")
Back to Journals » Cancer Management and Research » Volume 17
Clinical Remission Rates in Patients With Epithelial Ovarian Cancer Before and After the Onset of the COVID 19 Pandemic in an Integrated Healthcare Delivery System
Authors Mukherjee A, Ayoub N , Xu L, Cannavale KL, Gilfillan AD, Szamreta EA, Monberg MJ, Hodeib M, Chao CR
Received 30 August 2024
Accepted for publication 18 January 2025
Published 12 February 2025 Volume 2025:17 Pages 281—291
DOI https://doi.org/10.2147/CMAR.S487894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Amrita Mukherjee,1 Natalie Ayoub,2 Lanfang Xu,3 Kimberly L Cannavale,1 Alec D Gilfillan,1 Elizabeth A Szamreta,4 Matthew J Monberg,4 Melissa Hodeib,5 Chun R Chao1,6
1Department of Research & Evaluation, Kaiser Permanente Southern California, Pasadena, CA, USA; 2Department of Obstetrics and Gynecology, Adventist Health White Memorial Medical Center, Los Angeles, CA, USA; 3MedHealth Analytics Inc., Sugar Land, TX, USA; 4Outcomes Research, Merck & Co., Inc., Rahway, NJ, USA; 5Obstetrics & Gynecology Department, Kaiser Permanente Southern California, Riverside, CA, USA; 6Department of Health Systems Science, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, CA, USA
Correspondence: Chun R Chao, Department of Research and Evaluation, Kaiser Permanente Southern California, 100 S Los Robles Ave, Pasadena, CA, 91101, USA, Tel +1 626 564 3797, Fax +1 626 564 3409, Email [email protected]
Purpose: Evidence on the impact of the coronavirus disease 2019 (COVID-19) pandemic on outcomes in patients with ovarian cancer patients is limited. We compared remission outcomes in patients with ovarian cancer before and during the pandemic.
Patients and Methods: This retrospective cohort study included patients diagnosed with epithelial ovarian cancer between 01/01/2017 and 06/30/2021 at Kaiser Permanente Southern California. Pre and post pandemic periods were designated using March 4, 2020, as the cut-off. Stage I–IV patients who completed chemotherapy and/or surgery as first-line treatment were included. Data on remission outcomes (complete and clinical remission) were abstracted by manual chart reviews. Complete remission was defined as no evidence of disease; clinical remission included both complete and partial response to treatment. Modified Poisson regression was used to evaluate the association of pandemic and remission. Effect modification by race/ethnicity was evaluated.
Results: Of 748 ovarian cancer patients included, 72.7% and 27.3% patients were diagnosed before and during the pandemic, respectively. Complete remission was observed in 75.7% and 73.5% patients before and during the pandemic, respectively (p = 0.53). No statistically significant association of pandemic period with remission outcomes was observed in the adjusted models. However, race/ethnicity modified the association of pandemic period with complete remission (p-value < 0.01). White patients, but not other racial/ethnic groups, were 13% more likely to achieve complete remission during the pandemic than during the pre-pandemic [adjusted rate ratio (95% confidence interval): 1.13 (1.00– 1.28)].
Conclusion: Patients diagnosed with ovarian cancer achieved similar complete and clinical remission rates before and during the pandemic. Association of the pandemic period with complete remission varied for White vs non-White patients.
Keywords: ovarian cancer, COVID-19 pandemic, clinical remission, complete remission, race and ethnicity
Introduction
The COVID-19 pandemic brought unprecedented disruptions in the delivery of care across the globe. Care in cancer patients was particularly affected following recommendations to minimize potential COVID-19 exposure in these vulnerable, immunocompromised populations.1 Discontinuation of cancer screening programs, delays in cancer diagnosis and treatment initiation, altered treatment recommendations during the course of treatment, and delay in active cancer surveillance were reported after the onset of the pandemic in the United States (US).1–4 Patients with ovarian cancer, the most lethal gynecologic cancer among women, were no exception.5
A study conducted among gynecologic oncology patients, including patients with ovarian cancer, at three affiliated New York City hospitals reported a treatment delay, change in treatment plans or treatment cancellation during the first two months of the COVID-19 pandemic.6 Changes were reported in ovarian cancer treatment recommendations following the onset of the pandemic. To reduce COVID-19 exposure and surgery-related complications and hospitalizations, the American College of Surgeons (ACS) categorized ovarian cancer interval cytoreductive surgery, often the first line treatment choice, as “semi-urgent”.7 At the same time, to accommodate for delays in surgery and to reduce harm in patients with ovarian cancer, the national and international gynecologic oncology societies recommended preferential use of neoadjuvant chemotherapy during the pandemic.7–9 Although previous studies have reported on the adoption of altered treatment recommendations in ovarian cancer care,10–12 the impact of the COVID-19 pandemic on ovarian cancer outcomes remains under-studied.13
Besides treatment adaptations to meet the safety needs during the pandemic, the pandemic may also have negative impacts on patient outcomes through other mediators, such as changing household income and/or loss of insurance, and health care utilization barriers independent of insurance coverage, such as more limited options for transportation or childcare. To our knowledge, remission rates of ovarian cancer before and after the onset of the COVID-19 pandemic has not been extensively compared and reported.
To inform whether patients achieved similar rates of remission in the context of the pandemic, given altered treatment recommendations and patient-level socioeconomic factors, the objective of this study was to assess the association of the COVID-19 pandemic with cancer remission after completion of the first course of treatment in patients newly diagnosed with epithelial ovarian cancer at a large integrated healthcare delivery system.
Materials and Methods
Study Design, Setting, and Subjects
This retrospective cohort study was conducted at Kaiser Permanente Southern California (KPSC), the largest not-for profit healthcare organization in California, that serves more than 4.7 racially/ethnically and socioeconomically diverse members. Initially, 1047 patients diagnosed with incident epithelial ovarian cancer between January 1st, 2017 and June 30th, 2021 at KPSC were identified. Patients diagnosed with epithelial type ovarian cancer between 2017 and 2020 were identified from KPSC’s Surveillance, Endpoints, and End Results (SEER)-affiliated cancer registry. Patients diagnosed in 2021 were initially identified from KPSC’s electronic medical records (EMR) using ICD-10 diagnosis codes and subsequently confirmed by chart review. Patients who were diagnosed with COVID-19 anytime between ovarian cancer diagnosis and ovarian cancer treatment completion (first course of treatment) were excluded. This was done to reduce confounding by cancer treatment delays/interruptions following COVID-19 diagnosis. Finally, 748 patients with epithelial ovarian cancer were included in the analysis based on the following inclusion criteria: a) patients were aged 18–89 years at the time of incident ovarian cancer diagnosis, b) were active members of KPSC health plan at the time of ovarian cancer diagnosis, c) did not have any prior ovarian cancer diagnosis, d) did not have another cancer diagnosis within six months prior to their incident ovarian cancer diagnosis, e) had no missing information on age at diagnosis, cancer stage, and/or race/ethnicity, f) had at least 12 months of KPSC membership prior to ovarian cancer diagnosis, g) did not terminate KPSC membership within 12 months after ovarian cancer diagnosis, h) received ovarian cancer treatment at KPSC, i) received chemotherapy or surgery as the first line of treatment, and j) had follow-up evaluations to allow assessment of remission outcomes (Figure 1).
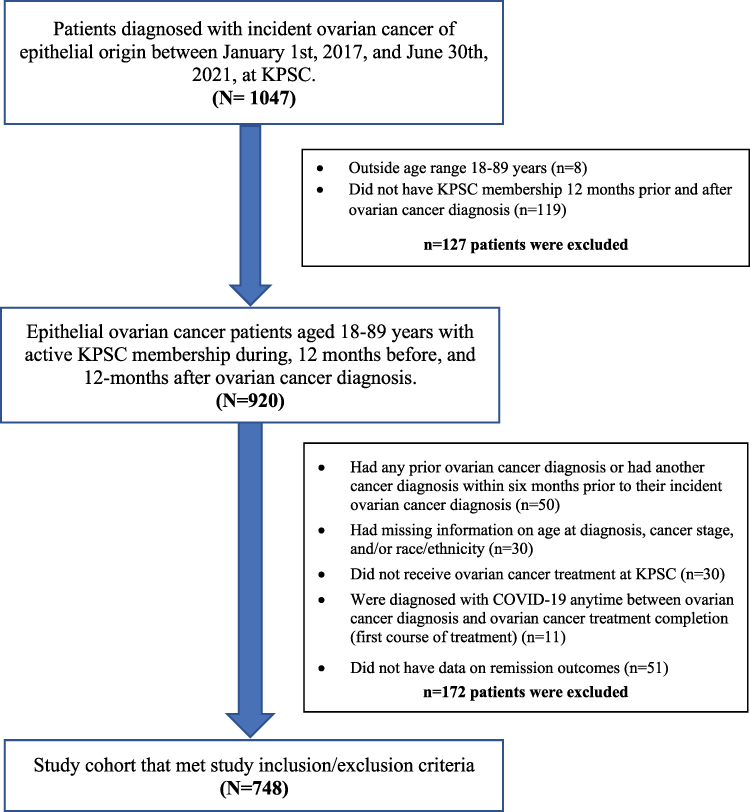 |
Figure 1 Flowchart showing study population of patients diagnosed with epithelial ovarian cancer between January 1st, 2017, and June 30th, 2021, at Kaiser Permanente Southern California. |
The study was approved by KPSC’s institutional review board (IRB). Due to the use of secondary, de-identified data, the requirement for written or verbal consent was waived. The data that support the findings of this study are not publicly available; however, data can be made available from the corresponding author upon reasonable request.
Data Collection
Data on ovarian cancer-related variables, including date of diagnosis, cancer stage, histology type, and treatment were extracted from KPSC’s SEER-registry and EMR, as appropriate, for patients diagnosed in 2017–2020. For patients diagnosed in 2021, International Classification of Diseases-10 (ICD-10) diagnosis codes (C56, C56.1, C56.2, C56.3, and C56.9) were used to identify ovarian cancer patients from KPSC’s EMR. Medical chart reviews were conducted manually to validate ovarian cancer diagnosis and to extract information on cancer histology and stage in patients identified from the EMR. Remission outcomes were also abstracted from standardized manual chart review using pre-specified definition (see below). For patients diagnosed in 2021, data on ovarian cancer treatment, including use of neoadjuvant chemotherapy, were obtained from EMR, supplemented by chart review. Data on sociodemographic and other clinical variables were extracted from the EMR.
Outcome, Exposure, and Covariates of Interest
Remission after completion of first course of ovarian cancer treatment was the outcome of interest. Remission outcomes included both complete and clinical remission. Complete remission was defined by the following: imaging (PET or CE scan) showing no evidence of disease; normal CA 125 values, or a physician note documenting confirmed complete remission following first-line treatment. Clinical remission included both complete remission and partial response. Partial response was defined as an incomplete/partial response to therapy. Remission outcomes were ascertained using medical records through 12 months from completion of first course of treatment for each study patient. Ten percent of the patients were double reviewed by two research staff for quality assurance. Our main exposure of interest was the COVID-19 pandemic period; pre-pandemic and pandemic periods were defined based on the cutoff date of implementation of stay-at-home order in California: March 4, 2020.
Covariates of interest included age at cancer diagnosis, race/ethnicity, cancer stage (FIGO), cancer histologic subtype, days from cancer diagnosis to treatment initiation, KPSC membership years prior to ovarian cancer diagnosis, overall comorbidity burden, and neighborhood deprivation index (NDI). Cancer stage included FIGO stages I–IV. Overall comorbidity burden was defined using the modified Charlson Comorbidities Index (CCI).14 Diagnosis of ovarian cancer was excluded from the CCI and unweighted scores based on comorbidities recorded in the EMR within 12 months prior to ovarian cancer diagnosis were reported.14 Neighborhood deprivation index (in quartiles), a measure for neighborhood socioeconomic status (SES), was derived from the American Community Survey 2015–2019 5-year estimates; using the methodology previously described.15
Statistical Analysis
Patient demographics and cancer characteristics for the overall study population and by the pandemic periods were reported using frequency (percentage) or mean (standard deviation); Chi-square and t-test p-values were reported, as appropriate. Since most of the remissions were achieved within 12 months of treatment completion, we focused on whether remission was achieved (a binary outcome) rather than time from treatment completion to remission. Because remission was not a rare outcome, we used modified Poisson regression with robust error variance to estimate rate ratios. Bivariate (crude) and multivariable (adjusted) models were performed to estimate associations of pandemic period with clinical and complete remission. In the adjusted models, potential confounders including age, race/ethnicity, stage, and covariates with crude p-value <0.10 in bivariate models were included. Since racial/ethnic disparities in ovarian cancer outcomes are well documented, a two-way interaction term between race/ethnicity and pandemic period were included in the adjusted model to check for potential effect modification by race/ethnicity. Level of significance was set at 0.05 and two-sided p-values were reported. All analyses were conducted in SAS version 9.4 (Cary, NC).
Results
Characteristics of the Study Population
Sociodemographic and clinical characteristics of the study population are shown in Table 1. Of 748 ovarian cancer patients included, 72.7% were diagnosed during the pre-pandemic period and 27.3% were diagnosed during the pandemic period. Patients diagnosed during the pandemic period were slightly younger than patients diagnosed in the pre-pandemic period [mean age 60.9 vs 62.6 years, respectively, p-value=0.11]. Overall, 46.8% patients were non-Hispanic White, followed by 33.0% Hispanic patients, 12.4% Asian/Pacific Islander/other races, and 7.5% non-Hispanic Black patients. Overall, FIGO stage III was the most common stage at cancer diagnosis (39.6%), followed by FIGO Stage I (27.8%), FIGO stage IV (21.5%), and FIGO stage II (11.1%). Overall, serous carcinoma was the most common cancer histologic subtype (57.4%). No statistically significant differences in race/ethnicity (p-value=0.09), FIGO stage (p-value=0.65), time to treatment initiation (p-value=0.71), CCI (p-value=0.11), NDI (p-value=0.62), and prior KPSC membership (p-value=0.82) were observed before and during the pandemic. Overall, 87.2% patients achieved clinical remission and 75.1% achieved complete remission after completion of first therapy; 12.8% patients did not respond to treatment. No statistically significant difference was observed in the unadjusted proportion of patients achieving clinical remission before and during the pandemic (87.7% vs 85.8%, respectively, p-value=0.49). Proportion of patients achieving complete remission before and during the pandemic was 75.7% and 73.5%, respectively (p-value=0.53).
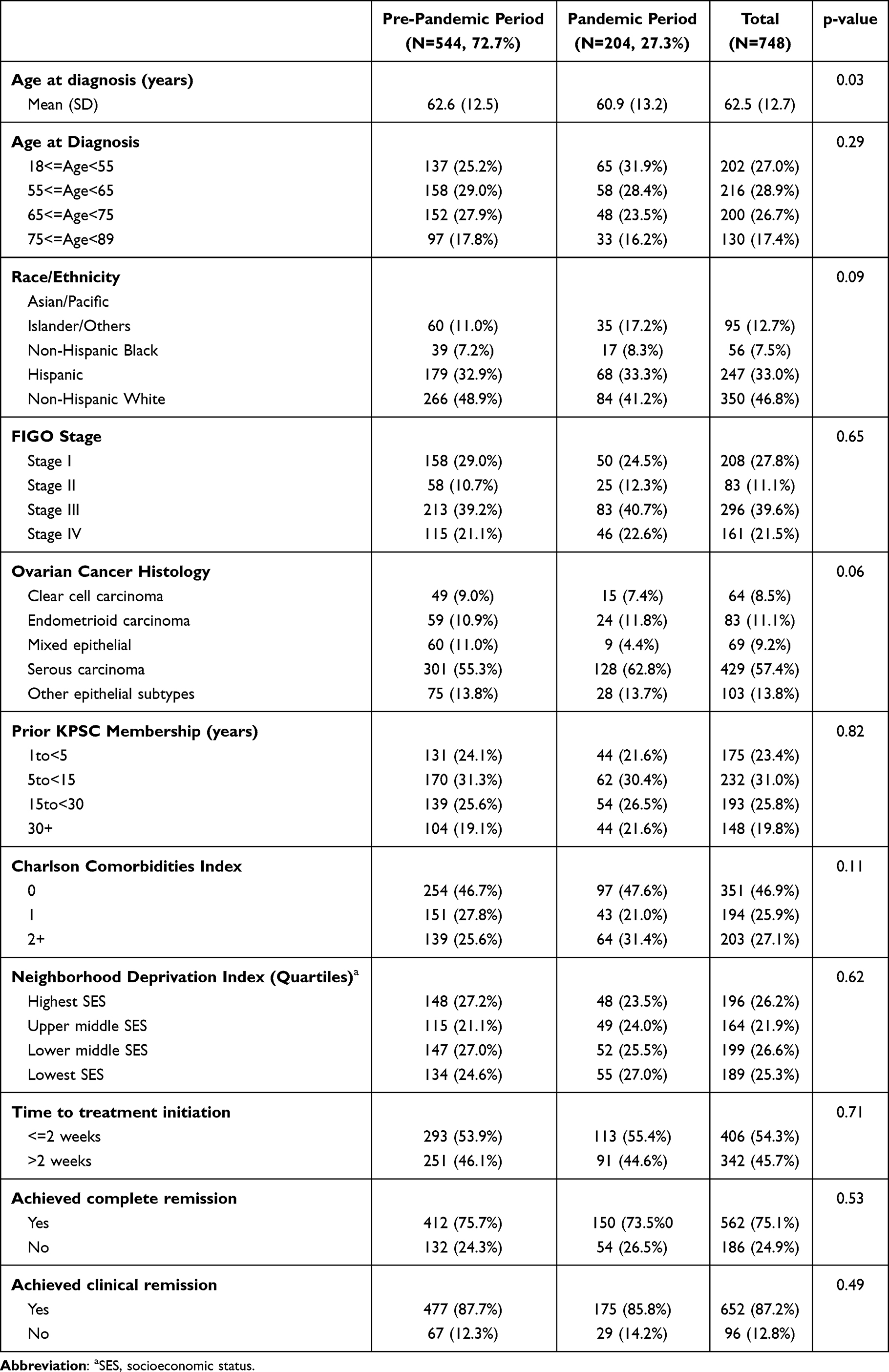 |
Table 1 Table Showing Sociodemographic and Clinical Characteristics of Patients Diagnosed With Epithelial Ovarian Cancer by the COVID-19 Pandemic Periods |
Complete Remission
Bivariate and multivariable associations of pandemic period and other covariates of interest with remission outcomes are shown in Table 2. In the bivariate model, pandemic period was not associated with complete remission [RR (95% CI): 0.97 (0.88–1.07)] (Figure 2). In the multivariable model, no association of the pandemic period with complete remission was observed after adjusting for age, race/ethnicity, FIGO stage, CCI, prior membership, and time to treatment initiation [adjusted RR (95% CI: 0.98 (0.90–1.06)]. Compared to non-Hispanic White patients, non-Hispanic Black patients were slightly less likely to achieve complete remission [adjusted RR (95% CI): 0.84 (0.68–1.04)]. Patients with FIGO stages III and IV were 21% and 36% less likely to achieve complete remission, than stage I patients, respectively [adjusted RR (95% CI): 0.79 (0.73–0.86) and 0.64 (0.55–0.75), respectively]. Patients with CCI score = 1 and 2+ were 16% and 19% less likely to achieve complete remission than patients with no Charlson comorbidities, respectively [adjusted RR (95% CI): 0.84 (0.77–0.92) and 0.81 (0.72–0.91), respectively]. Patients who initiated treatment >2 weeks after diagnosis were less likely to achieve complete remission than patients who initiated treatment within 2 weeks [adjusted RR (95% CI): 0.84 (0.76–0.93)].
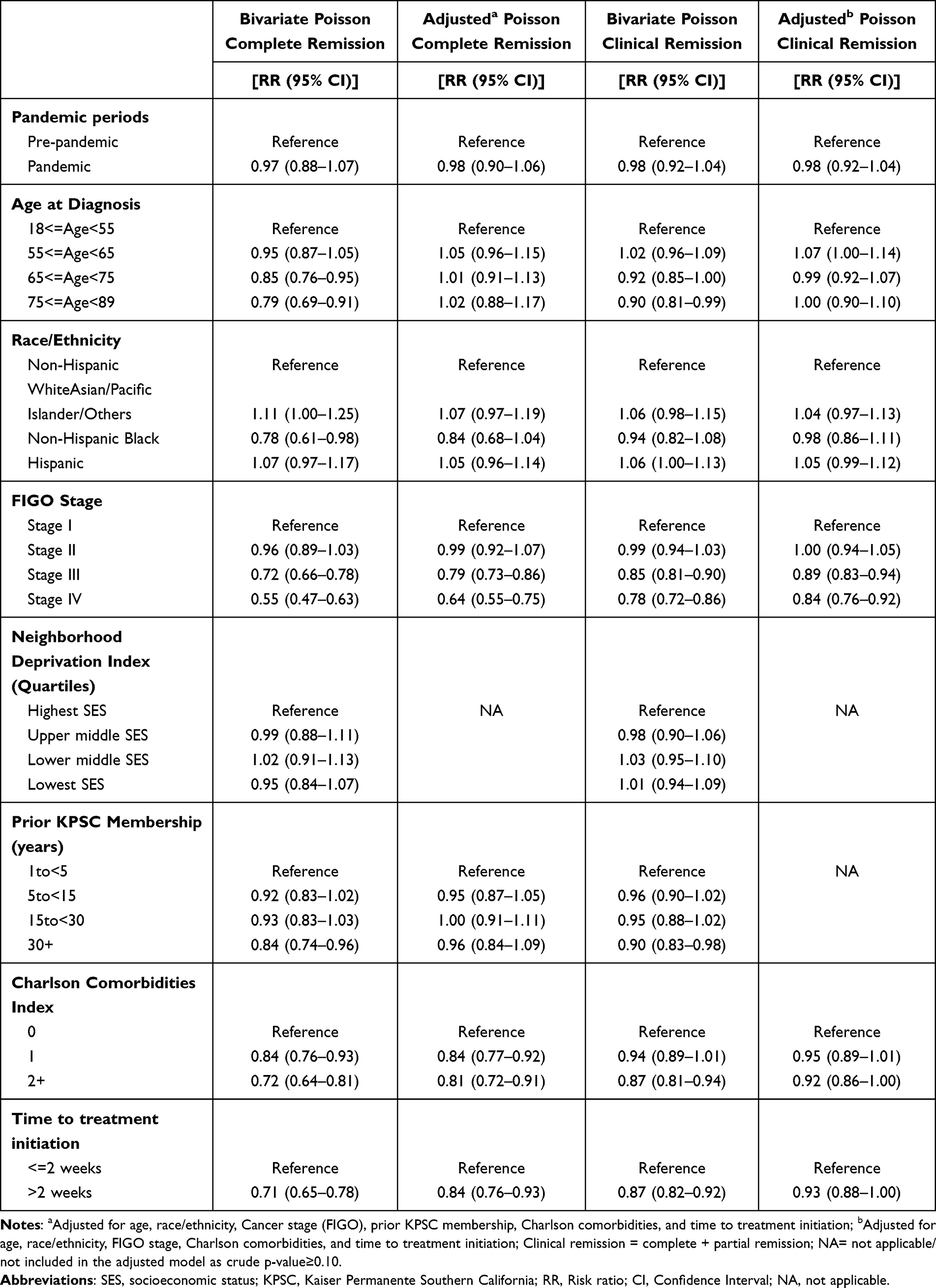 |
Table 2 Bivariate and Multivariable Association of the COVID-19 Pandemic With Complete and Clinical Remission After Completion of First Course of Ovarian Cancer Treatment |
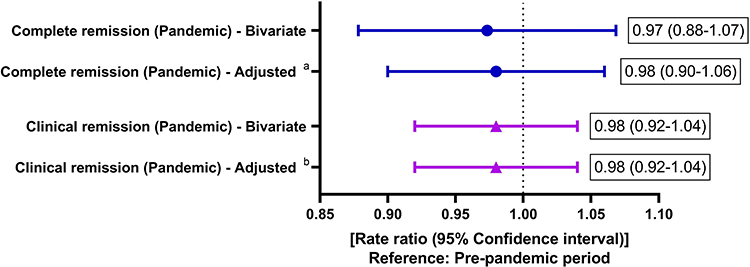 |
Figure 2 Forest plot showing bivariate and adjusted association of the pandemic periods with complete and clinical remission. Notes: aAdjusted for age, race/ethnicity, cancer stage (FIGO stage), prior KPSC membership, Charlson comorbidities, and time to treatment initiation. bAdjusted for age, race/ethnicity, cancer stage (FIGO stage), Charlson comorbidities, and time to treatment initiation. |
Clinical Remission
Pandemic period was not associated with clinical remission in bivariate or multivariable models (Table 2 and Figure 2). In the multivariable model, after adjusting for pandemic period, age, race/ethnicity, CCI, and time to treatment initiation, patients with FIGO stages III and IV were less likely to achieve clinical remission than patients with FIGO stage I [adjusted RR (95% CI): 0.89 (0.83–0.94) and 0.84 (0.76–0.92), respectively]. Patients who initiated treatment >2 weeks after diagnosis were slightly less likely to achieve clinical remission than patients who initiated treatment within 2 weeks [adjusted RR (95% CI): 0.93 (0.88–1.00)].
Effect Modification by Race/Ethnicity
The multivariable association of pandemic period with complete remission was modified by race/ethnicity (interaction p-value <0.01). After adjusting for age, FIGO stage, CCI, prior membership, and time to treatment initiation, non-Hispanic White patients during the pandemic period were 13% more likely to achieve complete remission than in the pre-pandemic period [RR (95% CI): 1.13 (1.00–1.28)]. No statistically significant differences in rates of complete remission during the pandemic period versus the pre-pandemic period were observed in Asian/Pacific Islander/other races [RR 95% CI): 0.96 (0.79–1.16)], non-Hispanic Black [RR (95% CI): 0.56 (0.29–1.06)], and Hispanic patients [RR (95% CI): 0.89 (0.76–1.04)]. The association of the pandemic periods with clinical remission was not modified by race/ethnicity (interaction p-value=0.90) (data not shown).
Discussion
In patients newly diagnosed with epithelial ovarian cancer at an integrated healthcare delivery system, rates of complete and clinical remission did not differ before and during the COVID-19 pandemic. No statistically significant associations were observed between race/ethnicity and remission outcomes in the adjusted model; however, the association of pandemic periods with complete remission varied by race/ethnicity. While Non-Hispanic White patients were more likely to achieve complete remission during the pandemic period than in the pre-pandemic period, no such association was observed in patients of other races/ethnicities. To our knowledge, this is the first study to evaluate the association of the COVID-19 pandemic with remission outcomes in patients with ovarian cancer.
Prior studies have reported significant delays in treatment initiation and modifications in treatment management after the onset of the pandemic in patients with epithelial ovarian cancer.6,10,16,17 However, evidence on the impact of the pandemic on ovarian cancer outcomes is limited and conflicting.10,13 In a multi-center, prospective cohort study, Fotopoulou et al demonstrated an increase in adverse outcomes, including disease progression and death, after the onset of the pandemic in patients with ovarian cancer.13 On the other hand, Algera et al reported no statistically significant differences in rates of postoperative complications and 30-day mortality in Dutch ovarian cancer patients during the pandemic.10 Antunes et al also reported no differences in post-operative complication rates before and after the onset of the pandemic,11 Although, none of these studies assessed ovarian cancer remission rates as the outcome of interest, Algera et al’s and Antunes et al’s studies provide evidence indicating no inferior patient outcomes during the COVID-19 pandemic.10,11 Our study adds to the evidence of comparable patient outcomes before and after the pandemic; we observed no differences in complete and clinical remission rates by pandemic period in the bivariate and multivariable analyses. However, unlike Algera et al’s and Antunes et al’s studies that included predominantly White ovarian cancer patients of European ancestry,10,11 our study cohort consisted of >50% patients of color.
Even though we did not observe any statistically significant racial/ethnic differences in ovarian cancer remission rates, non-Hispanic Black patients were slightly less likely to achieve complete remission compared to non-Hispanic White patients. Historically, non-Hispanic Black patients are less likely to receive guideline-appropriate treatment for ovarian cancer compared to non-Hispanic White patients.18 Differences in treatment quality, ovarian cancer molecular characteristics, socioeconomic characteristics, and access to care by race/ethnicity have attributed to survival disparities in patients with ovarian cancer.18 Since our cohort included insured patients in an integrated healthcare system with equal access to care, racial/ethnic disparities in remission rates were less evident in our cohort. However, the association of pandemic period with complete remission was modified by race/ethnicity. Non-Hispanic White patients were more likely to achieve complete remission during the pandemic period than during the pre-pandemic period, after adjusting for age, FIGO stage, CCI, and time to treatment initiation; however, complete remission rates were comparable before and during the pandemic in patients of Hispanic, non-Hispanic Black, and Asian/Pacific Islander/Other origin, in the adjusted models. The reasons for these racial/ethnic differences are not clear. Additional studies are needed to examine factors contributing to improved remission rates in non-Hispanic White patients after the onset of the pandemic and to assess why this improvement is lagging for other minority groups.
Cancer stage is an important prognostic factor in patients with ovarian cancer. Previous studies have reported poor progression-free survival and overall survival in ovarian cancer patients diagnosed at advanced FIGO stages.19,20 Similarly, we observed reduced remission rates in patients diagnosed with FIGO stages III and IV compared to FIGO stage I patients. We also observed reduced remission rates in patients with higher comorbidity burden at cancer diagnosis. Compared to patients with CCI=0, patients with CCI=2+ were less likely to achieve complete and clinical remission in the adjusted models. Even though evidence on the association of comorbidity burden and remission outcomes in ovarian cancer patients is scarce, our finding is not surprising. Previous studies have demonstrated comorbidity burden to be associated with advanced cancer stage and increased mortality in patients with ovarian cancer.18,21 In a meta-analysis, Karanth et al reported a lower likelihood of receiving ovarian cancer treatment and an increased mortality risk in patients with higher comorbidity burden.18 It is important to note that the statistically significant association of CCI with remission outcomes persisted after adjusting for FIGO stage, age, and other covariates of epidemiological and clinical relevance, in our study. This highlights comorbidity burden as an independent predictor of remission outcomes in patients with epithelial ovarian cancer. Future studies are warranted to assess if management of modifiable Charlson comorbidities may impact remission outcomes in ovarian cancer patients.
Unlike previous studies, we did not observe any difference in time from ovarian cancer diagnosis to treatment initiation by pandemic periods.6,11,16,22 However, patients who initiated treatment >2 weeks after diagnosis were less likely to achieve complete and clinical remission than patients who initiated cancer treatment within two weeks of diagnosis. This finding should be interpreted with caution. For some patients who received surgery as the first-line treatment, surgery date was recorded as their cancer diagnosis date in the EMR. It is possible that these patients received surgery for pelvic mass and their cancer was confirmed by perioperative biopsy; this might have resulted in over-estimation of the association between time to treatment initiation and remission outcomes in our study. Future studies involving rigorous medical chart reviews are warranted to exclude the possibility of information bias due to inconsistencies in measuring time from ovarian diagnosis to treatment initiation. The Institute of Medicine (IOM) cited timely access to cancer care as one of six aims for improving quality and outcomes in oncology patients;23 however, prior studies have mostly been restricted to assessing time to treatment with overall survival as the outcome of interest.24,25 Future studies in other contemporary ovarian cancer cohorts are needed to confirm if reducing time to treatment initiation may positively impact remission outcomes, which in turn may improve overall and cancer-specific survival in patients with ovarian cancer.
Our study had some limitations. First, there exists the possibility of unmeasured confounders and we did not have measure on all factor that may mediate potential difference in remission rates. For example, we did not have data on ovarian cancer molecular characteristics (although molecular characteristics are unlikely to differ by pandemic periods), and we used NDI as a proxy for individual level SES. Second, not all patients had follow-up visits that allowed the assessment of remission status. That said, only 6% of otherwise eligible patients lacked follow-up evaluations. Hence, any potential selection bias induced was likely minimal. Finally, our ovarian cancer cohort consisted of insured patients within an integrated health care system; our findings may not be generalizable to uninsured patients or patients within other types of health care system.
That said, our study has several strengths, including extensive EMR data supplemented by manual chart reviews for accurate capture of remission outcomes, the availability of detailed patient clinical characteristics such as comorbidities, and the inclusion of consecutive patients diagnosed with advanced epithelial ovarian cancer between January 2017 and June 2021. The KPSC setting allowed us to assess the association of the pandemic with remission outcomes without confounding by insurance status or differential access to care. We also had a diverse patient population that included >50% patients from racial/ethnic minorities which allowed us to evaluate potential differences in the relationship between pandemic period and remission outcomes by racial/ethnic groups.
Conclusion
Our study conducted in an integrated healthcare delivery system provided population-level evidence on the association of the COVID-19 pandemic and ovarian cancer remission outcomes. Comparable rates of complete and clinical remission before and after the onset of the pandemic offer some reassurance that outcomes of patients with ovarian cancer was not negatively impacted during the pandemic in our integrated healthcare system.
Ethics Statement
Our study complies with the Declaration of Helsinki.
Acknowledgments
The authors thank all patients included in the study. The abstract of this paper was presented at the 2023 American Society of Clinical Oncology (ASCO) Annual Meeting as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in the Journal of Clinical Oncology: https://ascopubs.org/doi/10.1200/JCO.2023.41.16_suppl.e17541; DOI:10.1200/JCO.2023.41.16_suppl.e17541.
Funding
This study was supported by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and AstraZeneca UK Ltd. Chao CR received research grant from Merck & Co, Inc. for this project. The grant was paid to Dr. Chao’s institution.
Disclosure
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: This study was supported by Merck Sharp & Dohme LLC, a subsidiary of Merck & Co., Inc., Rahway, NJ, USA, and AstraZeneca UK Ltd. Chao CR received research grant from Merck & Co, Inc. for this project. The grant was paid to Dr. Chao’s institution. Szamreta EA and Monberg M are employees of Merck & Co, Inc. The authors report no other conflicts of interest in this work.
References
1. Richards M, Anderson M, Carter P, Ebert BL, Mossialos E. The impact of the COVID-19 pandemic on cancer care. Nat Cancer. 2020;1(6):565–567. doi:10.1038/s43018-020-0074-y
2. Fedewa SA, Star J, Bandi P, et al. Changes in cancer screening in the US during the COVID-19 pandemic. JAMA Netw Open. 2022;5(6):e2215490. doi:10.1001/jamanetworkopen.2022.15490
3. Englum BR, Prasad NK, Lake RE, et al. Impact of the COVID-19 pandemic on diagnosis of new cancers: a national multicenter study of the veterans affairs healthcare system. Cancer. 2022;128(5):1048–1056. doi:10.1002/cncr.34011
4. Bakouny Z, Paciotti M, Schmidt AL, Lipsitz SR, Choueiri TK, Trinh QD. Cancer screening tests and cancer diagnoses during the COVID-19 pandemic. JAMA Oncol. 2021;7(3):458–460. doi:10.1001/jamaoncol.2020.7600
5. Jacome LS, Deshmukh SK, Thulasiraman P, Holliday NP, Singh S. Impact of COVID-19 pandemic on ovarian cancer management: adjusting to the new normal. Cancer Manag Res. 2021;13:359–366. doi:10.2147/CMAR.S287152
6. Frey MK, Fowlkes RK, Badiner NM, et al. Gynecologic oncology care during the COVID-19 pandemic at three affiliated New York City hospitals. Gynecol Oncol. 2020;159(2):470–475. doi:10.1016/j.ygyno.2020.09.005
7. Fader AN, Huh WK, Kesterson J, et al. When to operate, hesitate and reintegrate: society of gynecologic oncology surgical considerations during the COVID-19 pandemic. Gynecol Oncol. 2020;158(2):236–243. doi:10.1016/j.ygyno.2020.06.001
8. Colombo I, Zaccarelli E, Del Grande M, et al. ESMO management and treatment adapted recommendations in the COVID-19 era: gynaecological malignancies. ESMO Open. 2020;5(Suppl 3). doi:10.1136/esmoopen-2020-000827
9. Akladios C, Azais H, Ballester M, et al. Recommendations for the surgical management of gynecological cancers during the COVID-19 pandemic - FRANCOGYN group for the CNGOF. J Gynecol Obstet Hum Reprod. 2020;49(6):101729. doi:10.1016/j.jogoh.2020.101729
10. Algera MD, van Driel WJ, Slangen BFM, Kruitwagen R, Wouters M. participants of the Dutch gynecological oncology collaborator g. Impact of the COVID-19-pandemic on patients with gynecological malignancies undergoing surgery: a Dutch population-based study using data from the ‘Dutch Gynecological Oncology Audit’. Gynecol Oncol. 2022;165(2):330–338. doi:10.1016/j.ygyno.2022.02.013
11. Antunes D, Mendonca L, Melo A, Goncalves S, Nogueira Martins F, Nogueira Martins N. Impact of the COVID-19 pandemic on diagnosis and management of gynecological cancer: a single-center analysis. Medicina. 2022;58(12):1862. doi:10.3390/medicina58121862
12. Mandato VD, Aguzzoli L. Management of ovarian cancer during the COVID-19 pandemic. Int J Gynaecol Obstet. 2020;149(3):382–383. doi:10.1002/ijgo.13167
13. Fotopoulou C, Khan T, Bracinik J, et al. Outcomes of gynecologic cancer surgery during the COVID-19 pandemic: an international, multicenter, prospective CovidSurg-Gynecologic Oncology Cancer study. Am J Obstet Gynecol. 2022;227(5):735e1–735e25. doi:10.1016/j.ajog.2022.06.052
14. Charlson ME, Carrozzino D, Guidi J, Patierno C. Charlson comorbidity index: a critical review of clinimetric properties. Psychother Psychosom. 2022;91(1):8–35. doi:10.1159/000521288
15. Messer LC, Laraia BA, Kaufman JS, et al. The development of a standardized neighborhood deprivation index. J Urban Health. 2006;83(6):1041–1062. doi:10.1007/s11524-006-9094-x
16. Goenka L, Anandaradje A, Nakka T, et al. The ”collateral damage” of the war on COVID-19: impact of the pandemic on the care of epithelial ovarian cancer. Med Oncol. 2021;38(11):137. doi:10.1007/s12032-021-01588-6
17. Mandato VD, Torricelli F, Mastrofilippo V, et al. Impact of 2 years of COVID-19 pandemic on ovarian cancer treatment in IRCCS-AUSL of Reggio Emilia. Int J Gynaecol Obstet. 2023;163(2):679–688. doi:10.1002/ijgo.14937
18. Karanth S, Fowler ME, Mao X, et al. Race, socioeconomic status, and health-care access disparities in ovarian cancer treatment and mortality: systematic review and meta-analysis. JNCI Cancer Spectr. 2019;3(4):pkz084. doi:10.1093/jncics/pkz084
19. Paik ES, Lee YY, Lee EJ, et al. Survival analysis of revised 2013 FIGO staging classification of epithelial ovarian cancer and comparison with previous FIGO staging classification. Obstet Gynecol Sci. 2015;58(2):124–134. doi:10.5468/ogs.2015.58.2.124
20. Wei W, Li N, Sun Y, Li B, Xu L, Wu L. Clinical outcome and prognostic factors of patients with early-stage epithelial ovarian cancer. Oncotarget. 2017;8(14):23862–23870. doi:10.18632/oncotarget.13317
21. Tetsche MS, Dethlefsen C, Pedersen L, Sorensen HT, Norgaard M. The impact of comorbidity and stage on ovarian cancer mortality: a nationwide Danish cohort study. BMC Cancer. 2008;8:31. doi:10.1186/1471-2407-8-31
22. Moterani VC, Moterani NJW Jr, Candido Dos Reis FJ. Treatment delay and treatment pattern modifications among epithelial ovarian cancer patients during the COVID-19 pandemic: a retrospective cohort study. J Surg Oncol. 2022;126(7):1155–1161. doi:10.1002/jso.27048
23. Levit L, Balogh E, Nass S, Ganz PA, eds. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis. Medicine Io; 2013.
24. Huepenbecker SP, Sun CC, Fu S, et al. Association between time to diagnosis, time to treatment, and ovarian cancer survival in the United States. Int J Gynecol Cancer. 2022;32(9):1153–1163. doi:10.1136/ijgc-2022-003696
25. Alexander M, Blum R, Burbury K, et al. Timely initiation of chemotherapy: a systematic literature review of six priority cancers - results and recommendations for clinical practice. Intern Med J. 2017;47(1):16–34. doi:10.1111/imj.13190
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.