")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Comparative Impact of Intravenous Iron Sucrose and Ferric Carboxymaltose on Hypophosphatemia and Anemia Parameters in Iron Deficiency Anemia: A Retrospective Study
Authors Aslan S , Doğan S , Sarıaydın M, Vural A , Kuloglu E, Muhtaroğlu A
Received 31 March 2025
Accepted for publication 10 June 2025
Published 25 June 2025 Volume 2025:21 Pages 987—993
DOI https://doi.org/10.2147/TCRM.S529064
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Garry Walsh
Iron Sucrose and Ferric Carboxymaltose in Iron Deficiency Anemia – Video abstract [529064]
Views: 104
Sefer Aslan,1 Serhat Doğan,2 Mehmet Sarıaydın,3 Aşkı Vural,4 Ersin Kuloglu,1 Ali Muhtaroğlu5
1Giresun University Faculty of Medicine, Department of Internal Medicine, Giresun, Turkey; 2Kayseri Special Acibadem Hospital, Department of General Surgery, Kayseri, Turkey; 3VM Medical Park Pendik Hospital, Department of Internal Medicine, İstanbul, Turkey; 4Adıyaman University Medical School, Department of Internal Medicine, Adıyaman, Turkey; 5Giresun University Faculty of Medicine, Department of General Surgery, Giresun, Turkey
Correspondence: Sefer Aslan, Giresun University Faculty of Medicine, Department of Internal Medicine, Giresun, 28100, Turkey, Tel +90 505 2202703, Email [email protected]
Aim: This study aimed to determine the incidence of hypophosphatemia and evaluate anemia parameters following intravenous iron sucrose (IS) and iron carboxymaltose (FCM) therapy in patients diagnosed with iron deficiency anemia (IDA).
Methods: This retrospective study included 108 patients aged 18– 67 who were diagnosed with IDA and received either FCM or IS therapy. The patients were divided into two groups: iron sucrose (n=55, 51%) and ferric carboxymaltose (n=53, 49%). We collected and analysed data on patient demographics, doses of FCM and IS, and laboratory parameters including serum phosphorus, ferritin, total iron-binding capacity (TIBC), iron, and haemoglobin (Hg) values.
Results: The pre-treatment blood phosphorus levels were significantly lower in the IS group than in the FCM group (p = 0.029). Following intravenous iron treatment, the TIBC and phosphorus levels were higher in the IS group compared to the FCM group (p = 0.011 and p < 0.001, respectively). The ferritin levels were significantly higher in the FCM group compared to the IS group (p = 0.002).
Conclusion: It is important to be aware that hypophosphatemia may occur after intravenous iron therapy for iron deficiency anemia. Therefore, phosphate levels should be monitored closely following treatment. Furthermore, it would appear that hypophosphatemia is more prevalent following FCM therapy compared to IS.
Keywords: iron deficiency anemia, hypophosphatemia, ferric carboxymaltose, iron sucrose, parenteral iron therapy, serum phosphorus
Introduction
Iron deficiency anemia (IDA) remains the most prevalent nutritional disorder worldwide and constitutes a significant public health challenge. According to the World Health Organization (WHO), anemia affects approximately 1.62 billion people globally, with iron deficiency accounting for about 50% of all anemia cases. This burden disproportionately impacts women of reproductive age and young children, with recent WHO estimates indicating that around 30% of non-pregnant women (aged 15–49 years) and over 40% of pregnant women are anemic, the majority due to iron deficiency.1 In low- and middle-income countries, the prevalence can exceed 60% among pregnant women, exacerbating maternal morbidity, perinatal complications, and impaired cognitive development in offspring.2.
Furthermore, the economic consequences of IDA—including reduced productivity and increased healthcare costs—pose substantial challenges to health systems worldwide. Despite ongoing global efforts, progress in reducing the prevalence of IDA has plateaued in recent years, underscoring the urgent need for improved diagnostic, preventive, and therapeutic strategies. Prevalence is higher in developing countries and among specific vulnerable populations, including women and children. The World Health Organization (WHO) defines anemia as haemoglobin levels below 12 g/dL in women and 13 g/dL in men. Iron deficiency is the primary cause of this condition. Typically, ferritin values below 100 µg/L and transferrin saturation below 20% are used as markers to attribute anemia to iron deficiency.3,4
Several intravenous iron formulations are currently approved for clinical use, differing in their molecular structures, pharmacokinetics, and safety profiles. These include iron sucrose, ferric carboxymaltose, iron dextran (both low- and high-molecular weight forms), iron isomaltoside, ferric derisomaltose, and ferumoxytol. Among these, iron sucrose and ferric carboxymaltose are the most commonly used due to their favorable safety profiles and widespread availability. Newer agents like ferric derisomaltose allow for larger single doses with reduced infusion times, improving patient convenience and compliance.5
While oral iron supplementation remains the recommended initial treatment for IDA, gastrointestinal intolerance, including nausea, constipation, and diarrhoea, often results in poor adherence, making intravenous (IV) iron therapy a preferred alternative, especially in patients with severe anemia or those with malabsorption disorders.6 Among IV iron therapies, ferric carboxymaltose (FCM) and iron sucrose (IS) are the most commonly used due to their efficacy in rapidly restoring iron levels. Both treatments are particularly beneficial in cases of IDA secondary to conditions such as chronic kidney disease, inflammatory bowel disease, heavy menstrual bleeding, and postpartum haemorrhage.7,8
FCM and IS are two of the most commonly used intravenous iron preparations, and both have been shown to be highly effective in correcting anemia. FCM is a newer formulation that allows for higher doses of iron to be administered in a single session, potentially reducing the number of infusions needed to achieve therapeutic iron levels.7 IS, despite being a more established treatment, remains a popular choice due to its favourable safety profile and effectiveness in milder cases. Both agents are generally well tolerated, although they do carry certain risks.9
One emerging side effect of IV iron therapy is hypophosphatemia, a potentially serious condition characterised by low phosphate levels in the blood.10 Phosphorus is an essential element for numerous biological functions, including energy production (via ATP synthesis), bone mineralisation and cellular signalling.11 The total body phosphorus in an adult weighing 70 kg is approximately 700–800 mg, with the majority of this stored in bones as hydroxyapatite. There has been an increase in reports of transient hypophosphatemia following IV iron therapy, particularly with FCM. However, the exact mechanisms remain unclear. One proposed explanation is that fibroblast growth factor 23 (FGF-23) may be involved, as this inhibits renal phosphate reabsorption, thus reducing serum phosphate levels.12
From a clinical perspective, hypophosphatemia can manifest in a range of ways, from mild fatigue and muscle weakness to more severe complications such as osteomalacia, fractures, and respiratory failure. In light of these risks, monitoring phosphate levels after IV iron therapy, particularly in high-risk groups, has become a priority for clinicians. While both FCM and IS can induce hypophosphatemia, FCM has been linked to a higher incidence of this condition due to its rapid administration in larger doses.13
The objective of this study is to evaluate the comparative efficacy of FCM and IS in the treatment of IDA, with a particular focus on their impact on serum phosphorus levels. By examining these two widely used iron preparations, this study aims to provide evidence-based guidance on their use, emphasising the importance of monitoring phosphate levels to prevent adverse outcomes in patients receiving parenteral iron therapy.
Methods
Ethical Aspects
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Adıyaman University Non-Interventional Clinical Research Ethics Committee (or Ethics Committee) (protocol code 2022/7-55 dated October 25, 2022) for studies involving humans.
Study Design
This retrospective study was conducted between October 2022 and November 2022 as an archive search using the database of our hospital. The study included 108 patients aged 18–67 years who were admitted to the internal medicine outpatient clinic for oral intake disorder, severe anemia, inflammatory bowel disease, severe uterine bleeding, postpartum hemorrhage and gastrointestinal blood loss, admitted to the internal medicine service with the diagnosis of iron deficiency anemia (IDA) and receiving parenteral FCM or IS treatment. Informed consent was not applied due to the retrospective nature of the study. Exclusion criteria were: (i) a history of coagulopathy or anticoagulant use, (ii) patients under 18 and over 67 years of age, (iii) patients whose serum phosphorus levels could not be measured before and after treatment were excluded, (iv) patients with iron deficiency anemia receiving oral iron therapy, (v) patients with malignancy. Patients were divided into two groups: ferrous sucrose (n=55) and ferric carboxymaltose (n=53).
Iron Preparates
Intravenous Iron Sucrose: Iron Sucrose was approved by the United States Food and Drug Administration in November 2000. Iron Sucrose is an iron hydroxide sucrose complex with a molecular weight of 34,000–60,000 Daltons. Administration is by i.v. injection or infusion. When administered at the recommended dose of 1000 mg, 100 mg is administered i.v. over 5 minutes, 1–3 times per week. The rate of administration should not exceed 20 mg per minute.
Intravenous Ferric Carboxymaltose: It is a colloidal solution of nanoparticles consisting of a polynuclear iron (III)-(oxyhydroxy) oxide core stabilized with carboxymaltose and can be administered as a single high-dose 15-minute infusion.
The formula for the total iron dose administered (mg) was calculated using the formula weight (kg) x (difference between normal hemoglobin and patient hemoglobin) x 2.4 + 500. In cases receiving ferric carboxymaltose treatment exceeding 1000 mg, treatment was completed with a one-week interval. Iron sucrose treatment was administered at a dose of 100 mg daily for a maximum of three days per week.Hemoglobin was examined using the Sysmex XN 1000 device from blood samples taken after 8 hours of fasting, and creatinine, ferritin, transferrin saturation, calcium and phosphorus were examined using the Roche Cobos 6000 device.
Statistical Analysis
The study data were analyzed on IBM SPSS Statistics version 22 software. Normality of distribution of the study parameters was investigated with using the Kolmogorov–Smirnov and Shapiro Wilk tests. In addition to descriptive methods (mean plus standard deviation), data for normally distributed qualitative parameters were compared between the groups using Student’s t test, while non-normally distributed parameters were compared between two groups using the Mann Whitney U-test. Intragroup comparisons of normally distributed parameters were performed using the paired sample t test, while non-normally distributed parameters were compared using the Wilcoxon sign test. Significance was set at p<0.05.
Results
The study was performed with 108 women aged between 18 and 67 (mean age 38.15±9.72). The cases were evaluated under two groups - “Iron sucrose” (n=55) and “Ferric carboxymaltose” (n=53).
For the pre-treatment phosphorus levels of the included patients, the blood levels of the patients in the IS group were found to be significantly lower than those in the FCM group (p = 0.029). Pretreatment iron laboratory parameters, hemoglobin and phosphorus levels showed significant changes in both drugs after the treatments applied (p < 0.05). After iron treatments, TIBC and phosphorus levels were found to be higher in the group receiving IS than in the group receiving FCM (p = 0.011, p < 0.001, respectively).
The ferritin level was statistically significantly higher in the FCM group than in IS (p = 0.002) (Table 1).
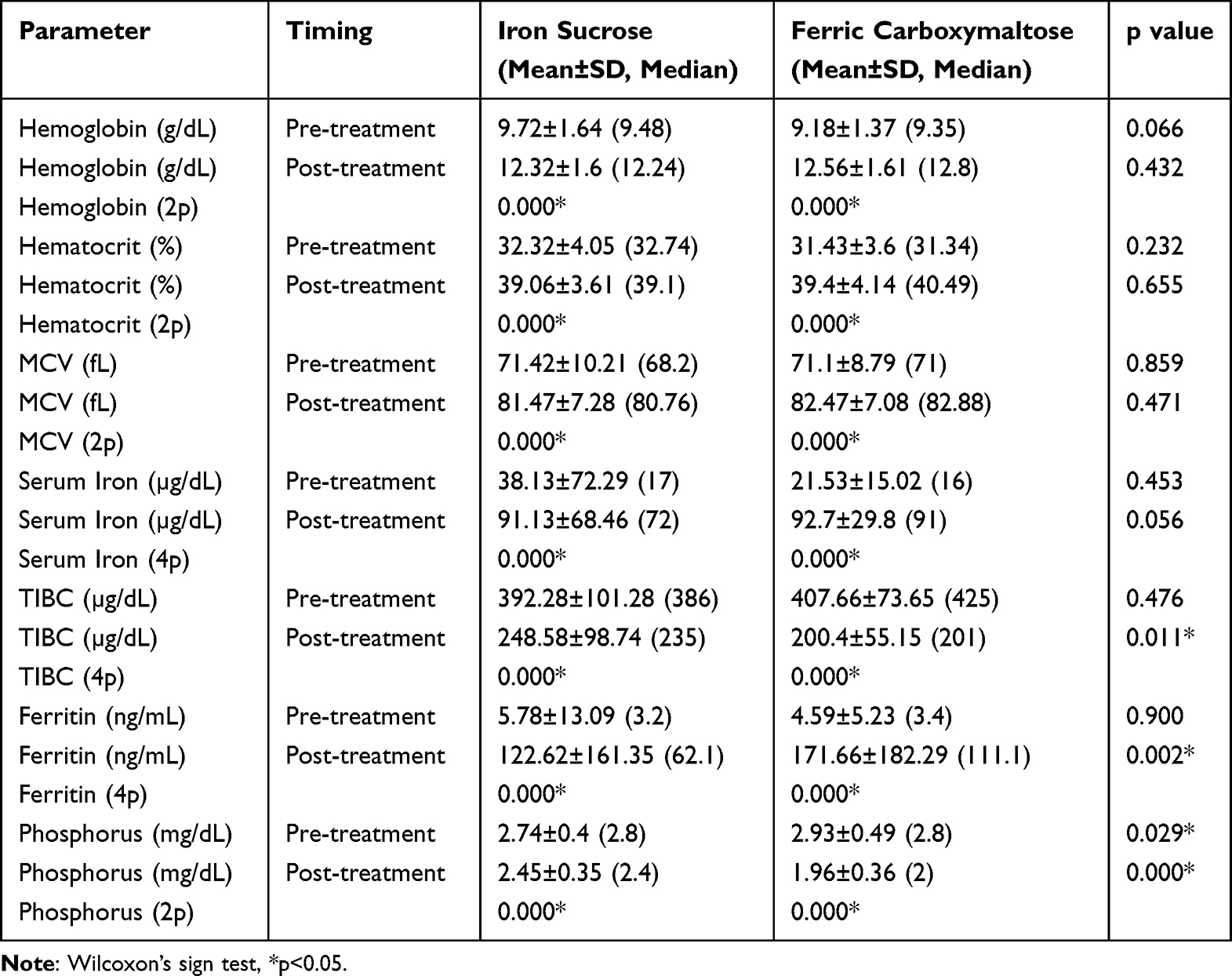 |
Table 1 Intra- and Intergroup Analyses |
The amount of increase in hemoglobin and ferritin levels after treatment in the FCM group was significantly higher compared to the IS group compared to the pre-treatment values (p=0.021 and p=0.002).
The amount of increase in iron levels after treatment in the FCM group was significantly lower compared to the IS group compared to the pre-treatment values (p=0.023).
The amount of decrease in TBIC levels after treatment was significantly higher in the FCM group compared to the IS group compared to the pre-treatment values (p=0.002).
The amount of decrease in phosphorus levels after treatment was significantly higher in the FCM group compared to the IS group compared to the pre-treatment values (p=0.000) (Table 2).
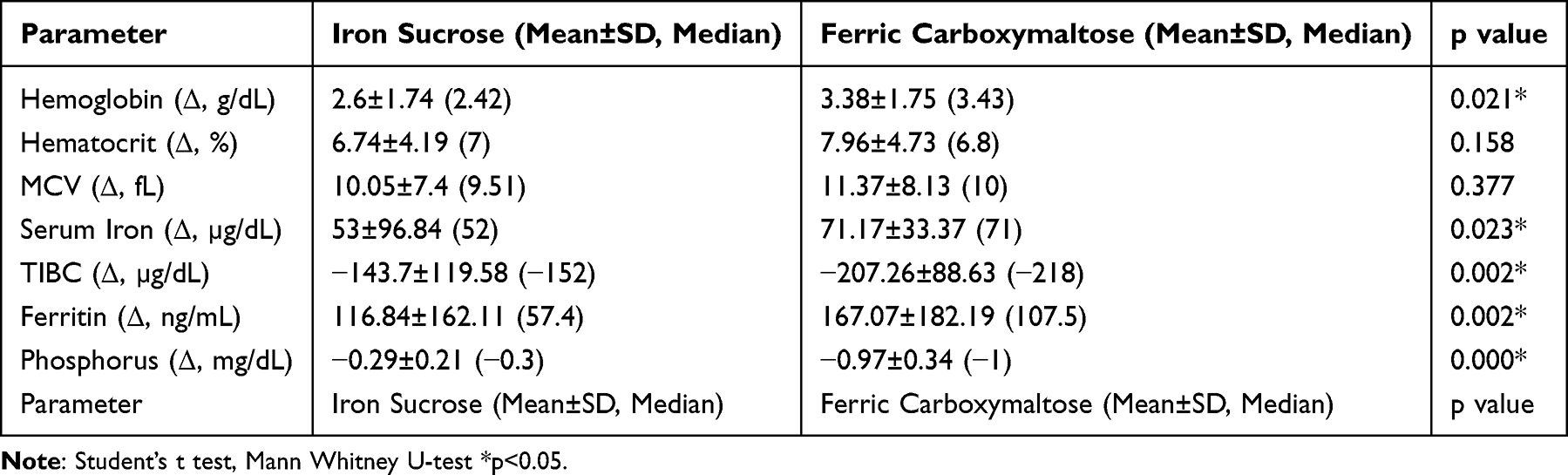 |
Table 2 Post-Treatment Changes in the Study Parameters Compared to Pre-Treatment Values Between the Groups |
Discussion
This study offers valuable insights into the comparative efficacy of FCM and IS in the treatment of IDA, with a particular emphasis on their impact on serum phosphorus levels. Although frequently disregarded, hypophosphatemia represents a significant adverse effect of intravenous iron therapy.14 Our findings contribute to the accumulating evidence based on this topic.
The results demonstrated that both FCM and IS effectively improved haemoglobin and ferritin levels in patients with IDA. However, a key differentiating factor between the two treatments is their impact on serum phosphorus levels. In accordance with the findings of previous research, it was observed that FCM was associated with a significantly greater reduction in serum phosphorus levels in comparison to IS.15 This finding is particularly relevant in light of the increasing clinical attention being paid to the risk of hypophosphataemia in patients receiving parenteral iron therapy.
The occurrence of hypophosphataemia following FCM therapy has been extensively documented in scientific literature.16 Fukumoto et al demonstrated that FCM-induced hypophosphatemia occurred in approximately 50% of patients with normal renal function, while IS caused hypophosphatemia in fewer than 10% of patients. Our findings corroborate this hypothesis, providing further evidence that FCM has a higher propensity to cause phosphate depletion, potentially due to its rapid administration and high dosing potential.17 The underlying mechanism is believed to be the upregulation of fibroblast growth factor 23 (FGF-23), which inhibits renal phosphate reabsorption, resulting in a significant reduction in serum phosphate levels.
The clinical significance of this finding cannot be overstated. Although hypophosphataemia was transient and did not reach severe levels in our cohort, prolonged or severe hypophosphataemia has been associated with serious complications, including osteomalacia, fractures and muscle weakness.18 Additionally, long-term hypophosphataemia may impair recovery in patients with chronic diseases, including those with inflammatory bowel disease or chronic kidney disease, where phosphorus plays a key role in bone and muscle health.
It is noteworthy that DeFilipp et al observed that in patients with iron deficiency secondary to bariatric surgery, FCM yielded a more rapid haemoglobin response than IS.19
This finding suggests that the accelerated correction of anemia with FCM may confer a clinical advantage in certain circumstances. However, they also emphasised the necessity for close monitoring of serum phosphorus levels, particularly in patients receiving repeated doses of FCM over a short period.
The implications of our findings for clinical practice are twofold. Firstly, while FCM is highly effective in rapidly correcting iron deficiency, clinicians must be vigilant about the potential for significant phosphate depletion, particularly in patients who may already be at risk of hypophosphataemia, such as those with malnutrition, chronic kidney disease, or prolonged use of phosphate binders. Secondly, IS may be a safer alternative for patients in whom the risk of hypophosphatemia is a concern. However, it should be noted that this alternative requires more frequent dosing and may not correct anemia as rapidly as FCM.
As no severe cases of hypophosphatemia were identified in our study, we recommend that serum phosphate levels be monitored routinely after IV iron therapy, particularly in high-risk groups. This recommendation aligns with those of Glaspy et al, who suggest that phosphate monitoring should be incorporated into the management of patients receiving FCM, particularly in the context of chronic kidney disease and other disorders that predispose patients to bone-mineral imbalances.20
Ferric carboxymaltose (FCM) is an effective and convenient option for treating iron deficiency anemia, allowing for rapid correction with high single-dose infusions. However, recent evidence highlights an increased risk of hypophosphatemia, particularly with repeated dosing. This effect is mediated by elevated fibroblast growth factor 23 (FGF23), leading to renal phosphate wasting and, in some cases, muscle weakness or bone pain. Although often asymptomatic and transient, monitoring serum phosphate levels is recommended in high-risk patients. The therapeutic benefit of FCM must be carefully weighed against its potential impact on mineral metabolism.21
Routine phosphate supplementation is not universally recommended for all patients receiving intravenous iron therapy. However, in cases of moderate to severe hypophosphatemia, particularly when symptomatic or prolonged, oral phosphate supplementation may be considered. Clinical guidelines suggest monitoring serum phosphate levels in high-risk individuals—such as those receiving repeated high-dose ferric carboxymaltose (FCM), with vitamin D deficiency, or underlying malnutrition—and initiating supplementation on a case-by-case basis. Additionally, correction of contributing factors such as vitamin D insufficiency is advised to support phosphate homeostasis.22
Strengths and Limitations
One key strength of our study is the relatively large sample size and the direct comparison between two commonly used intravenous iron preparations. However, it should be noted that the study is not without limitations. Firstly, the retrospective nature of the study may introduce biases related to data collection. Secondly, the lack of iFGF-23 and vitamin D level assessments limits our ability to fully explore the mechanisms of hypophosphatemia. Further prospective studies incorporating these parameters will be required to ascertain the precise biochemical pathways involved in FCM-induced hypophosphataemia.
Another limitation is the difference in the dosages of FCM and IS used, which may have influenced the results. Although higher doses of FCM were administered, the comparison reflects real-world practice, where FCM is often given in larger doses due to its pharmacokinetic properties.
Conclusion
Our study reveals the vital importance of monitoring phosphorus levels in patients receiving intravenous iron therapy, particularly those treated with FCM. While both FCM and IS are effective in correcting iron deficiency anemia, FCM carries a greater risk of inducing hypophosphatemia. This presents an exciting opportunity for clinicians to carefully consider the risk-benefit profile of these agents, especially in patients with pre-existing risk factors for phosphate depletion. Future research should focus on prospective trials with standardised dosing protocols and include biochemical assessments to further clarify the pathophysiology of FCM-induced hypophosphatemia, which will undoubtedly lead to more effective treatments in the future.
Ethics Declaration
Ethical approval of this study was obtained from the Ethics Department of Adıyaman University Faculty of Medicine with the decision dated 25.10.2022 and numbered 2022/7-55 before starting the research study.
Consent Statement
Informed consent was not obtained for this study because it was retrospective in nature. The requirement for consent was waived by the ethics committee, as the study involved the analysis of existing de-identified data, and no additional risks were posed to the patients.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was not supported or funded by any drug company.
Disclosure
The authors report no conflicts of interest for this work.
References
1. World Health Organization. The global prevalence of anaemia in 2011. Geneva: WHO; 2015. Available from: https://apps.who.int/iris/handle/10665/177094.
2. World Health Organization. Micronutrient deficiencies – iron deficiency anaemia. WHO; Available from: https://www.who.int/health-topics/anaemia#tab=tab_1.
3. Agarwal AM, Rets A. Laboratory approach to investigation of anemia in pregnancy. Int J Lab Hematol. 2021;43:65–70. doi:10.1111/ijlh.13551
4. Filippatos G, Ponikowski P, Farmakis D, et al; F Investigators. Association between hemoglobin levels and efficacy of intravenous ferric carboxymaltose in patients with acute heart failure and iron deficiency: an AFFIRM-AHF subgroup analysis. Circulation. 2023;147(22):1640–1653. doi:10.1161/CIRCULATIONAHA.122.060757.
5. Auerbach M, Macdougall IC. Safety of intravenous iron formulations: facts and folklore. Blood Transfus. 2014;12(3):296–300. doi:10.2450/2014.0021-14
6. Pollock RF, Biggar P. Indirect methods of comparison of the safety of ferric derisomaltose, iron sucrose and ferric carboxymaltose in the treatment of iron deficiency anemia. Expert Rev Hematol. 2020;13(2):187–195. doi:10.1080/17474086.2020.1709437
7. Argüelles-Arias F, Bermejo F, Borrás-Blasco J, et al. Cost-effectiveness analysis of ferric carboxymaltose versus iron sucrose for the treatment of iron deficiency anemia in patients with inflammatory bowel disease in Spain. Therap Adv Gastroenterol. 2022;15:17562848221086131. doi:10.1177/17562848221086131
8. Hagras AM, Hussein NA, Abdelazim I, Elhamamy N. Ferric carboxymaltose for treatment of iron deficiency and iron deficiency anemia caused by abnormal uterine bleeding. Prz Menopauzalny. 2022;21(4):223–228. doi:10.5114/pm.2022.124013
9. Jin J, Ran Z, Noseda E, et al. A randomized, controlled, open label non-inferiority trial of intravenous ferric carboxymaltose versus iron sucrose in patients with iron deficiency anemia in China. Front Med. 2024;18(1):98–108. doi:10.1007/s11684-023-1001-2
10. Seng NW, Barco JB, Wong MH, et al. Hypophosphatemia related to intravenous iron therapy with ferric carboxymaltose: a case series. Transfus Med. 2023;33(6):503–508. doi:10.1111/tme.12980
11. Penido MG, Alon US. Phosphate homeostasis and its role in bone health. Pediatr Nefrol. 2012;27(11):2039–2048. doi:10.1007/s00467-017-3713-5
12. Amanzadeh J, Reilly RF. Hypophosphatemia: an evidence-based approach to its clinical consequences and management. Nat Clin Pract Nephrol. 2006;2(3):
13. Schaefer B, Zoller H, Wolf M. Risk factors for and effects of persistent and severe hypophosphatemia following ferric carboxymaltose. J Clin Endocrinol Metab. 2022;107(4):1009–1019. doi:10.1210/clinem/dgab852
14. Van Doren L, Steinheiser M, Boykin K, Taylor KJ, Menendez M, Auerbach M. Expert consensus guidelines: intravenous iron uses, formulations, administration, and management of reactions. Am J Hematol. 2024;99(7):1338–1348. doi:10.1002/ajh.27220
15. Chu Z, Cushway T, Wong M, et al. Incidence and predictors of hypophosphataemia after ferric carboxymaltose use-A 3-year experience from a single institution in Singapore. Br J Haematol. 2023;202(6):1199–1204. doi:10.1111/bjh.18979
16. Zoller H, Wolf M, Blumenstein I, et al. Hypophosphataemia following ferric derisomaltose and ferric carboxymaltose in patients with iron deficiency anemia due to inflammatory bowel disease (PHOSPHARE-IBD): a randomised clinical trial. Gut. 2023;72(4):644–653. doi:10.1136/gutjnl-2022-327897
17. Fukumoto S, Murata T, Osuga Y, Pollock RF. IFGF23-related hypophosphatemic diseases: recent progress and future perspectives. Calcif Tissue Int. 2021;108(2):132–140. doi:10.1007/s00223-020-00749-5
18. Fierz YC, Kenmeni R, Gonthier A, Lier F, Pralong F, Coti Bertrand P. Severe and prolonged hypophosphatemia after intravenous iron administration in a malnourished patient. Eur J Clin Nutr. 2014;68(4):531–533. doi:10.1038/ejcn.2014.20
19. DeFilipp Z, Lister J, Gagné D, Shadduck RK, Prendergast L, Kennedy M. Serum phosphate levels and hypophosphatemia risk with ferric carboxymaltose versus iron sucrose in hematology patients. Transfusion. 2017;57(8):1959–1965. doi:10.1111/trf.14161
20. Glaspy JA, Lim-Watson MZ, Libre MA, et al. A randomized trial comparing iron isomaltoside 1000 with iron sucrose in patients with cancer-related anemia. Ann Oncol. 2013;24(4):943–950. doi:10.1093/annonc/mds578
21. Schouten BJ, Doogue MP, Soule SG, Hunt PJ. Iron polymaltose-induced hypophosphatemia in patients with chronic kidney disease. Nephrology. 2009;14(6):587–590. doi:10.1111/j.1440-1797.2009.01112.x
22. Schouten BJ, Hunt PJ, Livesey JH, Frampton CM, Soule SG. Fasting fibroblast growth factor 23 levels are associated with serum phosphate and bone turnover markers but not 1,25-dihydroxyvitamin D. J Clin Endocrinol Metab. 2009;94(11):4224–4230. doi:10.1210/jc.2009-0800
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.