")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Comparative Outcomes of Apical Induction Versus Pulp Revascularization in Young Permanent Anterior Teeth with Traumatic Pulp Necrosis
Authors Cheng G, Wu X, Li W, Lv Z
Received 21 February 2025
Accepted for publication 4 May 2025
Published 21 May 2025 Volume 2025:21 Pages 737—745
DOI https://doi.org/10.2147/TCRM.S522358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Gang Cheng, Xiuyin Wu, Wenbo Li, Zhijun Lv
Department of Stomatology, People’s Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, People’s Republic of China
Correspondence: Zhijun Lv, Email [email protected]
Objective: This study aims to evaluate and analyze the clinical application of pulp revascularization surgery in young permanent anterior teeth with pulp necrosis caused by trauma.
Methods: This study selected 40 cases of young permanent anterior teeth with pulp necrosis caused by trauma, treated at our hospital between August 2018 and December 2022. All patients met the complete inclusion criteria and were divided into a study group and a control group based on treatment methods. The study group received pulp revascularization surgery, and the control group received apical induction surgery. There were 20 patients in each group. Comparative observation indicators included clinical treatment outcomes, clinical-related indicators, pain levels, and patient family satisfaction.
Results: The treatment outcomes in the study group were significantly better than those in the control group (P < 0.05). The crown-to-root ratio in the study group was lower than that in the control group, and the root canal wall thickness was higher in the study group, with all P < 0.05. The pain level grading in the study group was significantly lower than that in the control group (P < 0.05). Satisfaction indicators for both patients and their families were significantly higher in the study group compared to the control group, with all P < 0.05.
Conclusion: Pulp revascularization surgery shows great potential in the clinical application for young permanent anterior teeth with pulp necrosis caused by trauma. It can effectively improve the treatment outcomes, clinical indicators, and alleviate pain, while significantly enhancing patient satisfaction. With continuous research and practice, this advanced treatment method is expected to provide a better oral health experience for patients and promote the development of the dental field.
Keywords: pulp revascularization surgery, young permanent teeth, anterior teeth, pulp necrosis caused by trauma, clinical application
Introduction
Oral health has always been a topic of significant concern, and especially in the dental field, the continuous emergence of treatment methods and technologies has made the management of various dental problems more precise and diverse. Traumatic injury to permanent anterior teeth is relatively common among adolescents and children, as their growth and development are not yet fully matured, making the pulp more susceptible to external stimuli that could lead to necrosis.1 Young permanent anterior teeth trauma refers to a type of dental injury occurring during adolescence and childhood, typically involving the facial or oral regions.2,3 Such trauma can result from accidents, sports injuries, falls, or other head-related injuries. Among the complications, pulp necrosis is relatively common, especially when the trauma causes damage to the pulp tissue. The pulp is the central part of the tooth, consisting of nerves and blood vessels.4 When a tooth is traumatized, the pulp may suffer from direct impact or chronic damage due to fractures, cracks, or other conditions. In such cases, blood supply to the pulp is compromised, which can eventually lead to pulp necrosis.5
Symptoms of pulp necrosis in young permanent anterior teeth may include tooth pain, discoloration, swelling, and sensitivity to hot and cold stimuli.6 In children and adolescents, due to the incomplete maturation of teeth, their ability to adapt to external stimuli is relatively weaker, making them more prone to pulp necrosis.7 Traditional treatments for this condition, such as root canal therapy and pulpectomy, rely on advanced nickel-titanium (NiTi) rotary instruments that have demonstrated high predictability in mechanical performance. For instance,8 showed that modern NiTi files like F-One Blue exhibit superior cyclic fatigue resistance (604.16 NCF vs 300.5 NCF) and flexibility (29 gcm vs 50 gcm bending load) compared to conventional instruments (eg, ProTaper Gold F2), highlighting the technical precision achievable in endodontics.8,9 However, even with these advancements, such methods inherently require the removal of vital pulp tissue, which may compromise the tooth’s long-term biological resilience and increase restorative challenges, including structural fragility and aesthetic compromises.
In this context, pulp revascularization surgery has emerged as a promising alternative, aiming to preserve pulp vitality and circumvent the need for conventional endodontic intervention.10 By promoting natural tissue regeneration, this forward-looking approach offers a biologically driven solution for restoring the health and function of traumatized teeth.11 This article explores the clinical application of pulp revascularization surgery in young permanent anterior teeth with pulp necrosis caused by trauma, examining its potential advantages in protecting tooth vitality, promoting regeneration, and improving patients’ quality of life. Through a deeper understanding of this innovative technology, we hope to advance a paradigm shift in oral medicine, prioritizing minimally invasive strategies that align with the patient’s inherent healing capacity.
Materials and Methods
Subjects
This study selected 40 patients who were treated for young permanent anterior teeth with pulp necrosis caused by trauma at the Department of Stomatology, our hospital, from August 2018 to December 2022. All enrolled patients were diagnosed through detailed clinical observation and assessment, and were strictly selected based on the complete inclusion criteria. The patients and their guardians were informed and consented to participate in this study by signing an informed consent form. A total of 40 cases were included. The patients were divided into two groups based on the treatment method: the study group (n = 20), who received pulp revascularization surgery, and the control group (n = 20), who received apical induction surgery. This study was approved by the Ethics Committee of People’s Hospital Affiliated to Shandong First Medical University (approval number: KQXF240011). The research process strictly adhered to the ethical guidelines of the Declaration of Helsinki. Informed consent was obtained from all study participants.
Inclusion and Exclusion Criteria
Inclusion Criteria
Complete medical records of patients. All patients had young permanent anterior teeth with pulp necrosis caused by trauma. The involved teeth were in Nolla stages 7–9. Good patient compliance and overall health status.
Exclusion Criteria
Patients with a history of antibiotic allergies or related systemic diseases. Patients with cracks or periodontal disease. Individuals with severe damage to vital organs such as the heart, lungs, or kidneys. Patients with cognitive disorders or communication difficulties.
Methods
Pulp Revascularization Surgery
Before surgery, we performed X-ray examinations to assess the periapical condition and the development of the root. All procedures were carried out under a microscope. After local anesthesia with 2% lidocaine, a rubber dam was applied for moisture control, and pulp exposure was performed. Then, the root canal was irrigated with 20 mL of 3% sodium hypochlorite solution and saline. For all cases undergoing this procedure, triple antibiotic paste (a mixture of ciprofloxacin, metronidazole, and minocycline) was uniformly used to disinfect the root canal. Calcium hydroxide was not used in this group to ensure consistency in the disinfection protocol. After placement of the intracanal medicament, glass ionomer was applied to seal the crown. The patient was re-examined after three weeks.
After local anesthesia and rubber dam isolation, temporary sealing materials were removed, and the root canal was irrigated again with 3% sodium hypochlorite, followed by ultrasonic cleaning and removal of the paste. The canal was dried with paper points. Using a 40# K-file, we pierced the periapical tissue and induced bleeding to a depth of 2–3 mm below the enamel-cementum junction. After 15 minutes, a collagen membrane was placed over the blood clot, followed by mineral trioxide aggregate (MTA). One week later, a glass ionomer cement was used as a base, and the final filling was performed with light-cured composite resin. Follow-up evaluations were performed at 3-month intervals for up to 12 months, using clinical examination and radiographic imaging to assess root development, periapical healing, and absence of symptoms. Treatment success was defined as continued root maturation and resolution of periapical radiolucency, whereas failure was identified by persistence or recurrence of symptoms, or lack of radiographic healing.
Apical Induction Surgery
After local anesthesia, we used conventional methods to prepare the cavity and perform pulp exposure, cleaning the necrotic infected pulp. After root canal preparation, the canal was dried. A calcium hydroxide paste was used for all cases in this group, and after one week of camphorated phenol root canal sealing, we ensured that there was no exudation or discomfort. We then used a spiral obturator to introduce the well-mixed calcium hydroxide paste into the root canal, injecting it layer by layer until full. X-ray examination was performed to ensure adequate filling. A glass ionomer was used for temporary filling of the cavity, and the patient was followed up until the apex closure was achieved. Afterward, conventional thermoplastic gutta-percha root canal filling was performed, followed by dental restoration.9,12 Follow-up for this group was also conducted at 3-month intervals for up to 12 months, utilizing both clinical assessments and radiographs to evaluate apical closure and symptom resolution. Treatment success was defined as radiographic evidence of apical closure without symptoms, while failure included persistence of open apex or clinical signs of infection.
Observation Indicators
Treatment Effect
The evaluation included three indicators: cure, improvement, and failure. The effective treatment rate was calculated as the sum of the number of cured and improved cases divided by the total number of cases, multiplied by 100%.
Clinical Indicators
Post-treatment, we measured the clinical indicators of the affected tooth in both groups using radiographic methods, including root length, crown-to-root ratio, and root canal wall thickness.
Pain Level
The Endodontic Interappointment Pain (EIP) scale was used to assess pain during root canal treatment. The scale had different levels: level 0 indicated no pain, level 1 indicated mild pain, level 2 indicated pain requiring medication, and level 3 indicated severe pain.
Satisfaction
A self-designed survey questionnaire was used to assess patient and family satisfaction. The questionnaire focused on four aspects: occlusal function, chewing ability, color, and overall aesthetics. The evaluation scale was 0 points for dissatisfaction and 10 points for full satisfaction.
Data Analysis
Data collection for this study was conducted using Excel software. Statistical analysis was performed using SPSS 22.0 software, and image generation was done with GraphPad Prism 8 software. Count data were expressed as percentages (%) and analyzed using the chi-square test; measurement data were expressed as mean ± standard deviation (±s) and analyzed using the t-test. P < 0.05 was considered statistically significant.
Results
Clinical Data
The study included 20 patients in each group, with a balanced gender distribution (13 males and 7 females per group). In the study group, ages ranged from 8 to 14 years (mean 10.25 ± 2.05 years), symptom onset time was 1–13 days (mean 5.50 ± 3.66 days), and Nolla stage distribution was 9 patients in stage 8 and 11 in stage 9. The control group had similar demographics: age 8–14 years (mean 10.90 ± 2.10 years), symptom duration 1–13 days (mean 5.20 ± 3.46 days), and Nolla stages 10 patients in stage 8 and 10 in stage 9. Comparative analysis revealed no statistically significant differences in baseline clinical data (P > 0.05), confirming the groups were well-matched for further evaluation (Table 1).
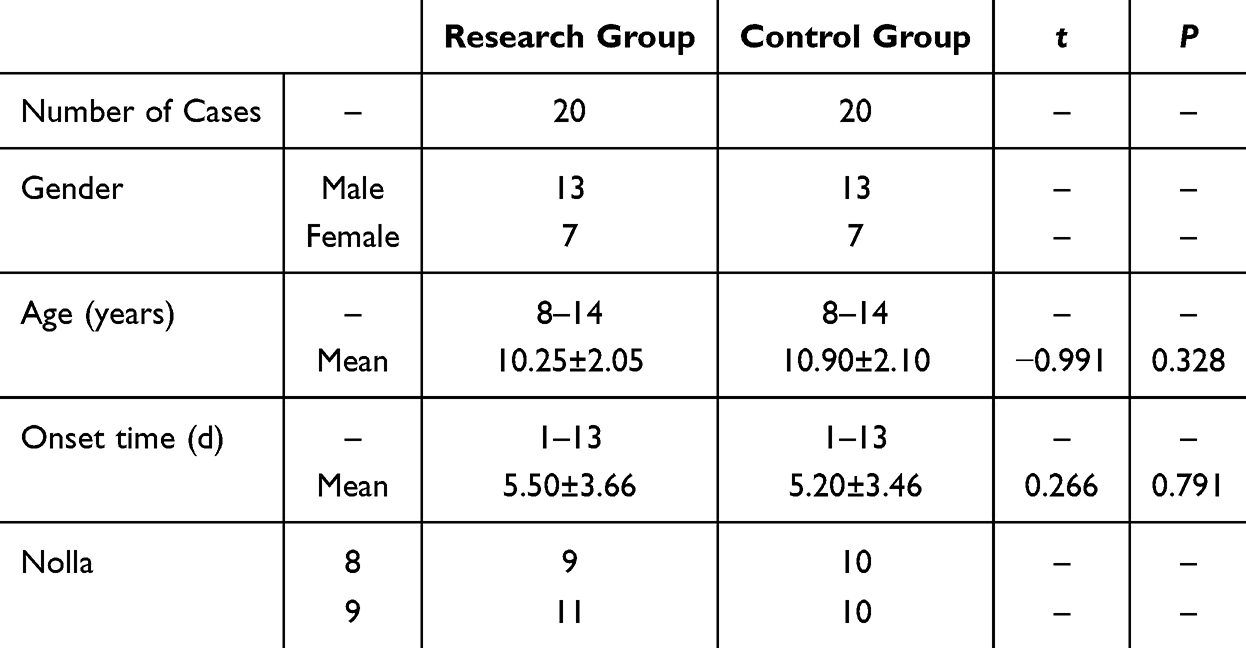 |
Table 1 Comparison of Clinical Data Between the Two Groups ( |

Treatment Effect
The clinical treatment outcomes differed significantly between the pulp revascularization surgery compared to the control group. In the research group, 16 out of 20 cases were classified as cured, 3 showed improvement, and only 1 case was deemed a failure. In contrast, the control group had 9 cured cases, 6 cases with improvement, and 5 treatment failures. The overall treatment effectiveness rate was notably higher in the research group at 95.00%, compared to 75.00% in the control group. Statistical analysis revealed a significant difference between the two groups (χ² = 5.891, P = 0.003), indicating that pulp revascularization was associated with a more favorable clinical outcome than apical induction surgery (Table 2). Taken together, the treatment effect in the study group was significantly better than that in the control group.
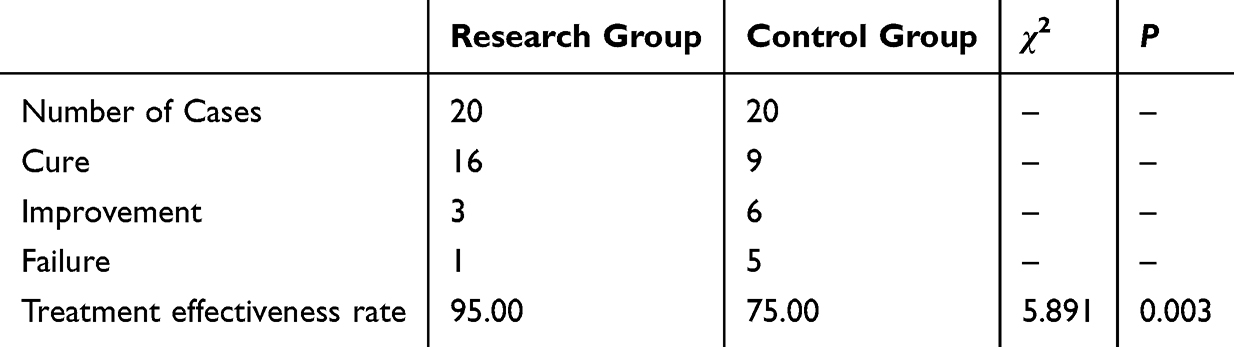 |
Table 2 Comparison of Clinical Treatment Effect Between the Two Groups (%) |
Clinical Indicators
Significant differences were observed in crown-to-root ratio and root canal wall thickness between the research group compared to the control group (Figure 1). After treatment, the crown-to-root ratio in the research group was significantly lower (0.68 ± 0.08) compared to the control group (0.79 ± 0.06, P < 0.05), indicating improved root development. Conversely, the root canal wall thickness was significantly greater in the research group (2.45 ± 0.37) than in the control group (2.30 ± 0.44, P < 0.05). These findings demonstrate that pulp revascularization surgery promoted more favorable anatomical outcomes in terms of both root elongation and canal wall reinforcement.
 |
Figure 1 Comparison of Clinical Indicators (Crown-to-Root Ratio, Root Canal Wall Thickness) Between the Two Groups. Note: *Indicates a significant difference between the two groups, P < 0.05. |
Pain Level
We conducted a detailed comparison of pain level classifications between the research (study) group and the control group. In the research group, 70.00% (14/20) of patients reported no pain (level 0), significantly higher than the 40.00% (8/20) in the control group. For mild pain (level 1), the research group had a lower incidence (20.00%, 4/20) compared to the control group (35.00%, 7/20), with statistical significance. The proportions of moderate pain (level 2) were comparable between groups (research: 10.00%, 2/20; control: 15.00%, 3/20), though not statistically significant. Notably, severe pain (level 3) was absent in the research group (0.00%) but reported in 10.00% (2/20) of the control group, a difference that was statistically significant. These results collectively demonstrated that the research group experienced significantly lower pain levels overall, with fewer cases of mild and severe pain, and a higher proportion of pain-free outcomes compared to the control group (Table 3).
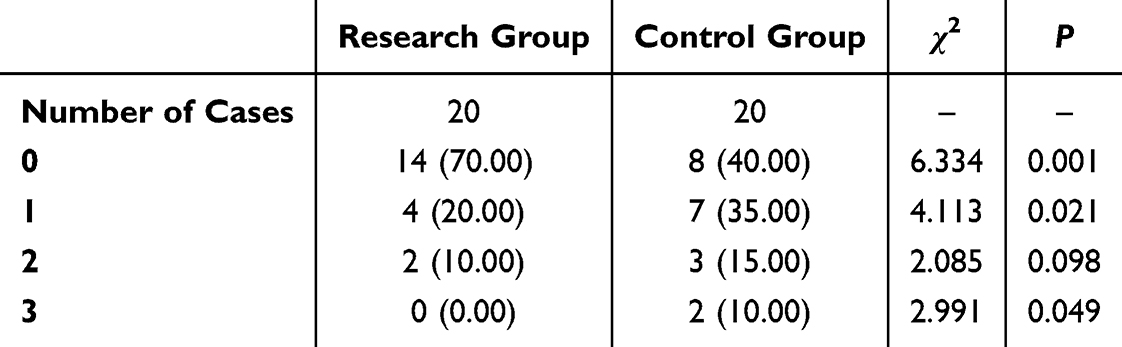 |
Table 3 Comparison of Pain Level Classification Between the Two Groups (%) |
Satisfaction
We compared the clinical outcomes between the research group (patients who underwent pulp revascularization surgery) and the control group (patients who received apical induction surgery) across four parameters: occlusion, chewing function, color shade, and overall aesthetics. Satisfaction levels were significantly higher in the research group compared to the control group. Specifically, the mean scores for occlusion, chewing function, color shade, and overall aesthetics were consistently higher in the research group than in the control group, with all differences reaching statistical significance (p < 0.05). These findings suggests that pulp revascularization provided superior functional and aesthetic outcomes from the perspective of both patients and their families (Figure 2).
 |
Figure 2 Comparison of Satisfaction Between Patients and Their Families in the Two Groups. Note: *Indicates a significant difference between the two groups, P < 0.05. |
Discussion
Pulp revascularization is an advanced regenerative technique that restores blood supply to damaged pulp using microvascular surgery, often involving autologous/allogeneic vessel and nerve transplantation.13,14 Particularly beneficial for young patients, it prevents developmental abnormalities and tooth discoloration from necrosis. The procedure involves meticulous evaluation, imaging, and surgical planning to optimize outcomes.15,16
Trauma-induced pulp necrosis in young permanent anterior teeth presents a significant clinical challenge. Pulp revascularization emerges as an innovative solution, demonstrating notable functional improvements in treated cases.17 The study revealed substantial postoperative enhancements in both occlusal function and mastication capacity, indicating this technique achieves not merely pulp repair but complete dental functional restoration. Critically, the induction of hard tissue formation and mineralization—a hallmark of successful revascularization—plays a pivotal role in this process. By stimulating the deposition of dentin-like tissue and reinforcing root structure, this method ensures long-term tooth preservation, addressing a key limitation of traditional endodontic treatments that sacrifice vitality for infection control.
The successful application of pulp revascularization offers better oral functionality for young patients and is expected to have a positive impact on their quality of life. Clinically, the success of revascularization is accomplished through a coordinated biological process: the synergistic action of stem cells promotes continued root development and regeneration of dentin-like tissue, while the formation of a blood clot scaffold provides a niche for cell migration and proliferation. Chemical disinfection of the root canal and the application of MTA sealant further create an optimal microenvironment for tissue regeneration.18 This method’s unique ability to induce organized hard tissue mineralization—rather than mere repair—distinguishes it as a biologically superior alternative. The resulting tissue not only seals the root canal but also mimics natural dentinogenesis, ensuring structural integrity and reducing the risk of future fractures. The entire process hinges on three interconnected mechanisms: the formation of a blood clot scaffold, the recruitment of stem cells, and the activation of growth factors. Together, these mechanisms facilitate not just pulp vitality reconstruction but also the continuation of root development, a feature unattainable with conventional endodontics.19,20
In assessing the clinical application of pulp revascularization, we conducted a detailed study on the treatment efficacy. The results showed that in cases of pulp necrosis caused by trauma to young permanent anterior teeth, pulp revascularization demonstrated encouraging treatment efficacy. These results are consistent with previous studies and provide strong evidence for replacing traditional treatments in daily clinical practice.21,22
The present study confirmed a significantly higher clinical treatment effectiveness rate in the pulp revascularization group (95.00%) compared to the control group. This superior outcome reflects the regenerative nature of the procedure, which not only resolves infection but promotes continued root development and functional recovery. Radiographic analysis revealed significantly improved anatomical parameters in the research group, including a lower crown-to-root ratio and greater root canal wall thickness, which suggest more robust root maturation. These structural enhancements provide long-term biomechanical advantages and lower the risk of root fractures.
Pulp necrosis in young permanent teeth is a frequent problem, particularly in caries- or trauma-prone children, often hindering tooth development. As the tooth’s innermost layer, the pulp is vital for dentin formation, sensation, and vascular supply. Traditional apical induction therapy, though effective, has limited benefits for continued tooth growth.23,24 Concentrated growth factor (CGF), used in pulp revascularization, is derived from the patient’s blood and, like platelet rich fibrin (PRF), requires no thrombin or anticoagulants. However, CGF outperforms PRF in regeneration, featuring enhanced fibrin clots, growth factors, and cell activators. Studies show CGF’s growth factors promote cell proliferation and angiogenesis, aiding pulp function restoration. Its cytokines help revive pulp vitality, serving as autologous growth factors and mucosal resources while activating platelets and the coagulation system. The fibrin-rich clot and growth factors synergistically enhance dental tissue regeneration.25,26
Pain assessment further emphasized the benefits of revascularization, with significantly fewer cases of moderate to severe pain and a higher proportion of pain-free outcomes. These improvements not only reflect better biological healing but also enhance patient comfort and satisfaction. Additionally, subjective evaluations showed markedly higher satisfaction scores in terms of occlusion, function, aesthetics, and shade in the revascularization group, confirming its positive psychosocial impact. Collectively, these outcomes support the transition from traditional apexification techniques to biologically based regenerative therapies in pediatric endodontics.
In conclusion, this study evaluated and compared the clinical efficacy, anatomical outcomes, pain levels, and patient satisfaction between pulp revascularization surgery and apical induction surgery. The findings demonstrated that pulp revascularization yielded significantly more favorable clinical and anatomical outcomes, reduced pain, and higher satisfaction levels than apical induction, underscoring its therapeutic value in the management of immature permanent teeth with necrotic pulp.
Conclusion
In summary, pulp revascularization showed great promise in the clinical application for young permanent anterior teeth pulp necrosis caused by trauma. It effectively improved treatment outcomes, clinical indicators, reduces pain, and significantly enhances patient satisfaction. Through continuous research and practice, this treatment method will likely provide better oral health experiences for patients and drive development in the field of dentistry. However, it is important to note that pulp revascularization is still in the process of continuous development and refinement. Clinicians need to carefully select the indications during the procedure and make reasonable decisions based on the specific conditions of the patient. Additionally, long-term follow-up and monitoring are essential to ensure treatment efficacy. Through regular clinical examinations and imaging evaluations, we can better understand the development of the teeth after surgery and the treatment effects. This is crucial for adjusting treatment plans, addressing complications in a timely manner, and maintaining long-term efficacy.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Al-Manei KK, Alzaidi S, Almalki G, Al-Manei K, Almotairy N. Incidence and influential factors in pulp necrosis and periapical pathosis following indirect restorations: a systematic review and meta-analysis. BMC Oral Health. 2023;23(1):195. doi:10.1186/s12903-023-02826-1
2. Matoug‐Elwerfelli M, ElSheshtawy AS, Duggal M, Tong HJ, Nazzal H. Vital pulp treatment for traumatized permanent teeth: a systematic review. Int Endodontic J. 2022;55(6):613–629. doi:10.1111/iej.13741
3. Spinas E, Deias M, Mameli A, Giannetti L. Pulp canal obliteration after extrusive and lateral luxation in young permanent teeth: a scoping review. Eur J Paediatric Dent. 2021;22(1):55–60. doi:10.23804/ejpd.2021.22.01.10
4. Kratunova E, Silva D. Pulp therapy for primary and immature permanent teeth: an overview. Gen Dent. 2018;66(6):30–38.
5. Taha NA, Khazali MA. Partial pulpotomy in mature permanent teeth with clinical signs indicative of irreversible pulpitis: a randomized clinical trial. J Endod. 2017;43(9):1417–1421. doi:10.1016/j.joen.2017.03.033
6. Zaleckiene V, Peciuliene V, Brukiene V, Drukteinis S. Traumatic dental injuries: etiology, prevalence and possible outcomes. Stomatologija. 2014;16(1):7–14.
7. Bourguignon C, Cohenca N, Lauridsen E, et al. International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020;36(4):314–330. doi:10.1111/edt.12578
8. Seracchiani M, Miccoli G, Reda R, et al. A comprehensive in vitro comparison of mechanical properties of two rotary endodontic instruments. World J Dent. 2020;11(3):185–188. doi:10.5005/jp-journals-10015-1729
9. Songtrakul K, Azarpajouh T, Malek M, Sigurdsson A, Kahler B, Lin LM. Modified apexification procedure for immature permanent teeth with a necrotic pulp/apical periodontitis: a case series. J Endod. 2020;46(1):116–123. doi:10.1016/j.joen.2019.10.009
10. Barbosa WLDS, Paranhos LR, Dantas MVDB, et al. Efficacy of pulp revascularization in the treatment of apical periodontitis in mature necrotic teeth: an umbrella review. Aust Endod J. 2025. doi:10.1111/aej.12928
11. Nasrin T. Exploring regenerative endodontics: pulp revascularization as an alternative to root canal therapy. J Dent Care. 2024;1(2):43–48.
12. Panda P, Mishra L, Govind S, Panda S, Lapinska B. Clinical outcome and comparison of regenerative and apexification intervention in young immature necrotic teeth—A systematic review and meta-analysis. J Clin Med. 2022;11(13):3909. doi:10.3390/jcm11133909
13. Hameed MH, Gul M, Ghafoor R, Badar SB. Management of immature necrotic permanent teeth with regenerative endodontic procedures-a review of literature. J Pak Med Assoc. 2019;69(10):1514–1520.
14. Wei Y, Lyu P, Bi R, et al. Neural regeneration in regenerative endodontic treatment: an overview and current trends. Int J Mol Sci. 2022;23(24):15492. doi:10.3390/ijms232415492
15. Eramo S, Natali A, Pinna R, Milia E. Dental pulp regeneration via cell homing. Int Endodontic J. 2018;51(4):405–419. doi:10.1111/iej.12868
16. Xie Z, Shen Z, Zhan P, et al. Functional dental pulp regeneration: basic research and clinical translation. Int J Mol Sci. 2021;22(16):8991. doi:10.3390/ijms22168991
17. Krastl G, Weiger R, Ebeleseder K, Galler K. Present status and future directions: endodontic management of traumatic injuries to permanent teeth. Int Endodontic J. 2022;55:1003–1019. doi:10.1111/iej.13672
18. Macwan C, Deshpande A. Mineral trioxide aggregate (MTA) in dentistry: a review of literature. J Oral Res Rev. 2014;6(2):71–74. doi:10.4103/2249-4987.152914
19. Cehreli ZC, Unverdi GE, Ballikaya E. Deciduous tooth pulp autotransplantation for the regenerative endodontic treatment of permanent teeth with pulp necrosis: a case series. J Endod. 2022;48(5):669–674. doi:10.1016/j.joen.2022.01.015
20. Dudeja PG, Grover S, Srivastava D, Dudeja KK, Sharma V. Pulp revascularization-it’s your future whether you know it or not? J Clin Diagn Res. 2015;9(4):ZR01. doi:10.7860/JCDR/2015/10149.5768
21. Feitosa VP, Mota MNG, Vieira LV, et al. Dental pulp autotransplantation: a new modality of endodontic regenerative therapy—follow-up of 3 clinical cases. J Endod. 2021;47(9):1402–1408. doi:10.1016/j.joen.2021.06.014
22. Lin L, Ricucci D, Huang GJ. Regeneration of the dentine–pulp complex with revitalization/revascularization therapy: challenges and hopes. Int Endodontic J. 2014;47(8):713–724. doi:10.1111/iej.12210
23. Corbella S, Ferrara G, El Kabbaney A, Taschieri S. Apexification, apexogenesis and regenerative endodontic procedures: a review of the literature= Apecificazione, apicogenesi e procedure di rigenerazione endodontica: una revisione della letteratura. Minerva Stomatol. 2014;63(11/12):375–389.
24. Murray PE. Review of guidance for the selection of regenerative endodontics, apexogenesis, apexification, pulpotomy, and other endodontic treatments for immature permanent teeth. Int Endodontic J. 2023;56:188–199. doi:10.1111/iej.13809
25. Murray PE. Platelet-rich plasma and platelet-rich fibrin can induce apical closure more frequently than blood-clot revascularization for the regeneration of immature permanent teeth: a meta-analysis of clinical efficacy. Front Bioeng Biotechnol. 2018;6:139. doi:10.3389/fbioe.2018.00139
26. Plakwicz P, Cudziło D, Czochrowska EM, Gawron K, Kuc-Michalska M, Kukuła KT. Pulp revascularization after autotransplantation of the mandibular canines with partially resected roots: report of 5 cases with follow-ups between 26 and 80 months. J Endod. 2023;49(5):478–486. doi:10.1016/j.joen.2023.03.006
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.