")
Back to Journals » Journal of Pain Research » Volume 18
Clinical Efficacy of Single- vs Dual-Level Transversus Abdominis Plane Block for Lower Segment Cesarean Section: A Prospective, Randomized, Controlled Study
Authors Cao WN, Qiu B, Li Y, Hu CL, Liu HC, Yuan KM, Wang FY
Received 6 February 2025
Accepted for publication 21 May 2025
Published 26 May 2025 Volume 2025:18 Pages 2689—2698
DOI https://doi.org/10.2147/JPR.S520944
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Wan-Na Cao,1,2 Bei Qiu,1 Ying Li,1 Chang-Long Hu,1 Hua-Cheng Liu,2 Kai-Ming Yuan,1,2 Fang-Yi Wang1,2
1Department of Anesthesiology, Taizhou Women and Children’s Hospital of Wenzhou Medical University, Taizhou, 318000, People’s Republic of China; 2Department of Anesthesiology and Perioperative Medicine, The Second Affiliated Hospital and Yuying Children’s Hospital of Wenzhou Medical University, Key Laboratory of Pediatric Anesthesiology, Ministry of Education, Wenzhou Medical University, Key Laboratory of Anesthesiology of Zhejiang Province, Wenzhou Medical University, Wenzhou, 325027, People’s Republic of China
Correspondence: Fang-Yi Wang, Email [email protected] Kai-Ming Yuan, Email [email protected]
Objective: Transversus abdominis plane block (TAPB) has been widely used for lower-segment cesarean sections (CS). However, traditional single-level TAPB may not provide sufficient analgesia for parturients. This study aimed to validate whether dual-level TAPB could offer more extensive blocking and better clinical outcomes.
Methods: A total of 114 full-term parturients undergoing lower-segment CS were included in this prospective, randomized, controlled study. Subjects were randomly assigned to receive either single-level (group SL) or dual-level (group DL) TAPB. Dual-level TAPB was performed at the umbilical level and the level above the anterior superior iliac spine, while single-level was performed only at the umbilical level. The primary outcome was the proportion of the abdomen successfully blocked 20 minutes after TAPB.
Results: Twenty minutes after TAPB, dual-level TAPB resulted in a more extensive cutaneous sensory block compared to single-level TAPB. The difference in the proportion of successfully blocked zones was statistically significant, with 46.9% (43.8%, 53.1%) in group SL versus 71.9% (62.5%, 75.0%) in group DL, p < 0.001. Notably, the proportion of parturients with the “surgical area” completely blocked was significantly higher in group DL (94.7%) than in group SL (82.5%) (p = 0.039). Compared to Group SL, the first request for postoperative analgesia was delayed in Group DL by 2.5 hours.
Conclusion: Compared to traditional single-level TAPB, dual-level TAPB produced more extensive cutaneous sensory block and better postoperative analgesia effects.
Keywords: block range, opioid consumption, visual analog scale
Introduction
Despite significant government efforts, the cesarean section (CS) rate in the mainland of China remains high.1 Post-CS pain is a common problem, with a considerable proportion of parturients experiencing moderate to severe pain.2 Acute pain can negatively impact maternal breastfeeding, early ambulation3 and may increase the risk of postpartum depression.4 Furthermore, inadequate pain management may result in the development of hyperalgesia and chronic pain.5,6
Retroperitoneal transverse incision (lower segment CS) is generally preferred over intraperitoneal vertical incision (classical CS)7,8 due to its advantages in adequate pelvic exposure, excellent postoperative strength, and satisfactory cosmetic results. However, iatrogenic injury can be traumatic in lower segment CS, particularly when a transverse incision is combined with an overlooked vertical injury.8 Nerves innervating the abdominal area should be considered for effective postoperative analgesia.
Transversus abdominis plane block (TAPB) has been widely applied for CS analgesia9,10 and is recommended as a major component of multimodal analgesia.11 The intercostal and subcostal nerves penetrate the transversus abdominis plane compartment posterior to the midaxillary line and interconnect,12 allowing for extensive local anesthetics spread and subsequent nerve block.
As gestational age advances, the abdomen of the pregnant woman progressively enlarges and distends, potentially affecting the spread of local anesthetics within the transversus abdominis plane. In addition, evidence has shown that TAPB for CS analgesia is superior to ilioinguinal-iliohypogastric nerve block,13 but less effective than their combination.14 Thus, TAPB performed at a single level may be insufficient. Ilioinguinal-iliohypogastric nerve is the extension of the L1 spinal nerve, which leaves the compartment anterior to the middle third of the iliac crest.12 Thus, this prospective randomized study aimed to validate a hypothesis that TAPB performed at a dual-level may provide more extensive blocking with better clinical outcomes.
Material and Methods
Study Setting
This prospective, randomized controlled study was designed in accordance with the Declaration of Helsinki and approved by the Ethics Review Committee of the Taizhou Women and Children’s Hospital of Wenzhou Medical University (Approval Number:2023-KY004-01) and registered at the Chinese Clinical Trial Registry (chictr.org.cn; ChiCTR2400080644, first registration date: 02/04/2024) before recruitment of the first candidate. Written informed consent was obtained from participants. As a result, 114 parturients were enrolled in the study between February and September 2024. We used the CONSORT checklist when writing our report.15 The CONSORT flowchart is shown in Figure 1.
 |
Figure 1 CONSORT flow chart of included and excluded patients. |
Patients’ Characteristics
Full-term parturients who were scheduled for elective lower segment CS under combined spinal and epidural anesthesia, aged ≥18 years old, with body mass index (BMI) ≤40 kg.m−2 and American Society of Anesthesiologists classification (ASA) I or II, were included.
The following exclusion criteria were implemented in this study: patients with liver and kidney insufficiency, severe cardiopulmonary and cerebral diseases, abnormal coagulation function, infection or damage at the puncture site, peripheral neuropathy, any contradictions to planned anesthesia, and allergy to local anesthetics.
Randomization and Masking
Subjects were randomly assigned to receive either single-level (Group SL) or dual-level (Group DL) TAPB at a 1:1 ratio. The randomization list was generated using computer-generated randomization software by an independent investigator and sealed in sequentially numbered opaque envelopes. Identical opaque envelopes were sequentially numbered, stored by the trial coordinator, and opened immediately prior to TAPB in accordance with the recruitment sequence.
TAPB was performed by an experienced fellow who was unblinded to the group assignment but not involved in subsequent anesthesia management, perioperative care, and postoperative follow-up. The punctured sites in both groups or un-punctured sites for control in group SL were masked with opaque tape. Observers collected patient-reported pain scores and adverse events, which were recorded in the medical charts or through reporting. The observers were not involved in postoperative abdominal assessments and were strictly excluded from observing any procedures within the surgical field. Other healthcare team members and the investigator who was responsible for patient recruitment, data collection, and follow-up assessments were blinded to group assignment.
Intervention
In a pre-anesthesia room, TAPB was performed for the parturient in supine position. Routine monitoring of vital signs was conducted before TAPB. Briefly, an HFL38/13-6 MHz high-frequency linear probe (S-Nerve Sonosite Inc, Bothell, WA, USA) was placed perpendicular to the anterior axillary line for guidance. After clearly identifying the external oblique muscle, internal oblique muscle, and transverse abdominis muscle, the transversus abdominis plane compartment was targeted with a 22G needle with medial-to-lateral direction by using an in-plane technique. Once the needle reached the compartment, confirmed by injection of 0.5 mL of normal saline, 0.375% ropivacaine was injected, and its distribution throughout the fascia layer was observed.
For group SL, bilateral TAPB was performed at the umbilical level and the anterior axillary line, with a total ropivacaine volume of 20 mL at each site. For group DL, additional TAPB was performed bilaterally at the level above the anterior superior iliac spine, with a 10 mL volume of ropivacaine at each site at both levels (four sites). This resulted in a total volume of 40 mL of 0.375% ropivacaine in both groups.
Anesthesia Management
Following the 20-minute TAPB evaluation, participants were transferred to the operating room for combined spinal-epidural anesthesia (CSEA) by another fellow blinded to their group assignment. Standard monitoring of vital signs was applied upon arrival at the operating room, followed by preloading with 10 mL.kg−1 of lactated Ringer’s solution.
In the operating room, CSEA was performed at the L3-4 lumbar intervertebral space using the “needle-through-needle” technique. Briefly, an 18G Tuohy needle was advanced, and epidural space was identified by using the loss of resistance technique to air. A 27G spinal needle was then advanced through the Tuohy needle to perform spinal anesthesia after confirming the free flow of cerebrospinal fluid, and 2.5 mL of 0.5% isobaric ropivacaine was injected. The spinal needle was withdrawn, and the epidural catheter was introduced into the epidural space at the required depth and secured. Before incision, epidural local anesthetics were not routinely administered unless the level of sensory block failed to reach T6 within 15 minutes. Epidural supplementation with short-acting local anesthetic (5 mL of 2% lidocaine, with a minimum interval of 10 min between additional doses) was provided only as needed.
Per protocol, general anesthesia was allowed as a rescue method in cases of CSEA failure or unintentional dural puncture by the Tuohy needle. Standard intraoperative care for CS was followed as outlined in the guidelines.16
Postoperative pain was managed with patient-controlled intravenous analgesia (PCIA). The PCIA pump was programmed to deliver a bolus of 3 μg sufentanil with a lockout time of 10 minutes, without a background infusion.
Outcome Assessments
The primary outcome measure was the proportion of the abdomen successfully blocked 20 minutes after TAPB. Each side of the abdomen was divided into 16 specific dermal zones, modified from Chen’s study and their criteria for successful cutaneous sensory block were followed.17 Cutaneous sensory block was assessed dichotomously (successful/failed) using cold stimulus testing. A block was considered successful if cold sensation was absent or markedly reduced compared to an unblocked area. In the present study, zones were described by vertical lines at the midline (A), midclavicular line (B), anterior axillary line (C), midaxillary line (D), and posterior axillary line (E); and by horizontal lines at the xiphoid level (a), umbilical level (c), pubic symphysis level (e), and lines in-between of lines a and c (b), lines c and e (d), shown in Figure 2.
 |
Figure 2 Abdominal zones and sonogram obtained at different levels. (A) anterior zone. (B) lateral zones. Midline (A), midclavicular line (B), anterior axillary line (C), midaxillary line (D), posterior axillary line (E); and by horizontal lines at the xiphoid level (a), umbilical level (c), pubic symphysis level (e), and lines in-between of lines (a) and (c) (b), lines c and e (d); “×” represents puncture sites. (C), sonogram obtained at umbilical level; (D), sonogram obtained at the level above anterior superior iliac spine level. The asterisk indicates needle target; EO, external oblique muscle; IO, internal oblique muscle; TA, transverse abdominis muscle. The arrows in (C) and (D) indicate the real-time ultrasound-confirmed needle tip location during the procedure. |
The secondary outcome measures included: (1) pain at rest or during movement, measured using the Visual Analogue Scale (VAS), at 3, 6, 9, 12, 16, 20, and 24 hours after TAPB. If VSA ≥ 4, the parturient was encouraged to self-administer sufentanil via PCIA. Additionally, pain originating from uterine contractions, other than incisional pain, was also recorded. (2) linear trapezoidal area under the curve (AUC) was utilized to analyze VAS scores at rest and during movement versus time over 12 and 24 hours. (3) Time to first request for postoperative analgesia by pressing PCIA after TAPB. (4) Number of effective pressings. (5) Sufentanil consumption within 12 and 24 hours after TAPB. (6) Patient satisfaction assessed using a 5-point Likert scale with the following response options: (a) strongly agree, (b) agree, (c) neutral/uncertain, (d) disagree, and (e) strongly disagree. (7) Any adverse events.
Sample Size Estimation and Statistical Analysis
Based on a pilot study of 20 parturients, the proportion of the abdomen successfully blocked 20 minutes after TAPB for single-level and dual-level approaches were approximately 45% and 69%, respectively. A sample size of 57 subjects per group was calculated to provide 80% power to detect a difference between the two approaches with a Type I error of 5% and a dropout rate of 10%, using a one-tailed Z-test.
Statistical analyses were performed using the IBM SPSS 16.0 (IBM Corp, Armonk, New York, USA) for Windows. The normality and homogeneity of variances of data were tested using the Shapiro–Wilk test and Levene’s tests, respectively. Continuous variables with normal distribution were expressed as mean ± SD, nonparametric data were shown as median [range], and categorical data were reported as number (%). Normally distributed data were analyzed using student t test. Nonparametric data were analyzed using the Mann–Whitney U-Test. Categorical data were analyzed using the χ2 test or Fisher’s exact test as appropriate. A p value of 0.05 was considered statistically significant.
Results
Patients’ Characteristics
Of the 132 full-term parturients initially screened for eligibility, 18 were excluded. The remaining 114 parturients, recruited between February and September 2024, were evenly randomized to group SL or group DL and included in the final analysis. All enrolled participants (100%) completed outcome assessments at every predefined time point, as illustrated in the CONSORT flow diagram (Figure 1). The baseline characteristics were generally balanced between the two groups, as detailed in Table 1.
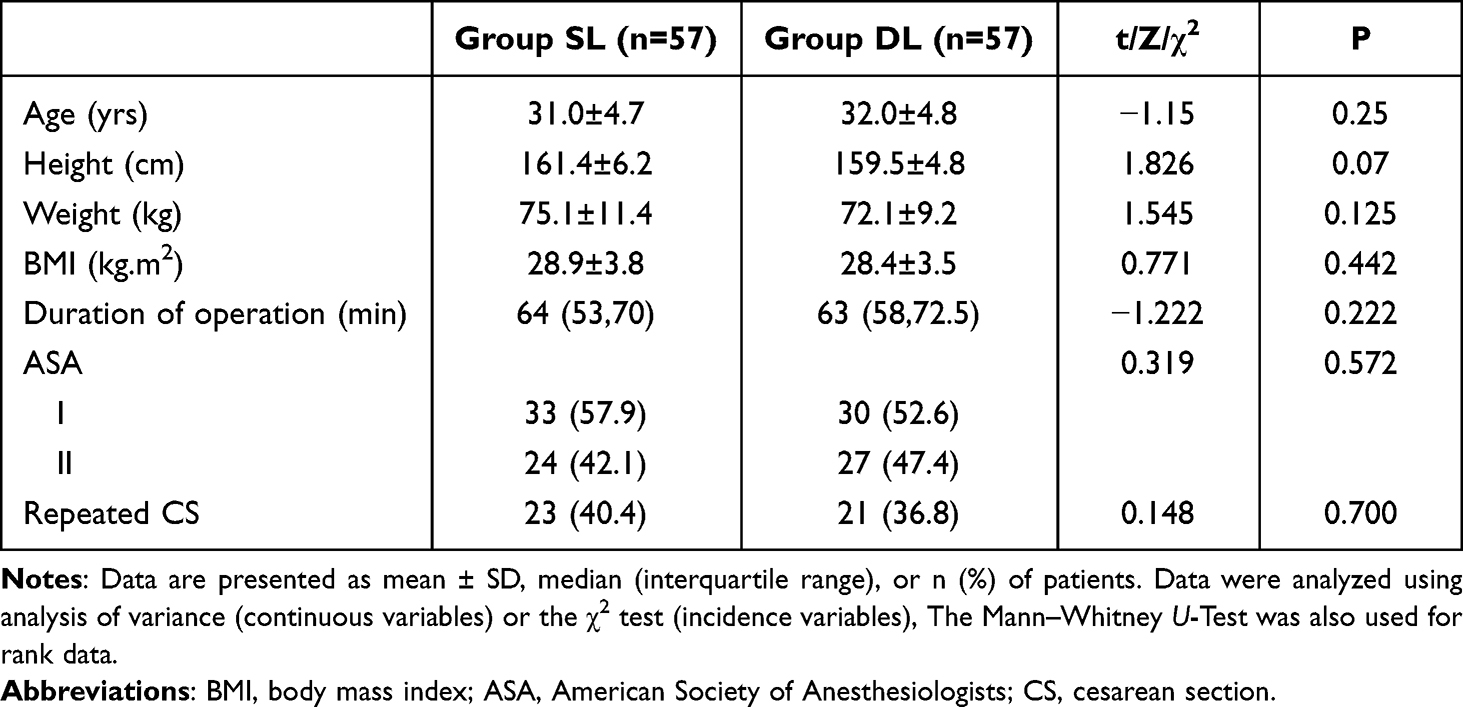 |
Table 1 Patient Demographics and Baseline Characteristics |
Primary Outcome
Twenty minutes after TAPB, dual-level TAPB resulted in a more extensive cutaneous sensory block compared to single-level TAPB. The difference in the proportion of successfully blocked zones was statistically significant, with a median (interquartile range) of 46.9% (43.8%, 53.1%) in group SL versus 71.9% (62.5%, 75.0%) in group DL (p < 0.001). Zones three and four on both sides (Figure 2) were considered most relevant to the incision, defined as the “surgical area” and analyzed further. Notably, the proportion of parturients with the surgical area completely blocked was significantly higher in group DL (94.7%) compared to group SL (82.5%) (p = 0.039).
Secondary Outcome
Compared to group SL, the first request for postoperative analgesia after TAPB was delayed in Group DL by 2.5 hours (p = 0.003). The number of effective pressings, sufentanil consumption within 12 hours (Cliff’s delta = 0.28), and the area under the curve (AUC) for pain VAS scores at rest (Cohen’s d = 0.54) and during movement (Cohen’s d = 0.43) over 12 hours were significantly lower in the DL group. However, the number of effective pressings, sufentanil consumption within 24 hours, and AUC pain VAS score at rest or during movement over 12–24 hours were comparable between the two groups, as shown in Table 2 and Figure 3.
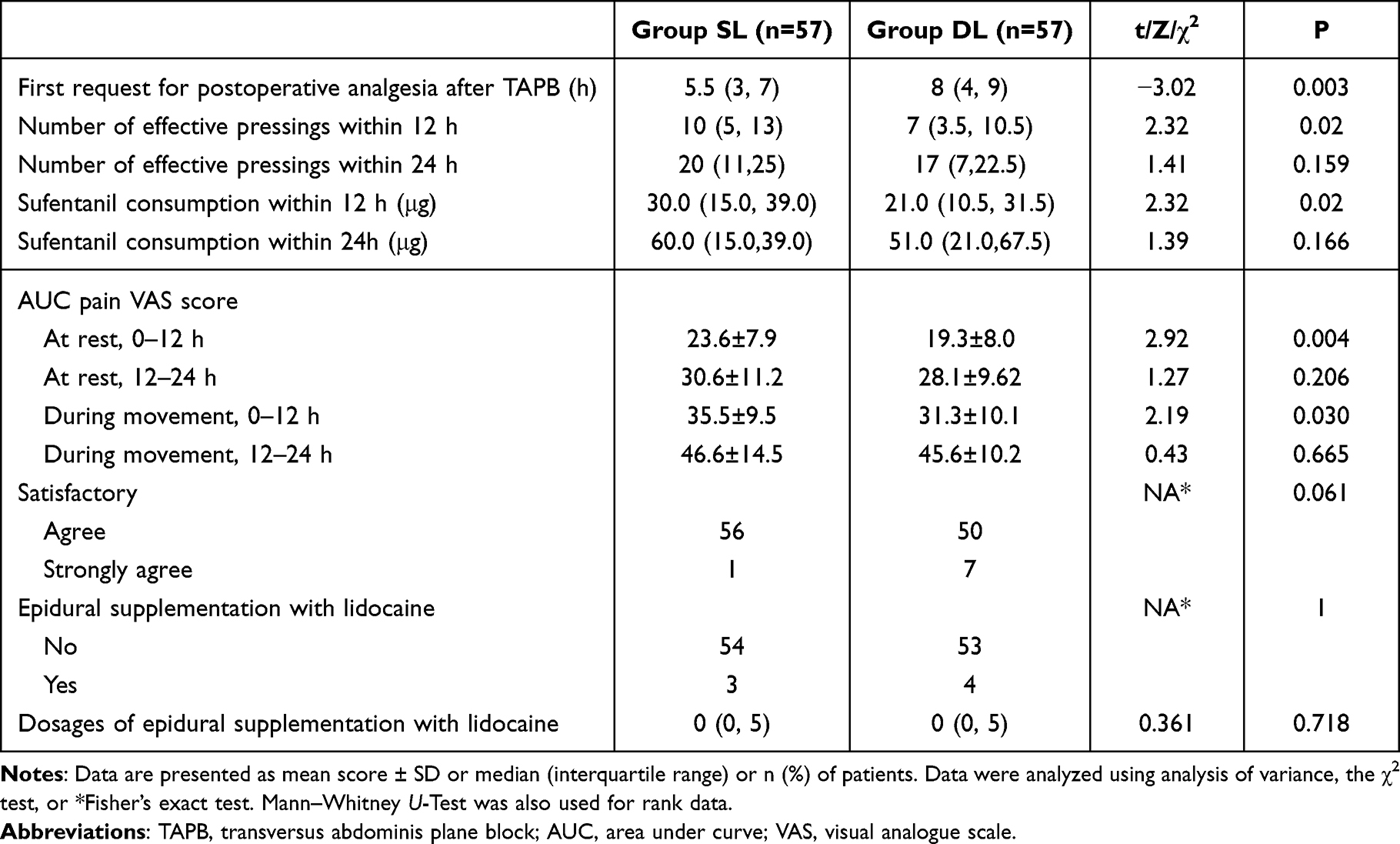 |
Table 2 Secondary Outcomes |
 |
Figure 3 Area under the curve (AUC) of pain VAS at rest or during movement. (A) AUC pain VAS over 12 h at rest; (B) AUC pain VAS over 12 h during movement; (C) AUC pain VAS over 12–24 h at rest; (D) AUC pain VAS over 12–24 h during movement. VAS is the visual analog scale for pain. |
Perioperative Adverse Events
Intraoperative blood loss exceeding 1000 mL occurred in two parturients, one in each group. Both patients received blood transfusions and were discharged after recovery. Supine hypotension was a common adverse event after CSEA, but no significant difference was observed between the two groups (9 in group SL vs 7 in group DL). Loading of fluids and left lateral tilt to 15°–30° was routinely applied prior to incision, and appropriate doses of norepinephrine were administered in case of hypotension.
Discussion
This is the first randomized controlled trial comparing the efficacy of ultrasound-guided dual-level TAPB for cesarean section with the traditional single-level approach, considering aspects of blockage coverage and quality of postoperative analgesia. Our findings demonstrate that dual-level TAPB resulted in more extensive cutaneous sensory block 20 minutes after TAPB compared to single-level TAPB, accompanied by delayed rescue for postoperative analgesia, reduced sufentanil consumption within 12 hours, and lower AUC for pain VAS score over 12 hours.
Analgesia for abdominal surgery can be achieved by blocking nerve transduction along the thoracolumbar nerves. Muscular compartments and fascia are effective targets for blocking because they are easily identified with ultrasound guidance and the extensive spread of local anesthetics within these structures. Various compartment and fascia blocks have been reported for CS, including erector spinae plane block (ESP),18 quadratus lumborum block (QLB),19 TAPB,13,14,20 ilioinguinal-iliohypogastric nerve block,13 and transversalis fascia plane (TFP) block.20 TAPB is the most widely used approach for CS.
The incision for lower segment CS is typically located between the levels of the anterior superior iliac spine and the pubic symphysis. Innervation for a transverse incision in combination with a vertical separation of rectus abdominis muscles may be extensive, as evidenced by the following: First, according to abdomen anatomy, the lower thoracic intercostal and subcostal nerves innervate the infra-umbilical area between the midline and midclavicular lines, lateral cutaneous branches of the T6–T11 spinal nerves supply the lateral abdominal wall between the costal margin and iliac crest and iliohypogastric and ilioinguinal nerves, branches of L1 spinal nerve and T12, supply the anterior abdomen at the level of the inguinal area and the medial thigh.12,21 Second, compared with the lateral approach, the posterior approach of TAPB22 and QLB23 is associated with reduced opioid consumption and reduced pain scores following CS. This may be due to the thoracolumbar nerves being more closely grouped and less branched out in the posterior approach, allowing for easier nerve coverage by the injectate. Third, the lateral approach combined with ilioinguinal-iliohypogastric nerve block offers better postoperative analgesia.14 Taken together, extensive blocking of abdominal innervation is required for lower-segment CS.
The major outcome of this study was the proportion of the abdomen successfully blocked 20 minutes after TAPB. Our results showed that the same volume of local anesthetics successfully blocked up to 71.9% of abdominal zones in group DL compared to 46.9% in group SL. TAPB was straightforward to perform at both levels prior to CS, and the fascial compartments were clearly visualized using ultrasound.
To date, there have been no similar studies on the blocking range after TAPB in parturients. Previous studies have explored TAPB with multiple quadrant injection methods.24–26 Consistent with our findings, separate injections using both intercostal and lateral classic TAPB provided more widespread dermatomal anesthesia than the targeted lateral approach.26 However, a total of 30 mL of 0.375% ropivacaine was used on each side, which was 50% more than the volume used in the present study.
A dosage of 20 mL of 0.2% to 0.375% ropivacaine is commonly applied for TAPB in parturients undergoing CS.22,27 Large dosages of local anesthetics should be avoided due to the potential risk of local anesthetic systemic toxicity. Increasing the injectate volume can expand the spread of the anesthesia, but this can be balanced by using more diluted concentrations of local anesthetic at the same conventional volume. However, lower concentrations may result in a shorter duration of block.28
A “surgical area” was defined in this study as the region between the umbilical level and pubic symphysis, medial to clavicular midlines. Notably, the proportion of parturients with the surgical area completely blocked was significantly higher in group DL (94.7%) compared to group SL (82.5%). This suggests that 20 mL of local anesthetics with the traditional lateral approach of TAPB may not provide sufficient blocking coverage for the incision.
The L1 spinal nerve and its branches, the iliohypogastric and ilioinguinal nerves, are located in the lower abdomen. If the traditional lateral approach of TAPB is planned, a larger volume of local anesthetics or a combination with a block at the lower abdominal compartment or fascia may be necessary, as supported by several studies.20
A recent RCT indicated that TFP block used for analgesic purposes, in comparison with TAPB, yielded a better-quality recovery period with a higher obstetric quality of recovery score and less postoperative opioid consumption.20 However, this superiority under this condition does not necessarily mean that TFP block should replace TAPB but rather be used in combination. This point has been further confirmed by El-Amrawy’s group, which found that combined ilioinguinal-iliohypogastric nerve block offers better postoperative analgesia with a significant delay in the first request for postoperative analgesia.14
Similar to El-Amrawy’s results,14 the combined TAPBs at the umbilical level and the level above the anterior superior iliac spine proposed in the present study showed delayed first request for postoperative analgesia, fewer effective pressings, reduced sufentanil consumption within 12 hours, and lower AUC pain VAS scores over 12 hours at rest or during movement compared to traditional single-level TAPB. These findings further support the value of the dual-level TAPB approach for CS analgesia.
In El-Amrawy’s study, the ilioinguinal and iliohypogastric nerves were blocked using 5 mL of local anesthetic near the deep circumflex iliac artery. In contrast, we performed a lower TAPB using 10 mL of local anesthetic instead of a targeted ilioinguinal and iliohypogastric nerve block. There were two main reasons for this modification. First, both the ilioinguinal and iliohypogastric nerves pierce the transversus abdominis at the anterior aspect of the iliac crest and travel between the transversus abdominis and internal oblique muscles.21 Given this anatomical course, these nerves could be effectively blocked more proximally via a lower TAPB, thus avoiding the need to identify the deep circumflex iliac artery, which was often difficult to visualize. Second, the upper and lower puncture sites were relatively close together, and the spread of local anesthetic along the TAP fascia allowed for a more even distribution of the injectate within the compartment.
There are some limitations to this study. (1) Except for visceral pain resulting from uterine contractions,29 only pain originating from the dermatomal distribution of skin incision and myotome innervation to abdominal wall layers can be blocked by TAPB in parturient after CS. Visceral pain was the major confounding factor for pain measurement-related secondary outcomes. Pain VAS scores during movement may be more specific than those at rest because visceral pain is less relevant to body movement. Alternatively, the low thoracic paravertebral block might provide analgesia for visceral pain with the possible spread of the injectate medially to the epidural space and blocking of visceral pain at the surrounding epidural levels.30 (2) The injectate volume at each side was split evenly for upper and lower TAPB. The optimal proportion for splitting needs further investigation. (3) The puncture sites for upper and lower TAPB were close to each other, which could be further modified by multiple quadrant injection with a single shot at an in-between level. (4) Dual TAPB may provide an even distribution of the injectate within the compartment, although this is difficult to quantify due to the limitations of ultrasound imaging. Future studies could incorporate dose–response evaluations and comparative effectiveness research involving alternative techniques—or combinations with TAPB—such as the quadratus lumborum block and the erector spinae plane block. (5) Multiple injections may increase discomfort for un-anesthetized parturients. Postoperative injection rather than preoperative injection is recommended if analgesia is only required for postoperative purposes.
Conclusion
In conclusion, compared to traditional single-level TAPB, dual-level TAPB performed at the umbilical level and the level above the anterior superior iliac spine produced more extensive cutaneous sensory block with better postoperative analgesia effects.
Data Sharing Statement
The individual de-identified participant data, the study protocol, and the statistical analysis plan can be obtained from the corresponding author upon reasonable request.
Acknowledgments
We thank LetPub (www.letpub.com.cn) for its linguistic assistance during the preparation of this manuscript.
Funding
This study was supported by Zhejiang Provincial Public Welfare Technology Applied Research (LGD22C090002) and Taizhou Science and Technology Bureau (23YWA53).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xia X, Zhou Z, Shen S, et al. Effect of a two-stage intervention package on the cesarean section rate in Guangzhou, China: a before-and-after study. PLoS Med. 2019;16(7):e1002846. doi:10.1371/journal.pmed.1002846
2. Eisenach JC, Pan PH, Smiley R, Lavand’homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
3. O’Carroll J, Carvalho B, Sultan P. Enhancing recovery after cesarean delivery - A narrative review. Best Pract Res Clin Anaesthesiol. 2022;36(1):89–105. doi:10.1016/j.bpa.2022.01.001
4. Lin R, Lu Y, Luo W, Zhang B, Liu Z, Xu Z. Risk factors for postpartum depression in women undergoing elective cesarean section: a prospective cohort study. Front Med. 2022;9:1001855. doi:10.3389/fmed.2022.1001855
5. Loos MJ, Scheltinga MR, Mulders LG, Roumen RM. The Pfannenstiel incision as a source of chronic pain. Obstet Gynecol. 2008;111(4):839–846. doi:10.1097/AOG.0b013e31816a4efa
6. Sun KW, Pan PH. Persistent pain after cesarean delivery. Int J Obstet Anesth. 2019;40:78–90. doi:10.1016/j.ijoa.2019.06.003
7. Kan A. Classical cesarean section. Surg J. 2020;6(Suppl 2):S98–S103. doi:10.1055/s-0039-3402072
8. Gizzo S, Andrisani A, Noventa M, et al. Caesarean section: could different transverse abdominal incision techniques influence postpartum pain and subsequent quality of life? A systematic review. PLoS One. 2015;10(2):e0114190. doi:10.1371/journal.pone.0114190
9. Sultan P, Patel SD, Jadin S, Carvalho B, Halpern SH. Transversus abdominis plane block compared with wound infiltration for postoperative analgesia following Cesarean delivery: a systematic review and network meta-analysis. Can J Anaesth. 2020;67(12):1710–1727. doi:10.1007/s12630-020-01818-x
10. Riemma G, Schiattarella A, Cianci S, et al. Transversus abdominis plane block versus wound infiltration for post-cesarean section analgesia: a systematic review and meta-analysis of randomized controlled trials. Int J Gynaecol Obstet. 2021;153(3):383–392. doi:10.1002/ijgo.13563
11. Roofthooft E, Joshi GP, Rawal N, et al. PROSPECT guideline for elective caesarean section: updated systematic review and procedure-specific postoperative pain management recommendations. Anaesthesia. 2021;76(5):665–680. doi:10.1111/anae.15339
12. Tran DQ, Bravo D, Leurcharusmee P, Neal JM. Transversus abdominis plane block: a narrative review. Anesthesiology. 2019;131(5):1166–1190. doi:10.1097/ALN.0000000000002842
13. Kiran LV, Sivashanmugam T, Kumar VRH, Krishnaveni N, Parthasarathy S. Relative efficacy of ultrasound-guided ilioinguinal-iliohypogastric nerve block versus transverse abdominis plane block for postoperative analgesia following lower segment cesarean section: a prospective, randomized observer-blinded trial. Anesth Essays Res. 2017;11(3):713–717. doi:10.4103/0259-1162.206855
14. El-Amrawy WZ, El-Attar AM. Classical TAP vs. I TAP using the same dose of local anesthetic in elective cesarean section: a randomized controlled trial. Pain Ther. 2024;13(3):495–508. doi:10.1007/s40122-023-00564-4
15. Schulz KF, Altman DG, Moher D, Group C. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332.
16. Caughey AB, Wood SL, Macones GA, et al. Guidelines for intraoperative care in cesarean delivery: enhanced recovery after surgery society recommendations (Part 2). Am J Obstet Gynecol. 2018;219(6):533–544. doi:10.1016/j.ajog.2018.08.006
17. Chen Q, Liang C, Liang J, Qiu J, Yang B. An image study on local anesthetic spread in healthy volunteers receiving subcostal exterior semilunaris transversus abdominis plane (SE-TAP) block. J Pain Res. 2021;14:2013–2019. doi:10.2147/JPR.S316582
18. Malawat A, Verma K, Jethava D, Jethava DD. Erector spinae plane block and transversus abdominis plane block for postoperative analgesia in cesarean section: a prospective randomized comparative study. J Anaesthesiol Clin Pharmacol. 2020;36(2):201–206. doi:10.4103/joacp.JOACP_116_19
19. Mieszkowski M, Janiak M, Borys M, et al. Effect of bilateral quadratus lumborum block type I on patient satisfaction and incidence of chronic postsurgical pain following Cesarean section-A randomized controlled trial. Int J Environ Res Public Health. 2021;18(17):9138. doi:10.3390/ijerph18179138
20. Pinarbasi A, Altiparmak B, Korkmaz Toker M, Pirincci F, Ugur B. Ultrasound-guided transversalis fascia plane block or transversus abdominis plane block for recovery after caesarean section: a randomised clinical trial. Eur J Anaesthesiol. 2024;41(10):769–778. doi:10.1097/EJA.0000000000002041
21. Daniels SP, Viers CD, Blaichman JI, Ross AB, Tang JY, Lee KS. US-guided musculoskeletal interventions of the body wall and core with MRI and US correlation. Radiographics. 2021;41(7):2011–2028. doi:10.1148/rg.2021210050
22. Faiz SHR, Alebouyeh MR, Derakhshan P, Imani F, Rahimzadeh P, Ghaderi Ashtiani M. Comparison of ultrasound-guided posterior transversus abdominis plane block and lateral transversus abdominis plane block for postoperative pain management in patients undergoing cesarean section: a randomized double-blind clinical trial study. J Pain Res. 2018;11:5–9. doi:10.2147/JPR.S146970
23. Blanco R, Ansari T, Riad W, Shetty N. Quadratus lumborum block versus transversus abdominis plane block for postoperative pain after cesarean delivery: a randomized controlled trial. Reg Anesth Pain Med. 2016;41(6):757–762. doi:10.1097/AAP.0000000000000495
24. Borglum J, Maschmann C, Belhage B, Jensen K. Ultrasound-guided bilateral dual transversus abdominis plane block: a new four-point approach. Acta Anaesthesiol Scand. 2011;55(6):658–663. doi:10.1111/j.1399-6576.2011.02430.x
25. Niraj G, Kelkar A, Hart E, et al. Comparison of analgesic efficacy of four-quadrant transversus abdominis plane (TAP) block and continuous posterior TAP analgesia with epidural analgesia in patients undergoing laparoscopic colorectal surgery: an open-label, randomised, non-inferiority trial. Anaesthesia. 2014;69(4):348–355. doi:10.1111/anae.12546
26. Borglum J, Jensen K, Christensen AF, et al. Distribution patterns, dermatomal anesthesia, and ropivacaine serum concentrations after bilateral dual transversus abdominis plane block. Reg Anesth Pain Med. 2012;37(3):294–301. doi:10.1097/AAP.0b013e31824c20a9
27. Mirza F, Carvalho B. Transversus abdominis plane blocks for rescue analgesia following Cesarean delivery: a case series. Can J Anaesth. 2013;60(3):299–303. doi:10.1007/s12630-012-9866-6
28. Christiansen CB, Madsen MH, Molleskov E, Rothe C, Lundstrom LH, Lange KHW. The effect of ropivacaine concentration on common peroneal nerve block duration using a fixed dose: a randomised, double-blind trial in healthy volunteers. Eur J Anaesthesiol. 2020;37(4):316–322. doi:10.1097/EJA.0000000000001112
29. Silverman M, Zwolinski N, Wang E, et al. Regional analgesia for cesarean delivery: a narrative review toward enhancing Outcomes in parturients. J Pain Res. 2023;10(16):3807–3835. doi:10.2147/JPR.S428332
30. Mitchell KD, Smith CT, Mechling C, Wessel CB, Orebaugh S, Lim G. A review of peripheral nerve blocks for cesarean delivery analgesia. Reg Anesth Pain Med. 2019;25:
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.