")
Back to Journals » International Journal of General Medicine » Volume 17
Combination of White Matter Hyperintensity and Neutrophil-to-Lymphocyte Ratio Predicts Short-Term Prognosis of Acute Ischemic Stroke Patients
Authors Zhang Q, Ma D, Du H, Wang T, Li W
Received 23 August 2024
Accepted for publication 9 December 2024
Published 14 December 2024 Volume 2024:17 Pages 6199—6206
DOI https://doi.org/10.2147/IJGM.S486511
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Qingyan Zhang,1,2 Danyue Ma,1,2 Hebin Du,3 Tiantian Wang,3 Wei Li3
1Key Laboratory of Ultra-Weak Magnetic Field Measurement Technology, Ministry of Education, School of Instrumentation and Optoelectronic Engineering, Beihang University, Beijing, 100191, People’s Republic of China; 2Zhejiang Provincial Key Laboratory of Ultra-Weak Magnetic-Field Space and Applied Technology, Hangzhou Innovation Institute of Beihang University, Hangzhou, 310000, People’s Republic of China; 3Department of Neurology, Nanjing Drum Tower Hospital Group Suqian Hospital, Suqian, 223800, People’s Republic of China
Correspondence: Wei Li, Department of Neurology, Nanjing Drum Tower Hospital Group Suqian Hospital, Suqian, 223800, People’s Republic of China, Tel +86-52784235896, Email [email protected]
Purpose: To assess the value of combination of white matter hyperintensity (WMH) and neutrophil-to-lymphocyte ratio (NLR) in predicting short-term prognosis of acute ischemic stroke (AIS) patients.
Patients and Methods: Three hundred and nine AIS patients were included in this prospective observational research. They were evaluated at 3-month after the onset of AIS using modified Rankin Scale (mRS) score. A mRS score of 0– 2 was defined as a favourable outcome, while an mRS score of 3– 6 was defined as an unfavourable outcome. Multivariate analysis was used to identify the independent associations of WMH and NLR with short-term prognosis of AIS patients, and receiver operating characteristic (ROC) curves were used to evaluate the predictive values of WMH, NLR and their combination for short-term prognosis of AIS patients, and Z test was used to compare the area under curve (AUC).
Results: Among 309 AIS patients, 201 (65.0%) had a favorable 3-month outcome, while 108 (35.0%) had an unfavorable outcome. According to the results of multivariate analysis, WMH, NLR and on-admission NIHSS score were independently associated with unfavourable outcome of AIS after adjusting for diabetes mellitus, atrial fibrillation, TOAST subtype and LDL-cholesterol. ROC curves showed that the AUCs of WMH, NLR and their combination for predicting short-term prognosis of AIS patients were 0.760 [standard error (SE): 0.029, 95% confidence interval (CI): 0.703– 0.817, P< 0.001], 0.717 (SE: 0.030, 95% CI: 0.661– 0.774, P< 0.001) and 0.906 (SE: 0.019, 95% CI: 0.868– 0.944, P< 0.001), respectively. The AUC of combination prediction was significantly higher than those of individual predictions (0.906 vs 0.760, Z=4.211, P< 0.001; 0.906 vs 0.717, Z=5.322, P< 0.001).
Conclusion: WMH and NLR were independently associated with short-term prognosis of AIS patients, and the combination of WMH and NLR could be applied in predicting short-term prognosis of AIS patients, having a high predictive value.
Keywords: acute ischemic stroke, short-term prognosis, white matter hyperintensity, neutrophil-to-lymphocyte ratio, prediction
Introduction
Stroke is a severe brain injury disease, and acute ischemic stroke (AIS) is the most common subtype accounting for about 85% of all subtypes.1 Stroke occupies the second leading cause of deaths and disability globally,2 and its prevalence and incidence in China have been escalating over the past decade.3 China has the largest amount of stroke patients in the world, leading to a huge burden on families of patients and a major drain on public health-care funding.4 Therefore, prognosis prediction of AIS is useful and preoccupying to families and society.
White matter hyperintensity (WMH) is a common neuroimaging manifestation involved in the aging process and reflects the presence of cerebral small-vessel disease.5,6 It is related to loss of microstructural white matter integrity and increased blood–brain barrier permeability,7 and can affect the remodeling of the myelin sheath after stroke.8 WMH has been demonstrated the association with poor functional outcomes after ischemic stroke,9 and can be used to predict post-stroke function and cognition impairment.7,10,11
Neuroinflammatory responses can aggravate ischemic brain damage and neurological dysfunction, playing a critical role in the pathophysiology of ischemic stroke.12–14 Neutrophil-to-lymphocyte ratio (NLR), as an inexpensive biomarker in systematic inflammatory process, has been confirmed to possess diagnostic and prognostic capabilities in many diseases.15–17 In AIS patients, NLR is associated with severity of stroke, recurrence of cerebral infarction, short-term mortality and functional prognosis.18,19 However, the value of WMH combined with NLR in predicting short-term prognosis of AIS patients has still not been investigated. In this study, combination of the neuroimaging marker (WMH) and the inflammatory biomarker (NLR) was first applied to predict short-term prognosis of AIS patients. The aim is to provide a more accurate tool for predicting short-term prognosis of AIS patients.
Patients and Methods
Patients
This study was a prospective observational research, enrolling a consecutive cohort of AIS patients in Nanjing Drum Tower Hospital Group Suqian Hospital between January 2023 and March 2024. This study was permitted by the Ethical Committee of Nanjing Drum Tower Hospital Group Suqian Hospital (SQ2021016045) and conducted strictly according to the guidelines of the Declaration of Helsinki. Written informed consents were provided by the participants before the study commencement.
Inclusion criteria included ① acute, first-ever, ischemic stroke confirmed by brain magnetic resonance imaging (MRI) scan; ② age ≥18 years old; ③ admitted within the first 24 h after the onset of symptoms; ④ complete clinical data including the magnetic resonance images, neutrophil and lymphocyte on admission. Exclusion criteria included ① transient ischemic attack; ② pre-stroke modified Rankin scale (mRS) score ≥2; ③ MRI demonstrating conditions other than cerebral infarction, such as encephalitis, cerebral tumors and hemorrhage; ④ severe kidney or liver dysfunction, or cardiac impairment, or coexistence of other severe systemic diseases; ⑤ other autoimmune conditions or neurodegenerative disorders affecting the nervous systems.
Data Collection
We collected the data of all participants, including demographics (sex, age, weight and height), relevant vascular-based risk factors (smoking, drinking, coronary heart disease, diabetes mellitus, hypertension, hyperlipidemia and atrial fibrillation), clinical data on admission (systolic blood pressure, diastolic blood pressure, NIHSS score, heart rate and random blood glucose), Trial of Org 10172 in acute stroke treatment (TOAST) subtypes, therapeutic methods, laboratory test parameters [white blood cell count (WBC), neutrophil count, lymphocyte count, HbA1c, monocyte (mmol/L), fibrinogen (g/L), homocysteine (µmol/L), triglyceride (mmol/L), total cholesterol (mmol/L), high-density lipoprotein (HDL)-cholesterol (mmol/L), low-density lipoprotein (LDL)-cholesterol (mmol/L)], and magnetic resonance images. The fasting venous blood samples were collected within 24 h after admission, and the magnetic resonance images were analyzed by two experienced neurologists blinded to clinical characteristics, laboratory test results and functional outcomes. Fazekas rating scale was used to assess WMH via deep WMH and periventricular WMH (P-WMH) rating separately. Total Fazekas score, the sum of deep WMH and P-WMH was computed and ranged from 0 to 6.
Outcome Evaluation
All participants were evaluated at 3-month after the onset of AIS using modified Rankin Scale (mRS) score. An mRS score of 0–2 was defined as a favourable outcome, while an mRS score of 3–6 was defined as an unfavourable outcome.
Statistical Analysis
All statistical analysis was performed using the Statistical Package for the Social Sciences version 22.0 (SPSS Inc., USA). The normality of continuous variables was ascertained by Kolmogorov–Smirnov test, and the variables with a normal distribution were described with mean ± standard deviation (SD) and compared for the differences between AIS patients with favourable and unfavourable outcome via Student’s t test, and the variables with a non-normal distribution were described with median (M) and interquartile range (IQR) and compared for the intergroup differences via Mann–Whitney U-test. Categorical variables were described with percentages/ratios (%) and compared for the intergroup differences via chi-square test. In order to determine the independent associations of WMH and NLR with unfavourable outcome of AIS, multivariate analysis was then performed for the variables with two-sided P<0.10 in univariate analysis via binary logistic regression model. Receiver operating characteristic (ROC) curves were used to evaluate the predictive values of WMH, NLR and their combination for unfavourable outcome of AIS, and Z test was used to compare the area under curve (AUC). A two-sided P value of <0.05 was used to compute the statistical significance.
Results
General Information
According to the inclusion and exclusion criteria, a total of 322 AIS patients were enrolled during the study period. Thirteen patients were not evaluated for the 3-month outcome. Finally, 309 AIS patients were included in this analysis. These 309 patients consisted of 191 males (61.8%) and 118 females (38.2%) with a mean age of 65.67 ± 12.05 years and a median admission NIHSS of 6 (IQR 3–13). Among them, 201 (65.0%) had a favorable 3-month outcome, while 108 (35.0%) had an unfavorable outcome.
Associations of WMH and NLR with Unfavourable Outcome of AIS
In order to determine the independent associations of WMH and NLR with unfavourable outcome of AIS, univariate analysis was first carried out between AIS patients with favourable and unfavourable outcome. As shown in Table 1, WMH, NLR, diabetes mellitus, atrial fibrillation, TOAST subtype and on-admission NIHSS score were statistically different (P < 0.05), while the remaining variables were not statistically different (P > 0.05). However, the P value of LDL-cholesterol was <0.10.
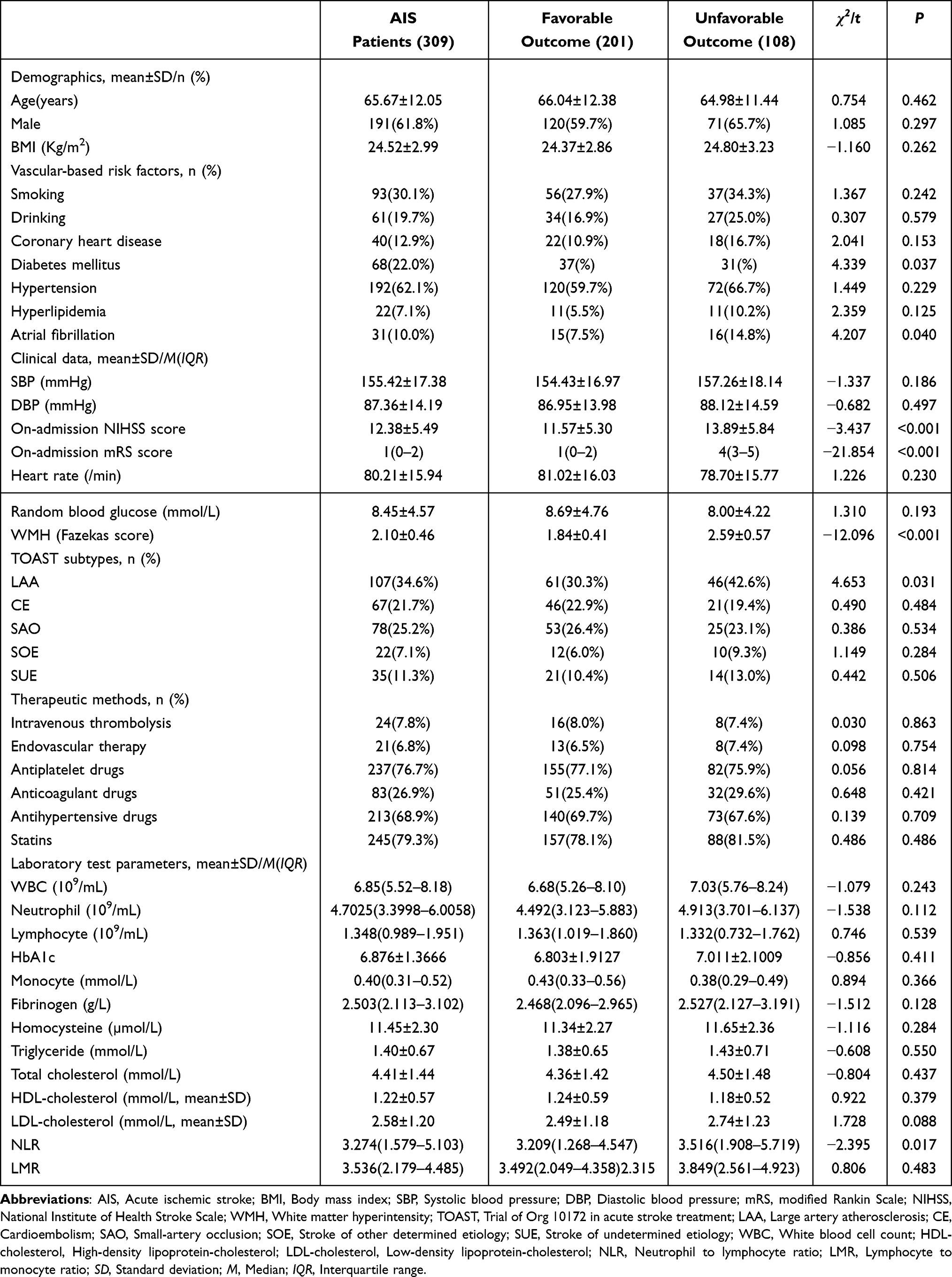 |
Table 1 Results of Univariate Analysis Between AIS Patients with Favorable and Unfavorable Outcome at 3-Month After the Onset of Symptoms |
Multivariate analysis was then performed for WMH, NLR, diabetes mellitus, atrial fibrillation, TOAST subtype, on-admission NIHSS score and LDL-cholesterol via binary logistic regression model. As shown in Table 2, WMH, NLR and admission NIHSS score were independently associated with unfavourable outcome of AIS after adjusting for diabetes mellitus, atrial fibrillation, TOAST subtype and LDL-cholesterol.
 |
Table 2 Results of Multivariate Analysis Results Between AIS Patients with Favorable and Unfavorable Outcome at 3-Month After the Onset of Symptoms |
Predictive Values
ROC curves (Figure 1) showed that the AUCs of WMH and NLR for predicting short-term prognosis of AIS patients were 0.760 [standard error (SE): 0.029, 95% confidence interval (CI): 0.703–0.817, P<0.001] and 0.717 (SE: 0.030, 95% CI: 0.661–0.774, P<0.001), respectively. In order to elevate the predictive value, a combination of WMH and NLR was employed. The result (Figure 1) showed that the AUC of combination prediction was 0.906 (SE: 0.019, 95% CI: 0.868–0.944, P < 0.001), significantly higher than those of individual predictions (0.906 vs 0.760, Z=4.211, P < 0.001; 0.906 vs 0.717, Z=5.322, P < 0.001).
 |
Figure 1 ROC curves for WMH, NLR and their combination in predicting short-term prognosis of AIS patients. |
Discussion
The mechanisms of the adverse impact of WMH on the prognosis of AIS patients remain poorly understood. First, WMH is related to integrity impairment of microstructural white matter and the blood–brain barrier (BBB),7 and integrity impairment of the BBB increases its permeability, frequently leading to blood extravasation. Second, WMH can affect the remodeling of the myelin sheath after stroke.8 Third, cerebrovascular reactivity and cerebral blood flow are decreased in WMH regions.20 Fourth, WMH is confirmed to be a risk factor for cerebral infarction, and its severity may be correlated with the progression and increase in infarct volume.5 Finally, WMH is involved in the progression from normal to mild cognitive impairment and is independently associated with dementia.11,21
Griessenauer et al reported that the WMH burden had an adverse effect on 3-month functional outcome in patients with large vessel occlusion (LVO) stroke or non-LVO stroke;22 and Derraz et al further reported that the WMH burden was related to poor 3-month functional outcome in LVO stroke patients undergoing endovascular thrombectomy, but it was not related to the occurrence of symptomatic intracranial hemorrhage or 90-day mortality.23 Zhu et al reported that the higher WMH burden was related to increased risk of major disability or death at 14 days or hospital discharge and 3 months in AIS patients.24 Park et al found that higher WMH burden was related to increased risk of recurrent stroke and a composite of stroke/myocardial infarction/vascular death during a 2-year follow-up in Asian patients with ischemic stroke,25 and Ryu et al also found a significant association between higher WMH burden and recurrent stroke through a 1-year follow-up in ischemic stroke patients.26 In addition, Molad et al found that higher WMH burden was correlated with poor cognitive performance after stroke.27 Our study confirmed the independent association of the WMH burden with poor short-term prognosis of AIS patients and moreover demonstrated its moderate predictive value.
In AIS, post-ischemic inflammation was resulted from activation of intravascular leukocytes, stagnant blood flow, and release of pro-inflammatory mediators from brain parenchyma, platelet granules and ischemic endothelium.12 Activated neuroinflammatory responses can aggravate ischemic brain damage and neurological dysfunction.12–14 Neutrophils have been shown to be able to aggravate oxidative stress, release pro-inflammatory mediators and increase the permeability of the BBB, thus leading to the aggravation of brain damage.28,29 The lymphocyte count is an indicator for general health and is affected by acute physiologic stress. Studies have confirmed its active involvement in a protective mechanism in the ischemic brain.30,31 Its decrease is correlated with the deterioration of immunological function and the early neuroinflammation, therefore resulting in poor clinical outcomes.32
NLR reflects the balance between neutrophils and lymphocytes in the peripheral blood, and its increase has been demonstrated to be involved in multiple atherosclerotic events including ischemic stroke, peripheral arterial occlusive disease, coronary artery disease and so on.33–35 Especially, NLR is associated with severity of stroke, recurrence of cerebral infarction, short-term mortality and functional prognosis in AIS patients, demonstrating the potential of serving as a prognostic predictor.18,19 Chen et al reported that NLR was independently associated with 3-month functional outcomes in AIS patients, possessing moderate predictive value with an AUC of 0.776.36 Xu et al found that NLR was an independent prognostic indicator for stroke progression and a poor 3-month functional status.37 Ying et al showed that increased NLR at admission was independently correlated with the initial stroke severity and poor 14-day prognosis in AIS patients with intracranial atherosclerotic stenosis.38 Wu et al reported that NLR and its dynamic changes were related to 3-month outcome and mortality in AIS patients receiving intravenous thrombolysis with good predictive values.39 Lee et al demonstrated that increased NLR was correlated with failed reperfusion in AIS patients undergoing endovascular treatment.40 Gong et al showed that NLR was related to post-thrombolysis early neurological improvement and early neurological deterioration in AIS patients receiving intravenous thrombolysis.41 Our study showed that NLR was independently associated with poor short-term prognosis in AIS patients, but its predictive value was relatively low.
In order to elevate the predictive value for short-term prognosis of AIS patients, a combination of WMH and NLR was employed in this study. The result showed that the AUC of combination prediction was significantly higher than those of individual predictions, reaching more than 0.900. Therefore, the combination of WMH and NLR could be applied in predicting short-term prognosis of AIS patients, having a high predictive value.
Conclusion
WMH and NLR were independently associated with short-term prognosis of AIS patients, and the combination of WMH and NLR could be applied in predicting short-term prognosis of AIS patients, having a high predictive value.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All the authors do not have any conflict of interest.
References
1. Haq S, Mathur M, Singh J, et al. Colour Doppler evaluation of extracranial carotid artery in patients presenting with acute ischemic stroke and correlation with various risk factors. J Clin Diagn Res. 2017;11(3):TC01–TC05. doi:10.7860/JCDR/2017/25493.9541
2. Feigin VL, Stark BA, Johnson CO; GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. 2021;20(10):795–820. doi:10.1016/S1474-4422(21)00252-0
3. Tu WJ, Hua Y, Yan F, et al. Prevalence of stroke in China, 2013-2019: a population-based study. Lancet Reg Health West Pac. 2022;28:100550. doi:10.1016/j.lanwpc.2022.100550
4. Wang W, Jiang B, Sun H, et al. NESS-China investigators. prevalence, incidence, and mortality of stroke in china: results from a nationwide population-based survey of 480 687 adults. Circulation. 2017;135(8):759–771. doi:10.1161/CIRCULATIONAHA.116.025250
5. Wardlaw JM, Smith EE, Biessels GJ, et al. STandards for reporting vascular changes on nEuroimaging (STRIVE v1). neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013;12(8):822–838. doi:10.1016/S1474-4422(13)70124-8
6. Charidimou A, Boulouis G, Haley K, et al. White matter hyperintensity patterns in cerebral amyloid angiopathy and hypertensive arteriopathy. Neurology. 2016;86(6):505–511. doi:10.1212/WNL.0000000000002362
7. Rost NS, Cougo P, Lorenzano S, et al. Diffuse microvascular dysfunction and loss of white matter integrity predict poor outcomes in patients with acute ischemic stroke. J Cereb Blood Flow Metab. 2018;38(1):75–86. doi:10.1177/0271678X17706449
8. Joutel A, Chabriat H. Pathogenesis of white matter changes in cerebral small vessel diseases: beyond vessel-intrinsic mechanisms. Clin Sci. 2017;131(8):635–651. doi:10.1042/CS20160380
9. Georgakis MK, Duering M, Wardlaw JM, et al. WMH and long-term outcomes in ischemic stroke: a systematic review and meta-analysis. Neurology. 2019;92(12):e1298–e1308. doi:10.1212/WNL.0000000000007142
10. Molad J, Hallevi H, Korczyn AD, et al. Vascular and neurodegenerative markers for the prediction of post-stroke cognitive impairment: results from the TABASCO study. J Alzheimers Dis. 2019;70(3):889–898. doi:10.3233/JAD-190339
11. Zamboni G, Griffanti L, Mazzucco S, et al. Age-dependent association of white matter abnormality with cognition after TIA or minor stroke. Neurology. 2019;93(3):e272–e282. doi:10.1212/WNL.0000000000007772
12. Anrather J, Iadecola C. Inflammation and stroke: an overview. Neurotherapeutics. 2016;13(4):661–670. doi:10.1007/s13311-016-0483-x
13. Schuhmann MK, Stoll G, Bieber M, et al. CD84 links T cell and platelet activity in cerebral thrombo-inflammation in acute stroke. Circ Res. 2020;127(8):1023–1035. doi:10.1161/CIRCRESAHA.120.316655
14. Parikh NS, Merkler AE, Iadecola C. Inflammation, autoimmunity, infection, and stroke: epidemiology and lessons from therapeutic intervention. Stroke. 2020;51(3):711–718. doi:10.1161/STROKEAHA.119.024157
15. Templeton AJ, McNamara MG, Šeruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju124
16. Bhat T, Teli S, Rijal J, et al. Neutrophil to lymphocyte ratio and cardiovascular diseases: a review. Expert Rev Cardiovasc Ther. 2013;11(1):55–59. doi:10.1586/erc.12.159
17. Templeton AJ, Ace O, McNamara MG, et al. Prognostic role of platelet to lymphocyte ratio in solid tumors: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2014;23(7):1204–1212. doi:10.1158/1055-9965.EPI-14-0146
18. Xue J, Huang W, Chen X, et al. Neutrophil-to-lymphocyte ratio is a prognostic marker in acute ischemic stroke. J Stroke Cerebrovasc Dis. 2017;26(3):650–657. doi:10.1016/j.jstrokecerebrovasdis.2016.11.010
19. Kocaturk O, Besli F, Gungoren F, et al. The relationship among neutrophil to lymphocyte ratio, stroke territory, and 3-month mortality in patients with acute ischemic stroke. Neurol Sci. 2019;40(1):139–146. doi:10.1007/s10072-018-3604-y
20. Wardlaw JM, Smith C, Dichgans M. Small vessel disease: mechanisms and clinical implications. Lancet Neurol. 2019;18(7):684–696. doi:10.1016/S1474-4422(19)30079-1
21. Yi T, Zhang Y, Chen WH, et al. for the DIRECT-MT investigators. Impact of leukoaraiosis in patients with acute ischemic stroke treated with thrombectomy: a post hoc analysis of the DIRECT-MT trial. J Neurointerv Surg. 2023;15(2):139–145. doi:10.1136/neurintsurg-2021-018293
22. Griessenauer CJ, McPherson D, Berger A, et al. Effects of white matter hyperintensities on 90-day functional outcome after large vessel and non-large vessel stroke. Cerebrovasc Dis. 2020;49(4):419–426. doi:10.1159/000509071
23. Derraz I, Abdelrady M, Ahmed R, et al. Impact of white matter hyperintensity burden on outcome in large-vessel occlusion stroke. Radiology. 2022;304(1):145–152. doi:10.1148/radiol.210419
24. Zhu S, Qian S, Xu T, et al. White matter hyperintensity, immediate antihypertensive treatment, and functional outcome after acute ischemic stroke. Stroke. 2020;51(5):1608–1612. doi:10.1161/STROKEAHA.119.028841
25. Park JH, Heo SH, Lee MH, et al.; PICASSO investigators. White matter hyperintensities and recurrent stroke risk in patients with stroke with small-vessel disease. Eur J Neurol. 2019;26(6):911–918. doi:10.1111/ene.13908
26. Ryu WS, Schellingerhout D, Hong KS, et al. White matter hyperintensity load on stroke recurrence and mortality at 1 year after ischemic stroke. Neurology. 2019;93(6):e578–e589. doi:10.1212/WNL.0000000000007896
27. Molad J, Kliper E, Korczyn AD, et al. Only white matter hyperintensities predicts post-stroke cognitive performances among cerebral small vessel disease markers: results from the TABASCO study. J Alzheimers Dis. 2017;56(4):1293–1299. doi:10.3233/JAD-160939
28. Stoll G, Nieswandt B. Thrombo-inflammation in acute ischaemic stroke - implications for treatment. Nat Rev Neurol. 2019;15(8):473–481. doi:10.1038/s41582-019-0221-1
29. Zhu B, Pan Y, Jing J, et al. CHANCE Investigators. Neutrophil counts, neutrophil ratio, and new stroke in minor ischemic stroke or TIA. Neurology. 2018;90(21):e1870–e1878. doi:10.1212/WNL.0000000000005554
30. Li Z, Cui L, Ma J, et al. Association between neutrophil to lymphocyte ratio and atrial fibrillation. Int J Cardiol. 2015;187:361–362. doi:10.1016/j.ijcard.2015.03.114
31. Liesz A, Zhou W, Na SY, et al. Boosting regulatory T cells limits neuroinflammation in permanent cortical stroke. J Neurosci. 2013;33(44):17350–17362. doi:10.1523/JNEUROSCI.4901-12.2013
32. Yang YL, Wu CH, Hsu PF, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020;50(5):e13230. doi:10.1111/eci.13230
33. Papa A, Emdin M, Passino C, et al. Predictive value of elevated neutrophil-lymphocyte ratio on cardiac mortality in patients with stable coronary artery disease. Clin Chim Acta. 2008;395(1–2):27–31. doi:10.1016/j.cca.2008.04.019
34. Erturk M, Cakmak HA, Surgit O, et al. Predictive value of elevated neutrophil to lymphocyte ratio for long-term cardiovascular mortality in peripheral arterial occlusive disease. J Cardiol. 2014;64(5):371–376. doi:10.1016/j.jjcc.2014.02.019
35. Wang L, Song Q, Wang C, et al. Neutrophil to lymphocyte ratio predicts poor outcomes after acute ischemic stroke: a cohort study and systematic review. J Neurol Sci. 2019;406:116445. doi:10.1016/j.jns.2019.116445
36. Chen C, Gu L, Chen L, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as potential predictors of prognosis in acute ischemic stroke. Front Neurol. 2021;11:525621. doi:10.3389/fneur.2020.525621
37. Xu C, Cai L, Yi T, et al. Neutrophil-to-lymphocyte ratio is associated with stroke progression and functional outcome in patients with ischemic stroke. Brain Behav. 2023;13(11):e3261. doi:10.1002/brb3.3261
38. Ying Y, Yu F, Luo Y, et al. Neutrophil-to-lymphocyte ratio as a predictive biomarker for stroke severity and short-term prognosis in acute ischemic stroke with intracranial atherosclerotic stenosis. Front Neurol. 2021;12:705949. doi:10.3389/fneur.2021.705949
39. Wu Q, Chen HS. Neutrophil-to-lymphocyte ratio and its changes predict the 3-month outcome and mortality in acute ischemic stroke patients after intravenous thrombolysis. Brain Behav. 2023;13(9):e3162. doi:10.1002/brb3.3162
40. Lee SH, Jang MU, Kim Y, et al. The neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios predict reperfusion and prognosis after endovascular treatment of acute ischemic stroke. J Pers Med. 2021;11(8):696. doi:10.3390/jpm11080696
41. Gong P, Liu Y, Gong Y, et al. The association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and lymphocyte to monocyte ratio with post-thrombolysis early neurological outcomes in patients with acute ischemic stroke. J Neuroinflammation. 2021;18(1):51. doi:10.1186/s12974-021-02090-6
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Association of the Neutrophil-to-Lymphocyte Ratio, Platelet-to-Lymphocyte Ratio, Lymphocyte-to-Monocyte Ratio and Systemic Inflammation Response Index with Short-Term Functional Outcome in Patients with Acute Ischemic Stroke
Zhang YX, Shen ZY, Jia YC, Guo X, Guo XS, Xing Y, Tian SJ
Journal of Inflammation Research 2023, 16:3619-3630
Published Date: 23 August 2023
The Prognosis of Neutrophil-to-Lymphocyte Ratio and Lymphocyte-to-Monocyte Ratio in Elderly with Acute Ischemic Stroke
Wang J, Zhao Y, Lv C, Li F
Clinical Interventions in Aging 2024, 19:1715-1720
Published Date: 19 October 2024