")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Clinical Efficacy of Microplasma Radiofrequency in Treating Post-Traumatic Pigmentary Deposition: A VISIA Quantitative Analysis
Authors Xu Y, Yin Y, Yang ZQ, Li J, Guo LN, Ma C
Received 6 December 2024
Accepted for publication 17 April 2025
Published 28 April 2025 Volume 2025:21 Pages 575—582
DOI https://doi.org/10.2147/TCRM.S508522
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Yan Xu,1 Yan Yin,1 Zai-Quan Yang,2 Jing Li,1 Li-Na Guo,1 Chao Ma1
1Department of Medical Cosmetology, Cangzhou Central Hospital, Cangzhou, Hebei, 061001, People’s Republic of China; 2Department of Infectious Diseases, Cangzhou Infectious Disease Hospital, Cangzhou, Hebei, 061001, People’s Republic of China
Correspondence: Chao Ma, Email [email protected]
Objective: To observe the clinical efficacy of microplasma radiofrequency in treating post-traumatic pigmentary deposition using VISIA quantitative analysis, an innovative approach not previously emphasized in microplasma radiofrequency studies.
Methods: Twenty patients with post-traumatic pigmentary deposition, treated at Cangzhou Central Hospital between July 2022 and December 2022, were selected. Pigmented areas were divided into four regions (A: control; B, C, D: treated with increasing energy parameters). Adverse effects (erythema, edema, micro-crusts, pruritus) were monitored at 2, 4, and 6 weeks post-treatment using CTCAE v5.0 criteria. Pigmentary deposition scores and VISIA parameters (spots, ultraviolet spots, red areas, brown spots) were evaluated.
Results: At 2, 4, and 6 weeks, Groups B, C, D showed significant reductions in pigment scores and VISIA parameters vs Group A (P < 0.05), with Group D (highest energy) achieving maximal improvement. Transient mild-moderate erythema (60– 100%), edema (40– 80%), and micro-crusts (20– 60%) occurred in treated groups, resolving spontaneously within 14 days; no severe adverse events were observed.
Conclusion: Microplasma radiofrequency significantly improves post-traumatic pigmentary deposition, with energy-dependent efficacy. Despite transient side effects at higher energies, its favorable safety profile supports clinical adoption. VISIA quantitative analysis provides robust objective evaluation, advancing standardization in pigment management.
Keywords: VISIA quantitative detection, microplasma radiofrequency, post-traumatic pigmentary deposition, clinical observation
Introduction
Pigmentary deposition is a common phenomenon of pigmentation changes in the human skin, with diverse manifestations that can result in variations in skin color, extent, and depth.1 The etiology of pigmentary deposition is multifaceted, with common causes including burns, scalds, trauma from accidents, inflammation, and other irritants.2 Trauma is a significant factor leading to pigmentary deposition, often accompanied by scar formation. Post-traumatic pigmentary deposition is particularly prevalent in Asian populations, where Fitzpatrick skin types III–IV predispose individuals to prolonged hyperpigmentation due to increased melanocyte activity following injury.3 When pigmentary deposition occurs on a patient’s face, it can have a substantial impact on their external appearance and daily life, with studies indicating higher psychological distress in visible pigmentary conditions among Asian cohorts.4
Historically, clinical interventions for pigmentary deposition primarily involved non-surgical methods. Common non-surgical approaches include the use of depigmenting topical medications (such as hydroquinone-based preparations or creams, vitamin A derivatives), abrasion procedures (including microdermabrasion and physical mechanical abrasion), intense pulsed light therapy, fractional lasers, and pixel lasers. The effectiveness of these treatment methods varies, but none have consistently achieved clinical or patient satisfaction.5,6 Microplasma radiofrequency is a novel technology for treating pigmentary deposition in clinical settings. Its technical principle involves exciting nitrogen in the interstitial spaces of the skin to transform it into a microplasma state, which acts on the skin, resulting in exfoliation and heat effects.7 The microplasma-induced thermal energy is hypothesized to disrupt melanin clusters within the epidermis, accelerate keratinocyte turnover, and downregulate tyrosinase activity, thereby reducing pigment retention.8 Additionally, the controlled thermal stimulation may promote collagen remodeling, improving both texture and tone in pigmented lesions.9
Previously, microplasma radiofrequency technology was mainly used for scar treatment, and several studies have confirmed its significant advantages in terms of scar treatment effectiveness and safety.10,11 It also exhibits a clear advantage in altering surface pigmentary deposition on scars. My preliminary experiments have shown that microplasma radiofrequency technology can expedite the regression of pigmentation in guinea pig skin and is effective in improving pigmentation deposition in a narrowband ultraviolet-irradiated guinea pig skin model. Scholars like Halachmi12 have conducted clinical research to confirm the positive therapeutic effects of microplasma radiofrequency technology on post-traumatic pigmentary deposition. However, their studies mostly relied on subjective evaluation criteria. To address this gap, VISIA Quantitative Analysis System—a high-resolution, multi-spectral imaging tool—has emerged as an objective method for quantifying skin pigmentation parameters (eg, spots, ultraviolet spots, red areas, brown spots) through standardized cross-polarized and UV photography.13 To date, there is a dearth of VISIA-supported quantitative analytical research on microplasma radiofrequency treatment for post-traumatic pigmentary deposition in clinical settings. Therefore, this study attempts to employ VISIA quantitative detection to assess the clinical outcomes of microplasma radiofrequency treatment for post-traumatic pigmentary deposition. The findings are presented below.
Materials and Methods
Study Subjects
We selected 20 patients with post-traumatic pigmentary deposition who were treated at our hospital between July 2022 and December 2022. Among them, there were 2 males and 18 females, with ages ranging from 19 to 40 years, and an average age of (27.84±4.62) years. Skin grading was performed according to the Fitzpatrick skin phototype classification system:14 9 patients were classified as Grade III (moderate brown skin, tans uniformly), and 11 patients were Grade IV (olive or dark brown skin, tans minimally). The time of onset of post-traumatic pigmentary deposition ranged from 3 months to 5 years, with an average time of (2.27±0.42) years. All patients met the complete inclusion criteria. This study has received ethical approval from Cangzhou Infectious Disease Hospital and complies with the requirements of the Helsinki Declaration. Informed consent was obtained from all study participants.
Inclusion and Exclusion Criteria
Inclusion Criteria: (1) Patients were clinically diagnosed with post-traumatic pigmentary deposition based on relevant medical examinations; (2) All included patients were adults; (3) Patients had not received any disease-related treatment interventions within the recent six months; (4) Patients were informed about the study and voluntarily signed informed consent.
Exclusion Criteria: (1) Patients with hypertrophic scar formation were excluded; (2) Pregnant or lactating women were excluded; (3) Patients with mental disorders or behavioral and cognitive impairments were excluded; (4) Patients who had received laser or drug treatments within the past six months were excluded; (5) Patients with severe organ pathology were excluded; (6) Individuals who were unwilling to cooperate with the study or unable to complete the study for various reasons were also excluded.
Methods
The Israeli FETON ion beam scar treatment device with a fixed treatment head was used. The single treatment range of the device was 12 mm, with a spacing of 1 mm between beam points. After cleaning the affected area, a compound lidocaine cream (25% lidocaine and 2.5% prilocaine, 50 mg, produced by Beijing Ziguang Pharmaceutical Co., Ltd.) was applied externally, and the area was covered with a plastic wrap for one hour. The skin was then cleansed with water to remove the surface anesthetic cream. The power setting was adjusted to 20–60W based on the severity of the scar and skin thickness.
Group A served as the blank control group and did not receive any treatment. Groups B, C, and D were treated using microplasma radiofrequency technology with different energy parameters: (1) Group B: Microplasma radiofrequency technology treatment (Treatment parameters: fixed, no sheath head, exposure time: 0.6s, output power: 20 Watt, treatment energy per emission point: 0.12J). (2) Group C: Microplasma radiofrequency technology treatment (Treatment parameters: fixed, no sheath head, exposure time: 0.6s, output power: 40 Watt, treatment energy per emission point: 0.24J). (3) Group D: Microplasma radiofrequency technology treatment (Treatment parameters: fixed, no sheath head, exposure time: 0.6s, output power: 60 Watt, treatment energy per emission point: 0.36J).
Groups B, C, and D each received a single session of microplasma radiofrequency technology treatment. After the treatment, patients were instructed to keep the wound dry and avoid washing the treated area for 7 days. During this period, a compound miconazole B ointment (Zhejiang Rishengchang Pharmaceutical Co., Ltd., National Drug Approval Number: H20061269, Specification: 10g) was applied topically, and recombinant human basic fibroblast growth factor (Nanhu Lang peptide Pharmaceutical Co., Ltd., National Drug Approval Number: S20040053, Specification: 2000IU per vial) was used. Adverse effects related to medications (eg, allergic reactions, irritation) and treatment (eg, erythema, edema) were monitored at each follow-up (2, 4, 6 weeks) and recorded. Patients were advised to avoid spicy foods, use sunscreen (SPF ≥30), and refrain from scrubbing or friction on the treated area.
Observational Parameters
- Pigmentary Deposition Assessment: Before treatment and at 2, 4, and 6 weeks after treatment, two blinded dermatologists (unaware of group allocation) evaluated pigmentary deposition using a 4-point scale adapted from the Dermal pigmentation area and severity score (DPASI).15 The scale was as follows: 0 points for no pigmentation (normal skin color), 1 point for light brown (mild), 2 points for medium brown (moderate), and 3 points for dark brown (severe). Intermediate scores were averaged. Inter-rater reliability was assessed using Cohen’s kappa (κ=0.82), indicating strong agreement.
- VISIA Quantitative Detection: Patients underwent imaging with the VISIA® Complexion Analysis System (Canfield Scientific, USA), which captures multi-spectral images (standard, cross-polarized, UV) to quantify various parameters. These include spots (discrete pigmented lesions, 1–10 mm, count range: 0–100), ultraviolet spots (subsurface melanin, score range: 0–100% UV reflectance), red areas (vascular/erythematous regions, score range: 0–100% hemoglobin intensity), and brown spots (epidermal/dermal pigmentation, score range: 0–100% melanin density). Percentiles were calculated relative to a matched population database (Fitzpatrick III–IV skin types).
- Adverse Effects Monitoring: Adverse effects related to medications (eg, allergic reactions, irritation) and treatment (eg, erythema, edema) were assessed at each follow-up visit (2, 4, and 6 weeks) and documented accordingly.
Statistical Methods
GraphPad Prism 8 was used for image processing software, while SPSS 26.0 was used for data analysis and organization. Descriptive statistics for categorical data are presented as n (%), and the chi-square test (χ²) was used to compare the statistical differences. For continuous data, values are expressed as mean (± standard deviation, s), and the t-test was used to compare statistical differences. A power analysis indicated that 20 patients provided 80% power (α=0.05) to detect a 30% reduction in VISIA scores. A significance level of P < 0.05 was considered meaningful.
Results
Comparison of Pigmentary Deposition
Before treatment, there were no significant differences in pigmentary deposition scores among the four groups (all, P > 0.05). At 2, 4, and 6 weeks post-treatment, Groups B, C, and D showed significantly lower scores compared to Group A (all, P < 0.05). Group D demonstrated the most pronounced reduction at all time points (Table 1).
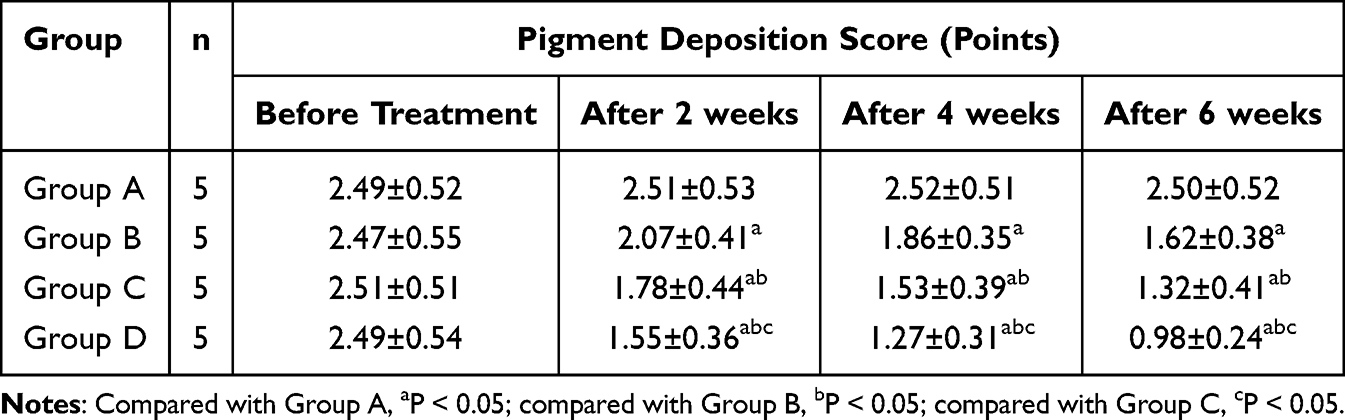 |
Table 1 Comparison of Pigmentary Deposition Scores (Mean ± 1SD) |
Comparison of VISIA Quantitative Detection
VISIA parameters (spots, ultraviolet spots, red areas, brown spots) showed progressive improvements in Groups B, C, and D compared to Group A (all, P < 0.05). Group D exhibited the greatest reduction across all parameters (Table 2 and Figure 1).
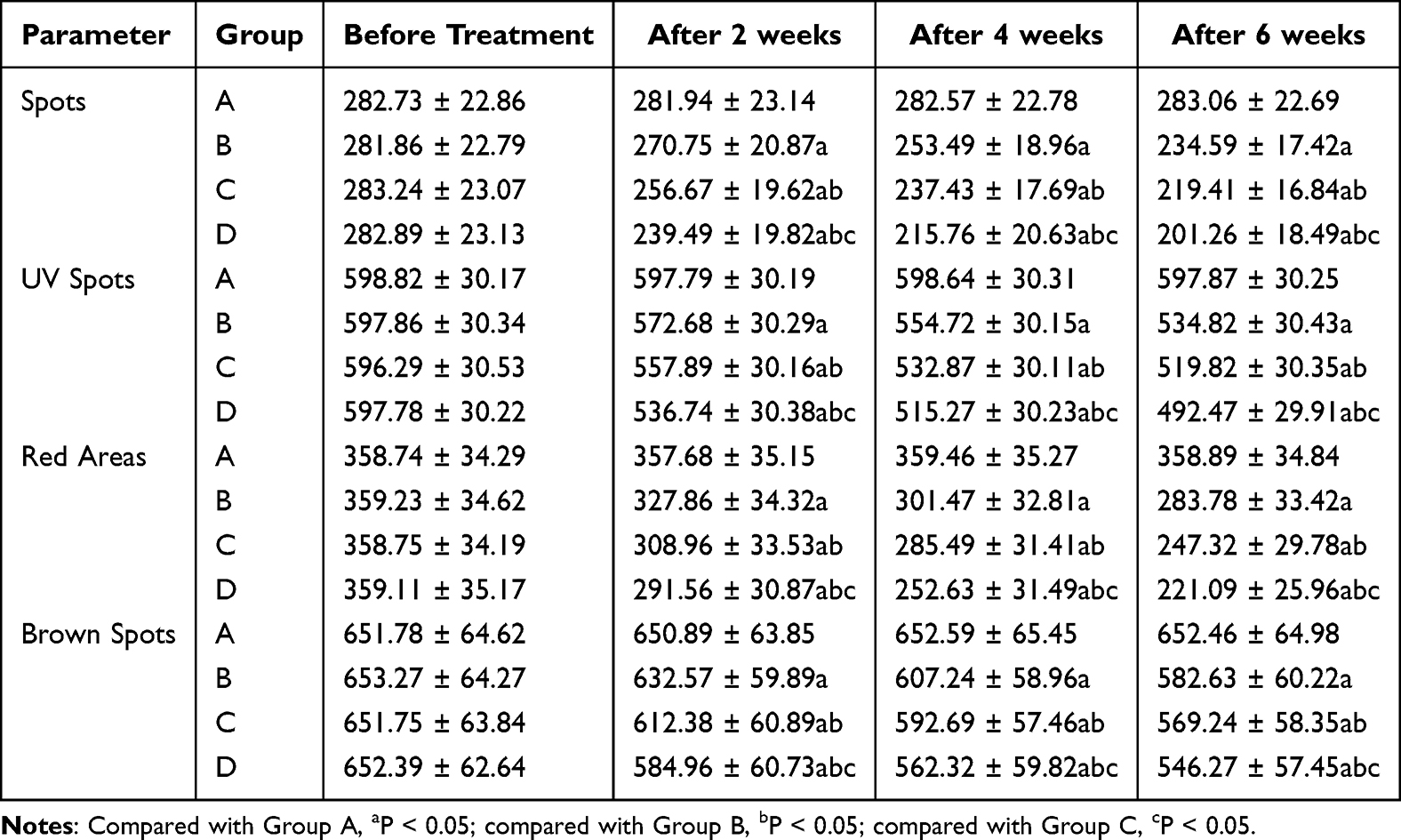 |
Table 2 VISIA Parameter Scores (Mean ± 1SD) |
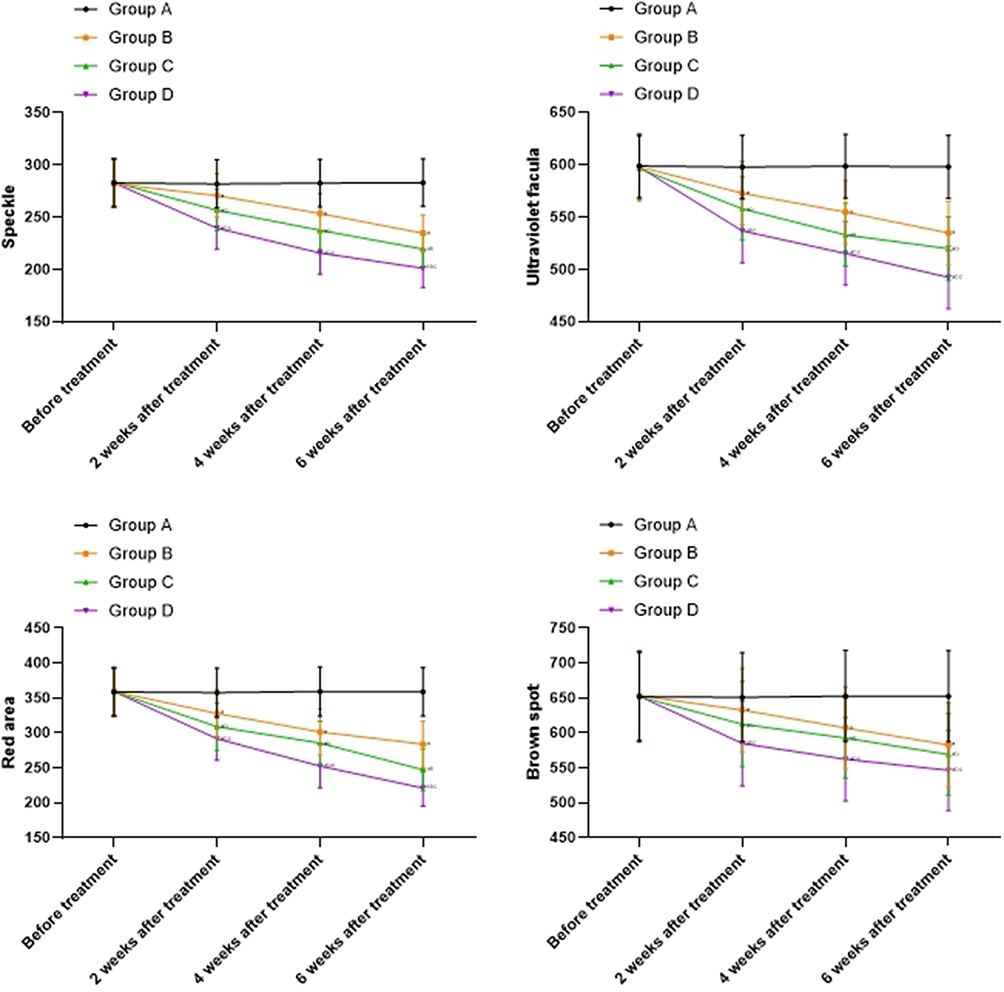 |
Figure 1 Comparison of VISIA Quantitative Detection. Notes: Compared with Group A, aP < 0.05; compared with Group B, bP < 0.05; compared with Group C, cP < 0.05. |
Adverse Effects Monitoring
No severe adverse events (eg, allergic reactions, infection) were observed. Mild to moderate transient erythema and edema occurred in all treated groups (B, C, D), resolving within 7–14 days (Table 3).
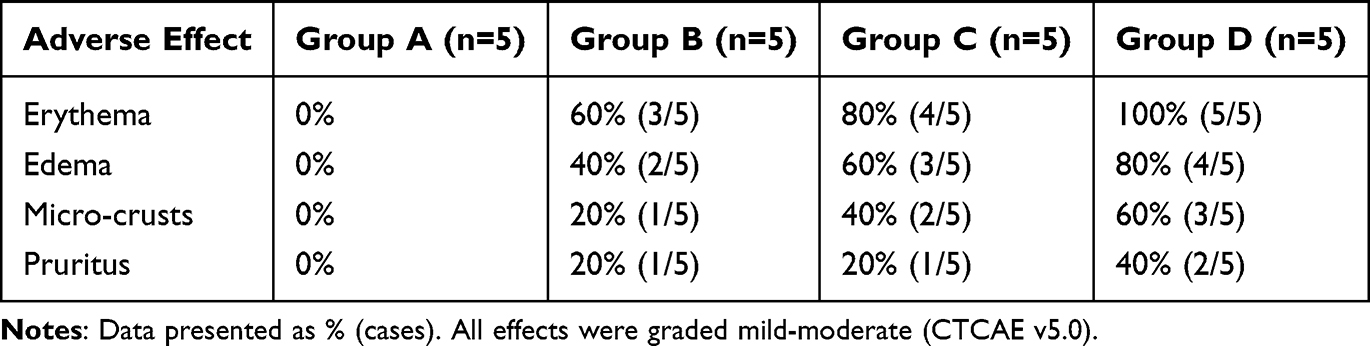 |
Table 3 Adverse Effects by Group and Timepoint |
Discussion
During the natural wound healing process, some patients may experience the formation of scars and pigmentary deposition, which is particularly prevalent among Asian populations with Fitzpatrick III–IV skin types due to heightened melanocyte activity post-injury.16 Various non-surgical methods have been employed in clinical practice to address scar formation and pigmentary deposition. Common approaches include topical medications, abrasion procedures, intense pulsed light therapy, pixel laser treatments, and fractional laser therapy. However, these methods have their limitations, and achieving satisfactory clinical outcomes for patients remains challenging. ① Topical Medications: Common pigment-reducing medications used in clinical practice include retinoic acid creams, hydroquinone products, and certain traditional Chinese medicines with skin-lightening properties. However, the effectiveness of these medications in clinical settings remains a subject of debate. ② Abrasion Procedures: Abrasion procedures, including mechanical abrasion and microdermabrasion, are commonly used. Mechanical abrasion requires precise control of the depth of abrasion and, therefore, demands a high level of technical expertise. Additionally, it carries a relatively high risk of complications. Microdermabrasion, as a superficial abrasion procedure, primarily targets aging skin’s keratinized cells, leading to limited effects on pigmentary deposition.17 ③ Intense Pulsed Light (IPL) Therapy: IPL therapy shows some efficacy in treating superficial pigmentary depositions such as freckles but is generally not effective in addressing pigmentary deposition resulting from trauma.18 ④ Pixel Laser: Pixel laser therapy induces micro-peeling effects on skin tissue, causing physical defects in skin tissue. This may increase the risk of pigmentary deposition. ⑤ Fractional Laser: Fractional laser therapy, known for its strong penetration ability, offers unique advantages in treating hypertrophic scars. However, research on its efficacy in treating pigmentary deposition is scarce. Due to its significant penetration ability, cautious application is required for facial pigmentary deposition treatment.19 In recent years, plasma radiofrequency technology, with its advantages of minimal damage, collagen regeneration promotion, simplicity of operation, and safety, has introduced a new approach to clinical treatment of pigmentary deposition. This technology does not depend on color pigments and provides a promising method for addressing pigmentary deposition.20
Plasma is a state of matter consisting primarily of free electrons and charged ions and is commonly regarded as the fourth state of matter.21 Plasma has found applications in various medical fields, including pathogen inactivation, blood coagulation, skin disease treatment, oral clinical uses, cancer cell therapy, and has yielded promising results.22 Microplasma radiofrequency skin reconstruction technology is a relatively new clinical technique. It was invented by Dr. Ziv Karnia, a physicist from Israel, and is based on the principles of radiofrequency and micro-peeling.23 Microplasma radiofrequency technology employs multi-point, micro-monopolar radiofrequency to excite nitrogen gas on the skin’s surface, generating multiple, controlled, and minimally invasive thermal channels. The heat produced by the monopolar radiofrequency at the end of the microchannels penetrates deep into the skin, reaching up to 500–1000 μm below the surface. This effectively heats the dermis and activates fibroblasts, promoting the degradation of existing collagen and the secretion of new collagen.24 Simultaneously, dehydrated skin tissue acts as a biological dressing, protecting the wound and reducing the risk of infection. The micro-injuries around the heated areas promote rapid wound healing.25 Researchers like Ruff have evaluated microplasma from a histological perspective using animal models and found that it has excellent tissue remodeling properties, resulting in smoother and finer regenerated epidermis.26 This suggests that microplasma radiofrequency technology not only provides reliable results but also significantly reduces the risk of adverse reactions. However, there is limited clinical research on the use of microplasma radiofrequency in treating post-traumatic pigmentary deposition. Although some studies suggest that microplasma radiofrequency has a role in treating post-traumatic pigmentary deposition,27 they often lack objective and scientifically valid facial pigment assessment metrics, making in-depth research on diagnosis and efficacy challenging. Furthermore, the choice of treatment parameters for microplasma radiofrequency therapy in such studies remains inconsistent, hindering the development of standardized guidelines.
In this study, we employed different microplasma radiofrequency treatment parameters to address the issue of pigment deposition in patients. The present study demonstrates that microplasma radiofrequency technology significantly improves post-traumatic pigmentary deposition, with higher energy parameters (Group D) yielding the most pronounced effects. This efficacy may be attributed to two key mechanisms: (1) Thermal disruption of melanin clusters through microplasma-induced subepidermal heating (500–1000 μm depth), which accelerates keratinocyte turnover and facilitates melanin exfoliation;28 (2) Downregulation of tyrosinase activity via controlled thermal stimulation, reducing de novo melanogenesis.29 The energy-dependent response observed in Group D aligns with histologic evidence showing dose-dependent collagen remodeling and melanophage clearance in high-energy settings.30
Notably, the superior outcomes in Group D likely reflect synergistic effects of deeper dermal penetration (enabled by 0.36J/point energy) and sustained fibroblast activation, which not only degrades pigmented collagen but also promotes neocollagenesis with normalized melanin distribution.31 This mechanistic duality—simultaneous pigment removal and structural normalization—may explain why higher-energy protocols achieve more complete depigmentation.
The VISIA quantitative analysis corroborated clinical observations, showing progressive reductions in spots, UV spots, red areas, and brown spots across treatment groups. The 46.2% reduction in brown spots (Group D at 6 weeks) surpasses reported outcomes for fractional CO2 lasers (28–35%) in similar populations,32 highlighting microplasma radiofrequency’s unique advantage in targeting both epidermal and dermal pigmentation.
Adverse effects analysis revealed an energy-dependent safety profile (Table 3). While transient erythema (100% in Group D) and micro-crusts (60%) were common, all resolved without intervention within 14 days, consistent with the self-limiting nature of microplasma-induced microthermal zones.33 Importantly, no hypopigmentation or scarring occurred, contrasting with laser therapies where hypopigmentation rates reach 12–18%.34 This favorable safety profile, combined with operator-independent reproducibility, positions microplasma radiofrequency as a viable option for pigmented skin types prone to post-inflammatory complications.
Study limitations warrant consideration: (1) Sample size constraints (n=20) limit subgroup analyses of skin types and lesion durations. (2) The short follow-up period (6 weeks) precludes assessment of long-term recurrence. (3) The single-center design may introduce selection bias. Future studies should validate these findings in larger cohorts (n≥100) with extended follow-up (≥12 months), directly compare microplasma radiofrequency against gold-standard therapies (eg, Q-switched lasers), and elucidate molecular mechanisms (eg, MITF/tyrosinase pathway modulation) through biopsy-based histopathology.
Conclusion
In conclusion, microplasma radiofrequency treatment demonstrates significant clinical efficacy in patients with post-traumatic pigment deposition. The implementation of this technology effectively improves the condition of pigment deposition and various VISIA assessment parameters. Furthermore, the greater the energy applied during microplasma radiofrequency treatment, the more favorable the results in terms of symptom improvement for the patients. Notably, adverse effects (erythema, micro-crusts) were transient and self-limiting, with no severe complications observed, supporting its safety profile in clinical practice.
These findings advocate for the integration of microplasma radiofrequency into dermatological protocols for traumatic hyperpigmentation, particularly in cases where conventional therapies (eg, lasers) pose a risk of hypopigmentation. Future studies should prioritize long-term efficacy assessment (≥12 months) to evaluate recurrence rates, conduct head-to-head comparisons with gold-standard therapies (eg, Q-switched Nd:YAG laser), and investigate the mechanistic effects of microplasma thermal energy on melanocyte signaling pathways. Addressing these gaps may establish microplasma radiofrequency as a first-line treatment for pigmentary deposition, offering a balance of efficacy, safety, and reproducibility.
Funding
This study was supported by ‘Clinical Observation of VISIA Quantitative Detection in the Treatment of Post-Traumatic Pigmentary Deposition with Microplasma Radiofrequency’, No.20220349.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lipsker D, Lenormand C. Hyperpigmentation. Ann Dermatol Venereol. 2019;146(10):666–682. doi:10.1016/j.annder.2019.05.005 Polish
2. Nautiyal A, Wairkar S. Management of hyperpigmentation: current treatments and emerging therapies. Pigm Cell Melanoma Res. 2021;34(6):1000–1014. doi:10.1111/pcmr.12986
3. Charoo NA. Hyperpigmentation: looking beyond hydroquinone. J Cosmet Dermatol. 2022;21(10):4133–4145. doi:10.1111/jocd.14746
4. Callender VD, Baldwin H, Cook-Bolden FE, et al. Effects of topical retinoids on acne and post-inflammatory hyperpigmentation in patients with skin of color: a clinical review and implications for practice. Am J Clin Dermatol. 2022;23(1):69–81. doi:10.1007/s40257-021-00643-2
5. Desai S, Hartman C, Grimes P, et al. Topical stabilized cysteamine as a new treatment for hyperpigmentation disorders: melasma, post-inflammatory hyperpigmentation, and lentigines. J Drugs Dermatol. 2021;20(12):1276–1279. doi:10.36849/JDD.6367
6. Zheng X, He S, Li Q, et al. Successful treatment of verrucous epidermal nevus with fractional micro-plasma radio-frequency technology and photodynamic therapy. J Cosmet Laser Ther. 2018;20(6):357–359. doi:10.1080/14764172.2018.1511914
7. Kong J, Zhou C, Pan L, Li M, Zhang L. Micro-plasma radiofrequency and silicone gel dressings for treating early post-traumatic facial scars: a retrospective study. J Plast Reconstr Aesthet Surg. 2023;87:10–16. Epub 2023 Sep 12. PMID: 37804642. doi:10.1016/j.bjps.2023.09.004
8. Lan T, Tang L, Xia A, Hamblin MR, Jian D, Yin R. Comparison of fractional micro-plasma radiofrequency and fractional microneedle radiofrequency for the treatment of atrophic acne scars: a pilot randomized split-face clinical study in China. Lasers Surg Med. 2021;53(7):906–913. Epub 2020 Dec 16. PMID: 33326634. doi:10.1002/lsm.23369
9. Liu L, Li H, Zhang W, Cao M, Yu L, Cheng X. Betamethasone transdermal administration combined with fractional Er: YAG lasers or microplasma radiofrequency technology improved hypertrophic scars: a retrospective study. J Cosmet Dermatol. 2024;23(8):2563–2573. Epub 2024 Apr 8. PMID: 38586909. doi:10.1111/jocd.16304
10. Liu W. Emerging technologies in scar management: remodeling of post-surgical linear scar using microplasma radiofrequency. In: Téot L, Mustoe TA, Middelkoop E, Gauglitz GG, editors. Textbook on Scar Management: State of the Art Management and Emerging Technologies [Internet]. Cham (CH): Springer; 2020. Chapter 53. PMID: 36351143.
11. Arkar K, Vasiliev MM, Petrov OF, et al. Dynamics of active brownian particles in plasma. Molecules. 2021;26(3):561. doi:10.3390/molecules26030561
12. Verner I, Naveh HP, Cotofana S. A novel ablative radiofrequency microplasma nonsurgical blepharoplasty for dermatochalasis. Dermatol Ther. 2020;33(6):e14002. doi:10.1111/dth.14002
13. Halachmi S, Orenstein A, Meneghel T, et al. A novel fractional micro-plasma radio-frequency technology for the treatment of facial scars and rhytids: a pilot study. J Cosmet Laser Ther. 2010;12(5):208–212. doi:10.3109/14764172.2010.514921
14. Żychowska M, Reich A. Chronic cutaneous lupus erythematosus in a white population: dermoscopic characteristics by clinical subtype, lesion location and disease duration. Dermatol Ther. 2022;12(9):2117–2133. Epub 2022 Aug 22. PMID: 35996053; PMCID: PMC9395958. doi:10.1007/s13555-022-00786-y
15. Kumaran MS, Dabas G, Vinay K, Parsad D. Reliability assessment and validation of the dermal pigmentation area and severity index: a new scoring method for acquired dermal macular hyperpigmentation. J Eur Acad Dermatol Venereol. 2019;33(7):1386–1392. Epub 2019 Apr 15. PMID: 30801771. doi:10.1111/jdv.15516
16. Ziolkowski NI, Pusic AL, Fish JS, et al. Psychometric findings for the SCAR-Q patient-reported outcome measure based on 731 children and adults with surgical, traumatic, and burn scars from four countries. Plast Reconstr Surg. 2020;146(3):331e–338e. PMID: 32842115. doi:10.1097/PRS.0000000000007078
17. Yoo J. Differential diagnosis and management of hyperpigmentation. Clin Exp Dermatol. 2022;47(2):251–258. doi:10.1111/ced.14747
18. Anvery N, Christensen RE, Dirr MA. Management of post-inflammatory hyperpigmentation in skin of color: a short review. J Cosmet Dermatol. 2022;21(5):1837–1840. doi:10.1111/jocd.14916
19. Wong ITY, Richer V. Prophylaxis of post-inflammatory hyperpigmentation from energy-based device treatments: a review [Formula: see text]. J Cutan Med Surg. 2021;25(1):77–86. doi:10.1177/1203475420957633
20. Tawfic SO, Abdel Hay R, Salim H, et al. Tranexamic acid versus fractional carbon dioxide laser in post-acne hyperpigmentation. Dermatol Ther. 2021;34(6):e15103. doi:10.1111/dth.15103
21. Zhang Z, Fei Y, Chen X, et al. Comparison of a fractional microplasma radio frequency technology and carbon dioxide fractional laser for the treatment of atrophic acne scars: a randomized split-face clinical study. Dermatol Surg. 2013;39(4):559–566. doi:10.1111/dsu.12103
22. Hirano R, Namazuda K, Suemitsu J, et al. Plasma separation using a membrane. Transfus Apher Sci. 2017;56(5):649–653. doi:10.1016/j.transci.2017.08.008
23. Li N, Zhen Z, Zhang R, et al. Nucleation and growth dynamics of graphene grown by radio frequency plasma-enhanced chemical vapor deposition. Sci Rep. 2021;11(1):6007. doi:10.1038/s41598-021-85537-3
24. Schröder M, Ochoa A, Breitkopf C. Numerical simulation of an atmospheric pressure RF-driven plasma needle and heat transfer to adjacent human skin using COMSOL. Biointerphases. 2015;10(2):029508. doi:10.1116/1.4916929
25. Mogal VT, Yin CS, O’Rorke R, et al. Tuning model drug release and soft-tissue bioadhesion of polyester films by plasma post-treatment. ACS Appl Mater Interfaces. 2014;6(8):5749–5758. doi:10.1021/am500454b
26. Ruff PGT. Thermal effects of percutaneous application of plasma/radiofrequency energy on porcine dermis and fibroseptal network. J Cosmet Dermatol. 2021;20(7):2125–2131. doi:10.1111/jocd.13845
27. Bossart S, Ramelet -A-A, Willenberg T, et al. Skin hyperpigmentation index facilitating quantification of hyperpigmentation in clinical practice. Dermatology. 2021;237(3):486–488. doi:10.1159/000509160
28. Zawodny P, Stój E, Kulig P, et al. VISIA skin analysis system as a tool to evaluate the reduction of pigmented skin and vascular lesions using the 532 Nm laser. Clin Cosmet Invest Dermatol. 2022;15:2187–2195. doi:10.2147/CCID.S380388
29. Maghfour J, Olayinka J, Hamzavi IH, et al. A focused review on the pathophysiology of post-inflammatory hyperpigmentation. Pigm Cell Melanoma Res. 2022;35(3):320–327. doi:10.1111/pcmr.13038
30. Dai S, He S, Huang X, et al. Safety and effectiveness of 5-aminolevulinic acid photodynamic therapy combined with fractional micro-plasma radio-frequency treatment for verrucous epidermal nevus: a retrospective study with long-term follow-up. J Dermatol. 2021;48(8):1229–1235. Epub 2021 Apr 25. PMID: 33896053. doi:10.1111/1346-8138.15923
31. Feng J, Ning J, Zhang L, Li X, Huang L. Microplasma radio frequency technology using stationary tips on pig skin: a histological study. J Cosmet Dermatol. 2024;23(7):2420–2426. Epub 2024 Mar 26. PMID: 38532267. doi:10.1111/jocd.16276
32. Fu M-L, Wu X-Y, Xu P, Chen X-D. Efficacy of microplasma radiofrequency versus CO2 laser therapy for seborrheic keratoses: a randomized, intraindividual comparative study. Dermatol Surg. 2021;47(7):1017–1018. PMID: 33867461. doi:10.1097/DSS.0000000000002896
33. Han J, Wang Z, Lv X, et al. Treatment of atrophic acne scarring with fractional microplasma radiofrequency: a multicentric experience. JPRAS Open. 2024;41:25–32. PMID: 38868740; PMCID: PMC11167203. doi:10.1016/j.jpra.2024.03.016
34. Zuo Y, Li A, He H, Wan R, Li Y, Li L. Assessment of features in facial hyperpigmentation: comparison study between VISIA and CSKIN. Skin Res Technol. 2022;28(6):846–850. Epub 2022 Oct 29. PMID: 36308512; PMCID: PMC9907609. doi:10.1111/srt.13216
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.