")
Back to Journals » Infection and Drug Resistance » Volume 18
Clinical Characteristics and Prognostic Factors of Severe COVID-19
Authors Yang Y , Huang Z, Pei Y, Huang Y, Chen C, Zhou T
Received 21 March 2025
Accepted for publication 12 June 2025
Published 25 June 2025 Volume 2025:18 Pages 3117—3125
DOI https://doi.org/10.2147/IDR.S525970
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Yun Yang,* Ziyi Huang,* Yongjian Pei, Yongkang Huang, Chen Chen, Tong Zhou
Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Soochow University, Suzhou, Jiangsu, 215004, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Tong Zhou, Department of Respiratory and Critical Care Medicine, The Second Affiliated Hospital of Soochow University, 1055 San Xiang Road, Suzhou, Jiangsu, 215004, People’s Republic of China, Email [email protected]
Purpose: Coronavirus disease-2019 (COVID-19) has high mortality and has caused heavy economic burden worldwide. In this study, we investigated the clinical characteristic and prognostic factors of patients with severe COVID-19. We aimed to identify the severe cases in early stages to improve the prognosis and mortality.
Patients and Methods: We collected the clinical data of 98 patients with severe COVID-19, who were admitted to the Second Affiliated Hospital of Soochow University (Jiangsu, China) from December 2022 to November 2023. The patients were divided into two groups, namely survivors and non-survivors, based on the outcomes of hospitalization. The risk factors affecting the prognosis of severe COVID-19 patients were identified by univariate analysis and multivariate logistic regression analysis. The predictive value of the individual and combined risk factors for the prognosis of severe COVID-19 was evaluated by the area under the receiver operating characteristic curve (AUROC).
Results: Compared with survivors, non-survivors had higher white blood cell (WBC) count, neutrophil count, Acute Physiology and Chronic Health Evaluation II (APACHE II) score, and platelet (PLT) count. Moreover, non-survivors exhibited a higher propensity to develop acute kidney injury (AKI) and receive mechanical ventilation (MV) and continuous renal replacement therapy (CRRT). Multivariate logistic regression analysis showed that WBC count, PLT count, APACHE II score, and MV were independent risk factors affecting the prognosis of severe COVID-19 patients, with AUC values of 0.807, 0.690, 0.761, and 0.751, respectively. The AUC of the combined risk factors was 0.897.
Conclusion: WBC count, PLT count, APACHE II score, and MV were independent risk factors for the poor prognosis of severe COVID-19 patients. High WBC count, PLT count, and APACHE II score, as well as the use of MV, showed good predictive value for the mortality of severe COVID-19 cases, especially when combined.
Keywords: COVID-19, white blood cell, platelet count, APACHE II score, mechanical ventilation
Introduction
In December 2019, a large number of people contracted unexplained pneumonia in Wuhan, China.1 Patients exhibited fever, cough, and myalgia or fatigue during the disease onset. Due to the lack of specific treatment options in the early stages, an increasing number of similar cases were identified in China and across the world, with some patients rapidly developing dyspnea or even acute respiratory distress syndrome (ARDS). Deep sequencing analysis from the lower respiratory tract samples of the patients led to the identification of a novel coronavirus.2 In February 2022, the World Health Organization (WHO) coined the term “COVID-19” for the pneumonia caused by the novel coronavirus. Based on the severity of the disease, COVID-19 could be classified as mild (laboratory confirmed, without pneumonia), moderate (laboratory confirmed and with pneumonia), severe, and critical (respiratory failure requiring mechanical ventilation, shock, or other organ failure that requires intensive care).3 Severe COVID-19 patients had poor prognosis and high mortality rates, which imposed a heavy burden on the global healthcare systems and economy.4 Previous studies had discovered partial clinical and laboratory characteristics which were associated with mortality in COVID-19. WBC count, neutrophil count, PLT count, APACHE II score, AKI and the use of MV and CRRT are associated with COVID-19.5–11 However, not enough studies discovered the predictive value of WBC count, PLT count, APACHE II score and the use of MV in severe COVID-19 and the combined diagnostic value of these four risk factors has not yet been reported. Therefore, in this study, we analyzed the clinical characteristics and prognostic risk factors of severe COVID-19 to improve our understanding of severe COVID-19 and to develop effective treatments to prevent and minimize its progression.
Materials and Methods
Study Design and Patients
We retrospectively analyzed 98 adult patients diagnosed with severe COVID-19, who were admitted to the Second Affiliated Hospital of Soochow University (Jiangsu, China) between December 2022 to November 2023. According to the guidelines provided by the China National Health Commission,12 COVID-19 diagnosis was based on the results of real-time reverse transcription–polymerase chain reaction (RT-PCR) test. Patients were considered to have severe COVID-19 if they satisfied any of the following criteria: (a) exhibited respiratory distress (respiratory rate ≥ 30 beats/min); (b) had ≤ 93% mean oxygen saturation in the resting state; (c) had a ≤ 300 mmHg (1 mmHg = 0.133 kPa) ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen (PaO2/FiO2); (d) exhibited respiratory failure and required mechanical ventilation (MV); (e) exhibited shock; (f) exhibited organ dysfunction and required ICU admission.
Data Collection
The following data was collected for each patient: age, body mass index (BMI), gender, chronic medical histories (hypertension, diabetes, cardiovascular disease, chronic obstructive pulmonary disease [COPD], malignancy, chronic kidney disease, neurological disease, immune system disease, and long-term glucocorticoid administration), symptoms from onset to hospital admission (fever, cough, hemoptysis, chest tightness, and chest pain), laboratory values on admission (white blood cells [WBC] count, neutrophil count, platelet [PLT] count, PaO2/FiO2, lactate dehydrogenase [LDH] level, D-dimer level, C-reactive protein [CRP] concentration, interleukin-6 [IL-6] level, procalcitonin [PCT] concentration, brain natriuretic peptide [BNP] level, and APACHE II score), comorbidities (acute kidney injury [AKI], liver dysfunction, Aspergillus infection, and hypoalbuminemia), and treatments (mechanical ventilation [MV], continuous renal replacement therapy [CRRT], antiviral treatment, antifungal treatment, glucocorticoid treatment, sivelestat sodium treatment, and tocilizumab treatment). This study was granted ethical approval (JD-LK2023025-I01) by the Ethics Committee of the Second Affiliated Hospital of Soochow University. Informed consent was obtained by all living patients. For patients who died, informed consent was obtained from a family member.
Statistical Analysis
Statistical analysis was performed using the SPSS v26 software (SPSS, Inc., Chicago, IL, USA). Normally distributed measurement data were presented as the mean ± standard deviation and compared using the independent samples t test; otherwise, the data were presented as the median and interquartile range and Wilcoxon rank sum test was used. Count data were presented as n or n (%) and compared using the Chi-squared (χ2) test or Fisher’s exact test. The independent risk factors influencing the adverse outcomes of severe COVID-19 patients were analyzed using the multivariate logistic regression analysis. MedCalc was used to draw the receiver operating characteristic (ROC) curves to evaluate the predictive value of the risk factors. The P value < 0.05 was considered statistically significant.
Results
Patient Characteristics
Of the 98 patients included in the study, 27 had died. The survivor and non-survivor groups showed no significant difference in age, BMI, gender, underlying disease, long-term glucocorticoid administration, neutrophil count, PaO2/FiO2, LDH level, CRP concentration, D-dimer level, IL-6 level, PCT concentration, and BNP level (P > 0.05; Tables 1 and 2). However, the survivor and non-survivor groups showed a significant difference in the WBC count, PLT count, and APACHE II score (P < 0.05; Table 2). AKI was more common in non-survivors than in survivors (P < 0.05). Moreover, compared to survivors, non-survivors were more likely to receive MV and CRRT (P < 0.05). The glucocorticoid dose for the initial 10 d was generally higher for non-survivors compared to survivors, although the difference was not statistically significant (P > 0.05). Furthermore, the survivor and non-survivor groups showed no significant difference in symptoms (fever, cough, hemoptysis, and chest pain), comorbidities (liver dysfunction, Aspergillus infection, and hypoalbuminemia), and treatments (antiviral, antifungal, sivelestat sodium, and tocilizumab treatments) (P > 0.05; Table 3).
 |
Table 1 Demographic and Baseline Characteristics of Severe COVID-19 Patients |
 |
Table 2 Laboratory Values of Severe COVID-19 Patients |
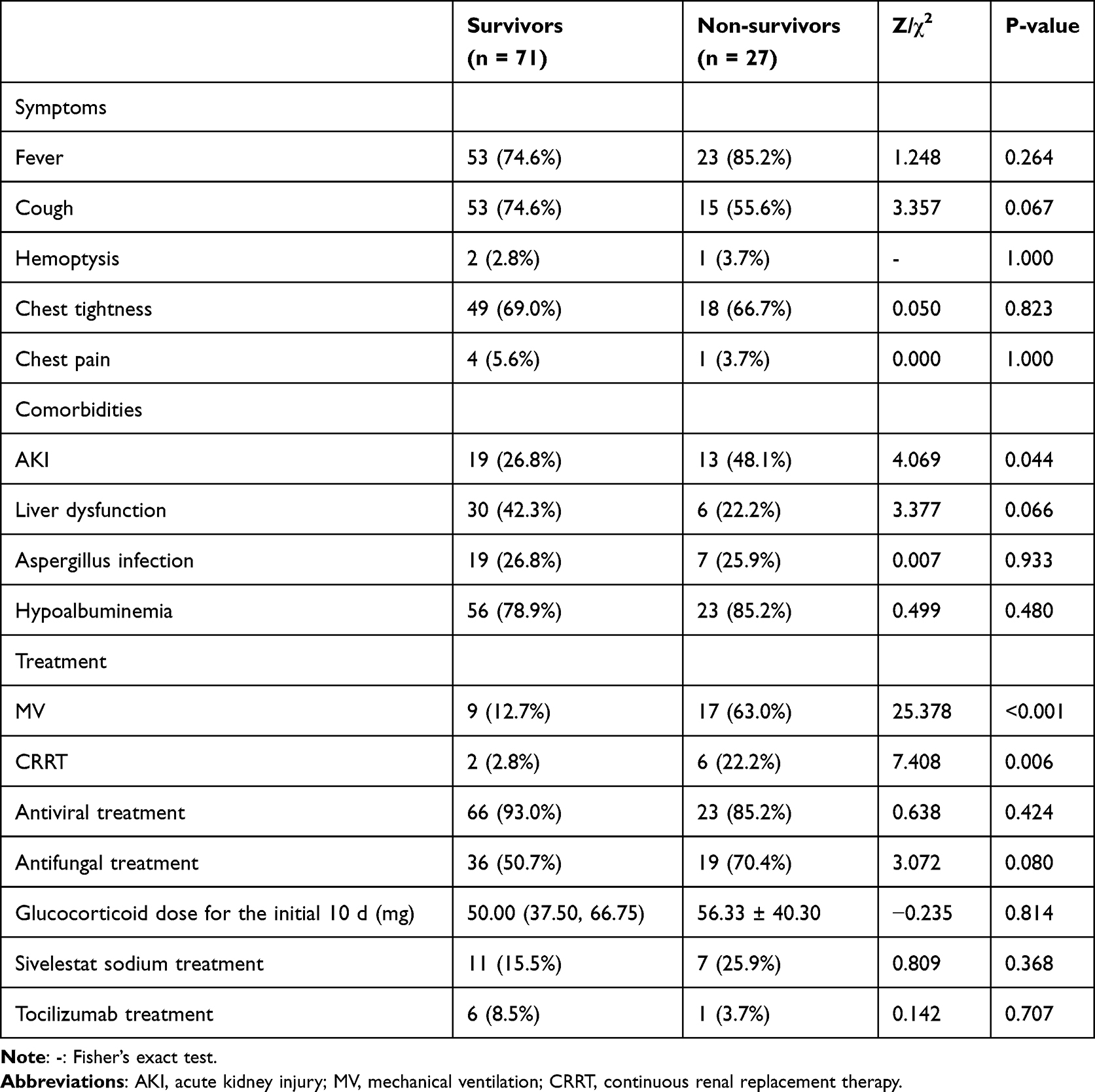 |
Table 3 Symptoms, Comorbidities, and Treatments of Severe COVID-19 Patients |
Prognostic Risk Factors for Severe COVID-19
The variance inflation factor (VIF) test results ranged from 1.119 to 1.647 (<10), indicating that there was no multicollinearity among the variables. Logistic regression analysis showed that WBC count (odds ratio [OR] = 1.272), PLT count (OR = 1.006), APACHE II score (OR = 1.207), and MV (OR = 6.960) were independent risk factors for the poor prognosis of severe COVID-19 patients (Table 4).
 |
Table 4 Multivariate Logistic Regression Analysis of Risk Factors Associated with the Prognosis of Severe COVID-19 |
Predictive Value of the Prognostic Risk Factors
The ROC curve analysis showed that the WBC count, APACHE II score, and MV had good predictive value for the outcomes of severe COVID-19 patients, with the area under the curve (AUC) values of 0.807, 0.761, and 0.751, respectively. PLT count also exhibited a predictive value for the prognosis of severe COVID-19 patients, with an AUC value of 0.690. The AUC of all four risk factors was 0.897, which was higher than that of any single factor (Z = 2.235, 3.452, 2.604, and 3.374, P < 0.05; Table 5 and Figure 1).
 |
Table 5 ROC Curve Analysis of the Risk Factors Associated with the Prognosis of Severe COVID-19 |
 |
Figure 1 Predictive values of individual risk factors alone and in combination for severe COVID-19 prognosis. Abbreviations: WBC, white blood cell; PLT, platelet; APACHE II, Acute Physiology and Chronic Health Evaluation II; MV, mechanical ventilation. |
Discussion
This retrospective study identified clinical characteristics and prognostic risk factors of severe COVID-19. The identified risk factors may enable the identification of potential severe COVID-19 patients in the early stages. Our results showed that high WBC count, neutrophil count, PLT count, and APACHE II score at baseline were associated with worse outcomes in COVID-19 patients. Additionally, COVID-19 patients who underwent MV and CRRT treatments had a greater chance of mortality. In addition to being independent risk factors, WBC count, PLT count, APACHE II score, and MV showed good predictive value for the outcomes of severe COVID-19 patients. The novelty of our study is that we confirmed the combination of these four risk factors had a higher value and accuracy in predicting the prognosis of severe COVID-19 cases.
Previous studies have found that elevated WBC and neutrophil levels are related to higher mortality of COVID-19 patients and that WBC is an independent risk factor for the death of COVID-19 patients.5,9 Upon infection, the immune system recognizes the coronavirus particles, triggering a WBC and neutrophil-induced cytokine storm, contributing to severe lung damage or ARDS in extreme cases.13,14 Our study confirmed that WBC and neutrophils were elevated in the non-survivor group. Additionally, our results showed that high WBC level was an independent risk factor (OR = 1.272) and a reliable predictive parameter for the mortality of severe COVID-19 patients. Specifically, for each unit increase in WBC count, the risk of death of severe COVID-19 patients increased by 1.272 times. Therefore, paying close attention to the changes in WBC and neutrophil levels may reduce the mortality rate of severe COVID-19 patients by ensuring timely treatment.
Previous studies reported lower PLT counts in severe COVID-19 cases.15–18 In contrast, our study found that PLT count was elevated among the non-surviving severe COVID-19 patients, consistent with the results of Yang et al.6 One explanation for this may be that as China announced new measures in December 2022, while rolling back COVID-19 restrictions, the novel coronavirus mutated during transmission.5 Besides, previous study has found that the PLT count of COVID-19 patients increased rapidly before the development of severe symptoms, reaching the highest level at 11–15 d after admission, and then declined rapidly,16 indicating that PLT count may decrease after the development of severe symptoms. In our study, PLT count was recorded upon admission. Therefore, dynamic changes in PLT count in severe COVID-19 cases may be more meaningful for predicting their prognosis. Our study showed that PLT count was an independent risk factor for the prognosis of severe COVID-19 patients (OR = 1.006). Specifically, for each unit increase in PLT count, the risk of death increased by 1.006 times in severe COVID-19 cases. Therefore, PLT count may serve as a predictive factor for the prognosis of severe COVID-19 patients.
APACHE II score is a scoring system based on age, physiologic measurements, and past medical history, and it is widely used to evaluate disease severity and hospital mortality in patients with serious diseases.19–21 Zou et al22 found that the APACHE II score can predict hospital mortality, with an APACHE II score > 17 indicating the possibility of particularly poor outcomes. Tameshkel et al23 found that a high APACHE II score is associated with intubation as well as prolonged intubation time. Consistent with previous research,21 our results revealed that the APACHE II score was significantly higher in the non-survivor group compared to the survivor group and that it may predict the risk of mortality in severe COVID-19 (OR = 1.207) cases. For each unit increase in the APACHE II score, the risk of death increased by 1.207 times in the severe COVID-19 cases. Notably, our research subjects were severe cases, these patients had more severe symptoms and higher mortality, so it was crucial to identify them, especially in the early time when medical resources were scarce. The APACHE II score calculated within 24 h of hospital admission showed a good predictive value in severe COVID-19 cases. Further research is required to explore whether the APACHE II score may be used to decrease mortality and improve the clinical outcomes of severe COVID-19 patients.
Dyspnea can result in respiratory failure and ARDS in severe COVID-19 patients during hospitalization.24 Long-term low oxygen saturation in multiple organ systems and MV are associated with high mortality and increased hospital stay duration in patients with COVID-19.8,25–28 MV plays an important role in the treatment of severe COVID-19 patients.29 Our findings showed that MV was more frequently used for non-survivor patients and that it was an independent risk factor for the outcomes of severe COVID-19 patients (OR = 6.960), with good predictive value. Specifically, the risk of death increased by 6.960 times when severe COVID-19 patients received MV treatment. MV is used to provide adequate gas exchange and to avoid ventilator-induced lung injury. However, there are a few complications to MV treatment. Late intubation causes aggravated lung injury and increases the risk of mortality among patients. While early intubation exposes the patients to unnecessary deep sedation, neuromuscular blockade, and ventilator-associated complications.30 Therefore, further studies are required to determine the effective use of MV for hypoxemic patients with severe COVID-19.
COVID-19 is a systemic disease that affects multiple organ systems.31,32 Our study found that AKI was an independent risk factor for the mortality of severe COVID-19 patients. AKI can be induced by inflammatory stress, including angiotensin II and hypertensive stress, diabetes-related metabolic stress, cytokine storm, high CRP level, over-reactive TGF-β signaling, complement activation, and lung-kidney crosstalk.10 Among the severe COVID-19 patients with AKI, CRRT was more frequently used for patients receiving MV. MV may affect kidney function by reducing kidney perfusion and glomerular filtration.11 Our study found that AKI was more common in non-survivors compared to survivors, consistent with a previous study.33 Notably, we found that CRRT was associated with poor outcomes in severe COVID-19 patients. One possible explanation for this may be the delayed application of CRRT for beneficial outcomes. However, whether CRRT can improve the progression of AKI in COVID patients remains to be determined. Early detection and treatment of kidney abnormalities, such as avoidance of nephrotoxic drugs and adequate hemodynamic support, as well as appropriate CRRT application time need to be investigated further.
Previous studies have reported that WBC count, PLT count, APACHE II score, and MV are associated with COVID-19. The combination of fibrinogen-to-albumin ratio and PLT level can predict the development of severe COVID-19 cases (AUC = 0.754).16 However, the combined diagnostic value of WBC count, PLT count, APACHE II score, and MV has not yet been demonstrated up to now. The results of our study showed that the combination of these four risk factors had a higher value and accuracy in predicting the prognosis of severe COVID-19 cases (AUC = 0.897) compared to the individual factors, with sensitivity and specificity of 81.50% and 87.30%, respectively. Consequently, a combination of WBC count, PLT count, APACHE II score, and MV can be used to identify potential severe COVID-19 cases in the early stages.
Our study has some limitations. First, because the OR value of PLT count was slight, its value as a prognostic indicator alone may be limited. Our study is a single-center retrospective study with a small sample size, which may limit the reliability and universality of our results. Second, there was limited information on the clinical outcomes of the patients owing to the retrospective nature of this study. Further studies should explore the effect of more specific information such as IL-10, CD4 T lymphocyte, and CD8 T lymphocyte levels in the prognosis of severe COVID-19 patients. Third, there were no records of the clinical data of patients after discharge, so we could not investigate the factors associated with the long-term outcomes of COVID-19.
Conclusions
Our study found that WBC count, PLT count, APACHE II score, and MV were independent risk factors for the prognosis of severe COVID-19 cases. These four indicators could be used independently or in combination to predict the outcomes of severe COVID-19 patients; moreover, they showed a higher predictive value upon combined application. Notably, COVID-19 has not been eliminated, and long COVID remains a challenge worldwide.34 The results of our study may enable the identification of potential severe COVID-19 patients in the early stages, which may contribute to the decrease in COVID-19-related mortality in China as well as other countries. Further studies need to be conducted to explore whether WBC count, PLT count, APACHE II score, and MV are associated with long COVID.
Abbreviations
COVID-19, Coronavirus disease 2019; AUROC, area under the receiver operating characteristic curve; WBC, white blood cell; APACHE II, Acute Physiology and Chronic Health Evaluation II; PLT, platelet; AKI, acute kidney injury; MV, mechanical ventilation; CRRT, continuous renal replacement therapy; ARDS, acute respiratory distress syndrome; RT-PCR, real-time reverse-transcriptase–polymerase-chain-reaction; PaO2/FiO2, the ratio of the partial pressure of arterial oxygen to the fraction of inspired oxygen; BMI, body mass index; COPD, chronic obstructive pulmonary disease; LDH, lactate dehydrogenase; CRP, C-reactive protein; IL-6, interleukin-6; PCT, procalcitonin; BNP, brain natriuretic peptide; ROC, receiver operating characteristic; OR, odds ratio; AUC, area under the curve; B, regression coefficient; SE, standard error of mean.
Data Sharing Statement
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Informed Consent
This study was performed in accordance with the Declaration of Helsinki and granted ethical approval (JD-LK2023025-I01) by the Ethics Committee of the Second Affiliated Hospital of Soochow University. Informed consent was obtained by all living patients. For patients who died, informed consent was obtained from a family member.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727–733. doi:10.1056/NEJMoa2001017
2. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
3. Zhao C, Bai Y, Wang C, et al. Risk factors related to the severity of COVID-19 in Wuhan. Int J Med Sci. 2021;18(1):120–127. doi:10.7150/ijms.47193
4. Xie NN, Zhang WC, Chen J, Tian FB, Song JX. Clinical characteristics, diagnosis, and therapeutics of COVID-19: a review. Curr Med Sci. 2023;43(6):1066–1076. doi:10.1007/s11596-023-2797-3
5. He F, Luo Q, Lei M, et al. Risk factors for severe cases of covid-19 a retrospective cohort study. Aging. 2020;12(15):15730. doi:10.18632/aging.103803
6. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. doi:10.1016/S2213-2600(20)30079-5
7. Cheng P, Wu H, Yang J, et al. Pneumonia scoring systems for severe COVID-19: which one is better. Virol J. 2021;18(1):33. doi:10.1186/s12985-021-01502-6
8. Forrest IS, Jaladanki SK, Paranjpe I, Glicksberg BS, Nadkarni GN, Do R. Non-invasive ventilation versus mechanical ventilation in hypoxemic patients with COVID-19. Infection. 2021;49(5):989–997. doi:10.1007/s15010-021-01633-6
9. Reusch N, De Domenico E, Bonaguro L, et al. Neutrophils in COVID-19. Front Immunol. 2021;12:652470. doi:10.3389/fimmu.2021.652470
10. Chen J, Wang W, Tang Y, Huang XR, Yu X, Lan HY. Inflammatory stress in SARS-COV-2 associated acute kidney injury. Int J Biol Sci. 2021;17(6):1497–1506. doi:10.7150/ijbs.58791
11. Ottolina D, Zazzeron L, Trevisi L, et al. Acute kidney injury (AKI) in patients with Covid-19 infection is associated with ventilatory management with elevated positive end-expiratory pressure (PEEP). J Nephrol. 2022;35(1):99–111. doi:10.1007/s40620-021-01100-3
12. Released by National Health Commission of People’s Republic of C, National Administration of Traditional Chinese Medicine on J. Diagnosis and treatment protocol for COVID-19 patients (tentative 10th version). Health Care Sci. 2023;2(1):10–24. doi:10.1002/hcs2.36
13. Palladino M. Complete blood count alterations in COVID-19 patients: a narrative review. Biochem Med. 2021;31(3):030501. doi:10.11613/BM.2021.030501
14. Wang K, Wang M, Liao X, et al. Locally organised and activated Fth1(hi) neutrophils aggravate inflammation of acute lung injury in an IL-10-dependent manner. Nat Commun. 2022;13(1):7703. doi:10.1038/s41467-022-35492-y
15. Lei R, Mohan C. Immunological biomarkers of COVID-19. Crit Rev Immunol. 2020;40(6):497–512. doi:10.1615/CritRevImmunol.2020035652
16. Bi X, Su Z, Yan H, et al. Prediction of severe illness due to COVID-19 based on an analysis of initial fibrinogen to albumin ratio and platelet count. Platelets. 2020;31(5):674–679. doi:10.1080/09537104.2020.1760230
17. Wan S, Yi Q, Fan S, et al. Relationships among lymphocyte subsets, cytokines, and the pulmonary inflammation index in coronavirus (COVID-19) infected patients. Br J Haematol. 2020;189(3):428–437. doi:10.1111/bjh.16659
18. Ganji A, Farahani I, Khansarinejad B, Ghazavi A, Mosayebi G. Increased expression of CD8 marker on T-cells in COVID-19 patients. Blood Cells Mol Dis. 2020;83:102437. doi:10.1016/j.bcmd.2020.102437
19. Bahtouee M, Eghbali SS, Maleki N, Rastgou V, Motamed N. Acute physiology and chronic health evaluation II score for the assessment of mortality prediction in the intensive care unit: a single-centre study from Iran. Nurs Crit Care. 2019;24(6):375–380. doi:10.1111/nicc.12401
20. Beigmohammadi MT, Amoozadeh L, Rezaei Motlagh F, et al. Mortality predictive value of APACHE II and SOFA scores in COVID-19 patients in the intensive care unit. Can Respir J. 2022;2022:5129314. doi:10.1155/2022/5129314
21. Fernandes S, Servio R, Patricio P, Pereira C. Validation of the Acute Physiology and Chronic Health Evaluation (APACHE) II score in COVID-19 patients admitted to the intensive care unit in times of resource scarcity. Cureus. 2023;15(2):e34721. doi:10.7759/cureus.34721
22. Zou X, Li S, Fang M, et al. Acute physiology and chronic health evaluation II score as a predictor of hospital mortality in patients of coronavirus disease 2019. Crit Care Med. 2020;48(8):e657–e665. doi:10.1097/CCM.0000000000004411
23. Safarnezhad Tameshkel F, Mandehgar-Najafabadi M, Ahmadzadeh M, et al. Evaluation of three common scoring systems in COVID-19 patients: neutrophil-lymphocyte ratio (NLR), the Acute Physiology and Chronic Health Evaluation II (APACHE II), and C-reactive protein (CRP). Ann Med Surg. 2024;86(2):811–818. doi:10.1097/MS9.0000000000001503
24. Wu C, Chen X, Cai Y, et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. JAMA Intern Med. 2020;180(7):934–943. doi:10.1001/jamainternmed.2020.0994
25. Lam E, Paz SG, Goddard-Harte D, Pak YN, Fogel J, Rubinstein S. Respiratory involvement parameters in hospitalized COVID-19 patients and their association with mortality and length of stay. Can J Respir Ther. 2022;58:1–8. doi:10.29390/cjrt-2021-057
26. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382(18):1708–1720. doi:10.1056/NEJMoa2002032
27. Elsayed HH, Hassaballa AS, Ahmed TA, Gumaa M, Sharkawy HY, Moharram AA. Variation in outcome of invasive mechanical ventilation between different countries for patients with severe COVID-19: a systematic review and meta-analysis. PLoS One. 2021;16(6):e0252760. doi:10.1371/journal.pone.0252760
28. Kishaba T, Maeda A, Nabeya D, Nagano H. Potential predictors of poor prognosis among critical COVID-19 pneumonia patients requiring tracheal intubation. Tohoku J Exp Med. 2020;252(2):103–107. doi:10.1620/tjem.252.103
29. Brioni M, Meli A, Grasselli G. Mechanical ventilation for COVID-19 patients. Semin Respir Crit Care Med. 2022;43(3):405–416. doi:10.1055/s-0042-1744305
30. Russotto V, Myatra SN, Laffey JG, et al. Intubation practices and adverse peri-intubation events in critically Ill patients from 29 countries. JAMA. 2021;325(12):1164–1172. doi:10.1001/jama.2021.1727
31. Wang D, Hu B, Hu C, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
32. Ma GG, Shen YX, Wu L, et al. Effect of liver injury on prognosis and treatment of hospitalized patients with COVID-19 pneumonia. Ann Transl Med. 2021;9(1):10. doi:10.21037/atm-20-4850
33. Cheng Y, Luo R, Wang K, et al. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020;97(5):829–838. doi:10.1016/j.kint.2020.03.005
34. Peluso MJ, Deeks SG. Mechanisms of long COVID and the path toward therapeutics. Cell. 2024;187(20):5500–5529. doi:10.1016/j.cell.2024.07.054Burnier
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Haematological Traits in Symptomatic and Asymptomatic COVID-19 Positive Patients for Predicting Severity and Hospitalization
Alkahtani AM, Alraey Y, Zaman GS, Al‐Shehri H, Alghamdi IS, Chandramoorthy HC, Al-Hakami AM, Alamri AM, Alshehri HA
Journal of Blood Medicine 2022, 13:447-459
Published Date: 27 August 2022
Platelet-to-White Blood Cell Ratio as a Predictor of Mortality in Patients with Severe COVID-19 Pneumonia: A Retrospective Cohort Study
Thungthienthong M, Vattanavanit V
Infection and Drug Resistance 2023, 16:445-455
Published Date: 24 January 2023
Determinants of Pneumothorax Among Mechanically Ventilated COVID-19 Intensive Care Unit Patients, a Single Centre Study
Hundie TG, Alemu ZA, Getachew LZ, Abera LA, Seyoum AB, Mogus LS, Admasu NM, Regassa GB, Tilahun YB, Bareamichael PI, Tessema AG, Derese TN
Journal of Multidisciplinary Healthcare 2023, 16:3977-3989
Published Date: 11 December 2023