise the risk of endometriosis.43 According to the hematogenous and lymphatic spread hypotheses, the increased risk of endometriosis in amenorrhoea patients may be due to menstrual irregularities, especially the frequent occurrence of anovulatory cycles, which prevent the normal expulsion of endometrial fragments. These fragments could then retrogradely flow through the fallopian tubes into the pelvic cavity, where they implant and grow as endometriotic lesions.7,44 Currently, there are few studies on the association between amenorrhoea and endometriosis. Based on the pathological mechanisms of both diseases, it is believed that the presence of amenorrhoea may increase the risk of developing endometriosis.
Additionally, this study found a potential bidirectional causal relationship between endometriosis and female infertility. In traditional bidirectional MR analysis, bidirectional causal relationships are often discarded to avoid reciprocal causality.45 However, given the complex pathological interactions between endometriosis and infertility, we retained this result for further exploration.46,47
Firstly, endometriosis leads to female infertility through various mechanisms. Chronic inflammation associated with endometriosis can cause pelvic adhesions, leading to fallopian tubes obstruction or distortion, which affects the meeting of eggs and sperm and the transportation of the fertilized egg.48,49 Furthermore, ectopic endometrial tissue can secrete multiple pro-inflammatory cytokines and growth factors, which can interfere with normal ovarian function, leading to ovulation disorders.50 Endometriosis also alters the uterine environment, making it difficult for the fertilized egg to implant successfully, resulting in infertility.51 Epidemiological studies support this view, showing that the infertility rate among endometriosis patients is significantly higher than that of women without endometriosis.52
Conversely, infertility may increase the risk of developing endometriosis through mechanisms related to changes in menstrual cycle dynamics. Infertility, particularly when associated with anovulatory cycles, can prevent the normal expulsion of endometrial fragments, leading to retrograde menstruation and implantation of endometriotic tissue in the pelvic cavity, which can develop into endometriotic lesions.53 Additionally, infertility treatments such as in vitro fertilization can increase the growth of ectopic endometrial tissue through ovulation induction drugs and repeated uterine procedures, facilitating implantation and growth of endometriotic lesions.54 This bidirectional association is further supported by clinical and epidemiological studies, showing a higher prevalence of endometriosis among infertility patients, and vice versa.55
The bidirectional causal relationship between endometriosis and infertility identified in this study is significant both clinically and in terms of research. Understanding these complex mutual influences suggests that effective management of one condition may help mitigate the risk or severity of the other. For example, early treatment of endometriosis could prevent the onset of infertility by reducing pelvic adhesions and preserving ovarian function. Similarly, addressing infertility in patients with endometriosis may reduce the progression of endometriotic lesions and improve fertility outcomes. These findings underscore the importance of an integrated approach in managing both conditions, with careful consideration of their mutual influence.
This study’s findings also highlight the need for future research to investigate the broader clinical implications of this bidirectional relationship. Understanding these mechanisms could inform more comprehensive disease management strategies, ultimately improving the overall health and quality of life for patients affected by endometriosis and infertility.
This study systematically explored the causal relationships between endometriosis and various gynecological diseases through bidirectional MR analysis. A key strength of the study lies in the use of large-scale genome-wide association data and the reliability and the application of multiple MR methods to ensure the reliability and robustness of the results. However, this study also has some limitations. First, the study data mainly come from individuals of European ancestry, which may limit the generalizability of the findings to other populations. Different populations and regions may have genetic and environmental differences that need further validation in future research. Future research should aim to include more diverse cohorts to better understand the variations in disease manifestations and mechanisms across different populations. Second, although the Mendelian Randomization method can effectively control for confounding factors, unmeasured pleiotropy may still affect the results’ accuracy. While various sensitivity analyses were conducted to detect and correct for pleiotropy, caution is still needed when interpreting the results. Previous MR studies focusing on endometriosis have often examined the causal relationships between endometriosis and BMI, uterine fibroids, malignant ovarian cancer, etc.30,56 Unlike previous studies, this study did not include ovarian cancer and BMI as related factors, which could have influenced the results. The strength and number of instrumental variables in the existing GWAS data may be limited.
Future research should enhance the analysis’s accuracy and precision by incorporating larger and more diverse data sources, increasing the number and strength of instrumental variables. Additionally, beyond establishing causal relationships, further research is needed to explore the specific biological mechanisms underlying the relationship between endometriosis and gynecological diseases. Using advanced techniques such as genome editing, eQTL and QTL analyses, cellular and animal models, could help elucidate the biological pathways and genetic mechanisms linking these conditions. Finally, a comprehensive strategy for the prevention and management of endometriosis and related gynecological diseases should include early screening, regular monitoring of ovarian function, optimizing infertility treatment plans, and strengthening the management of menstrual cycle abnormalities.1,57
In conclusion, this study explored the causal relationships between endometriosis and gynecological diseases through MR analysis. We identified potential negative causal relationships between endometriosis and POF, as well as between amenorrhoea and endometriosis, though these associations require further validation. The study also highlighted a complex bidirectional causal relationship between endometriosis and female infertility, indicating that managing one condition could potentially influence the progression of the other.
Data Sharing Statement
The data for this study were sourced from GWAS databases, primarily the GWAS catalog (https://gwas.mrcieu.ac.uk/).
Acknowledgments
Jiayi Guo and Yongjun Wang contributed equally to this work as co-first authors.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Horne AW, Missmer SA. Pathophysiology, diagnosis, and management of endometriosis. BMJ. 2022;379:e070750. doi:10.1136/bmj-2022-070750
2. Soliman AM, Yang H, Du EX, Kelley C, Winkel C. The direct and indirect costs associated with endometriosis: a systematic literature review. Hum Reprod. 2016;31(4):712–722. doi:10.1093/humrep/dev335
3. Ghiasi M, Kulkarni MT, Missmer SA. Is endometriosis more common and more severe than it was 30 years ago? J Minim Invasive Gynecol. 2020;27(2):452–461. doi:10.1016/j.jmig.2019.11.018
4. Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. 2020;382(13):1244–1256. doi:10.1056/NEJMra1810764
5. Kralickova M, Lagana AS, Ghezzi F, Vetvicka V. Endometriosis and risk of ovarian cancer: what do we know? Arch Gynecol Obstet. 2020;301(1):1–10. doi:10.1007/s00404-019-05358-8
6. Tomassetti C, Johnson NP, Petrozza J; International working group of AAGL, ESGE, ESHRE and WES, et al. An International Terminology for Endometriosis, 2021. Facts Views Vis Obgyn. 2021;13(4):295–304. doi:10.52054/FVVO.13.4.036
7. Dawson A, Fernandez ML, Anglesio M, Yong PJ, Carey MS. Endometriosis and endometriosis-associated cancers: new insights into the molecular mechanisms of ovarian cancer development. Ecancermedicalscience. 2018;12:803. doi:10.3332/ecancer.2018.803
8. Barreta A, Sarian L, Ferracini AC, et al. Endometriosis-associated ovarian cancer: population characteristics and prognosis. Int J Gynecol Cancer. 2018;28(7):1251–1257. doi:10.1097/IGC.0000000000001317
9. Symons LK, Miller JE, Kay VR, et al. The immunopathophysiology of endometriosis. Trends Mol Med. 2018;24(9):748–762. doi:10.1016/j.molmed.2018.07.004
10. Gallagher CS, Makinen N, Harris HR, et al. Genome-wide association and epidemiological analyses reveal common genetic origins between uterine leiomyomata and endometriosis. Nat Commun. 2019;10(1):4857. doi:10.1038/s41467-019-12536-4
11. Upson K, Missmer SA. Epidemiology of adenomyosis. Semin Reprod Med. 2020;38(2–3):89–107. doi:10.1055/s-0040-1718920
12. Mikhaleva LM, Davydov AI, Patsap OI, et al. Malignant transformation and associated biomarkers of ovarian endometriosis: a narrative review. Adv Ther. 2020;37(6):2580–2603. doi:10.1007/s12325-020-01363-5
13. Li B, Zhang Y, Zhang L, Zhang L. Association between endometriosis and metabolic syndrome: a cross-sectional study based on the National Health and Nutrition Examination Survey data. Gynecol Endocrinol. 2023;39(1):2254844. doi:10.1080/09513590.2023.2254844
14. Meczekalski B, Perez-Roncero GR, Lopez-Baena MT, Chedraui P, Perez-Lopez FR. The polycystic ovary syndrome and gynecological cancer risk. Gynecol Endocrinol. 2020;36(4):289–293. doi:10.1080/09513590.2020.1730794
15. Armeni E, Paschou SA, Goulis DG, Lambrinoudaki I. Hormone therapy regimens for managing the menopause and premature ovarian insufficiency. Best Pract Res Clin Endocrinol Metab. 2021;35(6):101561. doi:10.1016/j.beem.2021.101561
16. Huang QY, Chen SR, Chen JM, Shi QY, Lin S. Therapeutic options for premature ovarian insufficiency: an updated review. Reprod Biol Endocrinol. 2022;20(1):28. doi:10.1186/s12958-022-00892-8
17. Fiorentino G, Cimadomo D, Innocenti F, et al. Biomechanical forces and signals operating in the ovary during folliculogenesis and their dysregulation: implications for fertility. Hum Reprod Update. 2023;29(1):1–23. doi:10.1093/humupd/dmac031
18. Vannuccini S, Clifton VL, Fraser IS, et al. Infertility and reproductive disorders: impact of hormonal and inflammatory mechanisms on pregnancy outcome. Hum Reprod Update. 2016;22(1):104–115. doi:10.1093/humupd/dmv044
19. Meuleman C, Vandenabeele B, Fieuws S, Spiessens C, Timmerman D, D’Hooghe T. High prevalence of endometriosis in infertile women with normal ovulation and normospermic partners. Fertil Steril. 2009;92(1):68–74. doi:10.1016/j.fertnstert.2008.04.056
20. Skegro B, Bjedov S, Mikus M, et al. Endometriosis, pain and mental health. Psychiatry Danub. 2021;33(Suppl 4):632–636.
21. Shigesi N, Kvaskoff M, Kirtley S, et al. The association between endometriosis and autoimmune diseases: a systematic review and meta-analysis. Hum Reprod Update. 2019;25(4):486–503. doi:10.1093/humupd/dmz014
22. Li Y, Liu H, Ye S, et al. The effects of coagulation factors on the risk of endometriosis: a Mendelian randomization study. BMC Med. 2023;21(1):195. doi:10.1186/s12916-023-02881-z
23. Wang JX, Shen Y, Wang XL, Ma LL, Xu SQ. Causal relationship between endometriosis with infertility and ankylosing spondylitis. Sci Rep. 2023;13(1):13412. doi:10.1038/s41598-023-40647-y
24. Chen P, Jia L, Fang C, Li M. Mood disorders influencing endometriosis and adenomyosis: Mendelian randomisation study. BJPsych Open. 2024;10(3):e83. doi:10.1192/bjo.2024.46
25. Bowden J, Holmes MV. Meta-analysis and Mendelian randomization: a review. Res Synth Methods. 2019;10(4):486–496. doi:10.1002/jrsm.1346
26. Birney E. Mendelian randomization. Cold Spring Harb Perspect Med. 2022;12(4). doi:10.1101/cshperspect.a041302
27. An G, Zhao X, Zhao C. Unraveling the causal association between leukocyte telomere length and infertility: a two-sample Mendelian randomization study. PLoS One. 2024;19(3):e0298997. doi:10.1371/journal.pone.0298997
28. Adewuyi EO, Mehta D, Sapkota Y, et al. Genetic analysis of endometriosis and depression identifies shared loci and implicates causal links with gastric mucosa abnormality. Hum Genet. 2021;140(3):529–552. doi:10.1007/s00439-020-02223-6
29. Lv Y, Xia X, Lei L, et al. Health outcomes of age at menarche in European women: a two-sample Mendelian randomization study. Postgrad Med J. 2023;99(1175):993–999. doi:10.1093/postmj/qgad023
30. McGrath IM, International Endometriosis Genetics C, Montgomery GW, Mortlock S. Genomic characterisation of the overlap of endometriosis with 76 comorbidities identifies pleiotropic and causal mechanisms underlying disease risk. Hum Genet. 2023;142(9):1345–1360. doi:10.1007/s00439-023-02582-w
31. Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. Fertil Steril. 2012;98(3):511–519. doi:10.1016/j.fertnstert.2012.06.029
32. Vercellini P, Vigano P, Somigliana E, Fedele L. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014;10(5):261–275. doi:10.1038/nrendo.2013.255
33. Lin Z, Li X, Shi H, et al. Decoding the tumor microenvironment and molecular mechanism: unraveling cervical cancer subpopulations and prognostic signatures through scRNA-Seq and bulk RNA-seq analyses. Front Immunol. 2024;15:1351287. doi:10.3389/fimmu.2024.1351287
34. Huang L, Wang H, Shi M, Kong W, Jiang M. Lipid profile in patients with primary ovarian insufficiency: a systematic review and meta-analysis. Front Endocrinol. 2022;13:876775. doi:10.3389/fendo.2022.876775
35. Huang Y, Lv Y, Qi T, et al. Metabolic profile of women with premature ovarian insufficiency compared with that of age-matched healthy controls. Maturitas. 2021;148:33–39. doi:10.1016/j.maturitas.2021.04.003
36. Zhou XY, Li X, Zhang J, et al. Plasma metabolomic characterization of premature ovarian insufficiency. J Ovarian Res. 2023;16(1):2. doi:10.1186/s13048-022-01085-y
37. Venkatesh SS, Ferreira T, Benonisdottir S, et al. Obesity and risk of female reproductive conditions: a Mendelian randomisation study. PLoS Med. 2022;19(2):e1003679. doi:10.1371/journal.pmed.1003679
38. Wang L, Li X, Wang Y, et al. Endometriosis and epithelial ovarian cancer: a two-sample Mendelian randomization analysis. Sci Rep. 2023;13(1):21992. doi:10.1038/s41598-023-49276-x
39. Shao W, Lin Z, Xiahou Z, et al. Single-cell RNA sequencing reveals that MYBL2 in malignant epithelial cells is involved in the development and progression of ovarian cancer. Front Immunol. 2024;15:1438198. doi:10.3389/fimmu.2024.1438198
40. Klein DA, Emerick JE, Sylvester JE, Vogt KS. Disorders of puberty: an approach to diagnosis and management. Am Fam Physician. 2017;96(9):590–599.
41. Sampson JA. Perforating hemorrhagic (chocolate) cysts of the ovary: their importance and especially their relation to pelvic adenomas of endometrial type (adenomyoma of the uterus, rectovaginal septum, sigmoid, etc.). Arch Surg. 1921;3:245–323. doi:10.1001/archsurg.1921.01110080003001
42. Sampson JA. Metastatic or embolic endometriosis, due to the menstrual dissemination of endometrial tissue into the venous circulation. Am J Pathol. 1927;3(2):93–110143.
43. Suda K, Nakaoka H, Yoshihara K, et al. Clonal expansion and diversification of cancer-associated mutations in endometriosis and normal endometrium. Cell Rep. 2018;24(7):1777–1789. doi:10.1016/j.celrep.2018.07.037
44. Herreros-Villanueva M, Chen CC, Tsai EM, Er TK. Endometriosis-associated ovarian cancer: what have we learned so far? Clin Chim Acta. 2019;493:63–72. doi:10.1016/j.cca.2019.02.016
45. Ding Y, Fan S, Tang Y, et al. The association between blood lipids and systemic lupus erythematosus: a two-sample Mendelian randomization research. Metabolites. 2022;13(1):27. doi:10.3390/metabo13010027
46. Chen S, Yan S, Aiheti N, et al. A bi-directional Mendelian randomization study of sarcopenia-related traits and type 2 diabetes mellitus. Front Endocrinol. 2023;14:1109800. doi:10.3389/fendo.2023.1109800
47. Liu C, Liu N, Xia Y, Zhao Z, Xiao T, Li H. Osteoporosis and sarcopenia-related traits: a bi-directional Mendelian randomization study. Front Endocrinol. 2022;13:975647. doi:10.3389/fendo.2022.975647
48. Filip L, Duica F, Pradatu A, et al. Endometriosis associated infertility: a critical review and analysis on etiopathogenesis and therapeutic approaches. Medicina. 2020;56(9):460. doi:10.3390/medicina56090460
49. Schenken RS, Asch RH, Williams RF, Hodgen GD. Etiology of infertility in monkeys with endometriosis: luteinized unruptured follicles, luteal phase defects, pelvic adhesions, and spontaneous abortions. Fertil Steril. 1984;41(1):122–130. doi:10.1016/S0015-0282(16)47552-7
50. Marquardt RM, Kim TH, Shin JH, Jeong JW. Progesterone and estrogen signaling in the endometrium: what goes wrong in endometriosis? Int J Mol Sci. 2019;20(15):3822. doi:10.3390/ijms20153822
51. Hodgson RM, Lee HL, Wang R, Mol BW, Johnson N. Interventions for endometriosis-related infertility: a systematic review and network meta-analysis. Fertil Steril. 2020;113(2):374–382e372. doi:10.1016/j.fertnstert.2019.09.031
52. Ferrell K, Rohlfs A, Hansen K, Von Wald T. Endometriosis and infertility. S D Med. 2020;73(8):350–355.
53. Tulandi T. Endometriosis and pelvic pain awareness: infertility, suicidal ideation, and cancer. J Obstet Gynaecol Can. 2021;43(5):543–544. doi:10.1016/j.jogc.2021.03.001
54. Fauque P, De Mouzon J, Devaux A, et al. Reproductive technologies, female infertility, and the risk of imprinting-related disorders. Clin Clin Epigenet. 2020;12(1):191. doi:10.1186/s13148-020-00986-3
55. Maggiore ULR, Chiappa V, Ceccaroni M, et al. Epidemiology of infertility in women with endometriosis. Best Pract Res Clin Obstet Gynaecol. 2024;92:102454. doi:10.1016/j.bpobgyn.2023.102454
56. McGrath IM, Montgomery GW, Mortlock S. Insights from Mendelian randomization and genetic correlation analyses into the relationship between endometriosis and its comorbidities. Hum Reprod Update. 2023;29(5):655–674. doi:10.1093/humupd/dmad009
57. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. 2021;397(10276):839–852. doi:10.1016/S0140-6736(21)00389-5
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Causal Relationship Between Endometriosis and Pelvic Inflammatory Diseases: Mendelian Randomization Study
Liu K, Liu X, Cao T, Cui X, Sun P, Zhang L, Wu X
International Journal of Women's Health 2024, 16:727-735
Published Date: 24 April 2024
The Effect of Circulating Inflammatory Proteins on Endometriosis: A Mendelian Randomization Study
Wei Y, Zhao X, Li L
ImmunoTargets and Therapy 2024, 13:585-593
Published Date: 1 November 2024
Unveiling Potential Blood Markers for Endometriosis Through the Integration and Experimental Validation of Immune Cell Traits Genome and Genome-Wide Associated Data
Mei J, Jiang XY, Zhang B, Wang L, Zhang AX, Li JJ, Chen SX, Xu X, Hu JJ, Zhou SG
International Journal of Women's Health 2025, 17:845-853
Published Date: 19 March 2025
Endometriosis Severity and Risk of Preeclampsia: A Combined Mendelian Randomization and Observational Study
Zu Y, Xie Y, Zhang H, Chen L, Yan S, Wang Z, Fang Z, Lin S, Yan J
International Journal of Women's Health 2025, 17:923-935
Published Date: 27 March 2025