")
Back to Journals » Infection and Drug Resistance » Volume 18
Comparative Efficacy of Endoscopic Lesion Resection and Posterior Lesion Debridement, Bone Grafting, Fusion and Internal Fixation Combined With Medication in the Treatment of Lumbar Brucellosis Spondylitis
Authors Yusufu A, Haibier A , Ma Y
Received 23 October 2024
Accepted for publication 29 March 2025
Published 18 April 2025 Volume 2025:18 Pages 1923—1934
DOI https://doi.org/10.2147/IDR.S496495
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Alimujiang Yusufu,1,2,* Abuduwupuer Haibier,1,2,* Yuan Ma1
1Department of Spine Surgery, The Sixth Affiliated Hospital of Xinjiang Medical University, Orthopaedic Hospital of Xinjiang Uygur Autonomous Region, Urumqi, People’s Republic of China; 2Xinjiang Medical University, Xinjiang Uygur Autonomous Region, Urumqi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yuan Ma, Email [email protected]
Objective: This study intends to compare the efficacy and safety of endoscopic lumbar brucellosis with traditional posterior focus debridement, bone grafting, fusion and internal fixation combined with drugs in the treatment of lumbar brucellosis, and summarize the advantages and disadvantages of different surgical methods, in order to provide theoretical support for clinical surgical decision-making.
Methods: The data of 41 lumbar brucellosis patients admitted to the Department of spinal Surgery of the Sixth Affiliated Hospital of Xinjiang Medical University from January 2018 to June 2023 were divided into endoscopic group (Group A, n = 15) and open surgery group (Group B, n = 26). Two groups of general data, surgical and related indicators, blood biochemical and imaging indicators were recorded and analyzed, and the clinical recovery and complications were evaluated according to various scores.
Results: There was no statistical difference in baseline data between Group A and Group B, and it could be compared between the two groups; the postoperative lumbar VAS score and hemoglobin index of Group A were significantly better than that of Group B, and the difference was statistically significant (P< 0.05); Group A was significantly better than Group B in terms of operation time, intraoperative blood loss and postoperative time to go down, and the difference was statistically significant (P< 0.05); there was no significant difference between the two groups in other indicators (P> 0.05).
Conclusion: The two types of lumbar brucellosis treatment are safe and effective, and the clinical effect of endoscopic surgery is outstanding, which is more conducive to the postoperative rehabilitation of patients. It is recommended when conditions permit.
Keywords: lumbar brucellosis spondylitis, LBS, lumbar, lesion removal, endoscopic, posterior surgery
Introduction
Lumbar brucellosis spondylitis (LBS) mainly refers to a zoonotic infectious disease that develops symptoms such as neurological dysfunction, pain and fever after spinal infection with Brucellosis.1,2 One of the main characteristics of Brucella after invading the body is damage to bones and joints, the main sites being the spine, knee joints and hip joints.3–5 Early, combined, full-course, and regular antibiotic chemotherapy plays an important role in the overall treatment of lumbar LBS. When drug treatment fails or serious complications occur, patients with surgical indications should consider surgery in time.6 The end result of both conservative treatment and surgical treatment is bone fusion. Both treatment options require combination of antibacterial treatment. The optimal duration of antibiotic treatment is still controversial, but should not be less than 6 weeks.7
Currently, common surgical methods for treating LBS are divided into anterior approach, posterior approach, anterolateral approach, and combined anteroposterior approach according to the surgical approach.8 Traditional incision surgery has the advantages of clear field of view, large operable space and wide surgical indications, which is conducive to the complete removal of the lesion. However, there are many incisions, the need to change the position during the operation, long operation time, large amount of blood loss during the operation, etc., The operation is difficult and is not conducive to the patient’s postoperative recovery, which leads to its great limitation in clinical use.9,10 With the rise of minimally invasive concepts, minimally invasive spinal technology has been used in the surgical treatment of LBS.11 Endoscopic surgery has less trauma, shorter recovery period and more beautiful surgical incision than traditional incision,12 but this technique also has insufficient lesion clearance, limited surgical field, high technical requirements, and relatively narrow indications.13
There are few studies that directly compare the efficacy of these two different surgical methods in LBS. Therefore, this study retrospectively analyzed the clinical data of patients with LBS who underwent endoscopic debridement surgery and open surgery, and evaluated the feasibility, safety and effectiveness of the two surgical methods for the treatment of LBS, in order to provide some theoretical support for clinical surgical decisions.
Objects and Methods
Design
Retrospective cohort study.
Time and Location
A retrospective analysis of 41 patients with lumbar brucellosis admitted to the Department of Spinal Surgery of the Sixth Affiliated Hospital of Xinjiang Medical University from January 2018 to June 2023.
Object
The clinical data of 41 patients with LBS who underwent endoscopic lesion resection and posterior lesion resection, bone grafting, and internal fixation at the Spinal Surgery Department of the Sixth Affiliated Hospital of Xinjiang Medical University from January 2018 to June 2023 were selected. They were divided into endoscopic lesion resection group (group A, n=15) and posterior lesion resection, bone grafting, and internal fixation group (group B, n=26) according to different surgical methods. This study has been reviewed by the Ethics Committee of the Sixth Affiliated Hospital of Xinjiang Medical University. See Figure 1 for details.
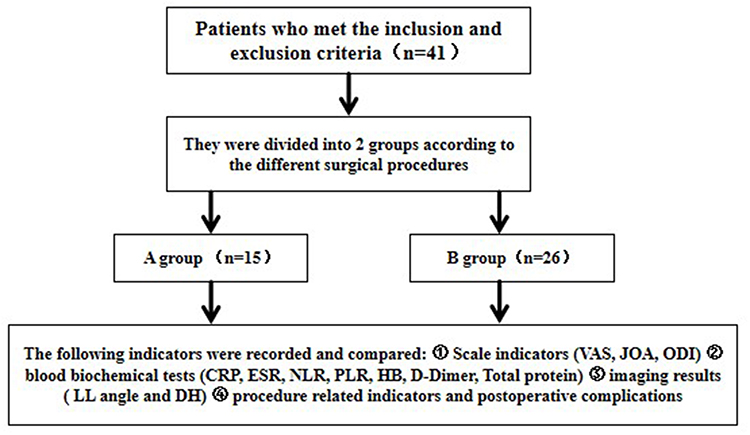 |
Figure 1 Flow chart of test grouping. |
Inclusion Criteria
Complete clinical data; Meets the expert consensus and diagnostic criteria for Brucella spondylitis;11 laboratory tests: (1) rose bengal plate, positive agglutination test; (2) red blood cell sedimentation rate Erythrocylethalization rate (ESR) and C-reactive protein (C reactive protein (CRP) increased; X-ray,CT, and MRI imaging examinations showed vertebral bone destruction, narrowing of the intervertebral space, paravertebral abscess, etc.; the lesions were all single level; the clinical symptoms were not relieved or aggravated after 6 weeks of conservative treatment; the surgical indications were met:14(1) Compression of the spinal cord or nerve roots showed persistent or progressive neurological deficits; (2) No significant effect on prolonged antibiotic treatment; (3) Obstinate low back pain that cannot be alleviated by non-surgical treatment.
Exclusion Criteria
(1) The patient is malnourished and cannot tolerate this operation; (2) The patient has obvious contraindications for the operation; (3) The patient has mental illness, etc. and cannot cooperate with this study; (4) The patient has complications of Brucella or tuberculosis in other sites.
Diagnostic Criteria for Lumbar Spine Brucellosis
Clinical manifestations: Fever, hyperhidrosis, fatigue, and low back pain (low back pain is the most common); (2) Laboratory examinations: elevated erythrocyte sedimentation rate and C-reactive protein, positive serological tests such as rose bengal plate agglutination test (RBPT), tube agglutination test (SAT), etc. Culturing of Brucella in blood, bone marrow, cerebrospinal fluid, etc. is the gold standard for diagnosis, but the positive culture rate is low; (3) Imaging examinations: lumbar bone destruction, narrowing of the intervertebral space can occur on X-ray, CT and MRI; (4) Postoperative pathological examination revealed Brucella infection.
Surgical Method
Preoperative Preparation
Before surgery, they took anti-brucellosis double drugs (rifampicin 0.6 g/d and doxycycline 0.2 g/d) regularly for 2–4 weeks, and were also given symptomatic treatments such as antipyretic, analgesic, and liver protection; corrected malnutrition and hypoproteinemia; understood the patient’s visual analog score (VAS) and spinal nerve function ASIA classification and other data.
Surgery Method
Posterior Pedicle Lesion Removal, Bone Grafting and Internal Fixation
After general anesthesia, the prone position was taken, and the posterior median approach was selected to fully expose the articular process, lamina, transverse process and spinous process of the affected vertebra to the surgical field. After accurate positioning, the pedicle was implanted in the vertebral body to correct the deformity. After the bone grafting was completed, hemostasis was performed, drainage tubes were placed, and the incision was closed.
Endoscopic Spinal Tuberculosis Focus Removal
After general anesthesia, the patient was placed in prone position and body surface positioning was performed, taking the left L4/L5 intervertebral space as an example. The base of the spinous process of L4 is positioned as the horizontal line with the C-arm fluoroscopy, and the line connecting the medial edge of the left pedicle is used as the longitudinal line. The intersection of 1.5–2 cm on both sides of the horizontal line and the longitudinal line is the puncture entry point. The operating area was routinely disinfected, and a 0.5 cm incision was made horizontally at the cranial and caudal puncture points. The expander and laminar dissector were placed in the direction of the responsible intervertebral space through bilateral incisions. Fluoroscopy confirmed that the tips of the expander and laminar dissector were located at the intervertebral space level, the medial edge of the pedicle, and the tips touched. An endoscope was placed through the cephalad observation channel, and a low-temperature plasma blade was placed into the caudal T-channel to stop bleeding and ablate tissue. Continuous normal saline irrigation was carried out. Under the microscope, the plasma blade exposed the lower lamina and inferior articular process of the L4 vertebral body upward, and exposed the upper lamina of the L5 vertebral body downward. Use laminar rongeur, osteotome, and grinding drill alternately to remove 2/3 of the L4 inferior articular process and a little lower edge of the L4 lamina, grind the inner edge of the L5 superior articular process, bite off the interlaminar, dura mater and nerve roots. The ligamentum flavum is fully exposed to the inflammatory lesion tissue, nerve roots, and intervertebral discs, and remove the nucleus pulposus tissue through the rupture of the annulus fibrosus with nucleus forceps. The nucleus pulposus tissue showed non-caseous necrosis, so appropriate pathological tissue was taken and sent for pathological examination. The pus within the spinal canal and around the vertebral body was cleared and destroyed by biting off the damaged bone, followed by radio frequency ablation of the fibrous ring, and the human allogeneic bone was placed and compacted; finally, pedicle screws were implanted for hemostasis, drainage tubes were placed, and the incision was closed.
Postoperative Management
The postoperative treatment was the same for both groups, and symptomatic treatments such as swelling and analgesia were given. Ceftriaxone sodium 3g/d was administered intravenously for 3 days to prevent infection. When the incision drainage fluid was less than 20mL/d, the drainage tube was withdrawn, and the patient gradually got out of bed to exercise while wearing a lumbar brace. Continue to take doxycycline, rifampicin combined with liver protection drugs in a standardized manner for 3 months, regularly review liver and kidney functions, and discontinue the drug until ESR and CRP return to normal range; review lumbar X-ray films and CT before discharge to evaluate the internal fixation system, lesion clearance, decompression and bone grafting.
Observation Indicators
Record and compare the following indicators between the two groups.①; Scale indicators: The recovery of patients’ clinical symptoms was evaluated according to the lowbackVAS, JOA, and ODI before and after 1 month and at the last follow-up;② Laboratory examinations: The preoperative and postoperative levels of CRP, ESR, HB, NLR, PLR, D-dimer and total protein were compared between the two groups of patients;③ Imaging examination: lumbar lordosis (LL) and disc space height (DH) were measured by X-ray and CT before and after operation;④ Surgery-related indicators and the occurrence of postoperative complications.
Statistical Methods
Statistical analysis was performed using “The Statistical Package for the Social Sciences” version 26.0 for Windows (IBM Corp., Armonk, NY, USA). Measurement data that conforms to the normal distribution are expressed as (x±s), and data between the two groups are compared using independent sample t-test; intra-group comparisons before surgery and at the last follow-up use paired t-test; comparisons between the two groups at multiple time points use repeated measures analysis of variance; measurement data that do not conform to the normal distribution use rank sum test. Counting data are expressed in frequency, and comparisons between groups are performed using X2 test or Fisher’s exact test; test level α=0.05, P<0.05 means that the difference is statistically significant.
Results
Analysis of the Number of Participants
A total of 41 patients with LBS were collected in this study and were divided into 2 groups according to the different surgical methods used, endoscopic group (Group A) and open surgery group (Group B). There were 15 patients in Group A, including 9 males and 6 females. The age was 48.73±12.12 years old, the average course of disease was 7.33±2.41 months, and the BMI was 24.24±3.62 kg/m2; There were 26 patients in Group B, including 17 males and 9 females, with an age of 52.46±11.618 years, an average course of disease of 6.15±2.03 months, and a BMI of 25.37± 4.53 kg/m2. See Figure 1 for details.
Comparison of Preoperative Data Between the Two Groups
There were no statistically significant differences between the two groups in gender, age, BMI, average course of disease, infected vertebral body segments, spinal cord ASIA grade, underlying diseases, blood biochemical indicators and imaging indicators (P>0.05, see Table 1).
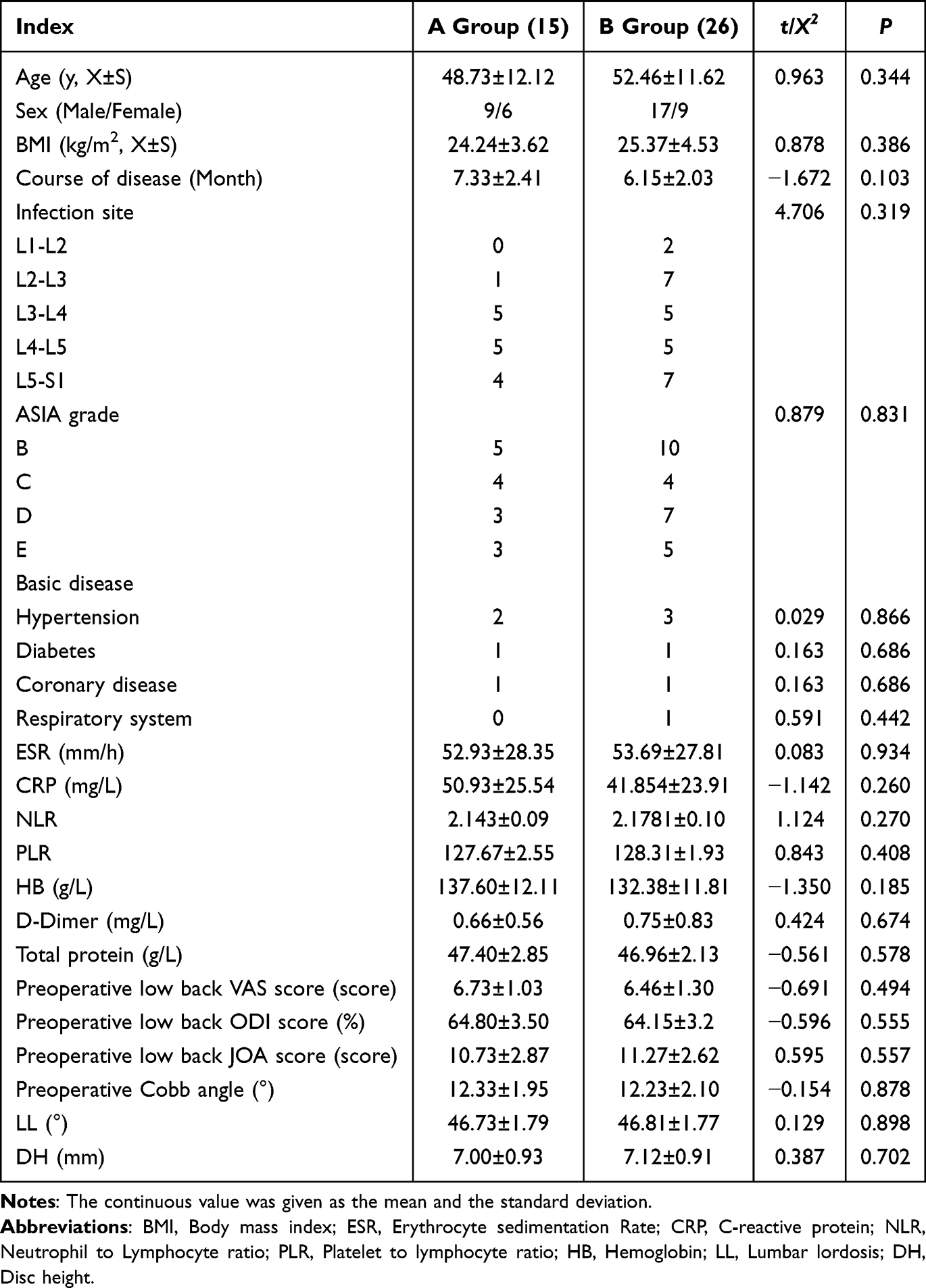 |
Table 1 Comparison of Patient Baseline Data |
Postoperative VAS, ODI and JOA Scores in Both Groups
Patients in both groups were followed up for 12 to 18 months, with an average of 14.8 months. The VAS,JOA score and ODI at each postoperative time in the two groups were significantly improved compared with the preoperative ones. The lumbar VAS at the last postoperative follow-up showed that the endoscopic group had a lower pain score, and the difference between the two groups was statistically significant (P<0.05); however, there was no statistically significant difference in JOA and ODI between the two groups (P>0.05, see Table 2).
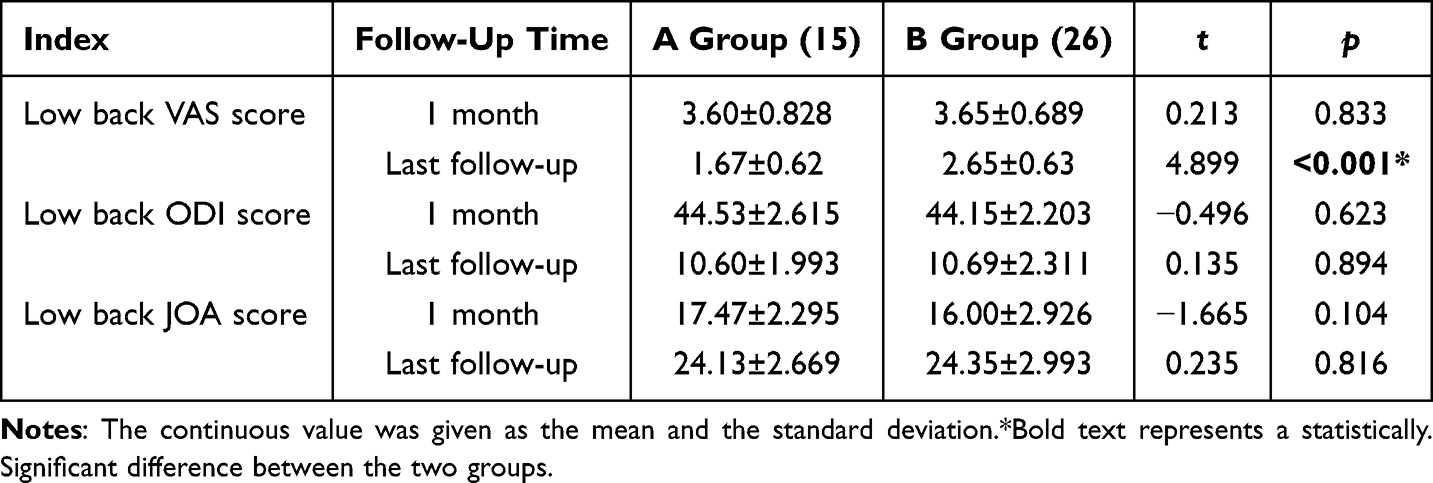 |
Table 2 Contrast of the Scale Indicators Between the Two Groups |
Comparison of Indexes at 1Month and Last Follow-Up Test in the Two Groups
Blood tests were performed after surgery in both groups. The postoperative hemoglobin in the endoscopic group was significantly higher than that in the open group, with statistical significance (P<0.05, see Figure 2); however, there was no significant difference in ESR, CRP, NLR, PLR, D-Dimer and Total protein between the two groups (P>0.05, see Table 3).
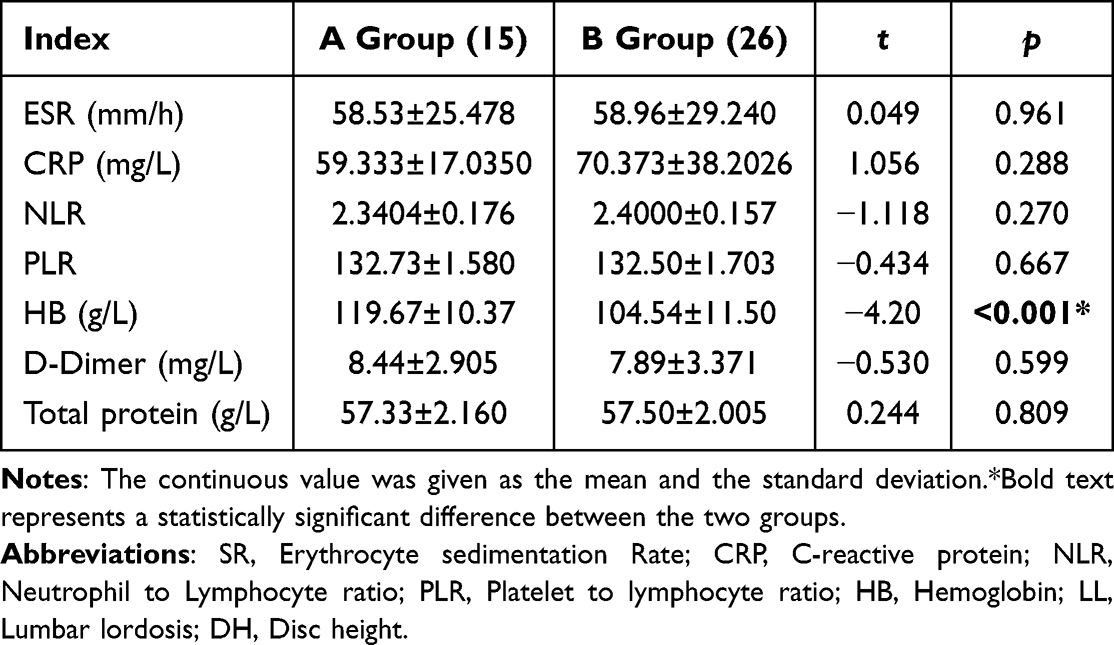 |
Table 3 Comparison of the Biochemical Blood Indexes Between the Two Groups |
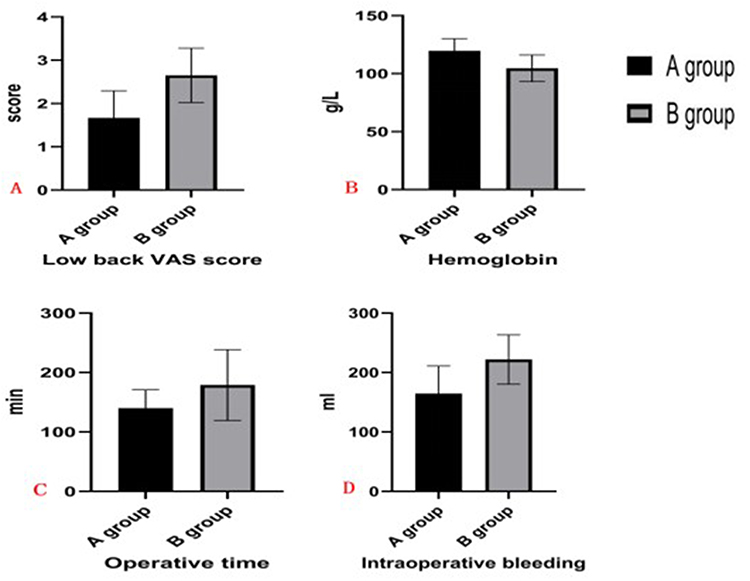 |
Figure 2 Box plot of secondary indicators compared between two groups of patients. Notes: (A) Postoperative low back pain VAS score, (B) Postoperative hemoglobin, (C) Operative time, (D) Intraoperative blood loss. |
Operation Time, Intraoperative Blood Loss, Postoperative Drainage Rate, Postoperative Drainage Time and LL Angle Were Compared in Both Group
Comparing the surgery-related indicators between the two groups, the results showed that the operation time, blood loss and Postoperative weight - bearing time in Group A were better than those in Group B, and the difference was statistically significant (P<0.05); but there were no statistically significant differences in postoperative hospital stay time, LL angle and DH between the two groups (P>0.05, see Table 4).
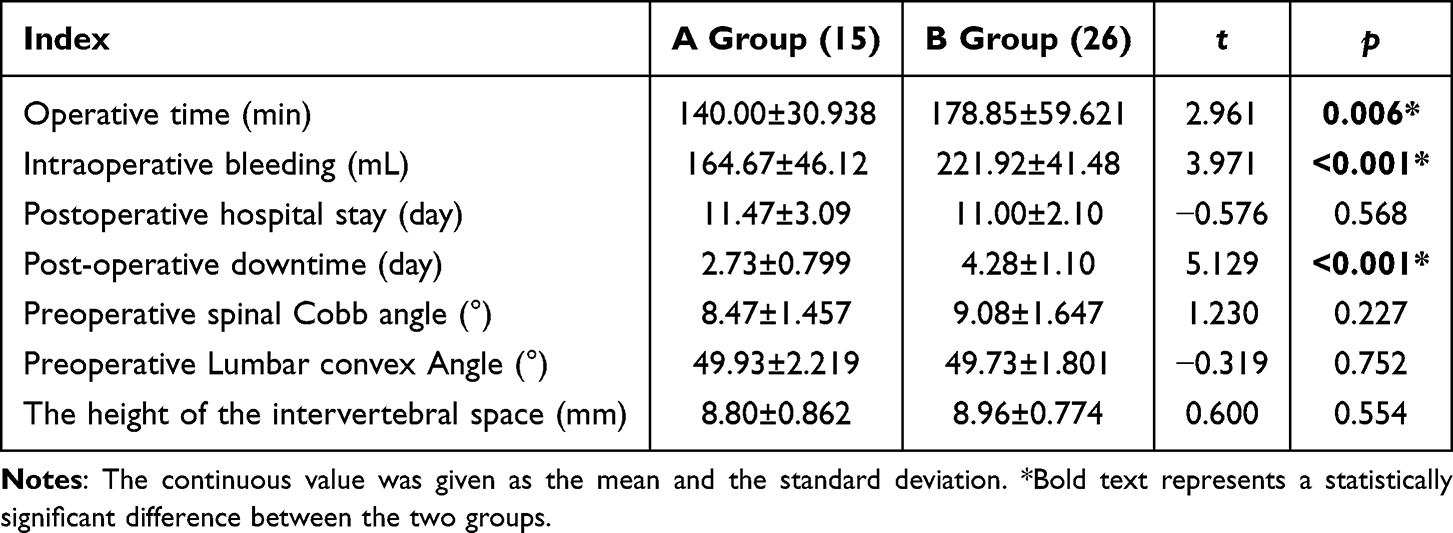 |
Table 4 Comparison of Surgery-Related Indicators Between the Two Groups |
Analysis of the Postoperative Complications in the Two Groups
Patients in both groups were followed up for 12 to 18 months, with an average of 14.8 months. After follow-up of patients in hospital or by telephone, it was found that adverse reactions occurred in both groups. One patient developed pressure sores after surgery in Group A and two patients in Group B; two patients in each Group 2 developed thrombosis after surgery; one patient in each Group 2 developed pulmonary infection after surgery; two patients in each Group 2 developed gastrointestinal symptoms after surgery; two patients in Group B had recurrence, but no patient in Group A had recurrence. There was no significant difference in the incidence of adverse reactions between the two groups (P>0.05, see Table 5).
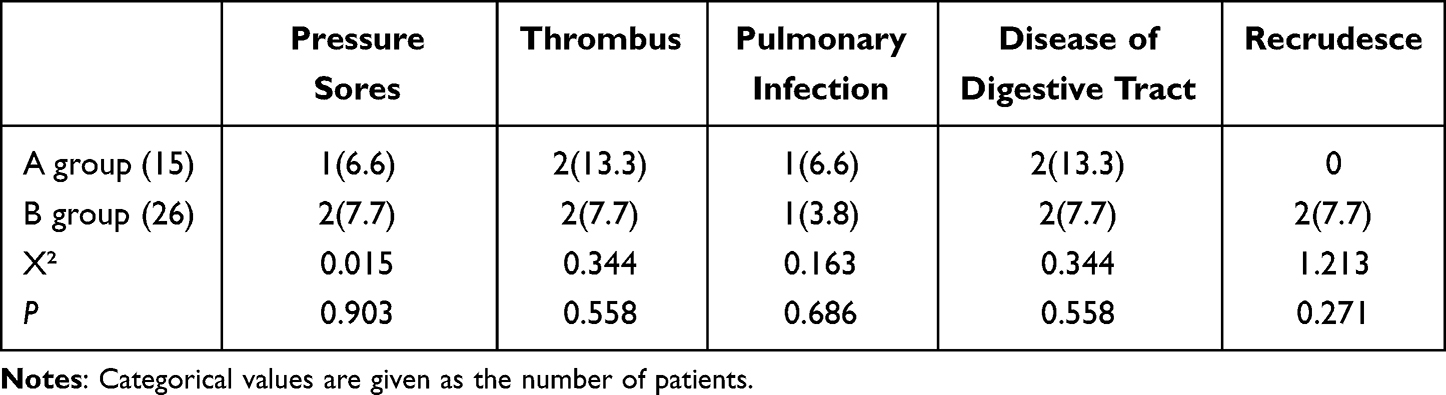 |
Table 5 Comparison of the Occurrence of Postoperative Adverse Reactions Between the Two Groups (n, %) |
Classic cases We by collecting two groups of patients before and after surgery follow-up image data comparison, compare the two different surgical methods will produce different surgical results, can be found in two groups of patients with postoperative spinal anatomical position, suggests two kinds of surgery are effective, intraoperative lesions inspection can confirm Brucella spondylitis (see Figures 3–5).
 |
Figure 3 Group A (endoscopic lesion clearance). The patient was a 50-year-old male with complaints of “back pain for 6 months accompanied by numbness and weakness of both lower limbs for 1 month” and was admitted to the hospital and was diagnosed with LBS. (A) and (B) are the positive and lateral DR images taken by the patient on admission; (C-F) shows the images before the surgery, The upper and lower endplates and edges of the vertebral body at the “white arrow” are eroded, which shows the bone defect and roughness of the vertebral margin. With the progression of the disease, the bone hyperplasia and sclerosis of the vertebral margin can appear. (G) and (H) shows the patient and the erosion lesion has been completely removed. |
 |
Figure 4 Pathological examination. (A) The patient’s Brucella rod lesion resected during surgery; (B) Pathological staining results (black arrow indicates Brucella). |
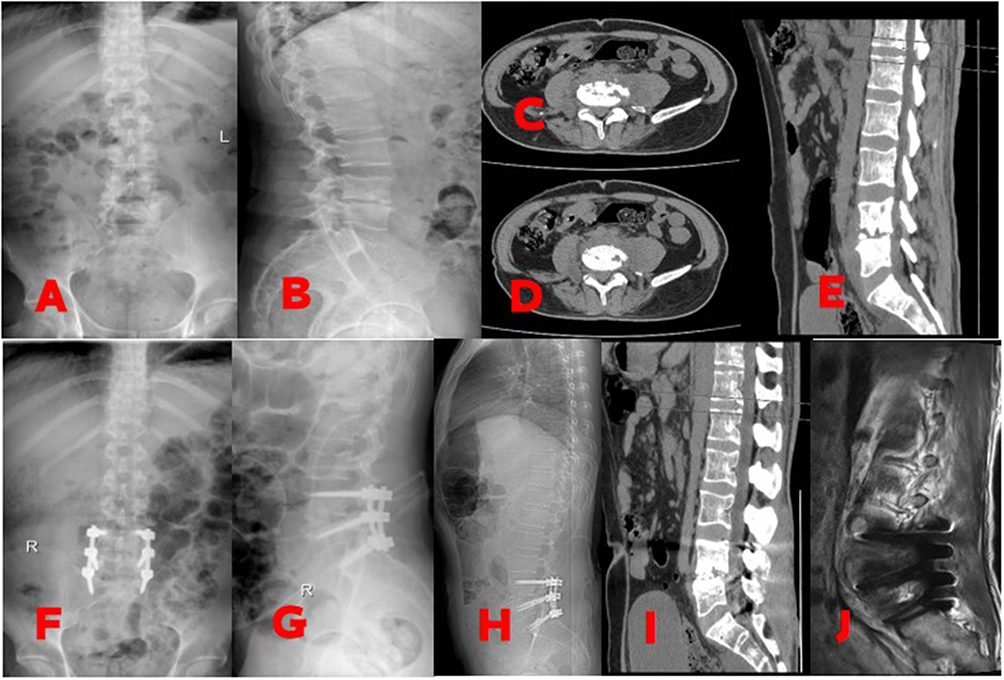 |
Figure 5 Group B (traditional incision lesion clearance, bone grafting, fusion and internal fixation). The 43-year-old male patient complained of “low back pain accompanied by weakness of both lower limbs for half a year” and was diagnosed with LBS; Figures (A-E) are the patient’s preoperative X-ray and CT results; Figures (F-J) are the patient’s postoperative X-ray, CT and MRI results. |
Group A (endoscopic lesion clearance), Pathological examination. Group B (traditional incision lesion clearance, bone grafting, fusion and internal fixation).
Discussion
LBS is one of the specific infectious diseases. The main clinical manifestations are vertebral abscess, vertebral destruction and inflammatory lesions of the intervertebral disc caused by Brucella infection.15,16 The disease is mainly cured through conservative treatment, but for those with significant lumbar instability, severe low back pain, and obvious neurological symptoms, if systemic conservative treatment drugs cannot relieve them, immediate surgical treatment is required.6,17,18 At present, there is no unified opinion on the surgical methods for this disease. Posterior focus clearance, bone graft, fusion and internal fixation is a more classic and recognized surgical method for the treatment of LBS. Compared with other surgical methods, this surgical method has the advantages of less incisions and less trauma. On the premise of not only achieving focus clearance, but also combining bone graft and internal fixation to maintain or rebuild spinal stability, correct deformities, and promote bone graft fusion. However, its destruction of posterior muscle ligaments can lead to postoperative complications such as chronic low back pain and muscle atrophy.19,20 Minimally invasive surgery through the intervertebral foramen approach has the advantages of significant postoperative efficacy and less trauma.8 After treating 15 patients with LBS with minimally invasive surgery through the intervertebral foramen approach, Wang Dong et al found that all patients had good postoperative bone graft healing, standard Brucella agglutination tests were all negative, and VAS and JOA scores were significantly improved compared with preoperative (P<0.01). However, these two surgical methods are rarely directly compared in patients with LBS, so this study evaluated and retrospectively compared the efficacy and safety of the two surgical methods.
The results of this study showed that the lumbar VAS score at the last postoperative follow-up in Group A was significantly lower than that in Group B, indicating that endoscopic surgery can reduce patients’ pain to a greater extent and improve their quality of life. A recent study by XU et al21 found that patients after lumbar foramen intervertebral lesion clearance had lower VAS and ODI than patients with traditional open surgery, which is basically consistent with our results. The postoperative hemoglobin index of patients in Group A was significantly higher than that of Group B, and the operating time and intraoperative blood loss of patients in Group A were significantly lower than those in Group B. This shows that traditional open surgery requires continuous stripping of soft tissue and small blood vessels during the operation, resulting in large amounts of blood loss and increased operation time, which causes greater damage to the patient’s body and longer postoperative recovery time. Endoscopic technology is operated in an aqueous environment. Continuous physiological saline flushing can compress tiny blood vessels and stop bleeding while ensuring clarity of the field of view under the microscope.The latest report by22 researchers shows that the use of endoscopic technology in spinal infection diseases can bring shorter operation time, bleeding volume and postoperative diversion, and can greatly shorten the recovery time of patients. Our results are similar to those, indicating that the endoscopic technique is less traumatic to the patients.Our results are similar, which suggests that endoscopic technology is less invasive to patients. ESR, CRP, NLR and PLR, as specific biochemical indicators of infectious diseases, did not decrease significantly after surgery in Group A and Group B. This may be related to the activation of the body’s inflammatory stress mechanism and the increase in the secretion of inflammatory factors.23 Our research results showed that post-operative imaging indicators showed that LL angle and DH in the two groups were significantly lower than before surgery, but there was no statistical significance between the two groups, which showed that both surgical methods have obvious treatment effects, both of which can improve postoperative interbody stability, restore the height of the intervertebral space, and contribute to postoperative rehabilitation. The above research results demonstrate that percutaneous endoscopic lesion resection as adjuvant treatment of LBS has clear preliminary clinical efficacy. This is a safe, feasible and effective method and provides a new direction for minimally invasive surgery to treat LBS.
Limitations of the Article
(1) The follow-up time of this study is short, which may have an impact on some outcome indicators; (2) The sample size included in this study is too small, and the statistical power is insufficient, which may have reporting bias; this may be because the number of patients with LBS is very small. It may also be that the trial team strictly controls the inclusion and exclusion criteria of samples, and randomized, large-sample, multi-center prospective studies will still be needed in the future; (3) Due to the diversity of patients, medical conditions, surgical methods, research methods, follow-up time and other variables, the reliability of the above conclusions needs to be confirmed by further prospective studies; (4) Due to the short follow-up period,Therefore, Cobb corner was not included.
Conclusion
To sum up, both surgical methods are safe and effective for the treatment of lumbar brucellosis; minimally invasive surgery through transforaminal approach has outstanding clinical efficacy in treating patients with LBS. It greatly reduces the patient’s pain and reduces the surgical time, bleeding volume and time to go to the ground, which is conducive to the patient’s postoperative recovery and is safer and more reliable. If conditions permit, it is recommended to choose endoscopic surgery for the treatment of LBS.
Abbreviations
LBS, Lumbar brucellosis spondylitis; BMI, Body mass index; ESR, Erythrocyte sedimentation Rate; CRP, C-reactive protein; NLR, Neutrophil to Lymphocyte ratio; PLR, Platelet to lymphocyte ratio; HB, Hemoglobin; LL, Lumbar lordosis; DH, Disc height.
Data Sharing Statement
The postoperative follow-up of patients with Brucella spondylitis (LBS) is incomplete, so the dataset analyzed in this study is not publicly available but is available to the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
We confirm that all experiments were performed in accordance with the Declaration of Helsinki. The study was approved by the Ethical Committee of the Sixth Affiliated Hospital of Xinjiang Medical University, NO. LFYLLSC202312 10-01. Each patient provided written informed consent before participating in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
National Natural Science Foundation of China (82260446); National Natural Science Foundation of China (81760411).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Hongjiang L, Yandong Z, Xianwei L. et al. Progress in diagnosis and treatment of spinal brucella infection [J]. J Cervical Back Pain. 2014;35(2):142–145.
2. Buzgan T, Karahocagil MK, Irmak H, et al. Clinical manifestations and complications in 1028 cases of brucellosis: a retrospective evaluation and review of the literature [J]. Int J Infect Dis. 2010;14(6):e469–78. doi:10.1016/j.ijid.2009.06.031
3. Chen Y, Yang JS, Li T, et al. One-stage Surgical Management for Lumbar Brucella Spondylitis by Posterior Debridement, Autogenous Bone Graft and Instrumentation: a Case Series of 24 Patients. Spine. 2017;42(19):E1112–e8. doi:10.1097/BRS.0000000000002093
4. Yaojun S, Xichang W, Yong L, et al. Analysis of magnetic resonance imaging characteristics of brucella spondylitis [J]. J Ningxia Med Univ. 2020;42(04):388–390.
5. Franco MP, Mulder M, Gilman RH, et al. Human brucellosis. Lancet Infect Dis. 2007;7(12):775–786. doi:10.1016/S1473-3099(07)70286-4
6. Abulizi Y, Cai X, Xu T, et al. Diagnosis and Surgical Treatment of Human Brucellar Spondylodiscitis. J Vis Exp. 2021;171:1.
7. Abudurexiti T, Haibier A, Yusufu A, et al. Retrospective Analysis of the Efficacy and Safety of Endoscopic Spinal Tuberculosis Focus Removal versus Posterior Pedicle Lesion Removal, Bone Grafting, and Internal Fixation Combined with Drug Chemotherapy for Thoracolumbar Tuberculosis. Infect Drug Resist. 2024;17:733–748. doi:10.2147/IDR.S449684
8. Lixing C, Xinming Y, Yongli J. Clinical efficacy of unilateral dual-channel endoscopic technique in the treatment of lumbar brucellosis spondylitis. J Pract Orthoped. 2024;30(05):438–442.
9. Chen L, Zhang J. Retrospective Evaluation of Short-Course versus Traditional Preoperative Chemotherapy in Thoracolumbar Spinal Tuberculosis Patients. Med Sci Monit. 2023;29:e941003. doi:10.12659/MSM.941003
10. Dunn RN, Ben Husien M. Spinal tuberculosis: review of current management. Bone Joint J. 2018;100(4):425–431. doi:10.1302/0301-620X.100B4.BJJ-2017-1040.R1
11. China Anti-tuberculosis Association Professional Branch of Bone and Joint Tuberculosis, China North China Bone Tuberculosis Alliance, China Western Bone Tuberculosis Alliance. Expert consensus on the diagnosis and treatment of brucella spondylitis [J]. China J Tuberculosis Prevent. 2022;44(6):531–538.
12. Ma S, Zhou Z, Wan Z, et al. Osteotomized debridement versus curetted debridement in posterior approach in treating thoracolumbar tuberculosis: a comparative study [J]. Eur Spine J. 2022;31(2):473–481. doi:10.1007/s00586-021-07075-w
13. Wu D, J SUN, Fan W, et al. Unilateral or Bilateral Percutaneous Endoscopic Debridement and Lavage Treatment for Lumbar Spinal Tuberculosis [J]. World Neurosurg. 2020;140:e73–e80. doi:10.1016/j.wneu.2020.04.132
14. Jie Y, Bin Z, Zhiquan W, et al. Efficacy analysis of transforaminal focus debridement and interbody fusion in the treatment of lumbar brucellosis [J]. China J Spine Spinal Cord. 2018;28(1):44–51.
15. Bagheri B, Ahmadi K, Chokan NM, et al. The Diagnostic Value of MRI in Brucella Spondylitis With Comparison to Clinical and Laboratory Findings [J]. Acta Inform Med. 2016;24(2):107–110. doi:10.5455/aim.2016.24.107-110
16. Zhihong C, Zhang N, Yuxi Z, et al. Observation on the effect of rat nerve growth factor on brucella spondylitis complicated with peripheral nerve injury. Ningxia Med J. 2016;38(11):1009–1011.
17. Ersoy Y, Sonmez E, Tevfik MR, et al. Comparison of three different combination therapies in the treatment of human brucellosis [J]. Tropical Doctor. 2005;35(4):210–212. doi:10.1258/004947505774938765
18. Colmenero JD, Cisneros JM, Orjuela SL, et al. Clinical course and prognosis of Brucella spondylitis [J]. Infection. 1992;20(1):38–42. doi:10.1007/BF01704893
19. Bei L, Yongming L, Jiandong Z, et al. Clinical efficacy comparison of UBE-LIF and posterior debridement, bone grafting, fusion and internal fixation in the treatment of lumbar brucellosis [J]. J Xi’an Jiaotong Univ. 2024;45(1):160–166.
20. Nazirhan S, Rui G, Shuwen Z, et al. Short-term efficacy comparison of self-anchored oblique lateral lumbar interbody fusion versus anterior fusion combined with posterior percutaneous pedicle screw fixation in the treatment of brucella spondylitis [J]. Chin J Bone Joint Surg. 2023;16(04):355–360.
21. Weiming X, Youwei G, Xu S, et al. Clinical efficacy and safety analysis of TLIF in patients with brucellosis [J]. J Inner Mongolia Medl Univ. 2020;42(6):561–4,75.
22. Kayierhan A, Haibier A, Aisaiti A, et al. Retrospective Analysis of the Efficacy and Safety of Endoscopic Spinal Tuberculosis and Brucellosis Lesion Removal and Posterior Pedicle Lesion Removal, Bone Grafting, Internal Fixation and Surgery Combined with Medical Chemotherapy in the Treatment of Spinal Tuberculosis and Brucellosis. Infect Drug Resist. 2024;17:3643–3656. doi:10.2147/IDR.S472558
23. Wu AM, Jin HM, Lin ZK, et al. Percutaneous anterior C1/2 transarticular screw fixation: salvage of failed percutaneous odontoid screw fixation for odontoid fracture. J Orthop Surg Res. 2017;12(1):141. doi:10.1186/s13018-017-0640-x
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.