")
Back to Journals » Journal of Pain Research » Volume 18
Comparison of Learning Curves and Clinical Outcomes in Unilateral Biportal Endoscopic Spinal Surgery Versus Percutaneous Transforaminal Endoscopic Surgery: A Cumulative Sum Analysis
Authors Yuan S , Chen R , Mei Y, Fan N, Wang T, Wang A, Du P, Xi Y, Zang L
Received 29 October 2024
Accepted for publication 27 January 2025
Published 6 February 2025 Volume 2025:18 Pages 631—642
DOI https://doi.org/10.2147/JPR.S485283
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Shuo Yuan,* Ruiyuan Chen,* Yuqi Mei,* Ning Fan, Tianyi Wang, Aobo Wang, Peng Du, Yu Xi, Lei Zang
Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lei Zang, Department of Orthopedics, Beijing Chaoyang Hospital, Capital Medical University, 5 JingYuan Road, Shijingshan District, Beijing, 100043, People’s Republic of China, Tel +86-10-51718268, Email [email protected]
Purpose: Endoscopic spine surgery has been widely performed to treat degenerative spinal diseases to mitigate the risks and complications associated with traditional open surgery. However, endoscopic procedures pose challenges, including a limited field of view and a restricted operating space, which can affect the surgeon’s learning curve. This study aimed to evaluate the learning curves for unilateral biportal endoscopic spinal surgery (UBESS) and percutaneous transforaminal endoscopic surgery (PTES) by performing cumulative sum (CUSUM) analysis and to assess their efficacies in managing degenerative spinal diseases.
Patients and Methods: This retrospective cohort study included 100 consecutive patients who underwent PTES and 100 consecutive patients who received UBESS. CUSUM analysis was conducted to assess the learning curve, with cutoff points used to categorize the early and late phases. These two phases were analyzed in terms of differences in operative time, hospital stay, complications, and patient-reported outcome measures (PROMs). Additionally, PROMs between the PTES and UBESS groups, which were performed by the same surgeon, were compared.
Results: CUSUM analysis revealed that the operative time for PTES and UBESS decreased after 35 and 28 cases, respectively. Both early- and late-phase cases exhibited significant improvement in all PROMs postoperatively. Furthermore, PROMs did not differ between patients who underwent PTES and those who underwent UBESS.
Conclusion: Both procedures achieved comparable clinical outcomes with low complication incidences. However, achieving proficiency in PTES required a learning curve of at least 35 cases, whereas that in UBESS required a minimum of 28 cases.
Keywords: learning curve, clinical outcome, unilateral biportal endoscopic spinal surgery, percutaneous transforaminal endoscopic surgery, cumulative sum analysis
Introduction
The prevalence of lumbar disc herniation (LDH) and lumbar spinal stenosis (LSS), which are common spinal diseases among older individuals, has been steadily increasing with the aging of the population.1,2 Herniated discs, abnormal fat accumulation, hyperplastic facet joints, and thickened ligamentum flavum (LF) cause spinal canal narrowing and/or nerve compression, resulting in symptoms such as intermittent claudication, lower limb radiation pain, and low back pain.1,3,4 Surgical intervention can provide rapid symptomatic relief in patients who are unresponsive to conservative treatments.5,6 Surgical options include traditional open surgery and minimally invasive endoscopic surgery. Traditional open surgery has demonstrated effectiveness, but it is associated with the disadvantages of extensive soft-tissue damage, heavy bleeding, and poor postoperative spinal stability.7–9
Percutaneous transforaminal endoscopy is a minimally invasive technique for treating LDH and LSS.10 This approach allows surgeons to directly access the lesion area through the intervertebral foramen, thereby minimizing damage to normal tissue.11 Percutaneous transforaminal endoscopic surgery (PTES) has shown therapeutic outcomes comparable to those of traditional open surgery while providing advantages such as reduced soft-tissue damage, lower postoperative pain, less bleeding, and a decreased risk of spinal instability.12–14 In recent years, the unilateral biportal endoscopy has been widely used for the treatment of LDH and LSS with satisfactory results.15–17 It is an effective combination of traditional open and endoscopic surgeries. Moreover, it is characterized by a familiar workspace, wide surgical field, and high operational flexibility for the surgeon.18,19
However, mastering these endoscopic procedures is difficult. These challenges originate from the limited endoscopic field of view20 and different surgical approaches. Unilateral biportal endoscopic spinal surgery (UBESS) has demonstrated efficacy comparable to that of PTES.21 However, no studies have focused on the learning curves of both PTES and UBESS performed by the same surgeon for treating LDH and LSS.
Therefore, in this study, we aimed to investigate the learning curves of PTES and UBESS by performing a cumulative sum (CUSUM) analysis of the operative time. Additionally, we compared the surgical data and clinical outcomes of both surgeries across various learning phases.
Methods
Patient Selection
We retrospectively analyzed consecutive patients who underwent minimally invasive spine surgery at our center from April 2023 to February 2024. The study included 100 consecutive patients who underwent PTES from April 5, 2023, to January 12, 2024, and 100 consecutive patients who underwent UBESS from May 12, 2023, to February 25, 2024. The same spine surgeon who had no prior experience in endoscopic surgery performed all the surgeries. This study was approved by the ethics committee of our hospital and was conducted in accordance with the guidelines of the Declaration of Helsinki. The ethics committee waived informed consent because this was a retrospective study.
The inclusion criteria were as follows: (1) symptoms of low back pain or lower limb radiation pain; (2) magnetic resonance imaging indicating LDH or LSS; (3) failure of conservative treatment for over three months; and (4) patients undergoing PTES or UBESS performed by the same surgeon. The exclusion criteria were: (1) lumbar spondylolisthesis greater than grade I; (2) history of lumbar spine surgery; (3) presence of spinal infection, tumor or tuberculosis; and (4) more than one surgical level.
Surgical Procedure
PTES
All procedures were performed under local anesthesia while the patient was in a prone position. The entry point was created 8–13 cm lateral to the spinal midline at the intervertebral level. Initially, a spinal needle was inserted into the facet joint and was subsequently replaced with a guidewire. Subsequently, an 8 mm working cannula was placed after expanding the surgical approach using serial hollow tapered cannulas. Next, a portion of the facet, including the capsule, and ventral and lateral sides of the superior articular process were removed using a burr saw to access the intraforaminal area. The resection range was enlarged to the medial side of the superior or partial inferior articular process, as necessary. Decompression was performed under direct vision with continuous irrigation. Osteophytes, thickened LF, perineural fat, and bulging disk surface were removed. The entire nerve root or dural sac was carefully probed to ensure complete decompression. Finally, a drain was placed, and the surgical incision was closed (Figure 1).
 |
Figure 1 Images from a patient treated with PTES. (A and B) Preoperative MRI showed L4–L5 LDH. (C) Puncturing through Kambin’s triangle. (D) Insertion of the working cannula. (E) Nerve root decompression. (F and G) Postoperative MRI showed that the L4–L5 herniated intervertebral disc had been removed. (H) Postoperative CT showed partial defect of facet joint. |
UBESS
All procedures were performed under general anesthesia while the patient was a prone position. Transverse incisions of 1–1.5 cm were established at the intersection of the upper and lower 1–1.5 cm of the target intervertebral space and the inner edge of the pedicle, respectively. The superior incision served as the channel for endoscope insertion, whereas the inferior incision was used for t surgical instrument insertion. A partial laminotomy was then performed. Portions of the inferior and superior laminae of the upper and lower lumbar spine, respectively, were removed using an electric drill. Subsequently, LF was removed. Osteophytes, perineural fat and herniated disc compressing the nerve were removed. The entire nerve root or dural sac was carefully probed to ensure complete decompression. Finally, a drain was placed, and the surgical incisions were closed (Figure 2).
 |
Figure 2 Images from a patient treated with UBESS. (A and B) Preoperative MRI showed L4–L5 LDH. (C) The position of the grinding drill was shown in the fluoroscopic view. (D) Nerve root decompression. (E) Herniated nucleus pulposus. (F and G) Postoperative MRI showed that the L4-L5 herniated intervertebral disc had been removed. (H) Postoperative CT showed defect of lamina after partial laminotomy. |
Data Collection
Demographic and clinical data, including age, sex, body mass index (BMI), surgical level, and approach side, from all patients were collected from medical records. Surgical data, including operative time, estimated volume of blood loss, hospital stay, and complications, were recorded postoperatively. Patient-reported outcome measures (PROMs) included visual analog scale (VAS) scores for low back pain and lower leg pain, Oswestry Disability Index (ODI) scores, and modified MacNab criteria. Patients were evaluated preoperatively, one month postoperatively, and at the final follow-up.
CUSUM Analysis
The CUSUM technique was used to analyze the operative time and quantify the learning curves of PTES and UBESS. This method involves iterative calculation and accumulation of the differences between individual data points and the mean of all data points. The formula is described as  .
.  represents the operative time for each sequential patient and U represents the mean operative time for the group of the patients. The scatter diagram of CUSUM analysis was drawn using Excel (Microsoft Excel 2010, version 14.0.6106.5005), and the function formula was established by curve fitting. The degree of curve fitting was judged by the coefficient R2, and the closer R2 was to 1, the higher the degree of curve fitting was. The model with the highest R2 was considered the best fitting model. The first derivation of the fitting curve was conducted, and the peak of the fitting curve was identified based on the slope value of the curve to categorize the learning phase accordingly. Additionally, we analyzed the presence of differences in demographic, clinical, surgical, and PROM data among patients at different phases.
represents the operative time for each sequential patient and U represents the mean operative time for the group of the patients. The scatter diagram of CUSUM analysis was drawn using Excel (Microsoft Excel 2010, version 14.0.6106.5005), and the function formula was established by curve fitting. The degree of curve fitting was judged by the coefficient R2, and the closer R2 was to 1, the higher the degree of curve fitting was. The model with the highest R2 was considered the best fitting model. The first derivation of the fitting curve was conducted, and the peak of the fitting curve was identified based on the slope value of the curve to categorize the learning phase accordingly. Additionally, we analyzed the presence of differences in demographic, clinical, surgical, and PROM data among patients at different phases.
Statistical Analysis
Statistical analysis was performed using SPSS 26.0 software (IBM SPSS 26.0, SPSS Inc). Intergroup comparisons were performed using independent samples t-tests and chi-square tests, whereas intragroup comparisons were performed using paired t-tests. A P-value < 0.05 was considered statistically significant.
Results
Characteristics of Patients
This study enrolled 200 patients, including 49 males and 51 females in the PTES group and 46 males and 54 females in the UBESS group. The mean ages were 62.12 ± 13.29 years and 61.50 ± 13.82 years in the PTES and UBESS groups, respectively. The mean BMIs were 25.87 ± 3.73 kg/m2 and 25.96 ± 3.54 kg/m2 in the PTES and UBESS groups, respectively. The surgical levels of L2–L4, L4–L5, and L5–S1 included 8, 66, and 26 cases in the PTES group and 13, 52, and 35 cases in the UBESS group, respectively. The average follow-up duration was 11.95 ± 3.12 months. No significant differences were observed between the two groups in terms of demographic and clinical data (Table 1).
 |
Table 1 Demographic and Clinical Information of Patients |
CUSUM Analysis
The CUSUM analysis revealed that the cutoff values for mastering PTES and UBESS were 35 (Figure 3) and 28 cases (Figure 4), respectively. Consequently, the PTES and UBESS groups were categorized into early phases (PTES: n = 35; UBESS: n = 28) and late phases (PTES: n = 65; UBESS: n = 72) according to the apex of the curves, respectively.
 |
Figure 3 CUSUM analysis of PTES group. |
 |
Figure 4 CUSUM analysis of UBESS group. |
Comparison of Early- and Late-Phase Cases
In PTES group, the operative time was significantly shorter in the late phase than that in the early phase (87.27 ± 13.36 min vs 121.82 ± 18.71 min, P < 0.001). Furthermore, no significant differences were observed in estimated blood loss (5.32 ± 6.15 mL vs 7.59 ± 6.06 mL, P = 0.068), complications (4 cases vs 4 cases, P = 0.722), and hospital stay (6.07 ± 3.82 days vs 5.64 ± 4.92 days, P = 0.619) (Table 2). The VAS and ODI scores were significantly improved at the final follow-up compared with those at the preoperative period (P < 0.05). However, no statistically significant differences were observed in these scores between the early and late groups of patients during preoperative, one-month postoperative, and final follow-up evaluations (P > 0.05). In the PTES group, surgical complications occurred in eight patients (8%), including five residual discs (15th, 29th, 54th, 64th, and 83rd), two recurrences (17th and 18th), and one inadequate decompression (79th).
 |
Table 2 Comparison of Surgical Data and Clinical Outcomes at Different Phases of PTES |
In the UBESS group, the operative time was significantly shorter in the late phase than that in the early phase (99.61 ± 16.43 min vs 155.42 ± 27.66 min, P < 0.001). However, there were no significant differences in the estimated blood loss volume (34.61 ± 26.83 mL vs 44.17 ± 28.65 mL, P = 0.137), complications (2 cases vs 5 cases, P = 0.769), and hospital stay (7.18 ± 4.06 days vs 8.63 ± 4.06 days, P = 0.133) (Table 3). The VAS and ODI scores were significantly improved at the final follow-up compared with those at the preoperative period (P < 0.05). However, there were no statistically significant differences in these scores between the early and late groups of patients during preoperative, one-month postoperative, and final follow-up evaluations (P > 0.05). In the UBESS group, seven patients (7%) experienced surgical complications, including five dural tears (7th, 23rd, 38th, and 75th), one epidural hematoma (69th), and one isthmus fracture (55th).
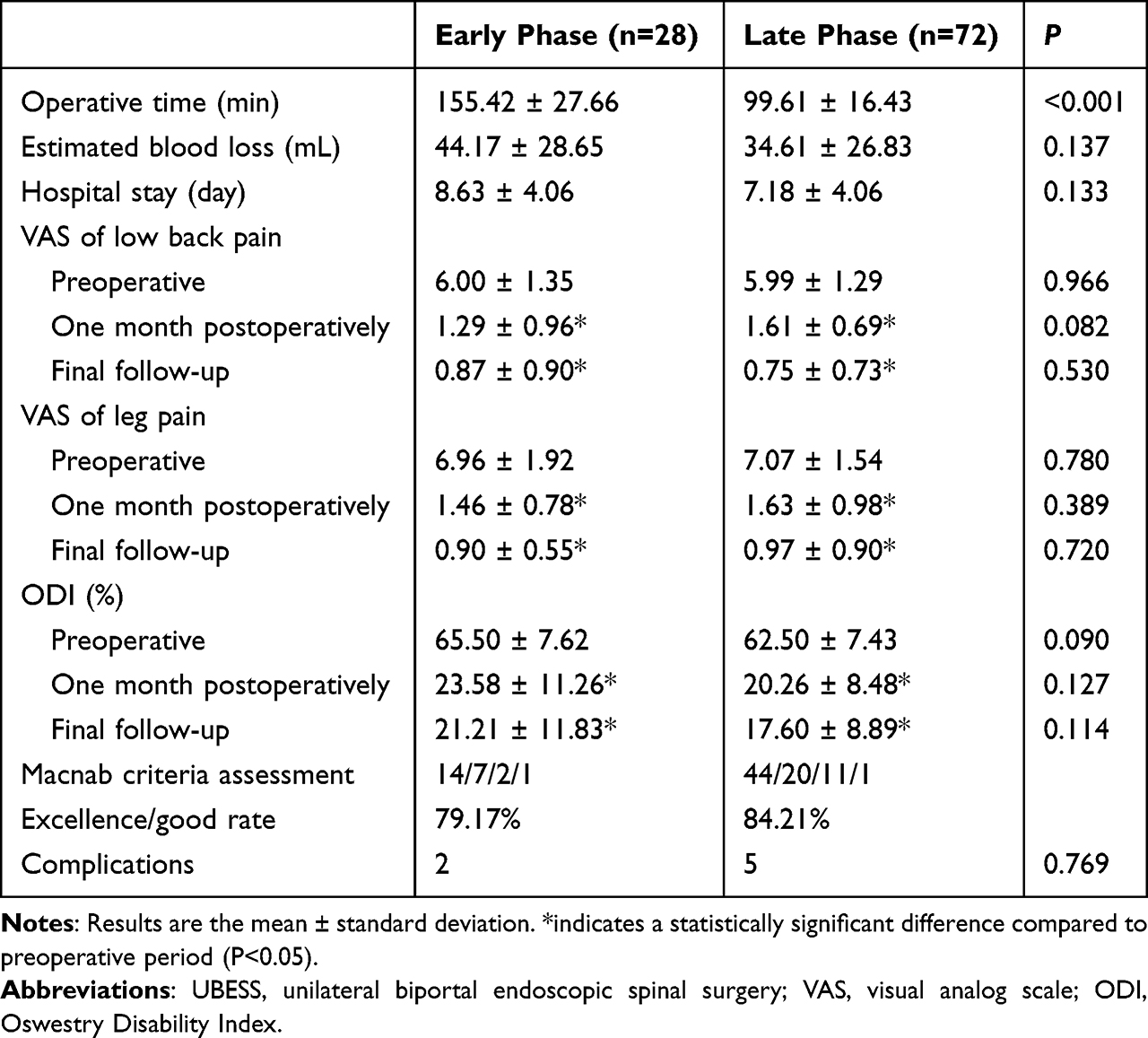 |
Table 3 Comparison of Surgical Data and Clinical Outcomes at Different Phases of UBESS |
Comparison Between PTES and UBESS Group
The PTES group had a significantly shorter operative time (102.47 ± 23.42 min vs 113.00 ±30.92 min, P = 0.007) and lower estimated blood loss volume (6.32 ± 6.15 mL vs 36.90 ± 27.44 mL, P < 0.001) than those in the UBESS group (Table 4). However, there was no significant difference in complications between the two groups (P > 0.05). The PTES group had a shorter hospital stay (6.70 ± 8.35 days vs 7.53 ± 4.09 days, P = 0.373) but with no statistical significance.
 |
Table 4 Comparison of Surgical Data and Clinical Outcomes Between PTES and UBESS |
Postoperative VAS and ODI scores significantly decreased in both groups compared with preoperative scores (P < 0.05). No significant differences were found between the two groups during preoperative, one-month postoperative, and final follow-up evaluations (P > 0.05). According to the MacNab criteria, the patient satisfaction rates were 83.93% and 84.09% in the UBESS and PTES groups, respectively, with no significant difference between them (P > 0.05).
Discussion
Endoscopic spine surgery been widely performed in recent years to prevent the risks and complications associated with traditional open surgery. However, endoscopic procedures are characterized by a limited field of view and a restricted operating space, which pose challenges to the surgeon’s learning curve. Operative time is frequently used as an indicator of a surgeon’s proficiency.22 In this study, we conducted CUSUM analysis, which is an average-based test method, to investigate the learning curves of PTES and UBESS based on the operative time.
PTES and UBESS for treating degenerative spinal diseases exhibited the advantages of small incisions, minimal local damage, and rapid recovery.1 PTES is performed under local anesthesia, which allows the patient to remain awake and communicate with the surgeon, thereby reducing the risk of nerve root damage. The PTES approach involves accessing the spinal canal through the intervertebral foramina via Kambin’s triangle, which is less disruptive to the synovial joints and prevents postoperative spinal instability. Additionally, LF preservation reduces postoperative perineural adhesions and scar formation. UBESS requires two channels in the posterior lumbar spine adjacent to the spinous processes, one for endoscopic observation and the other for instrumentation. Notably, UBESS allows the establishment of portals through the skin without using a cannula, thereby enabling a wider range of instrument movement, facilitating easier endoscopic manipulation, and allowing thorough decompression.1 However, each procedure presents unique challenges, including accurate and safe insertion of the working tube in PTES and manual creation of the working space in UBESS.
The learning curve reflects the rate of skill acquisition over a certain period and is usually determined by the number of surgical cases required for a beginner to reach relative proficiency.23,24 Previous studies investigated the learning curves of PTES20,23,25 or UBESS,1,26,27 with cutoff values of 25–54 and 24–54 cases, respectively. Li et al conducted the first comparative study on the learning curves of PTES and UBESS for treating LDH by the same surgeon, determining cutoff points of 40 and 15 cases for the two phases of the learning process, respectively.28 Although this study is significant, we consider that cases often involve both LDH and LSS in practical learning scenarios. Thus, a margin of error exists when analyzing the learning curve for treating LDH alone because the surgeon simultaneously gains experience in treating LDH while performing procedures for LSS. Consequently, Consequently, the design of our study are consistent with those in clinical practice. We thoroughly analyzed and summarized objective and reproducible experiences from all cases, particularly those with complications, to provide technical references for surgeons who are interested in spinal endoscopic techniques and to reduce unnecessary learning costs.
The CUSUM analysis revealed that the cutoff values for overcoming the learning curve were 35 and 28 cases for PETS and UBESS, respectively. The average operative time in the late phase was approximately 34 min shorter than that in the early phase in the PTES group (121.82 min vs 87.27 min), and the UBESS group exhibited a reduction of approximately 55 min (155.42 min vs 99.61 min). Numerous factors contribute to these differences. First, PTES uses an intervertebral foraminal approach, which involves a complex anatomical structure that makes it very difficult to accurately place the working channel into the surgical area, particularly in the L5–S1 level, where iliac crest obstruction increases the difficulty of placement and adjustment of the working channel. In addition, PTES requires the use of specialized surgical instruments, which further increases the difficulty of mastering this technique. Conversely, UBESS involves a posterior approach, similar to traditional open surgery, which makes it easier for surgeons experienced in open surgery to learn and master the technique.
Our study showed that PROMs at the final follow-up were significantly improved in both the PTES and UBESS groups compared with those in the preoperative period, indicating that satisfactory clinical outcomes were achieved in both groups. Furthermore, the modified MacNab criteria indicated comparable efficacy between the two groups, which is consistent with that reported in previous studies.21,29 However, UBESS was associated with significantly higher bleeding volume and longer operative time than those in PTES. Zhang et al demonstrated that bleeding was frequently underestimated in minimally invasive spine surgery because the procedures were performed under continuous saline irrigation, resulting in a lower intraoperative assessment of bleeding than the actual volume.30 UBESS requires a laminectomy to create a surgical approach, whereas PTES enables direct access to the spinal canal through the intervertebral foramina without extensive destruction of bone and muscle tissues. This difference in surgical approach may be associated with the significant variations in blood loss volume and operative time between the two procedures.
Dural tears are the most common complications of UBESS.31 Of the patients treated with UBESS, five (5%) developed dural tears due to radiofrequency use. The mean age of these five patients was 73.4 years, which was higher than the mean age of the UBESS group. The LF appears to be thicker in the older individuals,32 and presence of adhesions between the LF and the dural sac may reduce the available surgical space. One patient in UBESS group experienced an epidural hematoma at the late phase. Kim et al emphasized that high intraoperative water pressure may obscure bleeding from epidural vessels or bone, indicating the need for careful water pressure control during the procedure.33 Additionally, one patient developed a postoperative isthmus fracture, which was potentially caused by excessive intraoperative bone removal and postoperative overexertion. Incomplete decompression, residual discs, and recurrence are significant complications of PTES. This study revealed that two patients experienced postoperative recurrence and five patients had residual discs. The complete herniated disc removal is related to the position of the working cannula, type of disc herniation, and size of herniated fragments.34 Maayan et al suggested that more intraoperative fluoroscopies are required in the early phase of PTES to determine the correct cannula position.20 In this study, both recurrences occurred in the early phase of the PTES group. Yao et al determined less experience as a unique risk factor for LDH recurrence.35 Operative time is a crucial indicator of surgeon’s proficiency, but evaluating the learning curve should also consider procedural safety. In our study, no significant difference was found in the incidence of surgical complications across different phases of both the PTES and UBESS groups, which is consistent with those of the previous studies.27,28,36
We agree with the following recommendations regarding shortening the learning curves of PTES and UBESS and reducing the incidence of surgical complications. First, comprehensive training is crucial and should include theoretical courses, watching surgical videos, practicing on fresh cadavers, and observing real surgeries.37 Second, surgeons should begin with simple cases in the initial phase and operate under the supervision of an experienced surgeon to obtain adequate experience.38,39 Additionally, strict adherence to surgical indications is crucial. Deviating from these guidelines can cause surgical failures and prolongs the learning curve. Finally, surgeons should systematically review and analyze each case, particularly those with surgical complications, to improve their skills and competence.
One limitation of this study is that the same surgeon performed all procedures, and the learning curve of a single surgeon may not accurately represent the learning curve of other surgeons. Additionally, this was a retrospective study with a short postoperative follow-up period. Moreover, factors, such as access to training, team consistency, and equipment availability, may affect the learning curve. Multicenter prospective studies with a larger cohort of surgeons are necessary to confirm our findings.
Conclusion
This study analyzed the learning curves of PTES and UBESS by conducting a CUSUM analysis based on the operative time. The results indicated that 28 and 35 cases were required to master UBESS and PTES, respectively. Both procedures resulted in satisfactory clinical outcomes, and the learning process did not result in higher complication rates. Comprehensive training, appropriate case selection, strict surgical indication control, and timely experience summarization can help shorten the learning curve.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The research conducted has been performed in accordance with the Declaration of Helsinki. Approval for the study was obtained from the ethics committees of the Beijing Chaoyang Hospital (2021-KE-478). Informed consent to this study was waived because of this was a retrospective study, which was also approved by the institutional ethical review board. All patients’ data involved in this paper is guaranteed to be kept strictly confidential.
Funding
There is no funding that supported this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Xu J, Wang D, Liu J, et al. Learning curve and complications of unilateral biportal endoscopy: cumulative sum and risk-adjusted cumulative sum analysis. Neurospine. 2022;19(3):792–804. doi:10.14245/ns.2143116.558
2. Zaina F, Tomkins-Lane C, Carragee E, Negrini S. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst Rev. 2016;2016(1):Cd010264. doi:10.1002/14651858.CD010264.pub2
3. van der Windt DA, Simons E, Riphagen II, et al. Physical examination for lumbar radiculopathy due to disc herniation in patients with low-back pain. Cochrane Database Syst Rev. 2010;(2):Cd007431. doi:10.1002/14651858.CD007431.pub2
4. Kim K, Mendelis J, Cho W. Spinal epidural lipomatosis: a review of pathogenesis, characteristics, clinical presentation, and management. Global Spine J. 2019;9(6):658–665. doi:10.1177/2192568218793617
5. Lorio M, Kim C, Araghi A, Inzana J, Yue JJ. International society for the advancement of spine surgery policy 2019-surgical treatment of lumbar disc herniation with radiculopathy. Int J Spine Surg. 2020;14(1):1–17. doi:10.14444/7001
6. Phillips FM, Slosar PJ, Youssef JA, Andersson G, Papatheofanis F. Lumbar spine fusion for chronic low back pain due to degenerative disc disease: a systematic review. Spine. 2013;38(7):E409–22. doi:10.1097/BRS.0b013e3182877f11
7. Chiu RG, Patel S, Zhu A, Aguilar E, Mehta AI. Endoscopic versus open laminectomy for lumbar spinal stenosis: an international, multi-institutional analysis of outcomes and adverse events. Global Spine J. 2020;10(6):720–728. doi:10.1177/2192568219872157
8. Jung B, Han J, Song J, Ngan A, Essig D, Verma R. Interventional therapy and surgical management of lumbar disc herniation in spine surgery: a narrative review. Orthop Rev. 2023;15:88931. doi:10.52965/001c.88931
9. Park Y, Ha JW. Comparison of one-level posterior lumbar interbody fusion performed with a minimally invasive approach or a traditional open approach. Spine. 2007;32(5):537–543. doi:10.1097/01.brs.0000256473.49791.f4
10. Chen F, Xin J, Su C, Liu X, Cui X. Pain variability of tissues under endoscope in percutaneous endoscopic lumbar discectomy and its significance: a retrospective study. Pain Physician. 2021;24(6):E877–e882.
11. Ahn Y, Lee S, Son S, Kim H, Kim JE. Learning curve for transforaminal percutaneous endoscopic lumbar discectomy: a systematic review. World Neurosurg. 2020;143:471–479. doi:10.1016/j.wneu.2020.08.044
12. Jang JW, Lee DG, Park CK. Rationale and advantages of endoscopic spine surgery. Int J Spine Surg. 2021;15(suppl 3):S11–s20. doi:10.14444/8160
13. Hwa Eum J, Hwa Heo D, Son SK, Park CK. Percutaneous biportal endoscopic decompression for lumbar spinal stenosis: a technical note and preliminary clinical results. J Neurosurg Spine. 2016;24(4):602–607. doi:10.3171/2015.7.Spine15304
14. Yang JS, Chu L, Chen CM, et al. Foraminoplasty at the tip or base of the superior articular process for lateral recess stenosis in percutaneous endoscopic lumbar discectomy: a multicenter, retrospective, controlled study with 2-year follow-up. Biomed Res Int. 2018;2018:7692794. doi:10.1155/2018/7692794
15. Heo DH, Lee DC, Park CK. Comparative analysis of three types of minimally invasive decompressive surgery for lumbar central stenosis: biportal endoscopy, uniportal endoscopy, and microsurgery. Neurosurg Focus. 2019;46(5):E9. doi:10.3171/2019.2.Focus197
16. Park MK, Son SK, Park WW, Choi SH, Jung DY, Kim DH. Unilateral biportal endoscopy for decompression of extraforaminal stenosis at the lumbosacral junction: surgical techniques and clinical outcomes. Neurospine. 2021;18(4):871–879. doi:10.14245/ns.2142146.073
17. He Y, Wang H, Yu Z, Yin J, Jiang Y, Zhou D. Unilateral biportal endoscopic versus uniportal full-endoscopic for lumbar degenerative disease: a meta-analysis. J Orthop Sci. 2024;29(1):49–58. doi:10.1016/j.jos.2022.10.019
18. Lin GX, Huang P, Kotheeranurak V, et al. A systematic review of unilateral biportal endoscopic spinal surgery: preliminary clinical results and complications. World Neurosurg. 2019;125:425–432. doi:10.1016/j.wneu.2019.02.038
19. Min WK, Kim JE, Choi DJ, Park EJ, Heo J. Clinical and radiological outcomes between biportal endoscopic decompression and microscopic decompression in lumbar spinal stenosis. J Orthop Sci. 2020;25(3):371–378. doi:10.1016/j.jos.2019.05.022
20. Maayan O, Pajak A, Shahi P, et al. Percutaneous transforaminal endoscopic discectomy learning curve: a CuSum analysis. Spine. 2023;48(21):1508–1516. doi:10.1097/brs.0000000000004730
21. Jiang HW, Chen CD, Zhan BS, Wang YL, Tang P, Jiang XS. Unilateral biportal endoscopic discectomy versus percutaneous endoscopic lumbar discectomy in the treatment of lumbar disc herniation: a retrospective study. J Orthop Surg Res. 2022;17(1):30. doi:10.1186/s13018-022-02929-5
22. Sclafani JA, Kim CW. Complications associated with the initial learning curve of minimally invasive spine surgery: a systematic review. Clin Orthop Relat Res. 2014;472(6):1711–1717. doi:10.1007/s11999-014-3495-z
23. Sun B, Shi C, Xu Z, et al. Learning curve for percutaneous endoscopic lumbar diskectomy in Bi-needle technique using cumulative summation test for learning curve. World Neurosurg. 2019;129:e586–e593. doi:10.1016/j.wneu.2019.05.227
24. Sun B, Wu H, Xu Z, et al. Is selective nerve root block necessary for learning percutaneous endoscopic lumbar discectomy: a comparative study using a cumulative summation test for learning curve. Int Orthop. 2020;44(7):1367–1374. doi:10.1007/s00264-020-04558-1
25. Son S, Ahn Y, Lee SG, et al. Learning curve of percutaneous endoscopic transforaminal lumbar discectomy by a single surgeon. Medicine. 2021;100(4):e24346. doi:10.1097/md.0000000000024346
26. Chen L, Zhu B, Zhong HZ, et al. The learning curve of unilateral biportal endoscopic (UBE) spinal surgery by CUSUM analysis. Front Surg. 2022;9:873691. doi:10.3389/fsurg.2022.873691
27. Park SM, Kim HJ, Kim GU, et al. Learning curve for lumbar decompressive laminectomy in biportal endoscopic spinal surgery using the cumulative summation test for learning curve. World Neurosurg. 2019;122:e1007–e1013. doi:10.1016/j.wneu.2018.10.197
28. Li Z, Yang H, Zhang Y, et al. Percutaneous endoscopic transforaminal discectomy and unilateral biportal endoscopic discectomy for lumbar disc herniation: a comparative analysis of learning curves. Eur Spine J. 2024;33(6):2154–2165. doi:10.1007/s00586-024-08293-8
29. Cheng X, Wu Y, Chen B, Tang J. A comparative study of unilateral biportal endoscopic decompression and percutaneous transforaminal endoscopic decompression for geriatric patients with lumbar lateral recess stenosis. J Pain Res. 2023;16:2241–2249. doi:10.2147/jpr.S413502
30. Zhang H, Chen ZX, Sun ZM, et al. Comparison of the total and hidden blood loss in patients undergoing open and minimally invasive transforaminal lumbar interbody fusion. World Neurosurg. 2017;107:739–743. doi:10.1016/j.wneu.2017.08.113
31. Liang J, Lian L, Liang S, et al. Efficacy and complications of unilateral biportal endoscopic spinal surgery for lumbar spinal stenosis: a meta-analysis and systematic review. World Neurosurg. 2022;159:e91–e102. doi:10.1016/j.wneu.2021.12.005
32. de Divitiis E, Cappabianca P. Preserving the ligamentum flavum in lumbar discectomy: a new technique that prevents scar tissue formation in the first 6 months postsurgery. Neurosurgery. 2007;61(6):E1340. doi:10.1227/01.neu.0000306128.54281.7d
33. Kim W, Kim SK, Kang SS, Park HJ, Han S, Lee SC. Pooled analysis of unsuccessful percutaneous biportal endoscopic surgery outcomes from a multi-institutional retrospective cohort of 797 cases. Acta Neurochir. 2020;162(2):279–287. doi:10.1007/s00701-019-04162-2
34. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–56.
35. Yao Y, Liu H, Zhang H, et al. Risk factors for recurrent herniation after percutaneous endoscopic lumbar discectomy. World Neurosurg. 2017;100:1–6. doi:10.1016/j.wneu.2016.12.089
36. Choi DJ, Choi CM, Jung JT, Lee SJ, Kim YS. Learning curve associated with complications in biportal endoscopic spinal surgery: challenges and strategies. Asian Spine J. 2016;10(4):624–629. doi:10.4184/asj.2016.10.4.624
37. Wang H, Huang B, Li C, et al. Learning curve for percutaneous endoscopic lumbar discectomy depending on the surgeon’s training level of minimally invasive spine surgery. Clin Neurol Neurosurg. 2013;115(10):1987–1991. doi:10.1016/j.clineuro.2013.06.008
38. Choi G, Lee SH, Raiturker PP, Lee S, Chae YS. Percutaneous endoscopic interlaminar discectomy for intracanalicular disc herniations at L5-S1 using a rigid working channel endoscope. Neurosurgery. 2006;58(1 Suppl):ONS59–68;discussionONS59–68. doi:10.1227/01.neu.0000192713.95921.4a
39. Ruetten S, Komp M, Merk H, Godolias G. Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J Neurosurg Spine. 2007;6(6):521–530. doi:10.3171/spi.2007.6.6.2
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.