")
Back to Journals » Orthopedic Research and Reviews » Volume 17
Clinical Outcomes of Methotrexate Usage in Postoperative Arthroplasty Patients: An Evidence Based Review
Authors Koppert J, Heikoop D , Lanting BA
Received 23 February 2025
Accepted for publication 5 June 2025
Published 26 June 2025 Volume 2025:17 Pages 269—274
DOI https://doi.org/10.2147/ORR.S524513
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Clark Hung
Jason Koppert, David Heikoop, Brent A Lanting
Department of Orthopaedic Surgery, Schulich School of Medicine, Western University, London Health Sciences Center, London, Ontario, Canada
Correspondence: Brent A Lanting, London Health Sciences Center, 339 Windermere Road, London, ON, N6A 5A5, Canada, Tel +15196833335, Email [email protected]
Abstract: Patient dissatisfaction after joint arthroplasty remains common. Synovitis is known to contribute to patient dissatisfaction in patients with osteoarthritis. Methotrexate (MTX) is commonly used to prevent joint deterioration in rheumatoid arthritis, however it is much less common in the treatment of osteoarthritic patients. This review explores the effect of MTX on surgical outcomes in the general arthroplasty patient population. While most of the papers reviewed include patients with rheumatoid arthritis, we also review papers that include patients with osteoarthritis and juvenile idiopathic arthritis. Publications were queried in PUBMED and OVID MEDLINE using the following terms: arthroplasty, joint replacement, methotrexate, DMARDs, osteoarthritis, rheumatoid arthritis, arthritis. After applying exclusion criteria, we identified 12 publications for this review. Our results showed no significant increase in revisions or long-term infections were reported in patients taking MTX. One study reported detriment to nerve function with postoperative MTX use. All other studies reported no difference in post-operative pain or function scores. One study investigating the effect of MTX on mobility in rheumatoid arthritis patients following arthroplasty showed improvement in function in patients taking MTX. Thus, based on this review, perioperative MTX use does not appear to worsen arthroplasty outcomes. This review should suffice as a building block for further investigations and trials into MTX’s utility for arthroplasty patients.
Keywords: DMARD, osteoarthritis, rheumatoid arthritis, arthritis, joint replacement
Introduction
Arthroplasty outcomes and patient satisfaction vary depending on the type of arthroplasty. Notably knee arthroplasty can have up to a 19% dissatisfaction rate.1 Many factors contribute to patient dissatisfaction, including infection, malalignment, and of particular interest here: synovitis.2
Synovitis is a common topic of discussion in inflammatory arthropathies like rheumatoid arthritis (RA). In this setting, corticosteroids and disease modifying antirheumatic drugs (DMARDs) such as methotrexate (MTX) are used to treat the inflammation and reduce pain and symptoms. In the context of arthroplasty, MTX has been used in RA patients for several decades with notable effects on overall disease progression and evidence of prolongation of time to arthroplasty.3
Osteoarthritis (OA) is often spoken of as “wear and tear” arthritis, however there is a significant inflammatory component to OA as well. OA is often associated with synovitis as well as immune cell infiltration and high cytokine levels. In fact, worse synovitis has been associated with worse pain4 and altered gait.3 Given the significant effects of synovitis on pain and function in OA patients, some have asked whether OA-related inflammation could also be treated with MTX.4 In a recent prospective randomized controlled trial, 155 patients were administered MTX or a placebo medication for 12 months. In this study, patients in the MTX group had significantly less pain and stiffness and improved function than those in the placebo group, suggesting that oral MTX reduces pain and improves function in patients with OA.4 A subsequent metanalysis looking at 6 randomized controlled trials concluded that MTX was safe and effective in reducing pain and improving function in patients with knee OA.5 Seeing that MTX has been shown to be helpful in the treatment of OA before arthroplasty, it remains to be seen if some post-arthroplasty causes of pain in OA patients could be addressed through MTX.
The use of both steroids and MTX in the perioperative setting has been studied mostly in the setting of RA. In RA, physicians need to balance the theoretical risk of immunosuppression with the need to obtain adequate perioperative symptom control. Within the RA population, patients who have an active RA flare within 6 weeks of total joint arthroplasty have worse pain and function scores at the 1 year post-op mark than those with controlled RA.6 There is extensive evidence to suggest that continuous MTX use in the perioperative elective orthopaedic surgery setting has no effect on wound healing or infection rates.7 The literature surrounding steroid use in the perioperative setting is less clear, however there does not appear to be good evidence to support stopping steroids perioperatively.8 This is reinforced by a study by Ren et al suggesting that patients receiving DMARDs and glucocorticoid agents to control their symptoms in the perioperative period have better functional outcomes than those exclusively taking DMARDs or taking no RA medications at all in the perioperative period.9 Given that perioperative symptom control is important and use of traditional RA treatment modalities like steroids and MTX do not increase complication rates, the available evidence would suggest that these agents should be continued in the perioperative setting.
So far, most of the available research around DMARD use perioperatively focuses on outcomes like wound healing and infection or RA flares. While these are important measures, there is a need for a review of the clinical outcomes such as functional and pain scores associated with MTX in the generalized arthroplasty population. As was already established, MTX has been shown to be effective in treating OA prior to arthroplasty. Given that MTX is not harmful in the perioperative setting, it remains to be seen if there is utility in using MTX to treat post-operative pain in post-operative osteoarthritic joint replacements. This review’s purpose is to review the available literature surrounding the functional impacts of MTX on arthroplasty outcomes and lay the groundwork for additional research on the impacts of MTX on functional outcomes in osteoarthritic joint replacements.
Materials and Methods
Publications were queried using PUBMED and OVID MEDLINE for a list of keyword and MESH heading searches. We used the following terms: arthroplasty, joint replacement, methotrexate, DMARDs, osteoarthritis, rheumatoid arthritis, arthritis, and combinations of these keywords. After removal of duplicates, over 159 results resulted from this initial search strategy. Abstract and title analysis was used to narrow the application of exclusion criteria, any remaining publications were subjected to detailed review. After application of the exclusion criteria as detailed in Figure 1, 12 different publications remained. Search results were generated and reviewed by a second independent reviewer.
 |
Figure 1 Flowchart of included articles. |
Exclusion criteria included infection as an only outcome, case reports, review articles, non-English literature, histopathological or biochemical outcomes only, and follow-up less than 3 months.
Results
The pertinent findings of each paper included in this systematic review are summarized in Table 1. In total, we included 11 retrospective studies and 1 case control study. The number of participants in these papers ranged from 20 patients to 125,525 patients. Follow up times ranged from 6 months to over 18 years, and outcome measures ranged from functional outcomes like ROM to surgical outcomes like the number of revisions. Taken together, the evidence discussed in this review would suggest that MTX use does not lead to worse patient outcomes.
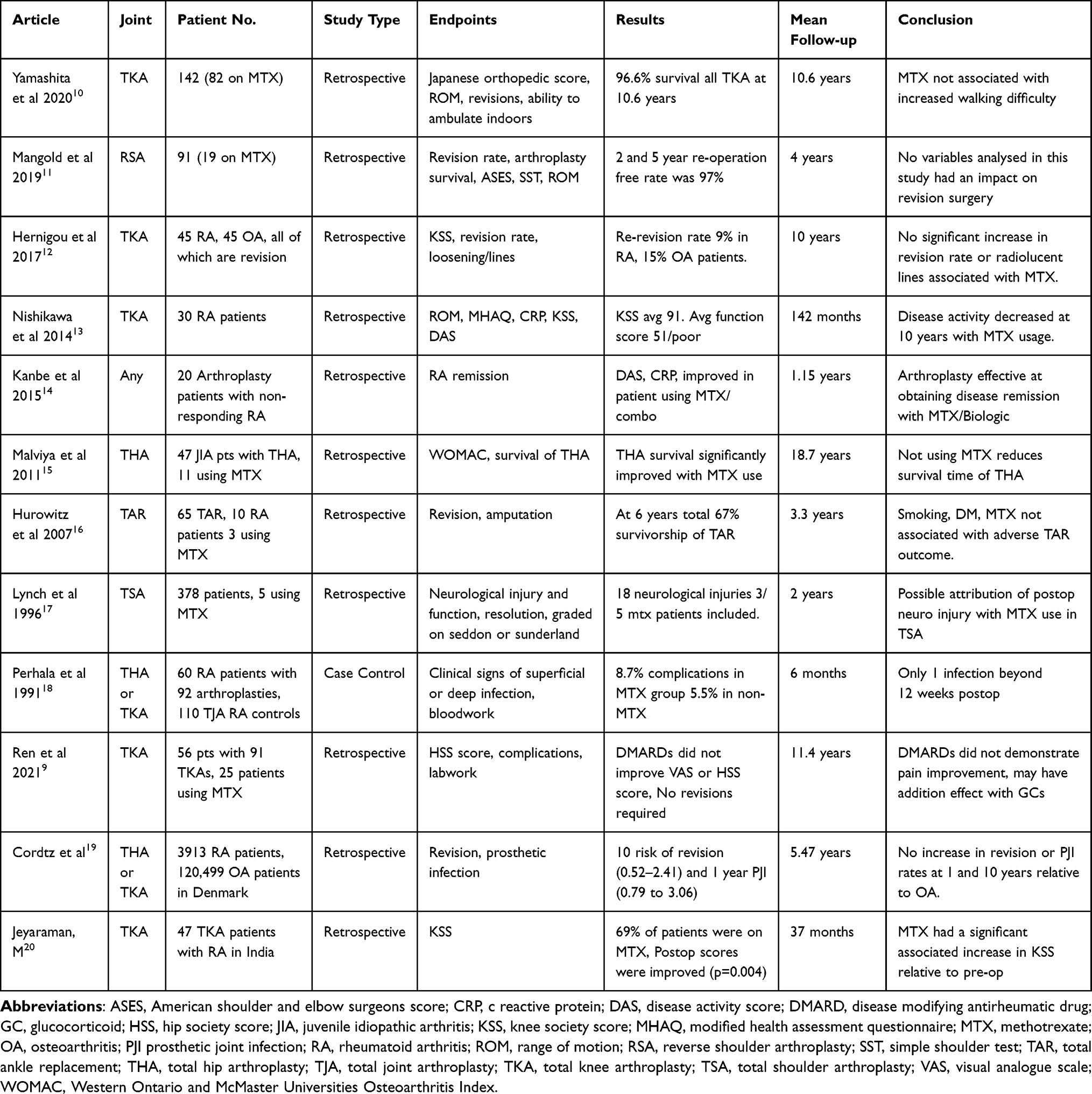 |
Table 1 Detailed Descriptions of the Included Studies |
We used the GRADE system to rank the quality of evidence of each of the studies included in this review.21 These studies are all retrospective in nature, making them inherently “Low” evidence under the GRADE framework. Regarding the outcome of methotrexate, the risk of bias in these studies was high, causing us to further downgrade the evidence quality to “very low” for all studies included in this review. We believe that the poor quality of research available to date reflects the novelty of the clinical question being posed in this review.
Discussion
To date, the evidence surrounding MTX use in arthritis applies mostly to the immediate perioperative period and risk of surgical site infection. This study represents a review of the body of evidence pertaining to clinical outcomes associated with MTX usage. In this review, only one publication reports detriment with regards to nerve function while all other studies reveal no difference in revision rate or postoperative pain and function scores. Here we demonstrate that further research and focus is needed with the potential to perform pilot studies examining the use of MTX as an adjunct for post arthroplasty pain and functional benefit.
Our search included all large joint arthroplasty in order to broaden our search from focusing on a specific large joint. A large body of research generated by our search criteria addressed the concerns around immediate perioperative wound complications of MTX. This question itself has mostly resulted in recommendations for continuation of the drug through the perioperative period.3,11
Only 6 studies presented in Table 1 collected post operative functional data or scoring assessments such as range of motion (ROM), the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), the Hip Society Score (HSS) and the Knee Society Score (KSS). The remainder of the studies focused on long-term incidence of infection and the need for revision surgeries. This highlights a relative paucity of clinically useful research regarding MTX in arthroplasty patients and emphasizes the need for further investigations to explore the impact of MTX on functional outcomes.
An interesting population that surfaced in this search involved juvenile idiopathic arthritis (JIA) patients undergoing arthroplasty. These patients appeared to benefit from methotrexate usage both before and after total joint replacements.15 JIA patients using MTX experienced both prolonged time to arthroplasty and prolonged arthroplasty longevity. Given that JIA patients are much younger than the average arthroplasty patient, the JIA patient population represents an ideal model for the study of MTX effect on long term outcomes.
Another unique aspect from our point of view is the increase in percentage of patients on MTX at the end of the study done Nishikawa et al.10 While this could indicate that the patient population is experiencing worsening RA, it also could mean that the symptoms of pain and function that were tolerable in post-op total knee arthroplasty (TKA) patients could be maintained by these increased doses of MTX.
One study investigating the use of perioperative MTX in total shoulder arthroplasty reported a postoperative increase in neurological complications.17 This study may have been underpowered with only 5 instances of patients with methotrexate seen in that population and 1 patient included twice for separate complications.
Only the study by Jeyaraman et al demonstrated a specific analysis of the effects of MTX on postoperative function scores.20 This represents the most powerful evidence in our collection that MTX may have a specifically beneficial effect for arthroplasty patients.
To our knowledge this review provides the only collection of papers that have been put together regarding the clinical question of whether methotrexate has any effect on metrics such as functional outcomes when used in patients post-arthroplasty. Included here are studies of ankle, shoulder, knee and hip arthroplasties, allowing a starting point for future methotrexate-based research into post-arthroplasty outcomes in each of these settings. This review demonstrates that this question is novel in nature and any specific research put forth towards answering this question is likely to have a large impact on the quality of evidence in this regard.
Significant limitations noted throughout the presented literature involved the vast majority of patients being female, MTX’s effect typically being a subgroup analysis, and poorly powered studies. Additionally, the evidence presented in this review is considered “very low” according to the GRADE system. These limitations may undermine the extraction of clinical conclusions regarding MTX but further emphasize the need for additional primary literature into the topic.
Conclusion
In summary, our search of available evidence presented here represents a better picture of MTX and its effect on arthroplasty outside of the immediate perioperative period. With much of the available body being recent literature, it seems to indicate that there is a role for further research into the specific outcomes of MTX and its clinical effects post arthroplasty. The available research is of very low quality, and heterogenous in population and outcome measures. However, throughout this wide sampling of patients, MTX does not appear to have detrimental effect on arthroplasty outcomes with no significant increase in revisions or long-term infections reported. This review should suffice as a building block for further investigations and trials into MTX’s utility for arthroplasty patients. Our goal in publishing this paper would be to increase the prevalence of MTX use as a sub-analysis of arthroplasty papers with clinical and patient-reported outcome measures.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bourne RB, Chesworth BM, Davis AM, Mahomed NN, Charron KDJ. Patient satisfaction after total knee arthroplasty: who is satisfied and who is not? Clin Orthop Relat Res. 2010;468(1):57–63. doi:10.1007/s11999-009-1119-9
2. Murakami AM, Hash TW, Hepinstall MS, Lyman S, Nestor BJ, Potter HG. MRI evaluation of rotational alignment and synovitis in patients with pain after total knee replacement. J Bone Joint Surg Br. 2012;94-B(9):1209–1215. doi:10.1302/0301-620X.94B9.28489
3. Widdifield J, Moura CA, Wang Y, et al. the longterm effect of early intensive treatment of seniors with rheumatoid arthritis: a comparison of 2 population-based cohort studies on time to joint replacement surgery. J Rheumatol. 2016;43(5):861–868. doi:10.3899/jrheum.151156
4. Kingsbury SR, Tharmanathan P, Arden NK, et al. Pain reduction with oral methotrexate in knee osteoarthritis: a randomized, placebo-controlled clinical trial. Ann Int Med. 2024;177(9):1145–1156. Trials 2015 Mar 4;16(1). doi:10.7326/M24-0303
5. Wong W, Huang Y, Wichienwantana N, Sun H, Pang J, Shi Y. Efficacy and safety of methotrexate in osteoarthritis: a systematic review and meta-analysis of randomized controlled trials. Osteoarthr Cartilage. 2025.
6. Goodman SM, Mirza SZ, DiCarlo EF, et al. Rheumatoid arthritis flares after total hip and total knee arthroplasty: outcomes at 1 year. Arthritis Care Res. 2020;72(7):925–932. doi:10.1002/acr.24091
7. Goodman SM, George MD. Should we stop or continue conventional synthetic (including glucocorticoids) and targeted DMARDs before surgery in patients with inflammatory rheumatic diseases? RMD Open. 2020;6(2):e001214. doi:10.1136/rmdopen-2020-001214
8. Scanzello CR, Figgie MP, Nestor BJ, Goodman SM. Perioperative management of medications used in the treatment of rheumatoid arthritis. HSS J. 2006;2(2):141–147. doi:10.1007/s11420-006-9012-5
9. Ren Y, Yang Q, Luo T, et al. Better clinical outcome of total knee arthroplasty for rheumatoid arthritis with perioperative glucocorticoids and disease-modifying anti-rheumatic drugs after an average of 11.4-year follow-up. J Orthop Surg Res. 2021;16(84):1–9. doi:10.1186/s13018-021-02232-9
10. Yamashita F, Funakoshi N, Mori D, Kizaki K. Long-term outcomes and duration of outdoor ambulation following primary total knee arthroplasty in patients with rheumatoid arthritis. J Orthop Sci. 2022;27(2):414–419. doi:10.1016/j.jos.2021.01.014
11. Mangold DR, Wagner ER, Cofield RH, Sanchez-Sotelo J, Sperling JW. Reverse shoulder arthroplasty for rheumatoid arthritis since the introduction of disease-modifying drugs. Int Orthop. 2019;43(11):2593–2600. doi:10.1007/s00264-019-04373-3
12. Hernigou P, Dubory A, Potage D, Roubineau F, Flouzat-Lachaniette CH. Outcome of knee revisions for osteoarthritis and inflammatory arthritis with postero-stabilized arthroplasties: a mean ten-year follow-up with 90 knee revisions. Int Orthop. 2016;41(4):757–763. doi:10.1007/s00264-016-3319-8
13. Nishikawa M, Owaki H, Takahi K, Fuji T. Disease activity, knee function, and walking ability in patients with rheumatoid arthritis 10 years after primary total knee arthroplasty. J Orthop Surg. 2014;22(1):84–87. doi:10.1177/230949901402200121
14. Kanbe K, Chiba J, Inoue Y, Taguchi M, Yabuki A. Biologic-free remission by orthopaedic surgery in non-responder to infliximab for rheumatoid arthritis. Springerplus. 2015;4(1). doi:10.1186/s40064-015-1397-5
15. Malviya A, Walker L, Avery P, et al. The long-term outcome of Hip replacement in adults with juvenile idiopathic arthritis. J Bone Joint Surg Br. 2011;93-B(4):443–448. doi:10.1302/0301-620X.93B4.26078
16. Hurowitz EJ, Gould J, Fleisig GS, Fowler R. Outcome analysis of agility total ankle replacement with prior adjunctive procedures: two to six year followup. Foot Ankle Int. 2007;28(3):308–312. doi:10.3113/FAI.2007.0308
17. Lynch NM, Cofield RH, Silbert PL, Hermann RC. Neurologic complications after total shoulder arthroplasty. J Shoulder Elbow Surg. 1996;5(1):53–61. doi:10.1016/S1058-2746(96)80031-0
18. Perhala RS, Wilke WS, Clough JD, Segal AM. Local infectious complications following large joint replacement in rheumatoid arthritis patients treated with methotrexate versus those not treated with methotrexate. Arthritis Rheum. 1991;34(2):146–152. doi:10.1002/art.1780340204
19. Cordtz R, Zobbe K, Højgaard P, et al. Predictors of revision, prosthetic joint infection and mortality following total hip or total knee arthroplasty in patients with rheumatoid arthritis: a nationwide cohort study using Danish healthcare registers. Ann Rheum Dis. 2017;77(2):281–288. doi:10.1136/annrheumdis-2017-212339
20. Jeyaraman M, Chaudhary D. Functional outcome of total knee replacement for inflammatory arthritis of knee. J Orthop Trauma Rehabil. 2020;221049172097184.
21. Balshem H, Helfand M, Schunemann HJ, et al. GRADE guidelines: 3. Rating the quality of evidence. J Clin Epidemiol. 2011;64(4):401–406. doi:10.1016/j.jclinepi.2010.07.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum Collagen Triple Helix Repeat Containing-1 Levels are Related to Radiological Affection and Disease Activity in Rheumatoid Arthritis
Nassef EM, Elabd HA, Elzomor HM, El Nagger BMMA, Ibrahim AS, Ibrahim AH, Kotb HG, Hassan DA, Abd ElAziz REM, Mohamed EES
Open Access Rheumatology: Research and Reviews 2022, 14:291-299
Published Date: 9 December 2022
The m6A/m1A/m5C-Related Methylation Modification Patterns and Immune Landscapes in Rheumatoid Arthritis and Osteoarthritis Revealed by Microarray and Single-Cell Transcriptome
Zheng H, Aihaiti Y, Cai Y, Yuan Q, Yang M, Li Z, Xu K, Xu P
Journal of Inflammation Research 2023, 16:5001-5025
Published Date: 1 November 2023
Immune Cell-Derived Exosomes in Inflammatory Disease and Inflammatory Tumor Microenvironment: A Review

Zhang R, Li M, Li H, Ran X, Jin F, Tan Q, Chen Z
Journal of Inflammation Research 2024, 17:301-312
Published Date: 17 January 2024
The Hippo-YAP Signaling Pathway in Osteoarthritis and Rheumatoid Arthritis
Li M, Zhang FJ, Bai RJ
Journal of Inflammation Research 2024, 17:1105-1120
Published Date: 19 February 2024
Network Analysis of Osteoarthritis Progression Using a Steiner Minimal Tree Algorithm
Xie Y, Shao F, Ji Y, Feng D, Wang L, Huang Z, Wu S, Sun F, Jiang H, Miyamoto A, Wang H, Zhang C
Journal of Inflammation Research 2024, 17:3201-3209
Published Date: 18 May 2024