")
Back to Journals » Journal of Pain Research » Volume 18
Characterizing the Optimal Diversity Training Programs for Physicians: A Survey sponsored by Pacific Spine and Pain Society
Authors Gendreau JL, Bauman MMJ, Brown NJ, Alfonzo Horowitz M, Chakravarti S, Mehkri Y, Grovey B, Lee E, Lee G, Cornidez E, Bhandal HS, Pope JE
Received 31 January 2025
Accepted for publication 9 May 2025
Published 27 May 2025 Volume 2025:18 Pages 2739—2750
DOI https://doi.org/10.2147/JPR.S512263
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ryan D’Souza
Julian L Gendreau,1 Megan MJ Bauman,2 Nolan J Brown,3 Melanie Alfonzo Horowitz,4 Sachiv Chakravarti,5 Yusuf Mehkri,6 Brittany Grovey,7 Eric Lee,8 Gemayel Lee,7 Eric Cornidez,9 Harjot S Bhandal,10 Jason E Pope10
1Whiting School of Engineering, Johns Hopkins, Baltimore, MD, USA; 2School of Medicine, Mayo Clinic, Phoenix, AZ, USA; 3Department of Neurological Surgery, University of California, Irvine, CA, USA; 4Department of Neurological Surgery, Johns Hopkins, Baltimore, MD, USA; 5Johns Hopkins University, Baltimore, MD, USA; 6University of Florida School of Medicine, Gainesville, FL, USA; 7Relive You Center for Advanced Pain Management, San Diego, CA, USA; 8Miliani Pain Center, Miliani, HI, USA; 9Pain Institute of Southern Arizona, Tucson, AZ, USA; 10Evolve Restorative Center, Santa Rosa, CA, USA
Correspondence: Jason E Pope, Evolve Restorative Center, Santa Rosa, CA, USA, Tel +1 615-521-0777, Email [email protected]
Introduction: Recently, increasing research has shown inferior outcomes in patients with respect to specific social determinants of health. Therefore, optimizing diversity training given to pain management providers is imperative for physicians to provide culturally competent healthcare and to improve patient outcomes. In this paper, we attempt to describe trends in the Pacific Spine and Pain Society (PSPS) membership to help discover optimal diversity education paradigms for pain management providers by performing a survey on behalf PSPS.
Methods: A survey was disseminated to all members of the PSPS at the 2022 annual meeting. Opinions were solicited with respect to respondents’ demographics, diversity training type, diversity training timing, and how this correlates with a respondent’s self-reported confidence in navigating diversity issues in the workplace. Cronbach’s alpha test was used to rate internal consistency while logistic regression models were used for statistical analysis.
Results: Cronbach’s alpha produced a rating of 0.91. A total of 164 individuals responded to the survey, with 115 (70%) being male and 98 (60%) did not consider themselves to be under-represented in medicine. Survey respondents who obtained diversity training post-fellowship (p = 0.004) and with interactive training type (p = 0.010) self-reported to be more confident in handling matters of diversity in the workplace. Respondents who were underrepresented (p = 0.018), females (p = 0.033), practice in the west coast (p = 0.036), academic practice (p=0.031), and non-rural areas (p = 0.033) were also found to be more confident in handling matters of diversity.
Conclusion: Practitioners who received diversity training post-fellowship and with interactive and role model formats felt most confident to handle matters of diversity. Underrepresented groups, females, individuals from non-rural practices and individuals from academic practices appear to feel more confident in handling these issues.
Keywords: bias, competency, cultural training, diversity, education, medicine, survey, workforce
Introduction
Recently, increasing research has shown inferior outcomes demonstrating that racial, ethnic, and gender disparities can directly impact patient care and may ultimately result in negative short- and long-term health outcomes.1,2 Further, cultural differences between patients and physicians have been shown to affect treatment plan adherence, communication, and decision-making.3,4 Therefore, optimizing diversity training given to pain management providers is imperative for physicians to provide culturally competent healthcare and to improve patient outcomes.1 Even though there are a variety of diversity training platforms, there is no data to support whether one platform is more “successful” than the other in establishing either competence or confidence in addressing culturally sensitive clinical care. The variety of these programs makes it difficult to measure how effective they are in training providers on how to address cultural differences when treating patients from diverse backgrounds.
The general goal of diversity training is to promote awareness of cultural differences and improve overall delivery of culturally competent care. It is unclear, however, exactly how diversity training directly improves clinical care. Furthermore, it is important to understand what factors will lead to improved diversity training and consequently pain treatment outcomes. Several medical groups, including accrediting bodies such as the Liaison Committee of Medical Education (LCME) and Accredited Council of Graduate Medical Education (ACGME), have developed guidelines and criteria which necessitate that physicians and other medical professionals (including those in training) understand and deliver culturally competent and sensitive care.2,5 Despite having these requirements across all LCME accredited institutions, there remains a need to further optimize and establish the best diversity education paradigms for the purpose of improving the delivery of healthcare.5
Recent studies have suggested that implementing cultural competency and bias training allows health professional trainees and clinicians to identify and address implicit biases at earlier stages of training.3 These have the additional benefit of exploring principles for providing cross-cultural care to patients from diverse backgrounds4 While results from culturally competent curricula have demonstrated improved patient satisfaction, outcomes, and safety,3 the implementation of these courses remains inconsistent across educational organizations and institutions. In addition to this, there are no studies in the current literature that discuss what type of diversity training leads to more confidence in dealing with diversity related issues. Specific to pain management, there are no studies to date to discuss any diversity training impact on provider confidence in addressing diversity related issues.
Currently, medical schools, residency programs, and fellowships have discretion in implementing cultural competency and bias training. Given there is no current widely accepted consensus on when to deliver diversity training throughout multiple education institutions, our organization sought to identify a) which types of formal training in cultural competency leads to increased confidence in addressing diversity issues in the workplace and b) to determine at which timeframe these education trainings lead to increased confidence in addressing diversity issues in the workplace. Secondary objectives include measuring whether being from an underrepresented cohort in medicine, sex, geographic location of practice, academic practice and rural practice type correlated with increased confidence in addressing diversity issues.
To do this, we surveyed health care providers that have attended an event, via the registration information, sponsored by Pacific Spine & Pain Society (PSPS) - a regional medical society open to all health care professionals and comprised mainly of pain management physicians, physiatrists, orthopedic spine surgeons, and neurosurgeons - to address these questions in the setting of a multidisciplinary healthcare workforce. To our knowledge, this investigation represents the first of its kind to identify disparities related to the formal bias training that providers in a multidisciplinary team receive, as well as gauge their level of comfort associated with identifying and addressing bias in the workplace.
Methods
Survey Dissemination
A survey was generated and administered to those health care professionals that have registered for a PSPS event. PSPS membership represents a diverse medical professional group, including pain management, anesthesiology, physiatry, psychiatry, neurology, advanced practice providers (nurse practitioners and physician assistants), orthopedic surgery, and neurosurgery. The survey was distributed electronically to registrants of a PSPS event (webinar or in person), including those that were gathered at the 2022 Annual Meeting of PSPS on September 2022 using Google Surveys (Google, Mountain View, CA) (Table 1). The survey was electronically disseminated and completed in the time period from March 1 – June 1, 2021. After, respondents had the option to complete the survey in person at the annual meeting. This 38-question survey asked respondents basic demographical identifiers, type of diversity education received, timing of diversity education received and to rate their level of confidence pertaining to addressing diversity issues in the workplace. This study received IRB exemption from the WCG IRB (Puyallup, WA, IRB: 1–1,394,931-1).
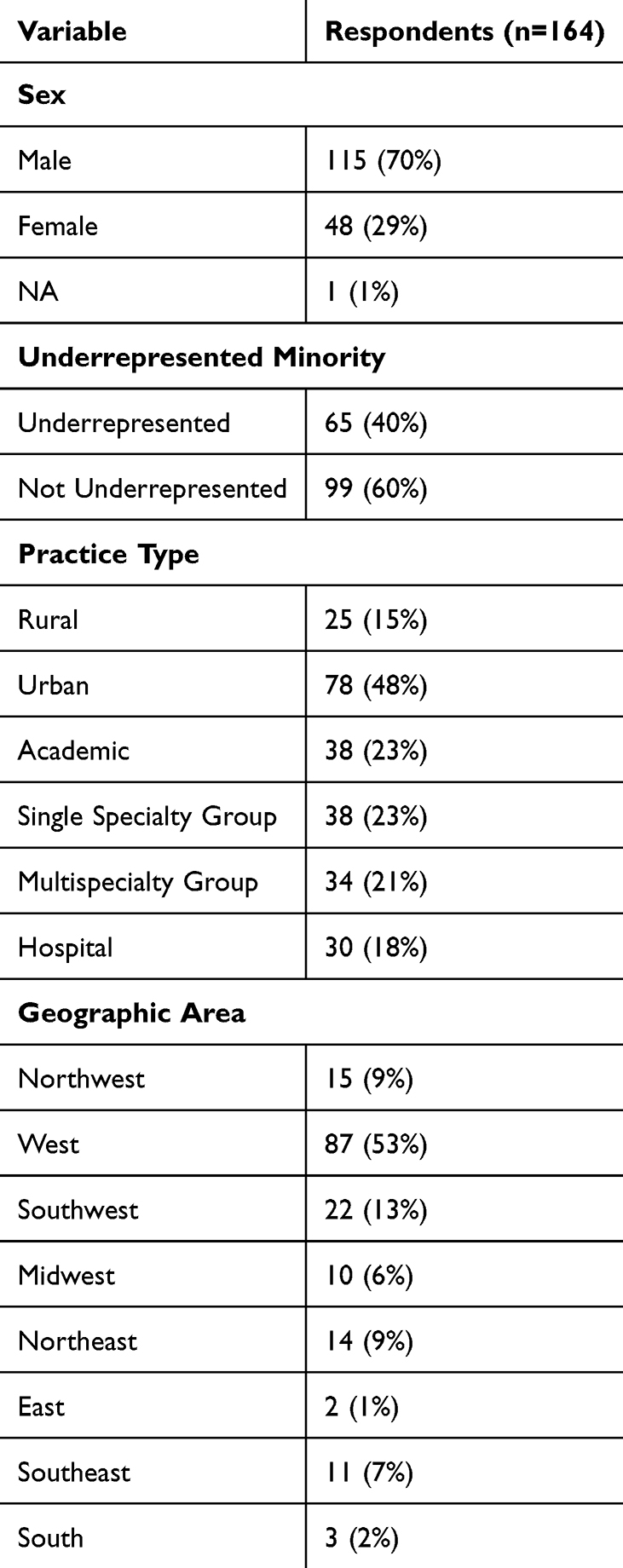 |
Table 1 Demographics of Respondents |
Statistical Analyses
All data was exported to Microsoft Excel Version 2019 (Redmond, Washington, USA) and tabulated. All statistical analyses were performed using R software (R Core Development Team, Vienna, Austria). Cronbach’s alpha assessment was used to rate internal consistency. Ratings of confidence in different scenarios were assessed using a Likert scale of 1–5 being from “not confident at all” to “very confident”. Average Likert scale scores were calculated for each question 7–31. These scalable measures were statistically assessed using bivariate and multivariate general logistic models. A threshold of p≤0.05 was used to establish statistical significance. Any individual that had missing variables was removed from all statistical analyses.
Qualitative Analyses
To address free-response comments, inductive thematic analysis was performed utilizing the top three most suggested themes exhibited in the free-response portion of the survey. Number of comments addressing each theme were tabulated.
Results
Initially, the survey was solicited to 164 total individuals, and 164 responses were received for the initial categorical analysis. After exclusion of missing variables for testing of internal consistency and logistic regression, only 120 remained for final statistical analysis. Table 2 lists the average Likert scale score for each question item 7–31.
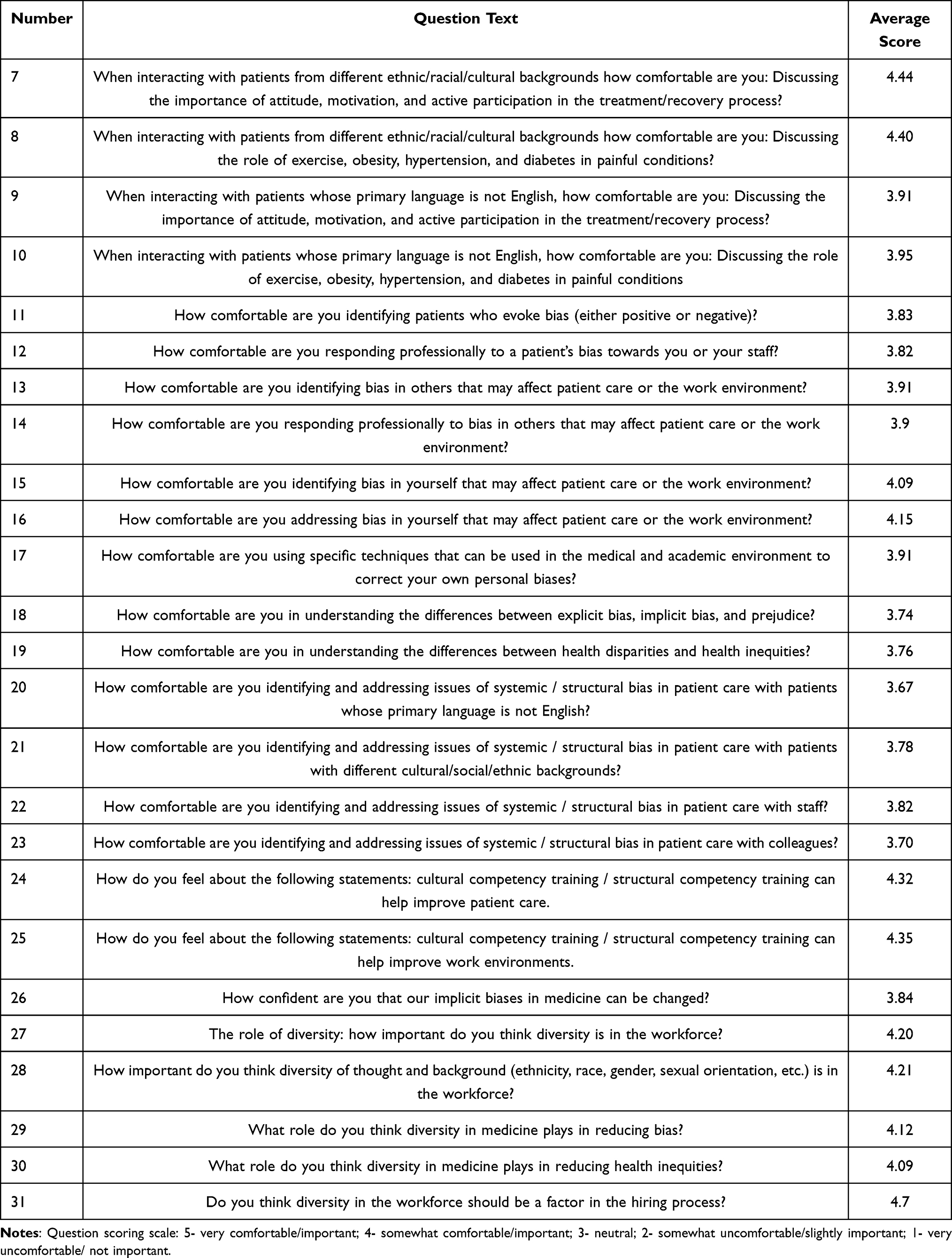 |
Table 2 Average Likert Scale Scores for Survey Questions 7–31 |
Demographics (Questions 1-4)
A total of 115 identified as male (70%; Table 1). Most respondents (99; 60%) did not consider themselves to be under-represented in medicine (in terms of gender, ethnicity, sexual orientation). Most (78; 48%) practiced in urban locations, 38 (23%) were involved in academic medicine and 30 (18%) reported that they were primarily hospital affiliated. Most respondents reported belonging to a single specialty group (38; 40%). With respect to geographical region, most providers were practiced in the west geographical location (87; 53%). The regions with lowest representation were the east (2; 1%).
Formal Education (Questions 5-6)
With respect to educational experience of participants, 76% reported having some formal education in understanding and minimizing bias. Formal training occurred in medical school for 38% of respondents, while 21% and 14% claimed to have received such training in post-fellowship training and residency, respectively. It should be noted that post-fellowship training was non-specific which could include CME courses, self-directed learning, or institutional programs in the workplace. Twenty-three (24%) reported that they had never received education in understanding and minimizing bias (Table 3).
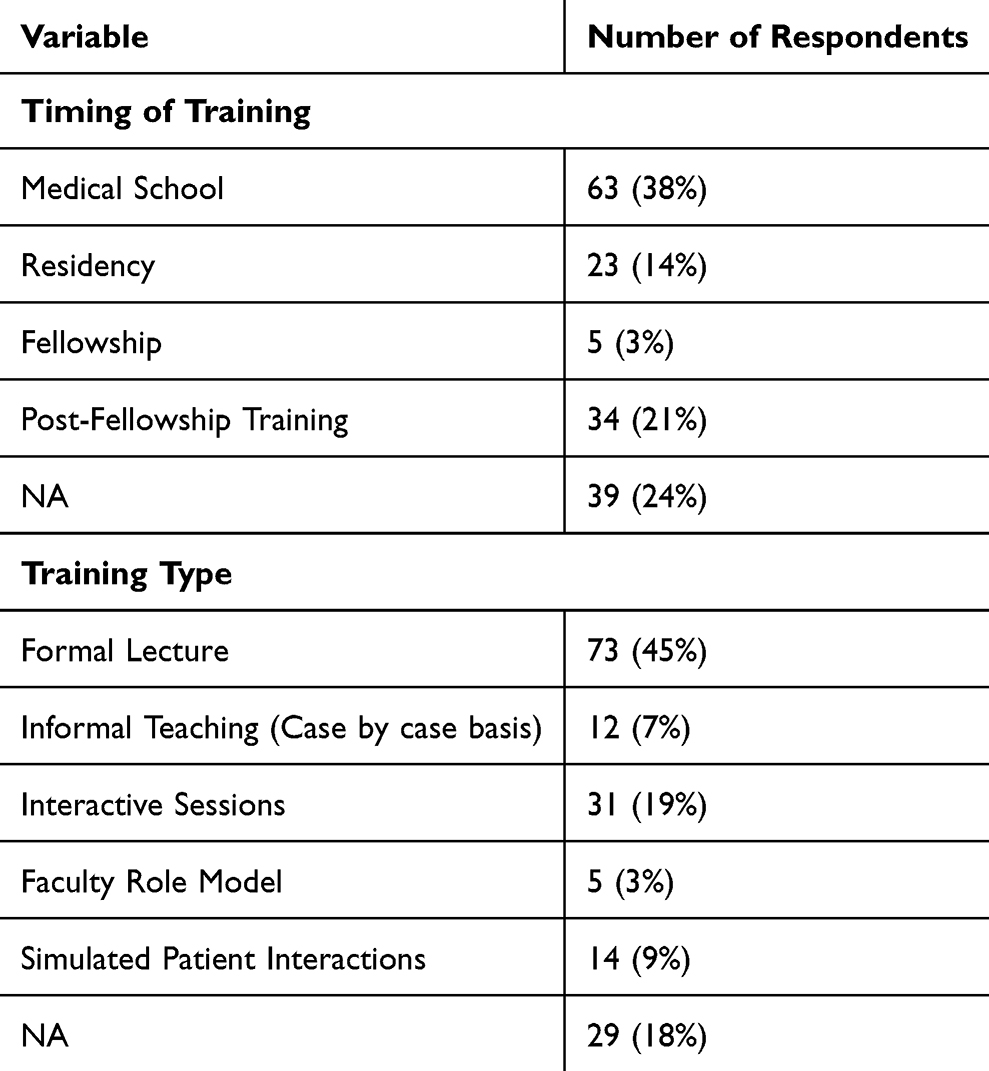 |
Table 3 Characteristics of Training Programs Reported by Respondents |
Most respondents identified formal lectures (44%) representing the methodology of education, while 27.4% received formal interactive sessions with cultural and diversity experts or simulated patient interactions. Informal teaching and role modeling occurred 10.37% of the time, of note, nearly 18% did not have any.
Comfortability of Interactions (Questions 7-10)
Most respondents were comfortable discussing active participation, motivation, attitude, in the treatment plan for those with diverse ethnic/racial/cultural backgrounds: 87.2% indicated they were very or somewhat comfortable, and 1.22% (2) respondents indicated they were somewhat uncomfortable No respondent indicated they were very uncomfortable In the discussion on the role of exercise, obesity, hypertension, diabetes in painful conditions, 88.42% were very comfortable or somewhat comfortable Only 6 (3.66%) indicated they were very or somewhat uncomfortable with the interaction. Regarding those responses with the influence of non-English as a primary language on discussing attitude, motivation, and active participation in treatment, 71.34% were very or somewhat comfortable, while 11.59% (19) were somewhat or very uncomfortable Regarding the influence of non-English as a primary language on the discussion of role of exercise, obesity, hypertension, and diabetes on painful conditions, 75% were very or somewhat comfortable, while 18 (10.98%) were very or somewhat uncomfortable.
Comfortability of Bias (11-16)
Concerning comfort level with the identification of patients that evoke bias, the weighted average demonstrated that more respondents were somewhat comfortable or very comfortable Regarding the comfort level of responding professionally to a patient’s bias towards the provider or the staff, 71.95% indicated that they were somewhat or very comfortable, while approximately 16% were somewhat uncomfortable or very uncomfortable Regarding the comfortability in identifying bias in others that may affect patient care or the work environment, 73.17% were comfortable, as compared to 9.15% that identified as uncomfortable. The same proportion represented how comfortable they were in responding to the identification of such bias. With regard to identification of bias within themselves that may affect patient care or the work environment, 78.66% felt somewhat comfortable or very comfortable, while only 3.66% were uncomfortable and none were very uncomfortable Regarding addressing such a bias within themselves, 82.31% were comfortable, 6.10% were somewhat uncomfortable, and none were very uncomfortable Table 2 lists the average Likert Scale score depicting provider comfort level for these questions included in the survey.
Techniques and Recognition (17-19)
Regarding the comfort of using specific techniques to correct personal bias in the medical and academic work environment, 68.90% were somewhat comfortable or very comfortable, while 6.71% were somewhat or very uncomfortable Regarding the understanding of the difference between explicit bias, implicit bias, and prejudice, 65% were comfortable, while 12.81% were uncomfortable Regarding the comfort of knowing the difference between health disparities and health inequities, 65.85% were comfortable, while only 10.37% were uncomfortable.
Addressing Issues (20-23)
Regarding comfort in addressing systemic/structural bias in patient care in patients where English is not the primary language, 60.36% were comfortable, while 11.59% were not comfortable Comfortability of addressing systemic and structural bias in patient care with different cultural/social/ethnic backgrounds, 66.46% were very or somewhat comfortable, while 6.71% were somewhat or very uncomfortable. Regarding addressing systemic or structural bias with staff, no one reported being very unformattable, while. 67.07% were very or somewhat comfortable. In addressing systemic or structural bias with a colleague, no one reported being very uncomfortable, while 65.24% reported being very or somewhat comfortable.
General Feelings (24-25)
Of those surveyed, the respondents felt that cultural competency training/structural competency training can help improve patient care was highly rated at 85.98%, while 1.22% strongly disagreed. Regarding work environment improvement, 86.59% agreed, while 2.44% disagreed and 1.22% strongly disagreed.
Confidence of Change (26)
Regarding confidence of positive change if training is implemented for implicit bias, 70.73% were confident and 10.37% were somewhat doubtful or very doubtful.
Diversity (27-31)
Importance of diversity in the work force was assessed, and 92.68% of respondents thought it was very important, important, or moderately important, while 3.05% indicated in was not important. Regarding diversity of thought and background in the workforce, 90.25% indicated it was very important, important, or moderately important, while 2.44% indicated it was not important. 90.85% of the respondents indicated that diversity in medicine plays a very important, important or moderate important role in reducing bias, while 3.05% indicated it was not important. 89.02% of the respondents felt diversity plays an important role in reducing health inequities, while 3.05% indicated it was not important. 85.36% felt diversity should play a role in the hiring process, while. 14.63% indicated it is not a factor. Table 4 provides a complete annotation of responses for each question of the survey.
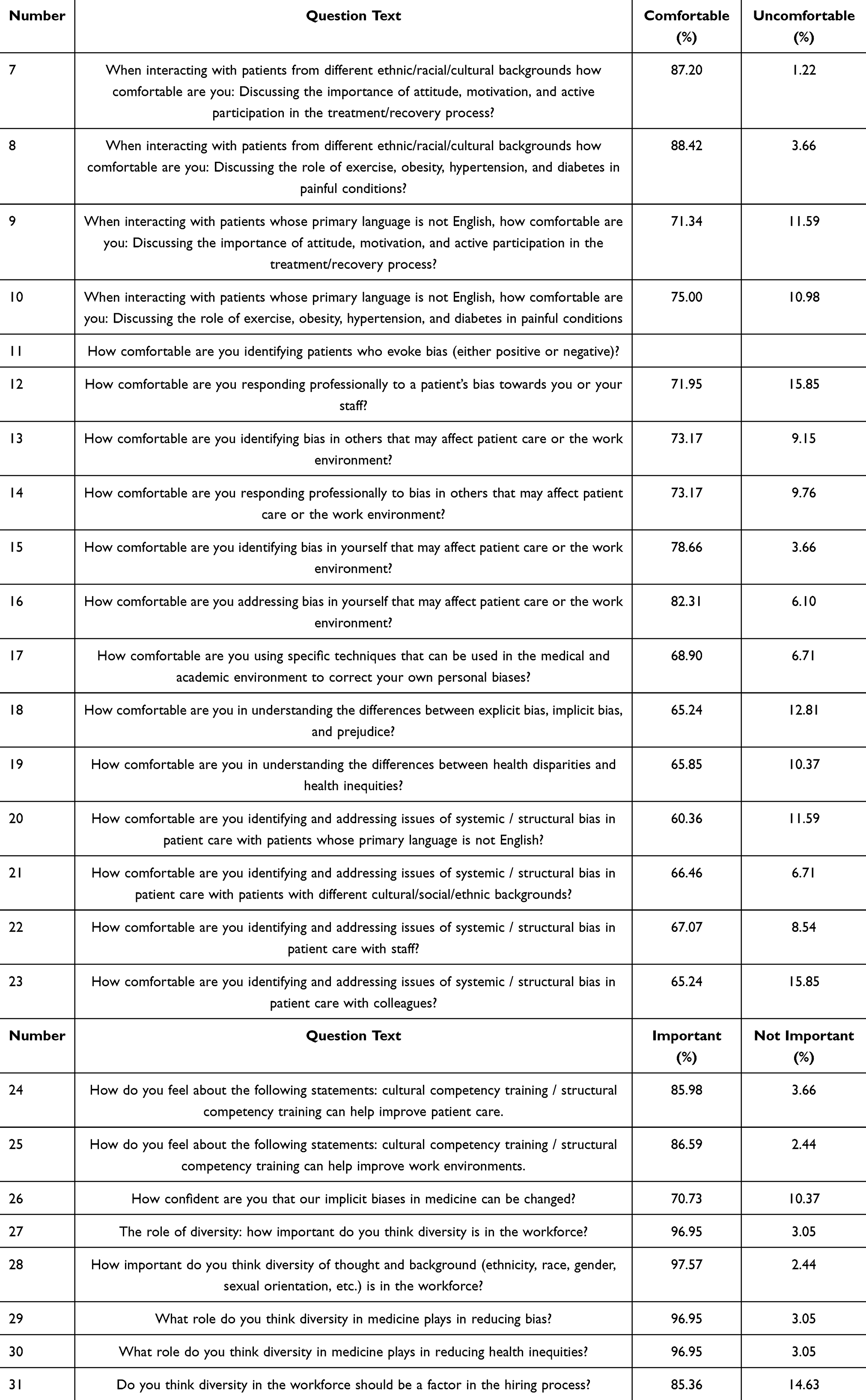 |
Table 4 Response Percentages for Survey Questions 7–31 |
Internal Consistency
Of the total respondents, a Cronbach’s alpha score of 0.91 was generated, which is considered excellent.6
Timing of Diversity Training
Providers who had diversity training in post fellowship training category were overall more comfortable with identifying and addressing bias in the work environment (p = 0.004). Post fellowship training applicants were also better at identifying and addressing issues in systemic and structural bias (p = 0.004) when compared to other training categories.
Type of Diversity Training
Providers that listed their diversity training as primarily stemming from emulating role models were more comfortable with interacting with patients from different ethnic/racial and cultural backgrounds (p = 0.0161) when compared to all other types of training. Providers who listed their diversity training as interactive were more confident in being able to use specific techniques to correct their own personal bias (p = 0.010) when compared to all other types of training.
Reported Underrepresented of Respondent
Providers who identified as underrepresented had increased scores in believing that competency training can help improve work environments (p = 0.018) when compared to respondents that did not identify as underrepresented.
Sex of Respondent
Providers with female sex had a higher likelihood of reporting that cultural competency training can improve patient care (p = 0.033), that implicit biases can be changed (p = 0.0150) and that diversity is important in the workforce (p = 0.035) when compared to males.
Geographic Location
Respondents with Eastern geographic locations had decreased scores on being able to identify bias in the work environment (p = 0.036), understanding differences in health disparities (p < 0.005), identifying issues in systemic bias (p < 0.025), detecting bias in work staff (p < 0.001) and identifying bias in colleagues (p < 0.001).
Rural Respondents
Respondents self-identifying in rural locations reported decreased confidence in having specific techniques to correct personal biases (p = 0.033), decreased confidence that implicit biases in medicine can be changed (p < 0.041) and decreased belief that diversity is important in the workforce (p < 0.048).
Academic Location
Respondents identifying in practicing at an academic practice had increased scores in being comfortable responding to bias in the workplace (p = 0.031), identifying and addressing systemic bias in patient care (p = 0.031), believing that cultural competency training is valuable (p = 0.007), believing that diversity is important (p = 0.039), believing that diversity reduces bias (p = 0.047) and believing that diversity improves healthcare (p=0.029).
Qualitative Responses
In total, 30 (18%) free-response comments were received of the total 164 surveys received.
Theme 1 (7 Responses)
Recognizing issues with diversity is a way to increase the functionality of the organization. It was a predominant theme that identifying diversity in the workplace and addressing these issues can improve patient care and outcomes. One respondent reported: “Diversity and inclusion efforts are mandatory to ensure a positive work environment for all particularly in the health arena”.
Theme 2 (3 Responses)
Hiring processes should focus on the most capable candidates and not solely on diversity issues. There was a large theme of individuals arguing that hiring endeavors should not consider diversity in its application, but a blinded process that only considers the applicants academic achievements. As one respondent replied:
In regard to several of these questions, I do believe diversity of thought and background are important to a well-balanced team. I believe that these diversities would help reduce bias as collective experiences could be helpful for improved understanding of others. However, I would not choose someone for being different over being qualified thus several of my answers are more moderate than the more extreme choices.
Additionally, another respondent quoted:
I look to hire the most competent person for the job, and train the appropriate skills needed to succeed in that role.
Theme 3 (3 Responses)
Addressing diversity would improve patient outcomes; however, making these changes is a difficult task overall. Many respondents agreed that diversity issues should be addressed, however it is often difficult to address often because of leader ideology and views. As one respondent reports:
It’s hard to change the culture of the work environment if the boss or leaders have strongly biased and political views. It’s hard to change culture if the boss is not agreeable and makes politically charged comments on a frequent basis.
An additional respondent also reports:
…Although I strongly support addressing, learning, teaching, and incorporating issues regarding cultural competency, racism, implicit and explicit bias, and prejudices in the healthcare arena, I am uncertain that addressing these issues without a complete structural and cultural overhaul of the healthcare system (and really the American way of life) will make any significant improvements in the overall outcomes in healthcare in America.
Sexual diversity also appears to be a difficult challenge to address as one respondent reports: “I have difficulty with addressing sexual diversity”. Finally, a respondent notes: “I would like to know of concrete suggestions to overcome diversity beyond recognizing this”.
Discussion
PSPS is a multidisciplinary group of specialists inclusive of multiple medical disciplines that diagnose, manage, and treat painful disorders related to the spine. Additionally, the society aims to enhance patient care and embrace innovation by facilitating collaboration amongst surgical and interventional pain specialists. Given open access to PSPS membership, we feel that the membership gives a fair and accurate representation of the interventional pain management specialist space. In surveying the members of the PSPS, this study found that those who received diversity training post-fellowship feel most qualified to handle diversity issues in the workplace. Further investigation in establishing specifically what type of formal post-fellowship training leads to more confidence in addressing these issues is warranted.
Additionally, we found that individuals receiving diversity training by emulating role models, who demonstrate key attributes such as empathy, cultural awareness, and effective communication, and through an interactive format, feel more confident in addressing diversity issues than those receiving more formal training. Institutional support may occur in the form of availability of ongoing resources, such as continuous access to diverse role models, funding for training initiatives, and policies that promote diversity education as part of professional development. In institutions with strong leadership commitment to diversity, interactive training formats may be more supported and maintained, leading to long-term improvements in confidence among participants. It is uncertain how proactive those surveyed were in seeking out these opportunities, and follow-up regarding this may be beneficial.
When addressing diversity education at the post-fellowship timeframe, efforts have been made to identify physician and faculty bias and to ensure that culturally competent care is provided. There has been an increased focus on establishing a curriculum for faculty educators to prevent faculty from bringing their implicit biases into the educational setting.7 Unfortunately, it has been found that often time constraints of medical professionals and resources can limit the effectiveness and availability of these interventions.8 Thus, training is often limited to education scenarios that are often short and in didactic formats. This is the opposite of what our study finds would be most beneficial. Even though these formats are not most optimal, these may be better than offering no didactic training at all, as Gonzalez et al demonstrate that even a single grand rounds seminar in implicit bias resulted in significantly increased comfort in addressing bias in medicine.9 Despite physicians’ busy schedules, this study shows that even small efforts and short interventions can still result in a noticeable difference.
Interestingly, even though our responses show that post-fellowship training leads to more confidence in addressing diversity issues, it appears that much effort has been made to deliver education training early within one’s medical training. In a survey study by Morris et al, 51% of respondents reported receiving formal implicit bias training during medical school.10 Post-fellowship training could be more effective since it is in more recent memory of the provider. It is also administered when the provider may have had more time to learn from the training when compared to another individual that has taken the training in a residency training environment.
Furthermore, many of these endeavors utilize formal training which is the opposite of what our survey suggests would be most ideal, at least in establishing confidence to address culturally sensitive issues. Medical schools have explored the implementation of standalone didactic sessions and longitudinal curricula aimed at increasing cultural awareness and highlighting injustices/biases that affect underrepresented individuals.11 In a survey of 15 medical schools by Williams et al, the most effective methods of increasing education about bias included longitudinal sessions.12 With respect to residency level education, among ophthalmology programs, most programs instituted efforts to recruit underrepresented minorities into their programs.13 However, only about half of these programs were shown to have formal diversity education.13 Schools may currently face barriers in implementing this programs, such as time constraint for training programs and additionally potential institutional resistance to changing curricula.
Additional statistical results of our study suggests that patients who are male, from eastern geographic locations, from rural practices, and from non-academic practices are also least confident in handling diversity issues. This may be because providers from practices in these regions are in areas with homogenous populations and less exposure to diverse sets of patients, thus limiting the development of skills necessary to address diversity issues. These groups of providers could be most concentrated for increasing diversity awareness. Even though this survey was given only to PSPS members, the authors feel that its membership is an acceptable representation of the pain management, physiatry, and spine surgery healthcare populations. It should be noted, however, that there may be a sampling bias given that this survey was given to only PSPS members. Further studies in other medical societies or the general healthcare workforce would be beneficial.
Finally, thematic analysis of free-response comments suggest that many individuals agree diversity education would result in overall better healthcare with improved patient outcomes. There is a significant proportion of pain physicians that believe candidates should be recruited irrespective of any diversity identifiers and should be acquired purely with credentials and past academic qualifications. A point that is in wide discussion in the medical diversity literature.
A final subgroup believes addressing diversity issues is necessary but is difficult due to the systemic processes that occur in the healthcare environment.
Limitations
We acknowledge a few limitations in our study. First, the survey was only sent to members of PSPS, which may limit the generalizability of our results. Second, our study could represent selection bias as individuals more interested in diversity issues are more likely to respond to the survey. Third, those from underrepresented background may have less access to educational events such as the PSPS annual meeting. Fourth, some sections of the survey only contained one question, limiting the ability to draw conclusions on that category. Fifth, we were unable to fully describe characteristics of survey non-responders. Lastly, since this study was survey-based, we are only able to draw correlations, but not causation.
Conclusion
Pain specialists PSPS members that receive diversity training post-fellowship and through interactive and role model format appear most confident in addressing diversity workplace issues. Further studies should investigate further to determine why they feel more confident. In addition to this, determining what type of training would be beneficial. Overall, most pain physicians agree addressing diversity issues in the workplace will improve patient outcomes.
Ethics Statement
The Institutional Review Board of WCG IRB granted an exemption for the current study, informed consent was also exempted under 45 CFR § 46.104(d)(2)i-iii. The guidelines outlined in the Declaration of Helsinki were followed.
Funding
The Pacific Spine and Pain Society provided an unrestricted educational grant to support the study.
Disclosure
Dr. Eric Cornidez reports personal fees from NALU MedicL, NEVRO, Saluda Medical, and Boston Scientific, outside the submitted work. Dr. Harjot Bhandal is a consultant for Saluda Medical, Abbott, and Biotronik, outside the submitted work. Dr. Jason Pope is the chairman for PSPS, serves as a consultant for Abbott, Medtronic, Saluda, Flowonix, SpineThera, PainTEQ, Vertos, Vertiflex, SPR Therapeutics, Tersera, Aurora Spine, Spark, Ethos, Biotronik, Mainstay, WISE, Boston Scientific, Thermaquil; has received grant and research support from: Abbott, Flowonix, Saluda, Aurora Spine, PainTEQ, Ethos, Muse, Boston Scientific, SPR Therapeutics, Mainstay, Vertos, AIS, Thermaquil; and is a shareholder of: PainTEQ, Vertos, SPR Therapeutics, Aurora Spine, Spark, Celeri Health, Neural Integrative Solutions, Pacific Research Institute, Thermaquil and Anesthetic Gas Reclamation. The authors report no other conflicts of interest in this work.
References
1. Jhutti-Johal J. Understanding and coping with diversity in healthcare. Health Care Anal. 2013;21(3):259–270. doi:10.1007/s10728-013-0249-0
2. Walsh RM, Jeyarajah DR, Matthews JB, et al. White paper: SSAT commitment to workforce diversity and healthcare disparities. J Gastrointest Surg. 2016;20(5):879–884. doi:10.1007/s11605-016-3107-1
3. Deliz JR, Fears FF, Jones KE, Tobat J, Char D, Ross WR. Cultural competency interventions during medical school: a scoping review and narrative synthesis. J Gen Intern Med. 2020;35(2):568–577. doi:10.1007/s11606-019-05417-5
4. Benoit LJ, Travis C, Swan Sein A, et al. Toward a bias-free and inclusive medical curriculum: development and implementation of student-initiated guidelines and monitoring mechanisms at one institution. Acad Med. 2020;95(12S):S145–S149. PMID: 32889934. doi:10.1097/ACM.0000000000003701
5. Barzansky B, Hash RB, Catanese V, Waechter D. What is the role of accreditation in achieving medical school diversity? AMA J Ethics. 2021;23(12):E946–E952. doi:10.1001/amajethics.2021.94
6. Mihas P. Qualitative research methods: approaches to qualitative data analysis. Tierney RJ, Rizvi F, Ercikan K, editors. International Encyclopedia of Education
7. Gonzalez CM, Garba RJ, Liguori A, et al. How to make or break implicit bias instruction: implications for curriculum development. Acad Med. 2018;93(11S):S74–S81. PMID: 30365433; PMCID: PMC6211195. doi:10.1097/ACM.0000000000002386
8. Gleicher ST, Chalmiers MA, Aiyanyor B, et al. Confronting implicit bias toward patients: a scoping review of post-graduate physician curricula. BMC Med Educ. 2022;22(1):696. PMID: 36175856; PMCID: PMC9520104. doi:10.1186/s12909-022-03720-0
9. Rodriguez N, Kintzer E, List J, et al. Implicit bias recognition and management: tailored instruction for faculty. J Natl Med Assoc. 2021;113(5):566–575. PMID: 34140145; PMCID: PMC8556183. doi:10.1016/j.jnma.2021.05.003
10. Morris MC, Cooper RL, Ramesh A, et al. Preparing medical students to address the needs of vulnerable patient populations: implicit bias training in US medical schools. Med Sci Educ. 2020;30(1):123–127. PMID: 34457650; PMCID: PMC8368413. doi:10.1007/s40670-020-00930-3
11. Berman MI, Hegel MT. Weight bias education for medical school faculty: workshop and assessment. J Nutr Educ Behav. 2017;49(7):605–606.e1. PMID: 28689615. doi:10.1016/j.jneb.2017.05.337
12. Williams RL, Romney C, Kano M, et al. Racial, gender, and socioeconomic status bias in senior medical student clinical decision-making: a national survey. J Gen Intern Med. 2015;30(6):758–767. PMID: 25623298; PMCID: PMC4441663. doi:10.1007/s11606-014-3168-3
13. Aguwa UT, Wang J, Woreta F, et al. Residency program diversity recruitment and education: survey of efforts and barriers to implementation. J Surg Educ. 2022;79(3):595–605. PMID: 34952819; PMCID: PMC9064934. doi:10.1016/j.jsurg.2021.11.016
14. Mensah MO, Sommers BD. The policy argument for healthcare workforce diversity. J Gen Intern Med. 2016;31(11):1369–1372. PMID: 27431386; PMCID: PMC5071285. doi:10.1007/s11606-016-3784-1
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.