")
Back to Journals » Infection and Drug Resistance » Volume 18
Clinical Efficacy of Continuous Renal Replacement Therapy in Patients with Pulmonary Tuberculosis Complicated with Sepsis: A Retrospective Observational Study
Authors Chen X, Lin X, Cheng F, Zheng S, Zhang Q, Wu T, Shi J
Received 6 November 2024
Accepted for publication 21 March 2025
Published 21 April 2025 Volume 2025:18 Pages 1975—1984
DOI https://doi.org/10.2147/IDR.S502113
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xin Chen, Xiaoqing Lin, Fang Cheng, Shilin Zheng, Qiang Zhang, Te Wu, Jichan Shi
Department of Infectious Disease, Wenzhou Central Hospital, Dingli Clinical College of Wenzhou Medical University, Wenzhou City, Zhejiang Province, People’s Republic of China
Correspondence: Jichan Shi, Department of Infectious Disease, Wenzhou Central Hospital, Dingli Clinical College of Wenzhou Medical University, No. 252 Baili East Road, Lucheng District, Wenzhou City, Zhejiang Province, 325000, People’s Republic of China, Tel +86 0577 88882121, Email [email protected]
Objective: To explore the clinical efficacy of continuous renal replacement therapy (CRRT) in patients with pulmonary tuberculosis (TB) complicated with sepsis, particularly focusing on 28-day mortality (primary objective), and to assess the impact of CRRT on inflammatory response, renal function, haemodynamics and overall prognosis (secondary objectives).
Methods: A total of 98 patients with pulmonary TB complicated by sepsis were included: 49 patients were enrolled in the control group and received routine treatment, whereas 49 patients were enrolled in the CRRT group and received CRRT based on the control group. Renal function indicators, inflammatory indicators, haemodynamic indicators and recovery status were analysed and compared.
Results: After 72 hours of treatment, C-reactive protein (CRP), serum creatinine (SCR), blood urea nitrogen (BUN) and plasma lactic in the CRRT group decreased (P < 0.001), procalcitonin (PCT) and N-terminal pro-B-type natriuretic peptide (NT-proBNP) were reduced (P < 0.01) and urine volume and mean arterial pressure (MAP) increased (P < 0.001). After 72 hours of treatment, CRP and PCT in the control group increased (P < 0.05), SCR, BUN and NT-proBNP increased (P < 0.001), plasma lactic was not significantly changed and MAP decreased (P < 0.05). The 28-day mortality in the CRRT group was lower than in the control group (28.6% vs 49%, P = 0.038), intensive care unit hospitalisation time was shorter than in the control group (11.27 ± 9.34 vs 15.43 ± 9.19 d, P = 0.028) and Acute Physiological Function and Chronic Health Status Scoring System II and Sequential Organ Failure Score scores were lower after treatment (P < 0.001). The difference was statistically significant.
Conclusion: Continuous renal replacement therapy can significantly improve inflammatory response, enhance haemodynamics, promote renal function recovery and increase overall treatment efficacy in patients with pulmonary TB complicated with sepsis.
Keywords: continuous renal replacement therapy, pulmonary tuberculosis, sepsis, clinical efficacy
Introduction
Tuberculosis (TB) is mainly caused by infection with Mycobacterium tuberculosis (MTB) and is the second most common infectious disease in the world after COVID-19.1 According to the World Health Organization, an estimated 9.9 million new cases of TB were diagnosed worldwide in 2021.2 China ranks third among countries with a high TB burden, after India and Indonesia.3 Patients with pulmonary TB often suffer from low immune function due to long-term invasion by MTB and experience damage to lung tissue and bronchial structures. Combined with bacterial, fungal or viral infections, they are more likely to develop severe pneumonia and sepsis.4,5 Sepsis is a systemic inflammatory response syndrome (SIRS) caused by infection, and delayed or ineffective treatment can rapidly progress to septic shock, which can cause fatal organ dysfunction in severe cases, with a mortality rate of 43%–61.8%.6,7 Patients with pulmonary TB complicated by sepsis have low immunity, face dual challenges from TB and infection, and exhibit overlapping clinical manifestations, which can obscure diagnosis. As a result, their mortality rate can be significantly higher than that of patients with sepsis alone.8,9
In recent years, continuous renal replacement therapy (CRRT) has become one of the important ways of treating sepsis.10 Continuous renal replacement therapy has been shown to effectively remove inflammatory mediators, endotoxins and metabolic waste, thereby reducing systemic inflammation and improving organ function. Given the dual inflammatory burden in patients with TB and sepsis, CRRT may offer significant benefits by mitigating both chronic and acute inflammatory responses.11
This study aims to explore the therapeutic effects of CRRT on patients with pulmonary TB and sepsis. The primary objective is to evaluate the effect of CRRT on 28-day mortality in patients with pulmonary TB complicated by sepsis. We hypothesised that CRRT would significantly reduce 28-day mortality compared with conventional treatment. The secondary objectives are to assess the impact of CRRT on the inflammatory response (measured by C-reactive protein [CRP] and procalcitonin [PCT] levels), renal function (measured by serum creatinine [SCR], blood urea nitrogen [BUN] and urine output), haemodynamics (measured by mean arterial pressure [MAP], N-terminal pro-B-type natriuretic peptide [NT-proBNP] and plasma lactate levels) and overall prognosis (measured by intensive care unit [ICU] hospitalisation time, Acute Physiological Function and Chronic Health Status Scoring System II [APACHE II] score and Sequential Organ Failure Score [SOFA] score). The results are reported as follows.
Materials and Methods
Study Participants and Inclusion Criteria
A total of 98 patients with pulmonary TB complicated with sepsis admitted to the ICU of the Department of Infectious Diseases of Wenzhou Central Hospital between March 2021 and November 2023 were selected as the research participants.
A Priori Estimate of Survival Difference: The expected difference in 28-day survival between the two groups was based on previous studies and clinical experience. It was hypothesised that CRRT could reduce the 28-day mortality rate from 50% in the control group to 30% in the CRRT group, resulting in an expected survival difference of 20%. This estimate was used for sample size calculation to ensure the study had adequate power to detect a clinically meaningful difference in survival.
Sample Size Calculation: The primary endpoint for sample size calculation was 28-day mortality. Based on previous studies, the 28-day mortality rate for patients with pulmonary TB complicated by sepsis was approximately 40%–60%.7,9 It was hypothesised that CRRT could significantly reduce the 28-day mortality rate by 20%. The following formula was used for sample size calculation:

where Zα/2 = 1.96 (for 95% confidence level), Zβ = 0.84 (for 80% power), P1 = 0.50 (expected mortality rate in the control group) and P2 = 0.30 (expected mortality rate in the CRRT group). The calculated sample size was approximately 47.44 per group, rounded up to 48. Therefore, the aim was to include 96 patients (48 per group). In this retrospective study, 98 patients (49 per group) were included, which exceeded the calculated sample size and further enhanced the reliability of the results.
Study Objectives: The primary objective was to determine whether CRRT could reduce 28-day mortality in patients with pulmonary TB complicated by sepsis. The secondary objectives included evaluating the effects of CRRT on inflammatory markers, renal function, haemodynamic stability and overall clinical outcomes, including ICU hospitalisation time and severity scores (APACHE II and SOFA).
To minimise selection bias, the following measures were taken during the study design phase. The inclusion criteria were as follows: (1) age ≥18 years and (2) pulmonary TB confirmed according to the health industry standard of the People’s Republic of China, Diagnosis for Pulmonary Tuberculosis WS288-2017.12 The diagnostic criteria included sputum smear for acid-fast bacilli (AFB), with detection of AFB in sputum samples (23 cases); sputum culture, with a positive culture for MTB in sputum samples for patients with a negative sputum smear (additional cases); imaging studies, showing typical radiological features of TB on chest X-ray or computed tomography, such as cavitation, tree-in-bud pattern and ground-glass opacity; clinical symptoms, including the presence of typical symptoms of TB such as persistent cough, sputum production, low-grade fever, night sweats and weight loss; laboratory tests, including positive serum TB antibodies, positive interferon-γ release assay or strong positive tuberculin skin test; and the exclusion of other diseases that could cause similar symptoms, such as pneumonia or lung cancer. In total, 98 patients were diagnosed with pulmonary TB based on these criteria, including 23 patients with a positive sputum smear for AFB and 75 patients confirmed through other diagnostic methods. (3) The diagnosis of sepsis complied with The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3).13 (4) Clinical data were complete. The exclusion criteria were as follows: (1) death within 24 hours of admission; (2) previous long-term maintenance haemodialysis; (3) pregnant or lactating women; (4) terminal stage of malignant tumour; and (5) missing clinical data. These criteria help screen out relatively homogeneous research populations, thereby reducing potential confounders. This study was approved by the Ethics Committee of Wenzhou Central Hospital (L2023-04-060). During the data collection process, integrity checks were conducted on clinical data from all patients to ensure no key variables were missed. For missing data, an intention-to-treat method was adopted to include all randomly assigned patients in the final analysis to reduce the bias introduced by missing data.
Treatment Programmes
According to whether CRRT was performed, the 98 patients were divided into the CRRT group and the control group, with 49 patients in each group. No patients used immunosuppressive drugs. The aetiological distribution of sepsis in both groups was as follows: bacterial infections occurred in 25 cases (51.0%) in the CRRT group and 23 cases (46.9%) in the control group, fungal infections occurred in 8 cases (16.3%) in the CRRT group and 7 cases (14.3%) in the control group and viral infections occurred in 16 cases (32.7%) in the CRRT group and 19 cases (38.8%) in the control group. No patients were found to have multiple causes of sepsis. These data were collected through laboratory tests, including blood cultures, sputum cultures, urine cultures, fungal antigen tests and viral nucleic acid tests. The control group adopted a conventional bundled management strategy based on the Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021,14 including measures such as administering broad-spectrum antibiotics within 1 hour of admission, switching to targeted antimicrobial drugs after bacterial culture and drug sensitivity testing, timely implementation of fluid resuscitation, use of vasoactive drugs when necessary, maintenance of water, electrolyte and acid-base balance, nutritional support and mechanical ventilation. Standard chemotherapy regimens for anti-TB treatment were selected based on the Guideline for Primary Care of Pulmonary Tuberculosis (2018).15 In addition to the standard routine treatment provided to the control group, the CRRT group also received CRRT (Gambro Lundia AB, Prismaflex; filter: Gambro Industries, Prismaflex M150set, Sweden). The femoral vein was selected to establish temporary circulatory access, and an indwelling double-lumen catheter (manufactured by Arrow International LLC, model: CS-15123-F) was used. According to Anticoagulation Strategies in Continuous Renal Replacement Therapy,16 heparin anticoagulation or anticoagulant-free CRRT was selected, with continuous venous-venous hemofiltration mode chosen and hemofiltration replacement basal fluid selected as the replacement fluid. The replacement fluid flow rate was set to 25–35 mL/kg/hour, and the blood flow rate was set to 100–180 mL/min. For patients with haemodynamic instability, the blood flow rate was gradually increased from 50 to 100 mL/min. During the treatment, the anticoagulant dose was adjusted according to whether the patient was bleeding and the dynamic monitoring of APTT. The ultrafiltration volume and CRRT treatment time were adjusted according to the patient’s 24-hour fluid intake and output, central venous pressure and other specific conditions. The CRRT group received an average of 3.5 sessions of CRRT treatment (range: 2–6 sessions). The average duration of each CRRT session was 24 hours (range: 12–48 hours). The total average duration of CRRT treatment per patient was 84 hours (range: 48–144 hours). The initiation and discontinuation of CRRT were based on the patient’s clinical condition, fluid balance and renal function, in accordance with the guidelines for the management of sepsis and septic shock.
Outcome Indicators
The inflammatory indexes, renal function indexes, haemodynamic indicators and recovery of the two groups of patients were observed before treatment and after 72 hours of treatment. (1) Inflammatory indicators: Serum albumin, rapid CRP and PCT. (2) Renal function indicators: SCR, BUN and urine volume. (3) Haemodynamic indicators: heart rate, MAP, plasma lactate and NT-proBNP. (4) Recovery: outcome regression (28-day mortality), ICU hospitalisation time, APACHE II score and SOFA score.
Fasting venous blood was collected from both groups of patients before and 72 hours after treatment. The supernatant was obtained after centrifugation. The enzyme-linked immunosorbent assay was used to determine CRP and PCT, the immunoturbidimetric assay was used to determine BUN and SCR, the automatic biochemical analyser was used to determine plasma lactate and electrochemiluminescence was used to determine NT-proBNP. The APACHE II score was calculated as the total Acute Physiology Score + age points + Chronic Health Points, with a minimum score of 0 and a maximum score of 71. The higher the score, the more severe the patient’s disease, the higher the risk of death and the worse the prognosis.17 The SOFA score can assess the functional status of the six major system organs of the patient: cardiovascular circulation, respiratory, liver, coagulation, nerve and kidney. The score range for each item was 0–4 points. Sepsis was diagnosed when the SOFA score increased by ≥2 points compared with the baseline.
Statistical Methods
Statistical analysis was performed using SPSS 27.0 software. Normally distributed quantitative data were expressed as mean ± standard deviation, and non-normally distributed data were expressed as median and interquartile range (M [P25, P75]). For normally distributed data, the t-test was used to compare the baseline clinical data between the groups. For non-normally distributed data, the Mann–Whitney U-test was used. Count data were expressed as n (%) and compared using the chi-squared test or Fisher’s exact test.
Analysis of covariance (ANCOVA): To control for potential confounding factors and baseline differences, ANCOVA was used to compare the outcomes between the CRRT and control groups. The following covariates were included in the model:
• Baseline inflammatory markers: CRP and PCT.
• Baseline renal function markers: SCR and BUN.
• Baseline haemodynamic markers: MAP and NT-proBNP.
• Other potential confounders: age, gender and comorbidities (eg diabetes and hypertension).
The analysis was performed using a stepwise regression approach to assess the impact of each covariate on the outcome variables and adjust the model for the best fit. Adjusted means were compared to evaluate the independent effect of CRRT treatment. A P-value of less than 0.05 was considered statistically significant.
Results
Clinical Baseline Characteristics and Group Comparison
Table 1 shows the 98 patients in the study, including 49 in the CRRT group and 49 in the control group. When grouping, the baseline characteristics of the two groups of patients were matched, including age, gender and comorbidities. Although the number of patients with diabetes in the CRRT group was higher than that in the control group (P < 0.05), there was no significant difference in other baseline indicators (P > 0.05), indicating that the two groups were balanced at the baseline level and comparable.
 |
Table 1 Clinical Baseline Characteristics and Group Comparison |
Comparison of Vital Signs and Laboratory Indicators
(1) Inflammatory Indicators: There was no significant difference in CRP between the two groups before treatment (P > 0.05), and PCT in the CRRT group was higher than that in the control group (P < 0.05). After treatment, CRP and PCT in the control group were higher than those before treatment (P < 0.05). In the CRRT group, after treatment, CRP was lower than before treatment (P < 0.001), and PCT was lower than before treatment (P < 0.01), with the differences being statistically significant. The results of ANCOVA showed that CRRT had a notable influence on CRP and PCT. The results of the detection of leukocyte level showed that there was no significant difference between the two groups before and after treatment, and there were significant differences between the groups before and after treatment (P<0.05). These results suggest that CRRT can reduce the inflammatory response.
(2) Renal Function Indicators: Before treatment, the levels of SCR and BUN were significantly higher in the CRRT group than in the control group (P < 0.001), indicating poorer baseline renal function in the CRRT group. After treatment, the levels of SCR and BUN in the CRRT group decreased significantly (P < 0.001), and they increased in the control group (P < 0.001). Urine output also increased significantly in the CRRT group (P < 0.001), suggesting improved renal function.
Interaction Analysis: Linear regression analysis revealed an interaction effect between the baseline levels of SCR and BUN in the treatment group on changes in these renal function indicators. Specifically, the initial severity of renal impairment (higher baseline SCR and BUN) influenced the magnitude of improvement observed with CRRT. This interaction indicated that the effectiveness of CRRT in improving renal function was greater in patients with more severe baseline renal dysfunction. Therefore, a single indicator (eg absolute change in SCR or BUN) could not fully capture the therapeutic effect of CRRT without considering the baseline renal function status.
(3) Haemodynamics: There was no significant difference in MAP, plasma lactate and NT-proBNP between the two groups before treatment (P > 0.05). After treatment, there was no significant change in plasma lactate in the control group, MAP was lower than before treatment (P < 0.05) and NT-proBNP was higher than before treatment (P < 0.001). After treatment, plasma lactate in the CRRT group was lower than before treatment (P < 0.001), MAP was higher than before treatment (P < 0.001) and NT-proBNP was lower than before treatment (P < 0.01), and the difference was statistically significant. The results of ANCOVA showed whether CRRT had a significant effect on MAP changes. These results suggested that CRRT could improve haemodynamic indicators. See Table 2 for details. The F-values presented in Tables 2 and 3 are derived from ANCOVA and represent the ratio of between-group variance to within-group variance. These F-values are used to assess the significance of differences between the CRRT and control groups for various outcome measures. A higher F-value indicates a greater likelihood that the observed differences are statistically significant, as confirmed by the corresponding P-values.
 |
Table 2 Comparison of Vital Signs and Laboratory Indicators |
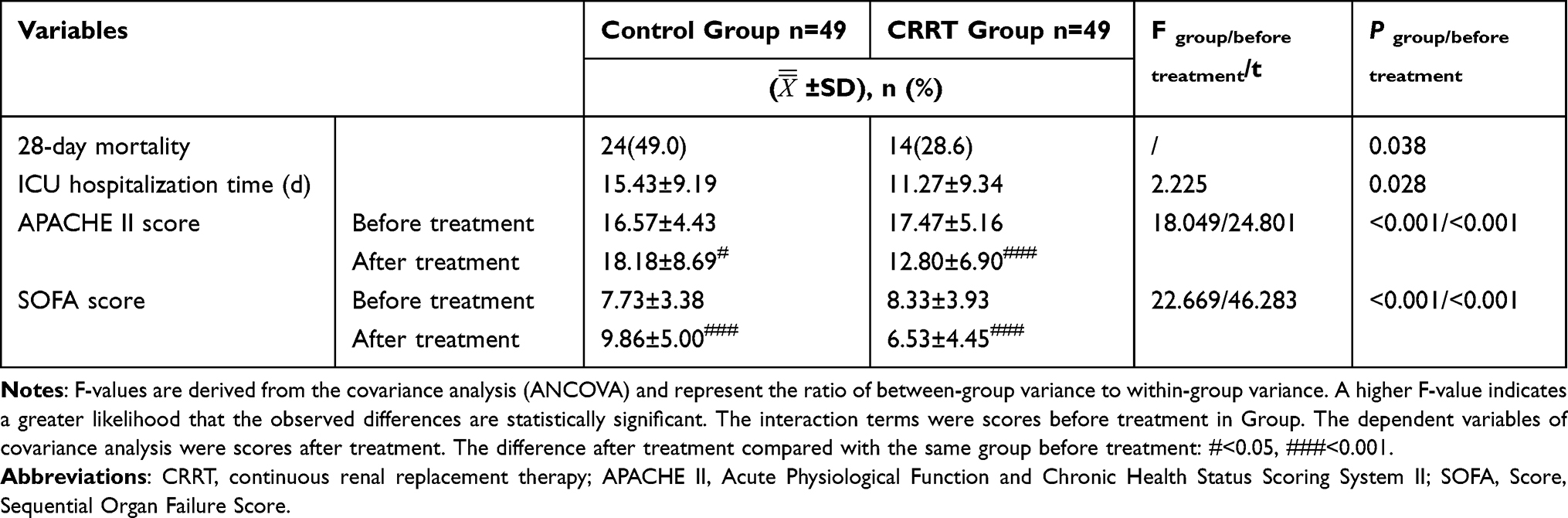 |
Table 3 Comparison of Recovery |
(4) Survival Analysis: The 28-day mortality rate in the CRRT group was significantly lower than that in the control group (28.6% vs 49%, P = 0.038). This observed difference in survival was consistent with our a priori estimate of a 20% reduction in mortality with CRRT. The actual observed difference was 20.4%, which was very close to our expected difference, further validating the effectiveness of CRRT in improving survival in patients with pulmonary TB complicated by sepsis.
Comparison of Recovery
The 28-day mortality in the CRRT group was lower than that in the control group (28.6% vs 49%, P = 0.038), and the ICU hospitalisation time in the CRRT group was shorter than that in the control group (11.27 ± 9.34 vs 15.43 ± 9.19 d, P = 0.028). There was no significant difference in the APACHE II score and SOFA score between the two groups before treatment (P>0.05). After treatment, the APACHE II score and SOFA score in the control group increased, but they decreased in the CRRT group, and the difference was statistically significant (P<0.001). The results of ANCOVA showed that CRRT had an obvious influence on the changes in the APACHE II score and SOFA score (P<0.001). These results suggest that CRRT can improve the overall prognosis. See Table 3 for details.
In summary, the 28-day mortality rate was significantly lower in the CRRT group (28.6%) compared with the control group (49%, P = 0.038), meeting the primary objective of the study. As for the secondary objectives, the CRRT group showed significant improvements in inflammatory markers (CRP and PCT), renal function (SCR, BUN and urine output) and haemodynamic stability (MAP, NT-proBNP and plasma lactate). Additionally, the CRRT group had shorter ICU hospitalisation time and lower APACHE II and SOFA scores after treatment, indicating better overall prognosis.
Discussion
In this study, we retrospectively analysed the treatment effect of CRRT in patients with pulmonary TB complicated with sepsis. The results showed that compared with the control group, patients in the CRRT group showed significant improvements in multiple key clinical indicators. First, the inflammatory indicators (CRP and PCT) of patients in the CRRT group were significantly reduced after 72 hours of treatment, indicating that CRRT treatment could effectively improve the inflammatory state. Second, renal function indicators (SCR, BUN and urine volume) in patients in the CRRT group improved significantly after treatment, even though patients in the CRRT group had poor renal function before treatment. In addition, CRRT treatment significantly improved the patients’ haemodynamic status (MAP, plasma lactate and NT-proBNP) and significantly reduced 28-day mortality and ICU hospitalisation days. Finally, CRRT treatment significantly reduced APACHE II scores and SOFA scores, further demonstrating the effectiveness of CRRT in improving the overall prognosis of patients. These results demonstrate that CRRT has significant clinical advantages in patients with pulmonary TB and sepsis, especially in improving inflammation, renal function and haemodynamic status, as well as improving patient survival and prognosis.
The occurrence of sepsis is related to the excessive secretion of inflammatory mediators, and the recognition of pathogens in the early stage of infection activates the human immune system. The large-scale release of cytokines into the blood to further generate inflammatory storms is considered to be the fundamental cause of major organ dysfunction in sepsis.18,19 Several literature reports have demonstrated that the blood purification effect of CRRT reduces cytokine levels in patients with sepsis, thereby blocking the inflammatory cascade reaction.20,21 The rationale for using CRRT in patients with TB + sepsis is based on the dual inflammatory burden in these patients. The chronic inflammation from TB and the acute inflammation from sepsis create a complex environment that can be effectively managed by CRRT. Continuous renal replacement therapy’s ability to remove inflammatory mediators and maintain haemodynamic stability makes it a valuable treatment option for improving outcomes in these patients. Our study demonstrated significant reductions in inflammatory markers (CRP and PCT) and improvements in renal function and haemodynamics, supporting the hypothesis that CRRT can mitigate the severe inflammatory state in patients with TB + sepsis.
A total of 98 eligible patients with pulmonary TB complicated with sepsis were included in this study. The average age of the patients was 60.56 ± 16.76 years old, including 77 men and 21 women; 28 patients were complicated with hypertension, 26 patients with diabetes, 7 patients with heart disease and 15 patients with chronic lung disease. The overall mortality rate was 38.8%, and the mortality rate of the control group without CRRT was as high as 49%, which was in line with the high mortality rate of pulmonary TB complicated with sepsis in the previous studies.7,9
In this study, 23 patients tested positive for AFB in sputum, and only 27 patients had initiated anti-TB treatment before hospitalisation. Some studies have shown that failure to initiate anti-TB treatment before hospitalisation increases the risk of death in patients with pulmonary TB complicated by sepsis.9 This may be due to the failure of early diagnosis and treatment of TB, which leads to disease progression, further spread of TB lesions, decreased immunity and poor treatment outcomes after co-infection. Therefore, early diagnosis and treatment of patients with pulmonary TB are crucial; it is expected to reduce the mortality rate of patients with pulmonary TB complicated by sepsis.
C-reactive protein and PCT increase rapidly when the body has an inflammatory response, which can reflect the condition and prognosis of patients with sepsis. In our study, CRP and PCT in the CRRT group decreased significantly after treatment, with statistical significance (P < 0.01), indicating that CRRT could reduce the inflammatory response of patients with pulmonary TB complicated with sepsis and improve the body’s immune function. This study lacks relevant research and analysis on the effects of CRRT on inflammatory cytokines because the clinical data on cytokines were incomplete. Therefore, further research should be conducted in the future. Metabolites such as BUN and SCR can reflect glomerular filtration function, and urine volume can reflect renal blood perfusion. In this study, SCR and BUN in the CRRT group before treatment were significantly higher than those in the control group, and urine output was significantly lower than in the control group. It is suggested that compared with the control group, the overall renal function of the CRRT group was worse. The possible reason is that this is a retrospective study, and clinicians tend to adopt CRRT when acute renal injury occurs in patients with pulmonary TB complicated with sepsis. This study showed that the BUN and SCR in the CRRT group decreased significantly after treatment, and the urine volume increased, with statistically significant differences (P < 0.001), indicating that CRRT can continuously and slowly purify the blood through extracorporeal circulation and has a renal protective effect on patients with pulmonary TB complicated with sepsis. Plasma lactate is a product of cellular anaerobic glycolysis and reflects the degree of tissue microcirculation ischemia and hypoxia in septic shock. N-terminal pro-B-type natriuretic peptide is a cardiac neurohormone produced by the cleavage of BNP, which reflects the degree of myocardial damage and the cardiac volume load after fluid resuscitation. This study shows that plasma lactate and NT-proBNP significantly decreased and MAP increased in the CRRT group after treatment, indicating that CRRT can maintain haemodynamic stability and is more advantageous for volume management in patients with pulmonary TB combined with septic shock, ensuring tissue perfusion while avoiding excessive fluid replenishment causing organ burden. The APACHE II score and SOFA score are commonly used indicators to reflect the severity and prognosis of the disease in the ICU. This study showed that the 28-day mortality rate of the CRRT group after treatment was lower than that of the control group (28.6% vs 49%, P = 0.038), the ICU hospitalisation days were shorter than those of the control group (11.27 ± 9.34 vs 15.43 ± 9.19 d, P = 0.028) and the APACHE II score and SOFA score were significantly decreased (P < 0.001), indicating that CRRT can improve the overall prognosis of patients with pulmonary TB complicated with sepsis.
Limitations of this study mainly include the following. First, this study is a single-centre retrospective study, and the sample size is limited, which may affect the universality and external validity of the results. Second, due to the retrospective design of the study, the data integrity and accuracy may be limited, and all potential confounding factors may not be controlled. Furthermore, individual differences in CRRT treatment regimens may affect the results, and a large-scale, multicentre prospective study is needed to verify the conclusions of this study in the future. It must be emphasised that there is currently a lack of unified guidelines on CRRT in regulating inflammatory responses and inflammatory mediators, and we suggest that future studies should further standardise treatment options for CRRT to reduce bias introduced by differences in treatment parameters.
Conclusion
This study demonstrated that CRRT significantly reduced 28-day mortality in patients with pulmonary TB complicated by sepsis, achieving the primary objective. Additionally, CRRT improved inflammatory response, renal function, haemodynamics and overall prognosis, supporting the secondary objectives. These findings suggest that CRRT is a valuable treatment option for this patient population and warrant further investigation in larger, prospective studies.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Jichan Shi at [email protected], upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee of Wenzhou Central Hospital (L2023-04-060). Informed consent was signed by all participants in this study.
Funding
The authors have received no financial support for the research, authorship, or publication of this manuscript.
Disclosure
None of the authors have any personal, financial, commercial, or academic conflicts of interest for this work.
References
1. Urbán-Solano A, Flores-Gonzalez J, Cruz-Lagunas A, et al. High levels of PF4, VEGF-A, and classical monocytes correlate with the platelets count and inflammation during active tuberculosis. Front Immunol. 2022;13:1016472. doi:10.3389/fimmu.2022.1016472
2. García-Morales L, Del Portillo P, Anzola JM, et al. The lack of the tetr-like repressor gene BCG_2177c (Rv2160A) may help mycobacteria overcome intracellular redox stress and survive longer inside macrophages when surrounded by a lipid environment. Front Cell Infect Microbiol. 2022;12:907890. doi:10.3389/fcimb.2022.907890
3. Zhang Q, Song W, Liu S, et al. An ecological study of tuberculosis incidence in China, from 2002 to 2018. Front Public Health. 2022;9:766362. doi:10.3389/fpubh.2021.766362
4. Orme IM, Robinson RT, Cooper AM. The balance between protective and pathogenic immune responses in the TB-infected lung. Nat Immunol. 2015;16(1):57–63. doi:10.1038/ni.3048
5. Henao-Tamayo M, Ordway DJ, Orme IM. Memory T cell subsets in tuberculosis: what should we be targeting? Tuberculosis. 2014;94(5):455–461. doi:10.1016/j.tube.2014.05.001
6. Hunt A. Sepsis: an overview of the signs, symptoms, diagnosis, treatment and pathophysiology. Emerg Nurse. 2019;27(5):32–41. doi:10.7748/en.2019.e1926
7. Medam S, Zieleskiewicz L, Duclos G, et al. Risk factors for death in septic shock: a retrospective cohort study comparing trauma and non-trauma patients. Medicine. 2017;96(50):e9241. doi:10.1097/MD.0000000000009241
8. Galvin J, Tiberi S, Akkerman O, et al. Pulmonary tuberculosis in intensive care setting, with a focus on the use of severity scores, a multinational collaborative systematic review. Pulmonology. 2022;28(4):297–309. doi:10.1016/j.pulmoe.2022.01.016
9. Cui KP, Chen HD, Lai M, et al. Analysis of risk factors of death in patients with tuberculosis-related septic shock in tuberculosis intensive care unit. J Clin Pulmonary Med. 2023;28(4):500–504,522. doi:10.3969/j.issn.1009-6663.2023.04.003
10. Wang C, Zheng J, Wang J, et al. Cox-LASSO analysis for hospital mortality in patients with sepsis received continuous renal replacement therapy: a MIMIC-III database study. Front Med. 2022;8:778536. doi:10.3389/fmed.2021.778536
11. Baeg SI, Jeon J, Kang D, et al. Impact of protocolized fluid management on electrolyte stability in patients undergoing continuous renal replacement therapy. Front Med. 2022;9:915072. doi:10.3389/fmed.2022.915072
12. National Health and Family Planning Commission of the People’s Republic of China. Diagnosis for pulmonary tuberculosis. China J Infect Control. 2018;17(7):642–652. doi:10.3969/j.issn.1671-9638.2018.07.019
13. Singer M, Deutschman CS, Seymour CW, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. 2016;315(8):801–810. doi:10.1001/jama.2016.0287
14. Evans L, Rhodes A, Alhazzani W, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021;47(11):1181–1247. doi:10.1007/s00134-021-06506-y
15. Chinese Medical Association, Chinese Medical Association Journal, Chinese Medical Association General Practice Branch, Chinese Medical Association Respiratory Disease Branch Infection Group, Chinese Medical Association “Chinese General Practitioner Journal” Editorial Committee, Respiratory Disease Primary Care Guidelines Writing Expert Group. Guideline for primary care of pulmonary tuberculosis (2018). Chin J Gen Pract. 2019;18(8):709–717 doi:10.3760/cma.j.issn.1671-7368.2019.08.002
16. Legrand M, Tolwani A. Anticoagulation strategies in continuous renal replacement therapy. Semin Dial. 2021;34(6):416–422. doi:10.1111/sdi.12959
17. Akavipat P, Thinkhamrop J, Thinkhamrop B, Sriraj W. ACUTE PHYSIOLOGY AND CHRONIC HEALTH EVALUATION (APACHE) II SCORE - THE CLINICAL PREDICTOR IN NEUROSURGICAL INTENSIVE CARE UNIT. Acta Clin Croat. 2019;58(1):50–56. doi:10.20471/acc.2019.58.01.07 PMID: 31363325; PMCID: PMC6629196.
18. Zhang L, Feng Y, Fu P. Blood purification for sepsis: an overview. Precis Clin Med. 2021;4(1):45–55. doi:10.1093/pcmedi/pbab005
19. Moriyama K, Nishida O. Targeting cytokines, pathogen-associated molecular patterns, and damage-associated molecular patterns in sepsis via blood purification. Int J Mol Sci. 2021;22(16):8882. doi:10.3390/ijms22168882
20. Pickkers P, Vassiliou T, Liguts V, et al. Sepsis management with a blood purification membrane: European experience. Blood Purif. 2019;47 Suppl 3:1–9. doi:10.1159/000499355
21. Zhang H, Zhu G, Yan L, Lu Y, Fang Q, Shao F. The absorbing filter Oxiris in severe coronavirus disease 2019 patients: a case series. Artif Organs. 2020;44(12):1296–1302. doi:10.1111/aor.13786
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.